WINLEVI- clascoterone cream
Winlevi by
Drug Labeling and Warnings
Winlevi by is a Prescription medication manufactured, distributed, or labeled by Sun Pharmaceutical Industries, Inc., Cosmo SpA, Curia Spain, S.A.U.. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use WINLEVI Cream safely and effectively. See full prescribing information for WINLEVI Cream.
WINLEVI ®(clascoterone) cream, for topical use
Initial U.S. Approval: 2020INDICATIONS AND USAGE
WINLEVI (clascoterone) cream is an androgen receptor inhibitor indicated for the topical treatment of acne vulgaris in patients 12 years of age and older. ( 1)
DOSAGE AND ADMINISTRATION
DOSAGE FORMS AND STRENGTHS
Cream 1%. ( 3)
CONTRAINDICATIONS
None ( 4)
WARNINGS AND PRECAUTIONS
- Local Irritation: Pruritus, burning, skin redness or peeling may be experienced with WINLEVI cream. If these effects occur, discontinue or reduce the frequency of application of WINLEVI cream. ( 5.1)
- Hypothalamic-pituitary-adrenal (HPA) axis suppression may occur during or after treatment with clascoterone. ( 5.2)
- Attempt to withdraw use if HPA axis suppression develops. ( 5.2)
- Pediatric patients may be more susceptible to systemic toxicity. ( 5.2, 8.4)
- Hyperkalemia: Elevated potassium levels were observed in some subjects during the clinical trials. ( 12.2)
ADVERSE REACTIONS
Most common adverse reactions occurring in 7 to 12% of patients are erythema/reddening, pruritus and scaling/dryness. Additionally, edema, stinging, and burning occurred in >3% of patients and were reported in a similar percentage of subjects treated with vehicle. ( 6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Sun Pharmaceutical Industries, Inc. 1-800-818-4555 or FDA at 1-800-FDA-1088 or http://www.fda.gov/medwatch.
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.
Revised: 7/2022
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
3 DOSAGE FORM AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Local Skin Reactions
5.2 Hypothalamic-pituitary-adrenal (HPA) Axis Suppression
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.4 Pediatric Use
8.5 Geriatric Use
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- * Sections or subsections omitted from the full prescribing information are not listed.
- 1 INDICATIONS AND USAGE
-
2 DOSAGE AND ADMINISTRATION
Cleanse the affected area gently. After the skin is dry, apply a thin uniform layer of WINLEVI cream twice per day, in the morning and the evening, to the affected area. Avoid accidental transfer of WINLEVI cream into eyes, mouth or other mucous membranes. If contact with mucous membranes occurs, rinse thoroughly with water.
WINLEVI cream is for topical use only. WINLEVI cream is not for ophthalmic, oral or vaginal use.
- 3 DOSAGE FORM AND STRENGTHS
- 4 CONTRAINDICATIONS
-
5 WARNINGS AND PRECAUTIONS
5.1 Local Skin Reactions
WINLEVI cream may induce local irritation (erythema/redness, pruritus, scaling/ dryness). Concomitant use with other potentially irritating topical products (medicated or abrasive soaps and cleansers, soaps and cosmetics that have a strong drying effect and products with high concentrations of alcohol, astringents, spices or lime) should be limited.
The product should not be applied to cuts, abrasions, eczematous or sunburned skin.
5.2 Hypothalamic-pituitary-adrenal (HPA) Axis Suppression
Hypothalamic-pituitary-adrenal (HPA) axis suppression was observed and may occur during or after treatment with clascoterone. In the PK trial, all subjects returned to normal HPA axis function at follow-up 4 weeks after stopping treatment [see Clinical Pharmacology (12.2)]. Conditions which augment systemic absorption include use over large surface areas, prolonged use, and the use of occlusive dressings.
If HPA axis suppression develops, an attempt should be made to withdraw the drug.
Pediatric patients may be more susceptible to systemic toxicity.
-
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
In two identical multicenter, randomized, double-blind, vehicle-controlled trials, 1421 subjects 12 years and older with facial acne vulgaris applied WINLEVI cream or vehicle twice daily for 12 weeks. Overall, 62% of the subjects were female, and 38% were male, 91% of the patients were Caucasian, and the mean age was 19.7 years.
Local skin reactions (edema, erythema/redness, pruritus, scaling/dryness, skin atrophy, stinging/burning, striae rubrea, telangiectasia) were observed during the 12-week treatment and occurred in a similar percentage of subjects treated with vehicle. Local skin reactions reported by ≥ 1% of subjects treated with WINLEVI cream are shown in the following table.
Table 1. Incidence of New or Worsening Local Skin Reactions Reported by ≥ 1% of Subjects Treated with WINLEVI Cream After Day 1 in 12-Week Controlled Clinical Trials
WINLEVI Cream 1%
(N=674 a)Vehicle Cream
(N=656 a)aThe denominators for calculating the percentages were the 674 of 709 subjects treated with WINLEVI cream and 656 of 712 subjects treated with vehicle in these trials who had local skin reaction results reported after Day 1.
Edema
24 (3.6%)
23 (3.5%)
Erythema/redness
82 (12.2%)
101 (15.4%)
Pruritus
52 (7.7%)
54 (8.2%)
Scaling/dryness
71 (10.5%)
68 (10.4%)
Skin atrophy
11 (1.6%)
17 (2.6%)
Stinging/burning
28 (4.2%)
28 (4.3%)
Striae rubrae
17 (2.5%)
10 (1.5%)
Telangiectasia
8 (1.2%)
12 (1.8%)
The following adverse reactions associated with the use of WINLEVI cream were identified in clinical trials and long-term safety studies.
Metabolism: hyperkalemia [seeClinical Pharmacology (12.2)]
Reproductive: polycystic ovaries, amenorrhea.
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
There are no available data on WINLEVI cream use in pregnant women to evaluate for a drug-associated risk of major birth defects, miscarriage, or adverse maternal or fetal outcomes. In animal reproduction studies, subcutaneous administration of clascoterone to pregnant rats and rabbits during organogenesis at doses 8 or 39 times the maximum recommended human dose (MRHD), respectively, increased malformations in rats and post-implantation loss and resorptions in rabbits (seeData).
The background risk of major birth defects and miscarriage for the indicated population is unknown. Adverse outcomes in pregnancy occur regardless of the health of the mother or the use of medications. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Data
Animal Data
In an embryofetal development study, clascoterone was administered subcutaneously to pregnant rats at doses of 1, 5, or 25 mg/kg/day during the period of organogenesis. No clascoterone-related maternal toxicity or effects on uterine parameters were noted at doses up to 25 mg/kg/day (336 times the MRHD based on AUC comparison). Clascoterone-related malformations were noted at all dose levels, without a dose relationship. Omphalocele was noted in a single fetus at each dose level. External and visceral malformations (severe dilation of the lateral and third cerebral ventricles; thin skin, small size, and protruding tongue) were noted in two additional fetuses at 1 mg/kg/day (8 times the MRHD based on AUC comparison).
In an embryofetal development study, clascoterone was administered subcutaneously to pregnant rabbits at doses of 0.1, 0.4, or 1.5 mg/kg/day during the period of organogenesis. Post-implantation loss and resorptions were increased at 1.5 mg/kg/day (39 times the MRHD based on AUC comparison). No developmental toxicity was noted at doses up to 0.4 mg/kg/day (12 times the MRHD based on AUC comparison). No clascoterone-related maternal toxicity or fetal malformations were noted at doses up to 1.5 mg/kg/day (39 times the MRHD based on AUC comparison).
In a prenatal and postnatal development study, clascoterone was administered subcutaneously to pregnant rats at doses of 0.5, 2.5, and 12.5 mg/kg/day beginning on gestation day 6 and continuing through lactation day 20. No significant maternal or developmental toxicity was observed at doses up to 12.5 mg/kg/day (163 times the MRHD based on AUC comparison).
8.2 Lactation
Risk Summary
There are no data regarding the presence of clascoterone or metabolite in human milk, the effects on the breastfed infant or the effects on milk production. The lack of clinical data during lactation precludes a clear determination of the risk of clascoterone to an infant during lactation; therefore, the developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for clascoterone and any potential adverse effects on the breastfed child from clascoterone or from the underlying maternal condition.
8.4 Pediatric Use
Safety and effectiveness of WINLEVI cream for the topical treatment of acne vulgaris have been established in 641 pediatric patients, aged 12 to 18 years in two identical multicenter, randomized, double-blind, vehicle-controlled, 12-week trials and 2 open-label pharmacokinetic studies [seeClinical Studies (14)].
Safety and effectiveness of WINLEVI cream for the topical treatment of acne vulgaris has not been established in pediatric patients under 12 years of age.
Hypothalamic-pituitary-adrenal (HPA) axis suppression was observed in 2/22 (9%) adolescent subjects. All subjects returned to normal HPA axis function at follow-up 4 weeks after stopping the treatment [seeClinical Pharmacology (12.2)].Children may be more susceptible to systemic toxicity when treated with clascoterone [seePharmacodynamics (12.2)].
8.5 Geriatric Use
Clinical studies of WINLEVI cream did not include sufficient numbers of subjects aged 65 years of age and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
-
11 DESCRIPTION
WINLEVI (clascoterone) cream contains clascoterone, an androgen receptor inhibitor, in a cream base for topical dermatologic use. WINLEVI cream is a white to almost white cream.
Chemically, clascoterone is cortexolone-17α propionate. Clascoterone is a white to almost white powder, practically insoluble in water. The compound has the empirical formula C 24H 34O 5and molecular weight of 402.5 g/mol. The structural formula is shown below.
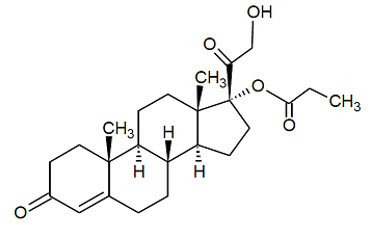
Each gram of WINLEVI cream 1% contains 10 mg of clascoterone in a cream base of cetyl alcohol, citric acid monohydrate, edetate disodium, mineral oil, mono- and di-glycerides, polysorbate 80, propylene glycol, purified water, and vitamin E.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Clascoterone is an androgen receptor inhibitor. The mechanism of action of WINLEVI cream for the topical treatment of acne vulgaris is unknown.
12.2 Pharmacodynamics
Hypothalamic-Pituitary-Adrenal (HPA) Axis Suppression
HPA axis suppression was evaluated in adult (n=20) and adolescent (n=22) subjects with acne vulgaris following twice daily application of WINLEVI cream for 2 weeks in the pharmacokinetic study described in Section 12.3. HPA axis suppression indicated by 30-minute post-stimulation serum cortisol level of ≤18 mcg/dL was observed in 1/20 (5%) of adult subjects and 2/22 (9%) of adolescent subjects at Day 14. All subjects returned to normal HPA axis function at follow-up 4 weeks after the end of treatment.
12.3 Pharmacokinetics
Absorption
Following topical treatment of WINLEVI cream for 2 weeks with a mean dose of approximately 6 grams applied twice daily to adult subjects with moderate to severe acne vulgaris (n=20), systemic concentrations of clascoterone were at steady state by Day 5. On Day 14, the mean ± SD maximum plasma concentration (C max) was 4.5 ± 2.9 ng/mL, the mean ± SD area under the plasma concentration-time over the dosing interval (AUC ꞇ) was 37.1 ± 22.3 h*ng/mL and the mean ± SD average plasma concentration (C avg) was 3.1 ± 1.9 ng/mL.
Distribution
Plasma protein binding of clascoterone is 84% to 89% and is independent of concentrations, in vitro.
Elimination
Metabolism
Following topical treatment with WINLEVI cream, the plasma concentrations of cortexolone, a possible primary metabolite of clascoterone, were detectable and generally below or near the lower limit of quantitation (0.5 ng/mL) in subjects ≥12 years of age with acne vulgaris.
The in vitro study indicated that incubation of 10 µmol/L clascoterone with human cryopreserved hepatocytes generated cortexolone as the possible primary metabolite and other unidentified metabolites, including conjugated metabolites.
Specific Populations
Pediatric Patients
In adolescent subjects ≥ 12 to <18 years of age (n=22) after 2 weeks of twice daily treatment with mean dose of approximately 6 grams of WINLEVI cream (or mean dose of approximately 4 grams in younger, smaller subjects), steady-state concentrations of clascoterone were achieved by Day 5. Clascoterone systemic exposure in adolescents was similar to those observed in adults.
Drug Interaction Studies
Clinical Studies
No clinical studies evaluating the drug interaction potential of WINLEVI cream have been conducted.
In Vitro Studies
CYP Enzymes:Clascoterone inhibited CYP 1A2, 2B6, 2C8, 2C9, 2C19, 2D6, 2E1, or 3A4 with an IC 50value of >40 µM. Clascoterone up to 30 µM did not induce CYP 1A2, 2B6, or 3A4. These findings suggest that WINLEVI cream has no clinically meaningful effect on the PK of drugs metabolized by CYP 1A2, 2B6, 2C8, 2C9, 2C19, 2D6, 2E1, or 3A4.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Clascoterone cream (0.1%, 1%, or 5%) was not carcinogenic after daily topical administration in a 2-year carcinogenicity study in rats. An increased incidence of the non-neoplastic finding of atrophy of the skin and subcutis at the application site was reported in males and females treated with 1% and 5% clascoterone cream.
Clascoterone was not mutagenic in the Ames reverse mutation assay and was not clastogenic in the in vitro human lymphocyte chromosomal aberration assay. In rats, clascoterone administered via subcutaneous injection did not induce micronuclei in the bone marrow at 500 or 1000 mg/kg but a slight increase in micronuclei occurred in 2 of 5 rats at 2000 mg/kg. The response was considered equivocal. Overall, the weight of evidence indicates that clascoterone does not represent a genotoxic risk.
In a fertility and early embryonic development study in rats, clascoterone was administered subcutaneously at doses of 0.5, 2.5, or 12.5 mg/kg/day from 2 – 4 weeks before mating through mating. Clascoterone increased pre-implantation loss at 12.5 mg/kg/day (163 times the MRHD based on AUC comparison). Clascoterone had no effects on mating or fertility in rats at doses up to 12.5 mg/kg/day (163 times the MRHD based on AUC comparison). No effects were noted on development at doses up to 2.5 mg/kg/day (33 times the MRHD based on AUC comparison).
-
14 CLINICAL STUDIES
The safety and efficacy of WINLEVI cream 1% applied twice daily for 12 weeks for the treatment of acne vulgaris were assessed in two identically-designed, multicenter, randomized, double-blind, vehicle-controlled clinical trials (Trial 1 [NCT02608450] and Trial 2 [NCT02608476]) enrolling 1440 subjects with facial acne vulgaris. The trials enrolled subjects 9 years or older with Investigator's Global Assessment (IGA) of moderate or severe facial acne vulgaris (score of 3 or 4), 30 to 75 inflammatory lesions (papules, pustules and nodules), and 30 to 100 non-inflammatory lesions (open and closed comedones).
A total of 1421 subjects 12 years and older with facial acne vulgaris were enrolled. Of these subjects, 641 (45%) were 12 to 17 years of age, and 780 (55%) were 18 years of age or older. In addition, 62% of the subjects were female, and 91% were Caucasian. At baseline, subjects had a mean inflammatory lesion count of 42.4 and a mean non-inflammatory lesion count of 61.4. Additionally, approximately 83% of subjects had an IGA score of 3 ("moderate").
Efficacy was assessed at Week 12 by the proportion of subjects in each treatment group with at least a 2-point reduction in IGA compared to baseline and an IGA score of 0 (clear) or 1 (almost clear), absolute change and percent change from baseline in non-inflammatory and inflammatory lesions. The IGA success rate and mean absolute and percent reduction from baseline in acne lesion counts after 12 weeks of treatment for subjects 12 years of age and older are presented in the following table.
Table 2. Clinical Efficacy of WINLEVI Cream 1% in Subjects with Acne Vulgaris at Week 12
Trial 1
Trial 2
WINLEVI Cream 1%
N=342Vehicle Cream
N=350WINLEVI Cream 1%
N=367Vehicle Cream
N=362IGA Successa
18.8%
8.7%
20.9%
6.6%
Difference from Vehicle
(95% CI)10.1%
(4.1%, 16.0%)14.3%
(8.9%, 19.7%)Non-inflammatory Lesions
Mean Absolute Reduction
20.4
13.0
19.5
10.8
Difference from Vehicle
(95% CI)7.3
(3.5, 11.1)8.7
(4.5, 12.4)Mean Percent Reduction
32.6%
21.8%
29.6%
15.7%
Difference from Vehicle
(95% CI)10.8%
(3.9%, 17.6%)13.8%
(7.5%, 20.1%)Inflammatory Lesions
Mean Absolute Reduction
19.3
15.4
20.1
12.6
Difference from Vehicle
(95% CI)3.9
(1.3, 6.5)7.5
(5.2, 9.9)Mean Percent Reduction
44.6%
36.3%
47.1%
29.7%
Difference from Vehicle
(95% CI)8.3%
(2.2%, 14.4%)17.5%
(11.8%, 23.1%)aInvestigator Global Assessment (IGA) success was defined as at least a 2-point reduction in IGA compared to baseline and an IGA score of 0 (clear) or 1 (almost clear).
-
16 HOW SUPPLIED/STORAGE AND HANDLING
WINLEVI cream 1% is supplied in an epoxy-lined aluminum blind-end tube with a polypropylene cap closure:
NDC: 47335-994-36
60-gram tube
- 17 PATIENT COUNSELING INFORMATION
- SPL UNCLASSIFIED SECTION
-
PATIENT PACKAGE INSERT
Patient Information
WINLEVI (Win-levē)
(clascoterone) creamImportant Information:WINLEVI cream is for use on the skin only (topical). Do not use WINLEVI cream in or on your eyes, mouth, or vagina.
What is WINLEVI cream?
WINLEVI cream is a prescription medicine used on the skin (topical) to treat acne vulgaris in people 12 years of age and older.
It is not known if WINLEVI cream is safe and effective in children under 12 years of age.- Before using WINLEVI cream, tell your healthcare provider about all of your medical conditions, including if you:
- have skin problems, including eczema, cuts or sunburn
- are pregnant or plan to become pregnant. It is not known if WINLEVI cream will harm your unborn baby.
- are breastfeeding or plan to breastfeed. It is not known if WINLEVI cream passes into your breast milk. Talk to your healthcare provider about the best way to feed your baby during treatment with WINLEVI cream.
Tell your healthcare provider about the medicines you take,including prescription and over-the-counter medicines, vitamins, and herbal supplements.How should I use WINLEVI cream?
- Use WINLEVI cream exactly as your healthcare provider tells you to use it.
- Before applying WINLEVI cream, gently wash and dry the affected skin area.
- After the skin is dry, apply a thin even layer of WINLEVI cream to the affected areas 2 times each day, in the morning and the evening.
- Wash your hands after applying WINLEVI cream.
What should I avoid while using WINLEVI cream?
- Avoid using WINLEVI cream on skin areas with cuts, abrasions, eczema, or on sunburned skin.
- Avoid getting WINLEVI cream into your eyes, lips, mouth, corners of the nose, or mucous membranes. If contact with mucous membranes happens, rinse well with water.
- Avoid using skin products that may dry or irritate your skin such as:
- medicated or abrasive soaps and cleansers
- soaps, cleansers, and cosmetics that have strong skin drying effects
- products that contain high amounts of alcohol
- astringents, spices, or lime
What are the possible side effects of WINLEVI cream?
WINLEVI cream can cause serious side effects, including:- Local skin reactions.WINLEVI cream may cause local skin irritation including itching, burning, skin redness or peeling.
- Symptoms of a disorder where the adrenal gland does not make enough of certain hormones (adrenal insufficiency) during treatment with WINLEVI.Your healthcare provider may stop your treatment with WINLEVI if you develop any adrenal problems.
The most common side effects of WINLEVI creaminclude reddening, scaling or dryness, and itching of the skin being treated.
These are not all of the possible side effects of WINLEVI cream.
Call your healthcare provider for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
You may also report side effects to Sun Pharmaceutical Industries, Inc. by calling 1-800-818-4555.How should I store WINLEVI cream?
- Store WINLEVI cream at room temperature between 68°F and 77°F (20°C to 25°C). Do not freeze.
- Throw away (discard) the unused portion 180 days after the date of dispensing or 1 month after first opening, whichever is sooner.
Keep WINLEVI cream and all medicines out of the reach of children.
General Information about the safe and effective use of WINLEVI cream.
Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. Do not use WINLEVI cream for a condition for which it was not prescribed. Do not give WINLEVI cream to other people, even if they have the same symptoms you have. It may harm them. You can ask your healthcare provider or pharmacist for information about WINLEVI cream that is written for health professionals.What are the ingredients in WINLEVI cream?
Active ingredient:clascoterone
Inactive ingredients:cetyl alcohol, citric acid monohydrate, edetate disodium, mineral oil, mono- and di-glycerides, polysorbate 80, propylene glycol, purified water, and vitamin E.
Manufactured in Italy for: Sun Pharmaceutical Industries Limited
Distributed by: Sun Pharmaceutical Industries, Inc., Cranbury, NJ 08512
WINLEVI is a licensed trademark of Cassiopea, S.p.A. exclusively licensed by Sun Pharmaceutical Industries, Ltd.
US Patents: https://www.cassiopea.com/patents
©2022 Sun Pharmaceutical Industries Limited, All right reserved.
This Patient Information has been approved by the U.S. Food and Drug Administration
Issued: 07/2022
2000405-3
- PRINCIPAL DISPLAY PANEL
-
INGREDIENTS AND APPEARANCE
WINLEVI
clascoterone creamProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 47335-994 Route of Administration TOPICAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength CLASCOTERONE (UNII: XN7MM8XG2M) (CLASCOTERONE - UNII:XN7MM8XG2M) CLASCOTERONE 1 g in 100 g Inactive Ingredients Ingredient Name Strength PROPYLENE GLYCOL (UNII: 6DC9Q167V3) 25 g in 100 g WATER (UNII: 059QF0KO0R) GLYCERYL MONO- AND DICAPRYLOCAPRATE (UNII: U72Q2I8C85) MINERAL OIL (UNII: T5L8T28FGP) CETYL ALCOHOL (UNII: 936JST6JCN) POLYSORBATE 80 (UNII: 6OZP39ZG8H) EDETATE DISODIUM (UNII: 7FLD91C86K) ALPHA-TOCOPHEROL (UNII: H4N855PNZ1) Product Characteristics Color white Score Shape Size Flavor Imprint Code Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 47335-994-36 1 in 1 CARTON 10/04/2021 1 60 g in 1 TUBE; Type 0: Not a Combination Product 2 NDC: 47335-994-94 12 in 1 CASE 10/04/2021 2 NDC: 47335-994-40 1 in 1 CARTON 2 2 g in 1 TUBE; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA213433 10/04/2021 Labeler - Sun Pharmaceutical Industries, Inc. (146974886) Establishment Name Address ID/FEI Business Operations Cosmo SpA 630431955 manufacture(47335-994) Establishment Name Address ID/FEI Business Operations Curia Spain, S.A.U. 563371111 api manufacture(47335-994)
Trademark Results [Winlevi]
Mark Image Registration | Serial | Company Trademark Application Date |
|---|---|
 WINLEVI 88517589 not registered Live/Pending |
CASSIOPEA S.P.A. 2019-07-16 |
 WINLEVI 86620123 5234655 Live/Registered |
CASSIOPEA SPA 2015-05-05 |
 WINLEVI 86592424 5230186 Live/Registered |
CASSIOPEA SPA 2015-04-09 |
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.