OLMESARTAN MEDOXOMIL AND HYDROCHLOROTHIAZIDE tablet, film coated
OLMESARTAN MEDOXOMIL and HYDROCHLOROTHIAZIDE by
Drug Labeling and Warnings
OLMESARTAN MEDOXOMIL and HYDROCHLOROTHIAZIDE by is a Prescription medication manufactured, distributed, or labeled by Macleods Pharmaceuticals Limited. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use OLMESARTAN MEDOXOMIL AND HYDROCHLOROTHIAZIDE TABLETS safely and effectively. See full prescribing information for OLMESARTAN MEDOXOMIL AND HYDROCHLOROTHIAZIDE TABLETS.
OLMESARTAN MEDOXOMIL and HYDROCHLOROTHIAZIDE tablets, for oral use
Initial U.S. Approval: 2003
See full prescribing information for complete boxed warning.
When pregnancy is detected, discontinue olmesartan medoxomil and hydrochlorothiazide tablets as soon as possible (5.1, 8.1).
Drugs that act directly on the renin-angiotensin system can cause injury and death to the developing fetus (5.1, 8.1).
INDICATIONS AND USAGE
Olmesartan medoxomil and hydrochlorothiazide tablets are a combination of olmesartan, an angiotensin II receptor blocker and hydrochlorothiazide, a thiazide diuretic indicated for the treatment of hypertension, to lower blood pressure. Lowering blood pressure reduces the risk of fatal and nonfatal cardiovascular events, primarily strokes and myocardial infarctions. (1)
Limitations of Use
Olmesartan medoxomil and hydrochlorothiazide tablets is not indicated for initial therapy. (1)
DOSAGE AND ADMINISTRATION
Recommended starting dose in patients not adequately controlled with olmesartan monotherapy, 40/12.5 mg (2)
Recommended starting dose in patients not adequately controlled with hydrochlorothiazide monotherapy, 20/12.5 mg (2)
Adjust dose after 2 to 4 weeks, as needed, to a maximum of 40 mg / 25 mg olmesartan / hydrochlorothiazide (2)
DOSAGE FORMS AND STRENGTHS
Tablets: (olmesartan medoxomil and hydrochlorothiazide) 20/12.5 mg; 40/12.5 mg; 40/25 mg (3)
CONTRAINDICATIONS
WARNINGS AND PRECAUTIONS
Hypotension: Correct volume-depletion prior to administration. (5.2)
Monitor renal function and potassium in susceptible patients (5.3)
Observe for signs of fluid or electrolyte imbalance. (5.5)
Acute angle-closure glaucoma (5.6)
Sprue-like enteropathy has been reported. Consider discontinuation of olmesartan medoxomil and hydrochlorothiazide tablets in cases where no other etiology is found (5.8)
ADVERSE REACTIONS
Most common adverse reactions (incidence ≥2%) are nausea, hyperuricemia, dizziness, and upper respiratory infection (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Macleods Pharma USA, Inc. at 1-888-943-3210 or 1-855-926-3384 or FDA at 1-800-332-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
Agents increasing potassium levels may lead to increase in serum potassium (7.1).
Lithium: Risk of lithium toxicity (7.2)
Non-Steroidal Anti-Inflammatory Drugs (NSAIDs): Reduced diuretic, natriuretic and antihypertensive effects; increased risk of renal toxicity (7.3)
Dual inhibition of the renin-angiotensin system: Increased risk of renal impairment, hypotension, and hyperkalemia (7.4)
Colesevelam hydrochloride: Consider administering olmesartan at least 4 hours before colesevelam hydrochloride dose (7.5)
Antidiabetic drugs: Dosage adjustment may be required (7.6)
Cholestyramine and colestipol: Reduced absorption of thiazides (7.6)
USE IN SPECIFIC POPULATIONS
Lactation: Breastfeeding is not recommended (8.2).
See 17 for PATIENT COUNSELING INFORMATION.
Revised: 5/2025
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
WARNING: FETAL TOXICITY
1 INDICATIONS & USAGE
2 DOSAGE & ADMINISTRATION
3 DOSAGE FORMS & STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Fetal Toxicity
5.2 Hypotension in Volume or Salt-Depleted Patients
5.3 Impaired Renal Function
5.4 Hypersensitivity Reactions
5.5 Electrolyte and Metabolic Imbalances
5.6 Acute Myopia and Secondary Angle-Closure Glaucoma
5.7 Systemic Lupus Erythematosus
5.8 Sprue-Like Enteropathy
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
6.2 Post marketing Experience
7 DRUG INTERACTIONS
7.1 Agents Increasing Serum Potassium
7.2 Lithium
7.3 Non-Steroidal Anti-Inflammatory Agents Including Selective Cyclooxygenase-2 Inhibitors (COX-2 Inhibitors)
7.4 Dual Blockade of the Renin Angiotensin System
7.5 Colesevelam Hydrochloride
7.6 The use of Hydrochlorothiazide with Other Drugs
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.4 Pediatric Use
8.5 Geriatric Use
8.6 Renal Impairment
8.7 Hepatic Impairment
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- * Sections or subsections omitted from the full prescribing information are not listed.
-
BOXED WARNING
(What is this?)
WARNING: FETAL TOXICITY
When pregnancy is detected, discontinue olmesartan medoxomil and hydrochlorothiazide tablets as soon as possible [see Warnings and Precautions (5.1) Use in Specific Populations (8.1)].
Drugs that act directly on the renin-angiotensin system (RAS) can cause injury and death to the developing fetus [see Warnings and Precautions (5.1) Use in Specific Populations (8.1)]. -
1 INDICATIONS & USAGE
Olmesartan medoxomil and hydrochlorothiazide tablets are indicated for the treatment of hypertension, to lower blood pressure. Olmesartan medoxomil and hydrochlorothiazide tablets are not indicated for the initial therapy of hypertension [see Dosage and Administration (2)].
Lowering blood pressure reduces the risk of fatal and nonfatal cardiovascular (CV) events, primarily strokes and myocardial infarctions. These benefits have been seen in controlled trials of antihypertensive drugs from a wide variety of pharmacologic classes including the class to which this drug principally belongs. There are no controlled trials demonstrating risk reduction with olmesartan medoxomil and hydrochlorothiazide tablets.
Control of high blood pressure should be part of comprehensive cardiovascular risk management, including, as appropriate, lipid control, diabetes management, antithrombotic therapy, smoking cessation, exercise, and limited sodium intake. Many patients will require more than one drug to achieve blood pressure goals. For specific advice on goals and management, see published guidelines, such as those of the National High Blood Pressure Education Program’s Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC).
Numerous antihypertensive drugs, from a variety of pharmacologic classes and with different mechanisms of action, have been shown in randomized controlled trials to reduce cardiovascular morbidity and mortality, and it can be concluded that it is blood pressure reduction, and not some other pharmacologic property of the drugs, that is largely responsible for those benefits. The largest and most consistent cardiovascular outcome benefit has been a reduction in the risk of stroke, but reductions in myocardial infarction and cardiovascular mortality also have been seen regularly.
Elevated systolic or diastolic pressure causes increased cardiovascular risk, and the absolute risk increase per mmHg is greater at higher blood pressures, so that even modest reductions of severe hypertension can provide substantial benefit. Relative risk reduction from blood pressure reduction is similar across populations with varying absolute risk, so the absolute benefit is greater in patients who are at higher risk independent of their hypertension (for example, patients with diabetes or hyperlipidemia), and such patients would be expected to benefit from more aggressive treatment to a lower blood pressure goal.
Some antihypertensive drugs have smaller blood pressure effects (as monotherapy) in black patients, and many antihypertensive drugs have additional approved indications and effects (e.g., on angina, heart failure, or diabetic kidney disease). These considerations may guide selection of therapy.
Olmesartan medoxomil and hydrochlorothiazide tablets may be used alone, or in combination with other antihypertensive drugs.
Limitations of Use
Olmesartan medoxomil and hydrochlorothiazide tablets is not indicated for the initial therapy of hypertension.
-
2 DOSAGE & ADMINISTRATION
The recommended starting dose of olmesartan medoxomil and hydrochlorothiazide tablets are 40/12.5 mg once daily in patients whose blood pressure is not adequately controlled with olmesartan monotherapy. Dose can be titrated up to 40 /25 mg if necessary.
The recommended starting dose of olmesartan medoxomil and hydrochlorothiazide tablets are 20/12.5 mg once daily in patients whose blood pressure is not adequately controlled with HCT monotherapy or who experience dose-limiting adverse reactions with hydrochlorothiazide. Dose can be titrated up to 40 /25 mg if necessary.
Patients titrated to the individual components (olmesartan and hydrochlorothiazide) may instead receive the corresponding dose of olmesartan medoxomil and hydrochlorothiazide tablets.
-
3 DOSAGE FORMS & STRENGTHS
Olmesartan medoxomil and hydrochlorothiazide tablets are supplied as film-coated, non-scored tablets:
20 mg/12.5 mg reddish-yellow, round, biconvex, film-coated tablets debossed with "T 1" on one side and plain on other side.
40 mg/12.5 mg reddish-yellow, oval, biconvex, film-coated tablets debossed with "T 2" on one side and plain on other side.
40 mg/25 mg pink, oval, biconvex, film-coated tablets debossed with ''T 3" on one side and plain on other side.
-
4 CONTRAINDICATIONS
Olmesartan medoxomil and hydrochlorothiazide tablets are contraindicated:
In patients with hypersensitivity to any component of olmesartan medoxomil and hydrochlorothiazide tablets [see Adverse Reactions (6.1, 6.2)]
In patients with anuria [see Warnings and Precautions (5.3) and Adverse Reactions (6.1)]
For co-administration with aliskiren in patients with diabetes [see Drug Interactions (7.4)]
-
5 WARNINGS AND PRECAUTIONS
5.1 Fetal Toxicity
Olmesartan medoxomil and hydrochlorothiazide tablets can cause fetal harm when administered to a pregnant woman. Use of drugs that act on the renin-angiotensin system (RAS) during the second and third trimesters of pregnancy reduces fetal renal function and increases fetal and neonatal morbidity and death. Resulting oligohydramnios can be associated with fetal lung hypoplasia and skeletal deformations. Potential neonatal adverse effects include skull hypoplasia, anuria, hypotension, renal failure, and death. When pregnancy is detected, discontinue olmesartan medoxomil and hydrochlorothiazide tablets as soon as possible [see Use in Specific Populations (8.1)].
Thiazides cross the placental barrier and appear in cord blood. Adverse reactions include fetal or neonatal jaundice and thrombocytopenia [see Use in Specific Populations (8.1)].
5.2 Hypotension in Volume or Salt-Depleted Patients
In patients with an activated renin-angiotensin system, such as volume-or salt-depleted patients (e.g., those being treated with high doses of diuretics), symptomatic hypotension may occur after initiation of treatment with olmesartan medoxomil and hydrochlorothiazide tablets. If hypotension does occur, the patient should be placed in the supine position and, if necessary, given an intravenous infusion of normal saline. When electrolyte and fluid imbalances have been corrected, olmesartan medoxomil and hydrochlorothiazide tablets usually can be continued without difficulty. A transient hypotensive response is not a contraindication to further treatment.
5.3 Impaired Renal Function
Changes in renal function including acute renal failure can be caused by drugs that inhibit the renin-angiotensin system and by diuretics. Patients whose renal function may depend in part on the activity of the renin-angiotensin system (e.g., patients with renal artery stenosis, chronic kidney disease, severe congestive heart failure, or volume depletion) may be at particular risk of developing acute renal failure on olmesartan medoxomil and hydrochlorothiazide tablets. Monitor renal function periodically in these patients. Consider withholding or discontinuing therapy in patients who develop a clinically significant decrease in renal function on olmesartan medoxomil and hydrochlorothiazide tablets [see Drug Interactions (7)].
5.4 Hypersensitivity Reactions
Hypersensitivity reactions to hydrochlorothiazide may occur in patients with or without a history of allergy or bronchial asthma, but are more likely in patients with such a history.
5.5 Electrolyte and Metabolic Imbalances
Olmesartan medoxomil and hydrochlorothiazide tablets contain hydrochlorothiazide which can cause hypokalemia and hyponatremia. Hypomagnesemia can result in hypokalemia which may be difficult to treat despite potassium repletion. Olmesartan medoxomil and hydrochlorothiazide tablets also contain olmesartan, a drug that inhibits the RAS. Drugs that inhibit the RAS can cause hyperkalemia. Monitor serum electrolytes periodically.
Hydrochlorothiazide may alter glucose tolerance and raise serum levels of cholesterol and triglycerides.
Hyperuricemia may occur or frank gout may be precipitated in patients receiving thiazide therapy.
Hydrochlorothiazide decreases urinary calcium excretion and may cause elevations of serum calcium. Monitor calcium levels.
5.6 Acute Myopia and Secondary Angle-Closure Glaucoma
Hydrochlorothiazide, a sulfonamide, can cause an idiosyncratic reaction, resulting in acute transient myopia and acute angle-closure glaucoma. Symptoms include acute onset of decreased visual acuity or ocular pain and typically occur within hours to weeks of drug initiation. Untreated acute angle-closure glaucoma can lead to permanent vision loss. The primary treatment is to discontinue hydrochlorothiazide as rapidly as possible. Prompt medical or surgical treatments may need to be considered if the intraocular pressure remains uncontrolled. Risk factors for developing acute angle-closure glaucoma may include a history of sulfonamide or penicillin allergy.
5.7 Systemic Lupus Erythematosus
Thiazide diuretics have been reported to cause exacerbation or activation of systemic lupus erythematosus.
5.8 Sprue-Like Enteropathy
Severe, chronic diarrhea with substantial weight loss has been reported in patients taking olmesartan months to years after drug initiation. Intestinal biopsies of patients often demonstrated villous atrophy. If a patient develops these symptoms during treatment with olmesartan, exclude other etiologies. Consider discontinuation of olmesartan medoxomil and hydrochlorothiazide tablets in cases where no other etiology is identified.
-
6 ADVERSE REACTIONS
The following adverse reactions with olmesartan medoxomil and hydrochlorothiazide tablets are described elsewhere:
Hypotension in Volume-or Salt-Depleted Patients [see Warnings and Precautions (5.2)]
Impaired Renal Function [see Warnings and Precautions (5.3)]
Hypersensitivity Reactions [see Warnings and Precautions (5.4)]
Electrolyte and Metabolic Imbalances [see Warnings and Precautions (5.5)]
Acute Myopia and Secondary Angle-Closure Glaucoma [see Warnings and Precautions (5.6)]
Systemic Lupus Erythematosus [see Warnings and Precautions (5.7)]
Sprue-Like Enteropathy [see Warnings and Precautions (5.8)]
6.1 Clinical Trials Experience
Because clinical studies are conducted under widely varying conditions, adverse reaction rates observed in the clinical studies of a drug cannot be directly compared to rates in the clinical studies of another drug and may not reflect the rates observed in practice.
Olmesartan medoxomil and hydrochlorothiazide
The concomitant use of olmesartan medoxomil and hydrochlorothiazide was evaluated for safety in 1243 hypertensive patients. Treatment with olmesartan medoxomil and hydrochlorothiazide was well tolerated, with an incidence of adverse events similar to that of placebo. Adverse reactions were generally mild, transient and not dependent on the dose of olmesartan medoxomil and hydrochlorothiazide.
The rate of withdrawals for adverse events in all trials of hypertensive patients was 2.0% (25/1243) on olmesartan medoxomil plus hydrochlorothiazide and 2.0% (7/342) on placebo.
In a placebo-controlled, factorial clinical trial of olmesartan medoxomil (2.5 mg to 40 mg) and hydrochlorothiazide (12.5 mg to 25 mg), the following adverse reactions reported in Table 1 occurred in >2% of patients, and more often on the olmesartan medoxomil and hydrochlorothiazide combination than on placebo.
Table 1: Adverse Reactions in a Factorial Trial of Patients with Hypertension
Olmesartan/HCTZ (N=247)
(%)
Olmesartan (N=125)
(%)
HCTZ (N=88) (%)
Placebo (N=42)
(%)
Nausea
3
2
1
0
Hyperuricemia
4
0
2
2
Dizziness
9
1
8
2
Upper Respiratory Infection
7
6
7
0
Other adverse reactions that have been reported with an incidence of greater than 1.0%, whether or not attributed to treatment, in the more than 1200 hypertensive patients treated with olmesartan medoxomil and hydrochlorothiazide in controlled or open-label trials are listed below.
Body as a Whole: chest pain, back pain, peripheral edema
Central and Peripheral Nervous System: vertigo
Gastrointestinal: abdominal pain, dyspepsia, gastroenteritis, diarrhea
Liver and Biliary System: SGOT increased, GGT increased, ALT increased
Metabolic and Nutritional: creatine phosphokinase increased
Musculoskeletal: arthritis, arthralgia, myalgia
Respiratory System: coughing
Skin and Appendages Disorders: rash
Urinary System: hematuriaFacial edema was reported in 2/1243 patients receiving olmesartan medoxomil and hydrochlorothiazide. Angioedema has been reported with angiotensin II receptor antagonists, including olmesartan medoxomil and hydrochlorothiazide tablets.
Hydrochlorothiazide
Other adverse reactions that have been reported with hydrochlorothiazide are listed below:
Body as a Whole: weakness
Digestive: pancreatitis, jaundice (intrahepatic cholestatic jaundice), sialadenitis, cramping, gastric irritation
Hematologic: aplastic anemia, agranulocytosis, leukopenia, hemolytic anemia, thrombocytopenia
Hypersensitivity: purpura, photosensitivity, urticaria, necrotizing angiitis (vasculitis and cutaneous vasculitis), fever, respiratory distress including pneumonitis and pulmonary edema, anaphylactic reactions
Metabolic: glycosuria, hyperuricemia
Musculoskeletal: muscle spasm
Nervous System/Psychiatric: restlessness Renal: renal dysfunction, interstitial nephritis
Skin: erythema multiforme including Stevens-Johnson syndrome, exfoliative dermatitis including toxic epidermal necrolysis
Special Senses: transient blurred vision, xanthopsiaClinical Laboratory Test Findings
Creatinine/blood urea nitrogen (BUN): Minor elevations in creatinine and BUN occurred in 1.7% and 2.5% respectively, of patients taking olmesartan medoxomil and hydrochlorothiazide tablets and 0% and 0% respectively, given placebo in controlled clinical trials.
6.2 Post marketing Experience
The following adverse reactions have been identified during post-approval use of olmesartan medoxomil and hydrochlorothiazide tablets. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure:
Body as a Whole: Asthenia
Gastrointestinal: Vomiting
Metabolic: Hyperkalemia
Musculoskeletal: Rhabdomyolysis
Skin and Appendages: Alopecia, pruritusData from one controlled trial and an epidemiologic study have suggested that high-dose olmesartan may increase cardiovascular (CV) risk in diabetic patients, but the overall data are not conclusive. The randomized, placebo-controlled, double-blind ROADMAP trial (Randomized Olmesartan And Diabetes MicroAlbuminuria Prevention trial, n=4447) examined the use of olmesartan, 40 mg daily, vs. placebo in patients with type 2 diabetes mellitus, normoalbuminuria, and at least one additional risk factor for CV disease. The trial met its primary endpoint, delayed onset of microalbuminuria, but olmesartan had no beneficial effect on decline in glomerular filtration rate (GFR). There was a finding of increased CV mortality (adjudicated sudden cardiac death, fatal myocardial infarction, fatal stroke, revascularization death) in the olmesartan group compared to the placebo group (15 olmesartan vs. 3 placebo, HR 4.9, 95% confidence interval [CI], 1.4, 17), but the risk of non-fatal myocardial infarction was lower with olmesartan (HR 0.64, 95% CI 0.35, 1.18).
The epidemiologic study included patients 65 years and older with overall exposure of > 300,000 patient-years. In the sub-group of diabetic patients receiving high-dose olmesartan (40 mg/d) for > 6 months, there appeared to be an increased risk of death (HR 2.0, 95% CI 1.1, 3.8) compared to similar patients taking other angiotensin receptor blockers. In contrast, high-dose olmesartan use in non-diabetic patients appeared to be associated with a decreased risk of death (HR 0.46, 95% CI 0.24, 0.86) compared to similar patients taking other angiotensin receptor blockers. No differences were observed between the groups receiving lower doses of olmesartan compared to other angiotensin blockers or those receiving therapy for < 6 months.
Overall, these data raise a concern of a possible increased CV risk associated with the use of high-dose olmesartan in diabetic patients. There are, however, concerns with the credibility of the finding of increased CV risk, notably the observation in the large epidemiologic study for a survival benefit in non-diabetics of a magnitude similar to the adverse finding in diabetics.
Non-melanoma Skin Cancer
Hydrochlorothiazide is associated with an increased risk of non-melanoma skin cancer. In a study conducted in the Sentinel System, increased risk was predominantly for squamous cell carcinoma (SCC) and in white patients taking large cumulative doses. The increased risk for SCC in the overall population was approximately 1 additional case per 16,000 patients per year, and for white patients taking a cumulative dose of ≥50,000mg the risk increase was approximately 1 additional SCC case for every 6,700 patients per year.
-
7 DRUG INTERACTIONS
7.1 Agents Increasing Serum Potassium
Coadministration of olmesartan medoxomil and hydrochlorothiazide tablets with other drugs that raise serum potassium levels may result in hyperkalemia. Monitor serum potassium in such patients.
7.2 Lithium
Increases in serum lithium concentrations and lithium toxicity have been reported during concomitant administration of lithium with angiotensin II receptor antagonists or hydrochlorothiazide. Monitor serum lithium levels during concomitant use.
7.3 Non-Steroidal Anti-Inflammatory Agents Including Selective Cyclooxygenase-2 Inhibitors (COX-2 Inhibitors)
Olmesartan medoxomil
In patients who are elderly, volume-depleted (including those on diuretic therapy), or with compromised renal function, co-administration of NSAIDs, including selective COX-2 inhibitors, with angiotensin II receptor antagonists (including olmesartan medoxomil) may result in deterioration of renal function, including possible acute renal failure. These effects are usually reversible. Monitor renal function periodically in patients receiving olmesartan medoxomil and NSAID therapy.
The antihypertensive effect of angiotensin II receptor antagonists, including olmesartan medoxomil may be attenuated by NSAIDs including selective COX-2 inhibitors.
Hydrochlorothiazide
In some patients the administration of a NSAID can reduce the diuretic, natriuretic, and antihypertensive effects of thiazide diuretics. Therefore, monitor blood pressure closely.
7.4 Dual Blockade of the Renin Angiotensin System
Dual blockade of the RAS with angiotensin receptor blockers, ACE inhibitors, or aliskiren is associated with increased risks of hypotension, hyperkalemia, and changes in renal function (including acute renal failure) compared to monotherapy. Most patients receiving the combination of two RAS inhibitors do not obtain any additional benefit compared to monotherapy. In general, avoid combined use of RAS inhibitors. Closely monitor blood pressure, renal function and electrolytes in patients on olmesartan medoxomil and hydrochlorothiazide tablets and other agents that affect the RAS.
Do not co-administer aliskiren with olmesartan medoxomil and hydrochlorothiazide tablets in patients with diabetes [see Contraindications (4)]. Avoid use of aliskiren with olmesartan medoxomil and hydrochlorothiazide tablets in patients with renal impairment (GFR <60 ml/min).
7.5 Colesevelam Hydrochloride
Concurrent administration of bile acid sequestering agent colesevelam hydrochloride reduces the systemic exposure and peak plasma concentration of olmesartan. Administration of olmesartan at least 4 hours prior to colesevelam hydrochloride decreased the drug interaction effect. Consider administering olmesartan at least 4 hours before the colesevelam hydrochloride dose [see Clinical Pharmacology (12.3)].
7.6 The use of Hydrochlorothiazide with Other Drugs
When administered concurrently the following drugs may interact with thiazide diuretics:
Antidiabetic drugs (oral agents and insulin): Dosage adjustment of the antidiabetic drug may be required.
Ion exchange resins: Staggering the dosage of hydrochlorothiazide and ion exchange resins (e.g., cholestyramine, colestipol) such that hydrochlorothiazide is administered at least 4 hours before or 4 - 6 hours after the administration of resins would potentially minimize the interaction [see Clinical Pharmacology (12.3)].
Corticosteroids, ACTH: Intensified electrolyte depletion, particularly hypokalemia.
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
Olmesartan medoxomil and hydrochlorothiazide tablets can cause fetal harm when administered to a pregnant woman. Use of drugs that act on the renin-angiotensin system during the second and third trimesters of pregnancy reduces fetal renal function and increases fetal and neonatal morbidity, and death. Most epidemiologic studies examining fetal abnormalities after exposure to antihypertensive use in the first trimester have not distinguished drugs affecting the renin-angiotensin system from other antihypertensive agents.
When pregnancy is detected, discontinue olmesartan medoxomil and hydrochlorothiazide tablets as soon as possible. Use alternative antihypertensive therapy during pregnancy.
The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Clinical Considerations
Disease-associated maternal and/or embryo/fetal risk
Hypertension in pregnancy increases the maternal risk for pre-eclampsia, gestational diabetes, premature delivery, and delivery complications (e.g., need for cesarean section and post-partum hemorrhage). Hypertension increases the fetal risk for intrauterine growth restriction and intrauterine death. Pregnant women with hypertension should be carefully monitored and managed accordingly.
Fetal/Neonatal Adverse Reactions
Olmesartan
Oligohydramnios in pregnant women who use drugs affecting the renin-angiotensin system in the second and third trimesters of pregnancy can result in the following: reduced fetal renal function leading to anuria and renal failure, fetal lung hypoplasia, skeletal deformations, including skull hypoplasia, hypotension, and death.
Perform serial ultrasound examinations to assess the intra amniotic environment. Fetal testing may be appropriate, based on the week of gestation. Patients and physicians should be aware, however, that oligohydramnios may not appear until after the fetus has sustained irreversible injury.
Closely observe infants with histories of in utero exposure to Olmesartan medoxomil and hydrochlorothiazide tablets for hypotension, oliguria, and hyperkalemia. If oliguria or hypotension occur, utilize measures to maintain adequate blood pressure and renal perfusion. Exchange transfusions or dialysis may be required as a means of reversing hypotension and supporting renal function [see Use in Specific Populations (8.4)].
Hydrochlorothiazide
Thiazides can cross the placenta, and concentrations reached in the umbilical vein approach those in the maternal plasma. Hydrochlorothiazide, like other diuretics, can cause placental hypoperfusion. It accumulates in the amniotic fluid, with reported concentrations up to 19 times that in umbilical vein plasma. Use of thiazides during pregnancy is associated with a risk of fetal or neonatal jaundice or thrombocytopenia. Since they do not prevent or alter the course of preeclampsia, these drugs should not be used to treat hypertension in pregnant women. The use of HCTZ for other indications (e.g., heart disease) in pregnancy should be avoided.
Data
Animal Data
Olmesartan
No teratogenic effects were observed when olmesartan medoxomil was administered to pregnant rats at oral doses up to 1000 mg/kg/day (240 times the maximum recommended human dose [MRHD] on a mg/m2 basis) or pregnant rabbits at oral doses up to 1 mg/kg/day (half the MRHD on a mg/m2 basis; higher doses could not be evaluated for effects on fetal development as they were lethal to the does). In rats, significant decreases in pup birth weight and weight gain were observed at doses ≥1.6 mg/kg/day, and delays in developmental milestones (delayed separation of ear auricula, eruption of lower incisors, appearance of abdominal hair, descent of testes, and separation of eyelids) and dose-dependent increases in the incidence of dilation of the renal pelvis were observed at doses ≥ 8 mg/kg/day. The no observed effect dose for developmental toxicity in rats is 0.3 mg/kg/day, about one-tenth the MRHD of 40 mg/day.
Olmesartan medoxomil and Hydrochlorothiazide.
No teratogenic effects were observed when 1.6:1 combinations of olmesartan medoxomil and hydrochlorothiazide were administered to pregnant mice at oral doses up to 1625 mg/kg/day (122 times the maximum recommended human dose MRHD on a mg/m2 basis) or pregnant rats at oral doses up to 1625 mg/kg/day (243 times the MRHD on a mg/m2 basis). In rats, however, fetal body weights at 1625 mg/kg/day (a toxic, sometimes lethal dose in the dams) were significantly lower than control. The no observed effect dose for developmental toxicity in rats, 162.5 mg/kg/day, is about 24 times, on a mg/m2 basis, the MRHD of 40 mg olmesartan medoxomil /25 mg hydrochlorothiazide/day (calculations based on a 60 kg patient).
Hydrochlorothiazide
No teratogenic effects were observed when hydrochlorothiazide was administered to mice and rats via gavage at doses up to 3000 and 1000 mg/kg/day, respectively (about 600 and 400 times the MRHD), on gestation days 6 through 15.
8.2 Lactation
Risk Summary
There is limited information regarding the presence of olmesartan medoxomil and hydrochlorothiazide tablets in human milk, the effects on the breastfed infant, or the effects on milk production. Olmesartan is present in rat milk (see Data). Hydrochlorothiazide is present in human milk. Because of the potential for adverse effects on the nursing infant, advise a nursing woman that breastfeeding is not recommended during treatment with olmesartan medoxomil and hydrochlorothiazide tablets.
Data
Presence of olmesartan in milk was observed after a single oral administration of 5 mg/kg [14C] olmesartan medoxomil to lactating rats.
8.4 Pediatric Use
Safety and effectiveness of olmesartan medoxomil and hydrochlorothiazide tablets in pediatric patients have not been established.
8.5 Geriatric Use
Clinical studies of olmesartan medoxomil and hydrochlorothiazide tablets did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal or cardiac function and of concomitant diseases or other drug therapy.
Olmesartan and hydrochlorothiazide are substantially excreted by the kidney, and the risk of toxic reactions to olmesartan medoxomil and hydrochlorothiazide tablets may be greater in patients with impaired renal function.8.6 Renal Impairment
Safety and effectiveness of olmesartan medoxomil and hydrochlorothiazide tablets in patients with severe renal impairment (CrCl ≤ 30 mL/min) have not been established. No dose adjustment is required in patients with mild (CrCl 60-90 mL/min) or moderate (CrCl 30-60) renal impairment.
-
10 OVERDOSAGE
Olmesartan medoxomil
Limited data are available related to overdosage of olmesartan medoxomil in humans. The most likely manifestations of overdosage would be hypotension and tachycardia; bradycardia could be encountered if parasympathetic (vagal) stimulation occurs. If symptomatic hypotension should occur, supportive treatment should be initiated. The dialyzability of olmesartan is unknown.
No lethality was observed in acute toxicity studies in mice and rats given single oral doses up to 2000 mg/kg olmesartan medoxomil. The minimum lethal oral dose of olmesartan medoxomil in dogs was greater than 1500 mg/kg.Hydrochlorothiazide
The most common signs and symptoms of hydrochlorothiazide overdose observed in humans are those caused by electrolyte depletion (hypokalemia, hypochloremia, hyponatremia) and dehydration resulting from excessive diuresis. If digitalis has also been administered, hypokalemia may accentuate cardiac arrhythmias. The degree to which hydrochlorothiazide is removed by hemodialysis has not been established. The oral LD50 of hydrochlorothiazide is greater than 10 g/kg in both mice and rats.
-
11 DESCRIPTION
Olmesartan medoxomil and hydrochlorothiazide tablets are a combination of an angiotensin II receptor antagonist (AT1 subtype), olmesartan medoxomil, USP and a thiazide diuretic, hydrochlorothiazide (HCTZ), USP.
Olmesartan medoxomil is 2,3-dihydroxy-2-butenyl 4-(1-hydroxy-1-methylethyl)-2-propyl-1-[p-(o-1H-tetrazol-5-ylphenyl)benzyl]imidazole-5-carboxylate, cyclic 2,3-carbonate.
Its molecular formula is C29H30N6O6 and its structural formula is:
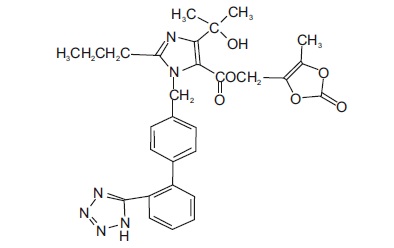
Olmesartan medoxomil, USP is a white to light yellowish-white powder or crystalline powder with a molecular weight of 558.6. It is practically insoluble in water and sparingly soluble in methanol.
Hydrochlorothiazide, USP is 6-chloro-3,4-dihydro-2H-1,2,4-benzo-thiadiazine-7-sulfonamide 1,1-dioxide. Its molecular formula is C7H8ClN3O4S2 and its structural formula is:
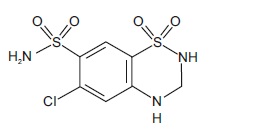
Hydrochlorothiazide, USP is a white, or practically white, crystalline powder with a molecular weight of 297.7. Hydrochlorothiazide, USP is slightly soluble in water but freely soluble in sodium hydroxide solution.
Olmesartan medoxomil and hydrochlorothiazide tablets are available for oral administration in tablets containing 20 mg or 40 mg of olmesartan medoxomil, USP combined with 12.5 mg of hydrochlorothiazide, USP or 40 mg of olmesartan medoxomil, USP combined with 25 mg of hydrochlorothiazide, USP. Inactive ingredients include: Lactose monohydrate, microcrystalline cellulose, sodium starch glycolate, hydroxypropyl cellulose, colloidal silicon dioxide, magnesium stearate, hypromellose, talc, titanium dioxide, iron oxide yellow and iron oxide red.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Olmesartan medoxomil
Angiotensin II is formed from angiotensin I in a reaction catalyzed by angiotensin converting enzyme (ACE, kininase II). Angiotensin II is the principal pressor agent of the renin-angiotensin system, with effects that include vasoconstriction, stimulation of synthesis and release of aldosterone, cardiac stimulation and renal reabsorption of sodium. Olmesartan blocks the vasoconstrictor effects of angiotensin II by selectively blocking the binding of angiotensin II to the AT1 receptor in vascular smooth muscle. Its action is, therefore, independent of the pathways for angiotensin II synthesis.An AT2 receptor is found also in many tissues, but this receptor is not known to be associated with cardiovascular homeostasis. Olmesartan has more than a 12,500-fold greater affinity for the AT1 receptor than for the AT2 receptor.
Blockade of the angiotensin II receptor inhibits the negative regulatory feedback of angiotensin II on renin secretion, but the resulting increased plasma renin activity (PRA) and circulating angiotensin II levels do not overcome the effect of olmesartan on blood pressure.
Hydrochlorothiazide
Hydrochlorothiazide is a thiazide diuretic. Thiazides affect the renal tubular mechanisms of electrolyte reabsorption, directly increasing excretion of sodium and chloride in approximately equivalent amounts. Indirectly, the diuretic action of hydrochlorothiazide reduces plasma volume, with consequent increases in plasma renin activity, increases in aldosterone secretion, increases in urinary potassium loss, and decreases in serum potassium. The renin-aldosterone link is mediated by angiotensin II, so co-administration of an angiotensin II receptor antagonist tends to reverse the potassium loss associated with these diuretics. The mechanism of the antihypertensive effect of thiazides is not fully understood.
12.2 Pharmacodynamics
Olmesartan medoxomil
Olmesartan medoxomil doses of 2.5 to 40 mg inhibit the pressor effects of angiotensin I infusion. The duration of the inhibitory effect was related to dose, with doses of olmesartan medoxomil >40 mg giving >90% inhibition at 24 hours.
Plasma concentrations of angiotensin I and angiotensin II and plasma renin activity (PRA) increase after single and repeated administration of olmesartan medoxomil to healthy subjects and hypertensive patients. Repeated administration of up to 80 mg olmesartan medoxomil had minimal influence on aldosterone levels and no effect on serum potassium.Hydrochlorothiazide
After oral administration of hydrochlorothiazide, diuresis begins within 2 hours, peaks in about 4 hours and lasts about 6 to 12 hours.Drug Interactions
Hydrochlorothiazide
Alcohol, barbiturates, or narcotics: Potentiation of orthostatic hypotension may occur.Skeletal muscle relaxants, non-depolarizing (e.g., tubocurarine): Increased responsiveness to the muscle relaxant may occur.
Digitalis glycosides: Thiazide-induced hypokalemia or hypomagnesemia may predispose to digoxin toxicity.
12.3 Pharmacokinetics
Absorption
Olmesartan: Olmesartan medoxomil is completely bioactivated by ester hydrolysis to olmesartan during absorption from the gastrointestinal tract. The absolute bioavailability of olmesartan is approximately 26%. After oral administration, the peak plasma concentration (Cmax) of olmesartan is reached after 1 to 2 hours. Food does not affect the bioavailability of olmesartan.
Olmesartan shows linear pharmacokinetics following single oral doses of up to 320 mg and multiple oral doses of up to 80 mg. Steady-state levels of olmesartan are achieved within 3 to 5 days and no accumulation in plasma occurs with once-daily dosing.Hydrochlorothiazide:
The estimated absolute bioavailability of hydrochlorothiazide after oral administration is about 70%. Peak plasma hydrochlorothiazide concentrations (Cmax) are reached within 2 to 5 hours after oral administration. There is no clinically significant effect of food on the bioavailability of hydrochlorothiazide.
The pharmacokinetics of hydrochlorothiazide is dose proportional in the range of 12.5 to 75 mg.
Distribution
Olmesartan: The volume of distribution of olmesartan is approximately 17 L. Olmesartan is highly bound to plasma proteins (99%) and does not penetrate red blood cells. The protein binding is constant at plasma olmesartan concentrations well above the range achieved with recommended doses.
In rats, olmesartan crossed the blood-brain barrier poorly, if at all. Olmesartan passed across the placental barrier in rats and was distributed to the fetus. Olmesartan was distributed to milk at low levels in rats.
Hydrochlorothiazide: Hydrochlorothiazide binds to albumin (40 to 70%) and distributes into erythrocytes. Following oral administration, plasma hydrochlorothiazide concentrations decline bi-exponentially, with a mean distribution half-life of about 2 hours and an elimination half-life of about 10 hours.
Hydrochlorothiazide crosses the placental but not the blood-brain barrier and is excreted in breast milk.
Metabolism
Olmesartan: Olmesartan does not undergo further metabolism.Hydrochlorothiazide: Hydrochlorothiazide is not metabolized.
Elimination
Olmesartan: Olmesartan appears to be eliminated in a biphasic manner with a terminal elimination half-life of approximately 13 hours. Total plasma clearance of olmesartan is 1.3 L/h, with a renal clearance of 0.6 L/h. Approximately 35% to 50% of the absorbed dose is recovered in urine while the remainder is eliminated in feces via the bile.
Hydrochlorothiazide: About 70% of an orally administered dose of hydrochlorothiazide is eliminated in the urine as unchanged drug.
Specific populations
Olmesartan medoxomil
Pediatric Patients: The pharmacokinetics of olmesartan were studied in pediatric hypertensive patients aged 1 to16 years. The clearance of olmesartan in pediatric patients was similar to that in adult patients when adjusted by the body weight. Olmesartan pharmacokinetics have not been investigated in pediatric patients less than 1 year of age.
Geriatric Patients: The pharmacokinetics of olmesartan were studied in the elderly (≥65 years). Overall, maximum plasma concentrations of olmesartan were similar in young adults and the elderly. Modest accumulation of olmesartan was observed in the elderly with repeated dosing; AUCss,τ was 33% higher in elderly patients, corresponding to an approximate 30% reduction in CLR.Male and Female Patients: Minor differences were observed in the pharmacokinetics of olmesartan in women compared to men. AUC and Cmax were 10-15% higher in women than in men.
Patients with Renal Impairment: In patients with renal insufficiency, serum concentrations of olmesartan were elevated compared to subjects with normal renal function. After repeated dosing, the AUC was approximately tripled in patients with severe renal impairment (creatinine clearance <20 mL/min). The pharmacokinetics of olmesartan in patients undergoing hemodialysis has not been studied.
Patients with Hepatic Impairment: Increases in AUC0-∞ and Cmax for olmesartan were observed in patients with moderate hepatic impairment compared to those in matched controls, with an increase in AUC of about 60%.Hydrochlorothiazide
Patients with Renal Impairment: In a study in individuals with impaired renal function, the mean elimination half-life of hydrochlorothiazide doubled in individuals with mild/moderate renal impairment (30 < CrCl < 90 mL/min) and tripled in severe renal impairment (≤ 30 mL/min), when compared to individuals with normal renal function (CrCl > 90 mL/min).
Drug Interactions Studies
Olmesartan
No significant drug interactions were reported in studies in which olmesartan medoxomil was co-administered with digoxin or warfarin in healthy volunteers.
The bioavailability of olmesartan medoxomil was not significantly altered by the co-administration of antacids [Al(OH)3/Mg(OH) 2].
Olmesartan medoxomil is not metabolized by the cytochrome P450 system and has no effects on P450 enzymes; thus, interactions with drugs that inhibit, induce, or are metabolized by those enzymes are not expected.Bile acid sequestering agent colesevelam
Concomitant administration of 40 mg olmesartan medoxomil and 3750 mg colesevelam hydrochloride in healthy subjects resulted in 28% reduction in Cmax and 39% reduction in AUC of olmesartan. Lesser effects, 4% and 15% reduction in Cmax and AUC respectively, were observed when olmesartan medoxomil was administered 4 hours prior to colesevelam hydrochloride [see Drug Interactions (7.5)].Hydrochlorothiazide
Drugs that alter gastrointestinal motility: The bioavailability of thiazide-type diuretics may be increased by anticholinergic agents (e.g. atropine, biperiden), apparently due to a decrease in gastrointestinal motility and the stomach emptying rate. Conversely, pro-kinetic drugs may decrease the bioavailability of thiazide diuretics.
Cholestyramine: In a dedicated drug interaction study, administration of cholestyramine 2 h before hydrochlorothiazide resulted in a 70% reduction in exposure to hydrochlorothiazide. Further, administration of hydrochlorothiazide 2 h before cholestyramine, resulted in 35% reduction in exposure to hydrochlorothiazide.
Lithium: Diuretic agents reduce the renal clearance of lithium and increase the risk of lithium toxicity [see Drug Interactions (7.2)].
Antineoplastic agents (e.g. cyclophosphamide, methotrexate): Concomitant use of thiazide diuretics may reduce renal excretion of cytotoxic agents and enhance their myelosuppressive effects.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Olmesartan medoxomil and hydrochlorothiazide
No carcinogenicity studies with olmesartan medoxomil and hydrochlorothiazide have been conducted.
Olmesartan medoxomil and hydrochlorothiazide in a ratio of 20:12.5 were negative in the Salmonella-Escherichia coli/mammalian microsome reverse mutation test up to the maximum recommended plate concentration for the standard assays. Olmesartan medoxomil and hydrochlorothiazide were tested individually and in combination ratios of 40:12.5, 20:12.5 and 10:12.5, for clastogenic activity in the in vitro Chinese hamster lung (CHL) chromosomal aberration assay. A positive response was seen for each component and combination ratio. However, no synergism in clastogenic activity was detected between olmesartan medoxomil and hydrochlorothiazide at any combination ratio. Olmesartan medoxomil and hydrochlorothiazide in a ratio of 20:12.5, administered orally, tested negative in the in vivo mouse bone marrow erythrocyte micronucleus assay at administered doses of up to 3144 mg/kg.
No studies of impairment of fertility with olmesartan medoxomil and hydrochlorothiazide have been conducted.
Olmesartan medoxomil
Olmesartan medoxomil was not carcinogenic when administered by dietary administration to rats for up to 2 years. The highest dose tested (2000 mg/kg/day) was, on a mg/m2 basis, about 480 times the maximum recommended human dose (MRHD) of 40 mg/day. Two carcinogenicity studies conducted in mice, a 6-month gavage study in the p53 knockout mouse and a 6-month dietary administration study in the Hras2 transgenic mouse, at doses of up to 1000 mg/kg/day (about 120 times the MRHD), revealed no evidence of a carcinogenic effect of olmesartan medoxomil.
Both olmesartan medoxomil and olmesartan tested negative in the in vitro Syrian hamster embryo cell transformation assay and showed no evidence of genetic toxicity in the Ames (bacterial mutagenicity) test. However, both were shown to induce chromosomal aberrations in cultured cells in vitro (Chinese hamster lung) and both tested positive for thymidine kinase mutations in the in vitro mouse lymphoma assay. Olmesartan medoxomil tested negative in vivo for mutations in the MutaMouse intestine and kidney, and for clastogenicity in mouse bone marrow (micronucleus test) at oral doses of up to 2000 mg/kg (olmesartan not tested).
Fertility of rats was unaffected by administration of olmesartan medoxomil at dose levels as high as 1000 mg/kg/day (240 times the MRHD) in a study in which dosing was begun 2 (female) or 9 (male) weeks prior to mating.
Hydrochlorothiazide
Two-year feeding studies in mice and rats conducted under the auspices of the National Toxicology Program (NTP) uncovered no evidence of a carcinogenic potential of hydrochlorothiazide in female mice (at doses of up to approximately 600 mg/kg/day) or in male and female rats (at doses of up to approximately 100 mg/kg/day). The NTP, however, found equivocal evidence for hepatocarcinogenicity in male mice.Hydrochlorothiazide was not genotoxic in vitro in the Ames mutagenicity assay of Salmonella typhimurium strains TA 98, TA 100, TA 1535, TA 1537 and TA 1538, or in the Chinese Hamster Ovary (CHO) test for chromosomal aberrations. It was also not genotoxic in vivo in assays using mouse germinal cell chromosomes, Chinese hamster bone marrow chromosomes, or the Drosophila sex-linked recessive lethal trait gene. Positive test results were obtained in the in vitro CHO Sister Chromatid Exchange (clastogenicity) assay, the Mouse Lymphoma Cell (mutagenicity) assay and the Aspergillus nidulans non-disjunction assay.
Hydrochlorothiazide had no adverse effects on the fertility of mice and rats of either sex in studies wherein these species were exposed, via their diet, to doses of up to 100 and 4 mg/kg, respectively, prior to mating and throughout gestation.
-
14 CLINICAL STUDIES
Olmesartan medoxomil and hydrochlorothiazide
In clinical trials 1230 patients were exposed to the combination of olmesartan medoxomil (2.5 mg to 40 mg) and hydrochlorothiazide (12.5 mg to 25 mg). These trials included one placebo-controlled factorial trial in mild-moderate hypertensive patients (n=502) with combinations of olmesartan medoxomil (10 mg, 20 mg, 40 mg, or placebo) and hydrochlorothiazide (12.5 mg, 25 mg, or placebo). The antihypertensive effect of the combination on trough blood pressure was related to the dose of each component (see Table 2).Once-daily dosing with 20 mg olmesartan medoxomil and 12.5 mg hydrochlorothiazide, 40 mg olmesartan medoxomil and 12.5 mg hydrochlorothiazide or 40 mg olmesartan medoxomil and 25 mg hydrochlorothiazide produced mean placebo-adjusted blood pressure reductions at trough (24 hours post-dosing) ranging from 17/8 to 24/14 mm Hg.
Table 2: Placebo-Adjusted Reductions in Sitting Systolic/Diastolic Blood Pressure (mmHg)
HCTZ
Olmesartan Medoxomil
0 mg
10 mg
20 mg
40 mg
0 mg
--
7/5
12/5
13/7
12.5 mg
5/1
17/8
17/8
16/10
25 mg
14/5
19/11
22/11
24/14
The antihypertensive effect had onset within 1 week and was near maximal at 4 weeks. The antihypertensive effect was independent of gender, but there were too few subjects to identify response differences based on race or age greater than or less than 65 years. No appreciable changes in trough heart rate were observed with combination therapy.
There are no trials of olmesartan medoxomil and hydrochlorothiazide tablets demonstrating reductions in cardiovascular risk in patients with hypertension, but at least one drug pharmacologically similar to olmesartan medoxomil has demonstrated such benefits, and hydrochlorothiazide demonstrated reduction of cardiovascular risk in patients with hypertension.
Olmesartan medoxomil
The antihypertensive effects of olmesartan medoxomil have been demonstrated in seven placebo-controlled studies at doses ranging from 2.5 to 80 mg for 6 to 12 weeks, each showing statistically significant reductions in peak and trough blood pressure. A total of 2693 patients (2145 olmesartan medoxomil; 548 placebo) with essential hypertension were studied. Olmesartan medoxomil once daily (QD) lowered diastolic and systolic blood pressure. The response was dose-related. An olmesartan medoxomil dose of 20 mg daily produced a trough sitting blood pressure (BP) reduction over placebo of about 10/6 mmHg and a dose of 40 mg daily produced a trough sitting blood pressure (BP) reduction over placebo of about 12/7 mmHg. Olmesartan medoxomil doses greater than 40 mg had little additional effect. The onset of the antihypertensive effect occurred within 1 week and was largely manifest after 2 weeks.The blood pressure lowering effect was maintained throughout the 24-hour period with olmesartan medoxomil once daily, with trough-to-peak ratios for systolic and diastolic response between 60 and 80%.
The blood pressure lowering effect of olmesartan medoxomil, with and without hydrochlorothiazide, was maintained in patients treated for up to 1 year. There was no evidence of tachyphylaxis during long-term treatment with olmesartan medoxomil or rebound effect following abrupt withdrawal of olmesartan medoxomil after 1 year of treatment.
The antihypertensive effect of olmesartan medoxomil was similar in men and women and in patients older and younger than 65 years. The effect was smaller in black patients (usually a low-renin population), as has been seen with other ACE inhibitors, angiotensin receptor blockers, and beta-blockers. Olmesartan medoxomil had an additional blood pressure lowering effect when added to hydrochlorothiazide.
-
16 HOW SUPPLIED/STORAGE AND HANDLING
Olmesartan medoxomil and hydrochlorothiazide tablets are supplied as:
20 mg/12.5 mg:Reddish yellow, round, biconvex, film-coated tablets debossed with "T 1" on one side and plain on other side. Each tablet contains 20 mg of olmesartan medoxomil, USP and 12.5 mg of hydrochlorothiazide, USP.
40 mg/12.5 mg: Reddish-yellow, oval, biconvex, film-coated tablets debossed with "T 2" on one side and plain on other side. Each tablet contains 40 mg of olmesartan medoxomil, USP and 12.5 mg of hydrochlorothiazide, USP.
40 mg/25 mg: Pink, oval, biconvex, film-coated tablets debossed with ''T 3" on one side and plain on other side. Each tablet contains 40 mg of olmesartan medoxomil, USP and 25 mg of hydrochlorothiazide, USP.
Tablets are supplied as follows:
20 mg/12.5 mg
40 mg/12.5 mg
40 mg/25 mg
Bottle of 30 tablets
NDC: 33342-173-07
NDC: 33342-174-07
NDC: 33342-175-07
Bottle of 90 tablets
NDC: 33342-173-10
NDC: 33342-174-10
NDC: 33342-175-10
Bottle of 1000 tablets
NDC: 33342-173-44
NDC: 33342-174-44
NDC: 33342-175-44
10 Blister cards of 10 tablets each
NDC: 33342-173-12
NDC: 33342-174-12
NDC: 33342-175-12
Storage
Store at 20° to 25°C (68° to 77°F); excursions permitted to 15° to 30°C (59° to 86°F) [See USP Controlled Room Temperature].
-
17 PATIENT COUNSELING INFORMATION
Pregnancy: Advise female patients of childbearing age about the consequences of exposure to olmesartan medoxomil and hydrochlorothiazide tablets during pregnancy. Discuss treatment options with women planning to become pregnant. Tell patients to report pregnancies to their physicians as soon as possible [See Warnings and Precautions (5.1) and Use in Specific Populations (8.1)].
Lactation: Advise nursing women not to breastfeed during treatment with olmesartan medoxomil and hydrochlorothiazide tablets [see Use in Specific Populations (8.2)].
Symptomatic hypotension and syncope: Advise patients that lightheadedness can occur, especially during the first days of therapy, and to report this symptom to a healthcare provider. Inform patients that dehydration from inadequate fluid intake, excessive perspiration, vomiting, or diarrhea may lead to an excessive fall in blood pressure. If syncope occurs advise patients, to contact their healthcare provider.
Potassium Supplements: Advise patients not to use potassium supplements or salt substitutes containing potassium without consulting their healthcare provider.
Acute myopia and secondary angle-closure glaucoma: Advise patients to discontinue olmesartan medoxomil and hydrochlorothiazide tablets and seek immediate medical attention if they experience symptoms of acute myopia or secondary angle-closure glaucoma [see Warnings and Precautions (5.6)].
Non-melanoma Skin Cancer: Instruct patients taking hydrochlorothiazide to protect skin from the sun and undergo regular skin cancer screening.
Manufactured by:
Macleods Pharmaceutical Ltd.
Daman (U.T.), 396210, INDIA
Manufactured for:
Macleods Pharma USA, Inc.
Princeton, NJ 08540
Revised : May 2025
-
PACKAGE LABEL.PRINCIPAL DISPLAY PANEL
Rx Only
Olmesartan Medoxomil and Hydrochlorothiazide Tablets, 20 mg/12.5 mg
Bottle of 30 Tablets
NDC: 33342-173-07
Rx Only
Olmesartan Medoxomil and Hydrochlorothiazide Tablets, 20 mg/12.5 mg
Bottle of 90 Tablets
NDC: 33342-173-10
Rx Only
Olmesartan Medoxomil and Hydrochlorothiazide Tablets, 20 mg/12.5 mg
Bottle of 1000 Tablets
NDC: 33342-173-44
Rx Only
Olmesartan Medoxomil and Hydrochlorothiazide Tablets, 20 mg/12.5 mg
Carton of 100 Tablets (10 x 10 Unit dose)
NDC: 33342-173-12
Rx Only
Olmesartan Medoxomil and Hydrochlorothiazide Tablets, 40 mg/12.5 mg
Bottle of 30 Tablets
NDC: 33342-174-07
Rx Only
Olmesartan Medoxomil and Hydrochlorothiazide Tablets, 40 mg/12.5 mg
Bottle of 90 Tablets
NDC: 33342-174-10
Rx Only
Olmesartan Medoxomil and Hydrochlorothiazide Tablets, 40 mg/12.5 mg
Bottle of 1000 Tablets
NDC: 33342-174-44
Rx Only
Olmesartan Medoxomil and Hydrochlorothiazide Tablets, 40 mg/12.5 mg
Carton of 100 Tablets (10 x 10 Unit dose)
NDC: 33342-174-12
Rx Only
Olmesartan Medoxomil and Hydrochlorothiazide Tablets, 40 mg/25 mg
Bottle of 30 Tablets
NDC: 33342-175-07
Rx Only
Olmesartan Medoxomil and Hydrochlorothiazide Tablets, 40 mg/25 mg
Bottle of 90 Tablets
NDC: 33342-175-10
Rx Only
Olmesartan Medoxomil and Hydrochlorothiazide Tablets, 40 mg/25 mg
Bottle of 1000 Tablets
NDC: 33342-175-44
Rx Only
Olmesartan Medoxomil and Hydrochlorothiazide Tablets, 40 mg/25 mg
Carton of 100 Tablets (10 x 10 Unit dose)
NDC: 33342-175-12
-
INGREDIENTS AND APPEARANCE
OLMESARTAN MEDOXOMIL AND HYDROCHLOROTHIAZIDE
olmesartan medoxomil and hydrochlorothiazide tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 33342-173 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength OLMESARTAN MEDOXOMIL (UNII: 6M97XTV3HD) (OLMESARTAN - UNII:8W1IQP3U10) OLMESARTAN MEDOXOMIL 20 mg HYDROCHLOROTHIAZIDE (UNII: 0J48LPH2TH) (HYDROCHLOROTHIAZIDE - UNII:0J48LPH2TH) HYDROCHLOROTHIAZIDE 12.5 mg Inactive Ingredients Ingredient Name Strength LACTOSE MONOHYDRATE (UNII: EWQ57Q8I5X) CELLULOSE, MICROCRYSTALLINE (UNII: OP1R32D61U) SODIUM STARCH GLYCOLATE TYPE A POTATO (UNII: 5856J3G2A2) HYDROXYPROPYL CELLULOSE (UNII: RFW2ET671P) SILICON DIOXIDE (UNII: ETJ7Z6XBU4) MAGNESIUM STEARATE (UNII: 70097M6I30) HYPROMELLOSES (UNII: 3NXW29V3WO) TALC (UNII: 7SEV7J4R1U) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) FERRIC OXIDE YELLOW (UNII: EX438O2MRT) FERRIC OXIDE RED (UNII: 1K09F3G675) Product Characteristics Color RED (Reddish-yellow) Score no score Shape ROUND Size 9mm Flavor Imprint Code T1 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 33342-173-07 30 in 1 BOTTLE; Type 0: Not a Combination Product 06/02/2023 2 NDC: 33342-173-10 90 in 1 BOTTLE; Type 0: Not a Combination Product 06/02/2023 3 NDC: 33342-173-44 1000 in 1 BOTTLE; Type 0: Not a Combination Product 06/02/2023 4 NDC: 33342-173-12 10 in 1 CARTON 06/02/2023 4 10 in 1 BLISTER PACK; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA204801 06/02/2023 OLMESARTAN MEDOXOMIL AND HYDROCHLOROTHIAZIDE
olmesartan medoxomil and hydrochlorothiazide tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 33342-174 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength OLMESARTAN MEDOXOMIL (UNII: 6M97XTV3HD) (OLMESARTAN - UNII:8W1IQP3U10) OLMESARTAN MEDOXOMIL 40 mg HYDROCHLOROTHIAZIDE (UNII: 0J48LPH2TH) (HYDROCHLOROTHIAZIDE - UNII:0J48LPH2TH) HYDROCHLOROTHIAZIDE 12.5 mg Inactive Ingredients Ingredient Name Strength LACTOSE MONOHYDRATE (UNII: EWQ57Q8I5X) CELLULOSE, MICROCRYSTALLINE (UNII: OP1R32D61U) SODIUM STARCH GLYCOLATE TYPE A POTATO (UNII: 5856J3G2A2) HYDROXYPROPYL CELLULOSE (UNII: RFW2ET671P) SILICON DIOXIDE (UNII: ETJ7Z6XBU4) MAGNESIUM STEARATE (UNII: 70097M6I30) HYPROMELLOSES (UNII: 3NXW29V3WO) TALC (UNII: 7SEV7J4R1U) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) FERRIC OXIDE YELLOW (UNII: EX438O2MRT) FERRIC OXIDE RED (UNII: 1K09F3G675) Product Characteristics Color RED (Reddish-yellow) Score no score Shape OVAL Size 15mm Flavor Imprint Code T2 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 33342-174-07 30 in 1 BOTTLE; Type 0: Not a Combination Product 06/02/2023 2 NDC: 33342-174-10 90 in 1 BOTTLE; Type 0: Not a Combination Product 06/02/2023 3 NDC: 33342-174-44 1000 in 1 BOTTLE; Type 0: Not a Combination Product 06/02/2023 4 NDC: 33342-174-12 10 in 1 CARTON 06/02/2023 4 10 in 1 BLISTER PACK; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA204801 06/02/2023 OLMESARTAN MEDOXOMIL AND HYDROCHLOROTHIAZIDE
olmesartan medoxomil and hydrochlorothiazide tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 33342-175 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength OLMESARTAN MEDOXOMIL (UNII: 6M97XTV3HD) (OLMESARTAN - UNII:8W1IQP3U10) OLMESARTAN MEDOXOMIL 40 mg HYDROCHLOROTHIAZIDE (UNII: 0J48LPH2TH) (HYDROCHLOROTHIAZIDE - UNII:0J48LPH2TH) HYDROCHLOROTHIAZIDE 25 mg Inactive Ingredients Ingredient Name Strength LACTOSE MONOHYDRATE (UNII: EWQ57Q8I5X) CELLULOSE, MICROCRYSTALLINE (UNII: OP1R32D61U) SODIUM STARCH GLYCOLATE TYPE A POTATO (UNII: 5856J3G2A2) HYDROXYPROPYL CELLULOSE (UNII: RFW2ET671P) SILICON DIOXIDE (UNII: ETJ7Z6XBU4) MAGNESIUM STEARATE (UNII: 70097M6I30) HYPROMELLOSES (UNII: 3NXW29V3WO) TALC (UNII: 7SEV7J4R1U) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) FERRIC OXIDE YELLOW (UNII: EX438O2MRT) FERRIC OXIDE RED (UNII: 1K09F3G675) Product Characteristics Color PINK Score no score Shape OVAL Size 15mm Flavor Imprint Code T3 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 33342-175-07 30 in 1 BOTTLE; Type 0: Not a Combination Product 06/02/2023 2 NDC: 33342-175-10 90 in 1 BOTTLE; Type 0: Not a Combination Product 06/02/2023 3 NDC: 33342-175-44 1000 in 1 BOTTLE; Type 0: Not a Combination Product 06/02/2023 4 NDC: 33342-175-12 10 in 1 CARTON 06/02/2023 4 10 in 1 BLISTER PACK; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA204801 06/02/2023 Labeler - Macleods Pharmaceuticals Limited (862128535) Establishment Name Address ID/FEI Business Operations Macleods Pharmaceuticals Limited 918608365 ANALYSIS(33342-173, 33342-174, 33342-175) , LABEL(33342-173, 33342-174, 33342-175) , MANUFACTURE(33342-173, 33342-174, 33342-175) , PACK(33342-173, 33342-174, 33342-175)
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.