PENICILLIN G PROCAINE injection, suspension
PENICILLIN G PROCAINE by
Drug Labeling and Warnings
PENICILLIN G PROCAINE by is a Prescription medication manufactured, distributed, or labeled by Pfizer Laboratories Div Pfizer Inc, King Pharmaceuticals LLC. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
- SPL UNCLASSIFIED SECTION
-
BOXED WARNING
(What is this?)
Prior to administration of the drug, carefully read the WARNINGS, ADVERSE REACTIONS, and DOSAGE AND ADMINISTRATION sections of the labeling.
- SPL UNCLASSIFIED SECTION
-
DESCRIPTION
This product is designed to provide a stable aqueous suspension of penicillin G procaine, ready for immediate use. This eliminates the necessity for addition of any diluent, required for the usual dry formulation of injectable penicillin.
Penicillin G procaine is chemically designated as (2S, 5R, 6R)-3,3-Dimethyl-7-oxo-6-(2-phenylacetamido)-4-thia-1-azabicyclo[3.2.0]heptane-2-carboxylic acid compound with 2-(diethylamino)ethyl p-aminobenzoate (1:1) monohydrate.
Its molecular formula is C16H18N2O4S∙C13H20N2O2∙H2O with a molecular weight of 588.72. Its structural formula is as follows:
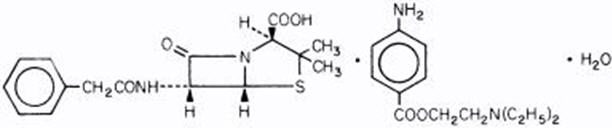
Each syringe, 1,200,000 units (2 mL size) or 600,000 units (1 mL size), contains penicillin G procaine in a stabilized aqueous suspension with sodium citrate buffer; and as w/v, approximately 0.5% lecithin, 0.5% carboxymethylcellulose, 0.5% povidone, 0.1% methylparaben, and 0.01% propylparaben.
Penicillin G Procaine Injectable Suspension is viscous and opaque. Read CONTRAINDICATIONS, WARNINGS, PRECAUTIONS, and DOSAGE AND ADMINISTRATION sections prior to use.
-
CLINICAL PHARMACOLOGY
Penicillin G procaine is an equimolecular compound of procaine and penicillin G, administered intramuscularly as a suspension. It dissolves slowly at the site of injection, giving a plateau type of blood level at about 4 hours which falls slowly over a period of the next 15 to 20 hours.
Approximately 60% of penicillin G is bound to serum protein. The drug is distributed throughout the body tissues in widely varying amounts. Highest levels are found in the kidneys with lesser amounts in the liver, skin, and intestines. Penicillin G penetrates into all other tissues to a lesser degree with a very small level found in the cerebrospinal fluid. With normal kidney function, the drug is excreted rapidly by tubular excretion. In neonates and young infants and in individuals with impaired kidney functions, excretion is considerably delayed. Approximately 60 to 90 percent of a dose of parenteral penicillin G is excreted in the urine within 24 to 36 hours.
Microbiology
Mechanism of Action
Penicillin G exerts a bactericidal action against penicillin-susceptible microorganisms during the stage of active multiplication. It acts through the inhibition of biosynthesis of cell-wall peptidoglycan, rendering the cell wall osmotically unstable.
Resistance
Penicillin is not active against penicillinase-producing bacteria, or against organisms resistant to beta-lactams because of alterations in the penicillin-binding proteins. Resistance to penicillin G has not been reported in Streptococcus pyogenes.
Antimicrobial Activity
Penicillin G procaine has been shown to be active against most isolates of the following bacteria, both in vitro and in clinical infections as described in the INDICATIONS AND USAGE section.
Gram-positive Bacteria
Streptococcus pyogenes
Streptococcus pneumoniae
While in vitro studies have demonstrated the susceptibility of most strains of the following organisms, clinical efficacy for infections other than those included in the INDICATIONS AND USAGE section has not been documented. Penicillin G is also active in vitro against susceptible strains of the following organisms: Neisseria meningitidis, Corynebacterium diphtheriae, Bacillus anthracis, Clostridium species, Actinomyces species, Spirillum minus, Streptobacillus moniliformis, Listeria monocytogenes, Leptospira species and Treponema pallidum.
-
INDICATIONS AND USAGE
To reduce the development of drug-resistant bacteria and maintain the effectiveness of Penicillin G Procaine and other antibacterial drugs, Penicillin G Procaine should be used only to treat or prevent infections that are proven or strongly suspected to be caused by susceptible bacteria. When culture and susceptibility information are available, they should be considered in selecting or modifying antibacterial therapy. In the absence of such data, local epidemiology and susceptibility patterns may contribute to the empiric selection of therapy.
Penicillin G procaine is indicated in the treatment of moderately severe infections in both adults and pediatric patients due to penicillin-G-susceptible microorganisms that are susceptible to the low and persistent serum levels common to this particular dosage form in the indications listed below. Therapy should be guided by bacteriological studies (including susceptibility tests) and by clinical response.
NOTE: When high, sustained serum levels are required, aqueous penicillin G, either IM or IV, should be used.
The following infections will usually respond to adequate dosages of intramuscular penicillin G procaine: Moderately severe to severe infections of the upper respiratory tract, skin and soft-tissue infections, scarlet fever, and erysipelas due to susceptible streptococci (Group A-without bacteremia).
NOTE: Streptococci in Groups A, C, G, H, L, and M are very sensitive to penicillin G. Other groups, including Group D (enterococcus), are resistant. Aqueous penicillin is recommended for streptococcal infections with bacteremia.
Moderately severe infections of the respiratory tract due to susceptible pneumococci.
NOTE: Severe pneumonia, empyema, bacteremia, pericarditis, meningitis, peritonitis, and arthritis of pneumococcal etiology are better treated with aqueous penicillin G during the acute stage.
Moderately severe infections of the skin and soft tissues due to susceptible staphylococci (penicillin G-susceptible).
NOTE: Reports indicate an increasing number of strains of staphylococci resistant to penicillin G, emphasizing the need for culture and sensitivity studies in treating suspected staphylococcal infections. Indicated surgical procedures should be performed.
Fusospirochetosis (Vincent's gingivitis and pharyngitis). Moderately severe infections of the oropharynx due to susceptible fusiform bacilli and spirochetes.
NOTE: Necessary dental care should be accomplished in infections involving the gum tissue.
Syphilis (all stages) due to susceptible Treponema pallidum.
NOTE: This drug should not be used in the treatment of beta-lactamase producing organisms which include most strains of Neisseria gonorrhea.
Yaws, Bejel, Pinta due to susceptible organisms.
Penicillin G procaine is an adjunct to antitoxin for prevention of the carrier stage of diphtheria due to susceptible C. diphtheriae.
Anthrax due to Bacillus anthracis, including inhalational anthrax (post-exposure): to reduce the incidence or progression of the disease following exposure to aerosolized Bacillus anthracis.
Rat-bite fever due to susceptible Streptobacillus moniliformis and Spirillum minus organisms.
Erysipeloid due to susceptible Erysipelothrix rhusiopathiae.
Subacute bacterial endocarditis, only in extremely sensitive infections, due to susceptible Group A streptococci.
- CONTRAINDICATIONS
-
WARNINGS
Penicillin G procaine should only be prescribed for the indications listed in this insert.
NOTE: This drug is no longer indicated in the treatment of gonorrhea.
Anaphylaxis
SERIOUS AND OCCASIONALLY FATAL HYPERSENSITIVITY (ANAPHYLACTIC) REACTIONS HAVE BEEN REPORTED IN PATIENTS ON PENICILLIN THERAPY. THESE REACTIONS ARE MORE LIKELY TO OCCUR IN INDIVIDUALS WITH A HISTORY OF PENICILLIN HYPERSENSITIVITY AND/OR A HISTORY OF SENSITIVITY TO MULTIPLE ALLERGENS. THERE HAVE BEEN REPORTS OF INDIVIDUALS WITH A HISTORY OF PENICILLIN HYPERSENSITIVITY WHO HAVE EXPERIENCED SEVERE REACTIONS WHEN TREATED WITH CEPHALOSPORINS. BEFORE INITIATING THERAPY WITH ANY PENICILLIN, CAREFUL INQUIRY SHOULD BE MADE CONCERNING PREVIOUS HYPERSENSITIVITY REACTIONS TO PENICILLINS, CEPHALOSPORINS, OR OTHER ALLERGENS. IF AN ALLERGIC REACTION OCCURS, THE DRUG SHOULD BE DISCONTINUED AND APPROPRIATE THERAPY INSTITUTED. SERIOUS ANAPHYLACTIC REACTIONS REQUIRE IMMEDIATE EMERGENCY TREATMENT WITH EPINEPHRINE. OXYGEN, INTRAVENOUS STEROIDS, AND AIRWAY MANAGEMENT, INCLUDING INTUBATION, SHOULD ALSO BE ADMINISTERED AS INDICATED.
Severe cutaneous adverse reactions
Severe cutaneous adverse reactions (SCAR), such as Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), drug reaction with eosinophilia and systemic symptoms (DRESS), and acute generalized exanthematous pustulosis (AGEP) have been reported in patients taking beta-lactam antibiotics. When SCAR is suspected, Penicillin G Procaine should be discontinued immediately and an alternative treatment should be considered.
Methemoglobinemia
Cases of methemoglobinemia have been reported in association with local anesthetic use. Although all patients are at risk for methemoglobinemia, patients with glucose-6-phosphate dehydrogenase deficiency, congenital or idiopathic methemoglobinemia, cardiac or pulmonary compromise, infants under 6 months of age, and concurrent exposure to oxidizing agents or their metabolites are more susceptible to developing clinical manifestations of the condition. If local anesthetics must be used in these patients, close monitoring for symptoms and signs of methemoglobinemia is recommended.
Signs of methemoglobinemia may occur immediately or may be delayed some hours after exposure, and are characterized by a cyanotic skin discoloration and/or abnormal coloration of the blood. Methemoglobin levels may continue to rise; therefore, immediate treatment is required to avert more serious central nervous system (CNS) and cardiovascular adverse effects, including seizures, coma, arrhythmias, and death. Discontinue Penicillin G Procaine and any other oxidizing agents. Depending on the severity of the signs and symptoms, patients may respond to supportive care, i.e., oxygen therapy, hydration. A more severe clinical presentation may require treatment with methylene blue, exchange transfusion, or hyperbaric oxygen.
Pseudomembranous Colitis
Pseudomembranous colitis has been reported with nearly all antibacterial agents, including penicillin G, and may range in severity from mild to life-threatening. Therefore, it is important to consider this diagnosis in patients who present with diarrhea subsequent to the administration of antibacterial agents.
Treatment with antibacterial agents alters the normal flora of the colon and may permit overgrowth of clostridium. Studies indicate that a toxin produced by Clostridium difficile is one primary cause of "antibiotic-associated colitis."
After the diagnosis of pseudomembranous colitis has been established, therapeutic measures should be initiated. Mild cases of pseudomembranous colitis usually respond to drug discontinuation alone. In moderate to severe cases, consideration should be given to management of fluids and electrolytes, protein supplementation and treatment with an antibacterial drug clinically effective against C. difficile colitis.
Procaine Reactions
Immediate toxic reactions to procaine may occur in some individuals, particularly when a large single dose is administered (4.8 million units). These reactions may be manifested by mental disturbances, including anxiety, confusion, agitation, depression, weakness, seizures, hallucinations, combativeness, and expressed "fear of impending death." The reactions noted in carefully controlled studies occurred in approximately one in 500 patients who received large doses of penicillin G procaine. Reactions are transient, lasting from 15 to 30 minutes.
Method of Administration
Do not inject into or near an artery or nerve.
Injection into or near a nerve may result in permanent neurological damage.
Inadvertent intravascular administration, including inadvertent direct intra-arterial injection or injection immediately adjacent to arteries, of Penicillin G Procaine Injectable Suspension and other penicillin preparations has resulted in severe neurovascular damage, including transverse myelitis with permanent paralysis, gangrene requiring amputation of digits and more proximal portions of extremities, and necrosis and sloughing at and surrounding the injection site consistent with the diagnosis of Nicolau syndrome. Such severe effects have been reported following injections into the buttock, thigh, and deltoid areas. Other serious complications of suspected intravascular administration which have been reported include immediate pallor, mottling, or cyanosis of the extremity, both distal and proximal to the injection site, followed by bleb formation; severe edema requiring anterior and/or posterior compartment fasciotomy in the lower extremity. The above-described severe effects and complications have most often occurred in infants and small children. Prompt consultation with an appropriate specialist is indicated if any evidence of compromise of the blood supply occurs at, proximal to, or distal to the site of injection.1–9 (See PRECAUTIONS, and DOSAGE AND ADMINISTRATION.)
FOR DEEP INTRAMUSCULAR INJECTION ONLY. Administer by DEEP INTRAMUSCULAR INJECTION ONLY in the upper, outer quadrant of the buttock (dorsogluteal) or the ventrogluteal site. Quadriceps femoris fibrosis and atrophy have been reported following repeated intramuscular injections of penicillin preparations into the anterolateral thigh. Therefore, administration in the anterolateral thigh is not recommended.
-
PRECAUTIONS
General
Prescribing Penicillin G Procaine in the absence of a proven or strongly suspected bacterial infection or a prophylactic indication is unlikely to provide benefit to the patient and increases the risk of the development of drug-resistant bacteria.
Penicillin should be used with caution in individuals with histories of significant allergies and/or asthma.
Care should be taken to avoid intravenous or intra-arterial administration, or injection into or near major peripheral nerves or blood vessels, since such injections may produce neurovascular damage. (See WARNINGS, and DOSAGE AND ADMINISTRATION.)
A small percentage of patients are sensitive to procaine. If there is a history of sensitivity, make the usual test: Inject intradermally 0.1 mL of a 1 to 2 percent procaine solution. Development of an erythema, wheal, flare, or eruption indicates procaine sensitivity. Sensitivity should be treated by the usual methods, including barbiturates, and procaine penicillin preparations should not be used. Antihistaminics appear beneficial in treatment of procaine reactions.
The use of antibiotics may result in overgrowth of nonsusceptible organisms. Constant observation of the patient is essential. If new infections due to bacteria or fungi appear during therapy, the drug should be discontinued and appropriate measures taken.
Whenever allergic reactions occur, penicillin should be withdrawn unless, in the opinion of the physician, the condition being treated is life-threatening and amenable only to penicillin therapy.
Information for Patients
Inform patients that use of local anesthetics may cause methemoglobinemia, a serious condition that must be treated promptly. Advise patients or caregivers to seek immediate medical attention if they or someone in their care experience the following signs or symptoms: pale, gray, or blue colored skin (cyanosis); headache; rapid heart rate; shortness of breath; lightheadedness; or fatigue.
Diarrhea is a common problem caused by antibiotics which usually ends when the antibiotic is discontinued. Sometimes after starting treatment with antibiotics, patients can develop watery and bloody stools (with or without stomach cramps and fever) even as late as two or more months after having taken the last dose of the antibiotic. If this occurs, patients should contact their physician as soon as possible.
Patients should be counseled that antibacterial drugs including Penicillin G Procaine should only be used to treat bacterial infections. They do not treat viral infections (e.g., the common cold). When Penicillin G Procaine is prescribed to treat a bacterial infection, patients should be told that although it is common to feel better early in the course of therapy, the medication should be taken exactly as directed. Skipping doses or not completing the full course of therapy may (1) decrease the effectiveness of the immediate treatment and (2) increase the likelihood that bacteria will develop resistance and will not be treatable by Penicillin G Procaine or other antibacterial drugs in the future.
Laboratory Tests
In suspected staphylococcal infections, proper laboratory studies, including susceptibility tests, should be performed.
In prolonged therapy with penicillin, and particularly with high-dosage schedules, periodic evaluation of the renal and hematopoietic systems is recommended. In such situations, use of penicillin for more than 2 weeks may be associated with an increased risk of neutropenia and an increased incidence of serum sickness-like reactions.
When treating gonococcal infections in which primary or secondary syphilis may be suspected, proper diagnostic procedures, including dark-field examinations, should be done. In all cases in which concomitant syphilis is suspected, monthly serological tests should be made for at least four months.
Drug Interactions
Tetracycline, a bacteriostatic antibiotic, may antagonize the bactericidal effect of penicillin and concurrent use of these drugs should be avoided.
Concurrent administration of penicillin and probenecid increases and prolongs serum penicillin levels by decreasing the apparent volume of distribution and slowing the rate of excretion by competitively inhibiting renal tubular secretion of penicillin.
Patients who are administered local anesthetics are at increased risk of developing methemoglobinemia when concurrently exposed to the following drugs, which could include other local anesthetics:
Examples of Drugs Associated with Methemoglobinemia: Class Examples Nitrates/Nitrites nitroglycerin, nitroprusside, nitric oxide, nitrous oxide Local anesthetics articaine, benzocaine, bupivacaine, lidocaine, mepivacaine, prilocaine, procaine, ropivacaine, tetracaine Antineoplastic agents cyclophosphamide, flutamide, hydroxyurea, ifosfamide, rasburicase Antibiotics dapsone, nitrofurantoin, para-aminosalicylic acid, sulfonamides Antimalarials chloroquine, primaquine Anticonvulsants phenobarbital, sodium valproate Other drugs acetaminophen, metoclopramide, quinine, sulfasalazine Carcinogenesis, Mutagenesis, Impairment of Fertility
No long-term animal studies have been conducted with these drugs.
Pregnancy
Teratogenic effects
Reproduction studies performed in the mouse, rat, and rabbit have revealed no evidence of impaired fertility or harm to the fetus due to penicillin G. Human experience with the penicillins during pregnancy has not shown any positive evidence of adverse effects on the fetus. There are, however, no adequate and well-controlled studies in pregnant women showing conclusively that harmful effects of these drugs on the fetus can be excluded. Because animal reproduction studies are not always predictive of human response, this drug should be used during pregnancy only if clearly needed.
Nursing Mothers
Penicillins are excreted in human milk. Caution should be exercised when penicillins are administered to a nursing woman.
Pediatric Use
Because of incompletely developed renal function in newborns, penicillin elimination may be delayed. Guidelines for administration of this drug to pediatric patients are presented in DOSAGE AND ADMINISTRATION.
Geriatric Use
Clinical studies of penicillin G procaine did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy. This drug is known to be substantially excreted by the kidney, and the risk of toxic reactions to this drug may be greater in patients with impaired renal function. (See CLINICAL PHARMACOLOGY ) Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function.
-
ADVERSE REACTIONS
Allergic Reactions
Penicillin is a substance of low toxicity but does possess a significant index of sensitization. The following hypersensitivity reactions associated with use of penicillin have been reported: Skin rashes, ranging from maculopapular eruptions to exfoliative dermatitis; urticaria; serum-sickness like reactions, including chills, fever, edema, arthralgia, and prostration. Severe and often fatal anaphylaxis has been reported (see WARNINGS). As with other treatments for syphilis, the Jarisch-Herxheimer reaction has been reported.
Procaine toxicity manifestations and hypersensitivity reactions have been reported (see WARNINGS and PRECAUTIONS).
Gastrointestinal
Pseudomembranous colitis has been reported with the use of penicillin G. Onset of pseudomembranous colitis symptoms may occur during or after antibiotic treatment (see WARNINGS).
-
DOSAGE AND ADMINISTRATION
Do not inject into or near an artery or nerve. Injection into or near a nerve may result in permanent neurologic damage (see WARNINGS).
Penicillin G procaine (aqueous) is for intramuscular injection only.
Administer by DEEP INTRAMUSCULAR INJECTION in the upper, outer quadrant of the buttock (dorsogluteal) or the ventrogluteal site. In neonates, infants and small children, the midlateral aspect of the thigh may be preferable. When doses are repeated, vary the injection site.
Because of the high concentration of suspended material in this product, the needle may be blocked if the injection is not made at a slow, steady rate.
Pneumonia (pneumococcal), moderately severe (uncomplicated): 600,000 to 1,000,000 units daily.
Streptococcal infections (Group A), moderately severe to severe tonsillitis, erysipelas, scarlet fever, upper respiratory tract, skin and soft tissue: 600,000 to 1,000,000 units daily for 10-day minimum.
Staphylococcal infections, moderately severe to severe: 600,000 to 1,000,000 units daily.
In pneumonia, streptococcal (Group A) and staphylococcal infections in pediatric patients under 60 pounds: 300,000 units daily.
Bacterial endocarditis (Group A streptococci) only in extremely sensitive infections: 600,000 to 1,000,000 units daily.
Penicillin G procaine is not recommended for prophylaxis against bacterial endocarditis. For prophylaxis against bacterial endocarditis in patients with congenital heart disease or rheumatic or other acquired valvular heart disease when undergoing dental procedures or surgical procedures of the upper respiratory tract, use penicillin V. For patients unable to take oral medications, aqueous penicillin G is recommended.
Syphilis
Primary, secondary, and latent with a negative spinal fluid in adults and pediatric patients over 12 years of age: 600,000 units daily for 8 days-total 4,800,000 units.
Late (tertiary, neurosyphilis, and latent syphilis with positive spinal-fluid examination or no spinal-fluid examination): 600,000 units daily for 10 to 15 days-total 6 to 9 million units.
Congenital syphilis under 70-lb. body weight: 50,000 units/kg/day for 10 days.
Yaws, Bejel, and Pinta: Treatment as for syphilis in corresponding stage of disease.
Diphtheria-adjunctive therapy with antitoxin: 300,000 to 600,000 units daily.
Diphtheria carrier state: 300,000 units daily for 10 days.
Anthrax-cutaneous: 600,000 to 1,000,000 units/day.
Anthrax-inhalational (post-exposure): 1,200,000 units every 12 hours in adults, 25,000 units per kilogram of body weight (maximum 1,200,000 unit) every 12 hours in children. The available safety data for penicillin G procaine at this dose would best support a duration of therapy of 2 weeks or less. Treatment for inhalational anthrax (post-exposure) must be continued for a total of 60 days. Physicians must consider the risks and benefits of continuing administration of penicillin G procaine for more than 2 weeks or switching to an effective alternative treatment.
Vincent's infection (fusospirochetosis): 600,000 to 1,000,000 units/day.
Erysipeloid: 600,000 to 1,000,000 units/day.
Streptobacillus moniliformis and Spirillum minus (rat-bite fever): 600,000 to 1,000,000 units/day.
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit.
-
HOW SUPPLIED
Penicillin G Procaine Injectable Suspension is supplied in packages of 10 syringes and ten 21 gauge, thin-wall 1-1/2 inch needles as follows:
1 mL size, containing 600,000 units per syringe (21 gauge, thin-wall 1-1/2 inch needle), NDC 60793-130-10.
2 mL size, containing 1,200,000 units per syringe (21 gauge, thin-wall 1-1/2 inch needle), NDC 60793-131-10.
Store in a refrigerator, 2° to 8°C (36° to 46°F).
Keep from freezing.
-
REFERENCES
- SHAW, E.: Transverse myelitis from injection of penicillin. Am. J. Dis. Child., 111:548, 1966.
- KNOWLES, J.: Accidental intra-arterial injection of penicillin. Am. J. Dis. Child., 111:552, 1966.
- DARBY, C. et al: Ischemia following an intragluteal injection of benzathine-procaine penicillin G mixture in a one-year-old boy. Clin. Pediatrics, 12:485, 1973.
- BROWN, L. & NELSON, A.: Postinfectious intravascular thrombosis with gangrene. Arch. Surg., 94:652, 1967.
- BORENSTINE, J.: Transverse myelitis and penicillin (Correspondence). Am. J. Dis. Child., 112:166, 1966.
- ATKINSON, J.: Transverse myelopathy secondary to penicillin injection. J. Pediatrics, 75:867, 1969.
- TALBERT, J. et al: Gangrene of the foot following intramuscular injection in the lateral thigh: A case report with recommendations for prevention. J. Pediatrics, 70:110, 1967.
- FISHER, T.: Medicolegal affairs. Canad. Med. Assoc. J., 112:395, 1975.
- SCHANZER, H. et al: Accidental intra-arterial injection of penicillin G. JAMA, 242:1289, 1979.
- SPL UNCLASSIFIED SECTION
-
PRINCIPAL DISPLAY PANEL - 1 mL Syringe Label
NDC: 60793-130-01
Penicillin G Procaine
Injectable Suspension, USP600,000 units per 1 mL syringe
FOR DEEP INTRAMUSCULAR INJECTION ONLY
WARNING: FATAL IF GIVEN BY OTHER ROUTESRefrigerate
Distributed by
Pfizer Inc
New York, NY 10017PAA107514
Lot:
EXP:(YYMMDD)
-
PRINCIPAL DISPLAY PANEL - 1 mL Syringe Package
Ten Syringes (1 mL size) and Ten 21 Gauge,
Thin-Wall 1-1/2 Inch NeedlesNDC: 60793-130-10
Contains 10 of NDC: 60793-130-01Penicillin G Procaine
Injectable Suspension, USP600,000 units per 1 mL syringe
FOR DEEP INTRAMUSCULAR INJECTION ONLY
WARNING: FATAL IF GIVEN BY OTHER ROUTES
BEFORE INJECTING, SEE PACKAGE INSERT FOR ADMINISTRATION INSTRUCTIONS.Pfizer Injectables
Rx only
-
PRINCIPAL DISPLAY PANEL - 2 mL Syringe Label
NDC: 60793-131-01
Penicillin G Procaine
Injectable Suspension, USP1,200,000 units per 2 mL syringe
(600,000 units per mL)FOR DEEP INTRAMUSCULAR INJECTION ONLY
WARNING: FATAL IF GIVEN BY OTHER ROUTESRefrigerate
Distributed by
Pfizer Inc
New York, NY 10017PAA107516
Lot:
EXP:(YYMMDD)
-
PRINCIPAL DISPLAY PANEL - 2 mL Syringe Package
Ten Syringes (2 mL size) and Ten 21 Gauge,
Thin-Wall 1-1/2 Inch NeedlesNDC: 60793-131-10
Contains 10 of NDC: 60793-131-01Penicillin G Procaine
Injectable Suspension, USP1,200,000 units per 2 mL syringe
(600,000 units per mL)FOR DEEP INTRAMUSCULAR INJECTION ONLY
WARNING: FATAL IF GIVEN BY OTHER ROUTES
BEFORE INJECTING, SEE PACKAGE INSERT FOR ADMINISTRATION INSTRUCTIONS.Pfizer Injectables
Rx only

-
INGREDIENTS AND APPEARANCE
PENICILLIN G PROCAINE
penicillin g procaine injection, suspensionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 60793-130 Route of Administration INTRAMUSCULAR Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength PENICILLIN G PROCAINE (UNII: 17R794ESYN) (PENICILLIN G - UNII:Q42T66VG0C) PENICILLIN G 600000 [iU] in 1 mL Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 60793-130-10 10 in 1 PACKAGE 04/26/1948 1 NDC: 60793-130-01 1 mL in 1 SYRINGE, GLASS; Type 2: Prefilled Drug Delivery Device/System (syringe, patch, etc.) Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA060101 04/26/1948 PENICILLIN G PROCAINE
penicillin g procaine injection, suspensionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 60793-131 Route of Administration INTRAMUSCULAR Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength PENICILLIN G PROCAINE (UNII: 17R794ESYN) (PENICILLIN G - UNII:Q42T66VG0C) PENICILLIN G 1200000 [iU] in 2 mL Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 60793-131-10 10 in 1 PACKAGE 04/26/1948 1 NDC: 60793-131-01 2 mL in 1 SYRINGE, GLASS; Type 2: Prefilled Drug Delivery Device/System (syringe, patch, etc.) Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA060101 04/26/1948 Labeler - Pfizer Laboratories Div Pfizer Inc (134489525) Establishment Name Address ID/FEI Business Operations King Pharmaceuticals LLC 962691478 ANALYSIS(60793-130, 60793-131) , LABEL(60793-130, 60793-131) , MANUFACTURE(60793-130, 60793-131) , PACK(60793-130, 60793-131)

© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.