Mupirocin by Medsource Pharmaceuticals MUPIROCIN ointment
Mupirocin by
Drug Labeling and Warnings
Mupirocin by is a Prescription medication manufactured, distributed, or labeled by Medsource Pharmaceuticals. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
DESCRIPTION
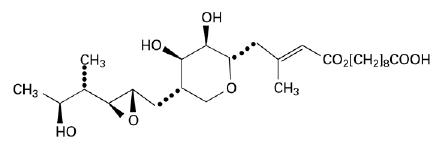
Each gram of Mupirocin Ointment USP, 2% contains 20 mg mupirocin in a bland water miscible ointment base (polyethylene glycol ointment, N.F.) consisting of polyethylene glycol 400 and polyethylene glycol 3350. Mupirocin is a naturally occurring antibiotic. The chemical name is ( E)-(2 S,3 R,4 R,5 S)-5-[(2 S,3 S,4 S,5 S)-2,3-Epoxy-5-hydroxy-4-methylhexyl]tetrahydro-3,4-dihydroxy-β- methyl-2 H-pyran-2-crotonic acid, ester with 9-hydroxynonanoic acid. The chemical structure is:
C 26H 44O 9 M.W. 500.63
-
CLINICAL PHARMACOLOGY
Application of 14C-labeled mupirocin ointment to the lower arm of normal male subjects followed by occlusion for 24 hours showed no measurable systemic absorption (< 1.1 nanogram mupirocin per milliliter of whole blood). Measurable radioactivity was present in the stratum corneum of these subjects 72 hours after application.
Following intravenous or oral administration, mupirocin is rapidly metabolized. The principal metabolite, monic acid, is eliminated by renal excretion, and demonstrates no antibacterial activity. In a trial conducted in 7 healthy adult male subjects, the elimination half-life after intravenous administration of mupirocin was 20 to 40 minutes for mupirocin and 30 to 80 minutes for monic acid. The pharmacokinetics of mupirocin has not been studied in individuals with renal insufficiency.
Microbiology
Mupirocin is an antibacterial agent produced by fermentation using the organism Pseudomonasfluorescens. Mupirocin inhibits bacterial protein synthesis by reversibly and specifically binding to bacterial isoleucyl transfer-RNA (tRNA) synthetase. Due to this unique mode of action, mupirocin does not demonstrate cross-resistance with other classes of antimicrobial agents.
When mupirocin resistance occurs, it results from the production of a modified isoleucyl-tRNA synthetase, or the acquisition of, by genetic transfer, a plasmid mediating a new isoleucyl-tRNA synthetase. High-level plasmid-mediated resistance (MIC > 512 mcg/mL) has been reported in increasing numbers of isolates of Staphylococcusaureus and with higher frequency in coagulase-negative staphylococci. Mupirocin resistance occurs with greater frequency in methicillin-resistant than methicillin-susceptible staphylococci. Because of the occurrence of mupirocin resistance in methicillin-resistant Staphylococcus aureus (MRSA), it is appropriate to test MRSA populations for mupirocin susceptibility prior to the use of mupirocin using a standardized method. 1,2,3
Mupirocin is bactericidal at concentrations achieved by topical administration. Mupirocin is highly protein-bound (> 97%), and the effect of wound secretions on the MICs of mupirocin has not been determined.
Mupirocin has been shown to be active against susceptible strains of S. aureus and Streptococcus pyogenes, both in vitro and in clinical trials (see INDICATIONS AND USAGE). The following in vitro data are available, but their clinical significance is unknown. Mupirocin is active against most isolates of Staphylococcus epidermidis.
- INDICATIONS AND USAGE
- CONTRAINDICATIONS
-
WARNINGS
Avoid contact with the eyes. In case of accidental contact, rinse well with water.
In the event of sensitization or severe local irritation from mupirocin ointment, usage should be discontinued.
Clostridium difficile-associated diarrhea (CDAD) has been reported with use of nearly all antibacterial agents, including mupirocin ointment, and may range in severity from mild diarrhea to fatal colitis. Treatment with antibacterial agents alters the normal flora of the colon leading to overgrowth of C. difficile.
C. difficile produces toxins A and B which contribute to the development of CDAD. Hypertoxin- producing isolates of C. difficile cause increased morbidity and mortality, as these infections can be refractory to antimicrobial therapy and may require colectomy. CDAD must be considered in all patients who present with diarrhea following antibacterial drug use. Careful medical history is necessary since CDAD has been reported to occur over two months after the administration of antibacterial agents.
If CDAD is suspected or confirmed, ongoing antibacterial drug use not directed against C. difficile may need to be discontinued. Appropriate fluid and electrolyte management, protein supplementation, antibacterial treatment of C. difficile, and surgical evaluation should be instituted as clinically indicated.
-
PRECAUTIONS
As with other antibacterial products, prolonged use may result in overgrowth of nonsusceptible organisms, including fungi.
Mupirocin ointment is not formulated for use on mucosal surfaces. Intranasal use has been associated with isolated reports of stinging and drying. A paraffin-based formulation – Bactroban ® Nasal (mupirocin calcium ointment) – is available for intranasal use.
Polyethylene glycol can be absorbed from open wounds and damaged skin and is excreted by the kidneys. In common with other polyethylene glycol-based ointments, mupirocin ointment should not be used in conditions where absorption of large quantities of polyethylene glycol is possible, especially if there is evidence of moderate or severe renal impairment.
Mupirocin ointment should not be used with intravenous cannulae or at central intravenous sites because of the potential to promote fungal infections and antimicrobial resistance.
Information for Patients
Use this medication only as directed by the healthcare provider. It is for external use only. Avoid contact with the eyes. If mupirocin ointment gets in or near the eyes, rinse thoroughly with water. The medication should be stopped and the healthcare provider contacted if irritation, severe itching, or rash occurs.
If impetigo has not improved in 3 to 5 days, contact the healthcare provider.
Drug Interactions
The effect of the concurrent application of mupirocin ointment and other drug products has not been studied.
Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term studies in animals to evaluate carcinogenic potential of mupirocin have not been conducted.
Results of the following studies performed with mupirocin calcium or mupirocin sodium in vitro and in vivo did not indicate a potential for genotoxicity: Rat primary hepatocyte unscheduled DNA synthesis, sediment analysis for DNA strand breaks, Salmonella reversion test (Ames), Escherichia coli mutation assay, metaphase analysis of human lymphocytes, mouse lymphoma assay, and bone marrow micronuclei assay in mice.
Reproduction studies were performed in male and female rats with mupirocin administered subcutaneously at doses up to 14 times a human topical dose (approximately 60 mg mupirocin per day) on a mg/m 2 basis and revealed no evidence of impaired fertility and reproductive performance from mupirocin.
Pregnancy
Teratogenic Effects
Pregnancy category B
Reproduction studies have been performed in rats and rabbits with mupirocin administered subcutaneously at doses up to 22 and 43 times, respectively, the human topical dose (approximately 60 mg mupirocin per day) on a mg/m 2 basis and revealed no evidence of harm to the fetus due to mupirocin. There are, however, no adequate and well-controlled studies in pregnant women. Because animal studies are not always predictive of human response, this drug should be used during pregnancy only if clearly needed.
Nursing Mothers
It is not known whether this drug is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when mupirocin ointment is administered to a nursing woman.
Pediatric Use
The safety and effectiveness of mupirocin ointment have been established in the age range of 2 months to 16 years. Use of mupirocin ointment in these age groups is supported by evidence from adequate and well-controlled trials of mupirocin ointment in impetigo in pediatric subjects studied as a part of the pivotal clinical trials (see CLINICAL STUDIES).
-
ADVERSE REACTIONS
The following local adverse reactions have been reported in connection with the use of mupirocin ointment: burning, stinging, or pain in 1.5% of subjects; itching in 1% of subjects; rash, nausea, erythema, dry skin, tenderness, swelling, contact dermatitis, and increased exudate in less than 1% of subjects.
Systemic allergic reactions, including anaphylaxis, urticaria, angioedema, and generalized rash have been reported in patients treated with formulations of mupirocin.
- DOSAGE AND ADMINISTRATION
-
CLINICAL STUDIES
The efficacy of topical mupirocin ointment in impetigo was tested in 2 trials. In the first, subjects with impetigo were randomized to receive either mupirocin ointment or vehicle placebo 3 times daily for 8 to 12 days. Clinical efficacy rates at end of therapy in the evaluable populations (adults and pediatric subjects included) were 71% for mupirocin ointment (n = 49) and 35% for vehicle placebo (n = 51). Pathogen eradication rates in the evaluable populations were 94% for mupirocin ointment and 62% for vehicle placebo. There were no side effects reported in the group receiving mupirocin ointment.
In the second trial, subjects with impetigo were randomized to receive either mupirocin ointment 3 times daily or 30 to 40 mg/kg oral erythromycin ethylsuccinate per day (this was an unblinded trial) for 8 days. There was a follow-up visit 1 week after treatment ended. Clinical efficacy rates at the follow-up visit in the evaluable populations (adults and pediatric subjects included) were 93% for mupirocin ointment (n = 29) and 78.5% for erythromycin (n = 28). Pathogen eradication rates in the evaluable populations were 100% for both test groups. There were no side effects reported in the group receiving mupirocin ointment.
Pediatrics
There were 91 pediatric subjects aged 2 months to 15 years in the first trial described above. Clinical efficacy rates at end of therapy in the evaluable populations were 78% for mupirocin ointment (n = 42) and 36% for vehicle placebo (n = 49). In the second trial described above, all subjects were pediatric except 2 adults in the group receiving mupirocin ointment. The age range of the pediatric subjects was 7 months to 13 years. The clinical efficacy rate for mupirocin ointment (n = 27) was 96%, and for erythromycin it was unchanged (78.5%).
-
HOW SUPPLIED
Mupirocin Ointment USP, 2% is supplied in 22 gram tubes (NDC: 0093-1010-42).
Store at 20 o to 25 oC (68 o to 77 oF) [See USP Controlled Room Temperature].
-
REFERENCES
1. Clinical and Laboratory Standards Institute (CLSI). Methods for Dilution Antimicrobial Susceptibility
Tests for Bacteria that Grow Aerobically; Approved Standard -Tenth Edition. CLSI document M07-
A10 [2015], Clinical and Laboratory Standards Institute, 950 West Valley Road, Suite 2500, Wayne,
Pennsylvania 19087, USA.2. Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Disk
Diffusion Susceptibility Tests; Approved Standard – Twelfth Edition. CLSI document M02-A12
[2015], Clinical and Laboratory Standards Institute, 950 West Valley Road, Suite 2500, Wayne,
Pennsylvania 19087, USA.3. Finlay JE, Miller LA, Poupard JA. Interpretive criteria for testing susceptibility of staphylococci to
mupirocin. Antimicrob Agents Chemother 1997;41(5):1137-1139.All brand names listed are the registered trademarks of their respective owners and are not trademarks of Teva Pharmaceuticals USA, Inc.
Manufactured In Croatia By:
PLIVA HRVATSKA d.o.o.
Zagreb, Croatia
Manufactured For:
TEVA PHARMACEUTICALS USA, INC.
North Wales, PA 19454
Rev. I 3/2015
- Package/Label Display Panel
-
INGREDIENTS AND APPEARANCE
MUPIROCIN
mupirocin ointmentProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 45865-722(NDC:0093-1010) Route of Administration TOPICAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength MUPIROCIN (UNII: D0GX863OA5) (MUPIROCIN - UNII:D0GX863OA5) MUPIROCIN 20 mg in 1 g Inactive Ingredients Ingredient Name Strength POLYETHYLENE GLYCOL 400 (UNII: B697894SGQ) POLYETHYLENE GLYCOL 3350 (UNII: G2M7P15E5P) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 45865-722-01 1 in 1 CARTON 11/07/2003 1 22 g in 1 TUBE; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA065085 11/07/2003 Labeler - Medsource Pharmaceuticals (833685915) Establishment Name Address ID/FEI Business Operations Medsource Pharmaceuticals 833685915 relabel(45865-722)
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.