LITFULO- ritlecitinib capsule
Litfulo by
Drug Labeling and Warnings
Litfulo by is a Prescription medication manufactured, distributed, or labeled by U.S. Pharmaceuticals, Pfizer Inc, Pfizer Ireland Pharmaceuticals Unlimited Company, Pfizer Manufacturing Deutschland GmbH. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use LITFULO safely and effectively. See full prescribing information for LITFULO.
LITFULO™ (ritlecitinib) capsules, for oral use
Initial U.S. Approval: 2023WARNING: SERIOUS INFECTIONS, MORTALITY, MALIGNANCY, MAJOR ADVERSE CARDIOVASCULAR EVENTS (MACE), and THROMBOSIS
See full prescribing information for complete boxed warning.
- Increased risk of serious bacterial, fungal, viral, and opportunistic infections that may lead to hospitalization or death, including tuberculosis (TB). Interrupt treatment if serious infection occurs until the infection is controlled. LITFULO should not be given to patients with active tuberculosis. Test for latent TB before and during therapy; start treating latent TB prior to use. Monitor all patients for active TB during treatment, even patients with initial negative, latent TB test. (5.1). Monitor all patients for signs and symptoms of infection during and after treatment with LITFULO. (5.1)
- Higher rate of all-cause mortality, including sudden cardiovascular death with another Janus kinase inhibitor (JAK) vs. TNF blockers in rheumatoid arthritis (RA) patients. LITFULO is not approved for use in RA patients. (5.2)
- Malignancies were reported in patients treated with LITFULO (5.3). Higher rate of lymphomas and lung cancers with another JAK inhibitor vs. TNF blockers in RA patients.
- Higher rate of MACE (defined as cardiovascular death, myocardial infarction, and stroke) with another JAK inhibitor vs. TNF blockers in RA patients. (5.4).
- Thrombosis has occurred in patients treated with LITFULO. Increased incidence of pulmonary embolism, venous and arterial thrombosis with another JAK inhibitor vs. TNF blockers. (5.5)
INDICATIONS AND USAGE
DOSAGE AND ADMINISTRATION
DOSAGE FORMS AND STRENGTHS
Capsules: 50 mg of ritlecitinib (3)
CONTRAINDICATIONS
LITFULO is contraindicated in patients with known hypersensitivity to ritlecitinib or any of its excipients. (4)
WARNINGS AND PRECAUTIONS
- Hypersensitivity: Discontinue LITFULO if a clinically significant hypersensitivity reaction occurs. (5.6)
- Laboratory Abnormalities: Perform ALC and platelet counts prior to LITFULO initiation. Treatment interruption or discontinuation are recommended based on ALC and platelet count abnormalities. (5.7)
- Vaccinations: Avoid use of live vaccines during or shortly prior to LITFULO treatment. (5.8)
ADVERSE REACTIONS
Most common adverse reactions (incidence ≥1%) are headache, diarrhea, acne, rash, urticaria, folliculitis, pyrexia, atopic dermatitis, dizziness, blood creatine phosphokinase increased, herpes zoster, red blood cell count decreased, and stomatitis. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Pfizer Inc. at 1-800-438-1985 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
- Certain CYP3A substrates: Additional monitoring and dose adjustment of CYP3A substrate should be considered. (7.1)
- Certain CYP1A2 substrates: Additional monitoring and dose adjustment of CYP1A2 substrate should be considered. (7.1)
- Certain CYP3A inducers: Coadministration with strong inducers of CYP3A is not recommended. (7.2)
USE IN SPECIFIC POPULATIONS
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide.
Revised: 6/2023
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
WARNING: SERIOUS INFECTIONS, MORTALITY, MALIGNANCY, MAJOR ADVERSE CARDIOVASCULAR EVENTS (MACE), and THROMBOSIS
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Evaluations and Immunizations Prior to Treatment Initiation
2.2 Recommended Dosage
2.3 Patients with Severe Hepatic Impairment
2.4 Treatment Interruption or Discontinuation
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Serious Infections
5.2 Mortality
5.3 Malignancy and Lymphoproliferative Disorders
5.4 Major Adverse Cardiovascular Events (MACE)
5.5 Thromboembolic Events
5.6 Hypersensitivity
5.7 Laboratory Abnormalities
5.8 Vaccinations
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
7 DRUG INTERACTIONS
7.1 Effects of LITFULO on Other Drugs
7.2 Effects of Other Drugs on LITFULO
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.4 Pediatric Use
8.5 Geriatric Use
8.6 Hepatic Impairment
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
13.2 Animal Toxicology and Pharmacology
14 CLINICAL STUDIES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- * Sections or subsections omitted from the full prescribing information are not listed.
-
BOXED WARNING
(What is this?)
WARNING: SERIOUS INFECTIONS, MORTALITY, MALIGNANCY, MAJOR ADVERSE CARDIOVASCULAR EVENTS (MACE), and THROMBOSIS
- Increased risk of serious bacterial, fungal, viral and opportunistic infections leading to hospitalization or death, including tuberculosis (TB). Interrupt treatment if serious infection occurs until the infection is controlled. LITFULO should not be given to patients with active tuberculosis. Test for latent TB before and during therapy; treat latent TB prior to use. Monitor all patients for active TB during treatment, even patients with initial negative, latent TB test. (5.1)
- Higher rate of all-cause mortality, including sudden cardiovascular death with another Janus kinase inhibitor (JAK) vs. TNF blockers in rheumatoid arthritis (RA) patients. LITFULO is not approved for use in RA patients. (5.2)
- Malignancies have occurred in patients treated with LITFULO [see Warnings and Precautions (5.3)]. Higher rate of lymphomas and lung cancers with another JAK inhibitor vs. TNF blockers in RA patients. (5.3)
- Higher rate of MACE (defined as cardiovascular death, myocardial infarction, and stroke) with another JAK inhibitor vs. TNF blockers in RA patients. (5.4)
- Thrombosis has occurred in patients treated with LITFULO. Increased incidence of pulmonary embolism, venous and arterial thrombosis with another JAK inhibitor vs. TNF blockers. (5.5)
- 1 INDICATIONS AND USAGE
-
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Evaluations and Immunizations Prior to Treatment Initiation
Perform the following evaluations prior to LITFULO initiation:
- Tuberculosis (TB) infection evaluation: LITFULO initiation is not recommended in patients with active TB. For patients with latent TB or those with a negative latent TB test who are at high risk for TB, start preventive therapy for latent TB prior to initiation of LITFULO [see Warnings and Precautions (5.1)].
- Viral hepatitis screening in accordance with clinical guidelines: LITFULO initiation is not recommended in patients with hepatitis B or hepatitis C [see Warnings and Precautions (5.1)].
- Treatment with LITFULO should not be initiated in patients with an absolute lymphocyte count (ALC) <500/mm3 or a platelet count <100,000/mm3 [see Warnings and Precautions (5.7)].
- Update immunizations according to current immunization guidelines [see Warnings and Precautions (5.8)].
2.2 Recommended Dosage
The recommended dosage of LITFULO is 50 mg orally once daily with or without food [see Clinical Pharmacology (12.3)].
Swallow capsules whole. Do not crush, split, or chew LITFULO capsules.
If a dose is missed, administer the dose as soon as possible unless it is less than 8 hours before the next dose, in which case, skip the missed dose. Thereafter, resume dosing at the regular scheduled time.
2.3 Patients with Severe Hepatic Impairment
LITFULO is not recommended in patients with severe (Child Pugh C) hepatic impairment [see Use in Specific Populations (8.6) and Clinical Pharmacology (12.3)].
2.4 Treatment Interruption or Discontinuation
If treatment interruption is indicated, a temporary treatment interruption for less than 6 weeks is not expected to result in significant loss of regrown scalp hair.
Hematologic Abnormalities
Recommendations for LITFULO treatment interruption or discontinuation for hematologic abnormalities are summarized in Table 1.
Table 1. Laboratory Monitoring Guidance Laboratory Measure Recommendation ALC = absolute lymphocyte count. Platelet Count
Treatment should be discontinued if platelet count is <50,000/mm3
Lymphocytes
Treatment should be interrupted if ALC is <500/mm3 and may be restarted once ALC return above this value.
ALC and platelet counts are recommended before treatment initiation and at 4 weeks after treatment initiation, and thereafter according to routine patient management [see Warnings and Precautions (5.7)].
- 3 DOSAGE FORMS AND STRENGTHS
-
4 CONTRAINDICATIONS
LITFULO is contraindicated in patients with known hypersensitivity to ritlecitinib or any of its excipients [see Warnings and Precautions (5.6)].
-
5 WARNINGS AND PRECAUTIONS
5.1 Serious Infections
Serious infections have been reported in patients receiving LITFULO. The most frequent serious infections have been appendicitis, COVID-19 infection (including pneumonia), and sepsis [see Adverse Reactions (6.1)]. Among opportunistic infections, multi-dermatomal herpes zoster was reported with LITFULO.
Avoid use of LITFULO in patients with an active, serious infection. Consider the risks and benefits of treatment prior to initiating LITFULO in patients:
- with chronic or recurrent infection
- who have been exposed to TB
- with a history of serious infection or an opportunistic infection
- who have resided or traveled in areas of endemic TB or mycoses, or
- with underlying conditions that may predispose them to infection
Closely monitor patients for the development of signs and symptoms of infection during and after treatment with LITFULO. Interrupt LITFULO if a patient develops a serious or opportunistic infection. A patient who develops a new infection during treatment with LITFULO should undergo prompt and complete diagnostic testing appropriate for an immunocompromised patient, appropriate antimicrobial therapy should be initiated, and the patient should be closely monitored. LITFULO may be resumed once the infection is controlled.
Tuberculosis
Screen patients for tuberculosis (TB) before starting therapy. LITFULO should not be given to patients with active TB. Anti-TB therapy should be started prior to initiating therapy with LITFULO in patients with a new diagnosis of latent TB or previously untreated latent TB. In patients with a negative latent TB test, consider anti-TB therapy before initiating treatment with LITFULO in those at high risk and consider screening patients at high risk for TB during treatment with LITFULO.
Viral Reactivation
Viral reactivation, including cases of herpes virus reactivation (e.g., herpes zoster), was reported in clinical trials [see Adverse Reactions (6.1)]. If a patient develops herpes zoster, consider interrupting treatment until the episode resolves.
Screening for viral hepatitis should be performed in accordance with clinical guidelines before starting therapy with LITFULO. Patients with evidence of HIV infection or hepatitis B or C infection were excluded from clinical trials.
5.2 Mortality
In a large, randomized, postmarketing safety study of another JAK inhibitor in RA patients 50 years of age and older with at least one cardiovascular risk factor, a higher rate of all-cause mortality, including sudden cardiovascular death, was observed in patients treated with the JAK inhibitor compared with TNF blockers. Consider the benefits and risks for the individual patient prior to initiating or continuing therapy with LITFULO.
5.3 Malignancy and Lymphoproliferative Disorders
Malignancies, including non-melanoma skin cancer (NMSC), were observed in clinical trials of LITFULO [see Adverse Reactions (6.1)].
In a large, randomized, postmarketing safety study of another JAK inhibitor in RA patients, a higher rate of malignancies (excluding non-melanoma skin cancer (NMSC)) was observed in patients treated with the JAK inhibitor compared to those treated with TNF blockers. A higher rate of lymphomas was observed in patients treated with the JAK inhibitor compared to those treated with TNF blockers. A higher rate of lung cancers was observed in current or past smokers treated with the JAK inhibitor compared to those treated with TNF blockers. In this study, current or past smokers had an additional increased risk of overall malignancies.
The risks and benefits of ritlecitinib treatment should be considered prior to initiating or continuing therapy in patients with a known malignancy other than a successfully treated NMSC or cervical cancer.
Periodic skin examination is recommended for patients who are at increased risk for skin cancer.
5.4 Major Adverse Cardiovascular Events (MACE)
In a large, randomized, postmarketing safety study of another JAK inhibitor in RA patients 50 years of age and older with at least one cardiovascular risk factor, a higher rate of major adverse cardiovascular events (MACE) defined as cardiovascular death, non-fatal myocardial infarction (MI), and non-fatal stroke was observed with the JAK inhibitor compared to those treated with TNF blockers. Patients who are current or past smokers are at additional increased risk.
Consider the benefits and risks for the individual patient prior to initiating or continuing therapy with LITFULO, particularly in patients who are current or past smokers and patients with other cardiovascular risk factors. Patients should be informed about the symptoms of serious cardiovascular events and the steps to take if they occur. Discontinue LITFULO in patients that have experienced a myocardial infarction or stroke.
5.5 Thromboembolic Events
An event of pulmonary embolism (PE) was reported in a patient receiving LITFULO [see Adverse Reactions (6.1)]. In a ritlecitinib higher dosing group, 1 patient reported an event of retinal artery occlusion.
In a large, randomized, postmarketing safety study of another JAK inhibitor in RA patients 50 years of age and older with at least one cardiovascular risk factor, higher rates of overall thrombosis, DVT, and PE were observed compared to those treated with TNF blockers.
Avoid LITFULO in patients who may be at increased risk of thrombosis. If symptoms of thrombosis or embolism occur, patients should interrupt LITFULO and be evaluated promptly and treated appropriately.
5.6 Hypersensitivity
Serious reactions including anaphylactic reactions, urticaria and rash have been observed in patients receiving LITFULO in clinical trials. If a clinically significant hypersensitivity reaction occurs, discontinue LITFULO and institute appropriate therapy [see Adverse Reactions (6.1)].
5.7 Laboratory Abnormalities
Treatment with LITFULO was associated with decreases in lymphocytes and platelets [see Adverse Reactions (6.1)].
Prior to LITFULO initiation, perform ALC and platelet counts [see Dosage and Administration (2.1)]. After initiating treatment with LITFULO, treatment interruption or discontinuation are recommended based on ALC and platelet count abnormalities [see Dosage and Administration (2.4)].
Liver Enzyme Elevations – Treatment with LITFULO was associated with increased incidence of liver enzyme elevation compared to placebo. Increases of ALT ≥5 times the upper limit of normal (ULN) and increases of AST ≥5 times the ULN were observed in patients in LITFULO clinical trials. Evaluate at baseline and thereafter according to routine patient management. Prompt investigation of the cause of liver enzyme elevation is recommended to identify potential cases of drug-induced liver injury. If increases in ALT or AST are observed and drug-induced liver injury is suspected, interrupt LITFULO until this diagnosis is excluded.
Creatine Phosphokinase (CPK) Elevations – Treatment with LITFULO was associated with increased incidence of CPK elevation compared to placebo.
5.8 Vaccinations
No data are available on the response to vaccination in patients receiving LITFULO. Use of live attenuated vaccines should be avoided during or shortly prior to initiating treatment. Prior to initiating LITFULO, it is recommended that patients be brought up to date with all immunizations, including prophylactic herpes zoster vaccinations, in agreement with current immunization guidelines.
-
6 ADVERSE REACTIONS
The following clinically significant adverse reactions are described elsewhere in the labeling:
- Serious Infections [see Warnings and Precautions (5.1)]
- Malignancy and Lymphoproliferative Disorders [see Warnings and Precautions (5.3)]
- Thromboembolic Events [see Warnings and Precautions (5.5)]
- Hypersensitivity [see Warnings and Precautions (5.6)]
- Laboratory Abnormalities [see Warnings and Precautions (5.7)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The safety of LITFULO was evaluated in three randomized, placebo-controlled clinical trials and one long-term trial in subjects with alopecia areata, including alopecia totalis and alopecia universalis, who were 12 years of age and older. A total of 1628 subjects were treated with LITFULO representing 2085 subject-years of exposure. There were 1011 subjects with at least 1 year of exposure to LITFULO. In the placebo-controlled period of clinical trials in alopecia areata, a total of 668 subjects were exposed to LITFULO with 130 receiving 50 mg once daily for up to 24 weeks. The median age of subjects was 33 years, 105 (11.9%) subjects were 12 to <18 years old and 22 (2.5%) subjects were 65 years of age or older. The majority of subjects were White (70.7%) and female (63.6%).
Adverse reactions occurring at ≥1% in the treated groups and at a higher rate than placebo are presented in Table 2. A total of 2 (1.5%) subjects treated with LITFULO 50 mg were discontinued from the trials due to adverse reactions.
Table 2. Adverse Reactions in Clinical Trials of LITFULO for the Treatment of Alopecia Areata* LITFULO
50 mg
N=130
n (%)Placebo
N=213
n (%)- * Reported in ≥1% of subjects and at a higher rate than placebo for up to 24 weeks.
- † Headache includes headache and migraine.
- ‡ Diarrhea includes diarrhea and frequent bowel movements.
- § Acne includes acne and acne pustular.
- ¶ Rash includes rash and dermatitis allergic.
Headache†
14 (10.8)
18 (8.5)
Diarrhea‡
13 (10.0)
8 (3.8)
Acne§
8 (6.2)
10 (4.7)
Rash¶
7 (5.4)
2 (0.9)
Urticaria
6 (4.6)
3 (1.4)
Folliculitis
4 (3.1)
4 (1.9)
Pyrexia
4 (3.1)
0
Dermatitis atopic
3 (2.3)
1 (0.5)
Dizziness
3 (2.3)
3 (1.4)
Blood creatine phosphokinase increased
2 (1.5)
0
Herpes zoster
2 (1.5)
0
Red blood cell count decreased
2 (1.5)
0
Stomatitis
2 (1.5)
0
Specific Adverse Reactions
Exposure adjusted incidence rates were adjusted by clinical trial size for all adverse reactions reported in this section.
Overall Infections
In the placebo-controlled trials, for up to 24 weeks, overall infections were reported in 66 subjects (80.35 per 100 subject-years) treated with placebo and 43 subjects (74.53 per 100 subject-years) treated with LITFULO 50 mg. Across clinical trials, including the long-term trial, overall infections were reported in 645 subjects (50.71 per 100 subject-years) treated with LITFULO 50 mg or higher.
Serious Infections
In the placebo-controlled trials, for up to 24 weeks, 3 subjects reported serious infections across all ritlecitinib doses studied. Across clinical trials, including the long-term trial, serious infections were reported in 12 subjects (0.66 per 100 subject-years) treated with LITFULO 50 mg or higher. The most common serious infections were related to appendicitis, COVID-19 infection (including pneumonia), and sepsis.
Herpes Zoster
In the placebo-controlled trials, for up to 24 weeks, herpes zoster was reported in 4 subjects across all ritlecitinib doses studied and 0 subjects treated with placebo. Across clinical trials, including the long-term trial, herpes zoster was reported in 21 subjects (1.17 per 100 subject-years) treated with LITFULO 50 mg or higher. Opportunistic infections of multi-dermatomal herpes zoster were reported in 1 subject (0.50 per 100 subject-years) treated with the ritlecitinib higher dose in the placebo-controlled trials and 2 subjects (0.1 per 100 subject-years) treated with LITFULO 50 mg or higher in all clinical trials.
Malignancy
In the placebo-controlled trials, for up to 24 weeks, 1 malignancy (breast cancer) was reported in 1 subject (1.33 per 100 subject-years) treated with ritlecitinib higher dose and no malignancy was reported in subjects treated with placebo. Across clinical trials, including the long-term trial, malignancies excluding NMSC were reported in 7 subjects (0.37 per 100 subject-years) treated with LITFULO 50 mg or higher.
Thromboembolic Events
Across clinical trials, including the long-term trial, pulmonary embolism (PE) was reported in 1 subject (0.06 per 100 subject-years) treated with LITFULO. There was 1 report of retinal artery occlusion and 1 report of acute myocardial infarction.
Urticaria
In the placebo-controlled trials, for up to 24 weeks, urticaria was reported in 28 subjects treated in all ritlecitinib doses studied and 3 subjects treated with placebo. The rate of urticaria was 8.23 per 100 subject-years in subjects treated with ritlecitinib 50 mg and 4.03 per 100 subject-years in subjects treated with placebo. Across clinical trials, including the long-term trial, urticaria was reported in 76 subjects treated with LITFULO 50 mg or higher. Among all subjects treated with ritlecitinib 50 mg or higher in the integrated safety analysis, the rate of urticaria was 4.10 per 100 subject-years. The median time to onset of an initial event was 8 weeks; median duration of urticaria was 7 days. Most of the cases were mild to moderate in severity.
Decreased Lymphocyte Counts
Across clinical trials, including the long-term trial confirmed ALC <500/mm3 occurred in 1 subject (<0.1%) treated with LITFULO 50 mg. Age appeared to be a risk factor for lower ALC in subjects ≥65 years of age.
Decreased Platelet Count
In the placebo-controlled trials, for up to 24 weeks, treatment with LITFULO was associated with a decrease in platelet count. Maximum effects on platelets were observed within 4 weeks, after which platelet count remained stable at a lower level with continued therapy. Across clinical trials, including the long-term trial, 1 subject (<0.1%) had a confirmed platelet count <100,000/mm3. No subject had a confirmed platelet count <75,000/mm3.
Creatine Phosphokinase (CPK) Elevations
In the placebo-controlled trials, for up to 24 weeks, events of blood CPK increased were reported in 2 (1.5%) subjects treated with LITFULO 50 mg and 0 subjects treated with placebo.
Liver Enzyme Elevations
In the placebo-controlled trials, for up to 24 weeks, events of increases in liver enzymes ≥3 times the upper limit of normal (ULN) were observed in subjects treated with LITFULO [see Warnings and Precautions (5.7)].
-
7 DRUG INTERACTIONS
7.1 Effects of LITFULO on Other Drugs
Table 3 includes clinically significant drug interactions affecting other drugs.
Table 3. Clinically Significant Interactions Affecting Other Drugs CYP3A Substrates Where Small Concentration Changes May Lead to Serious Adverse Reactions
Clinical Impact
Ritlecitinib is a CYP3A inhibitor. Concomitant use of ritlecitinib increases AUC and Cmax of CYP3A substrates [see Clinical Pharmacology (12.3)], which may increase the risk of adverse reactions of these substrates.
Intervention
Consider additional monitoring and dosage adjustment in accordance with approved product labeling of CYP3A substrates where small concentration changes may lead to serious adverse reactions when used with LITFULO.
CYP1A2 Substrates Where Small Concentration Changes May Lead to Serious Adverse Reactions
Clinical Impact
Ritlecitinib is a CYP1A2 inhibitor. Concomitant use of ritlecitinib increases AUC and Cmax of CYP1A2 substrates [see Clinical Pharmacology (12.3)], which may increase the risk of adverse reactions of these substrates.
Intervention
Consider additional monitoring and dosage adjustment in accordance with the approved product labeling of CYP1A2 substrates where small concentration changes may lead to serious adverse reactions when used concomitantly with LITFULO.
7.2 Effects of Other Drugs on LITFULO
Table 4 includes clinically significant drug interactions affecting LITFULO.
Table 4. Clinically Significant Interactions Affecting LITFULO CYP3A Inducers
Clinical Impact
Concomitant use of strong CYP3A inducer (e.g., rifampin) may decrease AUC and Cmax of ritlecitinib [see Clinical Pharmacology (12.3)], which may result in loss of or reduced clinical response.
Intervention
Coadministration with strong inducers of CYP3A is not recommended.
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Exposure Registry
If a patient becomes pregnant while receiving LITFULO, healthcare providers should report LITFULO exposure by calling 1-877-390-2940.
Risk Summary
Available data from clinical trials with LITFULO use in pregnant women are insufficient to identify a drug-associated risk of major birth defects, miscarriage or other adverse maternal or fetal outcomes. In animal reproduction studies, oral administration of ritlecitinib to pregnant rats and rabbits during organogenesis caused fetotoxicity and fetal malformations at exposures 49 and 55 times the maximum recommended human dose (MRHD) based on area under the curve (AUC) comparison, respectively (see Animal Data).
The background risks of major birth defects and miscarriage for the indicated population are unknown. All pregnancies carry some risk of birth defects, loss, or other adverse outcomes. The estimated background risks in the U.S. general population of major birth defects and miscarriages are 2-4% and 15-20% of clinically recognized pregnancies, respectively.
Data
In an embryo-fetal development study in pregnant rats, oral administration of ritlecitinib from gestation days 6 to 17 decreased fetal body weights and caused fetal skeletal malformations (malformed vertebrae and ribs) and variations (delayed ossification) at doses ≥175 mg/kg/day (49 times the MRHD based on AUC comparison). Maternal toxicity (lower body weights) was noted at 325 mg/kg/day (102 times the MRHD based on AUC comparison). There was no developmental toxicity at 75 mg/kg/day (16 times the MRHD based on AUC comparison).
In an embryo-fetal development study in pregnant rabbits, oral administration of ritlecitinib from gestation days 7 to 19 decreased mean fetal body weights and increased visceral malformations (malpositioned kidneys), skeletal malformations (supernumerary sternebrae, absent thoracic arch, and/or fused thoracic centra), and skeletal variations (delayed ossification) at 75 mg/kg/day (55 times the MRHD based on AUC comparison). There was no developmental toxicity at doses up to 25 mg/kg/day (12 times the MRHD based on AUC comparison).
In a pre- and postnatal development study in rats, oral administration of ritlecitinib from gestation day 6 through lactation day 20 had no effects on pre- and postnatal development at doses up to 75 mg/kg/day (14 times the MRHD based on AUC comparison). At 175 mg/kg/day (41 times the MRHD based on AUC comparison), ritlecitinib caused adverse lower postnatal survival and lower offspring body weights, which correlated with delayed sexual maturation in both sexes. Bred females in the F1 generation also exhibited lower mean numbers of corpora lutea at 175 mg/kg/day.
8.2 Lactation
Risk Summary
There are no data on the presence of ritlecitinib in human milk, the effects on the breastfed infant, or the effects on milk production. Ritlecitinib is present in the milk of lactating rats (see Data). When a drug is present in animal milk, it is likely that it will be present in human milk. Because of the serious adverse effects in adults, including risks of serious infection and malignancy, advise women not to breastfeed during treatment with LITFULO and for approximately 14 hours after the last dose (approximately 6 elimination half-lives).
8.4 Pediatric Use
The safety and effectiveness of LITFULO for the treatment of alopecia areata have been established in pediatric patients ages 12 years and older. A total of 181 pediatric patients ages 12 to <18 years were enrolled in alopecia areata clinical trials, with 105 pediatric patients ages 12 to <18 years with alopecia areata randomized in a pivotal, double-blind, placebo-controlled trial (Trial AA-I). Efficacy was consistent between the pediatric patients and adults [see Clinical Studies (14)]. The adverse reaction profile in the pediatric patients was similar to adults.
The safety and efficacy of LITFULO have not been established in pediatric patients under 12 years of age.
8.5 Geriatric Use
No dose adjustment is required for patients ≥65 years of age.
A total of 28 patients enrolled in alopecia areata trials were 65 years of age and older, and none were 75 years of age and older. Clinical trials of LITFULO did not include sufficient numbers of patients 65 years of age and older to determine whether they respond differently from younger adult patients.
As there is a higher incidence of infections in the elderly population in general, caution should be used when treating the elderly.
8.6 Hepatic Impairment
No dose adjustment is required in patients with mild (Child Pugh A) or moderate (Child Pugh B) hepatic impairment.
LITFULO is not recommended in patients with severe (Child Pugh C) hepatic impairment [see Dosage and Administration (2.3) and Clinical Pharmacology (12.3)].
-
10 OVERDOSAGE
LITFULO was administered in clinical trials up to a single oral dose of 800 mg. Adverse reactions were comparable to those seen at lower doses and no specific toxicities were identified. Pharmacokinetics (PK) data up to and including a single oral dose of 800 mg in healthy adult volunteers indicate that more than 90% of the administered dose is expected to be eliminated within 48 hours.
There is no specific antidote for overdose with LITFULO. Treatment should be symptomatic and supportive, and monitor patients for signs and symptoms of adverse reactions [see Clinical Trials Experience (6.1)].
In case of an overdose, call Poison Control Center at 1-800-222-1222 for latest recommendations.
-
11 DESCRIPTION
LITFULO (ritlecitinib) capsules are formulated with ritlecitinib tosylate, a kinase inhibitor.
Ritlecitinib tosylate is a white to off white to pale pink solid which is freely soluble in water. The chemical name is 1-{(2S,5R)-2-Methyl-5-[(7H-pyrrolo[2,3-d]pyrimidin-4-yl)amino]piperidin-1-yl}prop-2-en-1-one 4 methylbenzene-1-sulfonic acid.
The molecular formula for ritlecitinib tosylate is C22H27N5O4S. The molecular weight is 457.55 g/mol and its structural formula is:
LITFULO is supplied for oral administration as a 50 mg immediate-release capsule. Each capsule contains 50 mg ritlecitinib (equivalent to 80.13 mg ritlecitinib tosylate) and the following inactive ingredients: crospovidone, glyceryl dibehenate, lactose monohydrate, microcrystalline cellulose, and hypromellose (HPMC) capsule shells. The yellow/blue, opaque capsule shells contain Brilliant blue FCF – FD&C Blue, hypromellose, titanium dioxide, and yellow iron oxide.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
LITFULO is a kinase inhibitor.
Ritlecitinib irreversibly inhibits Janus kinase 3 (JAK3) and the tyrosine kinase expressed in hepatocellular carcinoma (TEC) kinase family by blocking the adenosine triphosphate (ATP) binding site. In cellular settings, ritlecitinib inhibits cytokine induced STAT phosphorylation mediated by JAK3-dependent receptors. Additionally, ritlecitinib inhibits signaling of immune receptors dependent on TEC kinase family members. The relevance of inhibition of specific JAK or TEC family enzymes to therapeutic effectiveness is not currently known.
12.2 Pharmacodynamics
Lymphocyte Subsets
A dose-dependent early decrease in absolute lymphocyte levels, T lymphocytes (CD3) and T lymphocyte subsets (CD4 and CD8) was associated with LITFULO treatment in patients with alopecia areata. In addition, there was a dose-dependent early decrease in NK cells (CD16/56) which remained stable at the lower level up to Week 48. For the 50 mg QD dose, there was an initial decrease in median lymphocyte levels which remained consistent up to Week 48. There was no change observed in B lymphocytes (CD19) in any treatment group.
12.3 Pharmacokinetics
Ritlecitinib AUC0-tau and Cmax increase in an approximately dose-proportional manner up to 200 mg. Steady state was reached approximately by Day 4.
Absorption
The ritlecitinib absolute oral bioavailability is approximately 64%. Ritlecitinib peak plasma concentrations were reached within 1 hour following an oral dose.
Effect of Food
Food does not have a clinically significant impact on the systemic exposures of ritlecitinib. The coadministration of a 100 mg ritlecitinib capsule with a high-fat meal reduced the ritlecitinib Cmax by ~32% and AUCinf was increased by 11%. In clinical trials, ritlecitinib was administered without regard to meals [see Dosage and Administration (2.2)].
Elimination
The ritlecitinib mean terminal half-life ranges from 1.3 to 2.3 hours.
Metabolism
The metabolism of ritlecitinib is mediated by multiple pathways with no single route contributing to more than 25% of the total metabolism. These pathways include:
- Glutathione S-transferase (GST): cytosolic GST A1/3, M1/3/5, P1, S1, T2, Z1 and microsomal GST 1/2/3
- CYP enzymes (CYP3A, CYP2C8, CYP1A2, and CYP2C9)
Specific Populations
No clinically relevant differences in the pharmacokinetics of ritlecitinib were observed based on age (12-73 years), body weight, gender, GST genotype, and race.
Patients with Renal Impairment
The AUC24 observed in patients with severe renal impairment (eGFR <30 mL/min) was 55.2% higher compared with the AUC24 in matched participants with normal renal functions. These differences are not considered clinically significant. Ritlecitinib has not been studied in patients with mild (eGFR 60 to <90 mL/min) or moderate (eGFR 30 to <60 mL/min) renal impairment, as a clinically relevant increase in ritlecitinib exposure is not expected in these patients. The eGFR and classification of renal function status of patients was done using the Modification of Diet in Renal Disease (MDRD) formula. Ritlecitinib has not been studied in patients with ESRD or in renal transplant recipients.
Patients with Hepatic Impairment
Patients with moderate (Child Pugh B) hepatic impairment had an 18.5% increase in ritlecitinib AUC24 compared to patients with normal hepatic function. Ritlecitinib has not been studied in patients with mild (Child Pugh A) hepatic impairment, as a clinically relevant increase in ritlecitinib exposure is not expected in these patients.
Ritlecitinib has not been studied in patients with severe (Child Pugh C) hepatic impairment and is not recommended for use in these patients [see Dosage and Administration (2.3) and Use In Specific Populations (8.6)].
Drug Interaction Studies
Clinical Studies
Effect of other drugs on ritlecitinib
The effect of coadministered drugs on the pharmacokinetics of ritlecitinib is presented in Table 5.
Table 5. Change in Pharmacokinetics of Ritlecitinib in the Presence of Coadministered Drugs - * Ratios for Cmax and AUCinf compare coadministration of ritlecitinib with the drug versus administration of ritlecitinib alone.
- † Drug interaction with CYP3A inhibitor is not clinically significant.
Coadministered Drugs
Regimen of Coadministered Drug
Dose of Ritlecitinib
Ratio* (90% Confidence Interval)
Cmax
AUCinf
Strong CYP3A inhibitor: Itraconazole†
200 mg once daily × 5 days
30 mg
1.03 (0.83, 1.27)
1.15 (1.05, 1.27)
Strong CYP enzyme inducer: Rifampin
600 mg once daily × 8 days
50 mg
0.75 (0.63, 0.89)
0.56 (0.52, 0.60)
Effect of ritlecitinib on other drugs
The effect of ritlecitinib on the pharmacokinetics of coadministered drugs is presented in Table 6.
Table 6. Change in Pharmacokinetics of Coadministered Drugs in the Presence of Ritlecitinib - * Ratios for Cmax and AUCinf compare coadministration of the drug with ritlecitinib versus administration of the drug alone.
- † Drug interactions with ritlecitinib for oral contraceptives, CYP2B6 substrates, CYP2C substrates, and substrates of OATP1B1, BCRP, OAT3, and OCT1 transporters are not clinically significant.
- ‡ AUClast of levonorgestrel was reported in lieu of AUCinf because the terminal phase of levonorgestrel was not well characterized.
- § Ritlecitinib dosage 4 times the approved recommended dosage.
- ¶ AUC0-72 of efavirenz was reported
- # Ritlecitinib dosage 8 times the approved recommended dosage.
Coadministered Drugs
Dose Regimen of Ritlecitinib
Ratio* (90% Confidence Interval)
Cmax
AUCinf
Oral contraceptive: Ethinyl estradiol (EE) and levonorgestrel (LN)†
50 mg once daily × 11 days
EE: 0.92 (0.84, 1.01)
LN: 0.80 (0.73, 0.88)
EE: 0.98 (0.91, 1.06)
LN‡: 0.88 (0.83, 0.93)
Sensitive CYP3A substrate: Midazolam [see Drug Interactions (7.1)]
200 mg once daily × 11 days§
1.81 (1.48, 2.21)
2.69 (2.16, 3.36)
Sensitive CYP1A2 substrate: Caffeine [see Drug Interactions (7.1)]
200 mg once daily × 9 days§
1.10 (1.04, 1.16)
2.65 (2.34, 3.00)
Sensitive CYP2B6 substrate: Efavirenz†
200 mg once daily × 11 days§
0.88 (0.77, 1.01)
1.00¶ (0.95, 1.04)
Sensitive CYP2C substrate: Tolbutamide†
200 mg once daily × 10 days§
1.03 (0.97, 1.10)
0.99 (0.92, 1.07)
Sensitive OATP1B1, BCRP and OAT3 substrate: Rosuvastatin†
200 mg once daily × 10 days§
0.73 (0.63, 0.83)
0.87 (0.75, 1.01)
Sensitive OCT1 substrate: Sumatriptan†
400 mg single dose coadministration#
0.87 (0.73, 1.03)
1.30 (1.17, 1.44)
400 mg single dose 8 hours prior to Sumatriptan#
1.50 (1.26, 1.78)
1.50 (1.35, 1.66)
In Vitro Studies
CYP Related Pathways: Ritlecitinib is not an inhibitor of CYP2D6.
Other Metabolic Pathways: Ritlecitinib is not an inhibitor of uridine 5’ diphospho glucuronosyltransferases (UGTs) (UGT1A1, UGT1A4, UGT1A6, UGT1A9, and UGT2B7), GSTs or sulfotransferases (SULTs).
Transporter Systems: Ritlecitinib is not an inhibitor of P-glycoprotein (P-gp) or bile salt export pump (BSEP).
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
In a 2-year rat carcinogenicity study, ritlecitinib increased the incidence of combined benign and malignant thymomas in female rats, and thyroid follicular adenomas and combined follicular adenomas and carcinomas in male rats at 100 mg/kg/day (29 times the MRHD based on AUC comparison). No ritlecitinib-related tumors were noted at doses up to 30 mg/kg/day (6.3 times the MRHD based on AUC comparison). No ritlecitinib-related tumors were noted in a 6-month Tg.rasH2 mouse carcinogenicity study at doses up to 300 mg/kg/day.
Ritlecitinib was not mutagenic in the in vitro bacterial reverse mutation assay (Ames assay). Ritlecitinib was positive in an in vitro micronucleus assay in TK6 cells. However, mechanistic studies determined that ritlecitinib is aneugenic and does not present a clinically relevant genotoxic concern. Additionally, in an in vivo rat bone marrow micronucleus assay, ritlecitinib was not aneugenic or clastogenic at doses up to 400 mg/kg/day.
Ritlecitinib had no effects on female rat fertility at doses up to 200 mg/kg/day (55 times the MRHD based on AUC comparison). Effects on male rat fertility were noted (higher preimplantation loss resulting in lower number of implantation sites and corresponding lower litter size in naïve females mated with ritlecitinib-dosed males) at 200 mg/kg/day (55 times the MRHD based on AUC comparison). No effects on male fertility were noted at doses up to 60 mg/kg/day (14 times the MRHD based on AUC comparison). No effects on spermatogenesis (sperm counts, production rate, motility, or morphology) were noted at any dose.
13.2 Animal Toxicology and Pharmacology
In two 9-month oral repeat dose toxicity studies in dogs, dose-related reversible axonal dystrophy was noted in the brainstem, spinal cord, sciatic nerve, nerve branches of the vagus nerve, and myenteric/submucosal plexuses of the GI tract at doses ≥20 mg/kg/day (14 times the MRHD based on AUC comparison). At 40 mg/kg/day (33 times the MRHD based on AUC comparison), ritlecitinib-related axonal dystrophy caused adverse reversible hearing loss and waveform deficits in brainstem auditory evoked potential (BAEP) testing. BAEP deficits were first noted during Month 7 of dosing and persisted through the end of dosing. No auditory threshold deficits were noted at 6 months after the end of dosing. No BAEP deficits were noted at doses ≤20 mg/kg/day. Additional mechanistic studies provided preliminary evidence that ritlecitinib-related hearing loss was not directly caused by JAK3 or TEC family kinase inhibition, but did not identify the underlying mechanism of axonal dystrophy in dogs.
-
14 CLINICAL STUDIES
The efficacy and safety of LITFULO were evaluated in one randomized, double-blind, placebo-controlled trial (Trial AA-I) in subjects 12 years of age and older with alopecia areata with ≥50% scalp hair loss, including alopecia totalis (AT) and alopecia universalis (AU).
Trial AA-I evaluated a total of 718 subjects who were randomized to one of the following treatment regimens for 48 weeks: 1) 200 mg once daily for 4 weeks followed by 50 mg once daily for 44 weeks; 2) 200 mg once daily for 4 weeks followed by 30 mg once daily for 44 weeks; 3) 50 mg once daily for 48 weeks; 4) 30 mg once daily for 48 weeks; 5) 10 mg once daily for 48 weeks; 6) placebo for 24 weeks followed by 200 mg once daily for 4 weeks and 50 mg once daily for 20 weeks; or 7) placebo for 24 weeks followed by 50 mg once daily for 24 weeks.
The recommended dose of LITFULO is 50 mg once daily and the results for this dose are discussed below.
Across all treatment groups 62% of subjects were female, 68% were White, 26% were Asian, and 4% were Black or African American. The majority of subjects (85%) were adults (≥18 years of age) with a mean age of 33.7 years. A total of 105 (15%) subjects 12 to <18 years of age and 20 (3%) subjects 65 years of age and older were enrolled. The mean baseline Severity of Alopecia Tool (SALT) score ranged from 88.3 to 93.0 across treatment groups; among subjects without AT/AU at baseline, the mean SALT score ranged from 78.3 to 87.0. The majority of subjects had abnormal eyebrows (83%) and eyelashes (75%) at baseline across treatment groups. The median duration since alopecia areata diagnosis was 6.9 years and the median duration of the current alopecia areata episode was 2.5 years. Randomization was stratified by AT/AU status with 46% of subjects classified as AT/AU based upon a baseline SALT score of 100.
Clinical Response
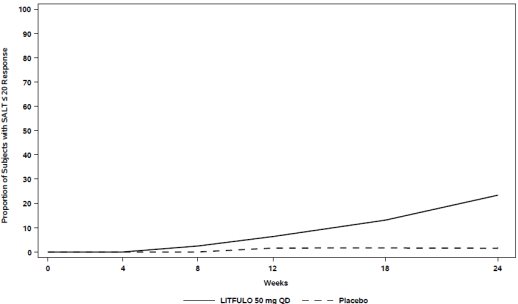
Assessment of scalp hair loss was based on the SALT score. At Week 24, a greater proportion of subjects had a SALT ≤20 response (20% or less of scalp hair loss) and SALT ≤10 response (10% or less of scalp hair loss) with LITFULO compared to placebo (Table 7). The percentage of subjects achieving SALT ≤20 response by visit is shown in Figure 1.
Table 7. Proportion of Subjects with Response on the SALT Scale at Week 24 LITFULO 50 mg QD
(N=130)
% RespondersPlacebo
(N=131)
% RespondersDifference from Placebo
(95% CI)Abbreviations: CI = confidence interval; N = total number of subjects; QD = once daily; SALT = Severity of Alopecia Tool. - * SALT ≤20 responders were subjects with scalp hair loss of ≤20%. SALT scores range from 0 to 100 with 0 = no scalp hair loss and 100 = total scalp hair loss.
- † SALT ≤10 responders were subjects with scalp hair loss of ≤10%.
SALT ≤20 response*
23.0
1.6
21.4 (13.4, 29.5)
SALT ≤10 response†
13.4
1.5
11.9 (5.4, 18.3)
Figure 1. SALT ≤20 Response through Week 24
-
16 HOW SUPPLIED/STORAGE AND HANDLING
LITFULO capsules are packaged in child-resistant, white, high-density polyethylene (HDPE) bottles with polypropylene (PP) cap with a foil heat induction seal liner. The bottles contain 1g of desiccant in a high-density polyethylene (HDPE) canister. Do not eat the desiccant.
Dosage Form
Strength
Description
Bottle Size
(number of capsules)
NDC Number
Capsules
50 mg of ritlecitinib
Size 3, opaque capsules with yellow body and blue cap. The body is printed with “RCB 50” and the cap is printed with “Pfizer” in black.
28 count bottle
0069-0334-28
-
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Medication Guide).
Administration
Advise patients not to crush, split or chew LITFULO capsules [see Dosage and Administration (2.2)].
Serious Infections
Inform patients that they may develop infections when taking LITFULO which in some cases can be serious. Instruct patients to tell their healthcare provider if they develop any signs or symptoms of an infection [see Warnings and Precautions (5.1)].
Advise patients that the risk of herpes zoster is increased in patients treated with LITFULO [see Warnings and Precautions (5.1)].
Malignancies
Inform patients that LITFULO may increase their risk of certain cancers, including skin cancers. Periodic skin examinations are recommended while using LITFULO [see Warnings and Precautions (5.3)].
Thromboembolic Events
Advise patients that events of PE and retinal artery occlusion have been reported in clinical trials with LITFULO. Instruct patients to seek immediate medical attention if they develop any signs or symptoms of a thrombosis [see Warnings and Precautions (5.5)].
Hypersensitivity Reactions
Advise patients to discontinue LITFULO and seek immediate medical attention if they develop any signs and symptoms of serious allergic reaction [see Warnings and Precautions (5.6)].
Laboratory Abnormalities
Inform patients that LITFULO may affect certain lab tests, and that blood tests are required before and during LITFULO treatment [see Dosage and Administration (2.1) and Warnings and Precautions (5.7)].
Vaccinations
Advise patients that vaccination with live vaccines is not recommended during LITFULO treatment and shortly prior to LITFULO treatment. Instruct patients to inform the healthcare practitioner that they are taking LITFULO prior to a potential vaccination [see Warnings and Precautions (5.8)].
Pregnancy
Advise pregnant females and females of reproductive potential to inform their healthcare providers if they are pregnant or intend to becomes pregnant during treatment with LITFULO. Instruct patients to report their pregnancy to Pfizer Inc. at 1-877-390-2940 [see Use in Specific Populations (8.1)].
Lactation
Advise women not to breastfeed during treatment with LITFULO and for 14 hours after the last dose [see Use in Specific Populations (8.2)].
-
SPL UNCLASSIFIED SECTION
For Medical Information about LITFULO, please visit www.pfizermedinfo.com or call 1-800-438-1985.
LAB-1469-1.0
-
MEDICATION GUIDE
Medication Guide
LITFULO™ (lit-FUL-oh)
(ritlecitinib)
capsules, for oral useWhat is the most important information I should know about LITFULO?
LITFULO may cause serious side effects, including:
1. Serious infections
LITFULO is a medicine that affects your immune system. LITFULO can lower the ability of your immune system to fight infections. Some people have had serious infections while taking LITFULO or other similar medicines, including tuberculosis (TB), and infections caused by bacteria, fungi, or viruses that can spread throughout the body and have been hospitalized. Some people taking similar medicines to LITFULO have died from these infections.
- Your healthcare provider should test you for TB before starting treatment with LITFULO.
- Your healthcare provider should watch you closely for signs and symptoms of TB during treatment with LITFULO.
You should not start taking LITFULO if you have any kind of infection unless your healthcare provider tells you it is okay.
You may be at a higher risk of developing shingles (herpes zoster).
Before starting LITFULO, tell your healthcare provider if you:
- are being treated for an infection.
- have an infection that has not gone away or that keeps coming back.
- have diabetes, chronic lung disease, HIV, or a weak immune system.
- have TB or have been in close contact with someone with TB.
- have had shingles (herpes zoster).
- have had hepatitis B or hepatitis C.
- live or have lived or have traveled to certain parts of the country (such as the Ohio and Mississippi River valleys and the Southwest) where there is an increased chance for getting certain kinds of fungal infections. These infections may happen or become more severe if you use LITFULO. Ask your healthcare provider if you do not know if you have lived in an area where these infections are common.
- think you have an infection or have symptoms of an infection such as:
- o fever, sweating, or chills
- o muscle aches
- o cough or shortness of breath
- o blood in your phlegm
- o weight loss
- o warm, red, or painful skin or sores on your body
- o diarrhea or stomach pain
- o burning when you urinate or urinating more often than usual
- o feeling very tired
After starting LITFULO, call your healthcare provider right away if you have any symptoms of an infection. LITFULO can make you more likely to get infections or make any infections that you have worse. If you get a serious infection, your healthcare provider may stop treatment with LITFULO until your infection is controlled.
2. Increased risk of death in people 50 years of age and older who have at least 1 heart disease (cardiovascular) risk factor and are taking a medicine in the class of medicines called Janus kinase (JAK) inhibitors. LITFULO is a kinase inhibitor medicine.
3. Cancer and immune system problems
LITFULO may increase your risk of certain cancers by changing the way your immune system works.
- Lymphoma and other cancers, including skin cancers, can happen in people taking LITFULO.
- People taking a medicine in the class of medicines called JAK inhibitors have a higher risk of certain cancers including lymphoma and lung cancer, especially if you are current or past smoker.
- Follow your healthcare provider’s advice about having your skin checked for skin cancer during treatment with LITFULO.
Tell your healthcare provider if you have ever had any type of cancer.
4. Increased risk of major cardiovascular events such as heart attack, stroke, or death in people 50 years of age and older who have at least 1 heart disease (cardiovascular) risk factor and taking a medicine in the class of medicines called JAK inhibitors, especially if you are a current or past smoker.
Get emergency help right away if you have any symptoms of a heart attack or stroke while using LITFULO, including:
- discomfort in the center of your chest that lasts for more than a few minutes, or that goes away and comes back
- severe tightness, pain, pressure, or heaviness in your chest, throat, neck, or jaw
- pain or discomfort in your arms, back, neck, jaw, or stomach
- shortness of breath with or without chest discomfort
- breaking out in a cold sweat
- nausea or vomiting
- feeling lightheaded
- weakness in one part or on one side of your body
- slurred speech
5. Blood clots
Blood clots in the veins of your legs (deep vein thrombosis, DVT), lungs (pulmonary embolism, PE), or eyes can happen in some people taking LITFULO. This may be life-threatening. Blood clots in the veins of the legs (deep vein thrombosis, DVT) and lungs (pulmonary embolism, PE) have happened more often in people who are 50 years of age and older with at least 1 heart disease (cardiovascular) risk factor taking a medicine in the class of medicines called JAK inhibitors.
- Tell your healthcare provider if you have had blood clots in the past.
-
Stop taking LITFULO and get medical help right away if you have any signs and symptoms of blood clots during treatment with LITFULO, including:
- o swelling, pain or tenderness in one or both legs
- o sudden, unexplained chest or upper back pain
- o shortness of breath or difficulty breathing
- o changes in vision, especially in one eye only
6. Allergic reactions
Symptoms that may mean you are having an allergic reaction have been seen during treatment with LITFULO. Some of these reactions were serious. Stop taking LITFULO and get emergency medical help right away if you have symptoms of allergic reaction, including:
- hives
- rash
- trouble breathing
- feeling faint or dizzy
- swelling of your lips, tongue, or throat
7. Changes in certain laboratory test results
Your healthcare provider should do blood tests before you start taking LITFULO and during treatment to check for the following:
- low lymphocyte count. Lymphocytes are white blood cells that help the body fight off infections.
- low platelet count. Platelets help form clots and stop or prevent bleeding.
- elevated liver enzymes. Liver enzymes help to tell if your liver is functioning normally. Elevated liver enzymes may indicate that your healthcare provider needs to do additional tests on your liver.
- increased creatine phosphokinase (CPK). Increased CPK levels in the blood are common with LITFULO and can also be severe.
You should not take LITFULO if your lymphocyte counts or platelet counts are too low or your liver tests are too high. Your healthcare provider may stop your LITFULO treatment for a period of time if needed because of changes in these blood test results.
See "What are the possible side effects of LITFULO?" for more information about side effects.
What is LITFULO?
LITFULO is a prescription medicine that is a kinase inhibitor. LITFULO is used to treat an immune system problem that causes severe hair loss (alopecia areata) in adults and children 12 years and older.
It is not known if LITFULO is safe and effective in children under 12 years of age.
Before taking LITFULO, tell your healthcare provider about all of your medical conditions, including if you:
- See "What is the most important information I should know about LITFULO?"
- have an infection
- are a current or past smoker
- have had a heart attack, other heart problems, or stroke
- have liver problems
- have low platelet counts or white blood cell counts
- have recently received or are scheduled to receive an immunization (vaccine). People who take LITFULO should not receive live vaccines during treatment or right before starting treatment with LITFULO.
-
are pregnant or plan to become pregnant. It is not known if LITFULO will harm your unborn baby.
Females who are able to become pregnant:- o Tell your healthcare provider if you are pregnant or plan to become pregnant during treatment with LITFULO.
- o There is a pregnancy registry for people who take LITFULO during pregnancy. Report pregnancies to Pfizer Inc. at 1-877-390-2940.
- are breastfeeding or plan to breastfeed. It is not known if LITFULO passes into your breast milk. Do not breastfeed during treatment with LITFULO and for 14 hours after your last dose of LITFULO. Talk to your healthcare provider about the best way to feed your baby during treatment with LITFULO.
Tell your healthcare provider about all the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. LITFULO and other medicines may affect each other causing side effects.
Know the medicines you take. Keep a list of them to show your healthcare provider and pharmacist whenever
you get a new medicine.
How should I take LITFULO?
- Take LITFULO exactly as your healthcare provider tells you to take it.
- Take LITFULO 1 time each day, with or without food.
- Swallow LITFULO capsules whole. Do not crush, split, or chew the capsules.
- If you miss a dose of LITFULO, take the missed dose as soon as you remember. If it is less than 8 hours before your next scheduled dose of LITFULO, skip the missed dose and take the next dose at your usual time.
If you take too much LITFULO, call the Poison Control Center at 1-800-222-1222 or go to the nearest hospital emergency room right away.
What are the possible side effects of LITFULO?
LITFULO may cause serious side effects, including:
See "What is the most important information I should know about LITFULO?"
The most common side effects of LITFULO include:
- headache
- diarrhea
- acne
- rash
- hives
- inflamed hair pores (folliculitis)
- fever
- eczema
- dizziness
- shingles
- decreased red blood cell counts
- mouth sores, redness and swelling of the lining of your mouth
These are not all the possible side effects of LITFULO.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
You may also report side effects to Pfizer at 1-800-438-1985.
How should I store LITFULO?
- Store LITFULO at room temperature between 68°F to 77°F (20°C to 25°C).
- Keep LITFULO in the original package.
- The LITFULO bottle has a child resistant closure and contains a cannister with a drying agent (desiccant). Do not eat the desiccant.
Keep LITFULO and all medicines out of the reach of children.
General information about the safe and effective use of LITFULO.
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use LITFULO for a condition for which it was not prescribed. Do not give LITFULO to other people, even if they have the same symptoms you have. It may harm them. You can ask your pharmacist or healthcare provider for information about LITFULO that is written for health professionals.
What are the ingredients in LITFULO?
Active ingredient: ritlecitinib
Inactive ingredients: crospovidone, glyceryl dibehenate, lactose monohydrate, microcrystalline cellulose, and hypromellose (HPMC) capsule shells. The yellow/blue, opaque capsule shells contain Brilliant blue FCF – FD&C Blue, hypromellose, titanium dioxide, and yellow iron oxide.
LAB-1525-1.0- This Medication Guide has been approved by the U.S. Food and Drug Administration. Issued: 6/2023
-
PRINCIPAL DISPLAY PANEL - 50 mg Capsule Bottle Label Sample
PROFESSIONAL SAMPLE – NOT FOR SALE
ALWAYS DISPENSE WITH MEDICATION GUIDENDC: 63539-334-28
Pfizer
Litfulo™
(ritlecitinib) capsules50 mg*
Do not crush, split, or chew the capsules
Do not eat the desiccant.28 Capsules
Rx only -
INGREDIENTS AND APPEARANCE
LITFULO
ritlecitinib capsuleProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 63539-334 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength RITLECITINIB TOSYLATE (UNII: EAG4T1459K) (RITLECITINIB - UNII:2OYE00PC25) RITLECITINIB 50 mg Inactive Ingredients Ingredient Name Strength MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) LACTOSE MONOHYDRATE (UNII: EWQ57Q8I5X) CROSPOVIDONE, UNSPECIFIED (UNII: 2S7830E561) GLYCERYL DIBEHENATE (UNII: R8WTH25YS2) HYPROMELLOSE, UNSPECIFIED (UNII: 3NXW29V3WO) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) FERRIC OXIDE YELLOW (UNII: EX438O2MRT) FD&C BLUE NO. 1 (UNII: H3R47K3TBD) Product Characteristics Color YELLOW (Body) , BLUE (Cap) Score no score Shape CAPSULE Size 16mm Flavor Imprint Code RCB;50;Pfizer Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 63539-334-28 28 in 1 BOTTLE; Type 0: Not a Combination Product 07/06/2023 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA215830 07/06/2023 Labeler - U.S. Pharmaceuticals (829076905) Registrant - Pfizer Inc (113480771) Establishment Name Address ID/FEI Business Operations Pfizer Ireland Pharmaceuticals Unlimited Company 985052076 ANALYSIS(63539-334) , API MANUFACTURE(63539-334) Establishment Name Address ID/FEI Business Operations Pfizer Manufacturing Deutschland GmbH 341970073 ANALYSIS(63539-334) , MANUFACTURE(63539-334) , PACK(63539-334) , LABEL(63539-334)

Trademark Results [Litfulo]
Mark Image Registration | Serial | Company Trademark Application Date |
|---|---|
 LITFULO 90723569 not registered Live/Pending |
Pfizer Inc. 2021-05-20 |
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.