ALVESCO ®(ciclesonide) inhalation aerosol, for oral inhalation use
Alvesco by
Drug Labeling and Warnings
Alvesco by is a Prescription medication manufactured, distributed, or labeled by Praxis, LLC. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
ALVESCO- ciclesonide aerosol, metered
Praxis, LLC
----------
ALVESCO ®(ciclesonide) inhalation aerosol, for oral inhalation use
7 DRUG INTERACTIONS
In clinical studies, concurrent administration of ciclesonide and other drugs commonly used in the treatment of asthma (albuterol, formoterol) had no effect on pharmacokinetics of des-ciclesonide [see Clinical Pharmacology ( 12.3)] .
In vitrostudies and clinical pharmacology studies suggested that des-ciclesonide has no potential for metabolic drug interactions or protein binding-based drug interactions [see Clinical Pharmacology ( 12.3)] .
In a drug interaction study, co-administration of orally inhaled ciclesonide and oral ketoconazole, a potent inhibitor of cytochrome P450 3A4, increased the exposure (AUC) of des-ciclesonide by approximately 3.6-fold at steady state, while levels of ciclesonide remained unchanged.
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
There are no available data on ALVESCO use in pregnant women to assess a drug associated risk of major birth defects, miscarriage, or adverse maternal or fetal outcomes. There is low systemic exposure following ALVESCO oral inhalation administration at the recommended dose [see Clinical Pharmacology ( 12.3)] .
In animal reproduction studies, ciclesonide administered by the oral route to pregnant rats during the period of organogenesis did not cause any evidence of fetal harm at doses up to 15 times the maximum recommended human daily oral inhalation dose (MRHDOID) of 640 mcg/day. Teratogenicity, characteristic of corticosteroids, decreased body weight and/or skeletal variations were observed in rabbit fetuses following administration of ciclesonide to pregnant rabbits by the subcutaneous route during the period of organogenesis at doses 0.15 times the MRHDOID and higher on a mcg/m 2basis (see Data). No evidence of fetal harm was observed in rabbits at doses of 0.03 times the MRHDOID.
All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. In the United States general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Clinical Considerations
Disease-Associated Maternal and/or Embryo/Fetal Risk
In women with poorly or moderately controlled asthma, there is an increased risk of several perinatal outcomes such as pre‑eclampsia in the mother and prematurity, low birth weight, and small for gestational age in the neonate. Pregnant women with asthma should be closely monitored and medication adjusted as necessary to maintain optimal asthma control.
Data
Animal Data
In an embryo-fetal development study in pregnant rats dosed by the oral route during the period of organogenesis from gestation days 6 to 15, ciclesonide did not cause any evidence of fetal harm at doses up to approximately 15 times the MRHDOID in adults (on a mcg/m 2basis with maternal oral dose up to 900 mcg/kg/day). Maternal toxicity, as evidenced by decreased body weight gain, was observed at approximately 15 times the MRHDOID in adults (on a mcg/m 2basis at a maternal dose of 900 mcg/kg/day); however, no adverse effects were observed at doses 5 times the MRHDOID and lower (on a mcg/m 2basis with maternal oral doses of 300 mcg/kg/day and lower).
In two embryo-fetal development studies in pregnant rabbits dosed by the subcutaneous route during the period of organogenesis from gestation days 6 to 18, ciclesonide caused acampsia (flexures of legs) in fetuses at doses 0.15 times the MRHDOID and higher (on a mcg/m 2basis with maternal oral doses of 5 mcg/kg/day and higher), decreased body weight, cleft palate, enlarged fontanelle, parchment-like skin, and incomplete ossification of bones in fetuses at doses 0.76 times the MRHDOID (on a mcg/m 2basis with a maternal subcutaneous dose of 25 mcg/kg/day), and embryo-fetal death at doses 3 times the MRHDOID and higher (on a mcg/m 2basis with maternal subcutaneous doses of 100 mcg/kg/day and higher). No evidence of fetal harm was observed at a dose 0.03 times the MRHDOID in adults (on a mcg/m 2basis at a maternal subcutaneous dose of 1 mcg/kg/day). Maternal toxicity was observed at doses 3 times the MRHDOID in adults (on a mcg/m 2basis with maternal subcutaneous doses of 100 mcg/kg/day and lower); however, no evidence of toxicity was observed at doses 0.76 times the MRHDOID and lower (on a mcg/m 2basis with maternal subcutaneous doses of 25 mcg/kg/day and lower).
In a prenatal and postnatal development study in pregnant rats dosed by the oral route from gestation day 6 to lactation day 20, ciclesonide produced no adverse developmental effects on offspring at doses up to approximately 15 times the MRHDOID (on a mcg/m 2basis at maternal oral doses up to 900 mcg/kg/day).
8.2 Lactation
Risk Summary
There are no data on the presence of ciclesonide or its metabolite in human milk, the effects on the breastfed infant, or the effects on milk production. It is not known whether oral inhalation administration of ciclesonide at the recommended dose could result in sufficient systemic absorption to produce detectable quantities in human milk [seeClinical Pharmacology ( 12.3)] . The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for ALVESCO, and any potential adverse effects on the breastfed infant from ALVESCO, or from the underlying maternal condition.
Clinical Considerations
The molecular weight of the prodrug ciclesonide (approximately 541 g/mol) is small enough to be excreted into breast milk; however, its high plasma protein binding affinity and very short half-life suggests that minimal amounts will be present within the milk. Conversely, the half-life of the active metabolite des-ciclesonide (approximately 471 g/mol) suggests that exposure to the nursing infant will be greater than that of the prodrug ciclesonide. Although ciclesonide and des-ciclesonide have negligible oral bioavailability (both less than 1% for each) due to low gastrointestinal absorption and high first-pass metabolism, the relative anti‑inflammatory activity of des-ciclesonide is 120 times greater than that of the ciclesonide and 12 times greater than that of dexamethasone [seeClinical Pharmacology ( 12.1)] . The effects of this exposure on a nursing infant are unknown, however, like all corticosteroids, suppression of the HPA function is a potential complication.
8.4 Pediatric Use
The safety and effectiveness of ALVESCO for the maintenance treatment of asthma as prophylactic therapy have been established in pediatric patients aged 12 years and older. Use of ALVESCO for this indication is supported by evidence from randomized, double-blind, placebo-controlled, parallel-group clinical trials in adult and pediatric patients 12 years of age and older with mild persistent to severe persistent asthma [see Clinical Studies ( 14)] .
The safety and effectiveness of ALVESCO have not been established in pediatric patients younger than 12 years of age.
Pediatric Patients 4 to 11 years of age
Effectiveness was not demonstrated in two randomized, double-blind, placebo-controlled studies that were conducted to evaluate the efficacy of ALVESCO 40, 80, or 160 mcg administered once daily for 12 weeks in patients 4 to 11 years of age with asthma. These studies included 1018 patients previously using either controller therapy (predominately inhaled corticosteroids) or reliever therapy (bronchodilator therapy alone). The patients had a mean baseline percent predicted FEV 1of 68%. The primary efficacy endpoint was morning pre-dose FEV 1. Other measures of efficacy included AM PEF, asthma symptoms, and rescue albuterol use. The studies showed inconsistent results and did not establish the efficacy of ALVESCO in patients 4 to 11 years of age.
Pediatric Patients 2 to 6 years of age
Effectiveness was not demonstrated in one randomized, double-blind, placebo-controlled study that was conducted to evaluate the efficacy of ALVESCO 40, 80, and 160 mcg administered once daily for 24 weeks in 992 patients 2 to 6 years of age with persistent asthma. The primary efficacy endpoint was time to the first severe asthma exacerbation [defined as worsening of asthma which required treatment with systemic (including oral) steroids or any other asthma medication besides treatment medication and rescue medication] or lack of improvement, whichever occurred first. No statistically significant differences were observed for the individual comparisons of ALVESCO 40, 80, and 160 mcg to placebo. Results from this study did not establish efficacy of ALVESCO in patients 2 to 6 years of age.
Studies in children under 2 years of age have not been conducted given the lack of efficacy observed in patients 2 to 11 years of age.
Effect on Growth
Controlled clinical studies have shown that orally inhaled corticosteroids may cause a reduction in growth velocity in pediatric patients. In these studies, the mean reduction in growth velocity was approximately one centimeter per year (range 0.3 to 1.8 cm per year) and appears to be related to dose and duration of exposure. This effect has been observed in the absence of laboratory evidence of hypothalamic-pituitary-adrenal (HPA) axis suppression, suggesting that growth velocity is a more sensitive indicator of systemic corticosteroid exposure in pediatric patients than some commonly used tests of HPA axis function. The long-term effects of this reduction in growth velocity associated with orally inhaled corticosteroids, including the impact on final adult height, are unknown. The potential for "catch up" growth following discontinuation of treatment with orally inhaled corticosteroids has not been adequately studied. The growth of pediatric patients receiving orally inhaled corticosteroids, including ALVESCO, should be monitored routinely (e.g., via stadiometry).
A 52-week, multi-center, double-blind, randomized, placebo-controlled, parallel-group study was conducted to assess the effect of orally inhaled ciclesonide on growth rate in 609 pediatric patients with mild persistent asthma, aged 5 to 8.5 years. Treatment groups included orally inhaled ciclesonide 40 mcg or 160 mcg or placebo given once daily. Growth was measured by stadiometer height during the baseline, treatment and follow-up periods. The primary comparison was the difference in growth rates between ciclesonide 40 mcg and 160 mcg and placebo groups. Conclusions cannot be drawn from this study because compliance could not be assured. There was no difference in efficacy measures between the placebo and the ALVESCO groups. Ciclesonide blood levels were also not measured during the one-year treatment period.
The potential growth effects of prolonged treatment with orally inhaled corticosteroids should be weighed against clinical benefits obtained and the availability of safe and effective noncorticosteroid treatment alternatives. To minimize the systemic effects of orally inhaled corticosteroids, including ALVESCO, each patient should be titrated to his/her lowest effective dose.
8.5 Geriatric Use
Clinical studies of ALVESCO did not include sufficient numbers of patients aged 65 years and older to determine whether they respond differently than younger patients. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range reflecting the greater frequency of decreased hepatic, renal, or cardiac function and of concomitant disease or other drug therapy.
10 OVERDOSAGE
Chronic overdosage may result in signs/symptoms of hypercorticism [see Warnings and Precautions ( 5.5)] .
11 DESCRIPTION
The active component of ALVESCO 80 mcg, and ALVESCO 160 mcg is ciclesonide, a non-halogenated glucocorticoid having the chemical name pregna-1,4-diene-3,20-dione, 16,17-[[(R)-cyclohexylmethylene]bis(oxy)]-11-hydroxy-21-(2-methyl-1-oxopropoxy)-,(11β,16α). The empirical formula is C 32H 44O 7and its molecular weight is 540.7. Its structural formula is as follows:
Ciclesonide is a white to yellow-white powder. It is soluble in dehydrated alcohol, acetone, dichloromethane, and chloroform.
ALVESCO 80 mcg and ALVESCO 160 mcg are pressurized, metered-dose aerosol units fitted with a dose indicator. ALVESCO is intended for oral inhalation only. Each unit contains a solution of ciclesonide in propellant HFA-134a (1,1,1,2 tetrafluoroethane) and ethanol. After priming, ALVESCO 80 mcg delivers 100 mcg from the valve and 80 mcg of ciclesonide from the actuator. ALVESCO 160 mcg delivers 200 mcg from the valve and 160 mcg of ciclesonide from the actuator. This product delivers 50 microliters (59.3 milligrams) of solution as a fine particle mist from the valve with each actuation. The actual amount of drug delivered to the lung may depend on patient factors, such as the coordination between the actuation of the device and inspiration through the delivery system. ALVESCO should be “primed” by actuating 3 times prior to using the first dose from a new canister or when the inhaler has not been used for more than 10 days. Avoid spraying in the eyes or face while priming ALVESCO.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Ciclesonide is a prodrug that is enzymatically hydrolyzed to a pharmacologically active metabolite, C21-desisobutyryl-ciclesonide (des-ciclesonide or RM1) following oral inhalation. Des-ciclesonide has anti-inflammatory activity with affinity for glucocorticoid receptors that is 120 times greater than the parent compound and 12 times greater than dexamethasone. The clinical significance of these findings is unknown.
The precise mechanisms of corticosteroid action in asthma are unknown. Inflammation is recognized as an important component in the pathogenesis of asthma. Corticosteroids have been shown to have a wide range of inhibitory activities against multiple cell types (e.g., mast cells, eosinophils, basophils, lymphocytes, macrophages, and neutrophils) and mediators (e.g., histamine, eicosanoids, leukotrienes, and cytokines) involved in the asthmatic response. These anti-inflammatory actions of corticosteroids may contribute to their efficacy in asthma. Though effective for the treatment of asthma, corticosteroids do not affect asthma symptoms immediately. Individual patients will experience a variable time to onset and degree of symptom relief. Maximum benefit may not be achieved for four weeks or longer after starting treatment. When corticosteroids are discontinued, asthma stability may persist for several days or longer.
12.2 Pharmacodynamics
The effect of ciclesonide by oral inhalation on the HPA axis was assessed in adults with mild asthma in a 29-day placebo-controlled study. Twenty-four-hour urinary-free cortisol was assessed in a total of 59 adults who were randomized to 320 mcg or 640 mcg ALVESCO, a comparator corticosteroid, or placebo twice daily. At the end of 29 days of treatment, the mean (SE) change from baseline in 24-hr urinary-free cortisol was -8.69 (5.6) mcg/day, -4.01 (5.03) mcg/day, and -8.84 (5.02) mcg/day for the placebo, ALVESCO 640 mcg/day, and ALVESCO 1280 mcg/day, respectively. The difference from placebo for the change from baseline in 24-hr urinary-free cortisol was +4.7 mcg/day [95% CI: -10.58; 19.93] and -0.16 mcg/day [95% CI: -15.20; 14.89] for the 640 mcg/day or 1280 mcg/day treatments, respectively. The effects observed with the comparator corticosteroid validate the sensitivity of the study to assess the effect of ciclesonide on the HPA axis.
12.3 Pharmacokinetics
Absorption: Ciclesonide and des-ciclesonide have negligible oral bioavailability (both are less than 1%) due to low gastrointestinal absorption and high first-pass metabolism. Serum concentrations of ciclesonide and des-ciclesonide were measured and compared following oral inhalation of 1280 mcg ALVESCO and intravenous administration of 800 mcg ciclesonide. The absolute bioavailability of ciclesonide was 22% and the relative systemic exposure of des-ciclesonide was 63%. The mean C maxfor des-ciclesonide was 1.02 ng/mL (range 0.6-1.5 ng/mL) in asthmatic patients following a single dose of 1280 mcg by oral inhalation. The mean C max(0.369 ng/mL) and AUC 0-∞(2.18 ng·hr/mL) of des‑ciclesonide following multiple dose administration of ciclesonide 320 mcg once daily increased up to 26% compared to single dose administration.
Distribution: Following intravenous administration of 800 mcg of ciclesonide, the volumes of distribution of ciclesonide and des-ciclesonide was approximately 2.9 L/kg and 12.1 L/kg, respectively. The percentage of ciclesonide and des-ciclesonide bound to human plasma proteins averaged ≥ 99% each, with ≤ 1% of unbound drug detected in the systemic circulation. Des-ciclesonide is not significantly bound to human transcortin.
Elimination: Following intravenous administration of 800 mcg of ciclesonide, the clearances of ciclesonide and des-ciclesonide were high (approximately 152 L/L/hr and 228 L/L/hr, respectively). 14C-labeled ciclesonide was predominantly excreted via the feces after intravenous administration (66%) indicating that excretion through bile is the major route of elimination. Approximately 20% or less of des-ciclesonide was excreted in the urine. The mean half-life of ciclesonide and des-ciclesonide was 0.71 hours and 6 to 7 hours, respectively. T maxof des-ciclesonide occurs at 1.04 hours following inhalation of ciclesonide.
Metabolism: Ciclesonide is hydrolyzed to a biologically active metabolite, des-ciclesonide, by esterases. Des-ciclesonide undergoes further metabolism in the liver to additional metabolites mainly by the cytochrome P450 (CYP) 3A4 isozyme and to a lesser extent by CYP 2D6. The full range of potentially active metabolites of ciclesonide has not been characterized. After intravenous administration of 14C-ciclesonide, 19.3% of the resulting radioactivity in the plasma is accounted for by ciclesonide or des-ciclesonide; the remainder may be a result of other, as yet, unidentified multiple metabolites.
Specific Populations: Population pharmacokinetic analysis showed that characteristics of des-ciclesonide after oral inhalation of ciclesonide were not appreciably influenced by a variety of subject characteristics such as body weight, age, race, and gender.
Patients with Renal Impairment: Studies in renally-impaired patients were not conducted since renal excretion of des-ciclesonide is a minor route of elimination (≤ 20%).
Patients with Hepatic Impairment: Compared to healthy subjects, the systemic exposure of des-ciclesonide (C maxand AUC) in patients with moderate to severe liver impairment increased in the range of 1.4 to 2.7 fold after 1280 mcg ex-actuator ciclesonide by oral inhalation. Dose adjustment in patients with liver impairment is not necessary.
Drug Interaction Studies: In a drug interaction study, co-administration of orally inhaled ciclesonide and oral ketoconazole, a potent inhibitor of cytochrome P450 3A4, increased the exposure (AUC) of ciclesonide active metabolite, des-ciclesonide, by approximately 3.6-fold at steady state, while levels of ciclesonide remained unchanged [see Drug Interactions ( 7)] .
In another single-dose drug interaction study, co-administration of orally inhaled ciclesonide and oral erythromycin, an inhibitor of cytochrome P450 3A4, had no effect on the pharmacokinetics of either ciclesonide and the active metabolite, des-ciclesonide, or erythromycin.
Based on in vitrostudies in human liver microsomes, des-ciclesonide had no significant potential to inhibit or induce the metabolism of other drugs metabolized by CYP450 enzymes. The inhibitory potential of ciclesonide on CYP450 isoenzymes has not been studied. Based on in vitrohuman hepatocyte studies, ciclesonide and des-ciclesonide had no potential to induce major CYP450 isozymes.
In vitrostudies demonstrated that the plasma protein binding of des-ciclesonide was not affected by warfarin or salicylic acid, indicating no potential for protein binding-based drug interactions.
In a population pharmacokinetic analysis including 98 subjects, co-administration of ALVESCO and albuterol had no effect on the pharmacokinetics of des-ciclesonide.
Concomitant administration of ALVESCO (640 mcg) and formoterol (24 mcg) did not change the pharmacokinetics of either des-ciclesonide or formoterol.
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Two-year carcinogenicity studies in B6C3F1 mice and Wistar rats were conducted to assess the carcinogenic potential of ciclesonide. Ciclesonide demonstrated no tumorigenic potential in a study with mice that received oral doses up to 900 mcg/kg/day (approximately 7 times the MRHDOID in adults and pediatric patients ≥ 12 years of age on a mcg/m 2basis) and a study with rats that received inhalation doses up to 193 mcg/kg/day (approximately 3 times the MRHDOID in adults and pediatric patients ≥ 12 years of age on a mcg/m 2basis).
Ciclesonide was not mutagenic in an Ames test or in the Chinese hamster lung V79 cell/hypoxanthine-guanine phosphoribosyl transferase (HGPRT) forward mutation assay and was not clastogenic in a human lymphocyte chromosomal aberration assay or in an in vitromicronucleus test. However, ciclesonide was clastogenic in an in vivomouse micronucleus test. The concurrent reference corticosteroid (dexamethasone) in this study showed similar findings.
Fertility and reproductive performance were unaffected in male and female rats dosed by the oral route up to 900 mcg/kg/day (approximately 15 times the MRHDOID in adults based on mcg/m 2).
14 CLINICAL STUDIES
14.1 Asthma
Adults and Pediatric Patients 12 Years of Age and Older
The efficacy of ALVESCO was evaluated in six randomized, double-blind, placebo-controlled, parallel-group clinical trials in adult and pediatric patients 12 years of age and older with mild persistent to severe persistent asthma. The six trials included two trials in which patients were treated with ALVESCO administered once daily for 12 weeks, two trials in which patients were treated with ALVESCO twice daily for 12 weeks, and two trials in which patients were treated with ALVESCO using once daily and twice daily dosing regimens for 12 or 16 weeks. These trials included a total of 2843 patients (1167 males and 1676 females) of whom 296 were pediatric patients 12 to 17 years of age. The primary efficacy endpoint in four of the six trials was the mean change from baseline in pre-dose FEV 1at endpoint (last observation). FEV 1was measured prior to the morning dose of study medication (at the end of the 24-hour dosing interval for once daily administration, and at the end of the 12-hour dosing interval for twice daily administration). In one of the six trials, the primary endpoint was the change from baseline in the average of the pre-dose FEV 1at Weeks 12 and 16, and in another trial, reduction of oral corticosteroid use was the primary efficacy endpoint. Additional efficacy variables were asthma symptoms, use of albuterol for rescue, AM PEF, nighttime awakenings, and withdrawal due to asthma worsening.
The two once daily dosing trials were identically designed and were conducted to evaluate the efficacy of ALVESCO 80, 160, and 320 mcg given once daily in the morning for 12 weeks in patients with mild to moderate asthma maintained on inhaled bronchodilators and/or corticosteroids. The results of these trials, along with other trials that explored twice daily dosing, indicate that once daily dosing is not the optimum dosing regimen for ALVESCO.
Four trials were designed to evaluate the efficacy of ALVESCO administered twice daily in patients with asthma who were previously maintained on bronchodilators alone, patients who were previously maintained on inhaled corticosteroids, and patients who were previously maintained on oral corticosteroids.
Patients Previously Maintained on Bronchodilators Alone
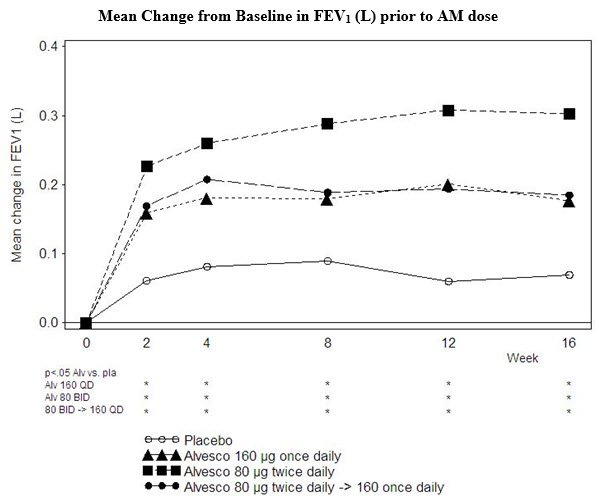
The efficacy of ALVESCO was studied in a randomized, double-blind, placebo-controlled trial in 691 patients with mild-to-moderate persistent asthma (mean baseline percent predicted FEV 1of 72%) previously using reliever therapy (bronchodilator therapy alone). In this trial, patients were treated with ALVESCO 160 mcg once daily in the morning for 16 weeks, ALVESCO 80 mcg twice daily for 16 weeks, or ALVESCO 80 mcg twice daily for 4 weeks followed by ALVESCO 160 mcg once daily in the morning for 12 weeks or placebo for 16 weeks. Compared to placebo, all ALVESCO doses showed statistically significant improvement at Week 16 in AM pre-dose FEV 1. However, the increase in AM pre-dose FEV 1in the patients treated with ALVESCO 80 mcg twice daily was significantly greater than that observed in patients treated with ALVESCO 160 mcg administered once daily. Compared to placebo, increases in AM pre-dose FEV 1were 0.12 L or 5.0% for ALVESCO 160 mcg once daily, 0.24 L or 10.4% for ALVESCO 80 mcg twice daily, 0.13 L or 5.0% for ALVESCO 80 mcg twice daily for 4 weeks followed by ALVESCO 160 mcg once daily. Other measures of asthma control, AM PEF, and need for rescue albuterol also improved in all the ALVESCO treatment groups compared to placebo but the improvement was greatest with the ALVESCO 80 mcg twice daily treatment arm. Discontinuations from the study for lack of efficacy were lower in the ALVESCO treatment groups compared to placebo. Fewer patients receiving ALVESCO experienced asthma worsening than did patients receiving placebo. The AM pre-dose FEV 1results are shown in Figure 1below.
Patients Previously Maintained on Inhaled Corticosteroids
The efficacy of ALVESCO in asthma patients previously maintained on inhaled corticosteroids was evaluated in two randomized, double-blind, placebo-controlled trials of 12-weeks treatment duration. In one trial, asthmatic patients with mild to moderate persistent asthma (mean baseline percent predicted FEV 1of 79%), previously maintained on controller therapy (predominantly inhaled corticosteroids) were treated with ALVESCO 160 mcg once daily in the morning, ALVESCO 80 mcg twice daily or placebo.
The AM pre-dose FEV 1results are shown in Figure 2below.

Statistically significantly more increases in AM pre-dose FEV 1compared to placebo were seen at 12 weeks for ALVESCO 160 mcg once daily (0.14 L or 5.7%) and ALVESCO 80 mcg twice daily (0.19 L or 7.5%). Asthma symptoms scores, AM PEF, and decreased need for rescue albuterol remained relatively stable in the ALVESCO treatment groups compared to slight worsening in the placebo. Compared to placebo, fewer patients receiving ALVESCO experienced worsening of asthma.
In the other trial, 257 patients with moderate to severe persistent asthma (mean baseline percent predicted FEV 1of 54%) were treated with ALVESCO 160 or 320 mcg twice daily for 12 weeks. The AM pre-dose FEV 1results are shown in Figure 3below.
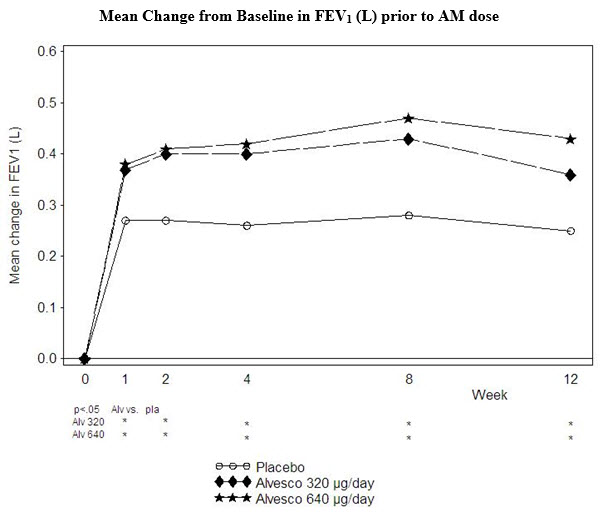
Compared to placebo, both ALVESCO doses showed statistically significantly more improvement in pre-dose FEV 1(0.11 L or 8.6% and 0.18 L or 11.8%). Other measures of asthma control, AM PEF, symptoms, and need for rescue albuterol also showed improvement compared to placebo. Compared to placebo, fewer patients treated with ALVESCO experienced worsening of asthma.
Patients treated with ALVESCO were also less likely to discontinue study participation due to asthma deterioration.
Patients Previously Maintained on Oral Corticosteroids
In a 12-week double-blind clinical trial, 140 patients with severe persistent asthma (mean FEV 1at baseline 53% predicted) who had failed prior efforts to eliminate oral prednisone use and had established their lowest effective prednisone dose were randomized to ALVESCO given by oral inhalation at doses of 320 or 640 mcg twice daily or placebo. The average prednisone dose at baseline was approximately 12 mg/day. Compared to patients on placebo whose prednisone requirements increased by 4%, those treated with ALVESCO 320 mcg and 640 mcg twice daily significantly reduced their prednisone requirements by 47% and 62%, respectively. At the same time, patients on ALVESCO maintained asthma control as reflected by lung function, symptoms, and need for rescue albuterol. A significantly larger percentage of patients on ALVESCO were able to reduce oral prednisone use by 50% or more as compared to placebo (64% and 77% of the patients treated with 320 mcg and 640 mcg, respectively twice daily as compared with 33% of patients on placebo). There was no statistically significant difference observed with ALVESCO 640 mcg twice daily compared to ALVESCO 320 mcg twice daily.
16 HOW SUPPLIED/STORAGE AND HANDLING
ALVESCO is available in the following strengths and canister presentations.
|
Micrograms per Actuation |
Number of Actuations per Canister |
Canister Weight |
Canister per Box |
NDC Number |
|
ALVESCO
|
60 |
6.1 g |
1 |
70515-711-01 |
|
ALVESCO
|
60 |
6.1 g |
1 |
70515-712-01 |
|
ALVESCO
|
30 |
4.7 g |
1 |
70515-711-04 |
|
ALVESCO
|
30 |
4.7 g |
1 |
70515-712-04 |
|
ALVESCO
|
60 |
6.1 g |
1 |
70515-711-05 |
|
ALVESCO
|
60 |
6.1 g |
1 |
70515-712-05 |
ALVESCO (ciclesonide) 80 mcg inhalation aerosol is supplied with a brown plastic actuator with a red dust cap. Each actuation of the inhaler delivers 80 mcg of ciclesonide from the actuator and contains 60 actuations fill/canister.
ALVESCO 160 (ciclesonide) mcg inhalation aerosol is supplied with a red plastic actuator with a red dust cap. Each actuation of the inhaler delivers 160 mcg of ciclesonide from the actuator and contains 60 actuations fill/canister.
ALVESCO canisters are for use with ALVESCO actuators only. The actuators are fitted with a dose indicator and should not be used with other medications. The correct amount of medication in each actuation cannot be assured from the canister labeled to contain 60 actuations when the dose indicator display window shows zero even though the canister is not completely empty. The canister should be discarded when the dose indicator display window shows zero.
Store at 25°C (77°F). Excursions between 15°C and 30°C (59°F and 86°F) are permitted (see USP). For optimal results, the canister should be at room temperature when used.
Contents under pressure. Do not puncture. Do not use or store near heat or open flame. Exposure to temperatures above 49°C (120°F) may cause bursting. Never throw canister into fire or incinerator.
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient Information and Instructions for Use)
Oropharyngeal Candidiasis
Patients should be advised that localized infections with Candida albicansoccurred in the mouth and pharynx in some patients. If oropharyngeal candidiasis develops, it should be treated with appropriate local or systemic (i.e., oral) antifungal therapy while still continuing with ALVESCO therapy, but at times therapy with the ALVESCO inhaler may need to be temporarily interrupted under close medical supervision. Rinsing the mouth after inhalation is advised [see Warnings and Precautions ( 5.1)] .
Acute Asthma Episodes
Patients should be advised that ALVESCO is not a bronchodilator and is not intended for use as rescue medication for acute asthma exacerbations. Acute asthma symptoms should be treated with an inhaled, short-acting beta 2-agonist such as albuterol. The patient should be instructed to contact their physician immediately if there is deterioration of their asthma [see Warnings and Precautions ( 5.2)] .
Immunosuppression and Risk of Infections
Patients who are on immunosuppressant doses of corticosteroids should be warned to avoid exposure to chickenpox or measles and, if exposed, to consult their physician without delay. Patients should be informed of potential worsening of existing tuberculosis, fungal, bacterial, viral, or parasitic infections, or ocular herpes simplex [see Warnings and Precautions ( 5.3)] .
Hypercorticism and Adrenal Suppression
Patients should be advised that ALVESCO may cause systemic corticosteroid effects of hypercorticism and adrenal suppression. Additionally, patients should be instructed that deaths due to adrenal insufficiency have occurred during and after transfer from systemic corticosteroids. Patients should taper slowly from systemic corticosteroids if transferring to ALVESCO [see Warnings and Precautions ( 5.5)] .
Reduction in Bone Mineral Density
Patients who are at an increased risk for decreased BMD should be advised that the use of corticosteroids may pose an additional risk and should be monitored and where appropriate, be treated for this condition [see Warnings and Precautions ( 5.6)] .
Effect on Growth
Patients should be informed that orally inhaled corticosteroids, including ALVESCO, may cause a reduction in growth velocity when administered to pediatric patients. Physicians should closely follow the growth of pediatric patients taking corticosteroids by any route [see Warnings and Precautions ( 5.7)] .
Use Daily for Best Effect
Patients should be advised to use ALVESCO at regular intervals, since its effectiveness depends on regular use. Maximum benefit may not be achieved for four weeks or longer after starting treatment. The patient should not increase the prescribed dosage but should contact their physician if symptoms do not improve or if the condition worsens. Patients should be instructed not to stop ALVESCO use abruptly. Patients should contact their physician immediately if use of ALVESCO is discontinued.
How to Use ALVESCO
Patients should use ALVESCO only with the actuator supplied with the product. When the dose indicator display window shows a red zone, approximately 20 inhalations are left, and a refill is required. Discard the inhaler when the indicator shows zero.
Manufactured for:
Covis Pharma
Zug, 6300 Switzerland
Made in United Kingdom
Patient Information
ALVESCO
®[ael-‘ves-ko℧]
(ciclesonide)
Note: For Oral Inhalation Only
Do notuse your ALVESCO near heat or an open flame.
Read this Patient Information leaflet before you start using ALVESCO and each time you get a refill. There may be new information. This information does not take the place of talking with your healthcare provider about your medical condition or your treatment. If you have any questions about ALVESCO, ask your healthcare provider or pharmacist.
What is ALVESCO?
ALVESCO is a prescription medicine used for the control and prevention of asthma in adults and children 12 years of age and older.
ALVESCO contains ciclesonide, which is a man-made (synthetic) corticosteroid. Corticosteroids are natural substances found in the body and reduce inflammation. When you inhale ALVESCO it may help to control and prevent your symptoms of asthma by reducing your airway inflammation.
ALVESCO is not for the relief of acute bronchospasm. ALVESCO is not a bronchodilator and does not treat sudden symptoms of an asthma attack such as wheezing, cough, shortness of breath, and chest pain or tightness. Always have a fast-acting bronchodilator medicine (rescue inhaler) with you to treat sudden symptoms.
It is not known if ALVESCO is safe and effective in children 11 years of age and younger.
Who should not use ALVESCO?
Do not use ALVESCO:
- to treat status asthmaticus or other sudden symptoms of asthma. ALVESCO is not a rescue inhaler and should not be used to give you fast relief from your asthma attack. Always use a rescue inhaler such as albuterol, during a sudden asthma attack.
- if you are allergic to ciclesonide or any of the ingredients in ALVESCO. See the end of this Patient Information leaflet for a complete list of ingredients in ALVESCO.
What should I tell my healthcare provider before using ALVESCO?
Before you use ALVESCO tell your healthcare provider if you:
- have or have had eye problems such as increased ocular pressure, glaucoma, or cataracts.
- have any infections including tuberculosis or ocular herpes simplex.
- have not had or been vaccinated for chicken pox or measles.
- are pregnant or plan to become pregnant. It is not known if ALVESCO will harm your unborn baby. Talk to your healthcare provider if you are pregnant or plan to become pregnant.
- are breastfeeding or plan to breastfeed. It is not known if ALVESCO passes into your breast milk. Talk to your healthcare provider about the best way to feed your baby if you are using ALVESCO.
Tell your healthcare provider about all the medicines you take, including prescription and non-prescription medicines, vitamins and herbal supplements.
Know the medicines you take. Keep a list of them to show your healthcare provider and pharmacist when you get a new medicine.
How should I use ALVESCO?
- Read the Instructions for Use at the end of this leaflet for specific information about the right way to use ALVESCO.
- Use ALVESCO exactly as your healthcare provider tells you to use it. Do not take more of your medicine, or take it more often than your healthcare provider tells you.
- You must use ALVESCO regularly. It may take 4 weeks or longer after you start using ALVESCO for your asthma symptoms to get better. Do not stop using ALVESCO even if you are feeling better, unless your healthcare provider tells you to.
- If your symptoms do not improve or get worse, call your healthcare provider.
- Your healthcare provider may prescribe a rescue inhaler for emergency relief of sudden asthma attacks. Call your healthcare provider if you have:
- an asthma attack that does not respond to your rescue inhaler or
- you need more of your rescue inhaler than usual.
- If you use another inhaled medicine, ask your healthcare provider for instructions on how to use it while you use ALVESCO.
What are the possible side effects of ALVESCO?
ALVESCO may cause serious side effects, including:
- Thrush (Candida), a fungal infection of your nose, mouth, or throat.Tell your healthcare provider if you have discomfort or pain in your throat, have hoarseness in your voice or have any redness or white colored patches in your mouth or throat. Rinse your mouth after you use your ALVESCO.
-
Immune system problems that may increase your risk of infections.You are more likely to get infections if you take medicines that may weaken your body’s ability to fight infections. Avoid contact with people who have contagious diseases such as chicken pox or measles while you use ALVESCO. Symptoms of an infection may include:
- fever
- pain
- aches
- chills
- feeling tired
- nausea
- vomiting
-
Adrenal insufficiency.Adrenal insufficiency is a condition in which the adrenal glands do not make enough steroid hormones. Your healthcare provider will follow you closely if you take steroids by mouth and are having them decreased (tapered) or you are being switched to ALVESCO. People have died while steroids are being decreased and when people have been switched from steroids by mouth to inhaled steroids like ALVESCO. If you are under stress, such as with surgery, after surgery or trauma, you may need steroids by mouth again.
Call your healthcare provider right away if you have the following symptoms of adrenal insufficiency:- tiredness
- weakness
- dizziness
- nausea that does not go away
- vomiting that does not go away
- Decreased bone mass (bone mineral density).People who use inhaled steroid medicines for a long time may have an increased risk of decreased bone mass which can affect bone strength. Talk to your healthcare provider about any concerns you may have about bone health.
- Slowed or delayed growth in children.A child’s growth should be checked regularly while using ALVESCO.
- Eye problems such as glaucoma and cataracts.If you have a history of glaucoma or cataracts or have a family history of eye problems, you should have regular eye exams while you use ALVESCO.
-
Increased wheezing (bronchospasm)can happen right away after using ALVESCO.
Stop using ALVESCO and use an inhaled fast-acting bronchodilator (rescue inhaler) right away.
Tell your healthcare provider right away so that a new medicine can be prescribed to control your asthma.
The most common side effects with ALVESCO include: - headache
- swelling of nose and throat (nasopharyngitis)
- swelling of the sinuses (sinusitis)
- throat pain
- upper respiratory infection
- joint pain (arthralgia)
- nasal congestion
- pain in arms, legs, and back
Tell your healthcare provider about any side effect that bothers you or that does not go away. These are not all of the possible side effects with ALVESCO. For more information, ask your healthcare provider or pharmacist.
Call your healthcare provider for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
How should I store ALVESCO?
- Store ALVESCO at room temperature between 59°F to 86°F (15°C to 30°C)
- Do notpuncture the ALVESCO canister
- Do notstore the ALVESCO canister near heat or a flame. Temperatures above 120°F (49°C) may cause the canister to burst.
- Do notthrow the ALVESCO canister into a fire or an incinerator.
- Safely throw away medicine that is out of date or no longer needed.
- Keep ALVESCO Aerosol and dry at all times.
Keep ALVESCO and all medicines out of reach of children.
General Information About the Safe and Effective use of ALVESCO
Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. Do not use ALVESCO for a condition for which it is not prescribed. Do not give ALVESCO to other people, even if they have the same symptoms that you have. It may harm them.
This Patient Information summarizes the most important information about ALVESCO. If you would like more information, talk with your healthcare provider. You can ask your pharmacist or healthcare provider for information about ALVESCO that is written for health professionals.
For more information, go to www.alvesco.us/.
What are the ingredients in ALVESCO?
Active ingredient:ciclesonide
Inactive ingredients:propellant HFA-134a and ethanol
Instructions for Use
ALVESCO
®[ael-‘ves- ko℧]
(ciclesonide)
Read this Instructions for Use for ALVESCO before you start using it and each time you get a refill. There may be new information. This leaflet does not take the place of talking to your healthcare provider about your medical condition or treatment.
Note: For Oral Inhalation Only
Do notuse your ALVESCO near heat or an open flame.
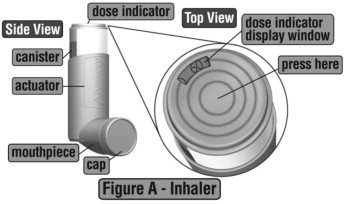
The parts of your ALVESCO
ALVESCO comes as a canister that fits into an actuator with a dose indicator. Do notuse the actuator with a canister of medicine from any other inhaler. Do notuse ALVESCO canister with an actuator from any other inhaler. (See Figure A)
Priming your ALVESCO for use
- Remove your ALVESCO from its package.
- Before you use ALVESCO for the first timeor if you have not used your medicine for 10 days in a row, you will need to prime your ALVESCO unit.
- Remove the plastic cap. Look at the dose indicator on top of the inhaler. Make sure that the dose indicator display window pointer is before the “60” inhalation mark before you use your ALVESCO for the first time.
- Hold the actuator upright. Spray 3 times into the air away from the face, by pressing down fully onto the center of the dose indicator button. (See Figure B)
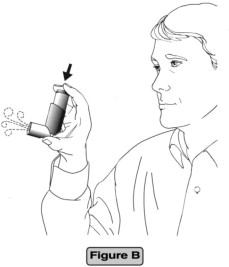
- Check the dose indicator display window after the priming sprays and before the first use to make sure it shows that there are 60 sprays left in your ALVESCO unit. If there are not 60 sprays left in your ALVESCO after the first use priming spray, return it to the pharmacy.
- Make sure the canister is firmly placed in the mouthpiece each time you use your ALVESCO.
- You do not need to shake your ALVESCO unit before you use it.
Using Your ALVESCO
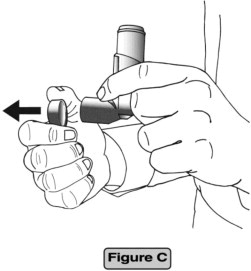
Step 1.Remove the cap from the mouthpiece. (See Figure C)
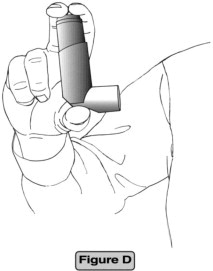
Step 2.Hold the actuator upright, between your thumb, forefinger, and middle finger with the mouthpiece pointing towards you. (See Figure D)
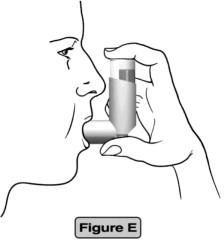
Step 3.Breathe out as fully as you comfortably can. Close your lips around the mouthpiece, keeping your tongue below it. (See Figure E)
Step 4.
- While breathing in deeply and slowly, press down on the center of the dose indicator with your finger. Press down fully on the canister until it stops moving in the actuator while delivering your dose.
- When you have finished breathing in, hold your breath for about 10 seconds, or for as long as is comfortable.
- Note: It is normal to hear a soft click from the indicator as it counts down during use.
Step 5.
Take your finger completely off the center of the dose indicator and remove the inhaler from your mouth. Breathe out gently. (See Figure F)

Step 6.Replace the cap to keep the mouthpiece clean.
Step 7.Rinse your mouth with water and spit it out. Do notswallow.
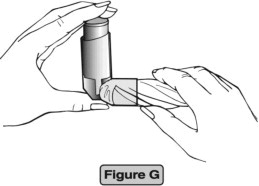
Cleaning your ALVESCO unit
- Clean the mouthpiece weekly with a clean dry tissue, both inside and out. (See Figure G)
- Wipe over the front of the small hole where the medicine comes out with a dry, folded tissue. (See Figure H)
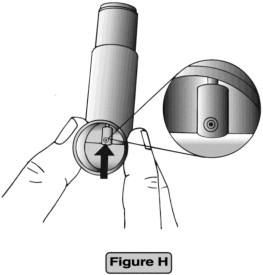
- Do not wash or put any part of your ALVESCO unit in water or any other liquids.
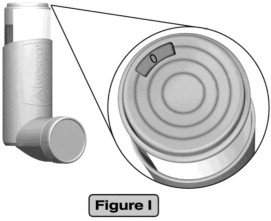
How to tell if your ALVESCO canister is empty
- Your ALVESCO unit is fitted with a dose indicator display which shows you how much of your medicine is left after each use.
- Each canister of ALVESCO contains enough medicine for you to spray your medicine 60 times. This does not count the first sprays used for priming.
- The dose indicator display counts down by 10 and will move every tenth time you take a puff (i.e., 60-50-40, etc.).
- The dose indicator display window will turn red when there are only 20 sprays left. This means that you need to replace your inhaler soon.
- When the dose indicator display window reads “0” you should throw away your ALVESCO unit. (See Figure I)
- Although your ALVESCO unit is fitted with a dose indicator display to help determine the number of sprays left, you should keep track of the number of sprays used from each canister of your ALVESCO unit.
This PPI and Instructions for Use has been approved by the U.S. Food and Drug Administration.
Manufactured for:
Covis Pharma
Zug, 6300 Switzerland
Made in United Kingdom
ALVESCO is a registered trademark of Covis Pharma.
©2023 Covis Pharma. All rights reserved.
PRINCIPAL DISPLAY PANEL - 80 mcg Carton
NDC: 70515-711-01 Net Contents: 6.1 g
Alvesco
®
ciclesonide
Inhalation Aerosol
80 mcg/actuation
60 Metered Actuations
FOR ORAL INHALATION WITH ALVESCO
®
INHALATION AEROSOL ACTUATOR ONLY
Rx Only
COVIS
Alvesco
®
ciclesonide
Inhalation Aerosol
80 mcg/actuation
GTIN: 00370515711013
S/N: XXXXXXXXXXXXXX
EXP: MM/YYYY
LOT: YYXXXX
Pharmacist:Dispense
with
Patient’s Instructions
for Use
from package
insert inside.
WARNING:Keep out of
reach of children. Avoid
spraying in eyes.
COVIS
Manufactured for:
Covis Pharma
Zug, 6300 Switzerland
Made in the United Kingdom
Each 6.1 g canister of
ALVESCO
®Inhalation
Aerosol contains a solution
of ciclesonide in propellant
HFA-134a (1,1,1,2
tetrafluoroethane) and
ethanol. The 80 mcg
strength of ALVESCO
®
Inhalation Aerosol delivers
100 mcg from the valve
and 80 mcg of ciclesonide
from the actuator.
Dosage and
Administration:
See package insert for
dosage information.
CONTENTS UNDER
PRESSURE.
Do not
puncture.
Do not use or store near
heat or open flame.
Exposure to temperatures
above 49°C (120°F) may
cause bursting. Never
throw canister into fire or
incinerator.
Store at 25°C (77°F);
excursions between
15–30°C (59–86°F) are
permitted [see USP]. For
optimal results, canister
should be at room
temperature when used.
PRINCIPAL DISPLAY PANEL - 160 mcg Carton
NDC: 70515-712-01 Net Contents: 6.1 g
Alvesco
®
ciclesonide
Inhalation Aerosol
160 mcg/actuation
60 Metered Actuations
FOR ORAL INHALATION WITH ALVESCO
®
INHALATION AEROSOL ACTUATOR ONLY
Rx Only
COVIS
Alvesco
®
ciclesonide
Inhalation Aerosol
160 mcg/actuation
GTIN: 00370515712010
S/N: XXXXXXXXXXXXXX
EXP: MM/YYYY
LOT: YYXXXX
Pharmacist:Dispense
with
Patient’s Instructions
for Use
from package
insert inside.
WARNING:Keep out of
reach of children. Avoid
spraying in eyes.
COVIS
Manufactured for:
Covis Pharma
Zug, 6300 Switzerland
Made in the United Kingdom
Each 6.1 g canister of
ALVESCO
®Inhalation
Aerosol contains a solution
of ciclesonide in propellant
HFA-134a (1,1,1,2
tetrafluoroethane) and
ethanol. The 160 mcg
strength of ALVESCO
®
Inhalation Aerosol delivers
200 mcg from the valve
and 160 mcg of ciclesonide
from the actuator.
Dosage and
Administration:
See package insert for
dosage information.
CONTENTS UNDER
PRESSURE.
Do not
puncture.
Do not use or store near
heat or open flame.
Exposure to temperatures
above 49°C (120°F) may
cause bursting. Never
throw canister into fire or
incinerator.
Store at 25°C (77°F);
excursions between
15–30°C (59–86°F) are
permitted [see USP]. For
optimal results, canister
should be at room
temperature when used.
| ALVESCO
ciclesonide aerosol, metered |
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
| ALVESCO
ciclesonide aerosol, metered |
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
| Labeler - Praxis, LLC (016329513) |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Praxis, LLC | 016329513 | manufacture(59368-409, 59368-408) , label(59368-408, 59368-409) , pack(59368-408, 59368-409) | |
Trademark Results [Alvesco]
Mark Image Registration | Serial | Company Trademark Application Date |
|---|---|
 ALVESCO 78883333 3607727 Live/Registered |
ALTANA Pharma AG 2006-05-15 |
 ALVESCO 78883320 3610461 Live/Registered |
ALTANA Pharma AG 2006-05-15 |
 ALVESCO 78621671 3212310 Dead/Cancelled |
NYCOMED GMBH 2005-05-03 |
 ALVESCO 78282980 2860362 Live/Registered |
COVIS PHARMA B.V. 2003-08-04 |
 ALVESCO 78056893 not registered Dead/Abandoned |
ALTANA PHARMA AG 2001-04-05 |
 ALVESCO 77074621 3573087 Live/Registered |
ALTANA PHARMA AG 2007-01-02 |
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.