These highlights do not include all the information needed to use SORAFENIB TABLETS safely and effectively. See full prescribing information for SORAFENIB TABLETS. Sorafenib tablets, for oral use Initial U.S. Approval: 2005
sorafenib by
Drug Labeling and Warnings
sorafenib by is a Prescription medication manufactured, distributed, or labeled by Bora Pharmaceutical Laboratories Inc., TWi Pharmaceuticals, Inc. Zhongli Plant. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
SORAFENIB- sorafenib tablet, film coated
Bora Pharmaceutical Laboratories Inc.
----------
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use SORAFENIB TABLETS safely and effectively.
See full prescribing information for SORAFENIB TABLETS. Sorafenib tablets, for oral use Initial U.S. Approval: 2005 RECENT MAJOR CHANGESWarnings and Precautions, Risk of Impaired Wound Healing (5.7) 5/2020 INDICATIONS AND USAGEDOSAGE AND ADMINISTRATIONThe recommended dosage is 400 mg orally twice daily without food. (2.1) (2) DOSAGE FORMS AND STRENGTHSTablets: 200 mg (3) (3) CONTRAINDICATIONSSorafenib tablets are contraindicated in patients with known severe hypersensitivity to sorafenib or any other component of sorafenib tablets. (4)
WARNINGS AND PRECAUTIONSCardiovascular Events: Consider temporary or permanent discontinuation of sorafenib tablets.(2.2, 5.1)
ADVERSE REACTIONSThe most common adverse reactions (≥20%) are diarrhea, fatigue, infection, alopecia, hand-foot skin reaction, rash, weight loss, decreased appetite, nausea, gastrointestinal and abdominal pains, hypertension, and hemorrhage. (6) (6) To report SUSPECTED ADVERSE REACTIONS, contact Twi Pharmaceuticals, Inc. at 1-844-518-2989 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch (6) DRUG INTERACTIONSStrong CYP3A Inducers: Avoid strong CYP3A4 inducers.(7.1) (7) USE IN SPECIFIC POPULATIONSLactation: Advise women not to breastfeed. (8.2) (8) See 17 for PATIENT COUNSELING INFORMATION. Revised: 9/2023 |
FULL PRESCRIBING INFORMATION
2.1 Recommended Dosage
The recommended dosage of sorafenib tablets is 400 mg orallytwice daily without food (at least 1 hourbefore or 2 hours after a meal) until the patient is no longer clinically benfiting from therapy or untilunacceptable toxicity.
2.2 Dose Modifications for Adverse Reactions
Recommended Dosage Modifications
The recommended dosage modifications for adverse reactions are provided in Tables 1, 2, and 3.
Table 1: Recommended Dose Reductions forAdverse Reactions
|
Dose Reduction |
Hepatocellular Carcinoma |
Differentiated Thyroid Carcinoma |
|
First Dose Reduction |
400 mg orally once daily |
400 mg orally in the morning and 200 mg orally in the evening about 12 hours apart OR 200 mg orally in the morning and 400 mg orally in the evening about 12 hours apart |
|
Second Dose Reduction |
200 mg orally once daily OR 400 every other day |
200 mg orally twice daily |
|
Third Dose Reduction |
None |
200 mg orally once daily |
Table 2: Recommended Dosage Modifications of Sorafenib Tablets for Adverse Reactions
|
Adverse Reaction |
Severity1 |
SorafenibTablets Dosage Modification |
|
Cardiovascular Events[see Warnings and Precautions (5.1)] |
||
|
Cardiac Ischemia and/or Infarction |
Grade 2 and above |
Permanently discontinue. |
|
Congestive Heart Failure |
Grade 3 |
Interrupt2 until Grade 1 or less, resume at reduced dose by 1 dose level.3 |
|
Grade 4 |
Permanently discontinue. |
|
|
Hemorrhage[see Warnings and Precautions (5.2)] |
Grade 2 and above requiring medical intervention |
Permanently discontinue. |
|
Hypertension[see Warnings and Precautions (5.3)] |
Grade 2 (symptomatic/persistent) OR Grade 2 symptomatic increase by greater than 20 mm Hg (diastolic) or greater than 140/90 mm Hg if previously within normal limits OR Grade 3 |
Interrupt until symptoms resolve and diastolic blood pressure less than 90 mm Hg, then resume at reduced dose by 1 dose level.3 If needed, reduce another dose level.3 |
|
Grade 4 |
Permanently discontinue. |
|
|
Gastrointestinal Perforation [see Warnings and Precautions (5.5)] |
Any grade |
Permanently discontinue. |
|
QT Interval Prolongation [see Warnings and Precautions (5.9)] |
Greater than 500 milliseconds OR Increase from baseline of 60 milliseconds or greater |
Interrupt and correct electrolyte abnormalities (magnesium, potassium, calcium). Use medical judgement before restarting. |
|
Drug-Induced Liver Injury [see Warnings and Precautions (5.10)] |
Grade 3 ALT or higher in the absence of another cause4 OR AST/ALT greater than 3 × upper limit normal (ULN) with bilirubin greater than 2 × ULN in the absence of another cause4 |
Permanently discontinue. |
|
Non-hematological toxicities[see Adverse Reactions (6.1)] |
Grade 2 |
Continue treatment at reduced dose by 1 dose level. |
|
Grade 3 |
||
|
1st occurrence |
Interrupt until Grade 2 or less, then resume at reduced dose by 1 dose level. |
|
|
No improvement within 7 days OR 2nd or 3rd occurrence |
Interrupt until Grade 2 or less, then resume at reduced dose by 2 dose levels. |
|
|
4th occurrence |
Interrupt until Grade 2 or less, then resume at reduced dose by 2 dose levels for HCC or 3 dose levels for DTC. |
|
|
Grade 4 |
Permanently discontinue. |
|
1 Adverse reactions graded according to National Cancer Institute Common Terminology Criteria for Adverse Events version 3.0 (NCI CTCAE v3.0).
2 If no recovery after 30 day interruption, discontinue treatment unless the patient is deriving clinical benefit.
3 If more than 2 dose reductions are required, permanently discontinue treatment.
4 In addition, any grade increased alkaline phosphatase in the absence of known bone pathology and Grade 2 or worse increased bilirubin; any 1 of the following: INR of 1.5 or greater, ascites and/or encephalopathy in the absence of underlying cirrhosis or other organ failure considered to be due to drug-induced liver injury.
Table 3: Recommended Dosage Modifications for Dermatologic Toxicities
|
Dermatologic Toxicity Grade |
Occurrence |
SorafenibTablets Dosage Modification |
|
|
Hepatocellular |
Differentiated Thyroid Carcinoma |
||
|
Grade 2: Painful erythema and swelling of the hands or feet and/or discomfort affecting the patient’s normal activities |
1st occurrence |
Continue sorafenib tablets and consider topical therapy for symptomatic relief. If no improvement within 7 days, see below. |
Decrease sorafenib tablets to 600 mg daily If no improvement within 7 days, see below. |
|
No improvement within 7 days at reduced dose OR 2nd and 3rd occurrence |
Interrupt sorafenib tablets until resolved or improved to Grade 0 to 1. |
Interrupt sorafenib tablets until completely resolved or improved to Grade 1. |
|
|
When resuming treatment, decrease dose by 1 dose level. |
When resuming treatment, decrease dose by 1 dose level for 2nd occurrence and 2 dose levels for 3rd occurrence. |
||
|
4th occurrence |
Discontinue sorafenib tablets treatment. |
||
|
Grade 3:Moist desquamation, ulceration, blistering, or severe pain of the hands or feet, resulting in inability to work or perform activities of daily living |
1st occurrence |
Interrupt sorafenib tablets until resolved or improved to Grade 0 to 1. |
Interrupt sorafenib tablets until completely resolved or improved to Grade 1. |
|
When resuming treatment, decrease dose by 1 dose level. |
When resuming treatment, decrease dose by 1 dose level. |
||
|
2nd occurrence |
Interrupt sorafenib tablets until resolved or improved to Grade 0 to 1. |
Interrupt sorafenib tablets until completely resolved or improved to Grade 1. |
|
|
When resuming treatment, decrease dose by 1 dose level. |
When resuming treatment, decrease dose by 2 dose levels. |
||
|
3rd occurrence |
Discontinue sorafenib tablets treatment. |
||
Following improvement of Grade 2 or 3 dermatologic toxicity to Grade 0 or 1 for at least 28 days on a reduced dose of sorafenib tablets, the dose of sorafenib tablets may be increased 1 dose level from the reduced dose. Approximately 50% of patients requiring a dose reduction for dermatologic toxicity are expected to meet these criteria for resumption of the higher dose and roughly 50% of patients resuming the previous dose are expected to tolerate the higher dose (that is, maintain the higher dose level without recurrent Grade 2 or higher dermatologic toxicity).
4 CONTRAINDICATIONS
Sorafenib tablets are contraindicated in patients with known severe hypersensitivity to sorafenib or any other component of sorafenib tablets.
Sorafenib tablets in combination with carboplatin and paclitaxel are contraindicated in patients with squamous cell lung cancer [see Warnings and Precautions (5.8)].
5.1 Cardiovascular Events
In the SHARP (HCC) study, the incidence of cardiac ischemia/infarction was 2.7% in sorafenib tablets-treated patients compared with 1.3% in those receiving placebo, and in the DECISION (DTC) study, the incidence of cardiac ischemia/infarction was 1.9% in the sorafenib tablets -treated group compared with 0% in patients receiving placebo. Patients with unstable coronary artery disease or recent myocardial infarction were excluded from this study. In multiple clinical trials, congestive heart failure has been reported in 1.9% of sorafenib tablets - treated patients (N=2276) [see Adverse Reactions (6.2)].
Consider temporary or permanent discontinuation of sorafenib tablets in patients who develop cardiovascular events [see Dosage and Administration (2.2)].
5.2 Hemorrhage
An increased risk of bleeding may occur following sorafenib tablets administration. In the SHARP (HCC) study, the rates of bleeding from esophageal varices (2.4% and 4%) and of bleeding with a fatal outcome from any site (2.4% and 4%) were similar in sorafenib tablets -treated patients and those receiving placebo, respectively. In the DECISION (DTC) study, bleeding was reported in 17.4% of sorafenib tablets -treated patients and 9.6% of those receiving placebo; however, the incidence of Grade 3 bleeding was similar (1% and 1.4%) in sorafenib tablets -treated patients and in those receiving placebo.
If any bleeding necessitates medical intervention, consider permanent discontinuation of sorafenib tablets [see Dosage and Administration (2.2)]. Due to the potential risk of bleeding, treat tracheal, bronchial, and esophageal infiltration with local therapy prior to administering sorafenib tablets in patients with DTC.
5.3 Hypertension
In the SHARP (HCC) study, hypertension was reported in 9.4% of sorafenib tablets -treated patients and 4.3% of patients receiving placebo. In the DECISION (DTC) study, hypertension was reported in 40.6% of sorafenib tablets -treated patients and 12.4% of patients receiving placebo. Hypertension was usually mild to moderate, occurred early in the course of treatment, and was managed with standard antihypertensive therapy. Permanent discontinuation due to hypertension occurred in 1 of 297 sorafenib tablets -treated patients in the SHARP (HCC) study, and 1 of 207 sorafenib tablets -treated patients in the DECISION (DTC) study.
Monitor blood pressure weekly during the first 6 weeks of sorafenib tablets. Thereafter, monitor blood pressure and treat hypertension, if required, in accordance with standard medical practice. In cases of severe or persistent hypertension despite institution of antihypertensive therapy, consider temporary or permanent discontinuation of sorafenib tablets [see Dosage and Administration (2.2)].
5.4 Dermatologic Toxicities
Hand-foot skin reaction and rash represent the most common adverse reactions attributed to sorafenib tablets. Rash and hand-foot skin reaction are usually Grade 1 and 2 and generally appear during the first six weeks of treatment with sorafenib tablets. Permanent discontinuation of therapy due to hand-foot skin reaction occurred in 4 (1.3%) of 297 sorafenib tablets -treated patients with HCC, and 11 (5.3%) of 207 sorafenib tablets -treated patients with DTC.
Management of dermatologic toxicities may include topical therapies for symptomatic relief, temporary treatment interruption and/or dose reduction of sorafenib tablets, or in severe or persistent cases, permanent discontinuation of sorafenib tablets [see Dosage and Administration (2.2)].
There have been reports of severe dermatologic toxicities, including Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN). These cases may be life-threatening. Discontinue sorafenib tablets if SJS or TEN are suspected.
5.5 Gastrointestinal Perforation
Gastrointestinal perforation has been reported in less than 1% of patients taking sorafenib tablets. In some cases this was not associated with apparent intra-abdominal tumor. In the event of a gastrointestinal perforation, permanently discontinue sorafenib tablets.
5.6 Increased Risk of Bleeding with Concomitant Us e of Warfarin
Infrequent bleeding or elevations in the International Normalized Ratio (INR) have been reported in some patients taking warfarin while on sorafenib tablets. Monitor patients taking concomitant warfarin regularly for changes in prothrombin time (PT), INR or clinical bleeding episodes.
5.7 Risk of Impaired Wound Healing
Impaired wound healing can occur in patients who receive drugs that inhibit the VEGF signaling pathway. Therefore, sorafenib tablets has the potential to adversely affect wound healing.
Withhold sorafenib tablets for at least 10 days prior to elective surgery. Do not administer for at least 2 weeks following major surgery and until adequate wound healing. The safety of resumption of sorafenib tablets after resolution of wound healing complications has not been established.
5.8 Increased Mortality Observed with Sorafenib Tablets Administered in Combination with Carboplatin/Paclitaxel and Gemcitabine/Cisplatin in Squamous Cell Lung Cancer
In a subset analysis of two randomized controlled trials in chemo-naive patients with Stage IIIB-IV non-small cell lung cancer, patients with squamous cell carcinoma experienced higher mortality with the addition of sorafenib tablets compared to those treated with carboplatin/paclitaxel alone (HR 1.81; 95% CI 1. 19, 2.74) and gemcitabine/cisplatin alone (HR 1.22; 95% CI 0.82, 1.80). The use of sorafenib tablets in combination with carboplatin/paclitaxel is contraindicated in patients with squamous cell lung cancer. Sorafenib tablets in combination with gemcitabine/cisplatin are not recommended in patients with squamous cell lung cancer. The safety and effectiveness of sorafenib tablets has not been established in patients with non-small cell lung cancer.
5.9 QT Interval Prolongation
Sorafenib tablets can prolong the QT/QTc interval. QT/QTc interval prolongation increases the risk for ventricular arrhythmias.
Avoid sorafenib tablets in patients with congenital long QT syndrome. Monitor electrolytes and electrocardiograms in patients with congestive heart failure, bradyarrhythmias, drugs known to prolong the QT interval, including Class Ia and III antiarrhythmics. Correct electrolyte abnormalities (magnesium, potassium, calcium). Interrupt sorafenib tablets if QTc interval is greater than 500 milliseconds or for an increase from baseline of 60 milliseconds or greater [see Clinical Pharmacology (12.2)].
5.10 Drug-Induced Liver Injury
Sorafenib-induced hepatitis is characterized by a hepatocellular pattern of liver damage with significant increases of transaminases which may result in hepatic failure and death. Increases in bilirubin and INR may also occur. The incidence of severe drug-induced liver injury, defined as elevated transaminase levels above 20 times the upper limit of normal or transaminase elevations with significant clinical sequelae (for example, elevated INR, ascites, fatal, or transplantation), was two of 3,357 patients (0.06%) in a global monotherapy database.
Monitor liver function tests regularly. In case of significantly increased transaminases without alternative explanation, such as viral hepatitis or progressing underlying malignancy, discontinue sorafenib tablets [see Dosage and Administration (2.2)].
5.11 Embryo-Fetal Toxicity
Based on its mechanism of action and findings in animals, sorafenib tablets may cause fetal harm when administered to a pregnant woman. Sorafenib caused embryo-fetal toxicities in animals at maternal exposures that were significantly lower than the human exposures at the recommended dose of 400 mg twice daily. Advise pregnant women and females of reproductive potential of the potential risk to a fetus. Advise females of reproductive potential to use effective contraception during treatment and for 6 months following the last dose of sorafenib tablets. Advise male patients with female partners of reproductive potential and pregnant partners to use effective contraception during treatment and for 3 months following the last dose of sorafenib tablets [see Use in Specific Populations (8.1, 8.3)].
5.12 Impairment of Thyroid Stimulating Hormone Suppression in Differentiated Thyroid Carcinoma
Sorafenib tablets impairs exogenous thyroid suppression. In the DECISION (DTC) study, 99% of patients had a baseline thyroid stimulating hormone (TSH) level less than 0.5 mU/L. Elevation of TSH level above 0.5 mU/L was observed in 41% of sorafenib tablets -treated patients as compared with 16% of those receiving placebo patients. For patients with impaired TSH suppression while receiving sorafenib tablets, the median maximal TSH was 1.6 mU/L and 25% had TSH levels greater than 4.4 mU/L.
Monitor TSH levels monthly and adjust thyroid replacement medication as needed in patients with DTC.
6 ADVERSE REACTIONS
The following clinically significant adverse reactions are discussed elsewhere in the labeling:
- Cardiovascular events [see Warnings and Precautions ( 5.1)]
- Hemorrhage [see Warnings and Precautions ( 5.2)]
- Hypertension [see Warnings and Precautions ( 5.3)]
- Dermatologic toxicities [see Warnings and Precautions ( 5.4)]
- Gastrointestinal perforation [see Warnings and Precautions ( 5.5)]
- QT interval prolongation [see Warnings and Precautions ( 5.9) and Clinical Pharmacology( 12.2)]
- Drug-induced liver injury [see Warnings and Precautions ( 5.10)]
- Impairment of TSH suppression in DTC [see Warnings and Precautions ( 5.12)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The data described reflect exposure to sorafenib tablets in 504 patients who participated in placebo-controlled studies in hepatocellular carcinoma N=297), or differentiated thyroid carcinoma (N = 207). The most common adverse reactions (≥20%), which were considered to be related to sorafenib tablets, in patients with HCC or DTC are diarrhea, fatigue, infection, alopecia, hand-foot skin reaction, rash, weight loss, decreased appetite, nausea, gastrointestinal and abdominal pains, hypertension, and hemorrhage.
Hepatocellular Carcinoma
Table 4 shows the percentage of patients in the SHARP (HCC) study experiencing adverse reactions that were reported in at least 10% of patients and at a higher rate in the Sorafenib Tablets -treated group than in those eceiving placebo.
Table 4: Adverse Reactions Reported in at Least 10% of Patients and at a Higher Rate in Sorafenib Tablets Arm than the Placebo Arm–SHARP (HCC)
|
Adverse Reaction 1 |
Sorafenib Tablets N = 297 |
Placebo N = 302 |
||||
|
All Grades% |
Grade 3% |
Grade 4% |
All Grades % |
Grade 3% |
Grade 4% |
|
|
Any Adverse Reaction |
98 |
39 |
6 |
96 |
24 |
8 |
|
Gastrointestinal | ||||||
|
Diarrhea |
55 |
10 |
< 1 |
25 |
2 |
0 |
|
Anorexia |
29 |
3 |
0 |
18 |
3 |
< 1 |
|
Nausea |
24 |
1 |
0 |
20 |
3 |
0 |
|
Vomiting |
15 |
2 |
0 |
11 |
2 |
0 |
|
Constipation |
14 |
0 |
0 |
10 |
0 |
0 |
|
Constitutional symptoms | ||||||
|
Fatigue |
46 |
9 |
1 |
45 |
12 |
2 |
|
Weight loss |
30 |
2 |
0 |
10 |
1 |
0 |
|
Pain | ||||||
|
Pain, abdomen |
31 |
9 |
0 |
26 |
5 |
1 |
|
Dermatology/skin | ||||||
|
Hand-foot skin reaction |
21 |
8 |
0 |
3 |
< 1 |
0 |
|
Rash/desquamation |
19 |
1 |
0 |
14 |
0 |
0 |
|
Alopecia |
14 |
0 |
0 |
2 |
0 |
0 |
|
Pruritus |
14 |
< 1 |
0 |
11 |
< 1 |
0 |
|
Dry skin |
10 |
0 |
0 |
6 |
0 |
0 |
|
Hepatobiliary/pancreas | ||||||
|
Liver dysfunction |
11 |
2 |
1 |
8 |
2 |
1 |
1Adverse reactions graded according to National Cancer Institute Common Terminology Criteria for Adverse Events version 3.0 (NCI CTCAE v3.0).
Hypertension was reported in 9% of patients treated with sorafenib tablets and 4% of those receiving placebo. Grade 3 hypertension was reported in 4% of sorafenib tablets -treated patients and 1% of those receiving placebo.
Hemorrhage/bleeding was reported in 18% of those receiving sorafenib tablets and 20% of patients receiving placebo. The rates of Grade 3 and 4 bleeding were also higher in patients receiving placebo (Grade 3 – 3% sorafenib tablets and 5% placebo and Grade 4 – 2% sorafenib tablets and 4% placebo). Bleeding from esophageal varices was reported in 2.4% in sorafenib tablets -treated patients and 4% of patients receiving placebo.
Renal failure was reported in <1% of patients treated with sorafenib tablets and 3% of patients receiving placebo. Clinical pancreatitis was reported in 1 of 297 sorafenib tablets -treated patients (Grade 2).
The rate of adverse reactions (including those associated with progressive disease) resulting in permanent discontinuation was similar in both the sorafenib tablets -treated patients and those receiving placebo (32% of sorafenib tablets -treated patients and 35% of patients receiving placebo).
Laboratory test abnormalities reported in SHARP are presented in Table 5.
Table 5: Laboratory Test Abnormalities Reported in SHARP (HCC)
|
Laboratory Parameter 1 |
Sorafenib Tablets N=297 |
Placebo N=302 |
||
|
All Grades(%) |
Grade 3 or 4(%) |
All Grades(%) |
Grade 3 or 4(%) |
|
|
Hypoalbuminemia |
59 |
0 |
47 |
0 |
|
Elevated Lipase |
40 |
9 |
37 |
9 |
|
Lymphopenia |
47 |
NR |
42 |
NR |
|
Thrombocytopenia |
46 |
4 |
41 |
< 1 |
|
Elevated INR |
42 |
4 |
34 |
2 |
|
Hypophosphatemia |
35 |
11 |
11 |
2 |
|
Elevated Amylase |
34 |
2 |
29 |
2 |
|
Hypocalcemia |
27 |
2.4 |
15 |
1 |
|
Hypokalemia |
10 |
< 1 |
6 |
< 1 |
1Laboratory parameters graded according to National Cancer Institute Common Terminology Criteria for Adverse Events version 3.0 (NCI CTCAE v3.0).
NR = not reported
Differentiated Thyroid Carcinoma
The safety of sorafenib tablets was evaluated in DECISION in 416 patients with locally recurrent or metastatic, progressive differentiated thyroid carcinoma (DTC) refractory to radioactive iodine (RAI) treatment randomized to receive 400 mg twice daily sorafenib tablets (n=207) or matching placebo (n=209) until disease progression or intolerable toxicity in a double-blind trial [see Clinical Studies (14.3)]. The data described below reflect a median exposure to sorafenib tablets for 46 weeks (range 0.3 to 135). The population exposed to sorafenib tablets was 50% male, and had a median age of 63 years.
Dose interruptions for adverse reactions were required in 66% of patients receiving sorafenib tablets and dose reductions were required in 64% of patients. Adverse reactions that resulted in treatment discontinuation were reported in 14% of sorafenib tablets -treated patients compared to 1.4% of patients receiving placebo.
Table 8 shows the percentage of DTC patients experiencing adverse reactions at a higher rate in sorafenib tablets -treated patients than in patients receiving placebo in the double-blind phase of the DECISION study. Grade 3 adverse reactions occurred in 53% of sorafenib tablets -treated patients compared to 23% of patients receiving placebo. Grade 4 adverse reactions occurred in 12% of sorafenib tablets-treated patients compared to 7% of patients receiving placebo.
Table 8: Selected Adverse Reactions Occurring at a Higher Incidence in Sorafenib Tablets -Treated Patients [Between Arm Difference of ≥ 5% (All Grades)1 or ≥ 2% (Grades 3 and 4)]
|
Adverse Reaction |
Sorafenib Tablets N = 207 |
Placebo N = 209 |
||
|
All Grades (%) |
Grades 3 and 4 (%) |
All Grades (%) |
Grades 3 and 4 (%) |
|
|
Skin and subcutaneous tissue disorders |
||||
|
PPES 5 |
69 |
19 |
8 |
0 |
|
Alopecia |
67 |
0 |
8 |
0 |
|
Rash |
35 |
5 |
7 |
0 |
|
Pruritus |
20 |
0.5 |
11 |
0 |
|
Dry skin |
13 |
0.5 |
5 |
0 |
|
Erythema |
10 |
0 |
0.5 |
0 |
|
Hyperkeratosis |
7 |
0 |
0 |
0 |
|
Gastrointestinal disorders |
||||
|
Diarrhea |
68 |
6 |
15 |
1 |
|
Stomatitis 3 |
24 |
2 |
3 |
0 |
|
Nausea |
21 |
0 |
12 |
0 |
|
Abdominal pain 2 |
20 |
1 |
7 |
1 |
|
Constipation |
16 |
0 |
8 |
0.5 |
|
Oral pain 4 |
14 |
0.5 |
6 |
0 |
|
Vomiting |
11 |
0 |
3 |
0 |
|
Investigations |
||||
|
Weight loss |
49 |
6 |
14 |
1 |
|
General disorders and administration site conditions |
||||
|
Fatigue |
41 |
5 |
20 |
1 |
|
Asthenia |
12 |
0 |
7 |
0 |
|
Pyrexia |
11 |
1 |
5 |
0 |
|
Vascular disorders |
||||
|
Hypertension 6 |
41 |
10 |
12 |
2 |
|
Metabolism and nutrition disorders |
||||
|
Decreased appetite |
30 |
2 |
5 |
0 |
|
Nervous system disorders |
||||
|
Headache |
17 |
0 |
6 |
0 |
|
Dysgeusia |
6 |
0 |
0 |
0 |
|
Musculoskeletal and connective tissue disorders |
||||
|
Pain in extremity |
15 |
1 |
7 |
0 |
|
Muscle spasms |
10 |
0 |
3 |
0 |
|
Respiratory, thoracic and mediastinal disorders |
||||
|
Dysphonia |
13 |
0.5 |
3 |
0 |
|
Epistaxis |
7 |
0 |
1 |
0 |
|
Neoplasms benign, malignant and unspecified |
||||
|
Squamous cell carcinoma of skin |
3 |
3 |
0 |
0 |
1 National Cancer Institute Common Terminology Criteria for Adverse Events Version 3.0
2 Includes the following terms: abdominal pain, abdominal discomfort, hepatic pain, esophageal pain, esophageal discomfort, abdominal pain lower, abdominal pain upper, abdominal tenderness, abdominal rigidity
3 Includes the following terms: stomatitis, aphthous stomatitis, mouth ulceration, mucosal inflammation
4 Includes the following terms: oral pain, oropharyngeal discomfort, glossitis, burning mouth syndrome, glossodynia
5 Palmar-plantar erythrodysesthesia syndrome (Hand-foot skin reaction)
6 Includes the following terms: hypertension, blood pressure increased, blood pressure systolic increased
The relative increase for the following laboratory abnormalities observed in sorafenib-treated patients as compared to patients receiving placebo in the DECISION study is similar to that observed in the RCC and HCC studies: lipase, amylase, hypokalemia, hypophosphatemia, neutropenia, lymphopenia, anemia, and thrombocytopenia. Hypocalcemia was more frequent and more severe in patients with DTC, especially those with a history of hypoparathyroidism, compared to patients with RCC or HCC. Other laboratory test abnormalities reported in DECISION are presented in Table 9.
Table 9: Laboratory Test Abnormalities Reported in DECISION (DTC)
|
Laboratory Parameter 1 |
Sorafenib Tablets N=207 |
Placebo N=209 |
||
|
All Grades (%) |
Grade 3 or 4 (%) |
All Grades (%) |
Grade 3 or 4 (%) |
|
|
Elevated ALT |
59 |
4 |
24 |
0 |
|
Elevated AST |
54 |
2 |
15 |
0 |
|
Hypocalcemia |
36 |
10 |
11 |
3 |
1Laboratory parameters graded according to National Cancer Institute Common Terminology Criteria for Adverse Events version 3.0 (NCI CTCAE v3.0).
Additional Data from Multiple Clinical Trials
The following additional drug-related adverse reactions and laboratory abnormalities were reported from clinical trials of sorafenib tablets (very common 10% or greater, common 1 to less than 10%, uncommon 0.1% to less than 1%, rare less than 0.1 %):
Cardiovascular:Common: congestive heart failure*†, myocardial ischemia and/or infarction Uncommon: hypertensive crisis* Rare: QT prolongation*
Dermatologic:Very common: erythema Common: exfoliative dermatitis, acne, flushing, folliculitis, hyperkeratosis Uncommon: eczema, erythema multiforme
Digestive:Very common: increased lipase, increased amylase Common: mucositis, stomatitis (including dry mouth and glossodynia), dyspepsia, dysphagia, gastrointestinal reflux Uncommon: pancreatitis, gastritis, gastrointestinal perforations*, cholecystitis, cholangitis
Note that elevations in lipase are very common (41%, see below); a diagnosis of pancreatitis should not be made solely on the basis of abnormal laboratory values
General Disorders:Very common: infection, hemorrhage (including gastrointestinal* and respiratory tract* and uncommon cases of cerebral hemorrhage*), asthenia, pain (including mouth, bone, and tumor pain), pyrexia, decreased appetite Common: influenza-like illness
Hematologic:Very common: leukopenia, lymphopenia Common: anemia, neutropenia, thrombocytopenia Uncommon: INR abnormal
Hepatobiliary disorders:Rare: drug-induced hepatitis (including hepatic failure and death)
Hypersensitivity:Uncommon: hypersensitivity reactions (including skin reactions and urticaria), anaphylactic reaction
Metabolic and Nutritional:Very common: hypophosphatemia Common: transient increases in transaminases, hypocalcemia, hypokalemia, hyponatremia, hypothyroidism Uncommon: dehydration, transient increases in alkaline phosphatase, increased bilirubin (including jaundice), hyperthyroidism
Musculoskeletal:Very common: arthralgia Common: myalgia, muscle spasms
Nervous System and Psychiatric:Common: depression, dysgeusia Uncommon: tinnitus, reversible posterior leukoencephalopathy*
Renal and Genitourinary:Common: renal failure, proteinuria Rare: nephrotic syndrome
Reproductive:Common: erectile dysfunction Uncommon: gynecomastia
Respiratory:Common: rhinorrhea Uncommon: interstitial lung disease-like events (includes reports of pneumonitis, radiation pneumonitis, acute respiratory distress, interstitial pneumonia, pulmonitis and lung inflammation)
In addition, the following medically significant adverse reactions were uncommon during clinical trials of sorafenib tablets: transient ischemic attack, arrhythmia, and thromboembolism. For these adverse reactions, the causal relationship to sorafenib tablets has not been established.
*adverse reactions may have a life-threatening or fatal outcome.
†reported in 1.9% of patients treated with sorafenib tablets (N= 2276).
6.2 Postmarketing Experience
The following adverse reactions have been identified during postapproval use of sorafenib tablets. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Blood and lymphatic disorders: Thrombotic microangiopathy (TMA)
Dermatologic:Stevens-Johnson syndrome and toxic epidermal necrolysis (TEN)
Hypersensitivity: Angioedema
Musculoskeletal: Rhabdomyolysis, osteonecrosis of the jaw
Respiratory: Interstitial lung disease-like events (which may have a life-threatening or fatal outcome)
Vascular: Arterial (including aortic) aneurysms, dissections, and rupture
7.1 Effect of Other Drugs on Sorafenib Tablets
Strong CYP3A4 Inducers
The concomitant use of sorafenib tablets with rifampin, a strong CYP3A4 inducer decreased the mean AUC of sorafenib, which may decrease the antitumor activity [see Clinical Pharmacology (12.3)]. Avoid concomitant use of sorafenib tablets with strong CYP3A4 inducers, when possible, because these drugs can decrease the systemic exposure to sorafenib.
Neomycin
The concomitant use of sorafenib tablets with neomycin decreased the mean AUC of sorafenib, which may decrease the antitumor activity. Avoid concomitant use of sorafenib tablets with neomycin. The effects of other antibiotics on the pharmacokinetics of sorafenib have not been studied [see Clinical Pharmacology (12.3)].
7.2 Concomitant Use of Warfarin
The concomitant use of sorafenib tablets and warfarin may increase the risk of bleeding or increased the INR. Monitor INR and for clinical bleeding episodes in patients taking warfarin while receiving sorafenib tablets [see Warnings and Precautions (5.6)].
8.1 Pregnancy
Risk Summary
Based on findings from animal studies and its mechanism of action [see Clinical Pharmacology (12.1)], sorafenib tablets may cause fetal harm when administered to a pregnant woman. There are no available data in pregnant women to inform a drug-associated risk. In animal reproduction studies, oral administration of sorafenib to pregnant rats and rabbits during the period of organogenesis resulted in embryo-fetal toxicities at maternal exposures that were significantly lower than human exposures at the recommended dose of 400 mg twice daily (see Data). Advise pregnant women and females of reproductive potential of the potential risk to a fetus.
The background risk of major birth defects and miscarriage for the indicated population is unknown. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Data
Animal Data
In animal reproduction studies, sorafenib was teratogenic and induced embryo-fetal toxicity (including increased post-implantation loss, resorptions, skeletal retardations, and retarded fetal weight) when administered orally to pregnant rats and rabbits during the period of organogenesis. The effects occurred at doses considerably below the recommended human dose of 400 mg twice daily (approximately 500 mg/m2/day on a body surface area basis). Adverse intrauterine development effects were seen at doses >0.2 .mg/kg/day (1.2 mg/m2/day) in rats and ≥0.3 mg/kg/day (≥3.6 mg/m2/day) in rabbits. These doses result in exposures (AUC) that are approximately 0.008 times the AUC in patients at the recommended dose.
8.2 Lactation
Risk Summary
There are no data on the presence of sorafenib or its metabolites in human milk, or its effects on the breast-fed child or on milk production. Sorafenib was present in milk of lactating rats (see Data). Because of the potential for serious adverse reactions in a breastfed child from sorafenib, advise women not to breastfeed during treatment with sorafenib and for 2 weeks after the last dose.
Data
Animal Data
Following administration of radiolabeled sorafenib to lactating Wistar rats, approximately 27% of the radioactivity was secreted into milk. The milk to plasma AUC ratio was approximately 5:1.
8.3 Females and Males of Reproductive Potential
Sorafenib tablets may cause fetal harm when administered to a pregnant woman [see Use in Specific Populations (8.1)].
Pregnancy Testing
Verify the pregnancy status of females of reproductive potential prior to the initiation of sorafenib tablets.
Contraception
Females
Advise females of reproductive potential to use effective contraception during treatment and for 6 months following the last dose of sorafenib tablets.
Males
Based on genotoxicity and findings in animal reproduction studies, advise males with female partners of reproductive potential and pregnant partners to use effective contraception during treatment with sorafenib tablets and for 3 months following the last dose of sorafenib tablets [see Use in Specific Populations (8.1), Nonclinical Toxicology (13.1)].
Infertility
Males
Based on findings in animal studies, sorafenib tablets may impair fertility in males of reproductive potential [see Nonclinical Toxicology (13.1)].
8.4 Pediatric Use
The safety and effectiveness of sorafenib tablets have not been established in pediatric patients.
Juvenile Animal Toxicity Data
Repeat dosing of sorafenib to young and growing dogs resulted in irregular thickening of the femoral growth plate at daily sorafenib doses ≥600 mg/m2 (approximately 0.3 times the AUC at the recommended human dose), hypocellularity of the bone marrow adjoining the growth plate at 200 mg/m2/day (approximately 0.1 times the AUC at the recommended human dose), and alterations of the dentin composition at 600 mg/m2/day. Similar effects were not observed in adult dogs when dosed for 4 weeks or less.
8.5 Geriatric Use
In total, 59% of HCC patients treated with sorafenib tablets were age 65 years or older and 19% were 75 and older. No differences in safety or efficacy were observed between older and younger patients, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
OVERDOSAGE
The adverse reactions observed at a dose of 800 mg twice daily (2 times the recommended dose) were primarily diarrhea and dermatologic. No information is available on symptoms of acute overdose in animals because of the saturation of absorption in oral acute toxicity studies conducted in animals.
In cases of suspected overdose, withhold sorafenib tablets and institute supportive care.
DESCRIPTION
Sorafenib, a kinase inhibitor, is the tosylate salt of sorafenib. Sorafenib tosylate has the chemical name 4-(4-{3-[4-Chloro-3-(trifluoromethyl)phenyl]ureido}phenoxy)N2-methylpyridine-2-carboxamide 4 methylbenzenesulfonate. The molecular formula of sorafenib tosylate is C21H16ClF3N4O3 x C7H8O3S and the molecular weight of sorafenib tosylate is 637.0 g/mole. Its structural
formula is:
:
Sorafenib tosylate is a white to yellowish or brownish solid. Sorafenib tosylate is practically insoluble in aqueous media, slightly soluble in ethanol and soluble in PEG 400.
Sorafenib Tablets, USP for oral use is supplied as film-coated tablets containing 200 mg sorafenib equivalent to 274 mg sorafenib tosylate and the following inactive ingredients: croscarmellose sodium, ferric oxide red, hypromellose, magnesium stearate, microcrystalline cellulose, polyethylene glycol, sodium lauryl sulphate, and titanium dioxide.
FDA approved dissolution test specifications differ from USP.
12.1 Mechanism of Action
Sorafenib is a kinase inhibitor that decreases tumor cell proliferation in vitro.
Sorafenib was shown to inhibit multiple intracellular (c-CRAF, BRAF and mutant BRAF) and cell surface kinases (KIT, FLT- 3, RET, RET/PTC, VEGFR-1, VEGFR- 2, VEGFR- 3, and PDGFR-ß). Several of these kinases are thought to be involved in tumor cell signaling, angiogenesis and apoptosis. Sorafenib inhibited tumor growth of HCC and DTC human tumor xenografts in immunocompromised mice. Reductions in tumor angiogenesis were seen in models of HCC upon sorafenib treatment, and increases in tumor apoptosis were observed in models of HCC and DTC.
12.2 Pharmacodynamics
Cardiac Electrophysiology
The effect of sorafenib tablets 400 mg twice daily on the QTc interval was evaluated in a multi-center, open- label, non-randomized trial in 53 patients with advanced cancer. No large changes in the mean QTc intervals (that is, >20 ms) from baseline were detected in the trial. After one 28-day treatment cycle, the largest mean QTc interval change of 8.5 ms (upper bound of two-sided 90% confidence interval, 13.3 ms) was observed at 6 hours post-dose on day 1 of cycle 2 [see Warnings and Precautions (5.9), Drug Interactions (7.3)].
12.3 Pharmacokinetics
Multiple doses of sorafenib tablets for 7 days resulted in a 2.5- to 7-fold accumulation compared to a single dose. Steady-state plasma sorafenib concentrations were achieved within 7 days, with a peak-to-trough ratio of mean concentrations of less than 2.
The steady-state concentrations of sorafenib following administration of sorafenib tablets 400 mg twice daily were evaluated in DTC and HCC patients. Patients with DTC have mean steady-state concentrations that are 1.8-fold higher than patients with HCC. The reason for increased sorafenib concentrations in DTC patients is unknown.
Mean C maxand AUC increased less than proportionally beyond oral doses of 400 mg administered twice daily.
Absorption
After administration of sorafenib tablets, the mean relative bioavailability was 38–49% when compared to an oral solution. Following oral administration, sorafenib reached peak plasma levels in approximately 3 hours.
Effects of Food
With a moderate-fat meal (30% fat; 700 calories), bioavailability was similar to that in the fasted state. With a high-fat meal (50% fat; 900 calories), bioavailability was reduced by 29% compared to that in the fasted state.
Distribution
In vitro binding of sorafenib to human plasma proteins was 99.5%.
Elimination
The mean elimination half-life of sorafenib was approximately 25 to 48 hours.
Metabolism
Sorafenib undergoes oxidative metabolism by hepatic CYP3A4, as well as glucuronidation by UGT1A9.
Excretion
Sorafenib accounted for approximately 70–85% of the circulating analytes in plasma at steady-state. Eight metabolites of sorafenib have been identified, of which 5 have been detected in plasma. The main circulating metabolite of sorafenib, the pyridine N-oxide that comprises approximately 9–16% of circulating analytes at steady-state, showed in vitropotency similar to that of sorafenib.
Following oral administration of a 100 mg dose of a solution formulation of sorafenib, 96% of the dose was recovered within 14 days, with 77% of the dose excreted in feces and 19% of the dose excreted in urine as glucuronidated metabolites. Unchanged sorafenib, accounting for 51% of the dose, was found in feces but not in urine.
Specific Populations
A study of the pharmacokinetics of sorafenib indicated that the mean AUC of sorafenib in Asians (N=78) was 30% lower than in Whites (N=40). Sex and age do not have a clinically meaningful effect on the pharmacokinetics of sorafenib.
Patients with Renal Impairment
Mild (CLcr 50-80 mL/min), moderate (CLcr 30 - <50 mL/min), and severe (CLcr <30 mL/min) renal impairment do not affect the pharmacokinetics of sorafenib [seeUse in Specific Populations (8.6)].
Patients with Hepatic Impairment
Mild (Child-Pugh A) and moderate (Child-Pugh B) hepatic impairment do not affect the pharmacokinetics of sorafenib [see Use in Specific Populations (8.7)].
Drug Interactions Studies
Effect of Strong CYP3A4 Inhibitors on Sorafenib: Ketoconazole, a strong inhibitor of CYP3A4 and P- glycoprotein, administered at a dose of 400 mg once daily for 7 days did not alter the mean AUC of a single oral dose of sorafenib tablets 50 mg in healthy subjects.
Effect of Strong CYP3A4 Inducers on Sorafenib: Concomitant use of sorafenib tablets with rifampin administered at a dose of 600 mg once daily for 5 days with a single oral dose of sorafenib tablets 400 mg in healthy volunteers resulted in a 37% decrease in the mean AUC of sorafenib.
Effect of Neomycin on Sorafenib:Neomycin administered as an oral dose of 1 g three times daily for 5 days decreased the mean AUC of sorafenib by 54% in healthy subjects administered a single oral dose of sorafenib tablets 400 mg.
Effect of Sorafenib on Other Drugs:Sorafenib tablets 400 mg twice daily for 28 days did not increase the systemic exposure of concomitantly administered midazolam (CYP3A4 substrate), dextromethorphan (CYP2D6 substrate), and omeprazole (CYP2C19 substrate) [see Clinical Pharmacology (12.3)].
Drugs that Increase Gastric pH:The aqueous solubility of sorafenib is pH dependent, with higher pH resulting in lower solubility. However, omeprazole, a proton pump inhibitor, administered at a dose of 40 mg once daily for 5 days, did not result in a clinically meaningful change in sorafenib single dose exposure.
In Vitro Studies
Sorafenib competitively inhibited CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6, and CYP3A4 in vitro. However, sorafenib tablets 400 mg twice daily for 28 days with substrates of CYP3A4, CYP2D6 and CYP2C19 did not increase the systemic exposure of these substrates [see Drug Interactions (7.3)].
Sorafenib did not increase CYP1A2 and CYP3A4 activities, suggesting that sorafenib is unlikely to induce CYP1A2 or CYP3A4 in humans.
Sorafenib inhibits glucuronidation by UGT1A1 and UGT1A9 in vitro. Sorafenib tablets could increase the systemic exposure of concomitantly administered drugs that are UGT1A1 or UGT1A9 substrates.
Sorafenib inhibited P-glycoprotein in vitro. Sorafenib tablets could increase the concentrations of concomitantly administered drugs that are P-glycoprotein substrates.
NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity studies have not been performed with sorafenib. Sorafenib was clastogenic when tested in an in vitromammalian cell assay (Chinese hamster ovary) in the presence of metabolic activation. Sorafenib was not mutagenic in the in vitroAmes bacterial cell assay or clastogenic in an in vivomouse micronucleus assay. One intermediate in the manufacturing process, which is also present in the final drug substance (<0.15%), was positive for mutagenesis in an in vitrobacterial cell assay (Ames test) when tested independently.
No specific studies with sorafenib have been conducted in animals to evaluate the effect on fertility. However, results from the repeat-dose toxicity studies suggest there is a potential for sorafenib to impair reproductive function and fertility. Multiple adverse effects were observed in male and female reproductive organs, with the rat being more susceptible than mice or dogs. Typical changes in rats consisted of testicular atrophy or degeneration, degeneration of epididymis, prostate, and seminal vesicles, central necrosis of the corpora lutea and arrested follicular development. Sorafenib-related effects on the reproductive organs of rats were manifested at daily oral doses ≥ 5 mg/kg (30 mg/m2 ). This dose results in an exposure (AUC) that is approximately 0.5 times the AUC in patients at the recommended human dose. Dogs showed tubular degeneration in the testes at 30 mg/kg/day (600 mg/m2/day). This dose results in an exposure that is approximately 0.3 times the AUC at the recommended human dose. Oligospermia was observed in dogs at 60 mg/kg/day (1200 mg/m2/day) of sorafenib.
CLINICAL STUDIES
14.1 Hepatocellular Carcinoma
The SHARP (HCC) study (NCT00105443) was an international, multicenter, randomized, double blind, placebo-controlled trial in patients with unresectable hepatocellular carcinoma. Overall survival was the primary endpoint. A total of 602 patients were randomized; 299 to sorafenib tablets 400 mg twice daily and 303 to matching placebo. All 602 randomized subjects were included in the ITT population for the efficacy analyses.
Demographics and baseline disease characteristics were similar between the sorafenib tablets and placebo arms with regard to age, gender, race, performance status, etiology (including hepatitis B, hepatitis C and alcoholic liver disease), TNM stage (stage I: <1% vs. <1%; stage II: 10.4% vs. 8.3%; stage III: 37.8% vs. 43.6%; stage IV: 50.8% vs. 46.9%), absence of both macroscopic vascular invasion and extrahepatic tumor spread (30.1% vs. 30.0%), and Barcelona Clinic Liver Cancer stage (stage B: 18.1% vs. 16.8%; stage C: 81.6% vs. 83.2%; stage D: <1% vs. 0%). Liver impairment by Child-Pugh score was comparable between the sorafenib tablets and placebo arms (Class A: 95% vs. 98%; B: 5% vs. 2%). Only one patient with Child-Pugh class C was entered. Prior treatments included surgical resection procedures (19.1% vs. 20.5%), locoregional therapies (including radiofrequency ablation,
percutaneous ethanol injection and transarterial chemoembolization; 38.8% vs. 40.6%), radiotherapy (4.3% vs. 5.0%) and systemic therapy (3.0% vs. 5.0%).
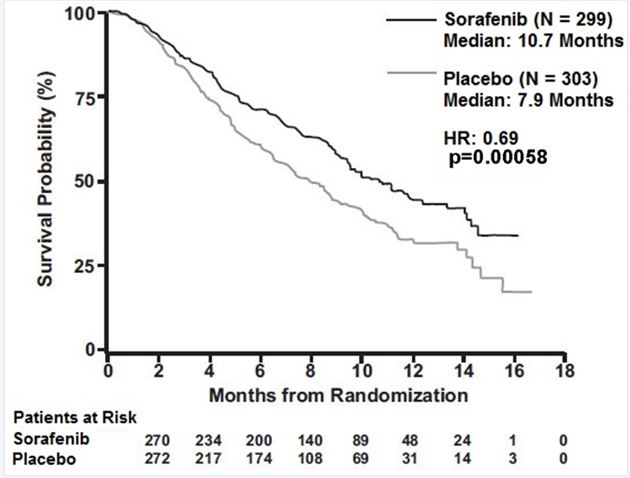
The trial was stopped for efficacy following a pre-specified second interim analysis for survival showing a statistically significant advantage for sorafenib tablets over placebo for overall survival (HR: 0.69, p= 0.00058) (see Table 10 and Figure 1). This advantage was consistent across all subsets analyzed.
Final analysis of time to tumor progression (TTP) based on data from an earlier time point (by independent radiologic review) also was significantly longer in the sorafenib tablets arm (HR: 0.58, p=0.000007) (see Table 10).
Table 10: Efficacy Results from SHARP (HCC)
|
Efficacy Parameter |
SorafenibTablets (N=299) |
Placebo (N=303) |
|
Overall Survival |
||
|
Number of Events |
143 |
178 |
|
Median, months |
10.7 |
7.9 |
|
(95% CI) |
(9.4, 13.3) |
(6.8, 9.1) |
|
Hazard Ratio1 (95% CI) |
0.69 (0.55, 0.87) |
|
|
P-value (log-rank test2 ) |
0.00058 |
|
|
Time to Progression3 |
||
|
Number of Events |
107 |
156 |
|
Median, months |
5.5 |
2.8 |
|
(95% CI) |
(4.1, 6.9) |
(2.7, 3.9) |
|
Hazard Ratio1 (95% CI) |
0.58 (0.45, 0.74) |
|
|
P-value (log-rank test2 ) |
0.000007 |
|
CI=Confidence interval
1 Hazard ratio, sorafenib/placebo, stratified Cox model
2 Stratified log rank (for the interim analysis of survival, the stopping boundary one-sided alpha = 0.0077)
3 The time-to-progression (TTP) analysis, based on independent radiologic review, was based on data from an earlier time point than the survival analysis
Figure 1: Kaplan-Meier Curve of Overall Survival in SHARP (HCC) (Intent-to-Treat Population)
14.3 Differentiated Thyroid Carcinoma
The safety and effectiveness of sorafenib tablets was evaluated in a multicenter, randomized (1:1), double-blind, placebo-controlled trial (DECISION; NCT00984282) conducted in 417 patients with locally recurrent or metastatic, progressive differentiated thyroid carcinoma (DTC) refractory to radioactive iodine (RAI) treatment. Randomization was stratified by age (< 60 years versus ≥ 60 years) and geographical region (North America, Europe, and Asia). All 417 subjects were included in the ITT population for the efficacy analyses.
All patients were required to have actively progressing disease defined as progression within 14 months of enrollment. RAI-refractory disease was defined based on four criteria that were not mutually exclusive. All RAI treatments and diagnostic scans were to be performed under conditions of a low iodine diet and adequate TSH stimulation. Following are the RAI-refractory criteria and the proportion of patients in the study that met each one: a target lesion with no iodine uptake on RAI scan (68%); tumors with iodine uptake and progression after RAI treatment within 16 months of enrollment (12%); tumors with iodine uptake and multiple RAI treatments with the last treatment greater than 16 months prior to enrollment, and disease progression after each of two RAI treatments administered within 16 months of each other (7%); cumulative RAI dose ≥ 600 mCi administered (34%). The major efficacy outcome measure was progression-free survival (PFS) as determined by a blinded, independent radiological review using a modified Response Evaluation Criteria in Solid Tumors v. 1.0 (RECIST). RECIST was modified by inclusion of clinical progression of bone lesions based on the need for external beam radiation (4.4% of progression events). Additional efficacy outcomes measures included overall survival (OS), tumor response rate, and duration of response.
Patients were randomized to receive sorafenib tablets 400 mg twice daily (n=207) or placebo (n=210). Of the 417 patients randomized, 48% were male, the median age was 63 years, 61% were 60 years or older, 60% were white, 62% had an ECOG performance status of 0, and 99% had undergone thyroidectomy. The histological diagnoses were papillary carcinoma in 57%, follicular carcinoma (including Hürthle cell) in 25%, and poorly differentiated carcinoma in 10%, and other in 8% of the study population. Metastases were present in 96% of the patients: lungs in 86%, lymph nodes in 51%, and bone in 27%. The median cumulative RAI activity administered prior to study entry was 400 mCi.
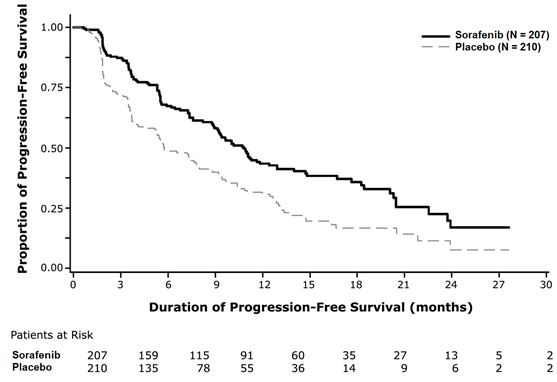
A statistically significant prolongation of PFS was demonstrated for sorafenib tablets -treated patients compared to those receiving placebo (Figure 3); no statistically significant difference was seen in the final overall survival (OS) analysis (Table 12). Crossover to open label sorafenib tablets occurred in 161 (77%) patients randomized to placebo after investigator-determined disease progression.
Table 12: Efficacy Results from DECISION in Differentiated Thyroid Carcinoma
|
Sorafenib Tablets N = 207 |
Placebo N = 210 |
|
|
Progression-free Survival1 |
||
|
Number of Deaths or Progression |
113 (55%) |
136 (65%) |
|
Median PFS in Months (95% CI) |
10.8 (9.1, 12.9) |
5.8 ( 5.3, 7.8) |
|
Hazard Ratio (95% CI) |
0.59 (0.46, 0.76) |
|
|
P-value 2 |
< 0.001 |
|
|
Overall Survival3 |
||
|
Number of Deaths |
103 (49.8%) |
109 (51.9%) |
|
Median OS in Months (95% CI) |
42.8 (34.6, 52.6) |
39.4 (32.7, 51.4) |
|
Hazard Ratio (95% CI) |
0.92 (0.71, 1.21) |
|
|
P-value2 |
0.570 |
|
|
Objective Response |
||
|
Number of Objective Responders 4 |
24 (12%) |
1 (0.5%) |
|
(95% CI) |
(7.6%, 16.8%) |
(0.01%, 2.7%) |
|
Median Duration of Response in Months (95% CI) |
10.2 (7.4, 16.6) |
NE |
1 Independent radiological review
2 Two-sided log-rank test stratified by age (< 60 years, ≥ 60 years) and geographic region (North America, Europe, Asia)
3 Conducted after 212 events, which occurred 36 months after the primary PFS analysis
4 All objective responses were partial responses
NR = Not Reached, CI = Confidence interval, NE = Not Estimable
Figure 3: Kaplan-Meier Curve of Progression-Free Survival in DECISION (DTC)
HOW SUPPLIED/STORAGE AND HANDLING
Sorafenib Tablets, USP are supplied as round, pink, film-coated tablets, debossed with “YB” on one side and “201” on the other side.
Bottles of 120 tablets
Bottles of 60 tablets
Store at 20°C to 25°C (68°F to 77°F); excursions permitted to 15°C to 30°C (59°F to 86°F) [see USP controlled room temperature]. Store in a dry place.
Patient Counseling Information
Advise the patient to read FDA-approved patient labeling (Patient Information).
Cardiovascular Events
Discuss with patients that cardiac ischemia and/or infarction and congestive heart failure, have been reported during sorafenib tablets treatment, and that they should immediately report any episodes of chest pain or other symptoms of cardiac ischemia or congestive heart failure [see Warnings and Precautions (5.1)].
Bleeding
Inform patients that sorafenib tablets can increase the risk of bleeding and that they should promptly report any episodes of bleeding [see Warnings and Precautions (5.2)].
Inform patients that bleeding or elevations in the International Normalized Ratio (INR) have been reported in some patients taking warfarin while on sorafenib tablets and that their INR should be monitored regularly [see Warnings and Precautions (5.6)].
Hypertension
Inform patients that hypertension can develop during sorafenib tablets treatment, especially during the first six weeks of therapy, and that blood pressure should be monitored regularly during treatment [see Warnings and Precautions (5.3)].
Skin Reactions
Advise patients of the possible occurrence of hand-foot skin reaction and rash during sorafenib tablets treatment and appropriate countermeasures [see Warnings and Precautions (5.4)].
Gastrointestinal Perforation
Advise patients that cases of gastrointestinal perforation have been reported in patients taking sorafenib tablets [see Warnings and Precautions (5.5)].
Risk of Impaired Wound Healing
Advise patients that sorafenib tablets may impair wound healing. Advise patients to inform their healthcare provider of any planned surgical procedure [see Warnings and Precautions (5.7)].
QT Interval Prolongation
Inform patients with a history of prolonged QT interval that sorafenib tablets can worsen the condition [see Warnings and Precautions (5.9) and Clinical Pharmacology (12.2)].
Drug-Induced Liver Injury
Inform patients that sorafenib tablets can cause hepatitis which may result in hepatic failure and death. Advise patients that liver function tests should be monitored regularly during treatment and to report signs and symptoms of hepatitis [see Warnings and Precautions (5.10)].
Embryo-Fetal Toxicity
Advise females to inform their healthcare provider if they are pregnant or become pregnant. Inform female patients of the risk to a fetus and potential loss of pregnancy [see Use in Specific Populations (8.1)]. Advise females of reproductive potential to use effective contraception during treatment with sorafenib tablets and for 6 months after the last dose. Advise male patients with female partners of reproductive potential or who are pregnant to use effective contraception during treatment with sorafenib tablets and for 3 months after receiving the last dose of sorafenib tablets [see Warnings and Precautions (5.11), Use in Specific Populations (8.1, 8.3)].
Lactation
Advise patients not to breastfeed while taking sorafenib tablets and for 2 weeks after receiving the last dose of sorafenib tablets [see Use in Specific Populations (8.2)].
Missed Doses
Instruct patients that if a dose of sorafenib tablets is missed, the next dose should be taken at the regularly scheduled time, and not double the dose. Instruct patients to contact their healthcare provider immediately if they take too much sorafenib tablets.
![]()
Distributed by: TWi Pharmaceuticals USA, Inc.
Paramus, NJ 07652
Manufactured by: Yabao Pharmaceutical Co., Ltd. Beijing
Beijing, China 101111
Manufactured by: TWi Pharmaceuticals, Inc.
Taoyuan City, 320023, Taiwan
| SORAFENIB
sorafenib tablet, film coated |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| Labeler - Bora Pharmaceutical Laboratories Inc. (656139511) |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Bora Pharmaceutical Laboratories Inc. | 656139511 | pack(43826-066) , label(43826-066) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| TWi Pharmaceuticals, Inc. Zhongli Plant | 658863394 | manufacture(43826-066) | |