XELSTRYM- dextroamphetamine patch, extended release
XELSTRYM by
Drug Labeling and Warnings
XELSTRYM by is a Prescription medication manufactured, distributed, or labeled by Noven Therapeutics, LLC, Noven Pharmaceuticals, Inc.. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use XELSTRYM safely and effectively. See full prescribing information for XELSTRYM.
XELSTRYM® (dextroamphetamine) transdermal system, CII
Initial U.S. Approval: 1975WARNING: ABUSE, MISUSE, AND ADDICTION
See full prescribing information for complete boxed warning.
XELSTRYM has a high potential for abuse and misuse, which can lead to the development of a substance use disorder, including addiction. Misuse and abuse of CNS stimulants, including XELSTRYM, can result in overdose and death (5.1, 9.2, 10):
- Before prescribing XELSTRYM, assess each patient’s risk for abuse, misuse, and addiction.
- Educate patients and their families about these risks, proper storage of the drug, and proper disposal of any unused drug.
- Throughout treatment, reassess each patient’s risk and frequently monitor for signs and symptoms of abuse, misuse, and addiction.
RECENT MAJOR CHANGES
Indications and Usage 09/2025 Warnings and Precautions (5.5) 09/2025 INDICATIONS AND USAGE
XELSTRYM is a central nervous system (CNS) stimulant indicated for the treatment of Attention Deficit Hyperactivity Disorder (ADHD) in adults and pediatric patients 6 years and older (1)
Limitations of Use:The use of XELSTRYM is not recommended in pediatric patients younger than 6 years of age because they had higher plasma exposure and a higher incidence of adverse reactions (e.g., weight loss) than patients 6 years and older at the same dosage (5.5, 8.4).
DOSAGE AND ADMINISTRATION
- Pediatric patients (6 to 17 years): Recommended starting dose is 4.5 mg/9 hours. Titrate dosage in weekly increments of 4.5 mg up to a maximum recommended dose of 18 mg/9 hours (2.2)
- Adults: Recommended starting dose is 9 mg/9 hours. Maximum recommended dose is 18 mg/9 hours (2.2)
- Apply one XELSTRYM transdermal system 2 hours before an effect is needed and remove within 9 hours (2.3)
- Apply XELSTRYM to one of the following sites: hip, upper arm, chest, upper back or flank. Change the site of application when applying a new transdermal system (2.3)
- Do not substitute for other amphetamine products on a milligram-per-milligram basis because of different amphetamine base compositions and differing pharmacokinetic profiles (2.5)
- Severe renal impairment: Maximum recommended dose is 13.5 mg/9 hours (2.6)
- End stage renal disease (ESRD): Maximum recommended dose is 9 mg/9 hours (2.6)
DOSAGE FORMS AND STRENGTHS
Transdermal system: 4.5 mg/9 hours, 9 mg/9 hours, 13.5 mg/9 hours, 18 mg/9 hours (3)
CONTRAINDICATIONS
WARNINGS AND PRECAUTIONS
- Risks to Patients with Serious Cardiac Disease: Avoid use in patients with known structural cardiac abnormalities, cardiomyopathy, serious cardiac arrhythmias, coronary artery disease, or other serious cardiac disease (5.2)
- Increased Blood Pressure and Heart Rate: Monitor blood pressure and pulse (5.3)
- Psychiatric Adverse Reactions: Prior to initiating XELSTRYM, screen patients for risk factors for developing a manic episode. If new psychotic or manic symptoms occur, consider discontinuing XELSTRYM (5.4)
- Long-Term Suppression of Growth in Pediatric Patients: Closely monitor growth (height and weight) in pediatric patients. Pediatric patients not growing or gaining height or weight as expected may need to have their treatment interrupted (5.5)
- Peripheral Vasculopathy, including Raynaud’s phenomenon: Careful observation for digital changes is necessary during XELSTRYM treatment. Further clinical evaluation (e.g., rheumatology referral) may be appropriate for patients who develop signs or symptoms of peripheral vasculopathy (5.6)
- Serotonin Syndrome: Increased risk when co-administered with serotonergic agents (e.g., SSRIs, SNRIs, triptans), but also during overdosage situations. If it occurs, discontinue XELSTRYM and initiate supportive treatment (5.7, 10)
- Contact Sensitization: Use of XELSTRYM may lead to contact sensitization. Discontinue XELSTRYM if contact sensitization is suspected (5.8)
- Application Site Reactions: During wear time or immediately after removal of XELSTRYM, local skin reactions may occur. Select a different application site each day to limit the occurrence of skin reactions (5.9)
- External Heat: Avoid exposing XELSTRYM to external heat sources during wear because both the rate and extent of absorption are increased (5.10)
- Motor and Verbal Tics, and Worsening of Tourette's Syndrome: Before initiating XELSTRYM, assess the family history and clinically evaluate patients for tics or Tourette’s syndrome. Regularly monitor patients for the emergence or worsening of tics or Tourette’s syndrome. Discontinue treatment if clinically appropriate (5.11)
ADVERSE REACTIONS
Most common adverse reactions (incidence ≥2% and greater than the rate for placebo) in pediatric patients 6 to 17 years treated with XELSTRYM were decreased appetite, headache, insomnia, tic, abdominal pain, vomiting, nausea, irritability, blood pressure increased, and heart rate increased (6.1)
Most common adverse reactions (incidence ≥5% and at a rate at least twice placebo) in adults treated with lisdexamfetamine were decreased appetite, insomnia, dry mouth, diarrhea, nausea, and anxiety (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Noven Therapeutics, LLC at 1-877-567-7857 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
USE IN SPECIFIC POPULATIONS
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide.
Revised: 9/2025
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
WARNING: ABUSE, MISUSE, AND ADDICTION
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Pretreatment Screening
2.2 Recommended Dosage
2.3 Important Administration Instructions
2.4 Switching from Other Amphetamine Products
2.5 Dosage in Patients with Renal Impairment
2.6 Dosage Modification due to Drug Interactions
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Abuse, Misuse, and Addiction
5.2 Risks to Patients with Serious Cardiac Disease
5.3 Increased Blood Pressure and Heart Rate
5.4 Psychiatric Adverse Reactions
5.5 Long-Term Suppression of Growth in Pediatric Patients
5.6 Peripheral Vasculopathy, including Raynaud’s Phenomenon
5.7 Serotonin Syndrome
5.8 Contact Sensitization
5.9 Application Site Reactions
5.10 Use of External Heat
5.11 Motor and Verbal Tics, and Worsening of Tourette’s Syndrome
6 ADVERSE REACTIONS
6.1 Clinical Trial Experience
6.2 Postmarketing Experience
7 DRUG INTERACTIONS
7.1 Drugs Having Clinically Important Interactions with Amphetamine
7.2 Drugs Having No Clinically Important Interactions with Amphetamine
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.4 Pediatric Use
8.5 Geriatric Use
8.6 Renal Impairment
9 DRUG ABUSE AND DEPENDENCE
9.1 Controlled Substance
9.2 Abuse
9.3 Dependence
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
13.2 Animal Toxicology and/or Pharmacology
14 CLINICAL STUDIES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- * Sections or subsections omitted from the full prescribing information are not listed.
-
BOXED WARNING
(What is this?)
WARNING: ABUSE, MISUSE, AND ADDICTION
XELSTRYM has a high potential for abuse and misuse, which can lead to the development of a substance use disorder, including addiction. Misuse and abuse of CNS stimulants, including XELSTRYM, can result in overdose and death [see OVERDOSAGE (10)], and this risk is increased with higher doses or unapproved methods of administration, such as snorting or injection.
Before prescribing XELSTRYM, assess each patient’s risk for abuse, misuse, and addiction. Educate patients and their families about these risks, proper storage of the drug, and proper disposal of any unused drug. Throughout XELSTRYM treatment, reassess each patient’s risk of abuse, misuse, and addiction and frequently monitor for signs and symptoms of abuse, misuse, and addiction [see WARNINGS AND PRECAUTIONS (5.1) and DRUG ABUSE AND DEPENDENCE (9.2)].
-
1 INDICATIONS AND USAGE
XELSTRYM® is indicated for the treatment of Attention Deficit Hyperactivity Disorder (ADHD) in adults and pediatric patients 6 years and older [see CLINICAL STUDIES (14)].
Limitations of Use
The use of XELSTRYM is not recommended in pediatric patients younger than 6 years of age because they had higher plasma exposure and a higher incidence of adverse reactions (e.g., weight loss) than patients 6 years and older at the same dosage [see Warnings and Precautions (5.5), Use in Specific Populations (8.4)].
-
2 DOSAGE AND ADMINISTRATION
2.1 Pretreatment Screening
Prior to treating patients with XELSTRYM, assess:
- for the presence of cardiac disease (i.e., perform a careful history, family history of sudden death or ventricular arrhythmia, and physical exam) [see WARNINGS AND PRECAUTIONS (5.2)].
- the family history and clinically evaluate patients for motor or verbal tics or Tourette’s syndrome before initiating XELSTRYM [see WARNINGS AND PRECAUTIONS (5.11)].
2.2 Recommended Dosage
Pediatric Patients 6 to 17 years
- Recommended starting dose of XELSTRYM in pediatric patients 6 to 17 years is 4.5 mg/9 hours. Dosage may be adjusted in weekly increments of 4.5 mg up to a maximum recommended dose of 18 mg/9 hours.
Adults
- Recommended starting dose of XELSTRYM in adults is 9 mg/9 hours. Dosage may be adjusted up to a maximum recommended dose of 18 mg/9 hours.
Apply XELSTRYM to the application site 2 hours before an effect is needed and remove within 9 hours after application. Dose titration and final dosage should be individualized depending on clinical response and tolerability.
2.3 Important Administration Instructions
- Apply one XELSTRYM transdermal system at a time for not more than 9 hours. Use only one XELSTRYM per 24 hours.
- Apply XELSTRYM to clean (void of lotions, oils, or gels), dry (not wet), and intact skin at the selected application site. Application sites include: hip, upper arm, chest, upper back, or flank. Select a different application site each time a new XELSTRYM transdermal system is applied [see WARNINGS AND PRECAUTIONS (5.9)].
- Avoid touching the adhesive side of XELSTRYM in order to avoid absorption of amphetamine. If the adhesive side is touched, immediately wash hands with soap and water.
- If the XELSTRYM transdermal system lifts at the edges, reattach XELSTRYM by pressing firmly and smoothing down the edges of the system. If XELSTRYM comes off completely, apply a new XELSTRYM transdermal system. XELSTRYM should not be applied or re-applied with dressings, tape or other common adhesives.
- Avoid exposing the application site to direct external heat sources, such as hair dryers, heating pads, electric blankets, heated water beds, etc., while wearing XELSTRYM [see WARNINGS AND PRECAUTIONS (5.10)]. When heat is applied to XELSTRYM after application, both the rate and the extent of absorption are increased [see CLINICAL PHARMACOLOGY (12.3)].
2.4 Switching from Other Amphetamine Products
For patients switching from another medication or any other amphetamine product, discontinue that treatment, and titrate with XELSTRYM using the titration schedule [see DOSAGE AND ADMINISTRATION (2.2)].
Do not substitute for other amphetamine products on a milligram-per-milligram basis because of different amphetamine base compositions and differing pharmacokinetic profiles [see CLINICAL PHARMACOLOGY (12.3)].
2.5 Dosage in Patients with Renal Impairment
In patients with severe renal impairment (GFR 15 to < 30 mL/min/1.73 m2), the maximum dose should not exceed 13.5 mg/9 hours. The maximum recommended dose in end stage renal disease (GFR < 15 mL/min/1.73 m2) patients is 9 mg/9 hours [see USE IN SPECIFIC POPULATIONS (8.6)].
2.6 Dosage Modification due to Drug Interactions
Agents that alter urinary pH can impact excretion and alter blood levels of amphetamines. Acidifying agents (e.g., ascorbic acid) decrease blood levels; adjust XELSTRYM dosage based on clinical response [see DRUG INTERACTIONS (7.1)].
- 3 DOSAGE FORMS AND STRENGTHS
-
4 CONTRAINDICATIONS
XELSTRYM is contraindicated in patients:
- with known hypersensitivity to amphetamine products or other components of XELSTRYM. Anaphylactic reactions, Stevens-Johnson Syndrome, angioedema, and urticaria have been observed in postmarketing reports [see ADVERSE REACTIONS (6.2)]
- taking monoamine oxidase inhibitors (MAOI), or within 14 days of stopping MAOIs (including MAOIs such as linezolid or intravenous methylene blue), because of an increased risk of hypertensive crisis [see WARNINGS AND PRECAUTIONS (5.7) and DRUG INTERACTIONS (7.1)]
-
5 WARNINGS AND PRECAUTIONS
5.1 Abuse, Misuse, and Addiction
XELSTRYM has a high potential for abuse and misuse. The use of XELSTRYM exposes individuals to the risks of abuse and misuse, which can lead to the development of a substance use disorder, including addiction. XELSTRYM can be diverted for non-medical use into illicit channels or distribution [see Drug Abuse and Dependence (9.2)]. Misuse and abuse of CNS stimulants, including XELSTRYM, can result in overdose and death [see Overdosage (10)], and this risk is increased with higher doses or unapproved methods of administration, such as snorting or injection.
Before prescribing XELSTRYM, assess each patient’s risk for abuse, misuse, and addiction. Educate patients and their families about these risks and proper disposal of any unused drug. Advise patients to store XELSTRYM in a safe place, preferably locked, and instruct patients to not give XELSTRYM to anyone else. Throughout XELSTRYM treatment, reassess each patient’s risk of abuse, misuse, and addiction and frequently monitor for signs and symptoms of abuse, misuse, and addiction.
5.2 Risks to Patients with Serious Cardiac Disease
Sudden death has been reported in patients with structural cardiac abnormalities or other serious cardiac disease who were treated with CNS stimulants at the recommended ADHD dosage.
Avoid XELSTRYM use in patients with known structural cardiac abnormalities, cardiomyopathy, serious cardiac arrhythmia, coronary artery disease, or other serious cardiac disease.
5.3 Increased Blood Pressure and Heart Rate
CNS stimulants cause an increase in blood pressure (mean increase about 2 to 4 mm Hg) and heart rate (mean increase about 3 to 6 bpm). Monitor all XELSTRYM-treated patients for potential tachycardia and hypertension.
5.4 Psychiatric Adverse Reactions
Exacerbation of Pre-existing Psychosis
CNS stimulants may exacerbate symptoms of behavior disturbance and thought disorder in patients with a pre-existing psychotic disorder.
Induction of a Manic Episode in Patients with Bipolar Disorder
CNS stimulants may induce a manic or mixed episode in patients. Prior to initiating XELSTRYM treatment, screen patients for risk factors for developing a manic episode (e.g., comorbid or history of depressive symptoms or a family history of suicide, bipolar disorder, and depression).
New Psychotic or Manic Symptoms
CNS stimulants, at the recommended dosage, may cause psychotic or manic symptoms (e.g., hallucinations, delusional thinking, or mania) in patients without a prior history of psychotic illness or mania. In a pooled analysis of multiple short-term, placebo-controlled studies of CNS stimulants, psychotic or manic symptoms occurred in approximately 0.1% of CNS stimulant-treated patients compared to 0% of placebo-treated patients. If such symptoms occur, consider discontinuing XELSTRYM.
5.5 Long-Term Suppression of Growth in Pediatric Patients
XELSTRYM is not approved for use and is not recommended in pediatric patients below 6 years of age [see Use in Specific Populations (8.4)].
CNS stimulants have been associated with weight loss and slowing of growth rate in pediatric patients. Closely monitor growth (weight and height) in XELSTRYM-treated pediatric patients treated with CNS stimulants, including XELSTRYM. In a 7-week trial with a dose-optimization phase and a placebo-controlled phase of XELSTRYM in pediatric patients 6 to 17 years old with ADHD, there was a mean decrease in weight while taking XELSTRYM. Additionally, in studies of another CNS stimulant, there was slowing of the increase in height [see ADVERSE REACTIONS (6.1)].
Pediatric patients not growing or gaining height or weight as expected may need to have their treatment interrupted. XELSTRYM is not approved for use in pediatric patients below 6 years of age [see USE IN SPECIFIC POPULATIONS (8.4)].
5.6 Peripheral Vasculopathy, including Raynaud’s Phenomenon
CNS stimulants, including XELSTRYM, used to treat ADHD are associated with peripheral vasculopathy, including Raynaud's phenomenon. Signs and symptoms are usually intermittent and mild; however, sequelae have included digital ulceration and/or soft tissue breakdown. Effects of peripheral vasculopathy, including Raynaud's phenomenon, were observed in post-marketing reports and at the therapeutic dosage of CNS stimulants in all age groups throughout the course of treatment. Signs and symptoms generally improved after dosage reduction or discontinuation of the CNS stimulant. Careful observation for digital changes is necessary during XELSTRYM treatment. Further clinical evaluation (e.g., rheumatology referral) may be appropriate for XELSTRYM-treated patients who develop signs or symptoms of peripheral vasculopathy.
5.7 Serotonin Syndrome
Serotonin syndrome, a potentially life-threatening reaction, may occur when amphetamines are used in combination with other drugs that affect the serotonergic neurotransmitter systems such as monoamine oxidase inhibitors (MAOIs), selective serotonin reuptake inhibitors (SSRIs), serotonin norepinephrine reuptake inhibitors (SNRIs), triptans, tricyclic antidepressants, fentanyl, lithium, tramadol, tryptophan, buspirone, and St. John's Wort [see DRUG INTERACTIONS (7.1)]. The co-administration with cytochrome P450 2D6 (CYP2D6) inhibitors may also increase the risk with increased exposure to XELSTRYM. In these situations, consider an alternative non-serotonergic drug or an alternative drug that does not inhibit CYP2D6 [see DRUG INTERACTIONS (7.1)].
Serotonin syndrome symptoms may include mental status changes (e.g., agitation, hallucinations, delirium, and coma), autonomic instability (e.g., tachycardia, labile blood pressure, dizziness, diaphoresis, flushing, hyperthermia), neuromuscular symptoms (e.g., tremor, rigidity, myoclonus, hyperreflexia, incoordination), seizures, and/or gastrointestinal symptoms (e.g., nausea, vomiting, diarrhea).
Concomitant use of XELSTRYM with MAOI drugs is contraindicated [see CONTRAINDICATIONS (4)].
Discontinue treatment with XELSTRYM and any concomitant serotonergic agents immediately if symptoms of serotonin syndrome occur, and initiate supportive symptomatic treatment. If concomitant use of XELSTRYM with other serotonergic drugs or CYP2D6 inhibitors is clinically warranted, initiate XELSTRYM with lower doses, monitoring patients for the emergence of serotonin syndrome during drug initiation or titration, and inform patients of the increased risk for serotonin syndrome.
5.8 Contact Sensitization
Use of XELSTRYM may lead to contact sensitization (allergic contact dermatitis). Erythema is commonly seen with use of XELSTRYM and is not by itself an indication of sensitization. However, contact sensitization should be suspected if erythema is accompanied by evidence of a more intense local reaction (edema, papules, vesicles) that does not significantly improve within 48 hours or spreads beyond the application site. Confirmation of a diagnosis of contact sensitization may require further diagnostic testing [see CONTRAINDICATION (4)].
Manifestations of systemic sensitization may include a flare-up of previous dermatitis or of prior positive patch-test sites, or generalized skin eruptions in previously unaffected skin. Other systemic reactions may include headache, fever, malaise, arthralgia, diarrhea, or vomiting. No cases of systemic sensitization have been observed in clinical trials of XELSTRYM.
Patients who develop contact sensitization to XELSTRYM and require oral treatment with amphetamine should be initiated on oral medication under close medical supervision. Discontinue XELSTRYM if contact sensitization is suspected. It is possible that some patients sensitized to amphetamine by exposure to XELSTRYM may not be able to take amphetamine in any form.
5.9 Application Site Reactions
Local skin reactions, such as pain, pruritus, burning sensation, erythema, discomfort, edema, and/or swelling were reported during the wear time or immediately after removal of XELSTRYM [see ADVERSE REACTIONS (6.1)]. Patients who experienced discomfort and/or pain during the wear time reported resolution within 2 to 4 hours after application.
The potential for application site reactions and increased skin irritation, discomfort or pain may occur with XELSTRYM if the same application site is used repeatedly. Patients should select a different application site each day to minimize skin reactions.
5.10 Use of External Heat
When heat is applied to XELSTRYM after application, both the rate and extent of absorption are increased. After application of a heating pad, amphetamine exposure (AUC0-9h) was about 1.5-times greater than without heating pad application [see CLINICAL PHARMACOLOGY (12.3)]. Advise patients to avoid exposing XELSTRYM to direct external heat sources such as hair dryers, heating pads, electric blankets, heated water beds, etc., while wearing XELSTRYM.
5.11 Motor and Verbal Tics, and Worsening of Tourette’s Syndrome
CNS stimulants, including amphetamine, have been associated with the onset or exacerbation of motor and verbal tics. Worsening of Tourette’s syndrome has also been reported [see ADVERSE REACTIONS (6.2)].
Before initiating XELSTRYM, assess the family history and clinically evaluate patients for tics or Tourette’s syndrome. Regularly monitor XELSTRYM-treated patients for the emergence or worsening of tics or Tourette’s syndrome, and discontinue treatment if clinically appropriate.
-
6 ADVERSE REACTIONS
The following adverse reactions are discussed in greater detail in other sections of the labeling
- Known hypersensitivity to amphetamine products or other ingredients of XELSTRYM [see CONTRAINDICATIONS (4)]
- Hypertensive Crisis When Used Concomitantly with Monoamine Oxidase Inhibitors [see CONTRAINDICATIONS (4) and DRUG INTERACTIONS (7.1)]
- Abuse, Misuse, and Addiction [see BOXED WARNING, WARNINGS AND PRECAUTIONS (5.1) and DRUG ABUSE AND DEPENDENCE (9.2, 9.3)]
- Risks to Patients with Serious Cardiac Disease [see WARNINGS AND PRECAUTIONS (5.2)]
- Increased Blood Pressure and Heart Rate [see WARNINGS AND PRECAUTIONS (5.3)]
- Psychiatric Adverse Reactions [see WARNINGS AND PRECAUTIONS (5.4)]
- Long-Term Suppression of Growth in Pediatric Patients [see WARNINGS AND PRECAUTIONS (5.5)]
- Peripheral Vasculopathy, including Raynaud's phenomenon [see WARNINGS AND PRECAUTIONS (5.6)]
- Serotonin Syndrome [see WARNINGS AND PRECAUTIONS (5.7)]
- Contact Sensitization [see WARNINGS AND PRECAUTIONS (5.8)]
- Application Site Reactions [see WARNINGS AND PRECAUTIONS (5.9)]
- Use of External Heat [see WARNINGS AND PRECAUTIONS (5.10)]
- Motor and Verbal Tics, and Worsening of Tourette’s Syndrome [see WARNINGS AND PRECAUTIONS (5.11)]
6.1 Clinical Trial Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
The safety of XELSTRYM for the treatment of ADHD in adults and pediatric patients 6 to 17 years is based on a study with XELSTRYM in pediatric patients (presented below) and adequate and well-controlled studies of lisdexamfetamine in adult and pediatric patients with ADHD.
XELSTRYM was studied in pediatric patients 6 to 17 years with ADHD. The safety data are from a 7-week study including a 5-week open-label dose optimization phase (n=110) followed by a 2-week randomized, parallel-group, crossover, placebo-controlled double-blind treatment phase (n=105) [see CLINICAL TRIALS (14)].
Adverse Reactions Leading to Discontinuation of Treatment
In the dose-optimization phase (no placebo comparator in this phase), 2.7% (3/110) of patients treated with XELSTRYM discontinued due to adverse reactions. These adverse reactions reported in one patient each were abdominal pain (0.9%), irritability (0.9%) and decreased appetite (0.9%). There were no discontinuations due to adverse reactions during the double-blind phase.
Adverse Reactions Occurring at an Incidence of 5% or More in XELSTRYM Treated Pediatric Patients Ages 6 to 17 Years During Dose-optimized Treatment
Adverse reactions (incidence of ≥ 5%) that occurred during the dose-optimization phase of the clinical study include: decreased appetite (54%), insomnia1 (32%), headache (21%), irritability (16%), abdominal pain2 (16%) affect lability3 (16%), application site pain4 (13%), nausea (9%), application site pruritus (7%), and fatigue (5%).
1insomnia includes insomnia, delayed sleep phase, initial insomnia, middle insomnia, and terminal insomnia
2abdominal pain includes abdominal pain and abdominal pain upper
3affect lability includes affect lability, emotional disorder, mood swings, and mood altered
4application site pain includes application site pain and application site burnAdverse Reactions Occurring at an Incidence of 2% or More of XELSTRYM-Treated Pediatric Patients Ages 6 to 17 Years During Double-blind Treatment
Adverse reactions (incidence of ≥ 2% and incidence greater than placebo) that occurred during the double-blind, placebo-controlled phase of the clinical study are shown in Table 1.
Table 1: Adverse Reactions Reported by ≥ 2% of Pediatric Patients 6 to 17 Years with ADHD Receiving XELSTRYM and Greater Incidence Than Placebo in the Double-Blind Phase
*The following terms were combined:
Insomnia includes insomnia, delayed sleep phase, initial insomnia, middle insomnia, and terminal insomnia
Abdominal pain includes abdominal pain and abdominal pain upper
Blood pressure increased includes blood pressure increased and blood pressure systolic increased
Heart rate increased includes heart rate increased and tachycardiaSystem Organ Class
Preferred TermXELSTRYM
All Doses
(n = 105)
%Placebo
(n = 105)
%Metabolism and nutrition disorders Decreased appetite 12 2 Nervous system disorders Headache 6 4 Psychiatric disorders Insomnia* 8 6 Affect lability 3 0 Tic 2 0 Gastrointestinal Disorders Vomiting 4 0 Abdominal pain* 4 2 Nausea 3 1 General disorders and administration site conditions Irritability 2 1 Investigations/Cardiac Disorders Blood pressure increased* 2 1 Heart rate increased* 2 0 Application Site Reactions
Based on daily patient diaries and dermal reaction scales at clinic assessments, local skin reactions were reported with XELSTRYM. During the wear time or immediately after removal of XELSTRYM, patients experienced pain, pruritus, burning sensation, erythema, discomfort, edema, and swelling.
Patients who experienced discomfort and pain at the application site during the wear time reported resolution within 2 to 4 hours after XELSTRYM application. Most dermal irritation was limited to the site of application. All patients who reported application site reactions in the 7-week pediatric classroom study continued to use XELSTRYM, and there were no discontinuations from the study due to application site reactions.
During the dose-optimization phase of the clinical study, 45% of patients reported application site discomfort associated with the use of XELSTRYM in daily patient diaries; 72% of patients reported discomfort at clinic visit assessments; and 13% of patients reported severe discomfort at clinic visit assessments. XELSTRYM 4.5 mg was the starting dose for all patients undergoing titration during the dose optimization phase and the majority of application site discomfort was reported at this starting dose. During the dose-optimization phase, 73% of patients reported application site irritation.
Application site reactions that occurred during the double-blind phase of the clinical study are presented in Table 2.
Table 2: Summary Application Site Reactions During the Double-Blind Phase
XELSTRYM
n/NPlacebo
n/NDiscomfort Reported in patient diaries 8/96 (8%) 8/98 (8%) Clinic assessments Any discomfort 72/104 (69%) 9/101 (9%) Severe discomfort 10/104 (10%) 4/101 (4%) Irritation Reported in patient diaries 64/103 (62%) 41/105 (39%) Reported at Clinic assessments 97/103 (94%) 55/101 (54%) Weight Loss and Slowing Growth Rate
In a 7-week trial of XELSTRYM with a 5-week dose optimization phase and a 2-week crossover placebo-controlled phase in pediatric patients ages 6 to 17 years, patients had a mean weight loss from baseline of -3.1 pounds after 5 weeks of XELSTRYM.
Leukopenia and Neutropenia
In the 2-week crossover phase of the 7-week trial of XELSTRYM in pediatric patients ages 6 to 17 years, shifts in WBCs from normal to low occurred in 10% of patients treated with XELSTRYM and 2% of patients treated with placebo. Shifts in neutrophils from normal to low occurred in 14% of patients treated with XELSTRYM and 6% of patients treated with placebo.
Weight Loss and Slowing Growth Rate in Pediatric Patients with ADHD with Lisdexamfetamine and Other Stimulants
Lisdexamfetamine
The long-term safety of XELSTRYM for the treatment of ADHD relies on information from adequate and well-controlled studies of lisdexamfetamine. In a controlled trial of lisdexamfetamine in pediatric patients 6 to 12 years, mean weight loss from baseline after 4 weeks of therapy was -0.9, -1.9, and -2.5 pounds, respectively, for patients receiving 30 mg, 50 mg, and 70 mg of lisdexamfetamine, compared to 1 pound weight gain for patients receiving placebo. Higher doses were associated with greater weight loss with 4 weeks of treatment. Careful follow-up for weight in pediatric patients 6 to 12 years who received lisdexamfetamine over 12 months suggests that consistently medicated pediatric patients (i.e., treatment for 7 days per week throughout the year) have a slowing in growth rate, measured by body weight as demonstrated by an age- and sex-normalized mean change from baseline in percentile, of -13.4 over 1 year (average percentiles at baseline and 12 months were 60.9 and 47.2, respectively). In a 4-week controlled trial of lisdexamfetamine in pediatric patients 13 to 17 years, mean weight loss from baseline to endpoint was -2.7, -4.3, and -4.8 pounds, respectively, for patients receiving 30 mg, 50 mg, and 70 mg of lisdexamfetamine, compared to a 2 pound weight gain for patients receiving placebo.
Other CNS stimulants
Careful follow-up of weight and height in pediatric patients 7 to 10 years who were randomized to either methylphenidate or non-medication treatment groups over 14 months, as well as in naturalistic subgroups of newly methylphenidate-treated and non-medication treated pediatric patients over 36 months (to the ages of 10 to 13 years), suggests that consistently medicated pediatric patients 7 to 13 years (i.e., treatment for 7 days per week throughout the year) have a temporary slowing in growth rate (on average, a total of about 2 cm less growth in height and 2.7 kg less growth in weight over 3 years), without evidence of growth rebound during this period of development. In a controlled trial of amphetamine (d- and l-enantiomer ration of 3:1) in pediatric patients 13 to 17 years, mean weight change from baseline within the initial 4 weeks of therapy was -1.1 pounds and -2.8 pounds, respectively, for patients receiving 10 mg and 20 mg of amphetamine. Higher doses were associated with greater weight loss within the initial 4 weeks of treatment [see WARNINGS AND PRECAUTIONS (5.5)].
Clinical Trials Experience in Adult Patients with ADHD Treated with Lisdexamfetamine
Adverse Reactions Associated with Discontinuation of Treatment in Adult ADHD Clinical Trials
In a controlled trial of lisdexamfetamine in adults with ADHD, 6% (21/358) of lisdexamfetamine-treated patients discontinued due to adverse reactions compared to 2% (1/62) of placebo-treated patients. The most frequently reported adverse reactions (1% or more and twice rate of placebo) were insomnia (8/358; 2%), tachycardia (3/358; 1%), irritability (2/358; 1%), hypertension (4/358; 1%), headache (2/358; 1%), anxiety (2/358; 1%), and dyspnea (3/358; 1%). Less frequently reported adverse reactions (less than 1% or less than twice rate of placebo) included palpitations, diarrhea, nausea, decreased appetite, dizziness, agitation, depression, paranoia and restlessness.
Adverse Reactions Occurring at an Incidence of ≥5% or More Among Lisdexamfetamine-Treated Patients with ADHD in Clinical Trials
The most common adverse reactions (incidence ≥5% and at a rate at least twice placebo) were: Decreased appetite, insomnia, dry mouth, diarrhea, nausea, and anxiety.
In addition, in the adult population, erectile dysfunction was observed in 2.6% of males on lisdexamfetamine and 0% on placebo; decreased libido was observed in 1.4% of subjects on lisdexamfetamine and 0% on placebo.
Weight Loss in Adults with ADHD
In a controlled adult trial of lisdexamfetamine, mean weight loss after 4 weeks of therapy was 2.8 pounds, 3.1 pounds, and 4.3 pounds, for patients receiving final doses of 30 mg, 50 mg, and 70 mg of lisdexamfetamine, respectively, compared to a mean weight gain of 0.5 pounds for patients receiving placebo.
Adverse Reactions with Other Amphetamine Products in Pediatric Patients and Adults with ADHD
Cardiac Disorders: Palpitations, tachycardia, and chest pain.
Gastrointestinal Disorders: Dry mouth, abdominal pain upper, dyspepsia, diarrhea, constipation, vomiting, nausea, and tooth disorder (e.g., teeth clenching, tooth infection).
General Disorders and Administration Site Conditions: Asthenia, fatigue, pyrexia, and feeling jittery.
Infections and Infestations: Infection, urinary tract infection.
Injury, Poisoning, and Procedural Complications: Accidental injury.
Investigations: Weight decreased, blood pressure increased, and ECG voltage criteria for ventricular hypertrophy.
Metabolism and Nutrition Disorders: Loss of appetite.
Musculoskeletal and Connective Tissue Disorders: Muscle twitching, growth retardation.
Nervous System Disorders: Somnolence, insomnia, tremor, dizziness, headache, tics, speech disorder (e.g., stuttering, excessive speech), psychomotor hyperactivity, and agitation.
Psychiatric Disorders: Depression, anxiety, dermatillomania, mood swings, anger, affect lability, logorrhea, irritability, nervousness, paranoia, and restlessness.
Reproductive System and Breast Disorders: Impotence, libido decreased, erectile dysfunction, and dysmenorrhea.
Respiratory, Thoracic, and Mediastinal Disorders: Dyspnea, rhinitis allergic.
Skin and Subcutaneous Tissue Disorders: Rash, photosensitivity reaction, and hyperhidrosis.
Vascular Disorders: Hypertension, epistaxis.
6.2 Postmarketing Experience
The following adverse reactions have been identified during post-approval use of amphetamines. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Cardiac Disorders: Palpitations, chest pain, sudden death, and myocardial infarction. There have been isolated reports of cardiomyopathy associated with chronic amphetamine use.
Eye Disorders: Vision blurred, diplopia, difficulties with visual accommodation, and mydriasis.
Gastrointestinal Disorders: Dysgeusia, constipation, intestinal ischemia, and other gastrointestinal disturbances.
Hepatobiliary Disorders: Eosinophilic hepatitis.
Immune System Disorders: Urticaria, rash, hypersensitivity reactions including angioedema and anaphylactic reaction. Serious skin rashes, including Stevens-Johnson Syndrome and toxic epidermal necrolysis, have been reported.
Musculoskeletal and Connective Tissue Disorders: Rhabdomyolysis.
Nervous System Disorders: Seizures, overstimulation, restlessness, dyskinesia, tremor, motor and verbal tics, and paresthesia (including formication).
Psychiatric Disorders: Psychotic episodes at recommended doses, depression, logorrhea, aggression, anger, dermatillomania, bruxism, dysphoria, euphoria, and irritability.
Reproductive System and Breast Disorders: Impotence, changes in libido, and frequent or prolonged erections.
Skin and Subcutaneous Tissue Disorders: Alopecia.
Vascular Disorders: Raynaud's phenomenon.
-
7 DRUG INTERACTIONS
7.1 Drugs Having Clinically Important Interactions with Amphetamine
Table 3: Drugs Having Clinically Important Interactions with Amphetamines
MAO Inhibitors (MAOI) Clinical Impact MAOI antidepressants slow amphetamine metabolism, increasing amphetamine’s effect on the release of norepinephrine and other monoamines from adrenergic nerve endings causing headaches and other signs of hypertensive crisis. Toxic neurological effects and malignant hyperpyrexia can occur, sometimes with fatal results. Intervention Do not administer XELSTRYM during or within 14 days following the administration of MAOI [see CONTRAINDICATIONS (4) and WARNINGS AND PRECAUTIONS (5.7)]. Serotonergic Drugs Clinical Impact The concomitant use of XELSTRYM and serotonergic drugs increases the risk of serotonin syndrome. Intervention Initiate with lower doses and monitor patients for signs and symptoms of serotonin syndrome, particularly during XELSTRYM initiation or dosage increase. If serotonin syndrome occurs, discontinue XELSTRYM and the concomitant serotonergic drug(s) [see WARNINGS AND PRECAUTIONS (5.7)]. CYP2D6 Inhibitors Clinical Impact The concomitant use of XELSTRYM and CYP2D6 inhibitors may increase the exposure of XELSTRYM compared to the use of the drug alone, and increase the risk of serotonin syndrome. Intervention Initiate with lower doses and monitor patients for signs and symptoms of serotonin syndrome, particularly during XELSTRYM initiation and after a dosage increase. If serotonin syndrome occurs, discontinue XELSTRYM and the CYP2D6 inhibitor [see WARNINGS AND PRECAUTIONS (5.7) and OVERDOSAGE (10)]. Alkalinizing Agents Clinical Impact Urinary alkalinizing agents can increase blood levels and potentiate the action of amphetamine. Intervention Co-administration of XELSTRYM and urinary alkalinizing agents should be avoided. Acidifying Agents Clinical Impact Urinary acidifying agents can lower blood levels and efficacy of amphetamines. Intervention Increase dose based on clinical response. Tricyclic Antidepressants Clinical Impact May enhance the activity of tricyclic or sympathomimetic agents causing striking and sustained increases in the concentration of dextroamphetamine in the brain; cardiovascular effects can be potentiated. Intervention Monitor frequently and adjust or use alternative therapy based on clinical response. 7.2 Drugs Having No Clinically Important Interactions with Amphetamine
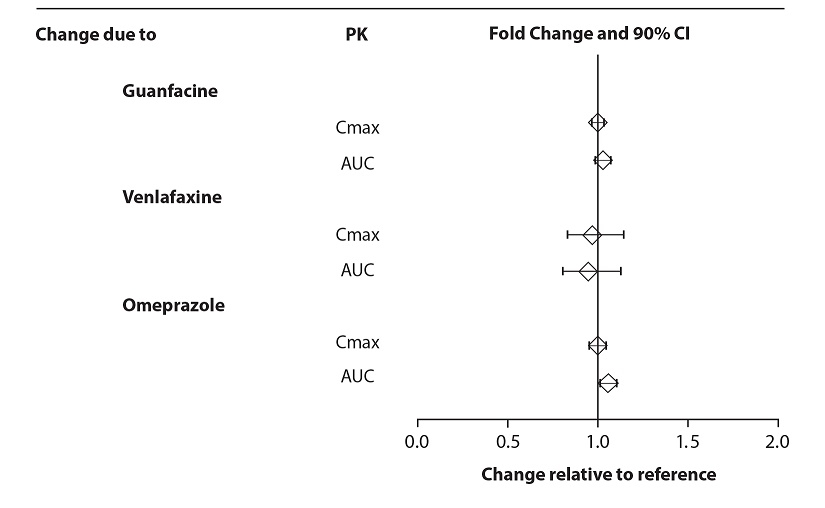
From a pharmacokinetic perspective, no dose adjustment of XELSTRYM is necessary when XELSTRYM is co-administered with guanfacine, venlafaxine, or omeprazole. In addition, no dose adjustment of guanfacine or venlafaxine is needed when XELSTRYM is co-administered [see CLINICAL PHARMACOLOGY (12.3)].
From a pharmacokinetic perspective, no dose adjustment for drugs that are substrates of CYP1A2 (e.g. theophylline, duloxetine, melatonin), CYP2D6 (e.g. atomoxetine, desipramine, venlafaxine), CYP2C19 (e.g. omeprazole, lansoprazole, clobazam), and CYP3A4 (e.g. midazolam, pimozide, simvastatin) is necessary when XELSTRYM is co-administered [see CLINICAL PHARMACOLOGY (12.3)].
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Exposure Registry
There is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to ADHD medications, including XELSTRYM, during pregnancy. Healthcare providers are encouraged to register patients by calling the National Pregnancy Registry for Psychiatric Medications at 1-866-961-2388 or visiting online at https://womensmentalhealth.org/research/pregnancyregistry/adhd-medications/.
Risk Summary
Available data from published epidemiologic studies and postmarketing reports on use of prescription amphetamine in pregnant women have not identified a drug-associated risk of major birth defects and miscarriage (see DATA). Adverse pregnancy outcomes, including premature delivery and low birth weight, have been seen in infants born to mothers taking amphetamines during pregnancy [see CLINICAL CONSIDERATIONS].
No apparent effects on morphological development were observed in embryo-fetal development studies, with oral administration of amphetamine to rats and rabbits during organogenesis. However, in a pre- and post-natal development study, amphetamine (d- to l- ratio of 3:1) administered orally to pregnant rats during gestation and lactation caused a decrease in pup survival and a decrease in pup body weight that correlated with a delay in developmental landmarks at clinically relevant doses of amphetamine. In addition, adverse effects on reproductive performance were observed in pups whose mothers were treated with amphetamine. Long-term neurochemical and behavioral effects have also been reported in animal developmental studies using clinically relevant doses of amphetamine (see DATA).
The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2 to 4% and 15 to 20%, respectively.
Fetal/Neonatal Adverse Reactions
Amphetamines, such as XELSTRYM, cause vasoconstriction and thereby may decrease placental perfusion. In addition, amphetamines can stimulate uterine contractions, increasing the risk of premature delivery. Infants born to mothers taking amphetamines during pregnancy have an increased risk of premature delivery and low birth weight.
Monitor infants born to mothers taking amphetamines for symptoms of withdrawal such as feeding difficulties, irritability, agitation, and excessive drowsiness.
Animal Data
Amphetamine (d- to l- enantiomer ratio of 3:1) had no apparent effects on embryofetal morphological development or survival when administered orally to pregnant rats and rabbits throughout the period of organogenesis at doses of up to 6 and 16 mg/kg/day, respectively. Fetal malformations and death have been reported in mice following parenteral administration of amphetamine doses of 50 mg/kg/day or greater to pregnant animals. Administration of these doses was also associated with severe maternal toxicity.
A study was conducted in which pregnant rats received daily oral doses of amphetamine (d- to l- enantiomer ratio of 3:1) of 2, 6, and 10 mg/kg from gestation day 6 to lactation day 20. All doses caused hyperactivity and decreased weight gain in the dams. A decrease in pup survival was seen at all doses. A decrease in pup body weight was seen at 6 and 10 mg/kg which correlated with delays in developmental landmarks, such as preputial separation and vaginal opening. Increased pup locomotor activity was seen at 10 mg/kg on day 22 postpartum but not at 5 weeks postweaning. When pups were tested for reproductive performance at maturation, gestational weight gain, number of implantations, and number of delivered pups were decreased in the group whose mothers had been given 10 mg/kg.
A number of studies from the literature in rodents indicate that prenatal or early postnatal exposure to amphetamine (d- or d, l-) at doses similar to those used clinically can result in long-term neurochemical and behavioral alterations. Reported behavioral effects include learning and memory deficits, altered locomotor activity, and changes in sexual function.
8.2 Lactation
Risk Summary
Based on limited case reports in published literature, amphetamine (d- or d, l-) is present in human milk, at relative infant doses of 2% to 13.8% of the maternal weight-adjusted dosage and a milk/plasma ratio ranging between 1.9 and 7.5. There are no reports of adverse effects on the breastfed infant. Long-term neurodevelopmental effects on infants from amphetamine exposure are unknown. It is possible that large dosages of amphetamine might interfere with milk production, especially in women whose lactation is not well established. Because of the potential for serious adverse reactions in nursing infants, including serious cardiovascular reactions, blood pressure and heart rate increase, suppression of growth, and peripheral vasculopathy, advise patients that breastfeeding is not recommended during treatment with XELSTRYM.
8.4 Pediatric Use
The safety and effectiveness of XELSTRYM have not been established in pediatric patients below the age of 6 years.
The safety and effectiveness of XELSTRYM have been established in pediatric patients with ADHD ages 6 to 17 years [see ADVERSE REACTIONS (6.1), CLINICAL PHARMACOLOGY (12.3), and CLINICAL STUDIES (14)].
Safety and efficacy of lisdexamfetamine were evaluated in a double-blind, randomized, parallel-group, placebo-controlled, fixed-dose study in pediatric patients 4 to 5 years with ADHD, followed by a 1-year open-label extension study. In these studies, patients experienced elevated rates of adverse reactions, including weight loss, decreased BMI, decreased appetite, insomnia, infections (upper respiratory and nasopharyngitis), irritability, and affect lability.
Growth Suppression
Growth should be monitored during treatment with stimulants, including XELSTRYM, and pediatric patients who are not growing or gaining weight as expected may need to have their treatment interrupted [see WARNINGS AND PRECAUTIONS (5.5) and ADVERSE REACTIONS (6.1)].
Juvenile Animal Data
Juvenile rats treated with mixed amphetamine salts early in the postnatal period through sexual maturation demonstrated transient changes in motor activity. Learning and memory were impaired. No recovery was seen following a drug free period. A delay in sexual maturation was observed, although there was no effect on fertility.
In a juvenile developmental study, rats received daily oral doses of amphetamine (d- to l- enantiomer ratio of 3:1) of 2, 6, or 20 mg/kg on days 7-13 of age; from day 14 to approximately day 60 of age, these doses were given twice daily for total daily doses of 4, 12, or 40 mg/kg. Post dosing hyperactivity was seen at all doses; motor activity measured prior to the daily dose was decreased during the dosing period but the decreased motor activity was largely absent after an 18 day drug-free recovery period. Performance in the Morris water maze test for learning and memory was impaired at the 40 mg/kg dose, and sporadically at the lower doses, when measured prior to the daily dose during the treatment period; no recovery was seen after a 19 day drug-free period. A delay in the developmental milestones of vaginal opening and preputial separation was seen at 40 mg/kg but there was no effect on fertility.
8.5 Geriatric Use
Clinical studies of XELSTRYM did not include subjects over 65 years to determine whether they respond differently from younger subjects.
Other reported clinical experience and pharmacokinetic data [see CLINICAL PHARMACOLOGY (12.3)] have not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should start at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
8.6 Renal Impairment
Due to reduced clearance in patients with severe renal impairment (GFR 15 to < 30 mL/min/1.73 m2), the maximum XELSTRYM dose should not exceed 13.5 mg/9 hours. The maximum recommended dose in end stage renal disease (GFR < 15 mL/min/1.73 m2) patients is 9 mg/9 hours XELSTRYM.
Dextroamphetamine is not dialyzable.
-
9 DRUG ABUSE AND DEPENDENCE
9.2 Abuse
XELSTRYM has a high potential for abuse and misuse which can lead to the development of a substance use disorder, including addiction [see WARNINGS AND PRECAUTIONS (5.1)]. XELSTRYM can be diverted for non-medical use into illicit channels or distribution.
Abuse is the intentional non-therapeutic use of a drug, even once, to achieve a desired psychological or physiological effect. Misuse is the intentional use, for therapeutic purposes, of a drug by an individual in a way other than prescribed by a health care provider or for whom it was not prescribed. Drug addiction is a cluster of behavioral, cognitive, and physiological phenomena that may include a strong desire to take the drug, difficulties in controlling drug use (e.g., continuing drug use despite harmful consequences, giving a higher priority to drug use than other activities and obligations), and possible tolerance or physical dependence.
Misuse and abuse of dextroamphetamine may cause increased heart rate, respiratory rate, or blood pressure; sweating; dilated pupils; hyperactivity; restlessness; insomnia; decreased appetite; loss of coordination; tremors; flushed skin; vomiting; and/or abdominal pain. Anxiety, psychosis, hostility, aggression, and suicidal or homicidal ideation have also been observed with CNS stimulants abuse and/or misuse. Misuse and abuse of CNS stimulants, including XELSTRYM, can result in overdose and death [see OVERDOSAGE (10)], and this risk is increased with higher doses or unapproved methods of administration, such as snorting or injection.
9.3 Dependence
Physical Dependence
XELSTRYM may produce physical dependence. Physical dependence is a state that develops as a result of physiological adaptation in response to repeated drug use, manifested by withdrawal signs and symptoms after abrupt discontinuation or a significant dose reduction of a drug.
Withdrawal signs and symptoms after abrupt discontinuation or dose reduction following prolonged use of CNS stimulants including XELSTRYM include dysphoric mood; depression; fatigue; vivid, unpleasant dreams; insomnia or hypersomnia; increased appetite; and psychomotor retardation or agitation.
Tolerance
XELSTRYM may produce tolerance. Tolerance is a physiological state characterized by a reduced response to a drug after repeated administration (i.e., a higher dose of a drug is required to produce the same effect that was once obtained at a lower dose).
-
10 OVERDOSAGE
Clinical Effects of Overdose
Overdose of CNS stimulants is characterized by the following sympathomimetic effects:
- Cardiovascular effects including tachyarrhythmias, and hypertension or hypotension. Vasospasm, myocardial infarction, or aortic dissection may precipitate sudden cardiac death. Takotsubo cardiomyopathy may develop.
- CNS effects including psychomotor agitation, confusion, and hallucinations. Serotonin syndrome, seizures, cerebral vascular accidents, and coma may occur.
- Life-threatening hyperthermia (temperatures greater than 104°F) and rhabdomyolysis may develop.
Overdose Management
Consider the possibility of multiple drug ingestion. Dextroamphetamine is not dialyzable. Remove all transdermal systems immediately and cleanse the area(s) to remove any remaining adhesive. The continuing absorption of dextroamphetamine from the skin, even after removal of the transdermal system, should be considered when treating patients with overdose.
Consider contacting the Poison Help line (1-800-222-1222) or a medical toxicologist for additional overdose management recommendations.
-
11 DESCRIPTION
XELSTRYM (dextroamphetamine) transdermal system, contains dextroamphetamine, a CNS stimulant.
Dextroamphetamine is the dextro isomer of the compound d,l-amphetamine. The chemical name for dextroamphetamine is (2S)-1-phenylpropan-2-amine. It is a clear to slightly amber colored liquid. Molecular weight of dextroamphetamine is 135.21 g/mol and the molecular formula is C9H13N. The chemical structure is:
XELSTRYM is provided in four strengths: 4.5 mg/9 hours, 9 mg/9 hours, 13.5 mg/9 hours, and 18 mg/9 hours. The composition per unit area of all dosage strengths is identical. Inactive ingredients include: acrylic adhesives, green ink, polyester/polyurethane backing, and polyester release liner.
Table 4: XELSTRYM (dextroamphetamine) transdermal system
Dosage Strength (dextroamphetamine) Dextroamphetamine Content per Transdermal System Transdermal System Size 4.5 mg / 9 hours 5 mg 4.76 cm2 9 mg / 9 hours 10 mg 9.52 cm2 13.5 mg / 9 hours 15 mg 14.29 cm2 18 mg / 9 hours 20 mg 19.05 cm2 Transdermal System Components
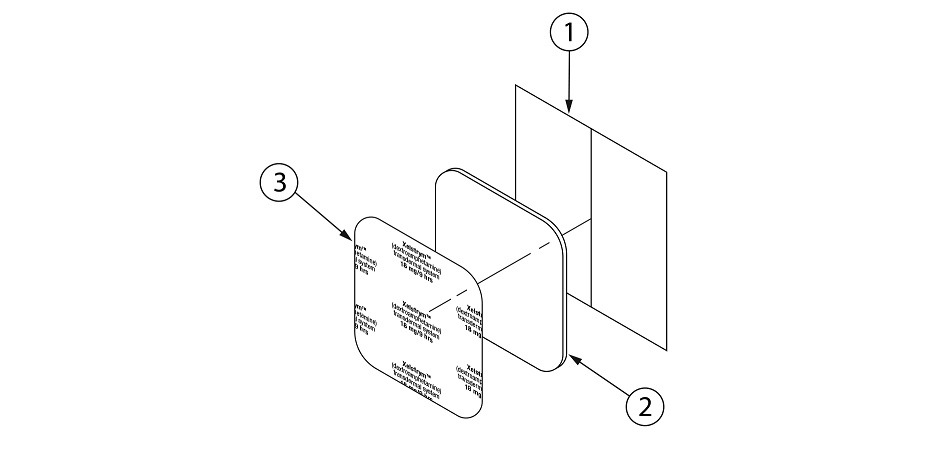
XELSTRYM consists of three layers (Figure 1). The layers are (1) oversized protective silicone-coated polyester release liner that is removed and discarded prior to application (2) acrylic adhesive matrix containing dextroamphetamine, and (3) polyester and polyurethane laminate film (backing).
Figure 1: XELSTRYM Transdermal System (Exploded View)
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Amphetamines are non-catecholamine sympathomimetic amines with CNS stimulant activity. The exact mode of therapeutic action in ADHD is not known.
12.2 Pharmacodynamics
Amphetamines block the reuptake of norepinephrine and dopamine into the presynaptic neuron and increase the release of these monoamines into the extraneuronal space.
12.3 Pharmacokinetics
Following a single 9-hour application of XELSTRYM in pediatric patients 6 to 12 years with ADHD, the Cmax and AUC of dextroamphetamine were dose-proportional over the dose range of 4.5 mg/9 hours to 18 mg/9 hours.
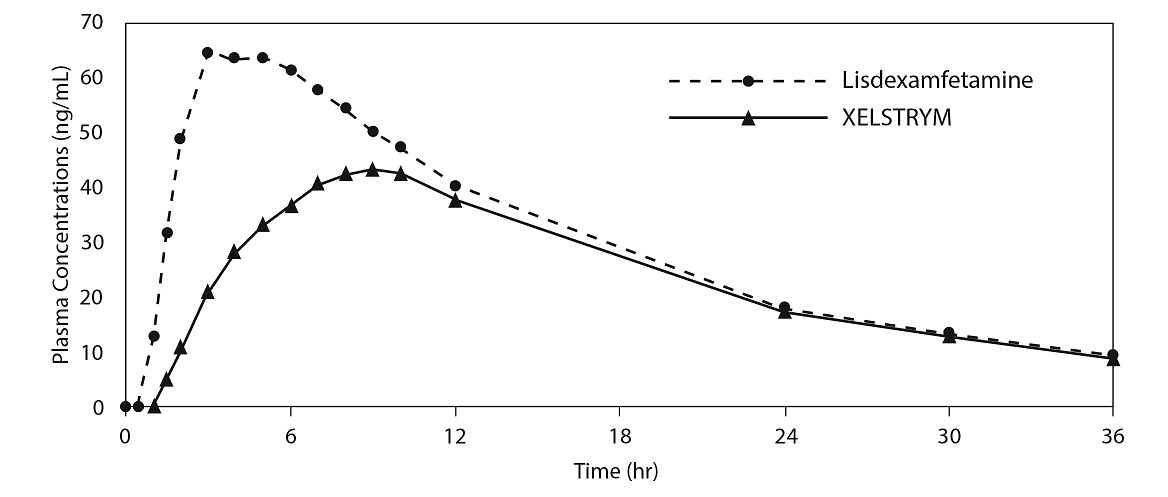
After a single dose of 18 mg/9 hours of XELSTRYM or 70 mg of lisdexamfetamine in adults, the peak plasma concentration (Cmax) of dextroamphetamine were 44.6 ng/mL and 67.6 ng/mL, respectively; and area under concentration curve (AUCinf) of dextroamphetamine were 996 ng*h/mL and 1260 ng*h/mL, respectively. Median time-to-peak concentrations (tmax) was 9 hours for XELSTRYM and 4 hours for lisdexamfetamine.
The plasma PK profiles of dextroamphetamine following administration of XELSTRYM and lisdexamfetamine are shown in Figure 2.
Figure 2: Mean Plasma Concentrations versus Time Profile of Dextroamphetamine After a Single Dose Administration of XELSTRYM and Lisdexamfetamine in Healthy Adults
After multiple dosing of 18 mg/9 hours of XELSTRYM with application site rotation in adults or 70 mg of lisdexamfetamine (simulated), Cmax of dextroamphetamine were 68.8 ng/mL and 84.5 ng/mL, respectively; AUC0-24 of dextroamphetamine were 1150 ng*h/mL and 1248 ng*h/mL, respectively.
Absorption
The amount of dextroamphetamine absorbed systemically is a function of both wear time and transdermal system size. Peak plasma levels of dextroamphetamine were typically reached at 6 to 9 hours after single application and 6 hours after repeat applications of XELSTRYM when worn up to 9 hours.
On average, approximately 90% of dextroamphetamine is delivered from the transdermal system over 9 hours. Inter-individual variability for XELSTRYM as coefficient of variation (%CV) for the dextroamphetamine Cmax and AUC was generally about 20% to 30%.
After repeat applications of XELSTRYM for 4 weeks in adults with ADHD, there was 46% increase in Cmax and 54% increase in AUC0-24 when applied with rotating application sites for each transdermal system. There was 86% increase in Cmax and 104% increase in AUC0-24 when XELSTRYM was applied on the same site for 28 days.
Application of a heating pad on XELSTRYM for 6 consecutive hours led to a faster absorption rate (median Tmax about 6.5 hours) as compared with XELSTRYM without a heating pad (median Tmax about 8.5 hours). Geometric least square mean ratios for dextroamphetamine exposure, calculated as Cmax and AUC0-9h, were about 116% and 150%, respectively, compared with XELSTRYM without a heating pad, indicating the apparent heat effect on dextroamphetamine absorption.
The application of XELSTYRM to different sites (hip, upper arm, chest, upper back and flank) did not alter dextroamphetamine PK.
Elimination
When XELSTRYM is removed after 9 hours wear time, the mean apparent elimination half-life of dextroamphetamine ranged from 6.4 to 11.5 hours in the pediatric and adult population, respectively.
Metabolism
Amphetamine is reported to be oxidized at the 4 position of the benzene ring to form 4-hydroxyamphetamine, or on the side chain α or β carbons to form alpha-hydroxy-amphetamine or norephedrine, respectively. Norephedrine and 4-hydroxy-amphetamine are both active and each is subsequently oxidized to form 4-hydroxy-norephedrine. Alpha-hydroxy-amphetamine undergoes deamination to form phenylacetone, which ultimately forms benzoic acid and its glucuronide and the glycine conjugate hippuric acid. Although the enzymes involved in amphetamine metabolism have not been clearly defined, CYP2D6 is known to be involved with formation of 4-hydroxy-amphetamine. Since CYP2D6 is genetically polymorphic, population variations in amphetamine metabolism are a possibility.
Excretion
With normal urine pHs, approximately half of an administered oral dose of amphetamine is recoverable in urine as derivatives of alpha-hydroxy-amphetamine and approximately another 30-40% of the dose is recoverable in urine as amphetamine itself. Since amphetamine has a pKa of 9.9, urinary recovery of amphetamine is highly dependent on pH and urine flow rates. Alkaline urine pHs result in less ionization and reduced renal elimination, and acidic pHs and high flow rates result in increased renal elimination with clearances greater than glomerular filtration rates, indicating the involvement of active secretion. Urinary recovery of amphetamine has been reported to range from 1% to 75%, depending on urinary pH, with the remaining fraction of the dose hepatically metabolized. Consequently, both hepatic and renal dysfunction have the potential to inhibit the elimination of amphetamine and result in prolonged exposures. In addition, drugs that affect urinary pH are known to alter the elimination of amphetamine, and any decrease in amphetamine's metabolism that might occur due to drug interactions or genetic polymorphisms is more likely to be clinically significant when renal elimination is decreased [see DRUG INTERACTIONS (7)].
Specific Populations
The shapes of pharmacokinetic profiles after XELSTRYM application were generally similar between the pediatric and the adult population. Based on population PK, the median Cmax in pediatric patients 6 to 17 years are predicted to be 120% and 180%, respectively, the median AUC in pediatric patients are predicted to be 112% and 148%, respectively, of those in adults with a dose of 18 mg/9 hours.
Exposures of dextroamphetamine in specific populations evaluated with lisdexamfetamine are summarized in Figure 3.
Figure 3: Dextroamphetamine Exposures in Specific Populations
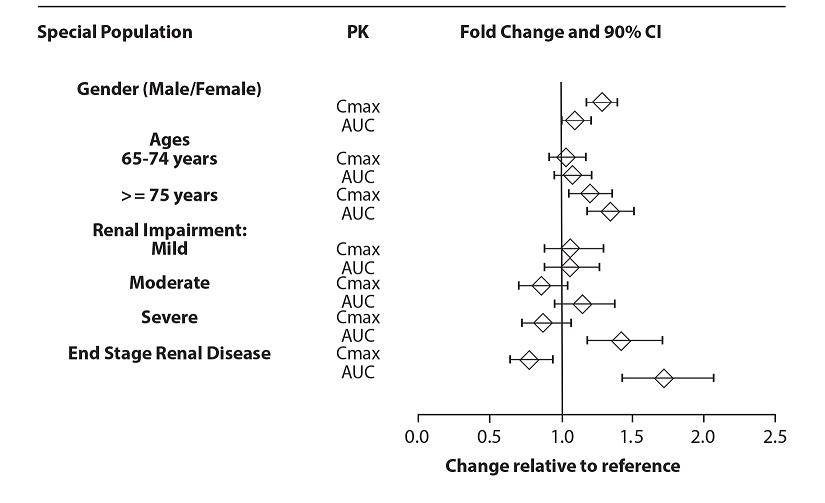
*Figure 3 shows the geometric mean ratios and the 90% confidence limits for Cmax and AUC of dextroamphetamine. Comparison for gender uses males as the reference. Comparison for age uses 55-64 years as the reference
Drug Interaction Studies
Effects of other drugs on the exposures of dextroamphetamine evaluated with lisdexamfetamine are summarized in Figure 4.
Figure 4: Effect of Other Drugs on Dextroamphetamine
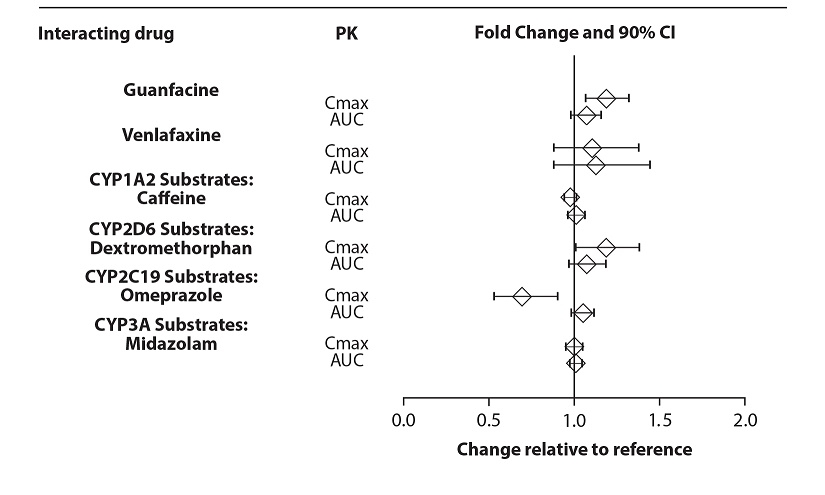
The effects of dextroamphetamine on the exposures of other drugs evaluated with lisdexamfetamine are summarized in Figure 5.
Figure 5: Effects of Dextroamphetamine on Other Drugs
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
No evidence of carcinogenicity was found in studies in which d,l-amphetamine (enantiomer ratio of 1:1) was administered to mice and rats in the diet for 2 years at doses of up to 30 mg/kg/day in male mice, 19 mg/kg/day in female mice, and 5 mg/kg/day in male and female rats. Dermal carcinogenicity studies with dextroamphetamine were not conducted.
Mutagenesis
Amphetamine, in the enantiomer ratio d- to l- ratio of 3:1, was not clastogenic in the mouse bone marrow micronucleus test in vivo and was negative when tested in the E. coli component of the Ames test in vitro. d,l-Amphetamine (1:1 enantiomer ratio) has been reported to produce a positive response in the mouse bone marrow micronucleus test, an equivocal response in the Ames test, and negative responses in the in vitro sister chromatid exchange and chromosomal aberration assays.
Impairment of Fertility
Amphetamine, in the enantiomer ratio d- to l- ratio of 3:1, did not adversely affect fertility or early embryonic development in the rat at doses of up to 20 mg/kg/day.
-
14 CLINICAL STUDIES
The efficacy of XELSTRYM for the treatment of ADHD in adults and pediatric patients 6 to 17 years was established in a study with XELSTRYM in pediatric patients (presented below) and also based on adequate and well-controlled studies of lisdexamfetamine in pediatric and adult patients. Efficacy of lisdexamfetamine in the treatment of ADHD has been established in three short-term trials in pediatric patients 6 to 12 years, one short-term trial in pediatric patients 13 to 17 years, one short-term trial in pediatric patients 6 to 17 years, two short-term trials in adults 18 to 55 years, and two randomized withdrawal trials in pediatric patients 6 to 17 years and adults 18 to 55 years.
Pediatric Patients 6 to 17 years with ADHD
The efficacy of XELSTRYM for the treatment of ADHD in pediatric patients 6 to 17 years was evaluated in a multi-center, randomized, double-blind, placebo-controlled, cross-over design, modified analog classroom study (Study 1; NCT01711021). The study was conducted in 110 patients who met DSM-IV-TR criteria for ADHD.
Following a 5-week open-label, dose optimization phase with XELSTRYM (4.5 mg/9 hours, 9 mg/9 hours, 13.5 mg/9 hours and 18 mg/9 hours), patients were randomized to one of two treatment sequences: 1) XELSTRYM (optimized dose) followed by placebo, each for one week, or 2) placebo followed by XELSTRYM (optimized dose), each for one week. Efficacy was assessed at the end of each week using the Swanson, Kotkin, Agler, M.Flynn, and Pelham (SKAMP) total score, a validated 13-item rating scale to assess manifestations of ADHD in a classroom setting. Items are specific to place (classroom setting) and time (during a typical classroom period), and the scale is used to assess multiple ratings taken within a day.
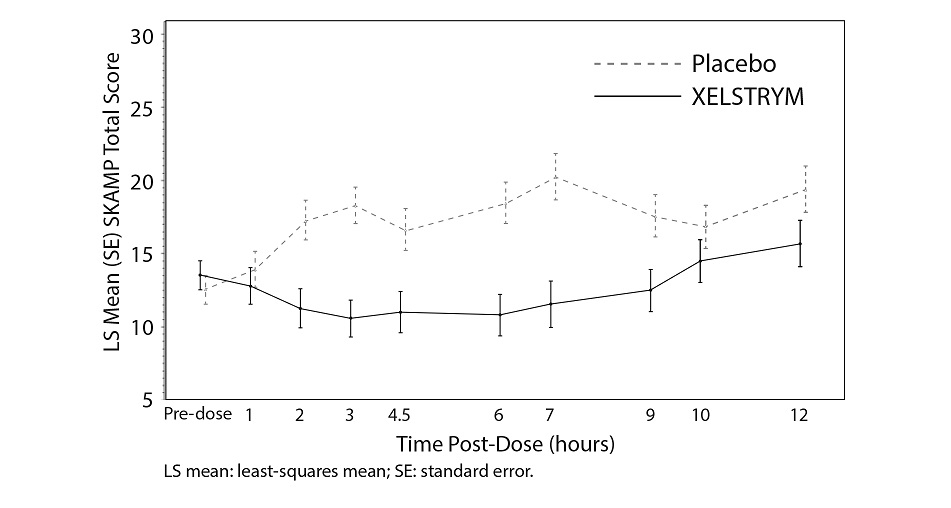
Efficacy was solely based on data from Period 1, which was the first week of the two-week double-blind, placebo-controlled, crossover treatment phase. A statistically significant separation from placebo was observed with use of XELSTRYM in Period 1 (Table 5). Changes in SKAMP total scores assessed at pre-dose (-0.5 hours) and at 1, 2, 3, 4.5, 6, 7, 9, 10, and 12 hours post-application are presented in Figure 6.
Table 5: Summary of Primary Efficacy Results: SKAMP Total Score Averaged Over Classroom Day in Pediatric Patients (6 to 17 years) with ADHD (Period 1 Data only)
SD: standard deviation; SE: standard error; LS Mean: least-squares mean; CI: confidence interval.
a Statistically significant to placebo.
b Pre-dose score on Period 1 classroom day.
c LS mean over hours 1, 2, 3, 4.5, 6, 7, 9, 10, and 12 hours post-dose on Period 1 classroom day.
d Difference (drug minus placebo) in least-squares means on Period 1 classroom day.Study Number Treatment Group Pre-Dose Score on
Classroom Dayb
Mean (SD)LS Meanc
(SE)Placebo-subtracted Differenced
(95% CI)Study 1 XELSTRYMa 13.6 (5.9) 12.4 (1.2) -4.7
(-8.0, -1.4)Placebo 12.7 (7.9) 17.1 (1.2) -------- Figure 6: LS Mean SKAMP Total Score After Treatment with XELSTRYM or Placebo in Period 1 Classroom Day in Pediatric Patients (6 to 17 years) with ADHD (Study 1)
Adhesion
Based on a clinical study in adult subjects wearing XELSTRYM 18 mg/9 hours, 233 of 238 transdermal systems (98%) exhibited 75% or greater surface area adhesion at all timepoints evaluated (every hour) throughout the 9-hour wear period. In another study in which pediatric patients 6 to 17 years and adult patients wearing XELSTRYM 4.5 mg/9 hours or 18 mg/9 hours were not confined to the clinical unit, 50 out of 58 transdermal systems (86%) exhibited 75% or greater surface area adhesion at 9 hours; 3 transdermal systems (5%) were reported as fully detached during the study.
-
16 HOW SUPPLIED/STORAGE AND HANDLING
How Supplied
XELSTRYM (dextroamphetamine) transdermal system is a translucent product with a printed backing on one side and a release liner on the other packaged in an individual pouch supplied as:
-
4.5 mg/9 hours transdermal system (system size: 4.76 cm2)
Carton of 30 transdermal systems, each transdermal system is packaged in an individual pouch
NDC: 68968-0205-3
-
9 mg/9 hours transdermal system (system size: 9.52 cm2)
Carton of 30 transdermal systems, each transdermal system is packaged in an individual pouch
NDC: 68968-0210-3
-
13.5 mg/9 hours transdermal system (system size: 14.29 cm2)
Carton of 30 transdermal systems, each transdermal system is packaged in an individual pouch
NDC: 68968-0215-3
-
18 mg/9 hours transdermal system (system size: 19.05 cm2)
Carton of 30 transdermal systems, each transdermal system is packaged in an individual pouch
NDC: 68968-0220-3
Storage and Handling
Store at 68°F to 77° F (20°C to 25° C); excursions permitted between 15°C to 30° C (59 to 86° F) [see USP Controlled Room Temperature]. Protect from light.
Store XELSTRYM in the individual sealed pouch until use. Apply immediately upon removal from the protective pouch.
-
4.5 mg/9 hours transdermal system (system size: 4.76 cm2)
-
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Medication Guide and Instructions for Use).
Abuse, Misuse, and Addiction
Educate patients and their families about the risks of abuse, misuse, and addiction of XELSTRYM, which can lead to overdose and death, and proper disposal of any unused drug [see WARNINGS AND PRECAUTIONS (5.1), DRUG ABUSE AND DEPENDENCE (9.2), OVERDOSAGE (10)]. Advise patients to store XELSTRYM in a safe place, preferably locked, and instruct patients to not give XELSTRYM to anyone else.
Risks to Patients with Serious Cardiac Disease
Advise patients that there are potential risks to patients with serious cardiac disease, including sudden death, with XELSTRYM use. Instruct patients to contact a healthcare provider immediately if they develop symptoms such as exertional chest pain, unexplained syncope, or other symptoms suggestive of cardiac disease [see WARNINGS AND PRECAUTIONS (5.2)].
Increased Blood Pressure and Heart Rate
Advise patients that XELSTRYM can elevate blood pressure and heart rate [see WARNINGS AND PRECAUTIONS (5.3)].
Psychiatric Adverse Reactions
Advise patients that XELSTRYM, at recommended doses, can cause psychotic or manic symptoms, even in patients without prior history of psychotic symptoms or mania [see WARNINGS AND PRECAUTIONS (5.4)].
Long-Term Suppression of Growth in Pediatric Patients
Advise patients that XELSTRYM may cause slowing of growth including weight loss [see WARNINGS AND PRECAUTIONS (5.5)].
Circulation problems in fingers and toes [Peripheral vasculopathy, including Raynaud's phenomenon]
Instruct patients beginning treatment with XELSTRYM about the risk of peripheral vasculopathy, including Raynaud's Phenomenon, and associated signs and symptoms: fingers or toes may feel numb, cool, painful, and/or may change from pale, to blue, to red. Instruct patients to report to their physician any new numbness, pain, skin color change, or sensitivity to temperature in fingers or toes. Instruct patients to call their physician immediately with any signs of unexplained wounds appearing on fingers or toes while taking XELSTRYM. Further clinical evaluation (e.g. rheumatology referral) may be appropriate for certain patients [see WARNINGS AND PRECAUTIONS (5.6)].
Serotonin Syndrome
Caution patients about the risk of serotonin syndrome with concomitant use of XELSTRYM and other serotonergic drugs including SSRIs, SNRIs, triptans, tricyclic antidepressants, fentanyl, lithium, tramadol, tryptophan, buspirone, St. John's Wort, and with drugs that impair metabolism of serotonin (in particular MAOIs, both those intended to treat psychiatric disorders and also others such as linezolid [see CONTRAINDICATIONS (4), WARNINGS AND PRECAUTIONS (5.7) and DRUG INTERACTIONS (7.1)]. Advise patients to contact their healthcare provider or report to the emergency room if they experience signs or symptoms of serotonin syndrome.
Application Site Reactions
Inform patients that application site reactions, including pain, pruritus, burning sensation, erythema, discomfort, edema, or swelling have been reported with the use of XELSTRYM. Inform patients that increased skin irritation, discomfort or pain may occur if the same application site is used repeatedly. Instruct patients to select a different application site each day to minimize skin reactions. Patients should monitor for these reactions while wearing or immediately after removal of XELSTRYM. Discontinue XELSTRYM if contact sensitization is suspected [see WARNINGS AND PRECAUTIONS (5.9)].
External Heat
Inform patients to avoid exposing XELSTRYM to external heat sources, such as hair dryers, heating pads, electric blankets, heated water beds, etc. [see WARNINGS AND PRECAUTIONS (5.10)].
Motor and Verbal Tics, and Worsening of Tourette’s Syndrome
Advise patients that motor and verbal tics and worsening of Tourette’s Syndrome may occur during treatment with XELSTRYM. Instruct patients to notify their healthcare provider if emergence of new tics or worsening of tics or Tourette’s syndrome occurs [see WARNINGS AND PRECAUTIONS (5.11)].
Concomitant Medications
Advise patients to notify their physicians if they are taking, or plan to take, any prescription or over-the-counter drugs because there is a potential for interactions [see DRUG INTERACTIONS (7.1)].
Pregnancy Registry
Advise patients that there is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to XELSTRYM during pregnancy [see USE IN SPECIFIC POPULATIONS (8.1)].
Pregnancy
Advise patients of the potential fetal effects from the use of XELSTRYM during pregnancy. Advise patients to notify their healthcare provider if they become pregnant or intend to become pregnant during treatment with XELSTRYM [see USE IN SPECIFIC POPULATIONS (8.1)].
Lactation
Advise women not to breastfeed if they are taking XELSTRYM [see USE IN SPECIFIC POPULATIONS (8.2)].
Impairment in Ability to Operate Machinery or Vehicles
XELSTRYM may impair the ability of the patient to engage in potentially hazardous activities such as operating machinery or vehicles. Instruct patients to find out how XELSTRYM will affect them before engaging in potentially hazardous activities [see ADVERSE REACTIONS (6.1, 6.2)].
Administration Instructions
Inform patients/caregivers:
- to apply one XELSTRYM transdermal system at a time for not more than 9 hours and use only one XELSTRYM per 24 hours.
- of the application sites: hip, upper arm, chest, upper back, or flank. Advise them to select a different application site each time a new XELSTRYM transdermal system is applied.
- to apply XELSTRYM to clean, dry, and intact skin.
- to wash their hands immediately if they touch the adhesive side of the transdermal system to avoid amphetamine absorption and to check XELSTRYM periodically throughout the wear time [see DOSAGE AND ADMINISTRATION (2.3)].
Manufactured by: Noven Pharmaceuticals, Inc., Miami, FL 33186
For more information, go to www.xelstrym.com or call 1-800-455-8070.
Xelstrym® is a registered trademark of Noven Therapeutics, LLC.
© 2025 Noven Pharmaceuticals, Inc.
102668-3 -
MEDICATION GUIDE
This Medication Guide has been approved by the U.S. Food and Drug Administration. Revised: 9/2025 Medication Guide
XELSTRYM® (Zel’ Strim)
(dextroamphetamine)
transdermal system, CIIWhat is the most important information I should know about XELSTRYM?
XELSTRYM may cause serious side effects, including:
-
Abuse, misuse, and addiction. XELSTRYM has a high chance for abuse and misuse and may lead to substance use problems, including addiction. Misuse and abuse of XELSTRYM, other amphetamine containing medicines, and methylphenidate containing medicines, can lead to overdose and death. The risk of overdose and death is increased with higher doses of XELSTRYM or when it is used in ways that are not approved, such as snorting or injection.
- Your healthcare provider should check you or your child’s risk for abuse, misuse, and addiction before starting treatment with XELSTRYM and will monitor you or your child during treatment.
- XELSTRYM may lead to physical dependence after prolonged use, even if taken as directed by your healthcare provider.
- Do not give XELSTRYM to anyone else. See “What is XELSTRYM?” for more information.
- Keep XELSTRYM in a safe place and properly dispose of any unused medicine. See “How should I store XELSTRYM?” for more information.
- Tell your healthcare provider if you or your child have ever abused or been dependent on alcohol, prescription medicines, or street drugs.
-
Risks for people with serious heart disease. Sudden death has happened in people who have heart defects or other serious heart disease.
Your healthcare provider should check you or your child carefully for heart problems before starting treatment with XELSTRYM. Tell your healthcare provider if you or your child have any heart problems, heart disease, or heart defects.Call your healthcare provider or go to the nearest hospital emergency room right away if you or your child have any signs of heart problems such as chest pain, shortness of breath, or fainting during treatment with XELSTRYM.
-
Increased blood pressure and heart rate.
Your healthcare provider should check your or your child’s blood pressure and heart rate regularly during treatment with XELSTRYM.
-
Mental (psychiatric) problems, including:
- new or worse behavior and thought problems
- new or worse bipolar illness
- new psychotic symptoms (such as hearing voices, or seeing or believing things that are not real) or new manic symptoms
Tell your healthcare provider about any mental problems you or your child have or about a family history of suicide, bipolar illness, or depression.
Call your healthcare provider right away if you or your child have any new or worsening mental symptoms or problems during treatment with XELSTRYM, especially hearing voices, seeing or believing things that are not real, or new manic symptoms.
What is XELSTRYM?
XELSTRYM is a central nervous system (CNS) stimulant prescription medicine used for the treatment of Attention-Deficit Hyperactivity Disorder (ADHD) in adults and children 6 years of age and older. XELSTRYM may help increase attention and decrease impulsiveness and hyperactivity in adults and children 6 years of age and older with ADHD.
XELSTRYM is not recommended for use in children under 6 years of age with ADHD.
XELSTRYM is a federally controlled substance (CII) because it contains dextroamphetamine that can be a target for people who abuse prescription medicines or street drugs. Keep XELSTRYM in a safe place to protect it from theft. Never give your XELSTRYM to anyone else, because it may cause death or harm them. Selling or giving away XELSTRYM may harm others and is against the law.
Do not use XELSTRYM if you or your child are:
- allergic to amphetamine products or any of the ingredients in XELSTRYM. See the end of the Medication Guide for a complete list of ingredients in XELSTRYM.
- taking or have taken within the past 14 days a medicine called a monoamine oxidase inhibitor (MAOI), including the antibiotic linezolid or the intravenous medicine called methylene blue.
Before using XELSTRYM, tell your healthcare provider about all medical conditions, including if you or your child:
- have heart problems, heart disease, heart defects, or high blood pressure
- have mental problems including psychosis, mania, bipolar illness, or depression or have a family history of suicide, bipolar illness, or depression
- have circulation problems in fingers and toes
- have kidney problems. Your healthcare provider may lower your dose.
- have or had repeated movements or sounds (tics) or Tourette's syndrome, or have a family history of tics or Tourette's syndrome
- are pregnant or plan to become pregnant. It is not known if XELSTRYM will harm the unborn baby.
- There is a pregnancy registry for women who are exposed to XELSTRYM during pregnancy. The purpose of the registry is to collect information about the health of women exposed to XELSTRYM and their babies. If you or your child becomes pregnant during treatment with XELSTRYM, talk to your healthcare provider about registering with the National Pregnancy Registry for Psychiatric Medications at 1-866-961-2388 or visit online at https://womensmentalhealth.org/clinical-and-research-programs/pregnancyregistry/othermedications/.
- are breastfeeding or plan to breastfeed. XELSTRYM passes into breast milk. You or your child should not breastfeed during treatment with XELSTRYM. Talk to your healthcare provider about the best way to feed the baby during treatment with XELSTRYM.
Tell your healthcare provider about all the medicines that you or your child take, including prescription and over-the-counter medicines, vitamins, and herbal supplements.
XELSTRYM may affect the way other medicines work and other medicines may affect how XELSTRYM works. Using XELSTRYM with other medicines may cause serious side effects. Sometimes the doses of other medicines will need to be changed while using XELSTRYM.
Especially tell your healthcare provider if you or your child take:
- selective serotonin reuptake inhibitors (SSRIs)
- medicines used to treat migraine headaches called triptans
- lithium
- tramadol
- buspirone
- serotonin norepinephrine reuptake inhibitors (SNRIs)
- tricyclic antidepressants
- fentanyl
- tryptophan
- St. John’s Wort
Your healthcare provider will decide whether XELSTRYM can be used with other medicines. Do not start any new medicine during treatment with XELSTRYM without first talking to your healthcare provider.
How should XELSTRYM be used?
- See the detailed “Instructions for Use” at the end of this XELSTRYM Medication Guide for information about the right way to apply, remove, and dispose of XELSTRYM.
- Your healthcare provider may change the dose if needed.
- Apply 1 XELSTRYM patch at a time for not more than 9 hours. Use only 1 XELSTRYM per 24 hours and change the site of application when applying a new patch.
- Apply the XELSTRYM patch 2 hours before the effect is needed and remove XELSTRYM within 9 hours after application.
If you or your child use too much XELSTRYM, call your healthcare provider or Poison Help line at 1-800-222-1222 or go to the nearest hospital emergency room right away.
What should I avoid while using XELSTRYM?
- Do not drive, operate heavy machinery, or do other potentially dangerous activities until you know how XELSTRYM affects you.
- After applying the XELSTRYM patch, avoid exposing the application site to direct external heat sources, such as hair dryers, heating pads or electric blankets, heat lamps, saunas, hot tubs, and heated water beds. Exposure to heat can cause too much medicine to pass into your body and cause serious side effects.
What are possible side effects of XELSTRYM?
XELSTRYM may cause serious side effects, including:
- See “What is the most important information I should know about XELSTRYM”
- Slowing of growth (weight and height) in children. Children should have their height and weight checked often during treatment with XELSTRYM. Your healthcare provider may stop the treatment with XELSTRYM if your child is not growing or gaining height or weight as expected.
-
Circulation problems in fingers and toes (peripheral vasculopathy, including Raynaud's phenomenon):
- fingers or toes may feel numb, cool, painful
- fingers or toes may change color from pale, to blue, to red
Tell your healthcare provider if you or your child have numbness, pain, skin color change, or sensitivity to temperature in your fingers or toes.
Call your healthcare provider right away if you or your child have any signs of unexplained wounds appearing on fingers or toes during treatment with XELSTRYM.
- Serotonin Syndrome. A potentially life-threatening problem called serotonin syndrome may happen when XELSTRYM is used with certain other medicines. See “Before using XELSTRYM, tell your healthcare provider about all medical conditions, including if you or your child:” Stop using XELSTRYM and call your healthcare provider or go to the nearest hospital emergency room right away if you or your child develop any of the following signs and symptoms of serotonin syndrome:
- agitation
- fast heartbeat
- flushing
- seizures
- coma
- sweating
- loss of coordination
- confusion
- dizziness
- tremors, stiff muscles, or muscle twitching
- seeing or hearing things that are not real (hallucination)
- changes in blood pressure
- high body temperature (hyperthermia)
- nausea, vomiting, diarrhea
- Allergic skin rash (contact sensitization). Stop using XELSTRYM and tell your healthcare provider right away if you or your child develop swelling or blisters at or around the application site. You may have a skin allergy to XELSTRYM. People who have skin allergies to XELSTRYM may develop an allergy to all amphetamine containing products, even amphetamine products that are taken by mouth.
- Application site reactions have happened with XELSTRYM while wearing the XELSTRYM patch, and after removal of the patch. Signs and symptoms of an application site reaction include, pain, Itching, burning feeling, redness, discomfort, or swelling at the application site. Call your healthcare provider if you or your child develop any application site reactions that do not resolve on their own.
- New or worsening tics or worsening Tourette’s syndrome. Tell your healthcare provider if you or your child get any new or worsening tics or worsening Tourette’s syndrome during treatment with XELSTRYM.
The most common side effects of XELSTRYM include:
- decreased appetite
- trouble sleeping
- stomach pain
- nausea
- increased blood pressure
- headache
- muscle twitching (tics)
- vomiting
- irritability
- increased heart rate
These are not all the possible side effects of XELSTRYM.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
How should I store XELSTRYM?
- Store XELSTRYM at room temperature between 68°F to 77℉F (20℃ to 25℃).
- Store XELSTRYM in a safe place, like a locked cabinet.
- Protect XELSTRYM from light and moisture.
- Keep XELSTRYM in their unopened pouches until you are ready to use them.
- Dispose of remaining unused or expired XELSTRYM by a medication take-back program at a U.S. Drug Enforcement Administration (DEA) authorized collection site. If no take-back program or DEA authorized collector is available, each unused patch should be removed from its individual pouch, separated from the protective liner, folded in half so the sticky sides stick together, and thrown away in a container with a lid in the household trash. Do not flush the XELSTRYM patch, pouch, or liner down the toilet. Visit www.fda.gov/drugdisposal for additional information on disposal of unused medicines.
Keep XELSTRYM and all medicines out of the reach of children.
General information about the safe and effective use of XELSTRYM.
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use XELSTRYM for a condition for which it was not prescribed. Do not give XELSTRYM to other people, even if they have the same symptoms that you have. It may harm them and it is against the law. You can ask your healthcare provider or pharmacist for information about XELSTRYM that is written for healthcare professionals.
What are the ingredients in XELSTRYM?
Active ingredient: dextroamphetamine
Inactive ingredients: acrylic adhesives, green ink, polyester/polyurethane backing, and polyester release liner
Manufactured by: Noven Pharmaceuticals, Inc., Miami, FL 33186
Xelstrym® is a registered trademark of Noven Therapeutics, LLC.
For more information, go to www.xelstrym.com or call 1-800-455-8070.
102668-3
-
Abuse, misuse, and addiction. XELSTRYM has a high chance for abuse and misuse and may lead to substance use problems, including addiction. Misuse and abuse of XELSTRYM, other amphetamine containing medicines, and methylphenidate containing medicines, can lead to overdose and death. The risk of overdose and death is increased with higher doses of XELSTRYM or when it is used in ways that are not approved, such as snorting or injection.
-
INSTRUCTIONS FOR USE
INSTRUCTIONS FOR USE
XELSTRYM® (Zel’ Strim)
(dextroamphetamine)
transdermal system, CIIThis Instructions for Use contains information on how to apply, remove, and dispose of XELSTRYM transdermal system (patch).
XELSTRYM transdermal system (patch) is for use on skin only.
Read this Instructions for Use before you start using XELSTRYM and each time you get a refill. There may be new information. This information does not take the place of talking to your healthcare provider about your or your child’s medical condition or treatment.
XELSTRYM is supplied in cartons containing 30 patches. Each patch is sealed in a pouch protecting it until you are ready to apply it.
Important information you need to know before applying XELSTRYM:
- Wear only 1 patch at a time.
- A new patch must be applied every day.
- Do not wear XELSTRYM for more than 9 hours. Use only 1 patch per day (per 24 hours).
- When you apply a new patch, choose a different application site from the one used the previous day to reduce the chance of skin reactions such as irritation, discomfort or pain at the application site.
- Avoid touching the sticky side of XELSTRYM with your fingers. If you accidentally touch the sticky side of the patch, wash your hands right away with soap and water to remove any potential medicine that may have stuck to your fingers. Do not use hand sanitizer in place of soap and water.
- Avoid exposing the application site to direct external heat sources, such as heating pads or electric blankets, heat lamps, saunas, hot tubs, heated water beds, and hair dryers.
- Check to see if the patch has become loose after bathing, showering or swimming.
- If the patch falls off:
- Do not reapply the same patch. Fold the patch in half so that the sticky sides are together and throw away the patch as instructed below in Steps 5 to 7.
- You should choose a different application site and apply a new patch.
- The total wear time for the first patch that fell off and the second replacement patch should not total more than 9 hours in 1 day (24 hours).
- Parents or caregivers of children prescribed XELSTRYM should instruct the child to tell an adult if the patch becomes loose or falls off.
Figure A (not to scale).
Applying XELSTRYM:
Step 1: Select the patch application site (see Figure B). - Choose 1 application site, on either the left or right side, to apply 1 patch. The recommended application sites include:
- chest
- upper arm
- upper back
- flank (sides of the waist)
- hip
- Do not apply a patch to any other site.
- Avoid areas of tight clothing, such as waistbands or straps.
- Choose a different application site from the one used the previous day when you apply a new patch.
- Check the expiration date before applying the patch.
Figure B
Step 2: Check the skin where XELSTRYM will be applied. Make sure it is: - Not damaged (cut, scraped, burned), irritated (rashes), or has any other skin problems
- Cleaned with soap and water (not an alcohol-based product), dry (not wet), with no powder, oil, lotion, or gel
- Hairless or nearly hairless. Applying the patch to a hairy application site could result in the patch falling off
If there is hair at the patch application site, do not shave the application site. Use scissors to clip hair as close to the skin as possible.
Step 3: Applying XELSTRYM - Do not open the pouch until you are ready to apply the patch.
- Using scissors, carefully cut along the right side of the pouch. Start at the dashed line marked on the pouch as “Step 1. Cut This Side” and cut along the entire length of the pouch, through the bar code (see Figure C).
- Next, carefully cut the top of the pouch along the dashed line marked on the pouch as “Step 2. Cut Across Top” (see Figure D).
- Gently remove the contents of the pouch and throw away the slip liners (additional pieces of clear plastic) above and below the patch (see Figure A, Figure E).
- Do not use the patch if it is cut or damaged
- Apply the patch right away after removing it from the pouch
Figure C
Figure D
Figure E
Figure F
Figure G
- Hold the edge of the remaining protective liner, slowly peel it off and smooth the patch down (see Figure H).
- Press the patch firmly with the palm of your hand (See Figure I).
- Smooth the patch to make sure it sticks well to your skin.
XELSTRYM patch should not be applied or reapplied with dressings, tape, or other adhesives.
Figure H
Figure I
-
Wash your hands with soap and water after applying the patch (see Figure J).
Do not use hand sanitizer in place of soap and water.
Figure J
Step 4: Check XELSTRYM regularly during the day to make sure it is completely sticking to the application site. Also check the patch when:
- using the bathroom
- after sleeping
- after bathing, showering or swimming
- undressing or changing clothes
- if sweating a lot
- If patch edges lift, smooth the patch down on the skin and press firmly with the palm of your hand. XELSTRYM patch should not be reapplied with dressings, tape, or other adhesives.
- If the patch falls off, do not reapply the same patch. Fold the patch in half so that the sticky sides are together and throw away the patch as instructed below in Steps 5 to 7. You may apply a new patch to a different application site. The total wear time for the first patch that fell off and the second replacement patch should not be more than a total of 9 hours in 1 day (24 hours).
- Parents or caregivers of children prescribed XELSTRYM should instruct the child to tell an adult if the patch becomes loose or falls off.
XELSTRYM Application Schedule for 9 Hour Wear Time:
If you put the patch on at: On the same day, remove the patch no later than: 6:00 a.m. 3:00 p.m 7:00 a.m. 4:00 p.m 8:00 a.m. 5:00 p.m 9:00 a.m. 6:00 p.m 10:00 a.m. 7:00 p.m 11:00 a.m. 8:00 p.m 12:00 p.m. 9:00 p.m Removing and Disposing Used XELSTRYM:
This Instructions for Use has been approved by the U.S. Food and Drug Administration.
© 2023 Noven Pharmaceuticals, Inc.
102668-3Revised: 10/2023 Step 5: After 9 hours, remove XELSTRYM and fold it in half so that the sticky sides stick together (see Figure K) to avoid accidental exposure to medicine. - If any adhesive (glue) remains on your skin after you remove the patch, apply an oil-based product or water and soap to the skin to remove the glue.
Figure K
Step 6: Throw away the used patch in a container with a lid right away (see Figure L). Figure L
Step 7: Wash your hands with soap and water after throwing the patch away (see Figure M).
Do not use hand sanitizer in place of soap and water.Figure M
Storing XELSTRYM
- Store XELSTRYM at room temperature between 68°F to 77°F (20°C to 25°C).
- Store XELSTRYM in a safe place, like a locked cabinet.
- Protect XELSTRYM from light and moisture.
- Keep XELSTRYM in their unopened pouches until you are ready to use them.
- Keep XELSTRYM and all medicines out of the reach of children.
Disposing of Unused XELSTRYM:
Dispose of remaining unused or expired XELSTRYM by a medication take-back program at a U.S. Drug Enforcement Administration (DEA) authorized collection site. If no take-back program or DEA authorized collector is available, each unused patch should be removed from its individual pouch, separated from the protective liner, folded in half so the sticky sides stick together, and thrown away in a container with a lid in the household trash. Do not flush the XELSTRYM patch, pouch, or liner down the toilet. Visit www.fda.gov/drugdisposal for additional information on disposal of unused medicines.
- PRINCIPAL DISPLAY PANEL - NDC: 68968-0205-3 - Carton Label - 4.5 mg/9 hours
- PRINCIPAL DISPLAY PANEL - NDC: 68968-0210-3 - Carton Label - 9 mg/9 hours
- PRINCIPAL DISPLAY PANEL - NDC: 68968-0215-3 - Carton Label - 13.5 mg/9 hours
- PRINCIPAL DISPLAY PANEL - NDC: 68968-0220-3 - Carton Label - 18 mg/9 hours
-
INGREDIENTS AND APPEARANCE
XELSTRYM
dextroamphetamine patch, extended releaseProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 68968-0205 Route of Administration TRANSDERMAL DEA Schedule CII Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength DEXTROAMPHETAMINE (UNII: TZ47U051FI) (DEXTROAMPHETAMINE - UNII:TZ47U051FI) DEXTROAMPHETAMINE 4.5 mg Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 68968-0205-3 30 in 1 CARTON 05/15/2023 1 NDC: 68968-0205-1 1 in 1 POUCH; Type 2: Prefilled Drug Delivery Device/System (syringe, patch, etc.) Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA215401 05/15/2023 XELSTRYM
dextroamphetamine patch, extended releaseProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 68968-0210 Route of Administration TRANSDERMAL DEA Schedule CII Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength DEXTROAMPHETAMINE (UNII: TZ47U051FI) (DEXTROAMPHETAMINE - UNII:TZ47U051FI) DEXTROAMPHETAMINE 9 mg Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 68968-0210-3 30 in 1 CARTON 05/15/2023 1 NDC: 68968-0210-1 1 in 1 POUCH; Type 2: Prefilled Drug Delivery Device/System (syringe, patch, etc.) Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA215401 05/15/2023 XELSTRYM
dextroamphetamine patch, extended releaseProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 68968-0215 Route of Administration TRANSDERMAL DEA Schedule CII Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength DEXTROAMPHETAMINE (UNII: TZ47U051FI) (DEXTROAMPHETAMINE - UNII:TZ47U051FI) DEXTROAMPHETAMINE 13.5 mg Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 68968-0215-3 30 in 1 CARTON 05/15/2023 1 NDC: 68968-0215-1 1 in 1 POUCH; Type 2: Prefilled Drug Delivery Device/System (syringe, patch, etc.) Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA215401 05/15/2023 XELSTRYM
dextroamphetamine patch, extended releaseProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 68968-0220 Route of Administration TRANSDERMAL DEA Schedule CII Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength DEXTROAMPHETAMINE (UNII: TZ47U051FI) (DEXTROAMPHETAMINE - UNII:TZ47U051FI) DEXTROAMPHETAMINE 18 mg Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 68968-0220-3 30 in 1 CARTON 05/15/2023 1 NDC: 68968-0220-1 1 in 1 POUCH; Type 2: Prefilled Drug Delivery Device/System (syringe, patch, etc.) Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA215401 05/15/2023 Labeler - Noven Therapeutics, LLC (166888268) Registrant - Noven Pharmaceuticals, Inc. (148585441) Establishment Name Address ID/FEI Business Operations Noven Pharmaceuticals, Inc. 148585441 MANUFACTURE(68968-0205, 68968-0210, 68968-0215, 68968-0220)
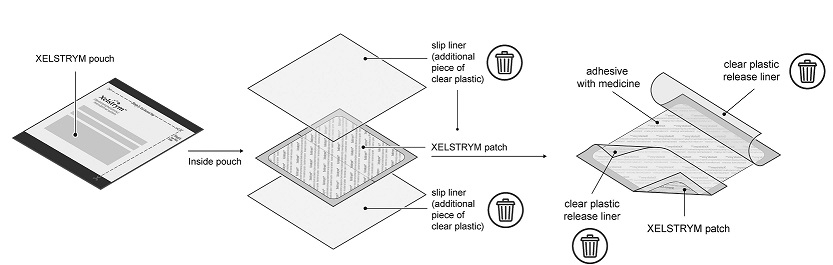
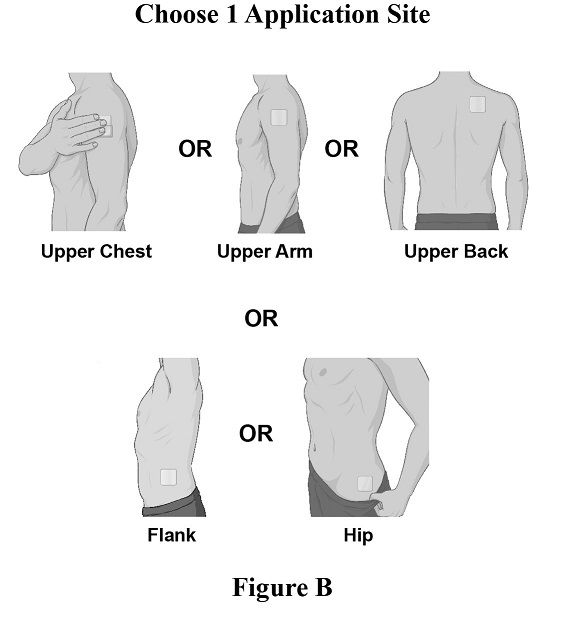

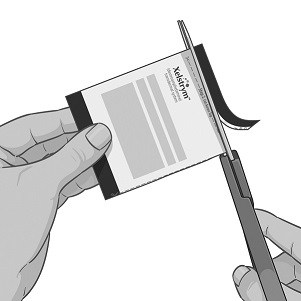
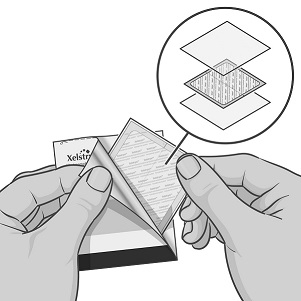
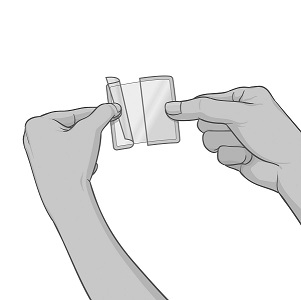
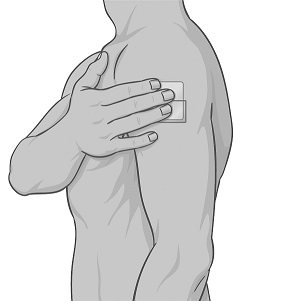
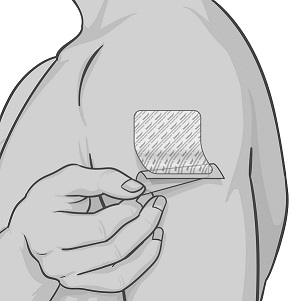


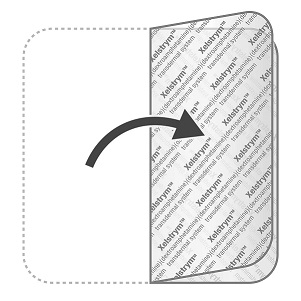


Trademark Results [XELSTRYM]
Mark Image Registration | Serial | Company Trademark Application Date |
|---|---|
 XELSTRYM 97525996 not registered Live/Pending |
Noven Therapeutics, LLC 2022-07-29 |
 XELSTRYM 88411346 not registered Live/Pending |
Noven Therapeutics, LLC 2019-05-01 |
 XELSTRYM 86785866 not registered Dead/Abandoned |
Noven Therapeutics, LLC 2015-10-13 |
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.