Buprenorphine by AvPAK BUPRENORPHINE tablet
Buprenorphine by
Drug Labeling and Warnings
Buprenorphine by is a Prescription medication manufactured, distributed, or labeled by AvPAK. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
Buprenorphine Tablet CIII
Rx only
These highlights do not include all the information needed to use BUPRENORPHINE SUBLINGUAL TABLETS safely and effectively. See full prescribing information for BUPRENORPHINE SUBLINGUAL TABLETS.
Initial U.S. Approval: 1981INDICATIONS AND USAGE
Buprenorphine sublingual tablet, contains buprenorphine, a partial opioid agonist, and is indicated for the treatment of opioid dependence and is preferred for induction. (1)
Buprenorphine sublingual tablet should be used as part of a complete treatment plan that includes counseling and psychosocial support. (1)DOSAGE AND ADMINISTRATION
- Administer buprenorphine sublingual tablet sublingually as a single daily dose. (2.1)
- Strongly consider prescribing naloxone at the time buprenorphine sublingual tablet is initiated or renewed because patients being treated for opioid use disorder have the potential for relapse, putting them at risk for opioid overdose. (2.2)
- To avoid precipitating withdrawal, induction with buprenorphine sublingual tablet should be undertaken when objective and clear signs of withdrawal are evident. (2.3)
- Buprenorphine and naloxone sublingual film or buprenorphine and naloxone sublingual tablet is generally initiated after two days of buprenorphine sublingual tablet titration. (2.4)
- Administer buprenorphine sublingual tablets as directed in the Full Prescribing Information. (2.3, 2.4, 2.5)
- Buprenorphine sublingual tablet must be administered whole. Do not cut, chew, or swallow buprenorphine sublingual tablets. (2.5)
- When discontinuing treatment, gradually taper to avoid signs and symptoms of withdrawal. (2.9)
DOSAGE FORMS AND STRENGTHS
Sublingual tablet: 2 mg buprenorphine and 8 mg buprenorphine. ( 3)
CONTRAINDICATIONS
Hypersensitivity to buprenorphine. ( 4)
WARNINGS AND PRECAUTIONS
- Addiction, Abuse, and Misuse:Buprenorphine can be abused in a similar manner to other opioids. Monitor patients for conditions indicative of diversion or progression of opioid dependence and addictive behaviors. Multiple refills should not be prescribed early in treatment or without appropriate patient follow-up visits. (5.1)
- Respiratory Depression:Life-threatening respiratory depression and death have occurred in association with buprenorphine use. Warn patients of the potential danger of self-administration of benzodiazepines or other CNS depressants while under treatment with buprenorphine sublingual tablets. (5.2,5.3)
- Unintentional Pediatric Exposure: Store buprenorphine sublingual tablet safely out of the sight and reach of children. Buprenorphine can cause severe, possibly fatal, respiratory depression in children. (5.4)
- Neonatal Opioid Withdrawal Syndrome: Neonatal opioid withdrawal syndrome (NOWS) is an expected and treatable outcome of prolonged use of opioids during pregnancy. (5.5)
- Adrenal Insufficiency:If diagnosed, treat with physiologic replacement of corticosteroids, and wean patient off of the opioid. (5.6)
- Risk of Opioid Withdrawal with Abrupt Discontinuation: If treatment is temporarily interrupted or discontinued, monitor patients for withdrawal and treat appropriately. (5.7)
- Risk of Hepatitis, Hepatic Events: Monitor liver function tests prior to initiation and during treatment and evaluate suspected hepatic events. (5.8)
- Precipitation of Opioid Withdrawal Signs and Symptoms: An opioid withdrawal syndrome is likely to occur with parenteral misuse of buprenorphine sublingual tablet by individuals physically dependent on full opioid agonists, or by sublingual administration before the agonist effects of other opioids have subsided. (5.10)
- Risk of Overdose in Opioid-Naïve Patients:Buprenorphine sublingual tablet is NOT appropriate as an analgesic. There have been reported deaths of opioid naïve individuals who received a 2 mg sublingual dose of buprenorphine. (5.11)
ADVERSE REACTIONS
Adverse events commonly observed with administration of buprenorphine are oral hypoesthesia, glossodynia, oral mucosal erythema, headache, nausea, vomiting, hyperhidrosis, constipation, signs and symptoms of withdrawal, insomnia, pain, and peripheral edema. ( 6)
To report SUSPECTED ADVERSE REACTIONS, contact AvKARE at 1-855-361-3993 or FDA at 1-800-FDA-1088, or www.fda.gov/medwatch.DRUG INTERACTIONS
Benzodiazepines: Use caution in prescribing buprenorphine sublingual tablet for patients receiving benzodiazepines or other CNS depressants and warn patients against concomitant self-administration/misuse. ( 7)
CYP3A4 Inhibitors and Inducers: Monitor patients starting or ending CYP3A4 inhibitors or inducers for potential over- or under- dosing. ( 7)
Antiretrovirals: Patients who are on chronic buprenorphine treatment should have their dose monitored if NNRTIs are added to their treatment regimen. Monitor patients taking buprenorphine and atazanavir with and without ritonavir, and reduce dose of buprenorphine if warranted. ( 7)
Serotonergic Drugs: Concomitant use may result in serotonin syndrome. Discontinue buprenorphine sublingual tablets if serotonin syndrome is suspected. ( 7)USE IN SPECIFIC POPULATIONS
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide.
Revised: 3/2024
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Important Dosage and Administration Instructions
2.2 Patient Access to Naloxone for the Emergency Treatment of Opioid Overdose
2.3 Induction
2.4 Maintenance
2.5 Method of Administration
2.6 Clinical Supervision
2.7 Patients With Severe Hepatic Impairment
2.8 Unstable Patients
2.9 Discontinuing Treatment
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Addiction, Abuse, and Misuse
5.2 Risk of Life-Threatening Respiratory and Central Nervous System (CNS) Depression
5.3 Managing Risks from Concomitant Use of Benzodiazepines or Other CNS Depressants
5.4 Unintentional Pediatric Exposure
5.5 Neonatal Opioid Withdrawal Syndrome
5.6 Adrenal Insufficiency
5.7 Risk of Opioid Withdrawal with Abrupt Discontinuation
5.8 Risk of Hepatitis, Hepatic Events
5.9 Hypersensitivity Reactions
5.10 Precipitation of Opioid Withdrawal Signs and Symptoms
5.11 Risk of Overdose in Opioid Naïve Patients
5.12 Use in Patients with Impaired Hepatic Function
5.13 Dental Adverse Events
5.14 QTc Prolongation
5.15 Impairment of Ability to Drive or Operate Machinery
5.16 Orthostatic Hypotension
5.17 Elevation of Cerebrospinal Fluid Pressure
5.18 Elevation of Intracholedochal Pressure
5.19 Effects in Acute Abdominal Conditions
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
6.2 Postmarketing Experience
7 DRUG INTERACTIONS
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.3 Females and Males of Reproductive Potential
8.4 Pediatric Use
8.5 Geriatric Use
8.6 Hepatic Impairment
8.7 Renal Impairment
9 DRUG ABUSE AND DEPENDENCE
9.1 Controlled Substance
9.2 Abuse
9.3 Dependence
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
16 HOW SUPPLIED / STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
Storage and Disposal
Safe Use
- * Sections or subsections omitted from the full prescribing information are not listed.
- 1 INDICATIONS AND USAGE
-
2 DOSAGE AND ADMINISTRATION
2.1 Important Dosage and Administration Instructions
Buprenorphine sublingual tablet is administered sublingually as a single daily dose. Buprenorphine sublingual tablet does not contain naloxone and is preferred for use only during induction. Following induction, buprenorphine and naloxone sublingual film or buprenorphine and naloxone sublingual tablet is preferred due to the presence of naloxone when clinical use includes unsupervised administration. The use of buprenorphine sublingual tablet for unsupervised administration should be limited to those patients who cannot tolerate buprenorphine and naloxone sublingual film or buprenorphine and naloxone sublingual tablet; for example, those patients who have been shown to be hypersensitive to naloxone.
Medication should be prescribed in consideration of the frequency of visits. Provision of multiple refills is not advised early in treatment or without appropriate patient follow-up visits.
2.2 Patient Access to Naloxone for the Emergency Treatment of Opioid Overdose
Discuss the availability of naloxone for the emergency treatment of opioid overdose with the patient and caregiver. Because patients being treated for opioid use disorder have the potential for relapse, putting them at risk for opioid overdose, strongly consider prescribing naloxone for the emergency treatment of opioid overdose, both when initiating and renewing treatment with buprenorphine sublingual tablet.
Also consider prescribing naloxone if the patient has household members (including children) or other close contacts at risk for accidental ingestion or opioid overdose [see Warnings and Precautions (5.2)]. Advise patients and caregivers that naloxone may also be administered for a known or suspected overdose with buprenorphine sublingual tablet itself. Higher than normal doses and repeated administration of naloxone may be necessary due to the long duration of action of buprenorphine sublingual tablet and its affinity for the mu-opioid receptor [see Overdosage (10)].
Inform patients and caregivers of their options for obtaining naloxone as permitted by individual state naloxone dispensing and prescribing requirements or guidelines (e.g., by prescription, directly from a pharmacist, or as part of a community-based program) [see Patient Counseling Information (17)].
2.3 Induction
Prior to induction, consideration should be given to the type of opioid dependence (i.e., long- or short-acting opioid products), the time since last opioid use, and the degree or level of opioid dependence.
Patients dependent on heroin or other short-acting opioid products:
At treatment initiation, the first dose of buprenorphine sublingual tablet should be administered only when objective and clear signs of moderate opioid withdrawal appear, and not less than 4 hours after the patient last used an opioid.
It is recommended that an adequate treatment dose, titrated to clinical effectiveness, should be achieved as rapidly as possible. The dosing on the initial day of treatment may be given in 2 mg to 4 mg increments if preferred. In some studies, gradual induction over several days led to a high rate of dropout of buprenorphine patients during the induction period.
In a one-month study, patients received 8 mg of buprenorphine sublingual tablet on Day 1 and 16 mg buprenorphine sublingual tablet on Day 2. From Day 3 onward, patients received either buprenorphine and naloxone sublingual tablet or buprenorphine sublingual tablet at the same buprenorphine dose as Day 2 based on their assigned treatment. Induction in the studies of buprenorphine solution was accomplished over 3 to 4 days, depending on the target dose.
Patients dependent on methadone or other long-acting opioid products:
Patients dependent upon methadone or other long-acting opioid products may be more susceptible to precipitated and prolonged withdrawal during induction than those on short-acting opioid products; therefore, the first dose of buprenorphine sublingual tablet should only be administered when objective and clear signs of moderate opioid withdrawal appear, and generally not less than 24 hours after the patient last used a long-acting opioid product.
There is little controlled experience with the transfer of methadone-maintained patients to buprenorphine. Available evidence suggests that withdrawal signs and symptoms are possible during induction onto buprenorphine. Withdrawal appears more likely in patients maintained on higher doses of methadone (>30 mg) and when the first buprenorphine dose is administered shortly after the last methadone dose.
2.4 Maintenance
- Buprenorphine and naloxone sublingual tablet is preferred for maintenance treatment.
- Where buprenorphine sublingual tablet is used in maintenance in patients who cannot tolerate the presence of naloxone, the dosage of buprenorphine sublingual tablets should be progressively adjusted in increments/decrements of 2 mg or 4 mg buprenorphine to a level that holds the patient in treatment and suppresses opioid withdrawal signs and symptoms.
- After treatment induction and stabilization, the maintenance dose of buprenorphine sublingual tablet is generally in the range of 4 mg to 24 mg buprenorphine per day depending on the individual patient. The recommended target dosage of buprenorphine sublingual tablet is 16 mg as a single daily dose. Dosages higher than 24 mg have not been demonstrated to provide any clinical advantage.
- When determining the prescription quantity for unsupervised administration, consider the patient’s level of stability, the security of his or her home situation, and other factors likely to affect the ability to manage supplies of take-home medication.
- There is no maximum recommended duration of maintenance treatment. Patients may require treatment indefinitely and should continue for as long as patients are benefiting and the use of buprenorphine sublingual tablet contributes to the intended treatment goals.
2.5 Method of Administration
Buprenorphine sublingual tablet must be administered whole. Do not cut, chew, or swallow buprenorphine sublingual tablet. Advise patients not to eat or drink anything until the tablet is completely dissolved.
Buprenorphine sublingual tablet should be placed under the tongue until it is dissolved. For doses requiring the use of more than two tablets, patients are advised to either place all the tablets at once or alternatively (if they cannot fit in more than two tablets comfortably), place two tablets at a time under the tongue. Either way, the patients should continue to hold the tablets under the tongue until they dissolve; swallowing the tablets reduces the bioavailability of the drug. To ensure consistency in bioavailability, patients should follow the same manner of dosing with continued use of the product.Proper administration technique should be demonstrated to the patient.
Advise patients to do the following after the product has completely dissolved in the oral mucosa: take a sip of water, swish gently around the teeth and gums, and swallow. Advise patients to wait for at least one hour after taking buprenorphine sublingual tablet before brushing teeth [see Warnings and Precautions (5.13), Postmarketing Experience (6.2), Information for Patients (17), and the Medication Guide].
2.6 Clinical Supervision
Treatment should be initiated with supervised administration, progressing to unsupervised administration as the patient’s clinical stability permits. The use of buprenorphine sublingual tablets for unsupervised administration should be limited to those patients who cannot tolerate buprenorphine and naloxone sublingual tablet, for example those patients with known hypersensitivity to naloxone. Buprenorphine and naloxone sublingual tablets and buprenorphine sublingual tablets are both subject to diversion and abuse. When determining the prescription quantity for unsupervised administration, consider the patient’s level of stability, the security of his or her home situation, and other factors likely to affect the ability of the patient to manage supplies of take-home medication.
Ideally, patients should be seen at reasonable intervals (e.g., at least weekly during the first month of treatment) based upon the individual circumstances of the patient. Medication should be prescribed in consideration of the frequency of visits. Provision of multiple refills is not advised early in treatment or without appropriate patient follow-up visits. Periodic assessment is necessary to determine compliance with the dosing regimen, effectiveness of the treatment plan, and overall patient progress.
Once a stable dosage has been achieved and patient assessment (e.g., urine drug screening) does not indicate illicit drug use, less frequent follow-up visits may be appropriate. A once-monthly visit schedule may be reasonable for patients on a stable dosage of medication who are making progress toward their treatment objectives. Continuation or modification of pharmacotherapy should be based on the healthcare provider’s evaluation of treatment outcomes and objectives such as:
1. Absence of medication toxicity.
2. Absence of medical or behavioral adverse effects.
3. Responsible handling of medications by the patient.
4. Patient’s compliance with all elements of the treatment plan (including recovery-oriented activities, psychotherapy, and/or other psychosocial modalities).
5. Abstinence from illicit drug use (including problematic alcohol and/or benzodiazepine use).
If treatment goals are not being achieved, the healthcare provider should re-evaluate the appropriateness of continuing the current treatment.
2.7 Patients With Severe Hepatic Impairment
Consider reducing the starting and titration incremental dose by half and monitor for signs and symptoms of toxicity or overdose caused by increased levels of buprenorphine.
2.8 Unstable Patients
Healthcare providers will need to decide when they cannot appropriately provide further management for particular patients. For example, some patients may be abusing or dependent on various drugs, or unresponsive to psychosocial intervention such that the healthcare provider does not feel that he/she has the expertise to manage the patient. In such cases, the healthcare provider may want to assess whether to refer the patient to a specialist or more intensive behavioral treatment environment. Decisions should be based on a treatment plan established and agreed upon with the patient at the beginning of treatment.
Patients who continue to misuse, abuse, or divert buprenorphine products or other opioids should be provided with, or referred to, more intensive and structured treatment.
2.9 Discontinuing Treatment
The decision to discontinue therapy with buprenorphine and naloxone sublingual tablets or buprenorphine sublingual tablets after a period of maintenance should be made as part of a comprehensive treatment plan. Advise patients of the potential to relapse to illicit drug use following discontinuation of opioid agonist/partial agonist medication-assisted treatment. Taper patients to reduce the occurrence of withdrawal signs and symptoms [see Warnings and Precautions (5.7)].
- 3 DOSAGE FORMS AND STRENGTHS
- 4 CONTRAINDICATIONS
-
5 WARNINGS AND PRECAUTIONS
5.1 Addiction, Abuse, and Misuse
Buprenorphine sublingual tablets contain buprenorphine, a Schedule III controlled substance that can be abused in a manner similar to other opioids, legal or illicit. Prescribe and dispense buprenorphine with appropriate precautions to minimize risk of misuse, abuse, or diversion, and ensure appropriate protection from theft, including in the home. Clinical monitoring appropriate to the patient’s level of stability is essential. Multiple refills should not be prescribed early in treatment or without appropriate patient follow-up visits [see Drug Abuse and Dependence (9.2)].
5.2 Risk of Life-Threatening Respiratory and Central Nervous System (CNS) Depression
Buprenorphine has been associated with life-threating respiratory depression and death. Many, but not all, postmarketing reports regarding coma and death involved misuses by self-injection or were associated with the concomitant use of benzodiazepines or other CNS depressants, including alcohol. Warn patients of the potential danger of self-administration of benzodiazepines or other CNS depressants while under treatment with buprenorphine sublingual tablets [see Warnings and Precautions (5.3), Drug Interactions (7)].
Use buprenorphine sublingual tablets with caution in patients with compromised respiratory function (e.g., chronic obstructive pulmonary disease, cor pulmonale, decreased respiratory reserve, hypoxia, hypercapnia, or preexisting respiratory depression).
Educate patients and caregivers on how to recognize respiratory depression and emphasize the importance of calling 911 or getting emergency medical help right away in the event of a known or suspected overdose [see Patient Counseling Information (17)].
Opioids can cause sleep-related breathing disorders including central sleep apnea (CSA) and sleep-related hypoxemia. Opioid use increases the risk of CSA in a dose-dependent fashion. In patients who present with CSA, consider decreasing the opioid dosage using best practices for opioid taper [see Dosage and Administration (2.9)].
Patient Access to Naloxone for the Emergency Treatment of Opioid Overdose
Discuss the availability of naloxone for the emergency treatment of opioid overdose with the patient and caregiver.
Because patients being treated for opioid use disorder have the potential for relapse, putting them at risk for opioid overdose, strongly consider prescribing naloxone for the emergency treatment of opioid overdose, both when initiating and renewing treatment with buprenorphine sublingual tablets.Also consider prescribing naloxone if the patient has household members (including children) or other close contacts at risk for accidental ingestion or opioid overdose [see Dosage and Administration (2.2)].
Advise patients and caregivers that naloxone may also be administered for a known or suspected overdose with buprenorphine sublingual tablets itself. Higher than normal doses and repeated administration of naloxone may be necessary due to the long duration of action of buprenorphine sublingual tablets and its affinity for the mu-opioid receptor [see Overdosage (10)].
Inform patients and caregivers of their options for obtaining naloxone as permitted by individual state naloxone dispensing and prescribing requirements or guidelines (e.g., by prescription, directly from a pharmacist, or as part of a community-based program). Educate patients and caregivers on how to recognize respiratory depression and, if naloxone is prescribed, how to treat with naloxone. Emphasize the importance of calling 911 or getting emergency medical help, even if naloxone is administered [see Patient Counseling Information (17)].
5.3 Managing Risks from Concomitant Use of Benzodiazepines or Other CNS Depressants
Concomitant use of buprenorphine and benzodiazepines or other CNS depressants increases the risk of adverse reactions including overdose and death. Medication-assisted treatment of opioid use disorder, however, should not be categorically denied to patients taking these drugs. Prohibiting or creating barriers to treatment can pose an even greater risk of morbidity and mortality due to the opioid use disorder alone.
As a routine part of orientation to buprenorphine treatment, educate patients about the risks of concomitant use of benzodiazepines, sedatives, opioid analgesics, and alcohol.
Develop strategies to manage use of prescribed or illicit benzodiazepines or other CNS depressants at initiation of buprenorphine treatment, or if it emerges as a concern during treatment. Adjustments to induction procedures and additional monitoring may be required. There is no evidence to support dose limitations or arbitrary caps of buprenorphine as a strategy to address benzodiazepine use in buprenorphine-treated patients. However, if a patient is sedated at the time of buprenorphine dosing, delay or omit the buprenorphine dose if appropriate.
Cessation of benzodiazepines or other CNS depressants is preferred in most cases of concomitant use. In some cases, monitoring in a higher level of care for taper may be appropriate. In others, gradually tapering a patient off of a prescribed benzodiazepine or other CNS depressant or decreasing to the lowest effective dose may be appropriate.For patients in buprenorphine treatment, benzodiazepines are not the treatment of choice for anxiety or insomnia. Before co-prescribing benzodiazepines, ensure that patients are appropriately diagnosed and consider alternative medications and non-pharmacologic treatments to address anxiety or insomnia. Ensure that other healthcare providers prescribing benzodiazepines or other CNS depressants are aware of the patient’s buprenorphine treatment and coordinate care to minimize the risks associated with concomitant use.
If concomitant use is warranted, strongly consider prescribing naloxone for the emergency treatment of opioid overdose, as is recommended for all patients in buprenorphine treatment for opioid use disorder [see Warnings and Precautions (5.2)].
In addition, take measures to confirm that patients are taking their medications as prescribed and are not diverting or supplementing with illicit drugs. Toxicology screening should test for prescribed and illicit benzodiazepines [see Drug Interactions (7)].
5.4 Unintentional Pediatric Exposure
Buprenorphine can cause severe, possibly fatal, respiratory depression in children who are accidentally exposed to it. Store buprenorphine-containing medications safely out of the sight and reach of children and destroy any unused medication appropriately [see Patient Counseling (17)].
5.5 Neonatal Opioid Withdrawal Syndrome
Neonatal opioid withdrawal syndrome (NOWS) is an expected and treatable outcome of prolonged use of opioids during pregnancy, whether that use is medically-authorized or illicit. Unlike opioid withdrawal syndrome in adults, NOWS may be life-threatening if not recognized and treated in the neonate. Healthcare professionals should observe newborns for signs of NOWS and manage accordingly [see Use in Specific Populations (8.1)].
Advise pregnant women receiving opioid addiction treatment with buprenorphine of the risk of neonatal opioid withdrawal syndrome and ensure that appropriate treatment will be available [see Use in Specific Populations (8.1)].This risk must be balanced against the risk of untreated opioid addiction which often results in continued or relapsing illicit opioid use and is associated with poor pregnancy outcomes. Therefore, prescribers should discuss the importance and benefits of management of opioid addiction throughout pregnancy.5.6 Adrenal Insufficiency
Cases of adrenal insufficiency have been reported with opioid use, more often following greater than one month of use. Presentation of adrenal insufficiency may include non-specific symptoms and signs including nausea, vomiting, anorexia, fatigue, weakness, dizziness, and low blood pressure. If adrenal insufficiency is suspected, confirm the diagnosis with diagnostic testing as soon as possible. If adrenal insufficiency is diagnosed, treat with physiologic replacement doses of corticosteroids. Wean the patient off of the opioid to allow adrenal function to recover and continue corticosteroid treatment until adrenal function recovers. Other opioids may be tried as some cases reported use of a different opioid without recurrence of adrenal insufficiency. The information available does not identify any particular opioids as being more likely to be associated with adrenal insufficiency.
5.7 Risk of Opioid Withdrawal with Abrupt Discontinuation
Buprenorphine is a partial agonist at the mu-opioid receptor and chronic administration produces physical dependence of the opioid type, characterized by withdrawal signs and symptoms upon abrupt discontinuation or rapid taper. The withdrawal syndrome is typically milder than seen with full agonists and may be delayed in onset [see Drug Abuse and Dependence (9.3)].When discontinuing buprenorphine, gradually taper the dosage [see Dosage and Administration (2.9)].
5.8 Risk of Hepatitis, Hepatic Events
Cases of cytolytic hepatitis and hepatitis with jaundice have been observed in individuals receiving buprenorphine in clinical trials and through postmarketing adverse event reports. The spectrum of abnormalities ranges from transient asymptomatic elevations in hepatic transaminases to case reports of death, hepatic failure, hepatic necrosis, hepatorenal syndrome, and hepatic encephalopathy. In many cases, the presence of preexisting liver enzyme abnormalities, infection with hepatitis B or hepatitis C virus, concomitant usage of other potentially hepatotoxic drugs, and ongoing injecting drug use may have played a causative or contributory role. In other cases, insufficient data were available to determine the etiology of the abnormality. Withdrawal of buprenorphine has resulted in amelioration of acute hepatitis in some cases; however, in other cases no dose reduction was necessary. The possibility exists that buprenorphine had a causative or contributory role in the development of the hepatic abnormality in some cases. Liver function tests, prior to initiation of treatment is recommended to establish a baseline. Periodic monitoring of liver function during treatment is also recommended. A biological and etiological evaluation is recommended when a hepatic event is suspected. Depending on the case, buprenorphine sublingual tablet may need to be carefully discontinued to prevent withdrawal signs and symptoms and a return by the patient to illicit drug use, and strict monitoring of the patient should be initiated.
5.9 Hypersensitivity Reactions
Cases of hypersensitivity to buprenorphine products have been reported both in clinical trials and in the postmarketing experience. Cases of bronchospasm, angioneurotic edema, and anaphylactic shock have been reported. The most common signs and symptoms include rashes, hives, and pruritus. A history of hypersensitivity to buprenorphine is a contraindication to the use of buprenorphine sublingual tablet.
5.10 Precipitation of Opioid Withdrawal Signs and Symptoms
Because of the partial agonist properties of buprenorphine, buprenorphine sublingual tablet may precipitate opioid withdrawal signs and symptoms in individuals physically dependent on full opioid agonists if administered sublingually or parenterally before the agonist effects of other opioids have subsided.
5.11 Risk of Overdose in Opioid Naïve Patients
There have been reported deaths of opioid naïve individuals who received a 2 mg dose of buprenorphine as a sublingual tablet for analgesia. Buprenorphine sublingual tablet is not appropriate as an analgesic.
5.12 Use in Patients with Impaired Hepatic Function
In a pharmacokinetic study, buprenorphine plasma levels were found to be higher and the half-life was found to be longer in subjects with moderate and severe hepatic impairment, but not in subjects with mild hepatic impairment.
For patients with severe hepatic impairment, a dose adjustment is recommended, and patients with moderate or severe hepatic impairment should be monitored for signs and symptoms of toxicity or overdose caused by increased levels of buprenorphine [see Dosage and Administration (2.7), Use in Specific Populations (8.6)].
5.13 Dental Adverse Events
Cases of dental caries, some severe (i.e., tooth fracture, tooth loss), have been reported following the use of transmucosal buprenorphine-containing products. Reported events include cavities, tooth decay, dental abscesses/infection, rampant caries, tooth erosion, fillings falling out, and, in some cases, total tooth loss. Treatment for these events included tooth extraction, root canal, dental surgery, as well as other restorative procedures (i.e., fillings, crowns, implants, dentures). Multiple cases were reported in individuals without any prior history of dental problems.
Refer patients to dental care services and encourage them to have regular dental checkups while taking buprenorphine sublingual tablet. Educate patients to seek dental care and strategies to maintain or improve oral health while being treated with transmucosal buprenorphine-containing products. Strategies include, but are not limited to, gently rinsing the teeth and gums with water and then swallowing after buprenorphine sublingual tablet has been completely dissolved in the oral mucosa. Advise patients to wait for at least one hour after taking buprenorphine sublingual tablet before brushing teeth [see Dosage and Administration (2.5), Information for Patients (17), Medication Guide].
5.14 QTc Prolongation
Thorough QT studies with buprenorphine products have demonstrated QT prolongation ≤15 msec. This QTc prolongation effect does not appear to be mediated by hERG channels. Based on these two findings, buprenorphine is unlikely to be pro-arrhythmic when used alone in patients without risk factors. The risk of combining buprenorphine with other QT- prolonging agents is not known.
Consider these observations in clinical decisions when prescribing buprenorphine sublingual tablet to patients with risk factors such as hypokalemia, bradycardia, recent conversion from atrial fibrillation, congestive heart failure, digitalis therapy, baseline QT prolongation, subclinical long-QT syndrome, or severe hypomagnesemia.
5.15 Impairment of Ability to Drive or Operate Machinery
Buprenorphine sublingual tablet may impair the mental or physical abilities required for the performance of potentially dangerous tasks such as driving a car or operating machinery, especially during treatment induction and dose adjustment. Caution patients about driving or operating hazardous machinery until they are reasonably certain that buprenorphine therapy does not adversely affect his or her ability to engage in such activities.
5.16 Orthostatic Hypotension
Like other opioids, buprenorphine sublingual tablet may produce orthostatic hypotension in ambulatory patients.
5.17 Elevation of Cerebrospinal Fluid Pressure
Buprenorphine, like other opioids, may elevate cerebrospinal fluid pressure and should be used with caution in patients with head injury, intracranial lesions and other circumstances when cerebrospinal pressure may be increased. Buprenorphine can produce miosis and changes in the level of consciousness that may interfere with patient evaluation.
-
6 ADVERSE REACTIONS
The following serious adverse reactions are described elsewhere in the labeling:
Addiction, Abuse, and Misuse [see Warnings and Precautions (5.1)]
Respiratory and CNS Depression [see Warnings and Precautions (5.2, 5.3)]
Neonatal Opioid Withdrawal Syndrome [see Warnings and Precautions (5.5)]
Adrenal Insufficiency [see Warnings and Precautions (5.6)]
Opioid Withdrawal [see Warnings and Precautions (5.7, 5.10)]
Hepatitis, Hepatic Events [see Warnings and Precautions (5.8)]
Hypersensitivity Reactions [see Warnings and Precautions (5.9)]
Orthostatic Hypotension [see Warnings and Precautions (5.16)]
Elevation of Cerebrospinal Fluid Pressure [see Warnings and Precautions (5.17)]
Elevation of Intracholedochal Pressure [see Warnings and Precautions (5.18)]6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The safety of buprenorphine sublingual tablet was supported by clinical trials using buprenorphine sublingual tablet, buprenorphine and naloxone sublingual tablet and other trials using buprenorphine sublingual solutions. In total, safety data were available from 3214 opioid-dependent subjects exposed to buprenorphine at doses in the range used in treatment of opioid addiction.
Few differences in adverse event profile were noted between buprenorphine sublingual tablet or buprenorphine administered as a sublingual solution.
The following adverse events were reported to occur by at least 5% of patients in a 4-week study (Table 1).
Table 1. Adverse Events≥ 5% by Body System and Treatment Group in a 4-week study
N(%)
N(%)
Body System / Adverse Event (COSTART Terminology)
Buprenorphine Sublingual Tablets
16 mg/day
N = 103
Placebo
N = 107
Body as a Whole
Asthenia
5 (4.9%)
7 (6.5%)
Chills
8 (7.8%)
8 (7.5%)
Headache
30 (29.1%)
24 (22.4%)
Infection
12 (11.7%)
7 (6.5%)
Pain
19 (18.4%)
20 (18.7%)
Pain Abdomen
12 (11.7%)
7 (6.5%)
Pain Back
8 (7.8%)
12 (11.2%)
Withdrawal Syndrome
19 (18.4%)
40 (37.4%)
Cardiovascular System
Vasodilation
4 (3.9%)
7 (6.5%)
Digestive System
Constipation
8 (7.8%)
3 (2.8%)
Diarrhea
5 (4.9%)
16 (15.0%)
Nausea
14 (13.6%)
12 (11.2%)
Vomiting
8 (7.8%)
5 (4.7%)
Nervous System
Insomnia
22 (21.4%)
17 (15.9%)
Respiratory System
Rhinitis
10 (9.7%)
14 (13.1%)
Skin and Appendages
Sweating
13 (12.6%)
11 (10.3%)
The adverse event profile of buprenorphine was also characterized in the dose-controlled study of buprenorphine solution, over a range of doses in four months of treatment. Table 2 shows adverse events reported by at least 5% of subjects in any dose group in the dose-controlled study.
Table 2. Adverse Events (≥ 5%) by Body System and Treatment Group in a 16-week Study
Body System /Adverse
Event (COSTART Terminology)
Buprenorphine Dose*
Very Low*
(N=184)
Low*
(N=180)
Moderate*
(N=186)
High*
(N=181)
Total*
(N=731)
N (%)
N (%)
N (%)
N (%)
N (%)
Body as a Whole
Abscess
9 (5%)
2 (1%)
3 (2%)
2 (1%)
16 (2%)
Asthenia
26 (14%)
28 (16%)
26 (14%)
24 (13%)
104 (14%)
Chills
11 (6%)
12 (7%)
9 (5%)
10 (6%)
42 (6%)
Fever
7 (4%)
2 (1%)
2 (1%)
10 (6%)
21 (3%)
Flu Syndrome
4 (2%)
13 (7%)
19 (10%)
8 (4%)
44 (6%)
Headache
51 (28%)
62 (34%)
54 (29%)
53 (29%)
220 (30%)
Infection
32 (17%)
39 (22%)
38 (20%)
40 (22%)
149 (20%)
Injury Accidental
5 (3%)
10 (6%)
5 (3%)
5 (3%)
25 (3%)
Pain
47 (26%)
37 (21%)
49 (26%)
44 (24%)
177 (24%)
Pain Back
18 (10%)
29 (16%)
28 (15%)
27 (15%)
102 (14%)
Withdrawal Syndrome
45 (24%)
40 (22%)
41 (22%)
36 (20%)
162 (22%)
Digestive System
Constipation
10 (5%)
23 (13%)
23 (12%)
26 (14%)
82 (11%)
Diarrhea
19 (10%)
8 (4%)
9 (5%)
4 (2%)
40 (5%)
Dyspepsia
6 (3%)
10 (6%)
4 (2%)
4 (2%)
24 (3%)
Nausea
12 (7%)
22 (12%)
23 (12%)
18 (10%)
75 (10%)
Vomiting
8 (4%)
6 (3%)
10 (5%)
14 (8%)
38 (5%)
Nervous System
Anxiety
22 (12%)
24 (13%)
20 (11%)
25 (14%)
91 (12%)
Depression
24 (13%)
16 (9%)
25 (13%)
18 (10%)
83 (11%)
Dizziness
4 (2%)
9 (5%)
7 (4%)
11 (6%)
31 (4%)
Insomnia
42 (23%)
50 (28%)
43 (23%)
51 (28%)
186 (25%)
Nervousness
12 (7%)
11 (6%)
10 (5%)
13 (7%)
46 (6%)
Somnolence
5 (3%)
13 (7%)
9 (5%)
11 (6%)
38 (5%)
Respiratory System
Cough Increase
5 (3%)
11 (6%)
6 (3%)
4 (2%)
26 (4%)
Pharyngitis
6 (3%)
7 (4%)
6 (3%)
9 (5%)
28 (4%)
Rhinitis
27 (15%)
16 (9%)
15 (8%)
21 (12%)
79 (11%)
Skin and Appendages
Sweat
23 (13%)
21 (12%)
20 (11%)
23 (13%)
87 (12%)
Special Senses
Runny Eyes
13 (7%)
9 (5%)
6 (3%)
6 (3%)
34 (5%)
*Sublingual solution. Doses in this table cannot necessarily be delivered in tablet form, but for comparison purposes:
“Very low” dose (1 mg solution) would be less than a tablet dose of 2 mg
“Low” dose (4 mg solution) approximates a 6 mg tablet dose
“Moderate” dose (8 mg solution) approximates a 12 mg tablet dose
“High” dose (16 mg solution) approximates a 24 mg tablet dose
6.2 Postmarketing Experience
The following adverse reactions have been identified during post approval use of buprenorphine. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
The most frequently reported postmarketing adverse events with buprenorphine not observed in clinical trials, excluding drug exposure during pregnancy, was drug misuse or abuse.
Serotonin syndrome: Cases of serotonin syndrome, a potentially life-threatening condition, have been reported during concomitant use of opioids with serotonergic drugs.
Adrenal insufficiency: Cases of adrenal insufficiency have been reported with opioid use, more often following greater than one month of use.
Anaphylaxis: Anaphylaxis has been reported with ingredients contained in buprenorphine.
Androgen deficiency: Cases of androgen deficiency have occurred with chronic use of opioids [see Clinical Pharmacology (12.2)].
Local reactions: Dental decay (including caries, tooth fracture, and tooth loss), glossodynia, glossitis, oral mucosal erythema, oral hypoesthesia, and stomatitis.Hypoglycemia:Cases of hypoglycemia have been reported in patients taking opioids. Most reports were in patients with at least one predisposing risk factor (e.g., diabetes).
To report SUSPECTED ADVERSE REACTIONS, contact AvKARE at 1-855-361-3993 or FDA at 1-800-FDA-1088, or www.fda.gov/medwatch.
-
7 DRUG INTERACTIONS
Table 3 includes clinically significant drug interactions with buprenorphine.
Table 3.Clinically Significant Drug Interactions
Benzodiazepines or other Central Nervous System (CNS) Depressants Clinical Impact: Due to additive pharmacologic effects, the concomitant use of benzodiazepines or other CNS depressants, including alcohol, increases the risk of respiratory depression, profound sedation, coma, and death. Intervention: Cessation of benzodiazepines or other CNS depressants is preferred in most cases of concomitant use. In some cases, monitoring in a higher level of care for taper may be appropriate. In others, gradually tapering a patient off of a prescribed benzodiazepine or CNS depressant or decreasing to the lowest effective dose may be appropriate.
Before co-prescribing benzodiazepines for anxiety or insomnia, ensure that patients are appropriately diagnosed and consider alternative medications and non-pharmacologic treatments [see Warnings and Precautions (5.2, 5.3)].
If concomitant use is warranted, strongly consider prescribing naloxone for the emergency treatment of opioid overdose, as is recommended for all patients in treatment for opioid use disorder [see Warnings and Precautions (5.2)].Examples: Alcohol, benzodiazepines and other sedatives/hypnotics, anxiolytics, tranquilizers, muscle relaxants, general anesthetics, antipsychotics, and other opioids. Inhibitors of CYP3A4 Clinical Impact: The concomitant use of buprenorphine and CYP3A4 inhibitors can increase the plasma concentration of buprenorphine, resulting in increased or prolonged opioid effects, particularly when an inhibitor is added after a stable dose of buprenorphine is achieved.
After stopping a CYP3A4 inhibitor, as the effects of the inhibitor decline, the buprenorphine plasma concentration will decrease [see Clinical Pharmacology (12.3)], potentially resulting in decreased opioid efficacy or a withdrawal syndrome in patients who had developed physical dependence to buprenorphine.Intervention: If concomitant use is necessary, consider dosage reduction of buprenorphine until stable drug effects are achieved. Monitor patients for respiratory depression and sedation at frequent intervals.
If a CYP3A4 inhibitor is discontinued, consider increasing the buprenorphine dosage until stable drug effects are achieved. Monitor for signs of opioid withdrawal.Examples: Macrolide antibiotics (e.g., erythromycin), azole-antifungal agents (e.g. ketoconazole), protease inhibitors (e.g., ritonavir) CYP3A4 Inducers Clinical Impact: The concomitant use of buprenorphine and CYP3A4 inducers can decrease the plasma concentration of buprenorphine [see Clinical Pharmacology (12.3)], potentially resulting in decreased efficacy or onset of a withdrawal syndrome in patients who have developed physical dependence to buprenorphine.
After stopping a CYP3A4 inducer, as the effects of the inducer decline, the buprenorphine plasma concentration will increase [see Clinical Pharmacology (12.3)], which could increase or prolong both therapeutic effects and adverse reactions and may cause serious respiratory depression.Intervention: If concomitant use is necessary, consider increasing the buprenorphine dosage until stable drug effects are achieved. Monitor for signs of opioid withdrawal.
If a CYP3A4 inducer is discontinued, consider buprenorphine dosage reduction and monitor for signs of respiratory depression.Examples: Rifampin, carbamazepine, phenytoin Antiretrovirals: Non-nucleoside reverse transcriptase inhibitors (NNRTIs) Clinical Impact: Non-nucleoside reverse transcriptase inhibitors (NNRTIs) are metabolized principally by CYP3A4. Efavirenz, nevirapine, and etravirine are known CYP3A inducers, whereas delavirdine is a CYP3A inhibitor. Significant pharmacokinetic interactions between NNRTIs (e.g., efavirenz and delavirdine) and buprenorphine have been shown in clinical studies, but these pharmacokinetic interactions did not result in any significant pharmacodynamic effects. Intervention: Patients who are on chronic buprenorphine treatment should have their dose monitored if NNRTIs are added to their treatment regimen. Examples: efavirenz, nevirapine, etravirine, delavirdine Antiretrovirals: Protease inhibitors (PIs) Clinical Impact: Studies have shown some antiretroviral protease inhibitors (PIs) with CYP3A4 inhibitory activity (nelfinavir, lopinavir/ritonavir, ritonavir) have little effect on buprenorphine pharmacokinetic and no significant pharmacodynamic effects. Other PIs with CYP3A4 inhibitory activity (atazanavir and atazanavir/ritonavir) resulted in elevated levels of buprenorphine and norbuprenorphine, and patients in one study reported increased sedation. Symptoms of opioid excess have been found in postmarketing reports of patients receiving buprenorphine and atazanavir with and without ritonavir concomitantly. Intervention: Monitor patients taking buprenorphine and atazanavir with and without ritonavir, and reduce dose of buprenorphine if warranted. Examples: atazanavir, ritonavir Antiretrovirals: Nucleoside reverse transcriptase inhibitors (NRTIs) Clinical Impact: Nucleoside reverse transcriptase inhibitors (NRTIs) do not appear to induce or inhibit the P450 enzyme pathway, thus no interactions with buprenorphine are expected. Intervention: None Serotonergic Drugs Clinical Impact: The concomitant use of opioids with other drugs that affect the serotonergic neurotransmitter system has resulted in serotonin syndrome. Intervention: If concomitant use is warranted, carefully observe the patient, particularly during treatment initiation and dose adjustment. Discontinue buprenorphine sublingual tablet if serotonin syndrome is suspected. Examples: Selective serotonin reuptake inhibitors (SSRIs), serotonin and norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants (TCAs), triptans, 5-HT3 receptor antagonists, drugs that affect the serotonin neurotransmitter system (e.g., mirtazapine, trazodone, tramadol), certain muscle relaxants (i.e., cyclobenzaprine, metaxalone), monoamine oxidase (MAO) inhibitors (those intended to treat psychiatric disorders and also others, such as linezolid and intravenous methylene blue). Monoamine Oxidase Inhibitors (MAOIs) Clinical Impact: MAOI interactions with opioids may manifest as serotonin syndrome or opioid toxicity (e.g., respiratory depression, coma). Intervention: The use of buprenorphine is not recommended for patients taking MAOIs or within 14 days of stopping such treatment. Examples: phenelzine, tranylcypromine, linezolid Muscle Relaxants Clinical Impact: Buprenorphine may enhance the neuromuscular blocking action of skeletal muscle relaxants and produce an increased degree of respiratory depression. Intervention: Monitor patients receiving muscle relaxants and buprenorphine for signs of respiratory depression that may be greater than otherwise expected and decrease the dosage of buprenorphine and/or the muscle relaxant as necessary.
Due to the risk of respiratory depression with concomitant use of skeletal muscle relaxants and opioids, strongly consider prescribing naloxone for the emergency treatment of opioid overdose [see Dosage and Administration (2.2), Warnings and Precautions (5.2, 5.3)].Diuretics Clinical Impact: Opioids can reduce the efficacy of diuretics by inducing the release of antidiuretic hormone. Intervention: Monitor patients for signs of diminished diuresis and/or effects on blood pressure and increase the dosage of the diuretic as needed. Anticholinergic Drugs Clinical Impact: The concomitant use of anticholinergic drugs may increase the risk of urinary retention and/or severe constipation, which may lead to paralytic ileus. Intervention: Monitor patients for signs of urinary retention or reduced gastric motility when buprenorphine is used concomitantly with anticholinergic drugs. -
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
The data on use of buprenorphine, the active ingredient in buprenorphine sublingual tablets, in pregnancy, are limited; however, these data do not indicate an increased risk of major malformations specifically due to buprenorphine exposure. There are limited data from randomized clinical trials in women maintained on buprenorphine that were not designed appropriately to assess the risk of major malformations [see Data].Observational studies have reported on congenital malformations among buprenorphine‐exposed pregnancies, but were also not designed appropriately to assess the risk of congenital malformations specifically due to buprenorphine exposure [see Data].
Reproductive and developmental studies in rats and rabbits identified adverse events at clinically relevant and higher doses. Embryofetal death was observed in both rats and rabbits administered buprenorphine during the period of organogenesis at doses approximately 6 and 0.3 times, respectively, the human sublingual dose of 16 mg/day of buprenorphine. Pre- and post-natal development studies in rats demonstrated increased neonatal deaths at 0.3 times and above and dystocia at approximately 3 times the human sublingual dose of 16 mg/day of buprenorphine. No clear teratogenic effects were seen when buprenorphine was administered during organogenesis with a range of doses equivalent to or greater than the human sublingual dose of 16 mg/day of buprenorphine. However, increases in skeletal abnormalities were noted in rats and rabbits administered buprenorphine daily during organogenesis at doses approximately 0.6 times and approximately equal to the human sublingual dose of 16 mg/day of buprenorphine, respectively. In a few studies, some events such as acephalus and omphalocele were also observed but these findings were not clearly treatment-related [see Data]. Based on animal data, advice pregnant women of the potential risk to a fetus.
The estimated background risks of major birth defects and miscarriage for the indicated population are unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2 to 4% and 15 to 20%, respectively.
Clinical Considerations
Disease-associated maternal and embryo-fetal risk
Untreated opioid addiction in pregnancy is associated with adverse obstetrical outcomes such as low birth weight, preterm birth, and fetal death. In addition, untreated opioid addiction often results in continued or relapsing illicit opioid use.
Dose Adjustment during Pregnancy and the Postpartum PeriodDosage adjustments of buprenorphine may be required during pregnancy, even if the patient was maintained on a stable dose prior to pregnancy. Withdrawal signs and symptoms should be monitored closely and the dose adjusted as necessary.
Fetal/neonatal adverse reactionsNeonatal opioid withdrawal syndrome may occur in newborn infants of mothers who are receiving treatment with buprenorphine sublingual tablets.
Neonatal opioid withdrawal syndrome presents as irritability, hyperactivity and abnormal sleep pattern, high pitched cry, tremor, vomiting, diarrhea, and/or failure to gain weight. Signs of neonatal withdrawal usually occur in the first days after birth. The duration and severity of neonatal opioid withdrawal syndrome may vary. Observe newborns for signs of neonatal opioid withdrawal syndrome and manage accordingly [see Warnings and Precautions (5.5)].
Labor or DeliveryOpioid‐dependent women on buprenorphine maintenance therapy may require additional analgesia during labor.
Data
Human Data
Studies have been conducted to evaluate neonatal outcomes in women exposed to buprenorphine during pregnancy. Limited data from trials, observational studies, case series, and case reports on buprenorphine use in pregnancy do not indicate an increased risk of major malformations specifically due to buprenorphine. Several factors may complicate the interpretation of investigations of the children of women who take buprenorphine during pregnancy, including maternal use of illicit drugs, late presentation for prenatal care, infection, poor compliance, poor nutrition, and psychosocial circumstances. Interpretation of data is complicated further by the lack of information on untreated opioid‐dependent pregnant women, who would be the most appropriate group for comparison. Rather, women on another form of opioid medication‐assisted treatment, or women in the general population are generally used as the comparison group. However, women in these comparison groups may be different from women prescribed buprenorphine‐containing products with respect to maternal factors that may lead to poor pregnancy outcomes.
In a multicenter, double‐blind, randomized, controlled trial [Maternal Opioid Treatment: Human Experimental Research (MOTHER)] designed primarily to assess neonatal opioid withdrawal effects, opioid‐dependent pregnant women were randomized to buprenorphine (n=86) or methadone (n=89) treatment, with enrollment at an average gestational age of 18.7 weeks in both groups. A total of 28 of the 86 women in the buprenorphine group (33%) and 16 of the 89 women in the methadone group (18%) discontinued treatment before the end of pregnancy.
Among women who remained in treatment until delivery, there was no difference between buprenorphine‐treated and methadone‐treated groups in the number of neonates requiring NOWS treatment or in the peak severity of NOWS. Buprenorphine‐exposed neonates required less morphine (mean total dose, 1.1 mg vs. 10.4 mg), had shorter hospital stays (10.0 days vs. 17.5 days), and shorter duration of treatment for NOWS (4.1 days vs. 9.9 days) compared to the methadone‐exposed group. There were no differences between groups in other primary outcomes (neonatal head circumference,) or secondary outcomes (weight and length at birth, preterm birth, gestational age at delivery, and 1‐ minute and 5‐minute Apgar scores), or in the rates of maternal or neonatal adverse events. The outcomes among mothers who discontinued treatment before delivery and may have relapsed to illicit opioid use are not known. Because of the imbalance in discontinuation rates between the buprenorphine and methadone groups, the study findings are difficult to interpret.
Animal Data
The exposure margins listed below are based on body surface area comparisons (mg/m2) to the human sublingual dose of 16 mg buprenorphine via buprenorphine sublingual tablets.
No definitive drug-related teratogenic effects were observed in rats and rabbits at IM doses up to 30 mg/kg/day (estimated exposure approximately 20 times and 35 times, respectively, the human sublingual dose of 16 mg). Maternal toxicity resulting in mortality was noted in these studies in both rats and rabbits. Acephalus was observed in one rabbit fetus from the low-dose group and omphalocele was observed in two rabbit fetuses from the same litter in the mid-dose group; no findings were observed in fetuses from the high-dose group. Maternal toxicity was seen in the high-dose group but not at the lower doses where the findings were observed. Following oral administration of buprenorphine to rats, dose-related post-implantation losses, evidenced by increases in the numbers of early resorptions with consequent reductions in the numbers of fetuses, were observed at doses of 10 mg/kg/day or greater (estimated exposure approximately 6 times the human sublingual dose of 16 mg). In the rabbit, increased post-implantation losses occurred at an oral dose of 40 mg/kg/day. Following IM administration in the rat and the rabbit, post-implantation losses, as evidenced by decreases in live fetuses and increases in resorptions, occurred at 30 mg/kg/day.
Buprenorphine was not teratogenic in rats or rabbits after IM or subcutaneous (SC) doses up to 5 mg/kg/day (estimated exposure was approximately 3 and 6 times, respectively, the human sublingual dose of 16 mg), after IV doses up to 0.8 mg/kg/day (estimated exposure was approximately 0.5 times and equal to, respectively, the human sublingual dose of 16 mg), or after oral doses up to 160 mg/kg/day in rats (estimated exposure was approximately 95 times the human sublingual dose of 16 mg) and 25 mg/kg/day in rabbits (estimated exposure was approximately 30 times the human sublingual dose of 16 mg). Significant increases in skeletal abnormalities (e.g., extra thoracic vertebra or thoraco-lumbar ribs) were noted in rats after SC administration of 1 mg/kg/day and up (estimated exposure was approximately 0.6 times the human sublingual dose of 16 mg), but were not observed at oral doses up to 160 mg/kg/day. Increases in skeletal abnormalities in rabbits after IM administration of 5 mg/kg/day (estimated exposure was approximately 6 times the human sublingual dose of 16 mg) in the absence of maternal toxicity or oral administration of 1 mg/kg/day or greater (estimated exposure was approximately equal to the human sublingual dose of 16 mg) were not statistically significant.
In rabbits, buprenorphine produced statistically significant pre-implantation losses at oral doses of 1 mg/kg/day or greater and post-implantation losses that were statistically significant at IV doses of 0.2 mg/kg/day or greater (estimated exposure approximately 0.3 times the human sublingual dose of 16 mg). No maternal toxicity was noted at doses causing post-implantation loss in this study.
Dystocia was noted in pregnant rats treated intramuscularly with buprenorphine from Gestation Day 14 through Lactation Day 21 at 5 mg/kg/day (approximately 3 times the human sublingual dose of 16 mg). Fertility, and pre- and post-natal development studies with buprenorphine in rats indicated increases in neonatal mortality after oral doses of 0.8 mg/kg/day and up (approximately 0.5 times the human sublingual dose of 16 mg), after IM doses of 0.5 mg/kg/day and up (approximately 0.3 times the human sublingual dose of 16 mg), and after SC doses of 0.1 mg/kg/day and up (approximately 0.06 times the human sublingual dose of 16 mg). An apparent lack of milk production during these studies likely contributed to the decreased pup viability and lactation indices. Delays in the occurrence of righting reflex and startle response were noted in rat pups at an oral dose of 80 mg/kg/day (approximately 50 times the human sublingual dose of 16 mg).8.2 Lactation
Risk Summary
Based on two studies in 13 lactating women maintained on buprenorphine treatment, buprenorphine and its metabolite norbuprenorphine were present in low levels in human milk and available data have not shown adverse reactions in breastfed infants. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for buprenorphine sublingual tablets and any potential adverse effects on the breastfed child from the drug or from the underlying maternal condition.
Clinical ConsiderationsAdvise breastfeeding women taking buprenorphine products to monitor the infant for increased drowsiness and breathing difficulties.
DataData were consistent from two studies (N=13) of breastfeeding infants whose mothers were maintained on sublingual doses of buprenorphine ranging from 2.4 to 24 mg/day, showing that the infants were exposed to less than 1% of the maternal daily dose.
In a study of six lactating women who were taking a median sublingual buprenorphine dose of 0.29 mg/kg/day 5 to 8 days after delivery, breast milk provided a median infant dose of 0.42 mcg/kg/day of buprenorphine and 0.33 mcg/kg/day of norbuprenorphine, equal to 0.2% and 0.12%, respectively, of the maternal weight-adjusted dose (relative dose/kg (%) of norbuprenorphine was calculated from the assumption that buprenorphine and norbuprenorphine are equipotent).
Data from a study of seven lactating women who were taking a median sublingual buprenorphine dose of 7 mg/day an average of 1.12 months after delivery indicated that the mean milk concentrations (Cavg) of buprenorphine and norbuprenorphine were 3.65 mcg/L and 1.94 mcg/L respectively. Based on the study data, and assuming milk consumption of 150 mL/kg/day, an exclusively breastfed infant would receive an estimated mean absolute infant dose (AID) of 0.55 mcg/kg/day of buprenorphine and 0.29 mcg/kg/day of norbuprenorphine, or a mean relative infant dose (RID) of 0.38% and 0.18%, respectively, of the maternal weight-adjusted dose.8.3 Females and Males of Reproductive Potential
Infertility
Chronic use of opioids may cause reduced fertility in females and males of reproductive potential. It is not known whether these effects on fertility are reversible [see Adverse Reactions (6.2), Clinical Pharmacology (12.2), Nonclinical Toxicology (13.1)].
8.4 Pediatric Use
The safety and effectiveness of buprenorphine sublingual tablet has not been established in pediatric patients.
8.5 Geriatric Use
Clinical studies of buprenorphine sublingual tablet, buprenorphine and naloxone sublingual film, or buprenorphine and naloxone sublingual tablet did not include sufficient numbers of subjects aged 65 and over to determine whether they responded differently than younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients.
Due to possible decreased hepatic, renal, or cardiac function and of concomitant disease or other drug therapy in geriatric patients, the decision to prescribe buprenorphine sublingual tablets should be made cautiously in individuals 65 years of age or older and these patients should be monitored for signs and symptoms of toxicity or overdose.8.6 Hepatic Impairment
The effects of hepatic impairment on the pharmacokinetics of buprenorphine were evaluated in a pharmacokinetic study. Buprenorphine is extensively metabolized in the liver and buprenorphine plasma levels were found to be higher and the half-life was found to be longer in subjects with moderate and severe hepatic impairment, but not in subjects with mild hepatic impairment.
For patients with severe hepatic impairment, a dose adjustment is recommended, and patients with moderate or severe hepatic impairment should be monitored for signs and symptoms of toxicity or overdose caused by increased levels of buprenorphine [see Dosage and Administration (2.7), Warnings and Precautions (5.12), Clinical Pharmacology (12.3)].
-
9 DRUG ABUSE AND DEPENDENCE
9.1 Controlled Substance
Buprenorphine sublingual tablet contains buprenorphine, a Schedule III controlled substance under the Controlled Substances Act.
9.2 Abuse
Buprenorphine, like morphine and other opioids, has the potential for being abused and is subject to criminal diversion. This should be considered when prescribing or dispensing buprenorphine in situations when the clinician is concerned about an increased risk of misuse, abuse, or diversion. Healthcare professionals should contact their state professional licensing board or state controlled substances authority for information on how to prevent and detect abuse or diversion of this product.
Patients who continue to misuse, abuse, or divert, buprenorphine products or other opioids should be provided or referred for more intensive and structured treatment.
Abuse of buprenorphine poses a risk of overdose and death. This risk is increased with the abuse of buprenorphine and alcohol and other substances, especially benzodiazepines.
The healthcare provider may be able to more easily detect misuse or diversion by maintaining records of medication prescribed including date, dose, quantity, frequency of refills, and renewal requests of medication prescribed.
Proper assessment of the patient, proper prescribing practices, periodic re-evaluation of therapy, and proper handling and storage of the medication are appropriate measures that help to limit abuse of opioid drugs.
9.3 Dependence
Buprenorphine is a partial agonist at the mu-opioid receptor and chronic administration produces physical dependence of the opioid type, characterized by moderate withdrawal signs and symptoms upon abrupt discontinuation or rapid taper. The withdrawal syndrome is typically milder than seen with full agonists and may be delayed in onset [see Warnings and Precautions (5.7)].
Neonatal opioid withdrawal syndrome (NOWS) is an expected and treatable outcome of prolonged use of opioids during pregnancy [see Warnings and Precautions (5.5)].
-
10 OVERDOSAGE
Clinical Presentation
The manifestations of acute overdose include pinpoint pupils, sedation, hypotension, hypoglycemia, respiratory depression, and death.
Treatment of OverdoseIn the event of overdose, the respiratory and cardiac status of the patient should be monitored carefully. When respiratory or cardiac functions are depressed, primary attention should be given to the re-establishment of adequate respiratory exchange through provision of a patent airway and institution of assisted or controlled ventilation. Oxygen, IV fluids, vasopressors, and other supportive measures should be employed as indicated.
In the case of overdose, the primary management should be the re-establishment of adequate ventilation with mechanical assistance of respiration, if required. Naloxone may be of value for the management of buprenorphine overdose. Higher than normal doses and repeated administration may be necessary. The long duration of action of buprenorphine sublingual tablet should be taken into consideration when determining the length of treatment and medical surveillance needed to reverse the effects of an overdose. Insufficient duration of monitoring may put patients at risk.
-
11 DESCRIPTION
Buprenorphine sublingual tablet is uncoated, round, biconvex, white to off-white tablet. It contains buprenorphine hydrochloride USP, a partial agonist at the mu-opioid receptor, and is available in two dosage strengths, 2 mg buprenorphine and 8 mg buprenorphine (as the free base, equivalent to 2.16 mg buprenorphine hydrochloride USP and 8.64 mg buprenorphine hydrochloride USP). Each tablet also contains lactose monohydrate, mannitol, povidone, anhydrous citric acid, sodium citrate, butylated hydroxyanisole, corn starch, pregelatinized starch, and magnesium stearate.
Chemically, buprenorphine hydrochloride is (2S)-2-[17-Cyclopropylmethyl-4,5α-epoxy-3-hydroxy-6-methoxy-6α,14-ethano-14α-morphinan-7α-yl]-3,3-dimethylbutan-2-ol hydrochloride. It has the following chemical structure:
Buprenorphine hydrochloride, USP has the molecular formula C 29H 41NO 4 HCl and the molecular weight is 504.10. It is an off-white crystalline powder, slightly soluble in water, freely soluble in methanol, soluble in alcohol and practically insoluble in cyclohexane.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Buprenorphine sublingual tablet contains buprenorphine, a partial agonist at the mu-opioid receptor and an antagonist at the kappa-opioid receptor.
12.2 Pharmacodynamics
Subjective Effects
Comparisons of buprenorphine to full opioid agonists such as methadone and hydromorphone suggest that sublingual buprenorphine produces typical opioid agonist effects which are limited by a ceiling effect.
Opioid agonist ceiling-effects were also observed in a double-blind, parallel group, dose-ranging comparison of single doses of buprenorphine sublingual solution (1 mg, 2 mg, 4 mg, 8 mg, 16 mg, or 32 mg), placebo and a full agonist control at various doses. The treatments were given in ascending dose order at intervals of at least one week to 16 opioid-experienced subjects who were not physically dependent. Both active drugs produced typical opioid agonist effects. For all measures for which the drugs produced an effect, buprenorphine produced a dose-related response. However, in each case, there was a dose that produced no further effect. In contrast, the highest dose of the full agonist control always produced the greatest effects. Agonist objective rating scores remained elevated for the higher doses of buprenorphine (8 mg to 32 mg) longer than for the lower doses and did not return to baseline until 48 hours after drug administration. The onset of effects appeared more rapidly with buprenorphine than with the full agonist control, with most doses nearing peak effect after 100 minutes for buprenorphine compared to 150 minutes for the full agonist control.
Physiologic Effects
Buprenorphine in IV (2 mg, 4 mg, 8 mg, 12 mg and 16 mg) and sublingual (12 mg) doses has been administered to opioid-experienced subjects who were not physically dependent to examine cardiovascular, respiratory and subjective effects at doses comparable to those used for treatment of opioid dependence. Compared to placebo, there were no statistically significant differences among any of the treatment conditions for blood pressure, heart rate, respiratory rate, O 2saturation, or skin temperature across time. Systolic BP was higher in the 8 mg group than placebo (3-hour AUC values). Minimum and maximum effects were similar across all treatments. Subjects remained responsive to low voice and responded to computer prompts. Some subjects showed irritability, but no other changes were observed.
The respiratory effects of sublingual buprenorphine were compared with the effects of methadone in a double-blind, parallel group, dose ranging comparison of single doses of buprenorphine sublingual solution (1 mg, 2 mg, 4 mg, 8 mg, 16 mg, or 32 mg) and oral methadone (15 mg, 30 mg, 45 mg, or 60 mg) in non-dependent, opioid-experienced volunteers. In this study, hypoventilation not requiring medical intervention was reported more frequently after buprenorphine doses of 4 mg and higher than after methadone. Both drugs decreased O 2saturation to the same degree.
Effects on the Endocrine SystemOpioids inhibit the secretion of adrenocorticotropic hormone (ACTH), cortisol, and luteinizing hormone (LH) in humans [see Adverse Reactions (6.2)]. They also stimulate prolactin, growth hormone (GH) secretion, and pancreatic secretion of insulin and glucagon.
Chronic use of opioids may influence the hypothalamic-pituitary-gonadal axis, leading to androgen deficiency that may manifest as low libido, impotence, erectile dysfunction, amenorrhea, or infertility.
The causal role of opioids in the clinical syndrome of hypogonadism is unknown because the various medical, physical, lifestyle, and psychological stressors that may influence gonadal hormone levels have not been adequately controlled for in studies conducted to date. Patients presenting with symptoms of androgen deficiency should undergo laboratory evaluation.Cardiac Electrophysiology
Thorough QT studies with buprenorphine products have demonstrated QT prolongation ≤15 msec.
12.3 Pharmacokinetics
Absorption
Plasma levels of buprenorphine increased with the sublingual dose of buprenorphine sublingual tablet (Table 3). There was wide inter-patient variability in the sublingual absorption of buprenorphine, but within subjects the variability was low. Both C maxand AUC of buprenorphine increased in a linear fashion with the increase in dose (in the range of 4 mg to 16 mg), although the increase was not directly dose-proportional.
Table 3. Pharmacokinetic Parameters of Buprenorphine and Norbuprenorphine after the sublingual administration of buprenorphine sublingual tablets Dose Analyte Mean
SDC max
(ng/mL)T max
(h)AUC inf
(h·ng/mL)t 1/2
(h)2 mg Buprenorphine Mean
SD1.25
0.5841.84
0.6210.93
3.94531.66
12.66Norbuprenorphine Mean
SD0.301
0.1272.36
2.7512.39
4.52639.28
20.858 mg Buprenorphine Mean
SD2.88
1.141.28
0.4628.39
10.2235.01
14.7Norbuprenorphine Mean
SD1.38
0.7521.75
2.1150.18
22.6144.33
19.2716 mg Buprenorphine Mean
SD4.70
2.161.42
0.5047.09
20.0336.51
13.99Norbuprenorphine Mean
SD2.65
1.621.52
1.3492.31
34.7440.35
12.07Distribution
Buprenorphine is approximately 96% protein bound, primarily to alpha and beta globulin.
Elimination
Metabolism
Buprenorphine undergoes both N-dealkylation to norbuprenorphine and glucuronidation. The N-dealkylation pathway is mediated primarily by CYP3A4. Norbuprenorphine, the major metabolite, can further undergo glucuronidation. Norbuprenorphine has been found to bind opioid receptors in vitro; however, it is not known whether norbuprenorphine contributes to the overall effect of buprenorphine sublingual tablets.
Excretion
A mass balance study of buprenorphine showed complete recovery of radiolabel in urine (30%) and feces (69%) collected up to 11 days after dosing. Almost all of the dose was accounted for in terms of buprenorphine, norbuprenorphine, and two unidentified buprenorphine metabolites. In urine, most of buprenorphine and norbuprenorphine was conjugated (buprenorphine, 1% free and 9.4% conjugated; norbuprenorphine, 2.7% free and 11% conjugated). In feces, almost all of the buprenorphine and norbuprenorphine were free (buprenorphine, 33% free and 5% conjugated; norbuprenorphine, 21% free and 2% conjugated).
When buprenorphine sublingual tablet is administered sublingually, buprenorphine has a mean elimination half-life from plasma ranging from 31 to 35 hours.
Drug Interactions Studies:
CYP3A4 Inhibitors and Inducers
Buprenorphine has been found to be a CYP2D6 and CYP3A4 inhibitor and its major metabolite, norbuprenorphine has been found to be a moderate CYP2D6 inhibitor in in vitrostudies employing human liver microsomes. However, the relatively low plasma concentrations of buprenorphine and norbuprenorphine resulting from therapeutic doses are not expected to raise significant drug-drug interaction concerns [see Drug Interactions (7)].
Specific Populations
Hepatic Impairment
In a pharmacokinetic study, the disposition of buprenorphine was determined after administering a 2.0 mg/0.5 mg buprenorphine and naloxone sublingual tablet in subjects with varied degrees of hepatic impairment as indicated by Child-Pugh criteria. The disposition of buprenorphine in patients with hepatic impairment was compared to disposition in subjects with normal hepatic function.
In subjects with mild hepatic impairment, the changes in mean C max, AUC 0-last, and half-life values of buprenorphine were not clinically significant.
For subjects with moderate and severe hepatic impairment, mean C max, AUC 0-last, and half-life values of buprenorphine were increased (Table 4) [see Warnings and Precautions (5.12), Use in Specific Populations (8.6)].
Table 4. Changes in Buprenorphine Pharmacokinetic Parameters in Subjects with Moderate and Severe Hepatic Impairment Hepatic
ImpairmentPK Parameters Increase in buprenorphine
compared to healthy subjectsModerate C max 8% AUC 0-last 64% Half-life 35% Severe C max 72% AUC 0-last 181% Half-life 57%
HCV infectionIn subjects with HCV infection but no sign of hepatic impairment, the changes in the mean C max, AUC 0-last, and half-life values of buprenorphine were not clinically significant in comparison to healthy subjects without HCV infection.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity
Carcinogenicity studies of buprenorphine were conducted in Sprague-Dawley rats and CD-1 mice. Buprenorphine was administered in the diet to rats at doses of 0.6, 5.5, and 56 mg/kg/day (estimated exposure was approximately 0.4, 3 and 35 times the recommended human daily sublingual dose of 16 mg on a mg/m 2basis) for 27 months. As in the buprenorphine/naloxone carcinogenicity study in rat, statistically significant dose-related increases in Leydig cell tumors occurred. In an 86-week study in CD-1 mice, buprenorphine was not carcinogenic at dietary doses up to 100 mg/kg/day (estimated exposure was approximately 30 times the recommended human daily sublingual dose of 16 mg on a mg/m 2basis).
MutagenicityBuprenorphine was studied in a series of tests utilizing gene, chromosome, and DNA interactions in both prokaryotic and eukaryotic systems. Results were negative in yeast ( S. cerevisiae) for recombinant, gene convertant, or forward mutations; negative in Bacillus subtilis“rec” assay, negative for clastogenicity in CHO cells, Chinese hamster bone marrow and spermatogonia cells, and negative in the mouse lymphoma L5178Y assay.
Results were equivocal in the Ames test: negative in studies in two laboratories, but positive for frame shift mutation at a high dose (5 mg/plate) in a third study. Results were positive in the Green-Tweets ( E. coli) survival test, positive in a DNA synthesis inhibition (DSI) test with testicular tissue from mice, for both in vivoand in vitroincorporation of [ 3H]thymidine, and positive in unscheduled DNA synthesis (UDS) test using testicular cells from mice.
Impairment of Fertility
Reproduction studies of buprenorphine in rats demonstrated no evidence of impaired fertility at daily oral doses up to 80 mg/kg/day (estimated exposure was approximately 50 times the recommended human daily sublingual dose of 16 mg on a mg/m 2basis) or up to 5 mg/kg/day IM or SC (estimated exposure was approximately 3 times the recommended human daily sublingual dose of 16 mg on a mg/m 2basis).
-
14 CLINICAL STUDIES
Clinical data on the safety and efficacy of buprenorphine sublingual tablets were derived from studies of buprenorphine sublingual tablet formulations, with and without naloxone, and from studies of sublingual administration of a more bioavailable ethanolic solution of buprenorphine.
Buprenorphine sublingual tablets were studied in 1834 patients; buprenorphine and naloxone sublingual tablets in 575 patients, and buprenorphine sublingual solutions in 2470 patients. A total of 1270 women received buprenorphine in those clinical trials. Dosing recommendations are based on data from one trial of both tablet formulations and two trials of the ethanolic solution. All trials used buprenorphine in conjunction with psychosocial counseling as part of a comprehensive addiction treatment program. There were no clinical studies conducted to assess the efficacy of buprenorphine as the only component of treatment.
In a double-blind placebo- and active-controlled study, 326 heroin-addicted subjects were randomly assigned to either buprenorphine and naloxone sublingual tablets, 16 mg/4 mg per day; buprenorphine sublingual tablets, 16 mg per day; or placebo sublingual tablets. For subjects randomized to either active treatment, dosing began with one 8 mg buprenorphine sublingual tablet on Day 1, followed by 16 mg (two 8 mg tablets) of buprenorphine sublingual tablet on Day 2. On Day 3, those randomized to receive buprenorphine and naloxone sublingual tablets were switched to the combination tablet. Subjects randomized to placebo received one placebo tablet on Day 1 and two placebo tablets per day thereafter for four weeks. Subjects were seen daily in the clinic (Monday through Friday) for dosing and efficacy assessments. Take-home doses were provided for weekends. Subjects were instructed to hold the medication under the tongue for approximately 5 to 10 minutes until completely dissolved. Subjects received counseling regarding HIV infection and up to one hour of individualized counseling per week. The primary study comparison was to assess the efficacy of buprenorphine and naloxone sublingual tablets and buprenorphine sublingual tablets individually against placebo sublingual tablet. The percentage of thrice-weekly urine samples that were negative for non-study opioids was statistically higher for both buprenorphine and naloxone sublingual tablets and buprenorphine sublingual tablets than for placebo sublingual tablets.
In a double-blind, double-dummy, parallel-group study comparing buprenorphine ethanolic solution to a full agonist active control, 162 subjects were randomized to receive the ethanolic sublingual solution of buprenorphine at 8 mg/day (a dose which is roughly comparable to a dose of 12 mg per day of buprenorphine sublingual tablets), or two relatively low doses of active control, one of which was low enough to serve as an alternative to placebo, during a 3 to 10 day induction phase, a 16-week maintenance phase and a 7-week detoxification phase. Buprenorphine was titrated to maintenance dose by Day 3; active control doses were titrated more gradually.
Maintenance dosing continued through Week 17, and then medications were tapered by approximately 20% to 30% per week over Weeks 18 to 24, with placebo dosing for the last two weeks. Subjects received individual and/or group counseling weekly.
Based on retention in treatment and the percentage of thrice-weekly urine samples negative for non-study opioids, buprenorphine was more effective than the low dose of the control, in keeping heroin addicts in treatment and in reducing their use of opioids while in treatment. The effectiveness of buprenorphine, 8 mg per day was similar to that of the moderate active control dose, but equivalence was not demonstrated.
In a dose-controlled, double-blind, parallel-group, 16-week study, 731 subjects were randomized to receive one of four doses of buprenorphine ethanolic solution: 1 mg, 4 mg, 8 mg, and 16 mg. Buprenorphine was titrated to maintenance doses over 1 to 4 days and continued for 16 weeks. Subjects received at least one session of AIDS education and additional counseling ranging from one hour per month to one hour per week, depending on site.
Based on retention in treatment and the percentage of thrice-weekly urine samples negative for non-study opioids, the three highest tested doses were superior to the 1 mg dose. Therefore, this study showed that a range of buprenorphine doses may be effective. The 1 mg dose of buprenorphine sublingual solution can be considered to be somewhat lower than a 2 mg tablet dose. The other doses used in the study encompass a range of tablet doses from approximately 6 mg to approximately 24 mg.
-
16 HOW SUPPLIED / STORAGE AND HANDLING
Buprenorphine sublingual tablets containing 2 mg buprenorphine (as the free base, equivalent to 2.16 mg buprenorphine hydrochloride USP) are uncoated, round, biconvex, white to off-white, sublingual tablets, debossed with ‘459’ on one side and plain on other side and are supplied as:
NDC: 50268-128-15 (10 tablets per card, 5 cards per carton).
Buprenorphine sublingual tablets containing 8 mg buprenorphine (as the free base, equivalent to 8.64 mg buprenorphine hydrochloride USP) are uncoated, round, biconvex, white to off-white, sublingual tablets, debossed with ‘460’ on one side and plain on other side and are supplied as:
NDC: 50268-129-15 (10 tablets per card, 5 cards per carton).
Store at 20° to 25°C (68° to 77°F); excursions permitted between 15° and 30°C (59° and 86°F) [see USP Controlled Room Temperature].
Protect from light.
Store buprenorphine sublingual tablets securely and dispose of properly [see Patient Counseling Information (17)].
-
17 PATIENT COUNSELING INFORMATION
Advise patients to read the FDA-approved patient labeling (Medication Guide).
Storage and Disposal
Because of the risks associated with accidental ingestion, misuse, and abuse, advise patients to store buprenorphine sublingual tablets securely, out of sight and reach of children, and in a location not accessible by others, including visitors to the home [see Warnings and Precautions(5.1, 5.4), Drug Abuse and Dependence (9.2)] . Inform patients that leaving buprenorphine sublingual tablets unsecured can pose a deadly risk to others in the home.
Advise patients and caregivers that when medicines are no longer needed, they should be disposed of promptly. Expired, unwanted, or unused buprenorphine sublingual tablets should be disposed of by flushing the unused medication down the toilet, if a drug take-back option is not readily available. Inform patients that they can visit www.fda.gov/drugdisposal for a complete list of medicines recommended for disposal by flushing, as well as additional information on disposal of unused medicines.
Safe Use
Before initiating treatment with buprenorphine sublingual tablet, explain the points listed below to caregivers and patients. Instruct patients to read the Medication Guide each time buprenorphine sublingual tablet is dispensed because new information may be available.
- Inform patients and caregivers that potentially fatal additive effects may occur if buprenorphine sublingual tablets are used with benzodiazepines or other CNS depressants, including alcohol. Counsel patients that such medications should not be used concomitantly unless supervised by a health care provider [see Warnings and Precautions (5.2, 5.3), Drug Interactions (7)].
- Educate patients and caregivers on how to recognize respiratory depression and emphasize the importance of calling 911 or getting emergency medical help right away in the event of a known or suspected overdose [see Warnings and Precautions (5.2)].
- Patient Access to Naloxone for the Emergency Treatment of Opioid Overdose
Because patients being treated for opioid use disorder are at risk for relapse, discuss the importance of having access to naloxone with the patient and caregiver. Also discuss the importance of having access to naloxone if there are household members (including children) or other close contacts at risk for accidental ingestion or opioid overdose.
Inform patients and caregivers of the options for obtaining naloxone as permitted by individual state naloxone dispensing and prescribing requirements or guidelines (e.g., by prescription, directly from a pharmacist, or as part of a community-based program).
Educate patients and caregivers on how to recognize the signs and symptoms of an opioid overdose.
Explain to patients and caregivers that naloxone’s effects are temporary, and that they must call 911 or get emergency medical help right away in all cases of known or suspected opioid overdose, even if naloxone is administered. Repeat administration may be necessary, particularly for overdose involving buprenorphine and naloxone sublingual tablet, because naloxone is often not effective at the doses available for patient access [see Dosage and Administration (2.2), Warnings and Precautions (5.2), Overdosage (10)].
If naloxone is prescribed, also advise patients and caregivers:
- How to treat with naloxone in the event of an opioid overdose
- To tell family and friends about their naloxone and to keep it in a place where family and friends can easily access it in an emergency
- To read the Patient Information (or other educational material) that will come with their naloxone. Emphasize the importance of doing this before an opioid emergency happens, so the patient and caregiver will know what to do.
- Advise patients that buprenorphine sublingual tablet contains an opioid that can be a target for people who abuse prescription medications or street drugs, to keep their tablets in a safe place, and to protect them from theft.
- Instruct patients to keep buprenorphine sublingual tablet in a secure place, out of the sight and reach of children. Accidental or deliberate ingestion by a child may cause respiratory depression that can result in death. Advise patients to seek medical attention immediately if a child is exposed to buprenorphine sublingual tablet.
- Inform patients that opioids could cause a rare but potentially life-threatening condition resulting from concomitant administration of serotonergic drugs. Warn patients of the symptoms of serotonin syndrome and to seek medical attention right away if symptoms develop. Instruct patients to inform their healthcare providers if they are taking, or plan to take serotonergic medications
[see Drug Interactions (7)].
- Inform patients that opioids could cause adrenal insufficiency, a potentially life-threatening condition. Adrenal insufficiency may present with non-specific symptoms and signs such as nausea, vomiting, anorexia, fatigue, weakness, dizziness, and low blood pressure. Advise patients to seek medical attention if they experience a constellation of these symptoms [see Warnings and Precautions (5.6)].
- Advise patients to never give buprenorphine sublingual tablet to anyone else, even if he or she has the same signs and symptoms. It may cause harm or death.
- Advise patients that selling or giving away this medication is against the law.
- Advise patients that, after buprenorphine sublingual tablets have completely dissolved in the oral mucosa, to take a sip of water, swish it gently around their teeth and gums, and swallow. Advise patients to wait for at least one hour after taking buprenorphine sublingual tablets before brushing teeth [see Warnings and Precautions (5.13)].
- Refer patients to dental care services and encourage them to have regular dental checkups while taking buprenorphine sublingual tablets. Instruct patients to inform their dentist that they have started therapy on buprenorphine sublingual tablets [see Warnings and Precautions (5.13)].
- Caution patients that buprenorphine sublingual tablet may impair the mental or physical abilities required for the performance of potentially dangerous tasks such as driving or operating hazardous machinery. Caution should be taken especially during drug induction and dose adjustment and until individuals are reasonably certain that buprenorphine therapy does not adversely affect their ability to engage in such activities [see Warnings and Precautions (5.15)].
- Advise patients not to change the dosage of buprenorphine sublingual tablet without consulting their healthcare providers.
- Advise patients that if they miss a dose of buprenorphine sublingual tablet they should take it as soon as they remember. If it is almost time for the next dose, they should skip the missed dose and take the next dose at the regular time.
- Advise patients to take buprenorphine sublingual tablet once a day.
- Inform patients that buprenorphine sublingual tablet can cause drug dependence and that withdrawal signs and symptoms may occur when the medication is discontinued.
- Advise patients seeking to discontinue treatment with buprenorphine for opioid dependence to work closely with their healthcare providers on a tapering schedule and inform them of the potential to relapse to illicit drug use associated with discontinuation of opioid agonist/partial agonist medication-assisted treatment.
- Advise patients that, like other opioids, buprenorphine sublingual tablet may produce orthostatic hypotension in ambulatory individuals [see Warnings and Precautions (5.16)].
- Advise patients to inform their healthcare providers if any other prescription medications, over-the-counter medications, or herbal preparations are prescribed or currently being used [see Drug Interactions (7)].
- Advise women that if they are pregnant while being treated with buprenorphine sublingual tablets, the baby may have signs of withdrawal at birth and that withdrawal is treatable [see Warnings and Precautions (5.5), Use in Specific Populations (8.1)].
- Advise women who are breastfeeding to monitor the infant for drowsiness and difficulty breathing [see Specific Populations (8.2)].
- Inform patients that chronic use of opioids may cause reduced fertility. It is not known whether these effects on fertility are reversible [see Use in Specific Populations (8.3)].
- Advise patients to inform their family members that, in the event of emergency, the treating healthcare providers or emergency room staff should be informed that the patient is physically dependent on an opioid and that the patient is being treated with buprenorphine sublingual tablet.
-
MEDICATION GUIDE
Buprenorphine Sublingual Tablets, CIII
(BUE-pre-NOR-feen)IMPORTANT:Keep buprenorphine sublingual tablet in a secure place away from children. Accidental use by a child is a medical emergency and can result in death. If a child accidentally takes buprenorphine sublingual tablet, get emergency help or call 911 right away. Tell your healthcare provider if you are living in a household where there are small children. What is the most important information I should know about buprenorphine sublingual tablet?
- Buprenorphine sublingual tablet contains a medicine called buprenorphine. Buprenorphine is an opioid that can cause serious and life-threatening breathing problems, especially if you take or use certain other medicines or drugs.
- Talk to your healthcare provider about naloxone. Naloxone is a medicine that is available to patients for the emergency treatment of an opioid overdose, including accidental use of buprenorphine sublingual tablet by a child. If naloxone is given, you must call 911 or get emergency medical help right away to treat an overdose or accidental use of an opioid.
- Buprenorphine sublingual tablets may cause serious and life‐threatening breathing problems. Get emergency help right away if you:
-
- feel faint
- feel dizzy
- are confused
- feel sleepy or uncoordinated
- have blurred vision
- have slurred speech
- are breathing slower than normal
- cannot think well or clearly
- Do not take buprenorphine sublingual tablet with certain medicines. Taking buprenorphine sublingual tablet with other opioid medicines, benzodiazepines, alcohol, or other central nervous system depressants (including street drugs) can cause severe drowsiness, decreased awareness, breathing problems, coma, and death.
- Do not inject (“shoot‐up”) buprenorphine sublingual tablet. Injecting buprenorphine sublingual tablet may cause life‐threatening infections and other serious health problems
- Do not switch from buprenorphine sublingual tablet to other medicines that contain buprenorphinewithout talking with your healthcare provider. The amount of buprenorphine in a dose of buprenorphine sublingual tablet is not the same as in other medicines that contain buprenorphine. Your healthcare provider will prescribe a starting dose of buprenorphine sublingual tablet that may be different than other buprenorphine containing medicines you may have been taking.
- Do not stop taking buprenorphine sublingual tablets suddenly. You could become sick and have withdrawal symptoms because your body has become used to the medicine (physical dependence). Physical dependence is not the same as drug addiction.
- In an emergency, have family members tell emergency department staff that you are physically dependent on an opioid and are being treated with buprenorphine sublingual tablet.
- Never give anyone else your buprenorphine sublingual tablet. They could die from taking it. Selling or giving away buprenorphine sublingual tablets is against the law.
- Store buprenorphine sublingual tablet securely, out of sight and reach of children, and in a location not accessible by others, including visitors to the home.
What is buprenorphine sublingual tablet? - Buprenorphine sublingual tablet is a prescription medicine used to treat opioid addiction in adults and is part of a complete treatment program that also includes counseling and behavioral therapy.
Who should not take buprenorphine sublingual tablet?
Do not take buprenorphine sublingual tabletif you are allergic to buprenorphine.Before taking buprenorphine sublingual tablets, tell yourhealthcare provider about all of your medical conditions, including if you have: - trouble breathing or lung problems
- an enlarged prostate (men)
- head injury or brain problem
- a curve in your spine that affects your breathing
- liver, kidney, or gallbladder problems
- mental health problems
- Addison’s disease
- alcoholism
- adrenal gland or thyroid gland problems
- tooth problems, including a history of cavities
- pregnant or plan to become pregnant.If you take buprenorphine sublingual tablets while pregnant, your baby may have symptoms of opioid withdrawal at birth that could be life‐threatening if not recognized and treated. Talk to your healthcare provider if you are pregnant or plan to become pregnant.
- Breastfeeding or plan to breastfeed. Buprenorphine can pass into your breast milk and harm your baby. Talk to your healthcare provider about the best way to feed your baby if you take buprenorphine sublingual tablets. Monitor your baby for increased drowsiness and breathing problems if you breastfeed during treatment with buprenorphine sublingual tablets.
How should I take buprenorphine sublingual tablet?
Read the Instructions for Use at the end of this Medication Guide for detailed instructions on how to take buprenorphine sublingual tablet.- Take buprenorphine sublingual tablet exactly as prescribed by your healthcare provider. Your healthcare provider may change your dose after seeing how it affects you. Do not change your dose unless your healthcare provider tells you to change it.
- Do not take buprenorphine sublingual tablet more often than prescribed by your healthcare provider.
- Buprenorphine sublingual tabletsis not for occasional or “as needed” use.
- If you are prescribed a dose of 2 or more buprenorphine sublingual tablets at the same time:
- Ask your healthcare provider for instructions on the right way to take buprenorphine sublingual tablet.
- Follow the same instructions every time you take a dose of buprenorphine sublingual tablet.
- Take the entire buprenorphine sublingual tablet. Do not cut, chew, or swallow buprenorphine sublingual tablet because the medicine will not work as well.
- After buprenorphine sublingual tablet is completely dissolved, rinse your mouth with water and swallow. Wait for at least one hour before brushing your teeth.
- Report any problems with your teeth immediately to your healthcare provider and schedule an appointment with a dentist. Tell your dentist that you have started taking buprenorphine sublingual tablets.
- If you miss a dose of buprenorphine sublingual tablet, take it as soon as you remember. If it is almost time for your next dose, skip the missed dose and take the next dose at your regular time. Do not take 2 doses at the same time unless your healthcare provider tells you to. If you are not sure about your dosing, call your healthcare provider.
- Dispose of expired, unwanted, or unused buprenorphine sublingual tablets by promptly flushing down the toilet (if a drug take-back option is not readily available). Visit www.fda.gov/drugdisposal for additional information on disposal of unused medicines.
What should I avoid while taking buprenorphine sublingual tablet? - Do not drive, operate heavy machinery, or perform any other dangerous activities until you know how buprenorphine affects you.Buprenorphine can cause drowsiness and slow reaction times. Buprenorphine can make you sleepy, dizzy, or lightheaded.
- You should not drink alcoholor take prescription or over‐the‐counter medicines that contain alcohol while taking buprenorphine sublingual tablet, because this can lead to loss of consciousness or even death.
What are the possible side effects of buprenorphine sublingual tablets?
Buprenorphine sublingual tablets can cause serious side effects, including:- Trouble breathing.Taking buprenorphine sublingual tablets with other opioid medicines, benzodiazepines, alcohol, or other central nervous system depressants can cause breathing problems that can lead to coma and death.
- Sleepiness, dizziness, and problems with coordination.
- Physical dependence orabuse.
-
Liver problems.Call your healthcare provider right away if you notice any of these symptoms:
- your skin or the white part of your eyes turns yellow (jaundice)
- loss of appetite
- dark or “tea‐colored” urine
- pain, aching, or tenderness on the right side of your stomach area
- light colored stools (bowel movements)
- nausea
- Your healthcare provider should do blood tests to check your liver before you start taking and while you take buprenorphine sublingual tablets.
- Allergic reaction.You may have a rash, hives, swelling of your face, wheezing, low blood pressure, or loss of consciousness. Call your healthcare provider or get emergency help right away.
-
Opioid withdrawal.Call your healthcare provider right away if you get any of these symptoms:
- shaking
- sweating more than normal
- feeling hot or cold more than normal
- runny nose
- watery eyes
- goose bumps
- diarrhea
- vomiting
- muscle aches
- Decrease in blood pressure.You may feel dizzy if you get up too fast from sitting or lying down.
-
The most common side effects of buprenorphine sublingual tablets include:
- headache
- nausea
- vomiting
- constipation
- pain
- increased sweating
- decrease in sleep (insomnia)
- Buprenorphine sublingual tablet may affect fertility in males and females. Talk to your healthcare provider if this is a concern for you.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.General information about the safe and effective use of buprenorphine sublingual tablet.
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not take buprenorphine sublingual tablet for a condition for which it was not prescribed. Do not give buprenorphine sublingual tablet to other people, even if they have the same symptoms you have. It may harm them and it is against the law.
You can ask your doctor or pharmacist for information that is written for healthcare professionals.
For more information call 1-855-361-3993.This Medication Guide has been approved by the U.S. Food and Drug Administration.
Manufactured for:
AvKARE
Pulaski, TN 38478Mfg. Rev. 11/23
AV 03/24 (P)
AvPAK -
INSTRUCTIONS FOR USE
Buprenorphine Sublingual Tablets, CIII
(BUE-pre-NOR-feen)
This “Instructions for Use” contains information on how to correctly takebuprenorphinesublingual tablets.
Important Information You Need to Know Before TakingBuprenorphinesublingual tablets:
- Your healthcare provider should show you how to take buprenorphine sublingual tablets the right way.
Preparing to takebuprenorphinesublingual tablets :
- Put the tablets under your tongue. Let them dissolve completely.
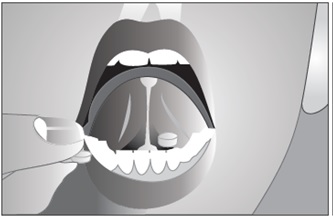
- While buprenorphine sublingual tablet is dissolving, do not chew or swallow the tablet because the medicine will not work as well.
- Talking while the tablet is dissolving can affect how well the medicine in buprenorphine sublingual tablet is absorbed.
- After buprenorphine sublingual tablet is completely dissolved, rinse your mouth with water and swallow. Wait for at least one hour before brushing teeth.
- If you miss a dose of buprenorphine sublingual tablet, take your medicine when you remember. If it is almost time for your next dose, skip the missed dose and take the next dose at your regular time. Do not take 2 doses at the same time unless your healthcare provider tells you to. If you are not sure about your dosing, call your healthcare provider.
- Do not stop taking buprenorphine sublingual tablet suddenly. You could become sick and have withdrawal symptoms because your body has become used to the medicine. Physical dependence is not the same as drug addiction. Your healthcare provider can tell you more about the differences between physical dependence and drug addiction. To have fewer withdrawal symptoms, ask your healthcare provider how to stop using buprenorphine sublingual tablet the right way.
If you take too many buprenorphine sublingual tablets or overdose, call Poison Control or get emergency medical help right away.
Storing Buprenorphine Sublingual tablets- Store buprenorphine sublingual tablets at room temperature between 20° to 25°C (68° to 77°F). Protect from light.
- Keep buprenorphine sublingual tablets in a safe place, out of the sight and reach of children.
- Retain blister card in carton until time of use.
Disposing of Buprenorphine Sublingual tablets:
- Dispose of unused buprenorphine sublingual tablets as soon as you no longer need them.
- Dispose of expired, unwanted or unused buprenorphine sublingual tablets by promptly flushing down the toilet (if a drug take-back option is not readily available). Visit www.fda.gov/drugdisposal for additional information on disposal of unused medicines.
Manufactured for:
AvKARE
Pulaski, TN 38478Mfg. Rev. 11/23
AV 03/24 (P)
AvPAK - PRINCIPAL DISPLAY PANEL - 2 mg
- PRINCIPAL DISPLAY PANEL - 8 mg
-
INGREDIENTS AND APPEARANCE
BUPRENORPHINE
buprenorphine tabletProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 50268-128(NDC:62756-459) Route of Administration SUBLINGUAL DEA Schedule CIII Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength BUPRENORPHINE HYDROCHLORIDE (UNII: 56W8MW3EN1) (BUPRENORPHINE - UNII:40D3SCR4GZ) BUPRENORPHINE 2 mg Inactive Ingredients Ingredient Name Strength LACTOSE MONOHYDRATE (UNII: EWQ57Q8I5X) MANNITOL (UNII: 3OWL53L36A) POVIDONE, UNSPECIFIED (UNII: FZ989GH94E) ANHYDROUS CITRIC ACID (UNII: XF417D3PSL) SODIUM CITRATE, UNSPECIFIED FORM (UNII: 1Q73Q2JULR) BUTYLATED HYDROXYANISOLE (UNII: REK4960K2U) MAGNESIUM STEARATE (UNII: 70097M6I30) STARCH, CORN (UNII: O8232NY3SJ) Product Characteristics Color white (white to off-white) Score no score Shape ROUND (biconvex) Size 6mm Flavor Imprint Code 459 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 50268-128-15 50 in 1 BOX 03/19/2024 1 NDC: 50268-128-11 1 in 1 BLISTER PACK; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA201760 03/19/2024 BUPRENORPHINE
buprenorphine tabletProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 50268-129(NDC:62756-460) Route of Administration SUBLINGUAL DEA Schedule CIII Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength BUPRENORPHINE HYDROCHLORIDE (UNII: 56W8MW3EN1) (BUPRENORPHINE - UNII:40D3SCR4GZ) BUPRENORPHINE 8 mg Inactive Ingredients Ingredient Name Strength LACTOSE MONOHYDRATE (UNII: EWQ57Q8I5X) MANNITOL (UNII: 3OWL53L36A) POVIDONE, UNSPECIFIED (UNII: FZ989GH94E) ANHYDROUS CITRIC ACID (UNII: XF417D3PSL) SODIUM CITRATE, UNSPECIFIED FORM (UNII: 1Q73Q2JULR) BUTYLATED HYDROXYANISOLE (UNII: REK4960K2U) MAGNESIUM STEARATE (UNII: 70097M6I30) STARCH, CORN (UNII: O8232NY3SJ) Product Characteristics Color white (white to off-white) Score no score Shape ROUND (biconvex) Size 10mm Flavor Imprint Code 460 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 50268-129-15 50 in 1 BOX 03/19/2024 1 NDC: 50268-129-11 1 in 1 BLISTER PACK; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA201760 03/19/2024 Labeler - AvPAK (832926666)

© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.