BAXFENDY- baxdrostat tablet, film coated
Drug Labeling and Warnings
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use BAXFENDY safely and effectively. See full prescribing information for BAXFENDY.
BAXFENDY™ (baxdrostat) tablets, for oral use
Initial U.S. Approval: 2026INDICATIONS AND USAGE
BAXFENDY is an aldosterone synthase inhibitor indicated for the treatment of hypertension in combination with other antihypertensive drugs, to lower blood pressure in adults who are not adequately controlled on other agents. Lowering blood pressure reduces the risk of fatal and nonfatal cardiovascular events, primarily strokes and myocardial infarctions. (1)
DOSAGE AND ADMINISTRATION
DOSAGE FORMS AND STRENGTHS
Tablets: 1 mg and 2 mg (3)
CONTRAINDICATIONS
None. (4)
WARNINGS AND PRECAUTIONS
- Hyperkalemia: Assess serum potassium before initiation and periodically thereafter. Assess more frequently in patients at increased risk of hyperkalemia. (5.1)
- Hyponatremia: Assess serum sodium before initiation and periodically thereafter. Assess more frequently in patients at increased risk of hyponatremia. (5.2)
ADVERSE REACTIONS
The most common adverse reaction (more frequent than placebo and ≥ 5% in BAXFENDY-treated patients) was hyperkalemia. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact AstraZeneca at 1-800-236-9933 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.
Revised: 5/2026
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Testing Prior to and After Initiation of BAXFENDY
2.2 Recommended Dosage
2.3 Administration Instructions
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Hyperkalemia
5.2 Hyponatremia
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
7 DRUG INTERACTIONS
7.1 Drugs That Increase Serum Potassium
7.2 Effect of Other Drugs on BAXFENDY
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.4 Pediatric Use
8.5 Geriatric Use
8.6 Renal Impairment
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 How Supplied
16.2 Storage and Handling
17 PATIENT COUNSELING INFORMATION
- * Sections or subsections omitted from the full prescribing information are not listed.
-
1 INDICATIONS AND USAGE
BAXFENDY, in combination with other antihypertensive drugs, is indicated for the treatment of hypertension, to lower blood pressure in adults who are not adequately controlled on other agents. Lowering blood pressure reduces the risk of fatal and nonfatal cardiovascular events, primarily strokes and myocardial infarctions. These benefits have been seen in controlled trials of antihypertensive drugs from a wide variety of pharmacologic classes. There are no controlled trials demonstrating risk reduction of these events with BAXFENDY.
Control of high blood pressure should be part of comprehensive cardiovascular risk management, including, as appropriate, lipid control, diabetes management, antithrombotic therapy, smoking cessation, exercise, and limited sodium intake. Many patients will require more than one drug to achieve blood pressure goals. For specific advice on goals and management, see published guidelines, such as those of the American College of Cardiology/American Heart Association (ACC/AHA).
Numerous antihypertensive drugs, from a variety of pharmacologic classes and with different mechanisms of action, have been shown in randomized controlled trials to reduce cardiovascular morbidity and mortality, and it can be concluded that it is blood pressure reduction, and not some other pharmacologic property of the drugs, that is largely responsible for those benefits. The largest and most consistent cardiovascular outcome benefit has been a reduction in the risk of stroke, but reductions in myocardial infarction and cardiovascular mortality also have been seen regularly.
Elevated systolic or diastolic pressure causes increased cardiovascular risk, and the absolute risk increase per mmHg is greater at higher blood pressures, so that even modest reductions of severe hypertension can provide substantial benefit. Relative risk reduction from blood pressure reduction is similar across populations with varying absolute risk, so the absolute benefit is greater in patients who are at higher risk independent of their hypertension (for example, patients with diabetes or hyperlipidemia), and such patients would be expected to benefit from more aggressive treatment to a lower blood pressure goal.
-
2 DOSAGE AND ADMINISTRATION
2.1 Testing Prior to and After Initiation of BAXFENDY
Consider the patient’s risk of hyperkalemia and hyponatremia before initiating BAXFENDY. Assess serum potassium and sodium before initiation of BAXFENDY and periodically thereafter. Correct serum potassium and sodium abnormalities prior to initiation of BAXFENDY [see Warnings and Precautions (5.1, 5.2)].
2.2 Recommended Dosage
The recommended dosage of BAXFENDY is 2 mg orally once daily.
For patients at increased risk of hyperkalemia or hyponatremia, the recommended dosage is 1 mg orally once daily [see Warnings and Precautions (5.1, 5.2)].
- 3 DOSAGE FORMS AND STRENGTHS
- 4 CONTRAINDICATIONS
-
5 WARNINGS AND PRECAUTIONS
5.1 Hyperkalemia
BAXFENDY can cause hyperkalemia [see Adverse Reactions (6.1)].
Assess serum potassium prior to initiation of BAXFENDY and monitor periodically during treatment. Correct serum potassium abnormalities prior to initiation of BAXFENDY [see Dosage and Administration (2.1, 2.2)]. More frequent monitoring is recommended for patients at increased risk of hyperkalemia (e.g., patients ≥ 65 years of age, those with diabetes mellitus or chronic kidney disease, and those receiving concomitant medications that increase serum potassium) [see Drug Interactions (7.1) and Geriatric Use (8.5)].
If hyperkalemia occurs, treat hyperkalemia and consider interrupting or discontinuing BAXFENDY. Consider more frequent monitoring of serum potassium in patients who restart BAXFENDY after experiencing hyperkalemia. Permanently discontinue BAXFENDY if clinically significant hyperkalemia recurs.
5.2 Hyponatremia
BAXFENDY can cause hyponatremia [see Adverse Reactions (6.1)].
Assess serum sodium prior to initiation of BAXFENDY and monitor periodically during treatment. Correct serum sodium abnormalities prior to initiation of BAXFENDY [see Dosage and Administration (2.1, 2.2)]. More frequent monitoring is recommended for patients with low baseline serum sodium concentrations and those at risk of hyponatremia, such as those receiving concomitant medications that may cause hyponatremia.
If clinically significant hyponatremia occurs, treat the hyponatremia and consider interrupting or discontinuing BAXFENDY. Consider more frequent monitoring of serum sodium in patients who restart BAXFENDY after experiencing hyponatremia. Permanently discontinue BAXFENDY if clinically significant hyponatremia recurs.
-
6 ADVERSE REACTIONS
The following clinically significant adverse reactions are also discussed elsewhere in the labeling:
- Hyperkalemia [see Warnings and Precautions (5.1)]
- Hyponatremia [see Warnings and Precautions (5.2)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The safety of BAXFENDY was evaluated over 12 weeks using the randomized, double-blind, placebo-controlled periods from three clinical trials in patients with hypertension not adequately controlled on other antihypertensive medications. Three of these trials [BaxHTN (NCT06034743), BrigHTN (NCT04519658), Bax24 (NCT06168409)] evaluated BAXFENDY 2 mg as add-on treatment and two trials [BaxHTN, BrigHTN] evaluated BAXFENDY 1 mg as add-on treatment. These data reflect exposure of 441 patients to BAXFENDY 2 mg and 333 patients to BAXFENDY 1 mg, with a mean treatment duration of 80 days for both BAXFENDY 2 mg and 1 mg. Analyses in this section are based on the 12‑week periods in these three trials. Uncontrolled, long-term safety data from 192 patients exposed to BAXFENDY 1 mg or 2 mg for a mean of 293 days and 172 patients exposed to BAXFENDY 2 mg for a mean of 327 days, were consistent with the safety profile observed during the 12-week, randomized, double-blind, placebo-controlled periods.
Hyperkalemia was the most frequently reported adverse reaction to BAXFENDY in the three clinical trials [see Warnings and Precautions (5.1)]. Hyperkalemia led to permanent discontinuation of treatment in 8 (1.8%) patients in the BAXFENDY 2 mg group, 2 (0.6%) patients in the BAXFENDY 1 mg group, and none in the placebo group.
Table 1 shows the most frequently reported adverse reactions to BAXFENDY during the 12-week period in the three clinical trials.
Table 1: Adverse Reactions Reported in ≥ 2% of Patients Treated with BAXFENDY and Greater (≥ 1%) than Placebo During the 12-Week, Randomized, Double-Blind Periods from Three Clinical Trials in Patients with Hypertension Adverse Reaction BAXFENDY 2 mg*
N=441
%BAXFENDY 1 mg†
N=333
%Placebo‡
N=442
%- * Frequencies derived from the pool of three hypertension studies (BaxHTN, BrigHTN, Bax24) with BAXFENDY 2 mg as add-on treatment.
- † Frequencies derived from the pool of two hypertension studies (BaxHTN, BrigHTN) with BAXFENDY 1 mg as add-on treatment.
- ‡ Frequencies derived from the pool of three hypertension studies (BaxHTN, BrigHTN, Bax24) with BAXFENDY 1 mg and/or 2 mg as add‑on treatment.
Hyperkalemia
10.2
6.6
2.5
Hypotension
3.6
2.1
0.5
Hyponatremia
3.2
2.1
0.9
Dizziness
2.9
3.0
0.9
Muscle spasms
2.9
1.8
0.7
Laboratory Tests
Serum Potassium
During the 12-week, randomized, double-blind periods from BAXFENDY clinical trials in patients with hypertension, increases in serum potassium (> 5.5 mEq/L) were reported for 12.2% of patients administered BAXFENDY 2 mg, 6.3% of patients administered BAXFENDY 1 mg, and 0.9% of placebo-treated patients.
Serum Sodium
During the 12-week, randomized, double-blind periods from BAXFENDY clinical trials in patients with hypertension, decreases in serum sodium (< 130 mEq/L) were reported for 3.7% of patients administered BAXFENDY 2 mg, 3.3% of patients administered BAXFENDY 1 mg, and 0.9% of placebo-treated patients.
Estimated Glomerular Filtration Rate (eGFR)
A decrease in mean eGFR was observed in BAXFENDY clinical trials in patients with hypertension. At Week 12, the mean placebo-corrected decrease in eGFR was 8.0 mL/min/1.73 m2 in the BAXFENDY 2 mg group and 7.1 mL/min/1.73 m2 in the BAXFENDY 1 mg group. In BAXFENDY-treated patients, the mean reduction in eGFR appeared to plateau by Week 12 and the mean eGFR increased after BAXFENDY discontinuation, suggesting a hemodynamic effect on renal function.
-
7 DRUG INTERACTIONS
7.1 Drugs That Increase Serum Potassium
Monitor serum potassium more frequently when BAXFENDY is used concomitantly with drugs that impair potassium excretion or increase serum potassium. Concomitant use may increase the risk of hyperkalemia [see Warnings and Precautions (5.1)].
7.2 Effect of Other Drugs on BAXFENDY
Strong and Moderate CYP3A Inducers
Monitor the therapeutic effect of BAXFENDY more frequently when concomitantly used with strong or moderate CYP3A inducers.
Baxdrostat is a CYP3A substrate. Strong or moderate CYP3A inducers may decrease baxdrostat plasma concentration, which may reduce the efficacy of BAXFENDY.
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
There are no available data on the use of BAXFENDY during pregnancy to evaluate for a drug-associated risk of major birth defects, miscarriage or adverse maternal or fetal outcome. Hypertension during pregnancy poses a risk to the mother and fetus (see Clinical Considerations). Although studies in animals have shown embryo-fetal toxicity at baxdrostat exposures > 29 times the human exposure at the clinical dose of 2 mg, the clinical significance of these findings is unclear (see Data).
The background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Report any pregnancies while treated with BAXFENDY to AstraZeneca at 1-800-236-9933.
Clinical Considerations
Disease-Associated Maternal and/or Embryo/Fetal Risk
Hypertension in pregnancy increases the risk for adverse maternal outcomes including pre-eclampsia, gestational diabetes, premature delivery, and delivery complications (e.g., need for cesarean section, and post-partum hemorrhage). Hypertension also increases the risk of adverse fetal outcomes including intrauterine growth restriction and stillbirth. Pregnant women with hypertension should be carefully monitored and managed accordingly.
Data
Animal Data
While baxdrostat had no effects on embryo-fetal development in rats or rabbits dosed through organogenesis at exposures up to 54‑fold (rat) and 29-fold (rabbit) the human dose of 2 mg, baxdrostat showed greatly reduced potency in rats compared to humans, which limits the interpretability of the rodent data. Higher baxdrostat doses were associated with increased incidence of adverse skeletal malformations in the rat and adverse decrease in rabbit fetal weights.
No adverse effects were noted in a pre- and postnatal study in rats dosed from gestation day 6 through lactation day 20 at exposures up to 65-fold the human exposure at 2 mg.
8.2 Lactation
Risk Summary
There are no data on the presence of baxdrostat in human milk, the effects on the breastfed infant, or the effects on milk production. Baxdrostat transfers to milk in lactating rats. When a drug is present in animal milk, it is likely that the drug will be present in human milk. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for BAXFENDY and any potential adverse effects on the breastfed infant from BAXFENDY or from the underlying maternal condition.
8.4 Pediatric Use
The safety and effectiveness of BAXFENDY in pediatric patients under 18 years of age have not been established.
8.5 Geriatric Use
No dose adjustment is required based on age [see Clinical Pharmacology (12.3)]. In the BaxHTN trial [see Clinical Studies (14)], 88 (33%) patients were 65 to 74 years of age, and 33 (12%) patients were ≥ 75 years of age in the BAXFENDY 2 mg group; and 71 (27%) patients were 65 to 74 years of age, and 25 (10%) patients were ≥ 75 years of age in the BAXFENDY 1 mg group. No overall differences in effectiveness were observed between these patients and younger adult patients. Hyperkalemia occurred at a higher incidence in patients ≥ 65 years of age [see Warnings and Precautions (5.1)]. Among patients 65 to 74 years of age, hyperkalemia occurred in 12 (14%) patients treated with BAXFENDY 2 mg, 7 (10%) patients treated with BAXFENDY 1 mg, and 3 (3%) patients treated with placebo. Among patients ≥ 75 years of age, hyperkalemia occurred in 7 (21%) patients treated with BAXFENDY 2 mg, none of the patients treated with BAXFENDY 1 mg, and none of the patients treated with placebo.
8.6 Renal Impairment
Safety and effectiveness of BAXFENDY initiated in patients with eGFR < 45 mL/min/1.73 m2 have not been established [see Clinical Studies (14)]. No dosage adjustment is required in patients with an eGFR ≥ 45 mL/min, unless assessed to be at risk of hyperkalemia [see Dosage and Administration (2.2) and Warnings and Precautions (5.1)].
-
10 OVERDOSAGE
BAXFENDY did not show any toxicity in healthy subjects at single oral doses up to 360 mg.
In the event of an overdose, consider contacting the Poison Help line (1-800-222-1222) or a medical toxicologist for additional overdosage management recommendations. It is also reasonable to employ supportive measures as dictated by the patient’s clinical status. The removal of baxdrostat by hemodialysis has not been studied.
-
11 DESCRIPTION
Baxdrostat is an aldosterone synthase inhibitor. The chemical name of baxdrostat is N-[(8R)-4-(1-methyl-2-oxo-1,2,3,4-tetrahydro-6-quinolinyl)-5,6,7,8-tetrahydro-8-isoquinolinyl]propanamide. The molecular formula is C22H25N3O2 and the molecular weight is 363.45 g/mol. The structural formula is:
BAXFENDY is available as a film-coated tablet for oral administration, containing 1 mg or 2 mg of baxdrostat. The inactive ingredients in BAXFENDY are croscarmellose sodium, lactose anhydrous, magnesium stearate, and microcrystalline cellulose. The film coating contains the following inactive ingredients: polyethylene glycol 3350, polyvinyl alcohol, talc, and titanium dioxide, in addition to ferric oxide red (1 mg strength tablets) or ferric oxide yellow (2 mg strength tablets).
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Baxdrostat is an inhibitor of human aldosterone synthase. Aldosterone contributes to hypertension by promoting the retention of sodium and water by the kidneys, which increases blood volume and, consequently, raises blood pressure. Aldosterone can cause vascular dysfunction, inflammation, and fibrosis. Inhibition of aldosterone synthase by baxdrostat decreases plasma aldosterone concentrations, thereby reducing blood pressure. Baxdrostat has a higher potency and selectivity for aldosterone synthase compared to the closely related enzyme 11β-hydroxylase (final enzyme in cortisol synthesis). In nonclinical and clinical studies, baxdrostat significantly lowered aldosterone concentrations without affecting cortisol responses over a wide dose range. Baxdrostat does not inhibit synthesis of sex hormones such as testosterone and estrone.
12.2 Pharmacodynamics
In healthy subjects, baxdrostat dosed at 1.5 mg to 2.5 mg with a normal salt diet and 2.5 mg to 5 mg with a low salt diet (0.75 to 2.5 times the maximum recommended dose), resulted in a decrease of up to approximately 70% and 83% in plasma aldosterone concentrations, respectively, after the initial dose. At Day 10, aldosterone concentrations remained up to approximately 68% lower than baseline in the normal salt group and 73% lower than baseline in the low salt group. In hypertensive patients, repeated administration of baxdrostat 0.5 mg (0.5 times the lowest recommended dose), 1 mg and 2 mg caused a sustained dose-dependent decrease in 24-hour urinary excretion of aldosterone, and a decrease in plasma aldosterone concentrations, while plasma renin activity increased. Decreased plasma aldosterone concentrations were observed up to 32 weeks, the last time point of assessment.
No effect on adrenocorticotropic hormone (ACTH) stimulated cortisol secretion was observed during treatment with BAXFENDY in healthy subjects with doses up to 360 mg (180 times the maximum recommended dose) administered as a single dose or with multiple ascending doses up to 10 mg (5 times the maximum recommended dose) at steady state, or in a dedicated randomized, double‑blind, placebo‑controlled trial in patients with hypertension treated with baxdrostat 2 mg for 8 weeks.
Cardiac Electrophysiology
Clinically significant QTc interval prolongation was not observed at 16 times the maximum recommended dose.
12.3 Pharmacokinetics
Baxdrostat geometric mean maximum plasma concentration (Cmax) was 19 ng/mL (%CV: 5.4) and the geometric mean area underneath the time concentration curve from time 0 to infinity (AUC0–inf) was 711 h*ng/mL (%CV: 32) following a single 2 mg dose. Baxdrostat AUC and Cmax increased in a dose‑proportional manner for the 1 and 2 mg doses in patients with hypertension, and steady state was reached by Day 8.
Absorption
Baxdrostat has an absolute bioavailability of 98%. Under fasted conditions, median time to maximum plasma concentration (tmax) was 2.5 hours (min: 1.0 hours, max: 5.0 hours) for the 2 mg dose. Baxdrostat did not show pH- dependent solubility at pharmacologically relevant concentrations.
Effect of Food
No clinically significant differences in baxdrostat pharmacokinetics were observed following administration of a high-fat, high-calorie meal (800 to 1000 calories with approximately 50% of the total caloric content from fat) in healthy subjects.
Distribution
The volume of distribution of baxdrostat at steady state is 205 L. The plasma protein binding of baxdrostat was 74% and the blood to plasma ratio was 0.95 in vitro.
Elimination
The mean effective half-life of baxdrostat was approximately 26 hours (range 23 to 32 hours). The mean total clearance was 2.8 L/h, and the mean renal clearance was 0.46 L/h.
Metabolism
Baxdrostat is primarily metabolized by CYP3A4 to an intermediate ketone metabolite, which is further metabolized by CBR1 (carbonyl reductase 1) to an alcohol metabolite (M2). After a single dose of radiolabeled baxdrostat, the parent compound accounted for 71% of total radioactivity exposure.
Excretion
After administration of a radiolabeled dose of baxdrostat, approximately 69% of the dose was recovered in urine (17% unchanged) and 15% in feces (6% unchanged).
Specific Populations
There were no clinically relevant effects of age (18 to 90 years), sex (37% females), body weight (43 to 224 kg), or race (White, Asian, and Black or African American) on the pharmacokinetics of baxdrostat.
Patients with Renal Impairment
In subjects with moderate or severe renal impairment (eGFR 15 to < 60 mL/min, not on dialysis), Cmax and AUC0–inf of baxdrostat were similar compared to the control group (eGFR ≥ 60 mL/min), with a geometric mean ratio (95% CI) for baxdrostat Cmax of 1.02 (0.82, 1.27) and AUC0–inf of 1.21 (0.81, 1.79). Compared to the control group, subjects with kidney failure treated with intermittent hemodialysis who were administered baxdrostat on a non-dialysis day had a geometric mean ratio (95% CI) for Cmax of 0.88 (0.71, 1.09) and AUC0‑inf of 0.68 (0.46, 0.99) [see Use in Specific Populations (8.6)].
Patients with Hepatic Impairment
In subjects with moderate hepatic impairment (Child-Pugh category B), Cmax and AUC0–inf of baxdrostat were similar to control subjects with normal hepatic function, with a geometric mean ratio (95% CI) for baxdrostat Cmax of 1.13 (0.97, 1.32) and AUC0–inf of 0.95 (0.73, 1.23). Baxdrostat has not been studied in patients with severe hepatic impairment.
Drug Interaction Studies
Clinical Studies
There was no clinically significant difference in baxdrostat exposure based on Cmax (1.30-fold geometric mean increase [95% CI: 1.20, 1.39]) or AUC (1.56-fold geometric mean increase [95% CI: 1.46, 1.66]) when used concomitantly with itraconazole (strong CYP3A and P‑gp inhibitor). There were no differences in the pharmacokinetics of either metformin (MATE1 and MATE2‑K transporter substrate) or the oral contraceptive ethinyl estradiol/levonorgestrel when used concomitantly with baxdrostat.
In Vitro Studies
Cytochrome P450 (CYP450) enzymes: Baxdrostat did not inhibit CYP1A2, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6 or CYP3A4/5, and did not induce CYP1A2, CYP2B6, or CYP3A4. Baxdrostat was not a substrate of CYP1A2, CYP2A6, CYP2B6, CYP2C9, CYP2C19, CYP2D6, CYP2E1, or CYP3A5.
UDP-Glucuronosyltransferase (UGT) enzymes: Baxdrostat did not inhibit UGT1A1, UGT1A3, UGT1A4, UGT1A6, UGT1A8, UGT1A9, UGT2B4, UGT2B7 or UGT2B15.
Transporter systems: Baxdrostat is a P-gp and BCRP substrate, but this is not expected to result in clinically significant drug-drug interactions. Baxdrostat did not inhibit the transporters BCRP, BSEP, OATP1B1, OATP1B3, OAT1, OAT3, OCT1, OCT2, or P-gp. Baxdrostat is not a substrate of OAT1, OAT3, OCT1, OCT2, OATP1B1, OATP1B3, MATE1, or MATE2-K.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Baxdrostat was not carcinogenic in a 6‑month carcinogenicity study in rasH2 transgenic mice. Administration of 5, 15, or 45 mg/kg/day of baxdrostat to rasH2 transgenic mice for 6 months did not increase the incidence of neoplastic findings. The exposure margin (based on AUC) was > 260‑fold compared to a human dose of 2 mg.
In a 2‑year carcinogenicity study in rats, baxdrostat was administered at daily doses of 0, 1, 3, or 10 mg/kg/day in males and 0, 0.3, 1, or 3 mg/kg/day in females. An increased incidence of benign and malignant thymoma was observed in males at 10 mg/kg/day. There were no neoplastic effects in males or females at 3 mg/kg/day (at least 36 times the human dose of 2 mg based on AUC).
Mutagenesis
Baxdrostat was not genotoxic when tested in a battery of in vitro and in vivo assays.
Impairment of Fertility
Male and female fertility studies in rats showed no effects of baxdrostat at exposures up to 126- and 218‑fold, respectively the human exposure at 2 mg.
-
14 CLINICAL STUDIES
The efficacy of BAXFENDY was evaluated in a multipart, phase 3, multicenter trial (BaxHTN, NCT06034743) in adults with systolic blood pressure ≥ 140 and < 170 mmHg who were prescribed at least 2 antihypertensive medications, including one diuretic and who had an eGFR ≥ 45 mL/min/1.73 m2 and a serum potassium of ≥ 3.5 and < 5.0 mEq/L. Following a 2-week placebo run-in period, 794 patients with a systolic blood pressure ≥ 135 mmHg were randomized equally and treated with BAXFENDY 1 mg, BAXFENDY 2 mg, or placebo once daily during an initial 12‑week double-blind treatment period. During this period, changes to background antihypertensive medication were prohibited unless patients became hypotensive or required rescue medication. Treatment with potassium supplements and potassium binders was allowed during the trial, but not simultaneous use of both an angiotensin receptor blocker (ARB) and angiotensin‑converting enzyme inhibitor (ACEi), or treatment with a mineralocorticoid receptor antagonist (MRA) or potassium sparing diuretic.
At the end of the 12 weeks, patients entered a 12-week, open-label treatment period. During the open-label period, patients who were on BAXFENDY 2 mg during the double-blind period continued the same dose of BAXFENDY, patients who received BAXFENDY 1 mg were re-randomized 4:1 to either BAXFENDY 2 mg or standard of care, and patients on placebo were re-randomized 1:4 to either BAXFENDY 2 mg or standard of care. At the end of the open-label period, 257 patients who were on BAXFENDY 2 mg in the open-label period were re-randomized 2:1 to receive either BAXFENDY 2 mg (n=172) or placebo (n=85) once daily during an 8-week double-blind, randomized withdrawal period.
The primary endpoints were change from baseline to Week 12 in seated office systolic blood pressure for BAXFENDY 2 mg once daily compared to placebo and for BAXFENDY 1 mg once daily compared to placebo. The key secondary endpoint was change in seated office systolic blood pressure for BAXFENDY 2 mg compared with placebo from the start (Week 24) to the end (Week 32) of the randomized withdrawal double-blind period of the trial.
The mean age of the patient population was 61 years, 62% were male, 63% were White, 26% Asian, 7% Black or African American, and 4% other, and 13% were of Hispanic or Latino ethnicity. The mean body mass index (BMI) at randomization was 31 kg/m2. Patient medical history included type 2 diabetes mellitus (37%), heart failure (6%), myocardial infarction (5%), and stroke (4%). Mean eGFR at baseline was 85 mL/min/1.73 m2.
Concomitant antihypertensive medicines during the trial included diuretics (100% of patients), either ACEi or ARB (90%), calcium channel blockers (70%), beta‑blockers (34%), and other antihypertensive medicines (17%). Approximately 41% of patients were on 3 background antihypertensive medications. At baseline, the mean systolic blood pressure was 149 mmHg and mean diastolic blood pressure was 87 mmHg.
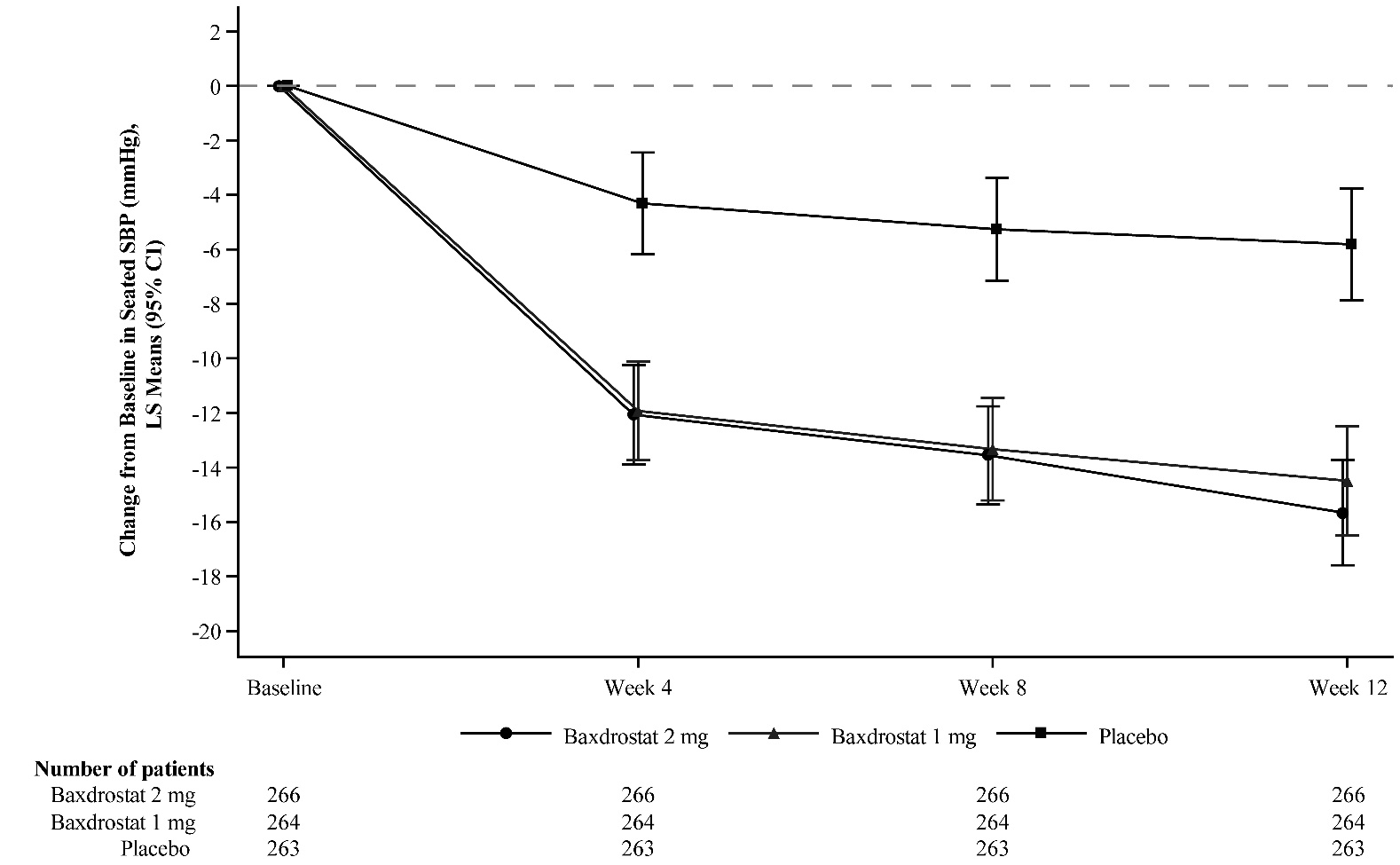
At Week 12, both BAXFENDY 1 mg and 2 mg were superior to placebo in reducing systolic blood pressure and diastolic blood pressure (Table 2). The mean change from baseline in systolic blood pressure over time in each treatment arm is shown in Figure 1.
Table 2: Treatment Effects on Blood Pressure at Week 12 (Full Analysis Set*), BaxHTN Trial Efficacy Parameter BAXFENDY 2 mg BAXFENDY 1 mg Placebo - * Full analysis set includes all randomized patients who received at least one administration of investigational medicinal product.
- † Seated blood pressure measurements were recorded using standardized automated blood pressure machines. Mean seated blood pressure is defined as the average of the last 2 seated blood pressure measurements of a total of 3 measurements.
- ‡ 1 patient in the placebo group was excluded from the analysis due to a missing baseline measurement.
- § Least square mean difference between BAXFENDY and placebo.
n=266
n=264
n=263
Baseline (mean)
149.1
149.7
149.0
Change from baseline (mean)
-15.7
-14.5
-5.8
Difference from placebo§ (95% CI)
-9.8
(-12.6, -7.0)
-8.7
(-11.5, -5.8)
p-value vs. placebo
< 0.0001
< 0.0001
n=266
n=264
n=263
Baseline (mean)
85.8
88.0
85.8
Change from baseline (mean)
-6.9
-6.3
-3.0
Difference from placebo§ (95% CI)
-3.9
(-5.7, -2.0)
-3.3
(-5.2, -1.4)
p-value vs placebo
< 0.0001
0.0008
Figure 1: Mean and 95% Confidence Intervals for Change from Baseline in Seated Systolic Blood Pressure (SBP) Over 12 Weeks, BaxHTN Trial
The treatment benefit of BAXFENDY over placebo on the primary endpoints was generally consistent across pre‑specified subgroups, including age, sex, BMI, renal function (eGFR), and systolic blood pressure at baseline.
Maintenance of the blood pressure lowering effect of BAXFENDY was demonstrated in the double-blind randomized‑withdrawal part of the trial. The change in mean systolic blood pressure during the 8-week randomized withdrawal period was ‑3.7 mmHg (95% CI ‑5.5, ‑1.9) in the BAXFENDY 2 mg arm and +1.4 mmHg (95% CI -1.2, 4.0) in the placebo arm, for a mean difference from placebo of -5.1 mmHg (95% CI -8.3, ‑1.9; p-value 0.002).
-
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 How Supplied
BAXFENDY (baxdrostat) tablets are available in the strengths and packages listed in Table 3.
Table 3: BAXFENDY Tablet Presentations Strength Description Package Type Package Size and NDC Number 1 mg
Pink, biconvex, round, film-coated tablets with “BX” debossed on one side and “1” on the other side
HDPE bottle with desiccant and child-resistant closure
30‑count: 0310-
6001-30
2 mg
Yellow, biconvex, round, film-coated tablets with “BX” debossed on one side and “2” on the other side
HDPE bottle with desiccant and child-resistant closure
30-count: 0310-
6002-30
-
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient Information).
Hyperkalemia and Hyponatremia
Inform patients that BAXFENDY can cause hyperkalemia and hyponatremia [see Warnings and Precautions (5.1, 5.2)].
Advise patients of the importance of regular blood tests to monitor serum potassium and sodium. Instruct patients to contact their healthcare provider immediately if they experience symptoms that may be caused by hyponatremia such as unusual fatigue, dizziness, dyspnea, headache, or confusion.
Advise patients receiving BAXFENDY to consult with their healthcare provider about the use of potassium supplements or salt substitutes containing potassium [see Warnings and Precautions (5.1, 5.2)].
Manufacturing Information
Distributed by: AstraZeneca Pharmaceuticals LP, Wilmington, DE 19850
BAXFENDY is a trademark of the AstraZeneca group of companies.
©AstraZeneca 2026
-
Patient Package Insert
PATIENT INFORMATION
BAXFENDY™ (bax fen’ dee)
(baxdrostat)
tablets, for oral use
What is BAXFENDY?
BAXFENDY is a prescription medicine used along with other blood pressure medicines to treat high blood pressure (hypertension) in adults whose blood pressure is not well controlled with other medicines.
It is not known if BAXFENDY is safe and effective in children under 18 years of age.
Before taking BAXFENDY, tell your healthcare provider about all of your medical conditions, including if you:
- have high potassium levels in your blood.
- have kidney problems.
- have diabetes.
- are pregnant or plan to become pregnant. It is not known if BAXFENDY can harm your unborn baby.
- are breastfeeding or plan to breastfeed. It is not known if BAXFENDY passes into your breast milk. Talk to your healthcare provider about the best way to feed your baby during treatment with BAXFENDY.
Tell your healthcare provider about all the medicines you take, including prescription and over-the-counter medicines, vitamins, and supplements. BAXFENDY may affect the way other medicines work, and other medicines may affect how BAXFENDY works.
Know the medicines you take. Keep a list of them to show your healthcare provider or pharmacist when you get a new medicine.
How should I take BAXFENDY?
- Take BAXFENDY exactly as your healthcare provider tells you to take it. Do not stop taking BAXFENDY unless your healthcare provider tells you to.
- Take BAXFENDY by mouth 1 time each day.
- Take BAXFENDY with or without food.
- Swallow BAXFENDY tablets whole. Do not cut, crush or chew BAXFENDY tablets.
- If you miss a dose, take the next dose at your regularly scheduled time. Do not take 2 doses of BAXFENDY in the same day to make up for a missed dose.
- If you take too much BAXFENDY, call your healthcare provider or Poison Help line at 1-800-222-1222, or go to the nearest emergency room right away.
What are the possible side effects of BAXFENDY?
BAXFENDY can cause side effects, including:
- Increased potassium levels in your blood (hyperkalemia). Your risk of developing hyperkalemia is increased if you are 65 years of age or older, have diabetes or kidney problems, or if you take other medicines that can increase potassium levels. Talk to your healthcare provider before using potassium supplements or salt substitutes that contain potassium during your treatment with BAXFENDY.
- Decreased sodium levels in your blood (hyponatremia). Your risk of developing hyponatremia is increased if you already have a low sodium blood level or take medicine that may cause hyponatremia. Tell your healthcare provider right away if you have any symptoms of low sodium levels during treatment. Symptoms of low sodium levels in your blood may include unusual fatigue, dizziness, headache, shortness of breath, or confusion.
Your healthcare provider will check your potassium and sodium levels in your blood before treatment with BAXFENDY and periodically during your treatment with BAXFENDY. Your healthcare provider may temporarily stop your treatment with BAXFENDY if you develop high potassium or low sodium levels in your blood.
The most common side effect of BAXFENDY is hyperkalemia.
These are not all of the possible side effects of BAXFENDY.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1‑800-FDA-1088.
How should I store BAXFENDY?
- Store BAXFENDY at room temperature between 68°F to 77°F (20°C to 25°C).
- Keep BAXFENDY tablets in the original bottle.
- The BAXFENDY bottle contains a desiccant packet to help keep your tablets dry (protect from moisture). Do not throw away the desiccant packet and keep it in the bottle.
- BAXFENDY comes in a bottle with a child-resistant closure.
Keep BAXFENDY and all medicines out of the reach of children.
General information about the safe and effective use of BAXFENDY.
Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. Do not use BAXFENDY for a condition for which it was not prescribed. Do not give BAXFENDY to other people, even if they have the same symptoms you have. It may harm them. You can ask your pharmacist or healthcare provider for information about BAXFENDY that is written for health professionals.
What are the ingredients in BAXFENDY?
Active ingredient: baxdrostat.
Inactive ingredients: croscarmellose sodium, lactose anhydrous, magnesium stearate, and microcrystalline cellulose. The film coating contains: polyethylene glycol 3350, polyvinyl alcohol, talc, and titanium dioxide, in addition to ferric oxide red (1 mg strength tablets) or ferric oxide yellow (2 mg strength tablets).
Distributed by: AstraZeneca Pharmaceuticals LP, Wilmington, DE 19850
BAXFENDY is a trademark of the AstraZeneca group of companies.
©AstraZeneca 2026
For more information, go to https://www.BAXFENDY.com or call 1-800-236-9933.
This Patient Information has been approved by the U.S. Food and Drug Administration. Issued: May 2026
-
Package/Label Display Panel
NDC: 0310-6001-30
BAXFENDY™
baxdrostat
tablets
1 mg
Rx only
Swallow tablets whole. Do not cut, crush, or chew tablets.
Store and dispense in original container with desiccant to protect from moisture.
30 Tablets
AstraZeneca
-
Package/Label Display Panel
NDC: 0310-6002-30
BAXFENDY™
baxdrostat
tablets
2 mg
Rx only
Swallow tablets whole. Do not cut, crush, or chew tablets.
Store and dispense in original container with desiccant to protect from moisture.
30 Tablets
AstraZeneca
-
INGREDIENTS AND APPEARANCE
BAXFENDY
baxdrostat tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 0310-6001 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength BAXDROSTAT (UNII: NF3P9Z8J5Y) (BAXDROSTAT - UNII:NF3P9Z8J5Y) BAXDROSTAT 1 mg Inactive Ingredients Ingredient Name Strength ANHYDROUS LACTOSE (UNII: 3SY5LH9PMK) MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) CROSCARMELLOSE SODIUM (UNII: M28OL1HH48) MAGNESIUM STEARATE (UNII: 70097M6I30) POLYVINYL ALCOHOL, UNSPECIFIED (UNII: 532B59J990) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) POLYETHYLENE GLYCOL 3350 (UNII: G2M7P15E5P) TALC (UNII: 7SEV7J4R1U) FERRIC OXIDE RED (UNII: 1K09F3G675) WATER (UNII: 059QF0KO0R) Product Characteristics Color PINK Score no score Shape ROUND (biconvex) Size 6mm Flavor Imprint Code BX;1 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 0310-6001-30 30 in 1 BOTTLE; Type 0: Not a Combination Product 05/15/2026 2 NDC: 0310-6001-95 7 in 1 BOTTLE; Type 0: Not a Combination Product 05/15/2026 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA219878 05/15/2026 BAXFENDY
baxdrostat tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 0310-6002 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength BAXDROSTAT (UNII: NF3P9Z8J5Y) (BAXDROSTAT - UNII:NF3P9Z8J5Y) BAXDROSTAT 2 mg Inactive Ingredients Ingredient Name Strength ANHYDROUS LACTOSE (UNII: 3SY5LH9PMK) MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) CROSCARMELLOSE SODIUM (UNII: M28OL1HH48) MAGNESIUM STEARATE (UNII: 70097M6I30) POLYVINYL ALCOHOL, UNSPECIFIED (UNII: 532B59J990) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) POLYETHYLENE GLYCOL 3350 (UNII: G2M7P15E5P) TALC (UNII: 7SEV7J4R1U) FERRIC OXIDE YELLOW (UNII: EX438O2MRT) WATER (UNII: 059QF0KO0R) Product Characteristics Color YELLOW Score no score Shape ROUND (biconvex) Size 8mm Flavor Imprint Code BX;2 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 0310-6002-30 30 in 1 BOTTLE; Type 0: Not a Combination Product 05/15/2026 2 NDC: 0310-6002-95 7 in 1 BOTTLE; Type 0: Not a Combination Product 05/15/2026 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA219878 05/15/2026 Labeler - AstraZeneca Pharmaceuticals LP (054743190)

© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.