TRIJARDY ®XR (empagliflozin, linagliptin, and metformin hydrochloride extended-release tablets), for oral use
Trijardy XR by
Drug Labeling and Warnings
Trijardy XR by is a Prescription medication manufactured, distributed, or labeled by Praxis, LLC. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
TRIJARDY XR- empagliflozin, linagliptin, metformin hydrochloride tablet, extended release
Praxis, LLC
----------
TRIJARDY ®XR (empagliflozin, linagliptin, and metformin hydrochloride extended-release tablets), for oral use
10 OVERDOSAGE
In the event of an overdose with TRIJARDY XR, consider contacting the Poison Help line (1-800-222-1222) or a medical toxicologist for additional overdosage management recommendations.
Overdose of metformin HCl has occurred, including ingestion of amounts greater than 50 grams. Lactic acidosis has been reported in approximately 32% of metformin overdose cases [see Warnings and Precautions (5.1)]. Metformin is dialyzable with a clearance of up to 170 mL/min under good hemodynamic conditions. Therefore, hemodialysis may be useful for removal of accumulated drug from patients in whom metformin overdosage is suspected.
Removal of empagliflozin by hemodialysis has not been studied, and removal of linagliptin by hemodialysis or peritoneal dialysis is unlikely.
11 DESCRIPTION
TRIJARDY XR tablets for oral use contain: empagliflozin, linagliptin, and metformin HCl.
Empagliflozin
Empagliflozin is an inhibitor of the SGLT2.
The chemical name of empagliflozin is D-Glucitol,1,5-anhydro-1-C-[4-chloro-3-[[4-[[(3S)-tetrahydro-3-furanyl]oxy]phenyl]methyl]phenyl]-, (1S).
The molecular formula is C 23H 27ClO 7and the molecular weight is 450.91. The structural formula is:
Empagliflozin is a white to yellowish, non-hygroscopic powder. It is very slightly soluble in water, sparingly soluble in methanol, slightly soluble in ethanol and acetonitrile, soluble in 50% acetonitrile/water, and practically insoluble in toluene.
Linagliptin
Linagliptin is an inhibitor of the DPP-4 enzyme.
The chemical name of linagliptin is 1H-Purine-2,6-dione, 8-[(3R)-3-amino-1-piperidinyl]-7-(2-butyn-1-yl)-3,7-dihydro-3-methyl-1-[(4-methyl-2-quinazolinyl)methyl]-
The molecular formula is C 25H 28N 8O 2and the molecular weight is 472.54. The structural formula is:

Linagliptin is a white to yellowish, not or only slightly hygroscopic solid substance. It is very slightly soluble in water. Linagliptin is soluble in methanol, sparingly soluble in ethanol, very slightly soluble in isopropanol, and very slightly soluble in acetone.
Metformin HCl
Metformin HCl ( N,N-dimethylimidodicarbonimidic diamide hydrochloride) is a biguanide. Metformin HCl is a white to off-white crystalline compound with a molecular formula of C 4H 11N 5∙HCl and a molecular weight of 165.63. Metformin HCl is freely soluble in water and is practically insoluble in acetone, ether, and chloroform. The pKa of metformin is 12.4. The pH of a 1% aqueous solution of metformin hydrochloride is 6.68. The structural formula is:
TRIJARDY XR
Each film-coated tablet of TRIJARDY XR consists of an extended-release metformin hydrochloride core tablet that is coated with the immediate-release drug substances: empagliflozin and linagliptin.
TRIJARDY XR tablets for oral administration are available in four strengths containing:
- 5 mg empagliflozin, 2.5 mg linagliptin, and 1,000 mg metformin HCl (equivalent to 779.86 mg of metformin)
- 10 mg empagliflozin, 5 mg linagliptin, and 1,000 mg metformin HCl (equivalent to 779.86 mg of metformin)
- 12.5 mg empagliflozin, 2.5 mg linagliptin, and 1,000 mg metformin HCl (equivalent to 779.86 mg of metformin)
- 25 mg empagliflozin, 5 mg linagliptin, and 1,000 mg metformin HCl (equivalent to 779.86 mg of metformin)
Each film-coated tablet of TRIJARDY XR contains the following inactive ingredients: Tablet Core: hypromellose, magnesium stearate, and polyethylene oxide. Film Coatings and Printing Ink: ammonium hydroxide, arginine, carnauba wax, ferric oxide yellow and ferric oxide red (10 mg/5 mg/1,000 mg), ferrosoferric oxide and ferric oxide red (12.5 mg/2.5 mg/1,000 mg), ferrosoferric oxide and ferric oxide yellow (5 mg/2.5 mg/1,000 mg and 25 mg/5 mg/1,000 mg), hydroxypropyl cellulose, hypromellose, isopropyl alcohol, n-butyl alcohol, polyethylene glycol, propylene glycol, purified water, shellac glaze, talc, and titanium dioxide.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
TRIJARDY XR
TRIJARDY XR contains: empagliflozin, a SGLT2 inhibitor, linagliptin, a DPP-4 inhibitor, and metformin, a biguanide.
Empagliflozin
Empagliflozin is an inhibitor of the SGLT2, the predominant transporter responsible for reabsorption of glucose from the glomerular filtrate back into the circulation. By inhibiting SGLT2, empagliflozin reduces renal reabsorption of filtered glucose and lowers the renal threshold for glucose, and thereby increases urinary glucose excretion.
Linagliptin
Linagliptin is an inhibitor of DPP-4, an enzyme that degrades the incretin hormones glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP). Thus, linagliptin increases the concentrations of active incretin hormones, stimulating the release of insulin in a glucose-dependent manner and decreasing the levels of glucagon in the circulation. Both incretin hormones are involved in the physiological regulation of glucose homeostasis. Incretin hormones are secreted at a low basal level throughout the day and levels rise immediately after meal intake. GLP-1 and GIP increase insulin biosynthesis and secretion from pancreatic beta cells in the presence of normal and elevated blood glucose levels. Furthermore, GLP-1 also reduces glucagon secretion from pancreatic alpha cells, resulting in a reduction in hepatic glucose output.
Metformin HCl
Metformin is an antihyperglycemic agent which improves glucose tolerance in patients with type 2 diabetes mellitus, lowering both basal and postprandial plasma glucose. Metformin decreases hepatic glucose production, decreases intestinal absorption of glucose, and improves insulin sensitivity by increasing peripheral glucose uptake and utilization. With metformin therapy, insulin secretion remains unchanged while fasting insulin levels and day-long plasma insulin response may decrease.
12.2 Pharmacodynamics
Empagliflozin
Urinary Glucose Excretion
In patients with type 2 diabetes mellitus, urinary glucose excretion increased immediately following a dose of empagliflozin and was maintained at the end of a 4-week treatment period averaging at approximately 64 grams per day with 10 mg empagliflozin and 78 grams per day with 25 mg empagliflozin once daily. Data from single oral doses of empagliflozin in healthy subjects indicate that, on average, the elevation in urinary glucose excretion approaches baseline by about 3 days for the 10 mg and 25 mg doses.
Urinary Volume
In a 5-day study, mean 24-hour urine volume increase from baseline was 341 mL on Day 1 and 135 mL on Day 5 of empagliflozin 25 mg once daily treatment.
Cardiac Electrophysiology
In a randomized, placebo-controlled, active-comparator, crossover study, 30 healthy subjects were administered a single oral dose of empagliflozin 25 mg, empagliflozin 200 mg (8 times the maximum recommended dose), moxifloxacin, and placebo. No increase in QTc was observed with either 25 mg or 200 mg empagliflozin.
Linagliptin
Linagliptin binds to DPP-4 in a reversible manner and increases the concentrations of incretin hormones. Linagliptin glucose-dependently increases insulin secretion and lowers glucagon secretion, thus resulting in a better regulation of the glucose homeostasis. Linagliptin binds selectively to DPP-4 and selectively inhibits DPP-4, but not DPP-8 or DPP-9 activity in vitroat concentrations approximating therapeutic exposures.
Cardiac Electrophysiology
In a randomized, placebo-controlled, active-comparator, 4-way crossover study, 36 healthy subjects were administered a single oral dose of linagliptin 5 mg, linagliptin 100 mg (20 times the recommended dose), moxifloxacin, and placebo. No increase in QTc was observed with either the recommended dose of 5 mg or the 100 mg dose. At the 100 mg dose, peak linagliptin plasma concentrations were approximately 38-fold higher than the peak concentrations following a 5-mg dose.
12.3 Pharmacokinetics
TRIJARDY XR
Administration of TRIJARDY XR with food resulted in no change in overall exposure of empagliflozin or linagliptin. For metformin extended-release, high-fat meals increased systemic exposure (as measured by area-under-the-curve [AUC]) by approximately 70% relative to fasting, while C maxis not affected. Meals prolonged T maxby approximately 3 hours.
Empagliflozin
The pharmacokinetics of empagliflozin has been characterized in healthy volunteers and patients with type 2 diabetes mellitus and no clinically relevant differences were noted between the two populations. The steady-state mean plasma AUC and C maxwere 1,870 nmol∙h/L and 259 nmol/L, respectively, with 10 mg empagliflozin once daily treatment, and 4,740 nmol∙h/L and 687 nmol/L, respectively, with 25 mg empagliflozin once daily treatment. Systemic exposure of empagliflozin increased in a dose-proportional manner in the therapeutic dose range. Empagliflozin does not appear to have time-dependent pharmacokinetic characteristics. Following once-daily dosing, up to 22% accumulation, with respect to plasma AUC, was observed at steady-state.
Absorption
After oral administration, peak plasma concentrations of empagliflozin were reached at 1.5 hours post-dose. Administration of 25 mg empagliflozin after intake of a high-fat and high-calorie meal resulted in slightly lower exposure; AUC decreased by approximately 16% and C maxdecreased by approximately 37%, compared to fasted condition. The observed effect of food on empagliflozin pharmacokinetics was not considered clinically relevant and empagliflozin may be administered with or without food.
Distribution
The apparent steady-state volume of distribution was estimated to be 73.8 L based on a population pharmacokinetic analysis. Following administration of an oral [ 14C]-empagliflozin solution to healthy subjects, the red blood cell partitioning was approximately 36.8% and plasma protein binding was 86.2%.
Elimination
The apparent terminal elimination half-life of empagliflozin was estimated to be 12.4 h and apparent oral clearance was 10.6 L/h based on the population pharmacokinetic analysis.
Metabolism
No major metabolites of empagliflozin were detected in human plasma and the most abundant metabolites were three glucuronide conjugates (2-O-, 3-O-, and 6-O-glucuronide). Systemic exposure of each metabolite was less than 10% of total drug-related material. In vitrostudies suggested that the primary route of metabolism of empagliflozin in humans is glucuronidation by the uridine 5'-diphospho-glucuronosyltransferases UGT2B7, UGT1A3, UGT1A8, and UGT1A9.
Excretion
Following administration of an oral [ 14C]-empagliflozin solution to healthy subjects, approximately 95.6% of the drug-related radioactivity was eliminated in feces (41.2%) or urine (54.4%). The majority of drug-related radioactivity recovered in feces was unchanged parent drug and approximately half of drug-related radioactivity excreted in urine was unchanged parent drug.
Linagliptin
Absorption
The absolute bioavailability of linagliptin is approximately 30%. A high-fat meal reduced C maxby 15% and increased AUC by 4%; this effect is not clinically relevant. Linagliptin may be administered with or without food.
Distribution
The mean apparent volume of distribution at steady-state following a single intravenous dose of linagliptin 5 mg to healthy subjects is approximately 1,110 L, indicating that linagliptin extensively distributes to the tissues. Plasma protein binding of linagliptin is concentration-dependent, decreasing from about 99% at 1 nmol/L to 75% to 89% at ≥30 nmol/L, reflecting saturation of binding to DPP-4 with increasing concentration of linagliptin. At high concentrations, where DPP-4 is fully saturated, 70% to 80% of linagliptin remains bound to plasma proteins and 20% to 30% is unbound in plasma. Plasma binding is not altered in patients with renal or hepatic impairment.
Elimination
Linagliptin has a terminal half-life of about 200 hours at steady-state, though the accumulation half-life is about 11 hours. Renal clearance at steady-state was approximately 70 mL/min.
Metabolism
Following oral administration, the majority (about 90%) of linagliptin is excreted unchanged, indicating that metabolism represents a minor elimination pathway. A small fraction of absorbed linagliptin is metabolized to a pharmacologically inactive metabolite, which shows a steady-state exposure of 13.3% relative to linagliptin.
Metformin HCl extended-release
Absorption
Following a single oral dose of 1,000 mg (2 × 500 mg tablets) metformin HCl extended-release after a meal, the time to reach maximum plasma metformin concentration (T max) is achieved at approximately 7 to 8 hours. In both single- and multiple-dose studies in healthy subjects, once daily 1,000 mg (2 × 500 mg tablets) dosing provides equivalent systemic exposure, as measured by AUC, and up to 35% higher C maxof metformin relative to the immediate-release given as 500 mg twice daily.
Single oral doses of metformin HCl extended-release from 500 mg to 2,500 mg resulted in less than proportional increase in both AUC and C max. Low-fat and high-fat meals increased the systemic exposure (as measured by AUC) from metformin extended-release tablets by about 38% and 73%, respectively, relative to fasting. Both meals prolonged metformin T maxby approximately 3 hours but C max, was not affected.
Distribution
The apparent volume of distribution (V/F) of metformin following single oral doses of immediate-release metformin HCl tablets 850 mg averaged 654±358 L. Metformin is negligibly bound to plasma proteins. Metformin partitions into erythrocytes, most likely as a function of time.
Elimination
Metformin has a plasma elimination half-life of approximately 6.2 hours. In blood, the elimination half-life is approximately 17.6 hours, suggesting that the erythrocyte mass may be a compartment of distribution.
Metabolism
Intravenous single-dose studies in normal subjects demonstrate that metformin does not undergo hepatic metabolism (no metabolites have been identified in humans) nor biliary excretion.
Excretion
Following oral administration, approximately 90% of the absorbed drug is excreted via the renal route within the first 24 hours. Renal clearance is approximately 3.5 times greater than creatinine clearance, which indicates that tubular secretion is the major route of metformin elimination.
Specific Populations
Geriatric Patients
Empagliflozin: Age did not have a clinically meaningful impact on the pharmacokinetics of empagliflozin based on a population pharmacokinetic analysis [see Use in Specific Populations (8.5)] .
Metformin HCl: Limited data from controlled pharmacokinetic studies of metformin HCl in healthy elderly subjects suggest that total plasma clearance of metformin is decreased, the half-life is prolonged, and C maxis increased, compared with healthy young subjects. From these data, it appears that the change in metformin pharmacokinetics with aging is primarily accounted for by a change in renal function.
Effects of Age, Body Mass Index, Gender, and Race
Empagliflozin: Age, body mass index (BMI), gender and race (Asians versus primarily Whites) do not have a clinically meaningful effect on pharmacokinetics of empagliflozin.
Linagliptin: Based on the population PK analysis, age, body mass index (BMI), gender and race do not have a clinically meaningful effect on pharmacokinetics of linagliptin [see Use in Specific Populations (8.5)] .
Metformin HCl: Metformin pharmacokinetic parameters did not differ significantly between normal subjects and patients with type 2 diabetes mellitus when analyzed according to gender. Similarly, in controlled clinical studies in patients with type 2 diabetes mellitus, the antihyperglycemic effect of metformin was comparable in males and females.
No studies of metformin pharmacokinetic parameters according to race have been performed. In controlled clinical studies of metformin HCl in patients with type 2 diabetes mellitus, the antihyperglycemic effect was comparable in Whites (n=249), Blacks or African Americans (n=51), and Hispanics or Latinos (n=24).
Patients with Renal Impairment
TRIJARDY XR: Studies characterizing the pharmacokinetics of empagliflozin, linagliptin, and metformin after administration of TRIJARDY XR in renally impaired patients have not been performed.
Empagliflozin: In patients with mild (eGFR: 60 to less than 90 mL/min/1.73 m 2), moderate (eGFR: 30 to less than 60 mL/min/1.73 m 2), and severe (eGFR: less than 30 mL/min/1.73 m 2) renal impairment and patients on dialysis due to kidney failure, AUC of empagliflozin increased by approximately 18%, 20%, 66%, and 48%, respectively, compared to subjects with normal renal function. Peak plasma levels of empagliflozin were similar in patients with moderate renal impairment and patients on dialysis due to kidney failure compared to subjects with normal renal function. Peak plasma levels of empagliflozin were roughly 20% higher in patients with mild and severe renal impairment, as compared to subjects with normal renal function. Population pharmacokinetic analysis showed that the apparent oral clearance of empagliflozin decreased, with a decrease in eGFR leading to an increase in drug exposure. However, the fraction of empagliflozin that was excreted unchanged in urine, and urinary glucose excretion, declined with decrease in eGFR.
Linagliptin: An open-label pharmacokinetic study evaluated the pharmacokinetics of linagliptin 5 mg in male and female patients with varying degrees of chronic renal impairment. The study included 6 healthy subjects with normal renal function (creatinine clearance [CrCl] ≥80 mL/min), 6 patients with mild renal impairment (CrCl 50 to <80 mL/min), 6 patients with moderate renal impairment (CrCl 30 to <50 mL/min), 10 patients with type 2 diabetes mellitus and severe renal impairment (CrCl <30 mL/min), and 11 patients with type 2 diabetes mellitus and normal renal function. Creatinine clearance was measured by 24-hour urinary creatinine clearance measurements or estimated from serum creatinine based on the Cockcroft-Gault formula.
Under steady-state conditions, linagliptin exposure in patients with mild renal impairment was comparable to healthy subjects.
In patients with moderate renal impairment under steady-state conditions, mean exposure of linagliptin increased (AUC τ,ssby 71% and C maxby 46%), compared with healthy subjects. This increase was not associated with a prolonged accumulation half-life, terminal half-life, or an increased accumulation factor. Renal excretion of linagliptin was below 5% of the administered dose and was not affected by decreased renal function. Patients with type 2 diabetes mellitus and severe renal impairment showed steady-state exposure approximately 40% higher than that of patients with type 2 diabetes mellitus and normal renal function (increase in AUC τ,ssby 42% and C maxby 35%). For both type 2 diabetes mellitus groups, renal excretion was below 7% of the administered dose.
These findings were further supported by the results of population pharmacokinetic analyses.
Metformin HCl: In patients with decreased renal function, the plasma and blood half-life of metformin is prolonged and the renal clearance is decreased [see Contraindications (4)and Warnings and Precautions (5.1)] .
Patients with Hepatic Impairment
TRIJARDY XR: Studies characterizing the pharmacokinetics of empagliflozin, linagliptin, and metformin after administration of TRIJARDY XR in hepatically impaired patients have not been performed.
Empagliflozin: In patients with mild, moderate, and severe hepatic impairment according to the Child-Pugh classification, AUC of empagliflozin increased by approximately 23%, 47%, and 75% and C maxincreased by approximately 4%, 23%, and 48%, respectively, compared to subjects with normal hepatic function.
Linagliptin: In patients with mild hepatic impairment (Child-Pugh class A) steady-state exposure (AUC τ,ss) of linagliptin was approximately 25% lower and C max,sswas approximately 36% lower than in healthy subjects. In patients with moderate hepatic impairment (Child-Pugh class B), AUC ssof linagliptin was about 14% lower and C max,sswas approximately 8% lower than in healthy subjects. Patients with severe hepatic impairment (Child-Pugh class C) had comparable exposure of linagliptin in terms of AUC 0-24and approximately 23% lower C maxcompared with healthy subjects. Reductions in the pharmacokinetic parameters seen in patients with hepatic impairment did not result in reductions in DPP-4 inhibition.
Drug Interaction Studies
Pharmacokinetic drug interaction studies with TRIJARDY XR have not been performed; however, such studies have been conducted with the individual components of TRIJARDY XR (empagliflozin, linagliptin, and metformin HCl).
Empagliflozin
In vitro Assessment of Drug Interactions
Empagliflozin does not inhibit, inactivate, or induce CYP450 isoforms. In vitrodata suggest that the primary route of metabolism of empagliflozin in humans is glucuronidation by the uridine 5'-diphospho-glucuronosyltransferases UGT1A3, UGT1A8, UGT1A9 and UGT2B7. Empagliflozin does not inhibit UGT1A1, UGT1A3, UGT1A8, UGT1A9, or UGT2B7. Therefore, no effect of empagliflozin is anticipated on concomitantly administered drugs that are substrates of the major CYP450 isoforms or UGT1A1, UGT1A3, UGT1A8, UGT1A9, or UGT2B7. The effect of UGT induction (e.g., induction by rifampicin or any other UGT enzyme inducer) on empagliflozin exposure has not been evaluated.
Empagliflozin is a substrate for P-glycoprotein (P-gp) and breast cancer resistance protein (BCRP), but it does not inhibit these efflux transporters at therapeutic doses. Based on in vitrostudies, empagliflozin is considered unlikely to cause interactions with drugs that are P-gp substrates. Empagliflozin is a substrate of the human uptake transporters OAT3, OATP1B1, and OATP1B3, but not OAT1 and OCT2. Empagliflozin does not inhibit any of these human uptake transporters at clinically relevant plasma concentrations and, therefore, no effect of empagliflozin is anticipated on concomitantly administered drugs that are substrates of these uptake transporters.
In vivo Assessment of Drug Interactions
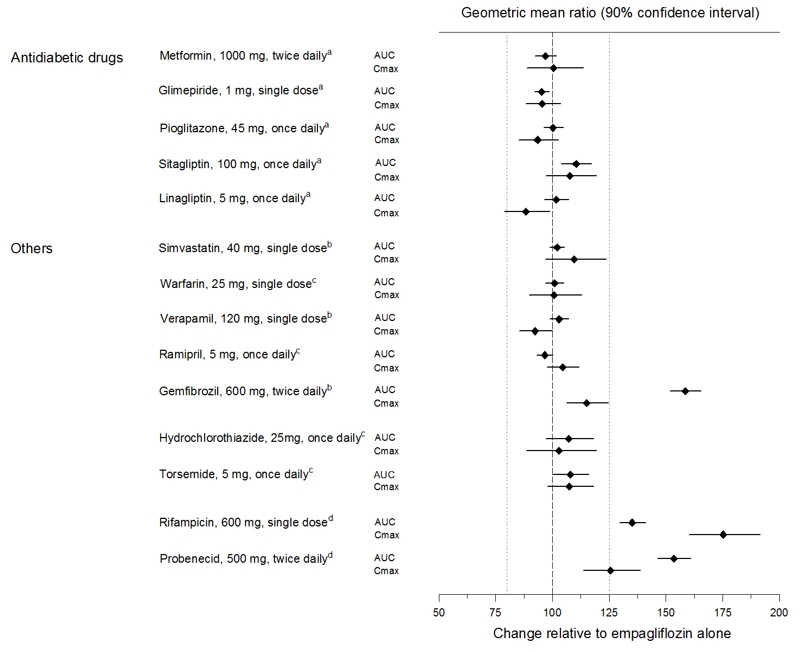
Empagliflozin pharmacokinetics were similar with and without coadministration of metformin, glimepiride, pioglitazone, sitagliptin, linagliptin, warfarin, verapamil, ramipril, and simvastatin in healthy volunteers and with or without coadministration of hydrochlorothiazide and torsemide in patients with type 2 diabetes mellitus (see Figure 1). In subjects with normal renal function, coadministration of empagliflozin with probenecid resulted in a 30% decrease in the fraction of empagliflozin excreted in urine without any effect on 24-hour urinary glucose excretion. The relevance of this observation to patients with renal impairment is unknown.
| aempagliflozin, 50 mg, once daily; bempagliflozin, 25 mg, single dose; cempagliflozin, 25 mg, once daily; dempagliflozin, 10 mg, single dose |
|
Figure 1 Effect of Various Medications on the Pharmacokinetics of Empagliflozin as Displayed as 90% Confidence Interval of Geometric Mean AUC and C maxRatios [reference lines indicate 100% (80% - 125%)] |
|
|
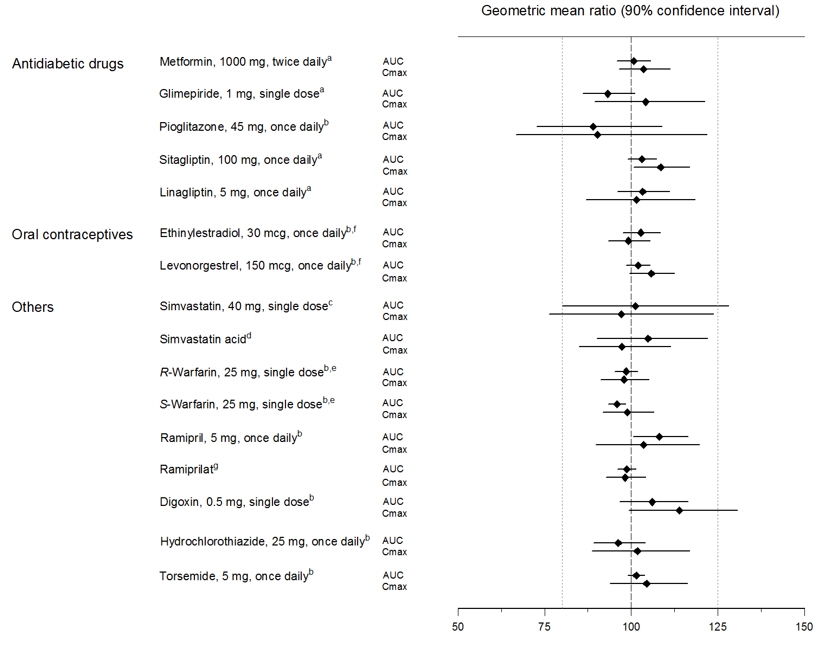
Empagliflozin had no clinically relevant effect on the pharmacokinetics of metformin, glimepiride, pioglitazone, sitagliptin, linagliptin, warfarin, digoxin, ramipril, simvastatin, hydrochlorothiazide, torsemide, and oral contraceptives when coadministered in healthy volunteers (see Figure 2).
| aempagliflozin, 50 mg, once daily; bempagliflozin, 25 mg, once daily; cempagliflozin, 25 mg, single dose; dadministered as simvastatin; eadministered as warfarin racemic mixture; fadministered as Microgynon ®; gadministered as ramipril |
|
Figure 2 Effect of Empagliflozin on the Pharmacokinetics of Various Medications as Displayed as 90% Confidence Interval of Geometric Mean AUC and C maxRatios [reference lines indicate 100% (80% - 125%)] |
|
|
Linagliptin
In vitro Assessment of Drug Interactions
Linagliptin is a weak to moderate inhibitor of CYP isozyme CYP3A4 but does not inhibit other CYP isozymes and is not an inducer of CYP isozymes, including CYP1A2, 2A6, 2B6, 2C8, 2C9, 2C19, 2D6, 2E1, and 4A11.
Linagliptin is a P-glycoprotein (P-gp) substrate and inhibits P-gp mediated transport of digoxin at high concentrations. Based on these results, and in vivodrug interaction studies, linagliptin is considered unlikely to cause interactions with other P-gp substrates at therapeutic concentrations.
In vivo Assessment of Drug Interactions
Strong inducers of CYP3A4 or P-gp (e.g., rifampin) decrease exposure to linagliptin to subtherapeutic and likely ineffective concentrations [see Drug Interactions (7)] . In vivostudies indicated evidence of a low propensity for causing drug interactions with substrates of CYP3A4, CYP2C9, CYP2C8, P-gp and organic cationic transporter (OCT).
Table 3 describes the effect of coadministered drugs on systemic exposure of linagliptin.
| Coadministered Drug | Dosing of Coadministered Drug a | Dosing of Linagliptin a | Geometric Mean Ratio
(ratio with/without coadministered drug) No effect=1.0 |
|
|---|---|---|---|---|
| AUC d | C max | |||
| aMultiple dose (steady-state) unless otherwise noted | ||||
| bFor information regarding clinical recommendations [see Drug Interactions (7)] . | ||||
| cSingle dose | ||||
| dAUC = AUC(0 to 24 hours) for single dose treatments and AUC = AUC(TAU) for multiple-dose treatments | ||||
| QD = once daily | ||||
| BID = twice daily | ||||
| TID = three times daily | ||||
| Metformin | 850 mg TID | 10 mg QD | 1.20 | 1.03 |
| Glyburide | 1.75 mg c | 5 mg QD | 1.02 | 1.01 |
| Pioglitazone | 45 mg QD | 10 mg QD | 1.13 | 1.07 |
| Ritonavir | 200 mg BID | 5 mg c | 2.01 | 2.96 |
| Rifampin b | 600 mg QD | 5 mg QD | 0.60 | 0.56 |
Table 4 describes the effect of linagliptin on systemic exposure of coadministered drugs.
| Coadministered Drug | Dosing of Coadministered Drug a | Dosing of Linagliptin a | Geometric Mean Ratio
(ratio with/without coadministered drug) No effect=1.0 |
||
|---|---|---|---|---|---|
| AUC c | C max | ||||
| aMultiple dose (steady-state) unless otherwise noted | |||||
| bSingle dose | |||||
| cAUC = AUC(INF) for single dose treatments and AUC = AUC(TAU) for multiple-dose treatments | |||||
| dAUC = AUC(0-168) and C max= E maxfor pharmacodynamic end points | |||||
| INR = International Normalized Ratio | |||||
| PT = Prothrombin Time | |||||
| QD = once daily | |||||
| TID = three times daily | |||||
| Metformin | 850 mg TID | 10 mg QD | metformin | 1.01 | 0.89 |
| Glyburide | 1.75 mg b | 5 mg QD | glyburide | 0.86 | 0.86 |
| Pioglitazone | 45 mg QD | 10 mg QD | pioglitazone
metabolite M-III metabolite M-IV | 0.94
0.98 1.04 | 0.86
0.96 1.05 |
| Digoxin | 0.25 mg QD | 5 mg QD | digoxin | 1.02 | 0.94 |
| Simvastatin | 40 mg QD | 10 mg QD | simvastatin
simvastatin acid | 1.34
1.33 | 1.10
1.21 |
| Warfarin | 10 mg b | 5 mg QD | R-warfarin
S-warfarin INR PT | 0.99
1.03 0.93 d 1.03 d | 1.00
1.01 1.04 d 1.15 d |
| Ethinylestradiol and levonorgestrel | ethinylestradiol 0.03 mg and levonorgestrel 0.150 mg QD | 5 mg QD | ethinylestradiol
levonorgestrel | 1.01
1.09 | 1.08
1.13 |
Metformin HCl
Table 5 describes the effect of coadministered drugs on plasma metformin systemic exposure.
| Coadministered Drug | Dosing of Coadministered Drug* | Dosing of Metformin HCl* | Geometric Mean Ratio
(ratio with/without coadministered drug) No effect=1.0 |
||
|---|---|---|---|---|---|
| AUC † | C max | ||||
| *All metformin and coadministered drugs were given as single doses | |||||
| †AUC = AUC(INF) | |||||
| ≠Metformin HCl extended-release tablets 500 mg | |||||
| ‡Ratio of arithmetic means | |||||
| **At steady-state with topiramate 100 mg every 12 hours and metformin 500 mg every 12 hours; AUC = AUC(0-12 hours) | |||||
| Glyburide | 5 mg | 500 mg≠ | metformin | 0.98‡ | 0.99‡ |
| Furosemide | 40 mg | 850 mg | metformin | 1.09‡ | 1.22‡ |
| Nifedipine | 10 mg | 850 mg | metformin | 1.16 | 1.21 |
| Propranolol | 40 mg | 850 mg | metformin | 0.90 | 0.94 |
| Ibuprofen | 400 mg | 850 mg | metformin | 1.05‡ | 1.07‡ |
| Cationic drugs eliminated by renal tubular secretion may reduce metformin elimination [see Drug Interactions (7)]. | |||||
| Cimetidine | 400 mg | 850 mg | metformin | 1.40 | 1.61 |
| Carbonic anhydrase inhibitors may cause metabolic acidosis [see Drug Interactions (7)] . | |||||
| Topiramate** | 100 mg | 500 mg | metformin | 1.25 | 1.17 |
Table 6 describes the effect of metformin on coadministered drug systemic exposure.
| Coadministered Drug | Dosing of Coadministered Drug* | Dosing of Metformin HCl* | Geometric Mean Ratio
(ratio with/without metformin) No effect=1.0 |
||
|---|---|---|---|---|---|
| AUC † | C max | ||||
| *All metformin and coadministered drugs were given as single doses | |||||
| †AUC = AUC(INF) unless otherwise noted | |||||
| §AUC(0-24 hours) reported | |||||
| ‡Ratio of arithmetic means, p-value of difference <0.05 | |||||
| ¶Ratio of arithmetic means | |||||
| Glyburide | 5 mg | 500 mg§ | glyburide | 0.78‡ | 0.63‡ |
| Furosemide | 40 mg | 850 mg | furosemide | 0.87‡ | 0.69‡ |
| Nifedipine | 10 mg | 850 mg | nifedipine | 1.10§ | 1.08 |
| Propranolol | 40 mg | 850 mg | propranolol | 1.01§ | 0.94 |
| Ibuprofen | 400 mg | 850 mg | ibuprofen | 0.97¶ | 1.01¶ |
| Cimetidine | 400 mg | 850 mg | cimetidine | 0.95§ | 1.01 |
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
TRIJARDY XR
No carcinogenicity, mutagenicity, or impairment of fertility studies have been conducted with the combination of empagliflozin, linagliptin, and metformin HCl.
Empagliflozin
Carcinogenesis was evaluated in 2-year studies conducted in CD-1 mice and Wistar rats. Empagliflozin did not increase the incidence of tumors in female rats dosed at 100, 300, or 700 mg/kg/day (up to 72 times the exposure from the maximum clinical dose of 25 mg). In male rats, hemangiomas of the mesenteric lymph node were increased significantly at 700 mg/kg/day or approximately 42 times the exposure from a 25 mg clinical dose. Empagliflozin did not increase the incidence of tumors in female mice dosed at 100, 300, or 1,000 mg/kg/day (up to 62 times the exposure from a 25 mg clinical dose). Renal tubule adenomas and carcinomas were observed in male mice at 1,000 mg/kg/day, which is approximately 45 times the exposure of the maximum clinical dose of 25 mg. These tumors may be associated with a metabolic pathway predominantly present in the male mouse kidney.
Empagliflozin was not mutagenic or clastogenic with or without metabolic activation in the in vitroAmes bacterial mutagenicity assay, the in vitroL5178Y tk +/-mouse lymphoma cell assay, and an in vivomicronucleus assay in rats.
Empagliflozin had no effects on mating, fertility or early embryonic development in treated male or female rats, up to the high dose of 700 mg/kg/day (approximately 155 times the 25 mg clinical dose in males and females, respectively).
Linagliptin
Linagliptin did not increase the incidence of tumors in male and female rats in a 2-year study at doses of 6, 18, and 60 mg/kg. The highest dose of 60 mg/kg is approximately 418 times the clinical dose of 5 mg/day based on AUC exposure. Linagliptin did not increase the incidence of tumors in mice in a 2-year study at doses up to 80 mg/kg (males) and 25 mg/kg (females), or approximately 35 and 270 times the clinical dose based on AUC exposure. Higher doses of linagliptin in female mice (80 mg/kg) increased the incidence of lymphoma at approximately 215 times the clinical dose based on AUC exposure.
Linagliptin was not mutagenic or clastogenic with or without metabolic activation in the Ames bacterial mutagenicity assay, a chromosomal aberration test in human lymphocytes, and an in vivomicronucleus assay.
In fertility studies in rats, linagliptin had no adverse effects on early embryonic development, mating, fertility, or bearing live young up to the highest dose of 240 mg/kg (approximately 943 times the clinical dose based on AUC exposure).
Metformin HCl
Long-term carcinogenicity studies have been performed in Sprague Dawley rats at doses of 150, 300, and 450 mg/kg/day in males and 150, 450, 900, and 1,200 mg/kg/day in females. These doses are approximately 2, 4, and 8 times in males, and 3, 7, 12, and 16 times in females of the maximum recommended human daily dose of 2,000 mg/kg/day based on body surface area comparisons. No evidence of carcinogenicity with metformin was found in either male or female rats. A carcinogenicity study was also performed in Tg.AC transgenic mice at doses of up to 2,000 mg/kg/day applied dermally. No evidence of carcinogenicity was observed in male or female mice.
Genotoxicity assessments in the Ames test, gene mutation test (mouse lymphoma cells), chromosomal aberrations test (human lymphocytes) and in vivomouse micronucleus tests were negative.
Fertility of male or female rats was not affected by metformin when administered at doses up to 600 mg/kg/day, which is approximately 3 times the maximum recommended human daily dose based on body surface area comparisons.
14 CLINICAL STUDIES
14.1 Empagliflozin and Linagliptin Add-on Combination Therapy with Metformin for Glycemic Control
A total of 686 patients with type 2 diabetes mellitus participated in a double-blind, active-controlled trial to evaluate the efficacy of empagliflozin 10 mg or 25 mg in combination with linagliptin 5 mg, compared to the individual components.
Patients with type 2 diabetes mellitus inadequately controlled on at least 1,500 mg of metformin per day entered a single-blind placebo run-in period for 2 weeks. At the end of the run-in period, patients who remained inadequately controlled and had an HbA1c between 7% and 10.5% were randomized 1:1:1:1:1 to one of 5 active-treatment arms of empagliflozin 10 mg or 25 mg, linagliptin 5 mg, or linagliptin 5 mg in combination with 10 mg or 25 mg empagliflozin as a fixed dose combination tablet.
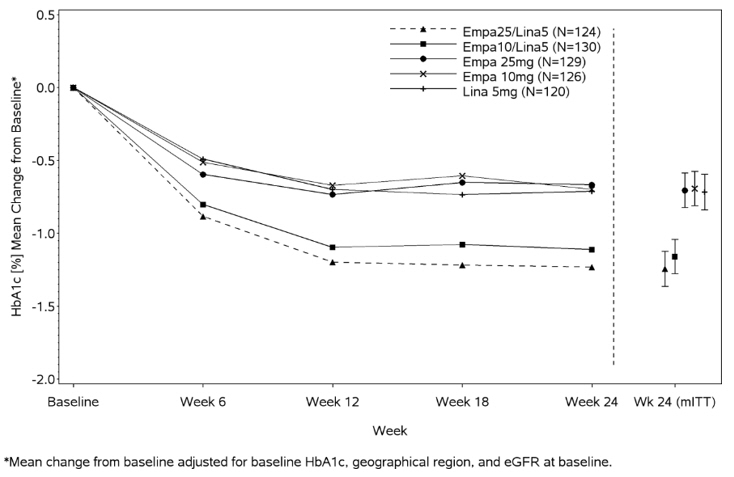
At Week 24, empagliflozin 10 mg or 25 mg used in combination with linagliptin 5 mg provided statistically significant improvement in HbA1c (p-value <0.0001) and FPG (p-value <0.001) compared to the individual components in patients who had been inadequately controlled on metformin (see Table 7, Figure 3). Treatment with empagliflozin 10 mg or 25 mg used in combination with linagliptin 5 mg also resulted in a statistically significant reduction in body weight compared to linagliptin 5 mg (p-value <0.0001). There was no statistically significant difference compared to empagliflozin alone.
| Empagliflozin
10 mg/ Linagliptin 5 mg | Empagliflozin
25 mg/ Linagliptin 5 mg | Empagliflozin
10 mg | Empagliflozin
25 mg | Linagliptin
5 mg |
|
|---|---|---|---|---|---|
| aFull analysis population (observed case) using MMRM. MMRM model included treatment, renal function, region, visit, visit by treatment interaction, and baseline HbA1c. | |||||
| bPatients with HbA1c above 7% at baseline: empagliflozin 25 mg/linagliptin 5 mg, n=123; empagliflozin 10 mg/linagliptin 5 mg, n=128; empagliflozin 25 mg, n=132; empagliflozin 10 mg, n=125; linagliptin 5 mg, n=119. Non-completers were considered failures (NCF). | |||||
| cFull analysis population using last observation carried forward. ANCOVA model included treatment, renal function, region, baseline weight, and baseline HbA1c. | |||||
| dp<0.001 for FPG; p<0.0001 for HbA1c and body weight | |||||
| HbA1c (%) | |||||
| Number of patients | n=135 | n=133 | n=137 | n=139 | n=128 |
| Baseline (mean) | 8.0 | 7.9 | 8.0 | 8.0 | 8.0 |
| Change from baseline (adjusted mean) | -1.1 | -1.2 | -0.7 | -0.6 | -0.7 |
| Comparison vs empagliflozin 25 mg or 10 mg (adjusted mean) (95% CI) a | -0.4 (-0.6, -0.2) d | -0.6 (-0.7, -0.4) d | -- | -- | -- |
| Comparison vs linagliptin 5 mg (adjusted mean) (95% CI) a | -0.4 (-0.6, -0.2) d | -0.5 (-0.7, -0.3) d | -- | -- | -- |
| Patients [n (%)] achieving HbA1c <7% b | 74 (58) | 76 (62) | 35 (28) | 43 (33) | 43 (36) |
| FPG (mg/dL) | |||||
| Number of patients | n=133 | n=131 | n=136 | n=137 | n=125 |
| Baseline (mean) | 157 | 155 | 162 | 160 | 156 |
| Change from baseline (adjusted mean) | -33 | -36 | -21 | -21 | -13 |
| Comparison vs empagliflozin 25 mg or 10 mg (adjusted mean) (95% CI) a | -12 (-18, -5) d | -15 (-22, -9) d | -- | -- | -- |
| Comparison vs linagliptin 5 mg (adjusted mean) (95% CI) a | -20 (-27, -13) d | -23 (-29, -16) d | -- | -- | -- |
| Body Weight | |||||
| Number of patients | n=135 | n=134 | n=137 | n=140 | n=128 |
| Baseline (mean) in kg | 87 | 85 | 86 | 88 | 85 |
| % change from baseline (adjusted mean) | -3.1 | -3.4 | -3.0 | -3.5 | -0.7 |
| Comparison vs empagliflozin 25 mg or 10 mg (adjusted mean) (95% CI) c | 0.0 (-0.9, 0.8) | 0.1 (-0.8, 0.9) | -- | -- | -- |
| Comparison vs linagliptin 5 mg (adjusted mean) (95% CI) c | -2.4 (-3.3, -1.5) d | -2.7 (-3.6, -1.8) d | -- | -- | -- |
Figure 3 Adjusted Mean HbA1c Change at Each Time Point (Completers) and at Week 24 (mITT population)
14.2 Empagliflozin Cardiovascular Outcomes in Patients with Type 2 Diabetes Mellitus and Atherosclerotic Cardiovascular Disease
EMPA-REG OUTCOME was a multicenter, multinational, randomized, double-blind parallel group trial that compared the risk of experiencing a major adverse cardiovascular event (MACE) between empagliflozin and placebo when these were added to and used concomitantly with standard of care treatments for diabetes mellitus and atherosclerotic CV disease. Concomitant antidiabetic medications were kept stable for the first 12 weeks of the trial. Thereafter, antidiabetic and atherosclerotic therapies could be adjusted, at the discretion of investigators, to ensure participants were treated according to the standard care for these diseases.
A total of 7,020 patients were treated (empagliflozin 10 mg = 2,345; empagliflozin 25 mg = 2,342; placebo = 2,333) and followed for a median of 3.1 years. Approximately 72% of the trial population was White, 22% was Asian, and 5% was Black or African American. The mean age was 63 years and approximately 72% were male.
All patients in the trial had inadequately controlled type 2 diabetes mellitus at baseline (HbA1c greater than or equal to 7%). The mean HbA1c at baseline was 8.1% and 57% of participants had diabetes mellitus for more than 10 years. Approximately 31%, 22% and 20% reported a past history of neuropathy, retinopathy and nephropathy to investigators, respectively and the mean eGFR was 74 mL/min/1.73 m 2. At baseline, patients were treated with one (~30%) or more (~70%) antidiabetic medications including metformin (74%), insulin (48%), sulfonylurea (43%) and dipeptidyl peptidase-4 inhibitor (11%).
All patients had established atherosclerotic CV disease at baseline including one (82%) or more (18%) of the following: a documented history of coronary artery disease (76%), stroke (23%) or peripheral artery disease (21%). At baseline, the mean systolic blood pressure was 136 mmHg, the mean diastolic blood pressure was 76 mmHg, the mean LDL was 86 mg/dL, the mean HDL was 44 mg/dL, and the mean urinary albumin to creatinine ratio (UACR) was 175 mg/g. At baseline, approximately 81% of patients were treated with renin angiotensin system inhibitors, 65% with beta-blockers, 43% with diuretics, 77% with statins, and 86% with antiplatelet agents (mostly aspirin).
The primary endpoint in EMPA-REG OUTCOME was the time to first occurrence of a Major Adverse Cardiac Event (MACE). A major adverse cardiac event was defined as occurrence of either a CV death or a non-fatal myocardial infarction (MI) or a non-fatal stroke. The statistical analysis plan had pre-specified that the 10 and 25 mg doses would be combined. A Cox proportional hazards model was used to test for non-inferiority against the pre-specified risk margin of 1.3 for the hazard ratio of MACE and superiority on MACE if non-inferiority was demonstrated. Type-1 error was controlled across multiples tests using a hierarchical testing strategy.
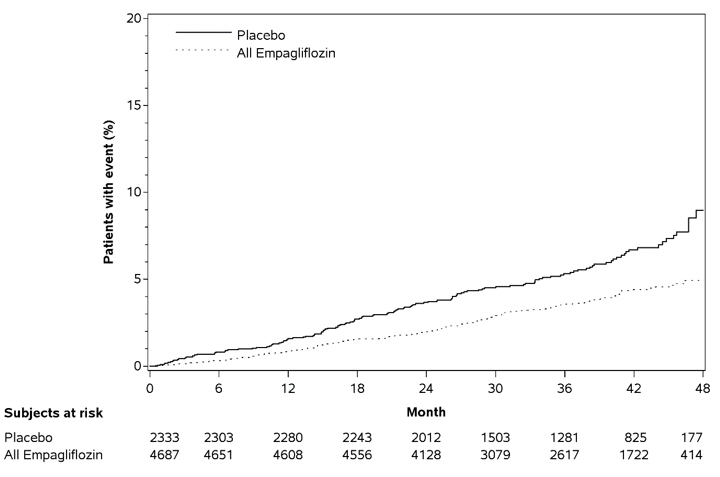
Empagliflozin significantly reduced the risk of first occurrence of primary composite endpoint of CV death, non-fatal myocardial infarction, or non-fatal stroke (HR: 0.86; 95% CI: 0.74, 0.99). The treatment effect was due to a significant reduction in the risk of CV death in subjects randomized to empagliflozin (HR: 0.62; 95% CI: 0.49, 0.77), with no change in the risk of non-fatal myocardial infarction or non-fatal stroke (see Table 8and Figures 4and 5). Results for the 10 mg and 25 mg empagliflozin doses were consistent with results for the combined dose groups.
| Placebo
N=2,333 | Empagliflozin
N=4,687 | Hazard ratio vs placebo
(95% CI) |
|
|---|---|---|---|
| aTreated set (patients who had received at least one dose of trial drug) | |||
| bp−value for superiority (2−sided) 0.04 | |||
| cTotal number of events | |||
| Composite of CV death, non-fatal myocardial infarction, non-fatal stroke
(time to first occurrence) b | 282 (12.1%) | 490 (10.5%) | 0.86 (0.74, 0.99) |
| Non-fatal myocardial infarction c | 121 (5.2%) | 213 (4.5%) | 0.87 (0.70, 1.09) |
| Non-fatal stroke c | 60 (2.6%) | 150 (3.2%) | 1.24 (0.92, 1.67) |
| CV death c | 137 (5.9%) | 172 (3.7%) | 0.62 (0.49, 0.77) |
Figure 4 Estimated Cumulative Incidence of First MACE
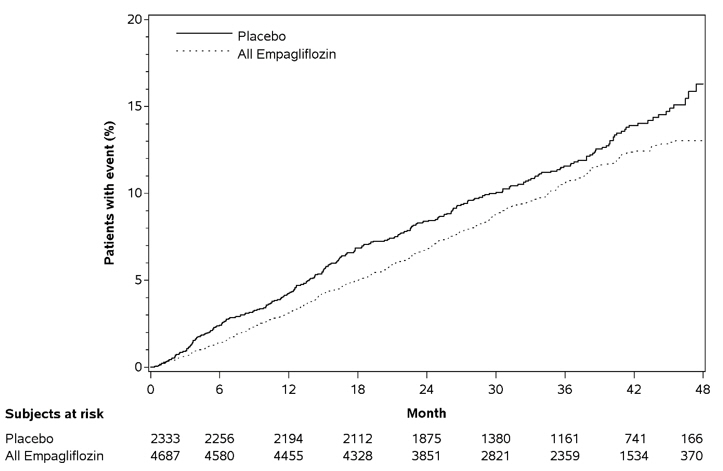
Figure 5 Estimated Cumulative Incidence of CV Death
The efficacy of empagliflozin on CV death was generally consistent across major demographic and disease subgroups.
Vital status was obtained for 99.2% of subjects in the trial. A total of 463 deaths were recorded during the EMPA-REG OUTCOME trial. Most of these deaths were categorized as CV deaths. The non-CV deaths were only a small proportion of deaths and were balanced between the treatment groups (2.1% in patients treated with empagliflozin, and 2.4% of patients treated with placebo).
14.3 Linagliptin Cardiovascular Safety Trials in Patients with Type 2 Diabetes Mellitus
CARMELINA
The CV risk of linagliptin was evaluated in CARMELINA (NCT0189753), a multinational, multi-center, placebo-controlled, double-blind, parallel group trial comparing linagliptin (N=3,494) to placebo (N=3,485) in adult patients with type 2 diabetes mellitus and a history of established macrovascular and/or renal disease. The trial compared the risk of major adverse cardiovascular events (MACE) between linagliptin and placebo when these were added to standard of care treatments for diabetes mellitus and other CV risk factors. The trial was event driven, the median duration of follow-up was 2.2 years and vital status was obtained for 99.7% of patients.
Patients were eligible to enter the trial if they were adults with type 2 diabetes mellitus, with HbA1c of 6.5% to 10%, and had either albuminuria and previous macrovascular disease (39% of enrolled population), or evidence of impaired renal function by eGFR and Urinary Albumin Creatinine Ratio (UACR) criteria (42% of enrolled population), or both (18% of enrolled population).
At baseline the mean age was 66 years, and the population was 63% male, 80% White, 9% Asian, 6% Black or African American and 36% were of Hispanic or Latino ethnicity. Mean HbA1c was 8.0% and mean duration of type 2 diabetes mellitus was 15 years. The trial population included 17% patients ≥75 years of age and 62% patients with renal impairment defined as eGFR <60 mL/min/1.73 m 2. The mean eGFR was 55 mL/min/1.73 m 2and 27% of patients had mild renal impairment (eGFR 60 to 90 mL/min/1.73 m 2), 47% of patients had moderate renal impairment (eGFR 30 to <60 mL/min/1.73 m 2) and 15% of patients had severe renal impairment (eGFR <30 mL/min/1.73 m 2). Patients were taking at least one antidiabetic drug (97%), and the most common were insulin and analogues (57%), metformin (54%) and sulfonylurea (32%). Patients were also taking antihypertensives (96%), lipid lowering drugs (76%) with 72% on statin, and aspirin (62%).
The primary endpoint, MACE, was the time to first occurrence of one of three composite outcomes which included CV death, non-fatal myocardial infarction or non-fatal stroke. The trial was designed as a non-inferiority trial with a pre-specified risk margin of 1.3 for the hazard ratio of MACE. A total of 434 patients on linagliptin and 420 patients on placebo experienced MACE. The incidence rate of MACE in both treatment arms: 56.3 MACE per 1,000 patient-years on placebo vs. 57.7 MACE per 1,000 patient-years on linagliptin. The estimated hazard ratio for MACE associated with linagliptin relative to placebo was 1.02 with a 95% confidence interval of (0.89, 1.17). The upper bound of this confidence interval, 1.17, excluded the risk margin of 1.3.
CAROLINA
The CV risk of linagliptin was evaluated in CAROLINA, a multi-center, multinational, randomized, double-blind parallel group trial comparing linagliptin (N=3,023) to glimepiride (N=3,010) in adult patients with type 2 diabetes mellitus and a history of established CV disease and/or multiple CV risk factors. The trial compared the risk of major adverse cardiovascular events (MACE) between linagliptin and glimepiride when these were added to standard of care treatments for diabetes mellitus and other CV risk factors. The trial was event driven, the median duration of follow-up was 6.23 years and vital status was obtained for 99.3% of patients.
Patients were eligible to enter the trial if they were adults with type 2 diabetes mellitus with insufficient glycemic control (defined as HbA1c of 6.5% to 8.5% or 6.5% to 7.5% depending on treatment-naïve, on monotherapy or on combination therapy), and were defined to be at high CV risk with previous vascular disease, evidence of vascular related end-organ damage, age ≥70 years, and/or two CV risk factors (duration of diabetes mellitus >10 years, systolic blood pressure >140 mmHg, current smoker, LDL cholesterol ≥135 mg/dL).
At baseline the mean age was 64 years and the population was 60% male, 73% White, 18% Asian, 5% Black or African American, and 17% were of Hispanic or Latino ethnicity. The mean HbA1c was 7.15% and mean duration of type 2 diabetes mellitus was 7.6 years. The trial population included 34% patients ≥70 years of age and 19% patients with renal impairment defined as eGFR <60 mL/min/1.73 m 2. The mean eGFR was 77 mL/min/1.73 m 2. Patients were taking at least one antidiabetic drug (91%) and the most common were metformin (83%) and sulfonylurea (28%). Patients were also taking antihypertensives (89%), lipid lowering drugs (70%) with 65% on statin, and aspirin (47%).
The primary endpoint, MACE, was the time to first occurrence of one of three composite outcomes which included CV death, non-fatal myocardial infarction or non-fatal stroke. The trial was designed as a non-inferiority trial with a pre-specified risk margin of 1.3 for the hazard ratio of MACE. A total of 356 patients on linagliptin and 362 patients on glimepiride experienced MACE. The incidence rate of MACE in both treatment arms: 20.7 MACE per 1,000 patient-years on linagliptin vs. 21.2 MACE per 1,000 patient-years on glimepiride. The estimated hazard ratio for MACE associated with linagliptin relative to glimepiride was 0.98 with a 95% confidence interval of (0.84, 1.14). The upper bound of this confidence interval, 1.14, excluded the risk margin of 1.3.
16 HOW SUPPLIED/STORAGE AND HANDLING
TRIJARDY XR tablets are available as follows:
| Tablet Strength | Color/Shape | Tablet Markings | Package Size | NDC Number |
|---|---|---|---|---|
| 5 mg Empagliflozin
2.5 mg Linagliptin 1,000 mg Metformin HCl Extended-Release | grey, oval-shaped,
film-coated tablet | Printed on one side in white ink with the Boehringer Ingelheim company symbol and "395" on the top line and "5/2.5" on the bottom line. | Bottles of 60
Bottles of 180 | 0597-0395-82
0597-0395-23 |
| 10 mg Empagliflozin
5 mg Linagliptin 1,000 mg Metformin HCl Extended-Release | tan, oval-shaped,
film-coated tablet | Printed on one side in white ink with the Boehringer Ingelheim company symbol and "380" on the top line and "10/5" on the bottom line. | Bottles of 30
Bottles of 90 | 0597-0380-13
0597-0380-68 |
| 12.5 mg Empagliflozin
2.5 mg Linagliptin 1,000 mg Metformin HCl Extended-Release | red, oval-shaped,
film-coated tablet | Printed on one side in white ink with the Boehringer Ingelheim company symbol and "385" on the top line and "12.5/2.5" on the bottom line. | Bottles of 60
Bottles of 180 | 0597-0385-77
0597-0385-86 |
| 25 mg Empagliflozin
5 mg Linagliptin 1,000 mg Metformin HCl Extended-Release | brown, oval-shaped,
film-coated tablet | Printed on one side in white ink with the Boehringer Ingelheim company symbol and "390" on the top line and "25/5" on the bottom line. | Bottles of 30
Bottles of 90 | 0597-0390-71
0597-0390-13 |
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Medication Guide).
Lactic Acidosis
Inform patients of the risks of lactic acidosis due to metformin, its symptoms, and conditions that predispose to its development. Advise patients to discontinue TRIJARDY XR immediately and to notify their healthcare provider promptly if unexplained hyperventilation, malaise, myalgia, unusual somnolence, or other nonspecific symptoms occur. Counsel patients against excessive alcohol intake and inform patients about importance of regular testing of renal function while receiving TRIJARDY XR. Instruct patients to inform their healthcare provider that they are taking TRIJARDY XR prior to any surgical or radiological procedure, as temporary discontinuation may be required until renal function has been confirmed to be normal [see Warnings and Precautions (5.1)] .
Diabetic Ketoacidosis in Patients with Type 1 Diabetes Mellitus and Other Ketoacidosis
Inform patients that TRIJARDY XR can cause potentially fatal ketoacidosis and that type 2 diabetes mellitus and pancreatic disorders (e.g., history of pancreatitis or pancreatic surgery) are risk factors.
Educate all patients on precipitating factors (such as insulin dose reduction or missed insulin doses, infection, reduced caloric intake, ketogenic diet, surgery, dehydration, and alcohol abuse) and symptoms of ketoacidosis (including nausea, vomiting, abdominal pain, tiredness, and labored breathing). Inform patients that blood glucose may be normal even in the presence of ketoacidosis.
Advise patients that they may be asked to monitor ketones. If symptoms of ketoacidosis occur, instruct patients to discontinue TRIJARDY XR and seek medical attention immediately [see Warnings and Precautions (5.2)] .
Pancreatitis
Inform patients that acute pancreatitis has been reported during use of linagliptin. Inform patients that persistent severe abdominal pain, sometimes radiating to the back, which may or may not be accompanied by vomiting, is the hallmark symptom of acute pancreatitis. Instruct patients to discontinue TRIJARDY XR promptly and contact their healthcare provider if persistent severe abdominal pain occurs [see Warnings and Precautions (5.3)] .
Volume Depletion
Inform patients that symptomatic hypotension may occur with TRIJARDY XR and advise them to contact their healthcare provider if they experience such symptoms [see Warnings and Precautions (5.4)] . Inform patients that dehydration may increase the risk for hypotension, and to maintain adequate fluid intake.
Serious Urinary Tract Infections
Inform patients of the potential for urinary tract infections, which may be serious. Provide them with information on the symptoms of urinary tract infections. Advise them to seek medical advice if such symptoms occur [see Warnings and Precautions (5.5)] .
Hypoglycemia with Concomitant Use with Insulin and Insulin Secretagogues
Inform patients that the risk of hypoglycemia is increased when TRIJARDY XR is used in combination with an insulin secretagogue (e.g., sulfonylurea) or insulin [see Warnings and Precautions (5.6)] .
Necrotizing Fasciitis of the Perineum (Fournier's Gangrene)
Inform patients that necrotizing infections of the perineum (Fournier's gangrene) have occurred with empagliflozin, a component of TRIJARDY XR. Counsel patients to promptly seek medical attention if they develop pain or tenderness, redness, or swelling of the genitals or the area from the genitals back to the rectum, along with a fever above 100.4°F or malaise [see Warnings and Precautions (5.7)].
Genital Mycotic Infections in Females (e.g., Vulvovaginitis)
Inform female patients that vaginal yeast infections may occur and provide them with information on the signs and symptoms of vaginal yeast infections. Advise them of treatment options and when to seek medical advice [see Warnings and Precautions (5.8)] .
Genital Mycotic Infections in Males (e.g., Balanitis or Balanoposthitis)
Inform male patients that yeast infection of the penis (e.g., balanitis or balanoposthitis) may occur, especially in uncircumcised males and patients with chronic and recurrent infections. Provide them with information on the signs and symptoms of balanitis and balanoposthitis (rash or redness of the glans or foreskin of the penis). Advise them of treatment options and when to seek medical advice [see Warnings and Precautions (5.8)] .
Lower Limb Amputation
Counsel patients about the importance of routine preventative foot care. Instruct patients to monitor for new pain or tenderness, sores or ulcers, or infections involving the leg or foot and to seek medical advice immediately if such signs or symptoms develop [see Warnings and Precautions (5.9)] .
Hypersensitivity Reactions
Inform patients that serious allergic reactions, such as anaphylaxis, angioedema, and exfoliative skin conditions, have been reported during postmarketing use of linagliptin or empagliflozin, components of TRIJARDY XR. If symptoms of allergic reactions (such as rash, skin flaking or peeling, urticaria, swelling of the skin, or swelling of the face, lips, tongue, and throat that may cause difficulty in breathing or swallowing) occur, patients must stop taking TRIJARDY XR and seek medical advice promptly [see Warnings and Precautions (5.10)] .
Vitamin B 12Deficiency
Inform patients about the importance of regular hematological parameters while receiving TRIJARDY XR [see Warnings and Precautions (5.11)] .
Severe and Disabling Arthralgia
Inform patients that severe and disabling joint pain may occur with this class of drugs. The time to onset of symptoms can range from one day to years. Instruct patients to seek medical advice if severe joint pain occurs [see Warnings and Precautions (5.12)] .
Bullous Pemphigoid
Inform patients that bullous pemphigoid has been reported during use of linagliptin. Instruct patients to seek medical advice if blisters or erosions occur [see Warnings and Precautions (5.13)].
Heart Failure
Inform patients of the signs and symptoms of heart failure. Before initiating TRIJARDY XR, patients should be asked about a history of heart failure or other risk factors for heart failure including moderate to severe renal impairment. Instruct patients to contact their healthcare provider as soon as possible if they experience symptoms of heart failure, including increasing shortness of breath, rapid increase in weight or swelling of the feet [see Warnings and Precautions (5.14)] .
Laboratory Tests
Inform patients that elevated glucose in urinalysis is expected when taking TRIJARDY XR [see Drug Interactions (7)] .
Pregnancy
Advise pregnant patients, and patients of reproductive potential, of the potential risk to a fetus with treatment with TRIJARDY XR [see Use in Specific Populations (8.1)] . Instruct patients to report pregnancies to their healthcare provider as soon as possible.
Lactation
Advise patients that breastfeeding is not recommended during treatment with TRIJARDY XR [see Use in Specific Populations (8.2)].
Patients of Reproductive Potential
Inform patients that treatment with metformin may result in ovulation in some premenopausal anovulatory patients, which may lead to unintended pregnancy [see Use in Specific Populations (8.3)] .
Administration Instructions
Inform patients that the tablets must be swallowed whole and never split, crushed, dissolved, or chewed and that incompletely dissolved TRIJARDY XR tablets may be eliminated in the feces.
Missed Dose
Instruct patients to take TRIJARDY XR only as prescribed. If a dose is missed, it should be taken as soon as the patient remembers. Advise patients not to double their next dose [see Dosage and Administration (2.6)] .
Distributed by:
Boehringer Ingelheim Pharmaceuticals, Inc.
Ridgefield, CT 06877 USA
Marketed by:
Boehringer Ingelheim Pharmaceuticals, Inc.
Ridgefield, CT 06877 USA
and
Eli Lilly and Company
Indianapolis, IN 46285 USA
Licensed from:
Boehringer Ingelheim International GmbH, Ingelheim, Germany.
TRIJARDY is a registered trademark of and used under license from Boehringer Ingelheim International GmbH.
Boehringer Ingelheim Pharmaceuticals, Inc. either owns or uses the Jardiance ®, Tradjenta ®, EMPA-REG OUTCOME ®, CARMELINA ®, and CAROLINA ®trademarks under license.
The other brands listed are trademarks of their respective owners and are not trademarks of Boehringer Ingelheim Pharmaceuticals, Inc.
Copyright © 2023 Boehringer Ingelheim International GmbH
ALL RIGHTS RESERVED
COL9014DK032023
SPL9015D
| MEDICATION GUIDE
TRIJARDY ®XR (try-JAR-dee XR) (empagliflozin, linagliptin, and metformin hydrochloride extended-release tablets) for oral use |
|||||
|---|---|---|---|---|---|
| This Medication Guide has been approved by the U.S. Food and Drug Administration. | Revised: October 2023 | ||||
| What is the most important information I should know about TRIJARDY XR?
TRIJARDY XR can cause serious side effects, including:
|
|||||
|
| ||||
You have a higher chance of getting lactic acidosis with TRIJARDY XR if you:
|
|||||
|
|||||
|
| ||||
|
|||||
|
| ||||
| Stop taking TRIJARDY XR and call your healthcare provider right away if you have pain in your stomach area (abdomen) that is severe and will not go away. The pain may be felt going from your abdomen to your back. The pain may happen with or without vomiting. These may be symptoms of pancreatitis. | |||||
|
|||||
|
|||||
|
| ||||
|
|||||
|
| ||||
| Talk to your healthcare provider about what to do if you get symptoms of a yeast infection of the vagina or penis. Your healthcare provider may suggest you use an over-the-counter antifungal medicine. Talk to your healthcare provider right away if you use an over-the-counter antifungal medication and your symptoms do not go away. | |||||
| What is TRIJARDY XR?
TRIJARDY XR is a prescription medicine that contains 3 diabetes medicines, empagliflozin (JARDIANCE), linagliptin (TRADJENTA), and metformin HCl. TRIJARDY XR can be used:
|
|||||
| Who should not take TRIJARDY XR?
Do not take TRIJARDY XR if you:
|
|||||
| What should I tell my healthcare provider before taking TRIJARDY XR?
Before taking TRIJARDY XR, tell your healthcare provider about all of your medical conditions, including if you:
|
|||||
How should I take TRIJARDY XR?
|
|||||
| What should I avoid while taking TRIJARDY XR?
Avoid drinking alcohol very often or drinking a lot of alcohol in a short period of time ("binge" drinking). It can increase your chances of getting serious side effects. |
|||||
| What are the possible side effects of TRIJARDY XR?
TRIJARDY XR may cause serious side effects, including:
|
|||||
|
|
|
| ||
|
|||||
|
|
| |||
|
|||||
| The most common side effects of TRIJARDY XR include: | |||||
|
| ||||
| Tell your healthcare provider if you have any side effect that bothers you or that does not go away.
These are not all the possible side effects of TRIJARDY XR. For more information, ask your healthcare provider or pharmacist. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. |
|||||
How should I store TRIJARDY XR?
|
|||||
| General information about the safe and effective use of TRIJARDY XR.
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use TRIJARDY XR for a condition for which it was not prescribed. Do not give TRIJARDY XR to other people, even if they have the same symptoms that you have. It may harm them. You can ask your pharmacist or healthcare provider for information about TRIJARDY XR that is written for health professionals. |
|||||
| What are the ingredients in TRIJARDY XR?
Active ingredients:empagliflozin, linagliptin, and metformin hydrochloride Inactive ingredients:Tablet core contains: hypromellose, magnesium stearate, and polyethylene oxide. The Film Coatings and Printing Ink contain: ammonium hydroxide, arginine, carnauba wax, ferric oxide yellow and ferric oxide red (10 mg/5 mg/1,000 mg), ferrosoferric oxide and ferric oxide red (12.5 mg/2.5 mg/1,000 mg), ferrosoferric oxide and ferric oxide yellow (5 mg/2.5 mg/1,000 mg and 25 mg/5 mg/1,000 mg), hydroxypropyl cellulose, hypromellose, isopropyl alcohol, n-butyl alcohol, polyethylene glycol, propylene glycol, purified water, shellac glaze, talc, and titanium dioxide. |
|||||
| Distributed by: Boehringer Ingelheim Pharmaceuticals, Inc. Ridgefield, CT 06877 USA
Marketed by: Boehringer Ingelheim Pharmaceuticals, Inc. Ridgefield, CT 06877 USA and Eli Lilly and Company, Indianapolis, IN 46285 USA Licensed from: Boehringer Ingelheim International GmbH, Ingelheim, Germany TRIJARDY is a registered trademark of and used under license from Boehringer Ingelheim International GmbH. Boehringer Ingelheim Pharmaceuticals, Inc. either owns or uses the Jardiance ®, Tradjenta ®, EMPA-REG OUTCOME ®, CARMELINA ®, and CAROLINA ®trademarks under license. The other brands listed are trademarks of their respective owners and are not trademarks of Boehringer Ingelheim Pharmaceuticals, Inc. Copyright © 2023 Boehringer Ingelheim International GmbH ALL RIGHTS RESERVED COL9014DK032023 For more information about TRIJARDY XR, including current prescribing information and Medication Guide, go to www.trijardyxr.com, scan the code, or call Boehringer Ingelheim Pharmaceuticals, Inc. at 1-800-542-6257.
|
|||||

PRINCIPAL DISPLAY PANEL - 5 mg/2.5 mg/1,000 mg Tablet Bottle Label
NDC: 0597-0395-82
Trijardy
®XR
(empagliflozin, linagliptin, and metformin
hydrochloride extended-release tablets)
5 mg/2.5 mg/1,000 mg*
DISPENSE WITH ACCOMPANYING MEDICATION GUIDE
60 tablets
Rx only
Boehringer
Ingelheim
Lilly
PRINCIPAL DISPLAY PANEL - 10 mg/5 mg/1,000 mg Tablet Bottle Label
NDC: 0597-0380-13
Trijardy
®XR
(empagliflozin, linagliptin,
and metformin hydrochloride
extended-release tablets)
10 mg/5 mg/1,000 mg*
DISPENSE WITH ACCOMPANYING
MEDICATION GUIDE
30 tablets
Rx only
Boehringer
Ingelheim
Lilly
PRINCIPAL DISPLAY PANEL - 12.5 mg/2.5 mg/1,000 mg Tablet Bottle Label
NDC: 0597-0385-77
Trijardy
®XR
(empagliflozin, linagliptin, and metformin
hydrochloride extended-release tablets)
12.5 mg/2.5 mg/1,000 mg*
DISPENSE WITH ACCOMPANYING MEDICATION GUIDE
60 tablets
Rx only
Boehringer
Ingelheim
Lilly
PRINCIPAL DISPLAY PANEL - 25 mg/5 mg/1,000 mg Tablet Bottle Label
NDC: 0597-0390-71
Trijardy
®XR
(empagliflozin, linagliptin,
and metformin hydrochloride
extended-release tablets)
25 mg/5 mg/1,000 mg*
DISPENSE WITH ACCOMPANYING
MEDICATION GUIDE
30 tablets
Rx only
Boehringer
Ingelheim
Lilly
| TRIJARDY XR
empagliflozin, linagliptin, metformin hydrochloride tablet, extended release |
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
| TRIJARDY XR
empagliflozin, linagliptin, metformin hydrochloride tablet, extended release |
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
|
||||||||||||||||||
| Labeler - Praxis, LLC (016329513) |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Praxis, LLC | 016329513 | label(59368-389, 59368-390) , manufacture(59368-389, 59368-390) , pack(59368-389, 59368-390) | |
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.