SOLIFENACIN SUCCINATE 5 MG- solifenacin succinate tablet, film coated SOLIFENACIN SUCCINATE 10 MG- solifenacin succinate tablet, film coated
solifenacin succinate by
Drug Labeling and Warnings
solifenacin succinate by is a Prescription medication manufactured, distributed, or labeled by Strides Pharma Inc., Strides Pharma Global Pte.Ltd., Vivimed Life Sciences Private Limited. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use SOLIFENACIN SUCCINATE TABLETS safely and effectively. See full prescribing information for SOLIFENACIN SUCCINATE TABLETS.
SOLIFENACIN SUCCINATE tablets, for oral use
Initial U.S. Approval: 2004INDICATIONS AND USAGE
Solifenacin succinate tablets, 5 mg and 10 mg are a muscarinic antagonist indicated for the treatment of overactive bladder with symptoms of urge urinary incontinence, urgency, and urinary frequency (1) (1)
DOSAGE AND ADMINISTRATION
5 mg tablet taken once daily, and if well tolerated may be increased to 10 mg once daily (2.1)
Do not exceed 5 mg tablet once daily in patients with:
o severe renal impairment [Creatinine Clearance] (CLcr <30 mL/min) (2.2)
o moderate hepatic impairment (Child-Pugh B) (2.3)
o concomitant use of potent CYP3A4 inhibitors (2.4)
Use of Solifenacin succinate tablets, 5 mg and 10 mg are not recommended in patients with severe hepatic impairment (Child-Pugh C) (2.3) (2)DOSAGE FORMS AND STRENGTHS
Tablets: 5 mg and 10 mg (3) (3)
CONTRAINDICATIONS
Urinary retention (4, 5.2)
Gastric retention (4, 5.3)
Uncontrolled narrow-angle glaucoma (4, 5.5)
In Patients who have demonstrated hypersensitivity to the drug (4, 6.2) (4)WARNINGS AND PRECAUTIONS
Angioedema and anaphylactic reactions: Reports of angioedema of the face, lips and/or larynx, in some cases occurring after the first dose, have been described. Anaphylactic reactions have been reported rarely (5.1)
Urinary Retention: Administer with caution to patients with clinically significant bladder outflow obstruction (5.2)
Gastrointestinal Disorders: Use with caution in patients with decreased gastrointestinal motility (5.3)
Central Nervous System Effects: Somnolence has been reported with Solifenacin succinate tablets, 5 mg and 10 mg. Advise patients not to drive or operate heavy machinery until they know how Solifenacin succinate tablets, 5 mg and 10 mg affects them (5.4)
Controlled Narrow-Angle Glaucoma: Use with caution in patients being treated for narrow-angle glaucoma (5.5)
QT Prolongation: Use with caution in patients with a known history of QT prolongation or patients who are taking medications known to prolong the QT interval (5.8) (5)ADVERSE REACTIONS
The most common adverse reactions (> 4% and > placebo) were dry mouth, and constipation at both 5 mg and 10 mg doses; and urinary tract infection, and blurred visions at the 10 mg dose (6.1) (6)
To report SUSPECTED ADVERSE REACTIONS, contact Strides Pharma Inc at 1-877-244-9825 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch. (6)
DRUG INTERACTIONS
Inhibitors of CYP3A4 may increase the concentration of Solifenacin succinate tablets, 5 mg and 10 mg. (7.1)
Inducers of CYP3A4 may decrease the concentration of Solifenacin succinate tablets, 5 mg and 10 mg. (7.2) (7)USE IN SPECIFIC POPULATIONS
Pregnancy and Nursing Mothers: Solifenacin succinate tablets, 5 mg and 10 mg should be used during pregnancy only if the potential benefit for the mother justifies the potential risk to the fetus. Solifenacin succinate tablets, 5 mg and 10 mg should not be administered during nursing (8.1, 8.3)
Pediatric Use: The safety and effectiveness of Solifenacin succinate tablets, 5 mg and 10 mg in pediatric patients have not been established (8.4) (8)See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.
Revised: 10/2019
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Dosing Information
2.2 Dose Adjustment in Patients with Renal Impairment
2.3 Dose Adjustment in Patients with Hepatic Impairment
2.4 Dose Adjustment in Patients Taking CYP3A4 Inhibitors
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Angioedema and Anaphylactic Reactions
5.2 Urinary Retention
5.3 Gastrointestinal Disorders
5.4 Central Nervous System Effects
5.5 Controlled Narrow-Angle Glaucoma
5.6 Hepatic Impairment
5.7 Renal Impairment
5.8 Patients with Congenital or Acquired QT Prolongation
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
6.2 Post-Marketing Experience
7 DRUG INTERACTIONS
7.1 Potent CYP3A4 Inhibitors
7.2 CYP3A4 Inducers
7.3 Drugs Metabolized by Cytochrome P450
7.4 Warfarin
7.5 Oral Contraceptives
7.6 Digoxin
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Labor and Delivery
8.3 Nursing Mothers
8.4 Pediatric Use
8.5 Geriatric Use
8.6 Renal Impairment
8.7 Hepatic Impairment
8.8 Gender
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- * Sections or subsections omitted from the full prescribing information are not listed.
- 1 INDICATIONS AND USAGE
-
2 DOSAGE AND ADMINISTRATION
2.1 Dosing Information
The recommended dose of Solifenacin succinate tablet is 5 mg once daily. If the 5 mg dose is well tolerated, the dose may be increased to 10 mg once daily.
Solifenacin succinate tablet should be taken with water and swallowed whole. Solifenacin succinate tablet can be administered with or without food.
2.2 Dose Adjustment in Patients with Renal Impairment
For patients with severe renal impairment (CLcr <30 mL/min), a daily dose of Solifenacin succinate tablet greater than 5 mg is not recommended [see Warnings and Precautions (5.7); Use in Specific Populations (8.6)].
2.3 Dose Adjustment in Patients with Hepatic Impairment
For patients with moderate hepatic impairment (Child-Pugh B), a daily dose of Solifenacin succinate tablet greater than 5 mg is not recommended. Use of Solifenacin succinate tablets in patients with severe hepatic impairment (Child-Pugh C) is not recommended [see Warnings and Precautions (5.6); Use in Specific Populations (8.7)].
- 3 DOSAGE FORMS AND STRENGTHS
-
4 CONTRAINDICATIONS
Solifenacin succinate tablets are contraindicated in patients with:
urinary retention [see Warnings and Precautions (5.2)],
gastric retention [see Warnings and Precautions (5.3)].
uncontrolled narrow-angle glaucoma [see Warnings and Precautions (5.5), and
in patients who have demonstrated hypersensitivity to the drug [see Adverse Reactions (6.2)]. -
5 WARNINGS AND PRECAUTIONS
5.1 Angioedema and Anaphylactic Reactions
Angioedema of the face, lips, tongue, and/or larynx have been reported with solifenacin. In some cases angioedema occurred after the first dose. Cases of angioedema have been reported to occur hours after the first dose or after multiple doses. Angioedema associated with upper airway swelling may be life threatening. If involvement of the tongue, hypopharynx, or larynx occurs, solifenacin should be promptly discontinued and appropriate therapy and/or measures necessary to ensure a patent airway should be promptly provided. Anaphylactic reactions have been reported rarely in patients treated with solifenacin succinate. Solifenacin succinate should not be used in patients with a known or suspected hypersensitivity to solifenacin succinate. In patients who develop anaphylactic reactions, solifenacin succinate should be discontinued and appropriate therapy and/or measures should be taken.
5.2 Urinary Retention
Solifenacin succinate tablets, like other anticholinergic drugs, should be administered with caution to patients with clinically significant bladder outflow obstruction because of the risk of urinary retention [see Contraindications (4)].
5.3 Gastrointestinal Disorders
Solifenacin succinate tablets, like other anticholinergics, should be used with caution in patients with decreased gastrointestinal motility [see Contraindications (4)].
5.4 Central Nervous System Effects
Solifenacin succinate tablets are associated with anticholinergic central nervous system (CNS) effects [see Adverse Reactions (6.2)]. A variety of CNS anticholinergic effects have been reported, including headache, confusion, hallucinations and somnolence. Patients should be monitored for signs of anticholinergic CNS effects, particularly after beginning treatment or increasing the dose. Advise patients not to drive or operate heavy machinery until they know how Solifenacin succinate tablets affects them. If a patient experiences anticholinergic CNS effects, dose reduction or drug discontinuation should be considered.
5.5 Controlled Narrow-Angle Glaucoma
Solifenacin succinate tablets should be used with caution in patients being treated for narrow-angle glaucoma [see Contraindications (4)].
5.6 Hepatic Impairment
Solifenacin succinate tablets should be used with caution in patients with hepatic impairment. Doses of Solifenacin succinate tablets greater than 5 mg are not recommended in patients with moderate hepatic impairment (Child-Pugh B). Solifenacin succinate tablets are not recommended for patients with severe hepatic impairment (Child-Pugh C) [see Dosage and Administration (2.3) and Use in Specific Populations (8.7)].
5.7 Renal Impairment
Solifenacin succinate should be used with caution in patients with renal impairment. Doses of Solifenacin succinate tablets greater than 5 mg are not recommended in patients with severe renal impairment (CLcr <30 mL/min) [see Dosage and Administration (2.2) and Use in Specific Populations (8.6)].
5.8 Patients with Congenital or Acquired QT Prolongation
In a study of the effect of Solifenacin on the QT interval in 76 healthy women [see Clinical Pharmacology (12.2)] the QT prolonging effect appeared less with solifenacin 10 mg than with 30 mg (three times the maximum recommended dose), and the effect of solifenacin 30 mg did not appear as large as that of the positive control moxifloxacin at its therapeutic dose. This observation should be considered in clinical decisions to prescribe Solifenacin succinate for patients with a known history of QT prolongation or patients who are taking medications known to prolong the QT interval.
-
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Solifenacin succinate has been evaluated for safety in 1811 patients in randomized, placebo-controlled trials. Expected adverse reactions of antimuscarinic agents are dry mouth, constipation, blurred vision (accommodation abnormalities), urinary retention, and dry eyes. The incidence of dry mouth and constipation in patients treated with Solifenacin succinate was higher in the 10mg compared to the 5 mg dose group.
In the four 12-week double-blind clinical trials, severe fecal impaction, colonic obstruction, and intestinal obstruction were reported in one patient each, all in the Solifenacin succinate 10 mg group. Angioneurotic edema has been reported in one patient taking Solifenacin succinate 5 mg. Compared to 12 weeks of treatment with Solifenacin succinate, the incidence and severity of adverse reactions were similar in patients who remained on drug for up to 12 months.
The most frequent adverse reaction leading to study discontinuation was dry mouth (1.5%). Table 1 lists the rates of identified adverse reactions, derived from all reported adverse events, in randomized, placebo-controlled trials at an incidence greater than placebo and in 1% or more of patients treated with Solifenacin succinate tablets 5 or 10 mg once daily for up to 12 weeks.
Table 1. Percentages of Patients with Identified Adverse Reactions, Derived from All Adverse Events Exceeding Placebo Rate and Reported by 1% or More Patients for Combined Pivotal Studies Placebo (%) Solifenacin succinate tablets 5 mg (%) Solifenacin succinate tablets 10 mg (%) Number of Patients 1216 578 1233 GASTROINTESTINAL DISORDERS Dry Mouth 4.2 10.9 27.6 Constipation 2.9 5.4 13.4 Nausea 2.0 1.7 3.3 Dyspepsia 1.0 1.4 3.9 Abdominal pain Upper 1.0 1.9 1.2 Vomiting NOS 0.9 0.2 1.1 INFECTIONS AND INFESTATIONS Urinary Tract Infection NOS 2.8 2.8 4.8 Influenza 1.3 2.2 0.9 Pharyngitis NOS 1.0 0.3 1.1 NERVOUS SYSTEM DISORDERS Dizziness 1.8 1.9 1.8 EYE DISORDERS Vision Blurred 1.8 3.8 4.8 Dry Eyes NOS 0.6 0.3 1.6 RENAL AND URINARY DISORDERS Urinary Retention 0.6 0 1.4 GENERAL DISORDERS AND ADMINISTRATION SITE CONDITIONS Edema Lower Limb 0.7 0.3 1.1 Fatigue 1.1 1.0 2.1 PSYCHIATRIC DISORDERS Depression NOS 0.8 1.2 0.8 RESPIRATORY, THORACIC AND MEDIASTINAL DISORDERS Cough 0.2 0.2 1.1 VASCULAR DISORDERS Hypertension NOS 0.6 1.4 0.5 6.2 Post-Marketing Experience
Because these spontaneously reported events are from the worldwide postmarketing experience, the frequency of events and the role of solifenacin in their causation cannot be reliably determined.
The following events have been reported in association with solifenacin use in worldwide postmarketing experience:
General: peripheral edema, hypersensitivity reactions, including angioedema with airway obstruction, rash, pruritus, urticaria, and anaphylactic reaction;
Central Nervous: headache, confusion, hallucinations, delirium and somnolence;
Cardiovascular: QT prolongation; Torsade de Pointes, atrial fibrillation, tachycardia, palpitations;
Hepatic: liver disorders mostly characterized by abnormal liver function tests, AST (aspartate aminotransferase), ALT (alanine aminotransferase), and GGT (gamma-glutamyl transferase);Renal: renal impairment;
Metabolism and nutrition disorders: decreased appetite and hyperkalemia;
Dermatologic: exfoliative dermatitis, erythema multiforme and dry skin;
Eye disorders: glaucoma;
Gastrointestinal disorders: gastroesophageal reflux disease, ileus, abdominal pain and dysgeusia;
Respiratory, thoracic and mediastinal disorders: dysphonia and nasal dryness;
Musculoskeletal and connective tissue disorders: muscular weakness; -
7 DRUG INTERACTIONS
7.1 Potent CYP3A4 Inhibitors
Following the administration of 10 mg of Solifenacin succinate tablets in the presence of 400 mg of ketoconazole, a potent inhibitor of CYP3A4, the mean Cmax and AUC of solifenacin increased by 1.5 and 2.7-fold, respectively. Therefore, it is recommended not to exceed a 5 mg daily dose of Solifenacin succinate when administered with therapeutic doses of ketoconazole or other potent CYP3A4 inhibitors [see Dosage and Administration (2.4) and Clinical Pharmacology (12.3)]. The effects of weak or moderate CYP3A4 inhibitors were not examined.
7.2 CYP3A4 Inducers
There were no in vivo studies conducted to evaluate the effect of CYP3A4 inducers on Solifenacin succinate. In vitro drug metabolism studies have shown that solifenacin is a substrate of CYP3A4. Therefore, inducers of CYP3A4 may decrease the concentration of solifenacin.
7.3 Drugs Metabolized by Cytochrome P450
At therapeutic concentrations, solifenacin does not inhibit CYP1A1/2, 2C9, 2C19, 2D6, or 3A4 derived from human liver microsomes.
7.4 Warfarin
Solifenacin has no significant effect on the pharmacokinetics of R-warfarin or S-warfarin [see Clinical Pharmacology (12.3)].
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
There are no adequate and well-controlled studies in pregnant women.
Reproduction studies have been performed in mice, rats and rabbits. After oral administration of 14C-solifenacin succinate to pregnant mice, drug-related material was shown to cross the placental barrier. No embryotoxicity or teratogenicity was observed in mice treated with 1.2 times (30 mg/kg/day) the expected exposure at the maximum recommended human dose [MRHD] of 10 mg. Administration of solifenacin succinate to pregnant mice at 3.6 times and greater (100 mg/kg/day and greater) the exposure at the MRHD, during the major period of organ development resulted in reduced fetal body weights. Administration of 7.9 times (250 mg/kg/day) the MRHD to pregnant mice resulted in an increased incidence of cleft palate. In utero and lactational exposures to maternal doses of solifenacin succinate of 3.6 times (100 mg/kg/day) the MRHD resulted in reduced peripartum and postnatal survival, reductions in body weight gain, and delayed physical development (eye opening and vaginal patency). An increase in the percentage of male offspring was also observed in litters from offspring exposed to maternal doses of 250 mg/kg/day. No embryotoxic effects were observed in rats at up to 50mg/kg/day (<1 times the exposure at the MRHD) or in rabbits at up to 1.8 times (50 mg/kg/day) the exposure at the MRHD. Because animal reproduction studies are not always predictive of human response, Solifenacin succinate should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
8.2 Labor and Delivery
The effect of Solifenacin succinate on labor and delivery in humans has not been studied.
There were no effects on natural delivery in mice treated with 1.2 times (30 mg/kg/day) the expected exposure at the maximum recommended human dose [MRHD] of 10 mg. Administration of solifenacin succinate at 3.6 times (100 mg/kg/day) the exposure at the MRHD or greater increased peripartum pup mortality.8.3 Nursing Mothers
After oral administration of 14C-solifenacin succinate to lactating mice, radioactivity was detected in maternal milk. There were no adverse observations in mice treated with 1.2 times (30 mg/kg/day) the expected exposure at the maximum recommended human dose [MRHD]. Pups of female mice treated with 3.6 times (100 mg/kg/day) the exposure at the MRHD or greater revealed reduced body weights, postpartum pup mortality or delays in the onset of reflex and physical development during the lactation period.
It is not known whether solifenacin is excreted in human milk. Because many drugs are excreted in human milk, Solifenacin succinate tablet should not be administered during nursing. A decision should be made whether to discontinue nursing or to discontinue Solifenacin succinate tablet in nursing mothers.
8.4 Pediatric Use
The safety and effectiveness of Solifenacin succinate in pediatric patients have not been established.
8.5 Geriatric Use
In placebo-controlled clinical studies, similar safety and effectiveness were observed between older (623 patients ≥ 65 years and 189 patients ≥ 75 years) and younger patients (1188 patients < 65 years) treated with Solifenacin succinate.
Multiple dose studies of Solifenacin succinate in elderly volunteers (65 to 80 years) showed that Cmax, AUC and t1/2 values were 20-25% higher as compared to the younger volunteers (18 to 55 years).
8.6 Renal Impairment
Solifenacin succinate should be used with caution in patients with renal impairment. There is a 2.1-fold increase in AUC and 1.6-fold increase in t1/2 of Solifenacin in patients with severe renal impairment. Doses of Solifenacin Succinate greater than 5 mg are not recommended in patients with severe renal impairment (CLcr < 30mL/min) [see Warnings and Precautions (5.7); Dosage and Administration (2.2)].
8.7 Hepatic Impairment
Solifenacin succinate should be used with caution in patients with reduced hepatic function. There is a 2-fold increase in the t1/2 and 35% increase in AUC of solifenacin in patients with moderate hepatic impairment. Doses of Solifenacin succinate greater than 5 mg are not recommended in patients with moderate hepatic impairment (Child-Pugh B). Solifenacin succinate are not recommended for patients with severe hepatic impairment (Child-Pugh C) [see Warnings and Precautions (5.6); Dosage and Administration (2.3)].
-
10 OVERDOSAGE
Overdosage with Solifenacin succinate tablets can potentially result in severe anticholinergic effects and should be treated accordingly. The highest dose ingested in an accidental overdose of solifenacin succinate was 280 mg in a 5-hour period. This case was associated with mental status changes. Some cases reported a decrease in the level of consciousness.
Intolerable anticholinergic side effects (fixed and dilated pupils, blurred vision, failure of heel-to-toe exam, tremors and dry skin) occurred on day 3 in normal volunteers taking 50 mg daily (5 times the maximum recommended therapeutic dose) and resolved within 7 days following discontinuation of drug.
In the event of overdose with Solifenacin succinate tablets, treat with gastric lavage and appropriate supportive measures. ECG monitoring is also recommended. -
11 DESCRIPTION
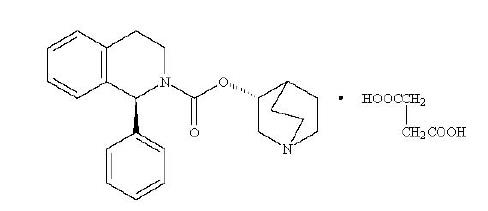
Solifenacin succinate tablets (Solifenacin succinate) are muscarinic receptor antagonist. Chemically, solifenacin succinate is butanedioic acid, compounded with (1S)-(3R)-1-azabicyclo [2.2.2]oct-3-yl 3,4-dihydro-1-phenyl-2(1H)-iso-quinolinecarboxylate (1:1) having an empirical formula of C23H26N2O2C4H6O4, and a molecular weight of 480.55. The structural formula of solifenacin succinate is:
Solifenacin succinate is white to pale yellowish-white crystal or crystalline powder. It is freely soluble in water, methanol and chloroform. Each Solifenacin succinate tablet contains 5 or 10 mg of solifenacin succinate and is formulated for oral administration. In addition to the active ingredient solifenacin succinate, each Solifenacin succinate tablet also contains the following inert ingredients: Colloidal Silicon dioxide (Aerosil 200) NF, Corn Starch NF (Maize Starch B-Pharma Grade),HPMC 2910/Hypromellose USP, Hydroxy Propyl Methyl Cellulose USP (Methocel E5 Premium LV), Iron Oxide Red NF (for 10 mg Solifenacin succinate tablet), Iron Oxide Yellow NF (for 5 mg Solifenacin succinate tablet), Lactose Monohydrate NF – Pharmatose 200 M (Milled), Lactose Monohydrate NF (Super Tab 11SD), Macrogol/PEG NF, Magnesium Stearate NF (Ligamed MF-2-V), Talc USP and Titanium Dioxide USP.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Solifenacin is a competitive muscarinic receptor antagonist. Muscarinic receptors play an important role in several major cholinergically mediated functions, including contractions of urinary bladder smooth muscle and stimulation of salivary secretion.
12.2 Pharmacodynamics
Cardiac Electrophysiology
The effect of 10 mg and 30 mg solifenacin succinate on the QT interval was evaluated at the time of peak plasma concentration of solifenacin in a multi-dose, randomized, double-blind, placebo and positive-controlled (moxifloxacin 400 mg) trial. Subjects were randomized to one of two treatment groups after receiving placebo and moxifloxacin sequentially. One group (n=51) went on to complete 3 additional sequential periods of dosing with solifenacin 10, 20, and 30 mg while the second group (n=25) in parallel completed a sequence of placebo and moxifloxacin. Study subjects were female volunteers aged 19 to 79 years. The 30 mg dose of solifenacin succinate (three times the highest recommended dose) was chosen for use in this study because this dose results in a solifenacin exposure that covers those observed upon co-administration of 10 mg Solifenacin succinate with potent CYP3A4 inhibitors (e.g. ketoconazole, 400 mg). Due to the sequential dose escalating nature of the study, baseline EKG measurements were separated from the final QT assessment (of the 30 mg dose level) by 33 days.
The median difference from baseline in heart rate associated with the 10 and 30 mg doses of solifenacin succinate compared to placebo was -2 and 0 beats/minute, respectively. Because a significant period effect on QTc was observed, the QTc effects were analyzed utilizing the parallel placebo control arm rather than the pre-specified intra-patient analysis. Representative results are shown in Table 2.
Table 2. QTc changes in msec (90%CI) from baseline at Tmax (relative to placebo)* Drug/Dose Fridericia method (using mean difference) Solifenacin 10 mg 2 (-3,6) Solifenacin 30 mg 8 (4,13) * Results displayed are those derived from the parallel design portion of the study and represent the comparison of Group 1 to time-matched placebo effects in Group 2
Moxifloxacin was included as a positive control in this study and, given the length of the study, its effect on the QT interval was evaluated in 3 different sessions. The placebo subtracted mean changes (90% CI) in QTcF for moxifloxacin in the three sessions were 11 (7, 14), 12 (8, 17), and 16 (12, 21), respectively.
The QT interval prolonging effect appeared greater for the 30 mg compared to the 10 mg dose of solifenacin. Although the effect of the highest solifenacin dose (three times the maximum therapeutic dose) studied did not appear as large as that of the positive control moxifloxacin at its therapeutic dose, the confidence intervals overlapped. This study was not designed to draw direct statistical conclusions between the drugs or the dose levels.
12.3 Pharmacokinetics
Absorption
After oral administration of Solifenacin succinate to healthy volunteers, peak plasma levels (Cmax) of solifenacin are reached within 3 to 8 hours after administration, and at steady state ranged from 32.3 to 62.9 ng/mL for the 5 and 10 mg Solifenacin succinate tablets, respectively. The absolute bioavailability of solifenacin is approximately 90%, and plasma concentrations of solifenacin are proportional to the dose administered.
Effect of food
Solifenacin succinate may be administered without regard to meals. A single 10 mg dose administration of Solifenacin succinate with food increased Cmax and AUC by 4% and 3%, respectively.Distribution
Solifenacin is approximately 98% (in vivo) bound to human plasma proteins, principally to α1-acid glycoprotein. Solifenacin is highly distributed to non-CNS tissues, having a mean steady-state volume of distribution of 600L.Metabolism
Solifenacin is extensively metabolized in the liver. The primary pathway for elimination is by way of CYP3A4; however, alternate metabolic pathways exist. The primary metabolic routes of solifenacin are through N-oxidation of the quinuclidin ring and 4R-hydroxylation of tetrahydroisoquinoline ring. One pharmacologically active metabolite (4R-hydroxy solifenacin), occurring at low concentrations and unlikely to contribute significantly to clinical activity, and three pharmacologically inactive metabolites (N-glucuronide and the N-oxide and 4R-hydroxy-N-oxide of solifenacin) have been found in human plasma after oral dosing.Excretion
Following the administration of 10 mg of 14C-solifenacin succinate to healthy volunteers, 69.2% of the radioactivity was recovered in the urine and 22.5% in the feces over 26 days. Less than 15% (as mean value) of the dose was recovered in the urine as intact solifenacin. The major metabolites identified in urine were N-oxide of solifenacin, 4R-hydroxy solifenacin and 4R-hydroxy-N-oxide of solifenacin and in feces 4R-hydroxy solifenacin. The elimination half-life of solifenacin following chronic dosing is approximately 45-68 hours.Drug Interactions
Potent CYP3A4 Inhibitors
In a crossover study, following blockade of CYP3A4 by coadministration of the potent CYP3A4 inhibitor, ketoconazole 400 mg, once daily for 21 days, the mean Cmax and AUC of solifenacin increased by 1.5 and 2.7-fold, respectively [see Dosage and Administration (2.4) and Drug Interactions (7.1)].Warfarin
In a crossover study, subjects received a single oral dose of warfarin 25 mg on the 10th day of dosing with either solifenacin 10 mg or matching placebo once daily for 16 days. For R-warfarin when it was coadministered with solifencin, the mean Cmax increased by 3% and AUC decreased by 2%. For S-warfarin when it was coadministered with solifenacin, the mean Cmax and AUC increased by 5% and 1%, respectively [see Drug Interaction (7.4)].Oral Contraceptives
In a crossover study, subjects received 2 cycles of 21 days of oral contraceptives containing 30 ug ethinyl estradiol and 150 ug levonorgestrel. During the second cycle, subjects received additional solifenacin 10 mg or matching placebo once daily for 10 days starting from 12th day of receipt of oral contraceptives. For ethinyl estradiol when it was administered with solifenacin, the mean Cmax and AUC increased by 2% and 3%, respectively. For levonorgestrel when it was administered with solifenacin, the mean Cmax and AUC decreased by 1% [see Drug Interactions (7.5)].Digoxin
In a crossover study, subjects received digoxin (loading dose of 0.25 mg on day 1, followed by 0.125 mg from days 2 to 8) for 8 days. Consecutively, they received solifenacin 10 mg or matching placebo with digoxin 0.125 mg for additional 10 days. When digoxin was coadministered with solifenacin, the mean Cmax and AUC increased by 13 % and 4%, respectively [see Drug Interactions (7.6)]. -
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
No increase in tumors was found following the administration of solifenacin succinate to male and female mice for 104 weeks at doses up to 200 mg/kg/day (5 and 9 times, respectively, of the exposure at the maximum recommended human dose [MRHD] of 10 mg), and male and female rats for 104 weeks at doses up to 20 and 15 mg/kg/day, respectively (<1 times the exposure at the MRHD).
Solifenacin succinate was not mutagenic in the in vitro Salmonella typhimurium or Escherichia coli microbial mutagenicity test or chromosomal aberration test in human peripheral blood lymphocytes with or without metabolic activation, or in the in vivo micronucleus test in rats.
Solifenacin succinate had no effect on reproductive function, fertility or early embryonic development of the fetus in male and female mice treated with 250 mg/kg/day (13 times the exposure at the MRHD) of solifenacin succinate, and in male rats treated with 50mg/kg/day (<1 times the exposure at the MRHD) and female rats treated with 100 mg/kg/day (1.7 times the exposure at the MRHD) of solifenacin succinate.
-
14 CLINICAL STUDIES
Solifenacin succinate was evaluated in four twelve-week, double-blind, randomized, placebo-controlled, parallel group, multicenter clinical trials for the treatment of overactive bladder in patients having symptoms of urinary frequency, urgency, and/or urge or mixed incontinence (with a predominance of urge). Entry criteria required that patients have symptoms of overactive bladder for ≥3 months duration. These studies involved 3027 patients (1811 on Solifenacin succinate and 1216 on placebo), and approximately 90% of these patients completed the 12-week studies. Two of the four studies evaluated the 5 and 10 mg Solifenacin succinate doses and the other two evaluated only the 10 mg dose. All patients completing the 12-week studies were eligible to enter an open label, long term extension study and 81% of patients enrolling completed the additional 40-week treatment period. The majority of patients were Caucasian (93%) and female (80%) with a mean age of 58 years.
The primary endpoint in all four trials was the mean change from baseline to 12 weeks in number of micturitions/24 hours. Secondary endpoints included mean change from baseline to 12 weeks in number of incontinence episodes/24 hours, and mean volume voided per micturition. The efficacy of Solifenacin succinate was similar across patient age and gender. The mean reduction in the number of micturitions per 24 hours was significantly greater with Solifenacin succinate tablets 5 mg (2.3; p<0.001) and Solifenacin succinate tablets 10 mg (2.7; P<0.001) compared to placebo, (1.4).
The mean reduction in the number of incontinence episodes per 24 hours was significantly greater with Solifenacin succinate 5 mg (1.5; p<0.001) and Solifenacin succinate 10 mg (1.8; p<0.001) treatment groups compared to placebo (1.1). The mean increase in the volume voided per micturition was significantly greater with Solifenacin succinate 5 mg (32.3 mL; p<0.001) and Solifenacin succinate 10 mg (42.5 mL; p<0.001) compared with placebo (8.5 mL).
The results for the primary and secondary endpoints in the four individual 12-week clinical studies of Solifenacin succinate are reported in Tables 3 through 6.
Table 3. Mean Change from Baseline to Endpoint for Solifenacin succinate tablets (5 mg and 10 mg daily) and Placebo: Study 1 Parameter Placebo (N=253) Mean (SE) Solifenacin succinate tablets 5 mg (N=266)
Mean (SE)Solifenacin succinate tablets 10 mg (N=264)
Mean (SE)Urinary Frequency (Number of Micturitions/24 hours)*
Baseline
Reduction
P value vs. placebo12.2 (0.26)
1.2 (0.21)12.1 (0.24)
2.2 (0.18)
<0.00112.3 (0.24)
2.6 (0.20)
<0.001Number of Incontinence Episodes/24 hours†
Baseline
Reduction
P value vs. placebo2.7 (0.23)
0.8 (0.18)2.6 (0.22)
1.4 (0.15)
<0.012.6 (0.23)
1.5 (0.18)
<0.01Volume Voided per micturition [mL]†
Baseline
Increase
P value vs. placebo143.8 (3.37)
7.4 (2.28)149.6 (3.35)
32.9 (2.92)
<0.001147.2 (3.15)
39.2 (3.11)
<0.001* Primary endpoint
† Secondary endpointTable 4. Mean Change from Baseline to Endpoint for Solifenacin succinate tablets (5 mg and 10 mg daily) and Placebo: Study 2 Parameter Placebo (N=281) Mean (SE) Solifenacin succinate tablets 5 mg (N=286)
Mean (SE)Solifenacin succinate tablets 10 mg (N=290)
Mean (SE)Urinary Frequency (Number of Micturitions/24 hours)*
Baseline
Reduction
P value vs. placebo12.3 (0.23)
1.7 (0.19)12.1 (0.23)
2.4 (0.17)
<0.00112.1 (0.21)
2.9 (0.18)
<0.001Number of Incontinence Episodes/24 hours†
Baseline
Reduction
P value vs. placebo3.2 (0.24)
1.3 (0.19)2.6 (0.18)
1.6 (0.16)
<0.012.8 (0.20)
1.6 (0.18)
0.016Volume Voided per micturition [mL]†
Baseline
Increase
P value vs. placebo147.2 (3.18)
11.3 (2.52)148.5 (3.16)
31.8 (2.94)
<0.001145.9 (3.42)
36.6 (3.04)
<0.001* Primary endpoint
† Secondary endpointTable 5. Mean Change from Baseline to Endpoint for Solifenacin succinate tablets (10 mg daily) and Placebo: Study 3 Parameter Placebo (N=309)
Mean (SE)Solifenacin succinate tablets 10 mg (N=306) Mean (SE) Urinary Frequency (Number of Micturitions/24 hours) *
Baseline
Reduction
P value vs. placebo11.5 (0.18)
1.5 (0.15)11.7 (0.18)
3.0 (0.15)
<0.001Number of Incontinence Episodes/24 hours†
Baseline
Reduction
P value vs. placebo3.0 (0.20)
1.1 (0.16)3.1 (0.22)
2.0 (0.19)
<0.001Volume Voided per Micturition [mL]†
Baseline
Increase
P value vs. placebo190.3 (5.48)
2.7 (3.15)183.5 (4.97)
47.2 (3.79)
<0.001* Primary endpoint
†Secondary endpointTable 6. Mean Change from Baseline to Endpoint for Solifenacin succinate tablets (10 mg daily) and Placebo: Study 4 Parameter Placebo (N=295) Mean (SE) Solifenacin succinate tablets 10 mg (N=298) Mean (SE) Urinary Frequency (Number of Micturitions/24 hours) *
Baseline
Reduction
P value vs. placebo11.8 (0.18)
1.3 (0.16)11.5 (0.18)
2.4 (0.15)
<0.001Number of Incontinence Episodes/24 hours†
Baseline
Reduction
P value vs. placebo2.9 (0.18)
1.2 (0.15)2.9 (0.17)
2.0 (0.15)
<0.001Volume Voided per Micturition [mL] †
Baseline
Increase
P value vs. placebo175.7 (4.44)
13.0 (3.45)174.1 (4.15)
46.4 (3.73)
<0.001* Primary endpoint
† Secondary endpoint -
16 HOW SUPPLIED/STORAGE AND HANDLING
Solifenacin succinate tablets are available in bottles as:
Each 5 mg tablet is Yellow colored, round, biconvex, film coated tablet with
 debossed on one side and
debossed on one side and  on the other side.
on the other side.Bottle of 30 NDC 64380-941-04
Bottle of 90 NDC 64380-941-05Each 10 mg tablet is Pink colored, round, biconvex, film coated tablet with
 debossed on one side and
debossed on one side and  on the other side.
on the other side.Bottle of 30 NDC 64380-942-04
Bottle of 90 NDC 64380-942-05Store at 25°C (77°F) with excursions permitted from 15°C to 30°C (59°F - 86°F) [see USP Controlled Room Temperature].
-
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient Information).
Patients should be informed that antimuscarinic agents such as Solifenacin succinate tablets have been associated with constipation and blurred vision. Patients should be advised to contact their physician if they experience severe abdominal pain or become constipated for 3 or more days. Because Solifenacin succinate tablets may cause blurred vision, patients should be advised to exercise caution in decisions to engage in potentially dangerous activities until the drug’s effect on the patient’s vision has been determined. Heat prostration (due to decreased sweating) can occur when anticholinergic drugs, such as Solifenacin succinate tablets, are used in a hot environment. Patients should read the patient leaflet entitled “Patient Information Solifenacin succinate tablets” before starting therapy with Solifenacin succinate tablets.
Patients should be informed that solifenacin may produce angioedema, which could result in life-threatening airway obstruction. Patients should be advised to promptly discontinue solifenacin therapy and seek immediate attention if they experience edema of the tongue or laryngopharynx, or difficulty breathing.
Manufactured by:
Vivimed Life Sciences Private Limited,
Plot No. 101, 102, 107 & 108,
SIDCO Pharmaceutical Complex, Alathur,
Kanchipuram – 603 110, Tamil Nadu, India.Distributed by:
Strides Pharma Inc.,
East Brunswick, NJ 08816 -
PATIENT PACKAGE INSERT
Patient Information
Solifenacin Succinate (soe" li fen' a sin sux' i nate)
TabletsRead the Patient Information that comes with Solifenacin succinate tablets before you start taking it and each time you get a refill. There may be new information. This leaflet does not take the place of talking with your doctor about your medical condition or treatment.
What are Solifenacin succinate tablets?
Solifenacin succinate tablets are a prescription medicine for adults used to treat the following symptoms due to a condition called overactivebladder:
Urge urinary incontinence: a strong need to urinate with leaking or wetting accidents
Urgency: a strong need to urinate right away
Frequency: urinating often.It is not known if Solifenacin succinate tablets are safe and effective in children.
Who should NOT take Solifenacin succinate tablets?
Do not take Solifenacin succinate tablets if you:
are not able to empty your bladder (urinary retention)
have delayed or slow emptying of your stomach (gastric retention)
have an eye problem called “uncontrolled narrow-angle glaucoma”
are allergic to solifenacin succinate or any of the ingredients in Solifenacin succinate tablets. See the end of this leaflet for a complete list of ingredients.What should I tell my doctor before taking Solifenacin succinate tablets?
Before you take Solifenacin succinate tablets, tell your doctor if you:
have any stomach or intestinal problems or problems with constipation
have trouble emptying your bladder or you have a weak urine stream
have an eye problem called “narrow angle glaucoma”
have liver problems
have kidney problems
have a rare heart problem called “QT prolongation”
are pregnant or plan to become pregnant. It is not known if Solifenacin succinate tablets will harm your unborn baby. Talk to your doctor if you are pregnant or plan to become pregnant.
are breastfeeding or plan to breastfeed. It is not known if Solifenacin succinate tablet passes into your breast milk. You and your doctor should decide if you will take Solifenacin succinate tablets or breastfeed. You should not do both.Tell your doctor about all the medicines you take, including prescription and nonprescription medicines, vitamins, and herbal supplements. Solifenacin succinate tablets may affect the way other medicines work, and other medicines may affect how Solifenacin succinate tablets works.
How should I take Solifenacin succinate tablets?
Take Solifenacin succinate tablets exactly as your doctor tells you to take it.
You should take 1 Solifenacin succinate tablet 1 time a day.
You should take Solifenacin succinate tablets with water and swallow the tablet whole.
You can take Solifenacin succinate tablets with or without food.
If you miss a dose of Solifenacin succinate tablets, begin taking Solifenacin succinate tablets again the next day. Do not take 2 doses of Solifenacin succinate tablets the same day.
If you take too much Solifenacin succinate tablets, call your doctor or go to the nearest hospital emergency room right away.What should I avoid while taking Solifenacin succinate tablets?
Solifenacin succinate tablets can cause blurred vision or drowsiness. Do not drive or operate heavy machinery until you know how Solifenacin succinate tablets affects you.What are the possible side effects of Solifenacin succinate tablets?
Solifenacin succinate tablets may cause serious side effects including:
Serious allergic reaction. Stop taking Solifenacin succinate tablets and get medical help right away if you have:
o hives, skin rash or swelling
o severe itching
o swelling of your face, mouth or tongue
o trouble breathing
The most common side effects of Solifenacin succinate tablets include:
dry mouth
constipation. Call your doctor if you get severe stomach area (abdominal) pain or become constipated for 3 or more days.
urinary tract infection
blurred vision
heat exhaustion or heat-stroke. This can happen when Solifenacin Succinate Tablets is used in hot environment. Symptoms may include:
o decreased sweating
o dizziness
o tiredness
o nausea
o increase in body temperature
Tell your doctor if you have any side effect that bothers you or that does not go away.These are not all the possible side effects of Solifenacin succinate tablets. For more information, ask your doctor or pharmacist.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
How should I store Solifenacin succinate tablets?
Store Solifenacin succinate tablets between 59°F to 86°F (15°C to 30°C). Keep the bottle closed.
Safely throw away medicine that is out of date or no longer need.Keep Solifenacin succinate tablets and all medicines out of the reach of children.
General information about the safe and effective use of Solifenacin succinate tablets.
Medicines are sometimes prescribed for purpose other than those listed in Patient Information leaflets. Do not use Solifenacin succinate tablets for a condition for which it was not prescribed. Do not give Solifenacin succinate tablets to other people, even if they have the same symptoms you have. It may harm them.This leaflet summarizes the most important information about Solifenacin succinate tablets. If you would like more information, talk with your doctor. You can ask your doctor or pharmacist for information about Solifenacin succinate tablets that is written for health professionals.
What are the ingredients in Solifenacin succinate tablets?
Active ingredient: solifenacin succinate
Inactive ingredients: Colloidal Silicon dioxide (Aerosil 200) NF, Corn Starch NF (Maize Starch B-Pharma Grade),HPMC 2910/Hypromellose USP, Hydroxy Propyl Methyl Cellulose USP (Methocel E5 Premium LV), Iron Oxide Red NF (for 10 mg Solifenacin succinate tablet), Iron Oxide Yellow NF (for 5 mg Solifenacin succinate tablet), Lactose Monohydrate NF – Pharmatose 200 M (Milled), Lactose Monohydrate NF (Super Tab 11SD), Macrogol/PEG NF, Magnesium Stearate NF (Ligamed MF-2-V), Talc USP and Titanium Dioxide USP.What is overactive bladder?
Overactive bladder occurs when you cannot control your bladder contractions. When these muscle contractions happen too often or cannot be controlled you can get symptoms of overactive bladder, which are urinary frequency, urinary urgency, and urinary incontinence (leakage).Rx Only
Manufactured by:
Vivimed Life Sciences Private Limited,
Plot No. 101, 102, 107 & 108,
SIDCO Pharmaceutical Complex,
Alathur, Kanchipuram – 603 110, Tamil nadu, India.Distributed by:
Strides Pharma Inc.,
East Brunswick, NJ 08816 -
PRINCIPAL DISPLAY PANEL
NDC 64380-941-04
Solifenacin Succinate Tablets
5 mg
30 film-coated tablets
Rx Only

NDC 64380-941-05
Solifenacin Succinate Tablets
5 mg
90 film-coated tablets
Rx Only

NDC 64380-942-04
Solifenacin Succinate Tablets
10 mg
30 film-coated tablets
Rx Only

NDC 64380-942-05
Solifenacin Succinate Tablets
10 mg
90 film-coated tablets
Rx Only

-
INGREDIENTS AND APPEARANCE
SOLIFENACIN SUCCINATE 5 MG
solifenacin succinate tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 64380-941 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength SOLIFENACIN SUCCINATE (UNII: KKA5DLD701) (SOLIFENACIN - UNII:A8910SQJ1U) SOLIFENACIN SUCCINATE 5 mg Inactive Ingredients Ingredient Name Strength SILICON DIOXIDE (UNII: ETJ7Z6XBU4) STARCH, CORN (UNII: O8232NY3SJ) HYPROMELLOSE 2910 (6 MPA.S) (UNII: 0WZ8WG20P6) MAGNESIUM STEARATE (UNII: 70097M6I30) LACTOSE MONOHYDRATE (UNII: EWQ57Q8I5X) TALC (UNII: 7SEV7J4R1U) POLYETHYLENE GLYCOL 8000 (UNII: Q662QK8M3B) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) FERRIC OXIDE YELLOW (UNII: EX438O2MRT) Product Characteristics Color yellow Score no score Shape ROUND (BICONVEX) Size 8mm Flavor Imprint Code 44;V Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 64380-941-04 30 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 12/01/2019 2 NDC: 64380-941-05 90 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 12/01/2019 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA212214 12/01/2019 SOLIFENACIN SUCCINATE 10 MG
solifenacin succinate tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 64380-942 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength SOLIFENACIN SUCCINATE (UNII: KKA5DLD701) (SOLIFENACIN - UNII:A8910SQJ1U) SOLIFENACIN SUCCINATE 10 mg Inactive Ingredients Ingredient Name Strength SILICON DIOXIDE (UNII: ETJ7Z6XBU4) STARCH, CORN (UNII: O8232NY3SJ) HYPROMELLOSE 2910 (6 MPA.S) (UNII: 0WZ8WG20P6) MAGNESIUM STEARATE (UNII: 70097M6I30) LACTOSE MONOHYDRATE (UNII: EWQ57Q8I5X) TALC (UNII: 7SEV7J4R1U) POLYETHYLENE GLYCOL 8000 (UNII: Q662QK8M3B) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) FERRIC OXIDE RED (UNII: 1K09F3G675) Product Characteristics Color pink Score no score Shape ROUND (BICONVEX) Size 8mm Flavor Imprint Code 45;V Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 64380-942-04 30 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 12/01/2019 2 NDC: 64380-942-05 90 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 12/01/2019 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA212214 12/01/2019 Labeler - Strides Pharma Inc. (650738743) Registrant - Strides Pharma Global Pte.Ltd. (659220961) Establishment Name Address ID/FEI Business Operations Vivimed Life Sciences Private Limited 860477684 manufacture(64380-941, 64380-942) , analysis(64380-941, 64380-942) , pack(64380-941, 64380-942)
 debossed on one side and
debossed on one side and  debossed on one side and
debossed on one side and © 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.