ERZOFRI EXTENDED-RELEASE- paliperidone palmitate injection
Erzofri extended-release by
Drug Labeling and Warnings
Erzofri extended-release by is a Prescription medication manufactured, distributed, or labeled by Shandong Luye Pharmaceutical Co., Ltd., Interquim, S.A., Curia Spain, S.A.U.. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use ERZOFRI ®safely and effectively. See full prescribing information for ERZOFRI ®.
ERZOFRI ®(paliperidone palmitate) extended-release injectable suspension, for intramuscular use
Initial U.S. Approval: 2006WARNING: INCREASED MORTALITY IN ELDERLY PATIENTS WITH DEMENTIA-RELATED PSYCHOSIS
See full prescribing information for complete boxed warning.
Elderly patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk of death. ERZOFRI is not approved for use in patients with dementia-related psychosis. ( 5.1)
RECENT MAJOR CHANGES
Warnings and Precautions ( 5.10) 1/2025 INDICATIONS AND USAGE
DOSAGE AND ADMINISTRATION
- For patients naïve to oral or injectable paliperidone, or oral or injectable risperidone, establish tolerability with oral paliperidone or oral risperidone prior to initiating treatment with ERZOFRI. ( 2.1)
- Each injection must be administered by a healthcare professional. ( 2.1)
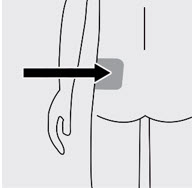
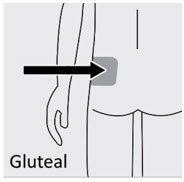
- Initiate ERZOFRI by intramuscular injection in the deltoid muscle. Following the initial dose, monthly doses can be administered in either the gluteal or deltoid muscle. Do not administer by any other route. ( 2.1)
- Dosage recommendations:
Indication Initial Dose
(deltoid)
Day 1Monthly Dosage *(deltoid or gluteal) Maximum Monthly Dosage - * Administered 4 weeks after the first injection.
- † Recommended monthly dosage for treatment of schizophrenia is 117 mg. Some patients may benefit from lower or higher monthly doses within the additional available strengths (39 mg, 78 mg, 156 mg, and 234 mg).
- ‡ Adjust dose based on tolerability and/or efficacy using available strengths. The 39 mg strength was not studied in the long-term schizoaffective disorder study.
Schizophrenia ( 2.1) 351 mg 39 mg to 234 mg † 234 mg Schizoaffective disorder ( 2.1) 351 mg 78 mg to 234 mg ‡ 234 mg - Missed dose: Refer to the Full Prescribing Information. ( 2.2)
- Mild renal impairment: Administer 234 mg on treatment Day 1 in the deltoid muscle. Follow with the recommended monthly maintenance dose of 78 mg, administered in the deltoid or gluteal muscle. Adjust monthly maintenance dose based on tolerability and/or efficacy within the strengths of 39 mg, 78 mg, 117 mg, or 156 mg. The maximum monthly dosage is 156 mg for patients with mild renal impairment. ( 2.4)
- See Full Prescribing Information for important preparation and administration information. ( 2.7)
DOSAGE FORMS AND STRENGTHS
Extended-release injectable suspension: 39 mg/0.25 mL, 78 mg/0.5 mL, 117 mg/0.75 mL, 156 mg/mL, 234 mg/1.5 mL, 351 mg/2.25 mL. ( 3)
CONTRAINDICATIONS
Known hypersensitivity to paliperidone, risperidone, or to any excipients in ERZOFRI. ( 4)
WARNINGS AND PRECAUTIONS
- Cerebrovascular Adverse Reactions, in Elderly Patients with Dementia-Related Psychosis:Increased incidence of cerebrovascular adverse reactions (e.g., stroke, transient ischemic attack, including fatalities). ( 5.2)
- Neuroleptic Malignant Syndrome:Manage with immediate discontinuation of drug and close monitoring. ( 5.3)
- QT Prolongation:Avoid use with drugs that also increase QT interval and in patients with risk factors for prolonged QT interval. ( 5.4)
- Tardive Dyskinesia:Discontinue drug if clinically appropriate. ( 5.5)
- Metabolic Changes:Monitor for hyperglycemia/diabetes mellitus, dyslipidemia, and weight gain. ( 5.6)
- Orthostatic Hypotension and Syncope:Use with caution in patients with known cardiovascular or cerebrovascular disease and patients predisposed to hypotension. ( 5.7)
- Leukopenia, Neutropenia, and Agranulocytosis:Perform complete blood counts (CBC) in patients with history of clinically significant low white blood cell count (WBC) or history of leukopenia or neutropenia. Consider discontinuing ERZOFRI if clinically significant decline in WBC in the absence of other causative factors. ( 5.9)
- Hyperprolactinemia:Prolactin elevations occur and persist during chronic administration. ( 5.10)
- Potential for Cognitive and Motor Impairment:Use caution when operating machinery. ( 5.11)
- Seizures:Use cautiously in patients with a history of seizures or with conditions that lower the seizure threshold. ( 5.12)
ADVERSE REACTIONS
The most common adverse reactions (incidence ≥ 5% and occurring at least twice as often as placebo) were injection site reactions, somnolence/sedation, dizziness, akathisia, and extrapyramidal disorder. ( 6)
To report SUSPECTED ADVERSE REACTIONS, contact Luye Innomind Pharma Shijiazhuang Co., Ltd. at 1-800-548-9765 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
- Drugs that may cause orthostatic hypotension:An additive effect may occur when co-administered with ERZOFRI. ( 7.1)
- Strong CYP3A4 and P-glycoprotein (P-gp) inducers: Avoid using a strong inducer of CYP3A4 and/or P-gp during a dosing interval for ERZOFRI. If concomitant use is necessary, consider using paliperidone extended-release tablets. ( 2.5, 7.1, 12.3)
USE IN SPECIFIC POPULATIONS
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.
Revised: 3/2025
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
WARNING: INCREASED MORTALITY IN ELDERLY PATIENTS WITH DEMENTIA- RELATED PSYCHOSIS
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dosage
2.2 Missed Doses
2.3 Use with Risperidone or with Oral Paliperidone
2.4 Dosage Recommendations for Patients with Renal Impairment
2.5 Dosage Modifications for Concomitant Use with Strong CYP3A4 Inducers and/or P-gp Inducers
2.6 Switching from Other Antipsychotics
2.7 Preparation and Administration Instructions
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Increased Mortality in Elderly Patients with Dementia-Related Psychosis
5.2 Cerebrovascular Adverse Reactions, Including Stroke, in Elderly Patients with Dementia-Related Psychosis
5.3 Neuroleptic Malignant Syndrome
5.4 QT Prolongation
5.5 Tardive Dyskinesia
5.6 Metabolic Changes
5.7 Orthostatic Hypotension and Syncope
5.8 Falls
5.9 Leukopenia, Neutropenia, and Agranulocytosis
5.10 Hyperprolactinemia
5.11 Potential for Cognitive and Motor Impairment
5.12 Seizures
5.13 Dysphagia
5.14 Priapism
5.15 Disruption of Body Temperature Regulation
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
6.2 Postmarketing Experience
7 DRUG INTERACTIONS
7.1 Drugs Having Clinically Important Interactions with ERZOFRI
7.2 Drugs Having No Clinically Important Interactions with ERZOFRI
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.3 Females and Males of Reproductive Potential
8.4 Pediatric Use
8.5 Geriatric Use
8.6 Renal Impairment
8.7 Hepatic Impairment
8.8 Patients with Parkinson's Disease or Lewy Body Dementia
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
14.1 Schizophrenia
14.2 Schizoaffective Disorder
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- * Sections or subsections omitted from the full prescribing information are not listed.
-
BOXED WARNING
(What is this?)
WARNING: INCREASED MORTALITY IN ELDERLY PATIENTS WITH DEMENTIA- RELATED PSYCHOSIS
Elderly patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk of death. ERZOFRI is not approved for use in patients with dementia-related psychosis.[see Warnings and Precautions (5.1)] .
- 1 INDICATIONS AND USAGE
-
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dosage
For patients who have never taken oral or injectable paliperidone, or oral or injectable risperidone, establish tolerability with oral paliperidone or oral risperidone prior to initiating treatment with ERZOFRI.
ERZOFRI must be administered by a healthcare professional as an intramuscular injection. Do not administer ERZOFRI by any other route. For detailed preparation and administration instructions, see Dosage and Administration (2.7).
See Table 1for dosage recommendations for ERZOFRI in the treatment of schizophrenia in adults or the treatment of schizoaffective disorder in adults as monotherapy and as an adjunct to mood stabilizers or antidepressants.
The initial dosage of ERZOFRI is 351 mg on treatment Day 1 administered in the deltoid muscle. Following the initial dose, monthly doses can be administered in either the deltoid or gluteal muscle [see Clinical Pharmacology (12.3)] .
Table 1: Dosage Recommendations for ERZOFRI Indication Initial Dose
(deltoid)
Day 1Monthly Dosage *
(deltoid or gluteal)Maximum Monthly Dosage - * Administered 4 weeks after the first injection.
- † The recommended monthly dosage for treatment of schizophrenia is 117 mg. Some patients may benefit from lower or higher monthly doses within the additional available strengths (39 mg, 78 mg, 156 mg, and 234 mg).
- ‡ Adjust dose based on tolerability and/or efficacy using available strengths. The 39 mg strength was not studied in the long-term schizoaffective disorder study.
Schizophrenia 351 mg 39 mg to 234 mg † 234 mg Schizoaffective disorder 351 mg 78 mg to 234 mg ‡ 234 mg Adjust dosage monthly depending on clinical response and tolerability. When making dose adjustments, the pharmacokinetic profile of ERZOFRI should be considered [see Clinical Pharmacology (12.3)] , as the full effect of the dose adjustment may not be apparent for several months.
2.2 Missed Doses
Dosing Window
To avoid a missed monthly dose, patients may be given the injection up to 7 days before or after the monthly time point.
Missed Dose
If a dose of ERZOFRI is missed, follow the dosing instructions provided in Table 2.
Table 2: Management of a Missed Dose of ERZOFRI TIMING OF MISSED DOSE DOSING 4 to 6 weeks since last injection Resume regular monthly dosing as soon as possible at the patient's previously stabilized dose, followed by injections at monthly intervals. More than 6 weeks to 6 months since last injection Resume the same dose the patient was previously stabilized on (unless the patient was stabilized on a dose of 234 mg, then the first 2 injections should each be 156 mg) in the following manner: - Administer a deltoid injection as soon as possible.
- Administer a second deltoid injection 1 week later at the same dose.
- Thereafter, resume administering the previously stabilized dose in the deltoid or gluteal muscle 1 month after the second injection.
More than 6 months since last injection Restart dosing with recommended initiation( see Section 2.1, Table 1) : - Administer a 351 mg deltoid injection on Day 1.
- Thereafter, resume administering the previously stabilized dose in the deltoid or gluteal muscle 1 month after the initial injection.
2.3 Use with Risperidone or with Oral Paliperidone
Paliperidone is the major active metabolite of risperidone. Exercise caution if ERZOFRI is co-administered with risperidone or with oral paliperidone for extended periods of time. Safety data involving concomitant use of ERZOFRI with other antipsychotics is limited.
2.4 Dosage Recommendations for Patients with Renal Impairment
For patients with mild renal impairment (creatinine clearance ≥ 50 mL/min to < 80 mL/min [Cockcroft-Gault Formula]), initiate ERZOFRI with a dose of 234 mg on treatment Day 1 in the deltoid muscle. Follow with the recommended monthly dosage of 78 mg, administered in either the deltoid or gluteal muscle. Adjust monthly dosage based on tolerability and/or response within the strengths of 39 mg, 78 mg, 117 mg, or 156 mg. The maximum monthly dosage is 156 mg for patients with mild renal impairment [see Use in Specific Populations (8.6)and Clinical Pharmacology (12.3)] .
ERZOFRI is not recommended in patients with moderate or severe renal impairment (creatinine clearance < 50 mL/min) [see Use in Specific Populations (8.6)and Clinical Pharmacology (12.3)].
2.5 Dosage Modifications for Concomitant Use with Strong CYP3A4 Inducers and/or P-gp Inducers
Avoid using a strong inducer of CYP3A4 and/or P-gp during the one-month dosing interval for ERZOFRI, if possible. If administering a strong inducer is necessary, consider managing the patient using paliperidone extended-release tablets [see Drug Interactions (7.1)and Clinical Pharmacology (12.3)] .
2.6 Switching from Other Antipsychotics
There are no systematically collected data to specifically address switching patients with schizophrenia or schizoaffective disorder from other antipsychotics to ERZOFRI or concerning concomitant administration with other antipsychotics.
Switching from Oral Antipsychotics
Previous oral antipsychotics can be gradually discontinued at the time of initiation of treatment with ERZOFRI. The recommended initial dosage of ERZOFRI is 351 mg on treatment Day 1, administered in the deltoid muscle [see Dosage and Administration (2.1)] . See Table 3for subsequent monthly dosage recommendations for ERZOFRI in patients switching from oral extended-release paliperidone tablets.
Table 3: Dosage Recommendations Following Initial Dose of ERZOFRI in Patients Switching from Oral Extended-Release Paliperidone Tablets Paliperidone Extended-Release Tablet ERZOFRI Dosing Frequency Once Daily Once every 4 weeks 12 mg 234 mg Dose 9 mg 156 mg 6 mg 117 mg 3 mg 39 mg to 78 mg Switching from Long-Acting Injectable Antipsychotics
When switching patients currently at steady-state on a long-acting injectable antipsychotic, initiate ERZOFRI therapy in place of the next scheduled injection.
Continue ERZOFRI at monthly intervals. The initial dosing regimen as described in Section 2.1 is not required. See Table 1for recommended monthly dosing. Based on previous clinical response and tolerability, some patients may benefit from lower or higher doses within the available strengths (39 mg, 78 mg, 117 mg, 156 mg, and 234 mg).
If ERZOFRI is discontinued, its pharmacokinetic characteristics must be considered. As recommended with other antipsychotic medications, the need for continuing existing extrapyramidal symptoms (EPS) medication should be re-evaluated periodically.
2.7 Preparation and Administration Instructions
- To be prepared and administered by a healthcare professional only.
- Read the instructions for preparation and administration below for preparation and administration considerations.
- For deltoid or gluteal intramuscular injection only. Do not inject by any other route.
- Administer the initial dosage of ERZOFRI in the deltoid muscle. Subsequent monthly dosages may be administered in the deltoid or gluteal muscle.
- As a universal precaution, always wear gloves.
- Do not substitute any component of the drug kit.
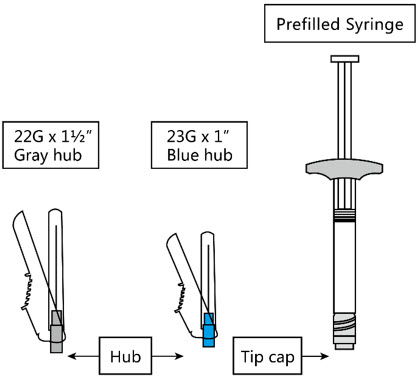
The kit contains a prefilled syringe and 2 safety needles (a 1 ½-inch 22 gauge needle and a 1-inch 23 gauge needle).
ERZOFRI is for single use only.
Step 1. Select Needle
For Deltoid injection For Gluteal injection 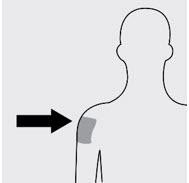
If the patient weighs less than 90 kg, use the 1-inch 23gauge needle (needle with bluecolored hub) Use the 1 ½-inch 22gauge needle (needle with graycolored hub) regardless of patient's weight If the patient weighs 90 kg or more, use the 1 ½-inch 22gauge needle (needle with graycolored hub) Step 2. Prepare for Injection
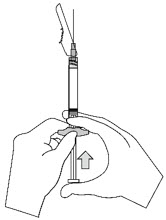
a. Open needle pouch b. Shake vigorously for at least 10 seconds c. Remove cap 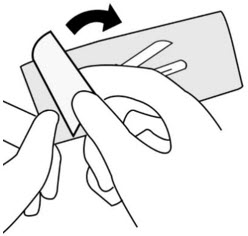
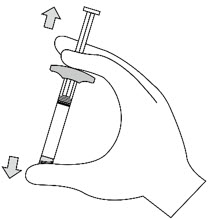
First, peel the safety needle pouch half way open. Place on a clean surface. Shake the syringe vigorously for a minimum of 10 seconds to ensure a homogeneous suspension. While holding the syringe upright, remove the rubber tip cap with an easy counterclockwise twisting motion. Do not touch syringe tip. d. Attach needle e. Remove needle sheath f. Remove air bubbles 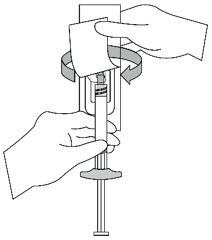
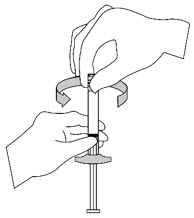
Grasp the needle sheath using the plastic peel pouch. Attach the safety needle to the luer connection of the syringe with an easy clockwise twisting motion.
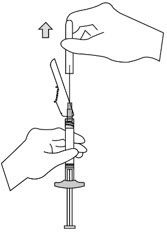
Do notremove the pouch until the syringe and needle are securely attached.Pull the needle sheath away from the needle with a straight pull. Do not twist the sheath as the needle may be loosened from the syringe. Bring the syringe with the attached needle in upright position to de-aerate. De-aerate the syringe by moving the plunger rod carefully forward. Step 3. Inject
Inject the entire contents intramuscularly slowly, deep into the selected deltoid or gluteal muscle of the patient. Do not administer by any other route. 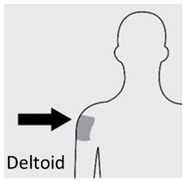
Step 4. After Injection
Secure Needle Dispose properly a 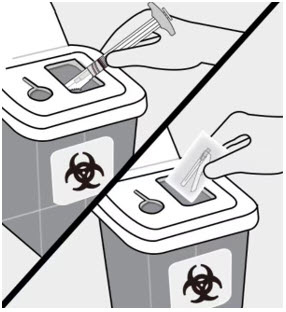
Dispose of the syringe and unused needle in an approved sharps container.
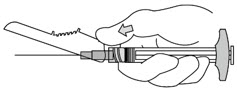
b 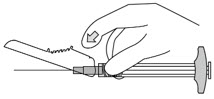
c 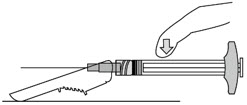
After the injection is complete, use either thumb or finger of one hand (a, b) or a flat surface (c) to activate the needle protection system. The needle protection system is fully activated when a 'click' is heard. -
3 DOSAGE FORMS AND STRENGTHS
Extended-release injectable suspension: white to off-white aqueous suspension available in dose strengths of 39 mg/0.25 mL, 78 mg/0.5 mL, 117 mg/0.75 mL, 156 mg/mL, 234 mg/1.5 mL, and 351 mg/2.25 mL paliperidone palmitate.
Each strength is provided as a kit, which includes: one single-dose prefilled syringe and 2 safety needles (a 1 ½-inch 22 gauge needle and a 1-inch 23 gauge needle).
-
4 CONTRAINDICATIONS
ERZOFRI is contraindicated in patients with a known hypersensitivity to either paliperidone or risperidone, or to any of the excipients in the ERZOFRI formulation. Hypersensitivity reactions, including anaphylactic reactions and angioedema, have been reported in patients treated with risperidone and in patients treated with paliperidone [see Adverse Reactions (6.1, 6.2)] .
-
5 WARNINGS AND PRECAUTIONS
5.1 Increased Mortality in Elderly Patients with Dementia-Related Psychosis
Elderly patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk of death. Analyses of 17 placebo-controlled trials (modal duration of 10 weeks), largely in patients taking atypical antipsychotic drugs, revealed a risk of death in drug-treated patients of between 1.6 to 1.7 times the risk of death in placebo-treated patients. Over the course of a typical 10-week controlled trial, the rate of death in drug-treated patients was about 4.5%, compared to a rate of about 2.6% in the placebo group.
Although the causes of death were varied, most of the deaths appeared to be either cardiovascular (e.g., heart failure, sudden death) or infectious (e.g., pneumonia) in nature. Observational studies suggest that, similar to atypical antipsychotic drugs, treatment with conventional antipsychotic drugs may increase mortality. The extent to which the findings of increased mortality in observational studies may be attributed to the antipsychotic drug as opposed to some characteristic(s) of the patients is not clear.
ERZOFRI is not approved for the treatment of patients with dementia-related psychosis [see Boxed Warningand Warnings and Precautions (5.2)] .
5.2 Cerebrovascular Adverse Reactions, Including Stroke, in Elderly Patients with Dementia-Related Psychosis
In placebo-controlled trials with risperidone, aripiprazole, and olanzapine in elderly subjects with dementia, there was a higher incidence of cerebrovascular adverse reactions (cerebrovascular accidents and transient ischemic attacks) including fatalities compared to placebo-treated subjects. No studies have been conducted with oral paliperidone, 1-month or 3-month paliperidone palmitate extended-release injectable suspensions, or ERZOFRI, in elderly patients with dementia. ERZOFRI is not approved for the treatment of patients with dementia-related psychosis [see Boxed Warningand Warnings and Precautions (5.1)] .
5.3 Neuroleptic Malignant Syndrome
Neuroleptic Malignant Syndrome (NMS), a potentially fatal symptom complex, has been reported in association with antipsychotic drugs, including paliperidone.
Clinical manifestations of NMS are hyperpyrexia, muscle rigidity, altered mental status including delirium, and autonomic instability (irregular pulse or blood pressure, tachycardia, diaphoresis, and cardiac dysrhythmia). Additional signs may include elevated creatine phosphokinase, myoglobinuria (rhabdomyolysis), and acute renal failure.
If NMS is suspected, immediately discontinue ERZOFRI and provide symptomatic treatment and monitoring.
5.4 QT Prolongation
Paliperidone causes a modest increase in the corrected QT (QTc) interval. The use of paliperidone should be avoided in combination with other drugs that are known to prolong QTc including Class 1A (e.g., quinidine, procainamide) or Class III (e.g., amiodarone, sotalol) antiarrhythmic medications, antipsychotic medications (e.g., chlorpromazine, thioridazine), antibiotics (e.g., gatifloxacin, moxifloxacin), or any other class of medications known to prolong the QTc interval. Paliperidone should also be avoided in patients with congenital long QT syndrome and in patients with a history of cardiac arrhythmias.
Certain circumstances may increase the risk of the occurrence of Torsades de pointes and/or sudden death in association with the use of drugs that prolong the QTc interval, including (1) bradycardia; (2) hypokalemia or hypomagnesemia; (3) concomitant use of other drugs that prolong the QTc interval; and (4) presence of congenital prolongation of the QT interval.
The effects of oral paliperidone on the QT interval were evaluated in a double-blind, active-controlled (moxifloxacin 400 mg single dose), multicenter QT study in adults with schizophrenia and schizoaffective disorder, and in three placebo- and active-controlled 6-week, fixed-dose efficacy trials in adults with schizophrenia.
In the QT study (n=141) of oral paliperidone, the 8 mg dose of immediate-release oral paliperidone (n=50) showed a mean placebo-subtracted increase from baseline in QTcLD (QT interval corrected for heart rate using the population specified linear derived method) of 12.3 msec (90% CI: 8.9; 15.6) on Day 8 at 1.5 hours post-dose. The mean steady-state peak plasma concentration for this 8 mg oral dose of immediate release paliperidone (C max ss= 113 ng/mL) was more than 2-fold the exposure observed with the maximum recommended 234 mg maintenance dose of another once-a-month paliperidone extended-release injectable suspension administered in the deltoid muscle (predicted median C max-ss= 50 ng/mL). In this same study, a 4 mg dose of the immediate-release oral formulation of paliperidone, for which C max-ss= 35 ng/mL, showed an increased placebo-subtracted QTcLD of 6.8 msec (90% CI: 3.6; 10.1) on Day 2 at 1.5 hours post-dose.
In the three fixed-dose efficacy studies of oral paliperidone extended release in subjects with schizophrenia, electrocardiogram (ECG) measurements taken at various time points showed only one subject in the oral paliperidone 12 mg group had a change exceeding 60 msec at one time- point on Day 6 (increase of 62 msec).
In the four fixed-dose efficacy studies of another once-a-month paliperidone palmitate extended-release injectable suspension in subjects with schizophrenia and in the long-term study in subjects with schizoaffective disorder, no subject experienced a change in QTcLD exceeding 60 msec and no subject had a QTcLD value of > 500 msec at any time point. In the maintenance study in subjects with schizophrenia, no subject had a QTcLD change > 60 msec, and one subject had a QTcLD value of 507 msec (Bazett's QT corrected interval [QTcB] value of 483 msec); this latter subject also had a heart rate of 45 beats per minute.
5.5 Tardive Dyskinesia
Tardive dyskinesia, a syndrome consisting of potentially irreversible, involuntary, dyskinetic movements, may develop in patients treated with antipsychotic drugs. Although the prevalence of the syndrome appears to be highest among the elderly, especially elderly women, it is impossible to predict which patients will develop the syndrome. Whether antipsychotic drug products differ in their potential to cause tardive dyskinesia is unknown.
The risk of developing tardive dyskinesia and the likelihood that it will become irreversible appear to increase with the duration of treatment and the cumulative dose. The syndrome can develop after relatively brief treatment periods, even at low doses. It may also occur after discontinuation of treatment.
Tardive dyskinesia may remit, partially or completely, if antipsychotic treatment is discontinued. Antipsychotic treatment itself may suppress (or partially suppress) the signs and symptoms of the syndrome and may thus mask the underlying process. The effect that symptomatic suppression has upon the long-term course of the syndrome is unknown.
Given these considerations, ERZOFRI should be prescribed in a manner that is most likely to minimize the occurrence of tardive dyskinesia. Chronic antipsychotic treatment should generally be reserved for patients: (1) who suffer from a chronic illness that is known to respond to antipsychotic drugs and (2) for whom alternative, equally effective, but potentially less harmful treatments are not available or appropriate. In patients who do require chronic treatment, use the lowest dose and the shortest duration of treatment producing a satisfactory clinical response. Periodically reassess the need for continued treatment.
If signs and symptoms of tardive dyskinesia appear in a patient on ERZOFRI, drug discontinuation should be considered. However, some patients may require treatment with ERZOFRI despite the presence of the syndrome.
5.6 Metabolic Changes
Atypical antipsychotic drugs have been associated with metabolic changes that may increase cardiovascular/cerebrovascular risk. These metabolic changes include hyperglycemia, dyslipidemia, and body weight gain. While all of the drugs in the class have been shown to produce some metabolic changes, each drug has its own specific risk profile.
Hyperglycemia and Diabetes Mellitus
Hyperglycemia and diabetes mellitus, in some cases extreme and associated with ketoacidosis or hyperosmolar coma or death, have been reported in patients treated with all atypical antipsychotics. These cases were, for the most part, seen in post-marketing clinical use and epidemiologic studies, not in clinical trials. Hyperglycemia and diabetes have been reported in trial subjects treated with another once-a-month paliperidone palmitate extended-release injectable suspension (also referred to as "PP1M" in this section). Assessment of the relationship between atypical antipsychotic use and glucose abnormalities is complicated by the possibility of an increased background risk of diabetes mellitus in patients with schizophrenia and the increasing incidence of diabetes mellitus in the general population. Given these confounders, the relationship between atypical antipsychotic use and hyperglycemia-related adverse events is not completely understood. However, epidemiological studies suggest an increased risk of hyperglycemia-related adverse reactions in patients treated with the atypical antipsychotics.
Patients with an established diagnosis of diabetes mellitus who are started on atypical antipsychotics should be monitored regularly for worsening of glucose control. Patients with risk factors for diabetes mellitus (e.g., obesity, family history of diabetes) who are starting treatment with atypical antipsychotics should undergo fasting blood glucose testing at the beginning of treatment and periodically during treatment. Any patient treated with atypical antipsychotics should be monitored for symptoms of hyperglycemia including polydipsia, polyuria, polyphagia, and weakness. Patients who develop symptoms of hyperglycemia during treatment with atypical antipsychotics should undergo fasting blood glucose testing. In some cases, hyperglycemia has resolved when the atypical antipsychotic was discontinued; however, some patients required continuation of anti-diabetic treatment despite discontinuation of the suspect drug.
Pooled data from the four placebo-controlled (one 9-week and three 13-week), fixed-dose studies of another PP1M in subjects with schizophrenia are presented in Table 4.
Table 4: Change in Fasting Glucose from Four Placebo-Controlled, 9- to 13-Week, Fixed-Dose Studies in Subjects with Schizophrenia Once-a-Month Paliperidone Palmitate Extended-Release Injectable Suspension Placebo 39 mg 78 mg 156 mg 234/39 mg * 234/156 mg * 234/234 mg * - * Initial deltoid injection of 234 mg followed by either 39 mg, 156 mg, or 234 mg every 4 weeks by deltoid or gluteal injection. Other dose groups (39 mg, 78 mg, and 156 mg) are from studies involving only gluteal injection. [ see Clinical Studies (14.1)].
Mean change from baseline (mg/dL) n=367 n=86 n-244 n=238 n=110 n=126 n=115 Serum Glucose Change from baseline -1.3 1.3 3.5 0.1 3.4 1.8 -0.2 Proportion of Patients with Shifts Serum Glucose Normal to High 4.6% 6.3% 6.4% 3.9% 2.5% 7.0% 6.6% (<100 mg/dL to ≥126 mg/dL) (11/241) (4/64) (11/173) (6/154) (2/79) (6/86) (5/76) In a long-term open-label pharmacokinetic and safety study in subjects with schizophrenia in which the highest maintenance dose available (234 mg) was evaluated, another PP1M was associated with a mean change in glucose of -0.4 mg/dL at Week 29 (n=109) and +6.8 mg/dL at Week 53 (n=100).
During the initial 25-week open-label period of a long-term study in subjects with schizoaffective disorder, another PP1M was associated with mean change in glucose of +5.3 mg/dL (n=518). At the endpoint of the subsequent 15-month double-blind period of the study, the PP1M was associated with a mean change in glucose of +0.3 mg/dL (n=131) compared with a mean change of +4.0 mg/dL in the placebo group (n=120).
Dyslipidemia
Undesirable alterations in lipids have been observed in patients treated with atypical antipsychotics.
Pooled data from the four placebo-controlled (one 9-week and three 13-week), fixed-dose studies of another PP1M in subjects with schizophrenia are presented in Table 5.
Table 5: Change in Fasting Lipids from Four Placebo-Controlled, 9- to 13-Week, Fixed-Dose Studies in Subjects with Schizophrenia Once-a-Month Paliperidone Palmitate Extended-Release Injectable Suspension Placebo 39 mg 78 mg 156 mg 234/39 mg * 234/156 mg * 234/234 mg * - * Initial deltoid injection of 234 mg followed by either 39 mg, 156 mg, or 234 mg every 4 weeks by deltoid or gluteal injection. Other dose groups (39 mg, 78 mg, and 156 mg) are from studies involving only gluteal injection. [see Clinical Studies (14.1)] .
Mean change from baseline (mg/dL) Cholesterol n=366 n=89 n=244 n=232 n=105 n=119 n=120 Change from baseline -6.6 -6.4 -5.8 -7.1 -0.9 -4.2 9.4 LDL n=275 n=80 n=164 n=141 n=104 n=117 n=108 Change from baseline -6.0 -4.8 -5.6 -4.8 0.9 -2.4 5.2 HDL n=286 n=89 n=165 n=150 n=105 n=118 n=115 Change from baseline 0.7 2.1 0.6 0.3 1.5 1.1 0.0 Triglycerides n=366 n=89 n=244 n=232 n=105 n=119 n=120 Change from baseline -16.7 7.6 -9.0 -11.5 -14.1 -20.0 11.9 Proportion of Patients with Shifts Cholesterol
Normal to High3.2% 2.0% 2.0% 2.1% 0% 3.1% 7.1% (<200 mg/dL to ≥240 mg/dL) (7/222) (1/51) (3/147) (3/141) (0/69) (2/65) (6/84) LDL
Normal to High1.1% 0% 0% 0% 0% (0/41) 0% 0% (<100 mg/dL to ≥160 mg/dL) (1/95) (0/29) (0/67) (0/46) (0/37) (0/44) HDL
Normal to Low13.8% 14.8% 9.6% 14.2% 12.7% 10.5% 16.0% (≥40 mg/dL to <40 mg/dL (28/203) (9/61) (11/115) (15/106) (9/71) (8/76) (13/81) Triglycerides
Normal to High3.6% 6.1% 9.2% 7.2% 1.3% 3.7% 10.7% (<150 mg/dL to ≥200 mg/dL) (8/221) (3/49) (14/153) (10/139) (1/79) (3/82) (9/84) In a long-term open-label pharmacokinetic and safety study in subjects with schizophrenia in which the highest maintenance dose available (234 mg) was evaluated, the mean changes from baseline in lipid values are presented in Table 6.
Table 6: Change in Fasting Lipids from Long-term Open-label Pharmacokinetic and Safety Study in Subjects with Schizophrenia Once-a-Month Paliperidone Palmitate Extended-Release Injectable Suspension 234 mg Week 29 Week 53 Mean change from baseline (mg/dL) Cholesterol n=112 n=100 Change from baseline -1.2 0.1 LDL n=107 n=89 Change from baseline -2.7 -2.3 HDL n=112 n=98 Change from baseline -0.8 -2.6 Triglycerides n=112 n=100 Change from baseline 16.2 37.4 The mean changes from baseline in lipid values during the initial 25-week open-label period and at the endpoint of the subsequent 15-month double-blind period in a long-term study of another PP1M in subjects with schizoaffective disorder are presented in Table 7.
Table 7: Change in Fasting Lipids from an Open-Label and Double-Blind Periods of a Long-Term Study in Subjects with Schizoaffective Disorder Open-Label Period Double-Blind Period Once-a-Month Paliperidone Palmitate Extended-Release Injectable Suspension Placebo Once-a-Month Paliperidone Palmitate Extended-Release Injectable Suspension Mean change from baseline (mg/dL) Cholesterol n=198 n=119 n=132 Change from baseline -3.9 -4.2 2.3 LDL n=198 n=117 n=130 Change from baseline -2.7 -2.8 5.9 HDL n=198 n=119 n=131 Change from baseline -2.7 -0.9 -0.7 Triglyceride n=198 n=119 n=132 Change from baseline 7.0 2.5 -12.3 Weight Gain
Weight gain has been observed with atypical antipsychotic use. Clinical monitoring of weight is recommended.
Data on mean changes in body weight and the proportion of subjects meeting a weight gain criterion of ≥ 7% of body weight from the four placebo-controlled (one 9-week and three 13-week), fixed-dose studies of another PP1M in subjects with schizophrenia are presented in Table 8.
Table 8: Mean Change in Body Weight (kg) and the Proportion of Subjects with ≥ 7% Gain in Body Weight from Four Placebo-Controlled, 9- to 13-Week, Fixed-Dose Studies in Subjects with Schizophrenia Once-a-Month Paliperidone Palmitate Extended-Release Injectable Suspension Placebo
n=45139 mg
n=11678 mg
n=280156 mg
n=267234/39 mg *
n=137234/156 mg *
n=144234/234 mg *
n=145- * Initial deltoid injection of 234 mg followed by either 39 mg, 156 mg, or 234 mg every 4 weeks by deltoid or gluteal injection. Other dose groups (39 mg, 78 mg, and 156 mg) are from studies involving only gluteal injection. [see Clinical Studies (14.1)] .
Weight (kg) Change from baseline -0.4 0.4 0.8 1.4 0.4 0.7 1.4 Weight Gain ≥ 7% increase from baseline 3.3 % 6.0% 8.9% 9.0% 5.8% 8.3% 13.1 % In a long-term open-label pharmacokinetic and safety study in which the highest maintenance dose available (234 mg) was evaluated, another PP1M was associated with a mean change in weight of +2.4 kg at Week 29 (n=134) and +4.3 kg at Week 53 (n=113).
During the initial 25-week open-label period of a long-term study in subjects with schizoaffective disorder, another PP1M was associated with a mean change in weight of +2.2 kg and 18.4% of subjects had an increase in body weight of ≥ 7% (n=653). At the endpoint of the subsequent 15-month double-blind period of the study, the PP1M was associated with a mean change in weight of -0.2 kg and 13.0% of subjects had an increase in body weight of ≥ 7% (n=161); the placebo group had a mean change in weight of -0.8 kg and 6.0% of subjects had an increase in body weight of ≥ 7% (n=168).
5.7 Orthostatic Hypotension and Syncope
Paliperidone can induce orthostatic hypotension and syncope in some patients because of its alpha- adrenergic blocking activity. Syncope was reported in < 1% (4/1293) of subjects treated with another once-a-month paliperidone palmitate extended-release injectable suspension (PP1M) in the recommended maintenance dose range of 39 mg to 234 mg in the four fixed- dose, double-blind, placebo-controlled trials compared with 0% (0/510) of subjects treated with placebo. In the four fixed-dose efficacy studies in subjects with schizophrenia, orthostatic hypotension was reported as an adverse event by < 1% (2/1293) of the PP1M-treated subjects compared to 0% (0/510) with placebo. Incidences of orthostatic hypotension and syncope in the long-term studies in subjects with schizophrenia and schizoaffective disorder were similar to those observed in the short-term studies.
Use ERZOFRI with caution in patients with known cardiovascular disease (e.g., heart failure, history of myocardial infarction or ischemia, conduction abnormalities), cerebrovascular disease, or conditions that predispose the patient to hypotension (e.g., dehydration, hypovolemia, and treatment with antihypertensive medications). Monitoring of orthostatic vital signs should be considered in patients who are vulnerable to hypotension.
5.8 Falls
Somnolence, postural hypotension, motor and sensory instability have been reported with the use of antipsychotics, including paliperidone palmitate, which may lead to falls and, consequently, fractures or other fall-related injuries. For patients, particularly the elderly, with diseases, conditions, or medications that could exacerbate these effects, assess the risk of falls when initiating antipsychotic treatment and recurrently for patients on long-term antipsychotic therapy.
5.9 Leukopenia, Neutropenia, and Agranulocytosis
In clinical trial and/or postmarketing experience, events of leukopenia and neutropenia have been reported temporally related to antipsychotic agents, including once-a-month paliperidone palmitate extended-release injectable suspension (PP1M). Agranulocytosis has also been reported.
Possible risk factors for leukopenia/neutropenia include pre-existing low white blood cell count (WBC)/absolute neutrophil count (ANC) and history of drug-induced leukopenia/neutropenia. In patients with a history of a clinically significant low WBC/ANC or a drug-induced leukopenia/neutropenia, perform a complete blood count (CBC) frequently during the first few months of therapy. In such patients, consider discontinuation of ERZOFRI at the first sign of a clinically significant decline in WBC in the absence of other causative factors.
Monitor patients with clinically significant neutropenia for fever or other symptoms or signs of infection and treat promptly if such symptoms or signs occur. Discontinue ERZOFRI in patients with severe neutropenia (absolute neutrophil count < 1000/mm 3) and follow their WBC until recovery.
5.10 Hyperprolactinemia
Like other drugs that antagonize dopamine D 2receptors, paliperidone elevates prolactin levels and the elevation persists during chronic administration. Paliperidone has a prolactin-elevating effect similar to that seen with risperidone, a drug that is associated with higher levels of prolactin than other antipsychotic drugs.
Hyperprolactinemia, regardless of etiology, may suppress hypothalamic GnRH, resulting in reduced pituitary gonadotrophin secretion. This, in turn, may inhibit reproductive function by impairing gonadal steroidogenesis in both female and male patients. Galactorrhea, amenorrhea, gynecomastia, and impotence have been reported in patients receiving prolactin-elevating compounds. Long-standing hyperprolactinemia when associated with hypogonadism may lead to decreased bone density in both female and male subjects.
Tissue culture experiments indicate that approximately one-third of human breast cancers are prolactin dependent in vitro, a factor of potential importance if the prescription of these drugs is considered in a patient with previously detected breast cancer. An increase in the incidence of pituitary gland, mammary gland, and pancreatic islet cell neoplasia (mammary adenocarcinomas, pituitary and pancreatic adenomas) was observed in the risperidone carcinogenicity studies conducted in mice and rats [see Nonclinical Toxicology (13.1)] . Published epidemiologic studies have shown inconsistent results when exploring the potential association between hyperprolactinemia and breast cancer.
Prolactin data from two long-term, double-blind, placebo-controlled studies with another PP1M are presented below; one study was in a population of patients with schizophrenia; the second study was in patients with schizoaffective disorder.
Schizophrenia
In a long-term maintenance trial of another once-a-month paliperidone palmitate extended-release injectable suspension (PP1M) in schizophrenia patients (Study 5) [see Clinical Studies (14.1)] , elevations of prolactin to above the reference range (> 18 ng/mL in males and > 30 ng/mL in females) relative to open-label baseline at any time during the double- blind phase were noted in a higher percentage of the patients in the PP1M group than those in the placebo group in males (51.9% versus 29.0%) and in females (50.5% versus 42.9%). During the double-blind phase, 4 females (4.2%) in the PP1M group experienced potentially prolactin-related adverse reactions (amenorrhea N=2; galactorrhea N=1; menstruation irregular N=1), while 2 females (2.2%) in the placebo group experienced potentially prolactin-related adverse reactions (amenorrhea N=1; breast pain N=1). One male (0.9%) in the PP1M group experienced erectile dysfunction and 1 male (0.9%) in placebo group experienced gynecomastia.
Prior to the double-blind phase (during the 33-week open-label phase of the long-term maintenance trial), the mean (SD) serum prolactin values at baseline were 14.9 (22.3) ng/mL in males (N=490) and 35.2 (39.6) ng/mL in females (N=358). At the end of the open-label phase, mean (SD) prolactin values were 24.7 (22.5) ng/mL in males (N=470) and 59.5 (38.1) ng/mL in females (N=333). During the open-label phases 49.2% of females and 47.7% of males experienced elevations of prolactin above the reference range relative to baseline, and a higher proportion of females experienced potentially prolactin-related adverse reactions compared to males (5.3% versus 1.8%). Amenorrhea (2.5%) in females and no single potentially prolactin-related adverse reaction in males were observed with a rate greater than 2%.
Schizoaffective Disorder
In a long-term maintenance trial of another PP1M in patients with schizoaffective disorder (Study SCA-3004) see Clinical Studies (14.2), elevations of prolactin to above the reference range (> 13.13 ng/mL in males and > 26.72 ng/mL in females) relative to open-label baseline at any time during the 15-month double-blind phase were noted in a higher percentage of patients in the PP1M group than those in the placebo group in males (55.6% versus 23.2%) and in females (44.3% versus 25.0%). During the 15-month double-blind phase, 11 females (13.9%) in the PP1M group had 14 potentially prolactin-related adverse reactions (hyperprolactinemia N=3; blood prolactin increased N=4; libido decreased N=1; amenorrhea N=3; galactorrhea N=3), while 5 females (5.8%) in the placebo group had 6 potentially prolactin-related adverse reactions (hyperprolactinemia N=2; blood prolactin increased N=1; amenorrhea N=2; galactorrhea N=1). Six males (7.1%) in the PP1M group experienced 6 potentially prolactin-related adverse reactions (hyperprolactinemia N=4; libido decreased N=1; erectile dysfunction N=1), while 1 male (1.2%) in the placebo group experienced adverse reaction of blood prolactin increased.
Prior to the 15-month double-blind phase (during the 25-week open-label phase of the long-term maintenance trial), the mean (SD) serum prolactin values at baseline were 14.6 (14.0) ng/mL in males (N=352) and 39.1 (44.6) ng/mL in females (N=302). At the end of the open-label phase, mean (SD) prolactin values were 32.8 (17.2) ng/mL in males (N=275) and 72.4 (46.5) ng/mL in females (N=239). During the open-label phase, 48.9% of females and 53.3% of males experienced elevations of prolactin above the reference range relative to baseline, and a higher proportion of females experienced potentially prolactin-related adverse reactions compared to males (10.0% versus 9.0%). Amenorrhea (5.8%) and galactorrhea (2.9%) in females and libido decrease (2.8%) and erectile dysfunction (2.5%) in males were observed with a rate greater than 2%.
5.11 Potential for Cognitive and Motor Impairment
Somnolence, sedation, and dizziness were reported as adverse reactions in subjects treated with another once-a-month paliperidone palmitate extended-release injectable suspension (PP1M) [see Adverse Reactions (6.1)] . Antipsychotics, including ERZOFRI, have the potential to impair judgment, thinking, or motor skills. Patients should be cautioned about performing activities requiring mental alertness, such as operating hazardous machinery or operating a motor vehicle, until they are reasonably certain that paliperidone therapy does not adversely affect them.
5.12 Seizures
In the four fixed-dose double-blind placebo-controlled studies in subjects with schizophrenia, <1% (1 out of 1,293) of subjects treated with another once-a-month paliperidone palmitate extended-release injectable suspension (PP1M) in the recommended dose range of 39 mg to 234 mg experienced a convulsion compared with <1% (1 out of 510) of placebo-treated subjects who experienced a grand mal convulsion.
Like other antipsychotic drugs, ERZOFRI should be used cautiously in patients with a history of seizures or other conditions that potentially lower the seizure threshold. Conditions that lower the seizure threshold may be more prevalent in patients 65 years or older.
5.13 Dysphagia
Esophageal dysmotility and aspiration have been associated with antipsychotic drug use. ERZOFRI and other antipsychotic drugs should be used cautiously in patients at risk for aspiration.
5.14 Priapism
Drugs with alpha-adrenergic blocking effects have been reported to induce priapism. Although no cases of priapism have been reported in clinical trials with another once-a-month paliperidone palmitate extended-release injectable suspension (PP1M), priapism has been reported with oral paliperidone during postmarketing surveillance. Severe priapism may require surgical intervention.
5.15 Disruption of Body Temperature Regulation
Disruption of the body's ability to reduce core body temperature has been attributed to antipsychotic agents. Appropriate care is advised when prescribing ERZOFRI to patients who will be experiencing conditions which may contribute to an elevation in core body temperature, e.g., exercising strenuously, exposure to extreme heat, receiving concomitant medication with anticholinergic activity, or being subject to dehydration.
-
6 ADVERSE REACTIONS
The following are discussed in more detail in other sections of the labeling:
- Increased mortality in elderly patients with dementia-related psychosis [see Boxed Warningand Warnings and Precautions (5.1)]
- Cerebrovascular adverse reactions, including stroke, in elderly patients with dementia-related psychosis [see Warnings and Precautions (5.2)]
- Neuroleptic malignant syndrome [see Warnings and Precautions (5.3)]
- QT prolongation [see Warnings and Precautions (5.4)]
- Tardive dyskinesia [see Warnings and Precautions (5.5)]
- Metabolic changes [see Warnings and Precautions (5.6)]
- Orthostatic hypotension and syncope [see Warnings and Precautions (5.7)]
- Falls [see Warnings and Precautions (5.8)]
- Leukopenia, neutropenia, and agranulocytosis [see Warnings and Precautions (5.9)]
- Hyperprolactinemia [see Warnings and Precautions (5.10)]
- Potential for cognitive and motor impairment [see Warnings and Precautions (5.11)]
- Seizures [see Warnings and Precautions (5.12)]
- Dysphagia [see Warnings and Precautions (5.13)]
- Priapism [see Warnings and Precautions (5.14)]
- Disruption of body temperature regulation [see Warnings and Precautions (5.15)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
The safety of ERZOFRI for the treatment of schizophrenia in adults and schizoaffective disorder in adults as monotherapy and as an adjunct to mood stabilizers or antidepressants is based upon adequate and well-controlled studies of another once-a-month paliperidone palmitate extended-release injectable suspension (also referred to as "PP1M" in this section). Below is a display of adverse reactions with another PP1M from those adequate and well-controlled studies.
Injection site reactions for ERZOFRI presented in this section (see " Pain and Injection Site Reactions with ERZOFRI" below) are based on pharmacokinetic studies.
Patient Exposure
The data described in this section are derived from a clinical trial database consisting of a total of 3,817 subjects (approximately 1,705 patient-years exposure) with schizophrenia who received at least one dose of PP1M in the recommended dose range of 39 mg to 234 mg and a total of 510 subjects with schizophrenia who received placebo. Among the 3,817 PP1M-treated subjects, 1,293 received PP1M in four fixed-dose, double- blind, placebo-controlled trials (one 9-week and three 13-week studies), 849 received PP1M in the maintenance trial (median exposure 229 days during the initial 33-week open-label phase of this study, of whom 205 continued to receive PP1M during the double-blind placebo-controlled phase of this study [median exposure 171 days]), and 1,675 received PP1M in five non-placebo controlled trials (three noninferiority active- comparator trials, one long-term open-label pharmacokinetic and safety study, and an injection site [deltoid-gluteal] cross-over trial). One of the 13-week studies included a 234 mg PP1M initiation dose followed by treatment with either 39 mg, 156 mg, or 234 mg every 4 weeks.
The safety of PP1M was also evaluated in a 15-month, long-term study comparing the other PP1M to selected oral antipsychotic therapies in adult subjects with schizophrenia. A total of 226 subjects received PP1M during the 15-month, open-label period of this study; 218 subjects received selected oral antipsychotic therapies. The safety of PP1M was similar to that seen in previous double-blind, placebo-controlled clinical trials in adult subjects with schizophrenia.
The safety of PP1M was also evaluated in a long-term study in adult subjects with schizoaffective disorder. A total of 667 subjects PP1M during the initial 25-week open-label period of this study (median exposure 147 days); 164 subjects continued to receive PP1M during the 15-month double-blind placebo-controlled period of this study (median exposure 446 days). Adverse reactions that occurred more frequently in the PP1M group than the placebo group (a 2% difference or more between groups) were weight increased, nasopharyngitis, headache, hyperprolactinemia, and pyrexia.
Adverse Reactions in Double-Blind, Placebo-Controlled Clinical Trials
Commonly Observed Adverse Reactions:The most common (at least 5% in any PP1M group) and likely drug-related (adverse events for which the drug rate is at least twice the placebo rate) adverse reactions from the double-blind, placebo-controlled trials in subjects with schizophrenia were injection site reactions, somnolence/sedation, dizziness, akathisia, and extrapyramidal disorder .No occurrences of adverse events reached this threshold in the long-term double-blind, placebo-controlled study in subjects with schizoaffective disorder.
Discontinuation of Treatment Due to Adverse Events:The percentage of subjects who discontinued due to adverse events in the four fixed-dose, double-blind, placebo-controlled schizophrenia trials were similar for PP1M- and placebo-treated subjects.
The percentage of subjects who discontinued due to adverse events in the open-label period of the long-term study in subjects with schizoaffective disorder was 7.5%. During the double-blind, placebo-controlled period of that study, the percentages of subjects who discontinued due to adverse events were 5.5% and 1.8% in PP1M- and placebo-treated subjects, respectively.
Dose-Related Adverse Reactions:Based on the pooled data from the four fixed-dose, double- blind, placebo-controlled trials in subjects with schizophrenia, among the adverse reactions that occurred with ≥ 2% incidence in the subjects treated with PP1M, only akathisia increased with dose. Hyperprolactinemia also exhibited a dose relationship, but did not occur at ≥ 2% incidence in PP1M-treated subjects from the four fixed-dose studies.
Adverse Reactions Occurring at an Incidence of 2% or More in a once-a-month paliperidone palmitate extended-release injectable suspension-Treated Patients:Table 9 lists the adverse reactions reported in 2% or more of PP1M -treated subjects and at a greater proportion than in the placebo group with schizophrenia in the four fixed-dose, double-blind, placebo-controlled trials.
Table 9: Incidences of Adverse Reactions 2% or More of a Once-a-Month Paliperidone Palmitate Extended-Release Injectable Suspension-Treated Patients (and Greater than Placebo) with Schizophrenia in Four Fixed-Dose, Double-Blind, Placebo-Controlled Trials Once-a-Month Paliperidone Palmitate Extended-Release Injectable Suspension System Organ Class
Adverse ReactionsPlacebo *
(N=510)39 mg
(N=130)78 mg
(N=302)156 mg
(N=312)234/39 mg †
(N=160)234/156 mg †
(N=165)234/234 mg †
(N=163)Percentages are rounded to whole numbers. Table includes adverse reactions that were reported in 2% or more of subjects in any of the once-a-month paliperidone palmitate extended-release injectable suspension dose groups and which occurred at greater incidence than in the placebo group. - * Placebo group is pooled from all studies and included either deltoid or gluteal injection depending on study design.
- † Initial deltoid injection of 234 mg followed by either 39 mg, 156 mg, or 234 mg every 4 weeks by deltoid or gluteal injection. Other dose groups (39 mg, 78 mg, and 156 mg) are from studies involving only gluteal injection. [see Clinical Studies (14.1)]
Total percentage of subjects with adverse reactions 70 75 68 69 63 60 63 Gastrointestinal disorders Abdominal discomfort/abdominal pain upper 2 2 4 4 1 2 4 Diarrhea 2 0 3 2 1 2 2 Dry mouth 1 3 1 0 1 1 1 Nausea 3 4 4 3 2 2 2 Toothache 1 1 1 3 1 2 3 Vomiting 4 5 4 2 3 2 2 General disorders and administration site conditions Asthenia 0 2 1 <1 0 1 1 Fatigue 1 1 2 2 1 2 1 Injection site reactions 2 0 4 6 9 7 10 Infections and infestations Nasopharyngitis 2 0 2 2 4 2 2 Upper respiratory tract infection 2 2 2 2 1 2 4 Urinary tract infection 1 0 1 <1 1 1 2 Investigations Weight increased 1 4 4 1 1 1 2 Musculoskeletal and connective tissue disorders Back pain 2 2 1 3 1 1 1 Musculoskeletal stiffness 1 1 <1 <1 1 1 2 Myalgia 1 2 1 <1 1 0 2 Pain in extremity 1 0 2 2 2 3 0 Nervous system disorders Akathisia 3 2 2 3 1 5 6 Dizziness 1 6 2 4 1 4 2 Extrapyramidal disorder 1 5 2 3 1 0 0 Headache 12 11 11 15 11 7 6 Somnolence/sedation 3 5 7 4 1 5 5 Psychiatric disorders Agitation 7 10 5 9 8 5 4 Anxiety 7 8 5 3 5 6 6 Nightmare <1 2 0 0 0 0 0 Respiratory, thoracic and mediastinal disorders Cough 1 2 3 1 0 1 1 Vascular disorders Hypertension 1 2 1 1 1 1 0 Adverse reactions for which the once-a-month paliperidone palmitate extended-release injectable suspension incidence was equal to or less than placebo are not listed in the table, but included the following: dyspepsia, psychotic disorder, schizophrenia, and tremor. The following terms were combined: somnolence/sedation, breast tenderness/breast pain, abdominal discomfort/abdominal pain upper/stomach discomfort, and tachycardia/sinus tachycardia/heart rate increased. All injection site reaction-related adverse reactions were collapsed and are grouped under "Injection site reactions".
Other Adverse Reactions Observed During the Clinical Trial Evaluation of Once-a-Month Paliperidone Palmitate Extended-Release Injectable Suspension
The following list does not include reactions: 1) already listed in previous tables or elsewhere in labeling, 2) for which a drug cause was remote, 3) which were so general as to be uninformative, or 4) which were not considered to have significant clinical implications.
Cardiac disorders:atrioventricular block first degree, bradycardia, bundle branch block, palpitations, postural orthostatic tachycardia syndrome, tachycardia
Ear and labyrinth disorders:vertigo
Eye disorders:eye movement disorder, eye rolling, oculogyric crisis, vision blurred
Gastrointestinal disorders:constipation, dyspepsia, flatulence, salivary hypersecretion
Immune system disorders:hypersensitivity
Investigations:alanine aminotransferase increased, aspartate aminotransferase increased, electrocardiogram abnormal
Metabolism and nutrition disorders:decreased appetite, hyperinsulinemia, increased appetite
Musculoskeletal and connective tissue disorders:arthralgia, joint stiffness, muscle rigidity, muscle spasms, muscle tightness, muscle twitching, nuchal rigidity
Nervous system disorders:bradykinesia, cerebrovascular accident, cogwheel rigidity, convulsion, dizziness postural, drooling, dysarthria, dyskinesia, dystonia, hypertonia, lethargy, oromandibular dystonia, parkinsonism, psychomotor hyperactivity, syncope
Psychiatric disorders:insomnia, libido decreased, restlessness
Reproductive system and breast disorders:amenorrhea, breast discharge, breast enlargement/breast swelling, breast tenderness/breast pain, ejaculation disorder, erectile dysfunction, galactorrhea, gynecomastia, menstrual disorder, menstruation delayed, menstruation irregular, sexual dysfunction
Respiratory, thoracic and mediastinal disorders:nasal congestion
Skin and subcutaneous tissue disorders:drug eruption, pruritus, pruritus generalized, rash, urticaria
Demographic Differences
An examination of population subgroups in the double-blind placebo-controlled trials did not reveal any evidence of differences in safety on the basis of age, gender, or race alone; however, there were few subjects 65 years of age and older.
Extrapyramidal Symptoms (EPS)
Pooled data from the two double-blind, placebo-controlled, 13-week, fixed-dose trials in adult subjects with schizophrenia provided information regarding EPS. Several methods were used to measure EPS: (1) the Simpson-Angus global score which broadly evaluates parkinsonism, (2) the Barnes Akathisia Rating Scale global clinical rating score which evaluates akathisia, (3) the Abnormal Involuntary Movement Scale scores which evaluates dyskinesia, and (4) use of anticholinergic medications to treat EPS (Table 10), and (5) incidence of spontaneous reports of EPS (Table 11).
Table 10: Extrapyramidal Symptoms (EPS) Assessed by Incidence of Rating Scales and Use of Anticholinergic Medication – Schizophrenia Studies in Adults Percentage of Subjects Once-a-Month Paliperidone Palmitate Extended-Release Injectable Suspension Scale Placebo
(N=262)39 mg
(N=130)78 mg
(N=223)156 mg
(N=228)- * For parkinsonism, percent of subjects with Simpson-Angus Total score > 0.3 at endpoint (Total score defined as total sum of items score divided by the number of items)
- † For Akathisia, percent of subjects with Barnes Akathisia Rating Scale global score ≥ 2 at endpoint
- ‡ For Dyskinesia, percent of subjects with a score ≥ 3 on any of the first 7 items or a score ≥ 2 on two or more of any of the first 7 items of the Abnormal Involuntary Movement Scale at endpoint
- § Percent of subjects who received anticholinergic medications to treat EPS
Parkinsonism * 9 12 10 6 Akathisia † 5 5 6 5 Dyskinesia ‡ 3 4 6 4 Use of Anticholinergic Medications § 12 10 12 11 Table 11: Extrapyramidal Symptoms (EPS)-Related Events by MedDRA Preferred Term – Schizophrenia Studies in Adults Percentage of Subjects Once-a-Month Paliperidone Palmitate Extended-Release Injectable Suspension EPS Group Placebo
(N=262)39 mg
(N=130)78 mg
(N=223)156 mg
(N=228)Parkinsonism group includes: Extrapyramidal disorder, hypertonia, musculoskeletal stiffness, parkinsonism, drooling, masked facies, muscle tightness, hypokinesia
Hyperkinesia group includes: Akathisia, restless legs syndrome, restlessness
Dyskinesia group includes: Dyskinesia, choreoathetosis, muscle twitching, myoclonus, tardive dyskinesia
Dystonia group includes: Dystonia, muscle spasmsOverall percentage of subjects with EPS-related adverse events 10 12 11 11 Parkinsonism 5 6 6 4 Hyperkinesia 2 2 2 4 Tremor 3 2 2 3 Dyskinesia 1 2 3 1 Dystonia 0 1 1 2 The results across all phases of the maintenance trial in subjects with schizophrenia exhibited comparable findings. In the 9-week, fixed-dose, double-blind, placebo-controlled trial, the proportions of parkinsonism and akathisia assessed by incidence of rating scales were higher in the PP1M 156 mg group (18% and 11%, respectively) than in the PP1M 78 mg group (9% and 5%, respectively) and placebo group (7% and 4%, respectively).
In the 13-week study in subjects with schizophrenia involving 234 mg initiation dosing, the incidence of any EPS was similar to that of the placebo group (8%), but exhibited a dose-related pattern with 6%, 10%, and 11% in the PP1M 234/39 mg, 234/156 mg, and 234/234 mg groups, respectively. Hyperkinesia was the most frequent category of EPS-related adverse events in this study, and was reported at a similar rate between the placebo (4.9%) and PP1M 234/156 mg (4.8%) and 234/234 mg (5.5%) groups, but at a lower rate in the 234/39 mg group (1.3%).
In the long-term study in subjects with schizoaffective disorder, EPS reported during the 25-week open-label PP1M treatment included hyperkinesia (12.3%), parkinsonism (8.7%), tremor (3.4%), dyskinesia (2.5%), and dystonia (2.1%). During the 15-month double-blind treatment, the incidence of any EPS was similar to that of the placebo group (8.5% and 7.1% respectively). The most commonly reported treatment-emergent EPS-related adverse events (> 2%) in any treatment group in the double-blind phase of the study (PP1M versus placebo) were hyperkinesia (3.7% versus 2.9%), parkinsonism (3.0% versus 1.8%), and tremor (1.2% versus 2.4%).
Dystonia
Symptoms of dystonia, prolonged abnormal contractions of muscle groups, may occur in susceptible individuals during the first few days of treatment. Dystonic symptoms include: spasm of the neck muscles, sometimes progressing to tightness of the throat, swallowing difficulty, difficulty breathing, and/or protrusion of the tongue. While these symptoms can occur at low doses, they occur more frequently and with greater severity with high potency and at higher doses of first-generation antipsychotic drugs. An elevated risk of acute dystonia is observed in males and younger age groups.
Pain Assessment and Injection Site Reactions
In the pooled data from the two 13-week, fixed-dose, double-blind, placebo-controlled trials of another PP1M in subjects with schizophrenia, the mean intensity of injection pain reported by subjects using a visual analog scale (0 = no pain to 100 = unbearably painful) decreased in all treatment groups from the first to the last injection (placebo: 10.9 to 9.8; 39 mg: 10.3 to 7.7; 78 mg: 10.0 to 9.2; 156 mg: 11.1 to 8.8). The results from both the 9-week, fixed-dose, double-blind, placebo-controlled trial and the double-blind phase of the maintenance trial exhibited comparable findings.
In the 13-week study involving 234 mg initiation dosing in subjects with schizophrenia, occurrences of induration, redness, or swelling, as assessed by blinded study personnel, were infrequent, generally mild, decreased over time, and similar in incidence between the PP1M and placebo groups. Investigator ratings of injection pain were similar for the placebo and PP1M groups. Investigator evaluations of the injection site after the first injection for redness, swelling, induration, and pain were rated as absent for 69-100% of subjects in both the PP1M and placebo groups. At Day 92, investigators rated absence of redness, swelling, induration, and pain in 95-100% of subjects in both the PP1M and placebo groups.
ERZOFRI was evaluated in 281 patients with schizophrenia or schizoaffective disorder in an open-label randomized parallel arm study. The percentage of patients in the open-label study reporting injection site-related adverse reactions at the first injection for patients treated with ERZOFRI (all reported as injection site pain) was similar to the percentage of patients treated with another PP1M.
Additional Adverse Reactions Reported in Clinical Trials with Oral Paliperidone
The following is a list of additional adverse reactions that have been reported in clinical trials with oral paliperidone:
Cardiac disorders: bundle branch block left, sinus arrhythmia
Gastrointestinal disorders: abdominal pain, small intestinal obstruction
General disorders and administration site conditions: edema, edema peripheral
Immune system disorders: anaphylactic reaction
Infections and infestations:rhinitis
Musculoskeletal and connective tissue disorders: musculoskeletal pain, torticollis, trismus
Nervous system disorders: grand mal convulsion, parkinsonian gait, transient ischemic attack
Psychiatric disorders:sleep disorder
Reproductive system and breast disorders: breast engorgement
Respiratory, thoracic and mediastinal disorders:pharyngolaryngeal pain, pneumonia aspiration
Skin and subcutaneous tissue disorders:rash papular
Vascular disorders:hypotension, ischemia
6.2 Postmarketing Experience
The following adverse reactions have been identified during post-approval use of paliperidone; because these reactions were reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure: angioedema, catatonia, ileus, somnambulism, swollen tongue, thrombotic thrombocytopenic purpura, urinary incontinence, and urinary retention.
Cases of anaphylactic reaction after injection with another once-a-month paliperidone palmitate extended-release injectable suspension product have been reported during postmarketing experience in patients who have previously tolerated oral risperidone or oral paliperidone.
Paliperidone is the major active metabolite of risperidone. Adverse reactions reported with oral risperidone and risperidone long-acting injection can be found in the Adverse Reactions (6)sections of the package inserts for those products.
-
7 DRUG INTERACTIONS
7.1 Drugs Having Clinically Important Interactions with ERZOFRI
Because paliperidone palmitate is hydrolyzed to paliperidone [see Clinical Pharmacology (12.3)] , results from studies with oral paliperidone should be taken into consideration when assessing drug-drug interaction potential.
Table 12 presents clinically significant drug interactions with ERZOFRI.
Table 12: Clinically Important Drug Interactions with ERZOFRI Centrally Acting Drugs and Alcohol Clinical Rationale: Given the primary CNS effects of paliperidone, concomitant use of centrally acting drugs and alcohol may modulate the CNS effects of ERZOFRI. Clinical Recommendation: ERZOFRI should be used with caution in combination with other centrally acting drugs and alcohol [see Adverse Reactions (6.1, 6.2)] . Drugs with Potential for Inducing Orthostatic Hypotension Clinical Rationale: Because ERZOFRI has the potential for inducing orthostatic hypotension, an additive effect may occur when ERZOFRI is administered with other therapeutic agents that have this potential [see Warnings and Precautions (5.7)] . Clinical Recommendation: Monitor orthostatic vital signs in patients who are vulnerable to hypotension [see Warnings and Precautions (5.7)] . Strong Inducers of CYP3A4 and P-gp Clinical Rationale: The concomitant use of paliperidone and strong inducers of CYP3A4 and P-gp may decrease the exposure of paliperidone [see Clinical Pharmacology (12.3)] . Clinical Recommendation: Avoid using CYP3A4 and/or P-gp inducers with ERZOFRI during the 1-month dosing interval, if possible. If administering a strong inducer is necessary, consider managing the patient using paliperidone extended-release tablets [see Dosage and Administration (2.5)] . Levodopa and Other Dopamine Agonists Clinical Rationale: Paliperidone may antagonize the effect of levodopa and other dopamine agonists. Clinical Recommendation: Monitor and manage patient as clinically appropriate. 7.2 Drugs Having No Clinically Important Interactions with ERZOFRI
Based on pharmacokinetic studies with oral paliperidone, no dosage adjustment of ERZOFRI is required when administered with valproate [see Clinical Pharmacology (12.3)]. Additionally, no dosage adjustment is necessary for valproate when co-administered with ERZOFRI [See Clinical Pharmacology (12.3)].
Pharmacokinetic interaction between lithium and ERZOFRI is also unlikely.
Paliperidone is not expected to cause clinically important pharmacokinetic interactions with drugs that are metabolized by cytochrome P450 isozymes. In vitrostudies indicate that CYP2D6 and CYP3A4 may be involved in paliperidone metabolism; however, there is no evidence in vivothat inhibitors of these enzymes significantly affect the metabolism of paliperidone. Paliperidone is not a substrate of CYP1A2, CYP2A6, CYP2C9, and CYP2C19; an interaction with inhibitors or inducers of these isozymes is unlikely. [see Clinical Pharmacology (12.3)]
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Exposure Registry
There is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to atypical antipsychotics, including ERZOFRI, during pregnancy. Healthcare providers are encouraged to advise patients to register by contacting the National Pregnancy Registry for Atypical Antipsychotics at 1-866-961-2388 or online at http://womensmentalhealth.org/clinical- and-research-programs/pregnancyregistry/.
Risk Summary
Neonates exposed to antipsychotic drugs during the third trimester of pregnancy are at risk for extrapyramidal and/or withdrawal symptoms following delivery (see Clinical Considerations) . Overall, available data from published epidemiologic studies of pregnant women exposed to paliperidone have not established a drug-associated risk for major birth defects, miscarriage, or adverse maternal or fetal outcomes (see Data) . There are risks to the mother associated with untreated schizophrenia and with exposure to antipsychotics, including ERZOFRI, during pregnancy (see Clinical Considerations). Paliperidone has been detected in plasma in adult subjects up to 176 days after a single-dose administration of ERZOFRI [see Clinical Pharmacology (12.3)] , and the clinical significance of ERZOFRI administered before pregnancy or anytime during pregnancy is not known.
The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defects, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
In animal reproduction studies, there were no treatment related effects on the offspring when pregnant rats were injected intramuscularly with paliperidone palmitate during the period of organogenesis at doses up to 10 times the maximum recommended human dose (MRHD) of 234 mg paliperidone palmitate based on mg/m 2body surface area (BSA). There were no increases in fetal abnormalities when pregnant rats and rabbits were treated orally with paliperidone during the period of organogenesis with up to 8 times the MRHD of 12 mg of paliperidone based on mg/m 2BSA. Additional reproduction toxicity studies were conducted with orally administered risperidone, which is extensively converted to paliperidone ( see Animal data).
Clinical Considerations
Disease-associated maternal and/or embryo/fetal risk
There is a risk to the mother from untreated schizophrenia, including increased risk of relapse, hospitalization, and suicide. Schizophrenia and bipolar I disorder are associated with increased adverse perinatal outcomes, including preterm birth. It is not known if this is a direct result of the illness or other comorbid factors.
Fetal/Neonatal Adverse Reactions
Extrapyramidal and/or withdrawal symptoms, including agitation, hypertonia, hypotonia, tremor, somnolence, respiratory distress, and feeding disorder have been reported in neonates who were exposed to antipsychotic drugs, including paliperidone palmitate, during the third trimester of pregnancy. These symptoms have varied in severity. Monitor neonates exhibiting extrapyramidal and/or withdrawal symptoms and manage symptoms appropriately. Some neonates recovered within hours or days without specific treatment; others required prolonged hospitalization.
Data
Human Data
Published data from observational studies, birth registries, and case reports on the use of atypical antipsychotics during pregnancy do not report a clear association with antipsychotics and major birth defects. A prospective observational study including 6 women treated with risperidone, the parent compound of paliperidone, demonstrated placental passage of risperidone and paliperidone. A retrospective cohort study from a Medicaid database of 9,258 women exposed to antipsychotics during pregnancy did not indicate an overall increased risk for major birth defects. There was a small increase in the risk of major birth defects (RR= 1.26, 95% CI 1.02-1.56) and of cardiac malformations (RR=1.26, 95% CI 0.88-1.81) in a subgroup of 1,566 women exposed to the parent compound of paliperidone, risperidone, during the first trimester of pregnancy; however, there is no mechanism of action to explain the difference in malformation rates.
Animal Data
There were no treatment-related effects on the offspring when pregnant rats were injected intramuscularly with paliperidone palmitate extended-release injectable suspension during the period of organogenesis at doses up to 250 mg/kg, which is 10 times MRHD of 234 mg paliperidone palmitate as a monthly maintenance dose based on body surface area (BSA).
In animal reproduction studies, there were no increases in fetal abnormalities when pregnant rats and rabbits were treated orally with paliperidone during the period of organogenesis with up to 8 times the MRHD of 12 mg based on BSA.
Additional reproduction toxicity studies were conducted with orally administered risperidone, which is extensively converted to paliperidone. Cleft palate was observed in the offspring of pregnant mice treated with risperidone at 3 to 4 times the MRHD of 16 mg based on BSA; maternal toxicity occurred at 4 times the MHRD. There was no evidence of teratogenicity in embryo-fetal developmental toxicity studies with risperidone in rats and rabbits at doses up to 6 times the MRHD of 16 mg risperidone based on BSA. When the offspring of pregnant rats, treated with risperidone at 0.6 times the MRHD based on BSA, reached adulthood, learning was impaired. Increased neuronal cell death occurred in the fetal brains of the offspring of pregnant rats treated at 0.5 to 1.2 times the MRHD; the postnatal development and growth of the offspring were delayed.
In rat reproduction studies with risperidone, pup deaths occurred at oral doses which are less than the MRHD of risperidone based on BSA; it is not known whether these deaths were due to a direct effect on the fetuses or pups or, to effects on the dams (see RISPERDAL ®prescribing information).
8.2 Lactation
Risk Summary
Limited data from published literature report the presence of paliperidone in human breast milk. There is no information on the effects on the breastfed infant or the effects on milk production; however, there are reports of sedation, failure to thrive, jitteriness, and extrapyramidal symptoms (tremors and abnormal muscle movements) in breastfed infants exposed to paliperidone's parent compound, risperidone (see Clinical Considerations) . Paliperidone has been detected in plasma in adult subjects up to 176 days after a single-dose administration of ERZOFRI [see Clinical Pharmacology (12.3)], and the clinical significance on the breastfed infant is not known. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for ERZOFRI and any potential adverse effects on the breastfed child from ERZOFRI or from the mother's underlying condition.
8.3 Females and Males of Reproductive Potential
Infertility
Females
Based on the pharmacologic action of paliperidone (D 2receptor antagonism), treatment with ERZOFRI may result in an increase in serum prolactin levels, which may lead to a reversible reduction in fertility in females of reproductive potential [see Warnings and Precautions (5.10)].
8.4 Pediatric Use
Safety and effectiveness of ERZOFRI in pediatric patients have not been established.
Juvenile Animal Toxicity Data
In a study in which juvenile rats were treated with oral paliperidone from Days 24 to 73 of age, a reversible impairment of performance in a test of learning and memory was seen, in females only, with a no-effect dose of 0.63 mg/kg/day, which produced plasma levels (AUC) of paliperidone similar to those in adolescents dosed at a 12 mg/day oral dose. No other consistent effects on neurobehavioral or reproductive development were seen up to the highest dose tested (2.5 mg/kg/day), which produced plasma levels of paliperidone 2-3 times those in adolescents.
Juvenile dogs were treated for 40 weeks with oral risperidone, which is extensively metabolized to paliperidone in animals and humans, at doses of 0.31, 1.25, or 5 mg/kg/day. Decreased bone length and density were seen with a no-effect dose of 0.31 mg/kg/day, which produced plasma levels (AUC) of risperidone plus paliperidone, which were similar to those in children and adolescents receiving the MRHD of oral risperidone. In addition, a delay in sexual maturation was seen at all doses in both males and females. The above effects showed little or no reversibility in females after a 12-week drug-free recovery period.
The long-term effects of ERZOFRI on growth and sexual maturation have not been fully evaluated in pediatric patients.
8.5 Geriatric Use
Clinical studies of ERZOFRI did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients.
Paliperidone palmitate is substantially excreted by the kidney and clearance is decreased in patients with renal impairment [see Clinical Pharmacology (12.3)] , who should be given reduced doses. Because geriatric patients are more likely to have decreased renal function, adjust dose based on renal function [see Dosage and Administration (2.4)].
8.6 Renal Impairment
Use of ERZOFRI is not recommended in patients with moderate or severe renal impairment (creatinine clearance < 50 mL/min). Dose reduction is recommended for patients with mild renal impairment (creatinine clearance ≥ 50 mL/min to < 80 mL/min) [see Dosage and Administration (2.4)and Clinical Pharmacology (12.3)] .
8.7 Hepatic Impairment
ERZOFRI has not been studied in patients with hepatic impairment. Based on a study with oral paliperidone, no dose adjustment is required in patients with mild or moderate hepatic impairment. Paliperidone has not been studied in patients with severe hepatic impairment [see Clinical Pharmacology (12.3)] .
8.8 Patients with Parkinson's Disease or Lewy Body Dementia
Patients with Parkinson's Disease or Dementia with Lewy Bodies can experience increased sensitivity to ERZOFRI. Manifestations can include confusion, obtundation, postural instability with frequent falls, extrapyramidal symptoms, and clinical features consistent with neuroleptic malignant syndrome.
-
10 OVERDOSAGE
Human Experience
While experience with paliperidone overdose is limited, among the few cases of overdose reported in premarketing trials with oral paliperidone, the highest estimated ingestion was 405 mg. Observed signs and symptoms included extrapyramidal symptoms and gait unsteadiness. Other potential signs and symptoms include those resulting from an exaggeration of paliperidone's known pharmacological effects, i.e., drowsiness and sedation, tachycardia and hypotension, and QT prolongation. Torsades de pointes and ventricular fibrillation have been reported in a patient in the setting of overdose with oral paliperidone.
Paliperidone is the major active metabolite of risperidone. Refer to the OVERDOSAGE section of the risperidone prescribing information for overdose experience with risperidone.
Management of Overdosage
There is no specific antidote to paliperidone. Provide supportive care, including close medical supervision and monitoring. Treatment should consist of general measures employed in the management of overdosage with any drug. Consider the possibility of multiple drug overdosage. Ensure an adequate airway, oxygenation, and ventilation. Monitor cardiac rhythm and vital signs. Use supportive and symptomatic measures.
Consider the pharmacokinetic profile of ERZOFRI and the half-life of paliperidone when assessing treatment needs and recovery.
Consider contacting the Poison Help Line (1-800-222-1222) or medical toxicologist for additional overdosage management recommendations.
-
11 DESCRIPTION
ERZOFRI (paliperidone palmitate) extended-release injectable suspension contains a racemic mixture of (+)- and (-)- paliperidone palmitate. Paliperidone palmitate, is an atypical antipsychotic belonging to the chemical class of benzisoxazole derivatives. The chemical name is (9 RS)-3-[2-[4-(6-Fluoro-1,2-benzisoxazol-3-yl)piperidin-1-yl]ethyl]-2-methyl-4-oxo-6,7,8,9-tetrahydro-4 H-pyrido[1,2- a]pyrimadin-9-yl hexadecanoate. Its molecular formula is C 39H 57FN 4O 4and its molecular weight is 664.89. The structural formula is:
Paliperidone palmitate is very slightly soluble in ethanol and methanol, practically insoluble in water, and slightly soluble in ethyl acetate.
ERZOFRI is available as a white to off-white sterile aqueous extended-release suspension for intramuscular injection in the following dose strengths of paliperidone palmitate (deliverable volume) in single-dose prefilled syringes: 39 mg (0.25 mL), 78 mg (0.5 mL), 117 mg (0.75 mL), 156 mg (1 mL), 234 mg (1.5 mL), and 351 mg (2.25 mL). The drug product hydrolyzes in vivo to the active moiety, paliperidone, resulting in dose strengths of 25 mg, 50 mg, 75 mg, 100 mg, 150 mg, and 225 mg of paliperidone, respectively.
The inactive ingredients are citric acid monohydrate (5 mg/mL), dibasic sodium phosphate anhydrous (5 mg/mL), monobasic sodium phosphate monohydrate (2.5 mg/mL), polyethylene glycol 4000 (30 mg/mL), polysorbate 20 (12 mg/mL), sodium hydroxide to adjust pH, and water for injection. The drug product pH is 6.5 to 7.5.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Paliperidone palmitate is hydrolyzed to paliperidone [see Clinical Pharmacology (12.3)] . Paliperidone is the major active metabolite of risperidone. The mechanism of action of paliperidone in the listed indications is unclear. However, the drug's effect in schizophrenia could be mediated through a combination of central dopamine Type 2 (D 2)and serotonin Type 2 (5HT 2A) receptor antagonism.
12.2 Pharmacodynamics
Paliperidone is an antagonist at the central dopamine Type 2 (D 2) and serotonin Type 2 (5HT 2A) receptors with binding affinities (Ki values) of 1.6-2.8 nM for D 2and 0.8-1.2 nM for 5HT 2Areceptors. Paliperidone also acts as an antagonist at the α 1and α 2adrenergic receptors and H 1histaminergic receptors. Paliperidone has no affinity for cholinergic muscarinic or β 1- and β 2-adrenergic receptors. The pharmacological activity of the (+)- and (-)- paliperidone enantiomers is qualitatively and quantitatively similar .
12.3 Pharmacokinetics
The overall exposures (AUC) of paliperidone following another once-a-month paliperidone palmitate extended-release injectable suspension (also referred to as "PP1M" in this section) administration was dose-proportional over a dose range of 39 mg to 234 mg, and peak plasma concentrations (C max) were less than dose-proportional for doses exceeding 78 mg. Steady state plasma exposures of ERZOFRI are reached 7 days after the first injection.
Absorption
After intramuscular injection, paliperidone palmitate is hydrolyzed to paliperidone and absorbed into the systemic circulation. Following a single intramuscular dose of ERZOFRI, the plasma concentrations of paliperidone gradually rise to reach maximum plasma concentrations at a median T maxof 16 to 28 days. The release of the drug starts as early as day 1 and lasts for as long as 176 days.
Following multiple intramuscular injections of ERZOFRI (351 mg on day 1 and 156 mg on day 29 and every 28 days for a total of 6 consecutive injections) in patients, the geometric least square mean C max, trough plasma concentrations (C trough) and average plasma concentrations (C avg) were 43.7 ng/mL, 28.5 ng/mL and 30.3 ng/mL, respectively, during the initial regimen period; at steady state, C max-ss, C trough,ssand AUC tau-sswere 42.6 ng/mL, 28.3 ng/mL and 909 ng*hr/mL, respectively.
Following multiple intramuscular injections of another PP1M (234 mg on day 1 and 156 mg on day 8 and every 28 days for a total of 7 consecutive injections), the geometric least square mean C max, C troughand C avgwere 58.7 ng/mL, 30.1 ng/mL and 37.8 ng/mL, respectively, during the initial regimen period; at steady state, C max-ss, C trough,ssand AUC tau-ssof another once-a-month paliperidone palmitate extended-release injectable suspension for paliperidone were 43.8 ng/mL, 30.4 ng/mL and 953 ng*hr/mL, respectively.
Following intramuscular injection of a single dose of ERZOFRI 156 mg in the deltoid muscle, the geometric mean C maxwas approximately 43% higher compared with injections of 156 mg in the gluteal muscle. Following intramuscular injection of a single dose of ERZOFRI 351 mg in the deltoid muscle, the geometric mean C maxwas approximately 21% higher compared with injections of 351 mg in the gluteal muscle. Over the dose range of 39 mg to 234 mg, the AUC infafter a single dose injection in the deltoid muscle was comparable to the AUC infafter a single dose injection in the gluteal muscle.
Following intramuscular injection of single doses (39 mg to 234 mg) of another PP1M in the deltoid muscle, on average, a 28% higher C maxwas observed compared with injection in the gluteal muscle. The mean steady-state peak:trough ratio for PP1M dose of 156 mg was 1.8 following gluteal administration and 2.2 following deltoid administration.
Following administration of paliperidone palmitate, the (+) and (-) enantiomers of paliperidone interconvert, reaching an AUC (+) to (-) ratio of approximately 1.6 to 1.8.
Distribution
Based on a population analysis of data from ERZOFRI clinical trials, the apparent volume of distribution of paliperidone is 2840 L.
The plasma protein binding of racemic paliperidone is 74%.
Elimination
Metabolism
Four metabolic pathways have been identified in vivo, none of which accounted for more than 10% of the dose: dealkylation, hydroxylation, dehydrogenation, and benzisoxazole scission. Although in vitrostudies suggested a role for CYP2D6 and CYP3A4 in the metabolism of paliperidone, there is no evidence in vivothat these isozymes play a significant role in the metabolism of paliperidone. Population pharmacokinetics analyses indicated no discernible difference on the apparent clearance of paliperidone after administration of oral paliperidone between extensive metabolizers and poor metabolizers of CYP2D6 substrates.
The median apparent half-life of paliperidone following ERZOFRI single-dose administration at 156 mg is approximately 27 days.
Excretion
In a study with oral immediate-release 14C-paliperidone, one week following administration of a single oral dose of 1 mg immediate-release 14C-paliperidone, 59% of the dose was excreted unchanged into urine, indicating that paliperidone is not extensively metabolized in the liver. Approximately 80% of the administered radioactivity was recovered in urine and 11% in the feces.
Drug Interaction Studies
No specific drug interaction studies have been performed with ERZOFRI. The information below is obtained from studies with oral paliperidone.
Effects of other drugs on the exposures of paliperidone are summarized in Figure 1. After oral administration of 20 mg/day of paroxetine (a potent CYP2D6 inhibitor), an increase in mean C maxand AUC values at steady-state was observed (see Figure 1). Higher doses of paroxetine have not been studied. The clinical relevance is unknown. After oral administration, a decrease in mean C maxand AUC values at steady state is expected when patients are treated with carbamazepine, a strong inducer of both CYP3A4 and P-gp [see Drug Interactions (7.1)] . This decrease is caused, to a substantial degree, by a 35% increase in renal clearance of paliperidone.
Figure 1: Effects of Other Drugs on Paliperidone Pharmacokinetics
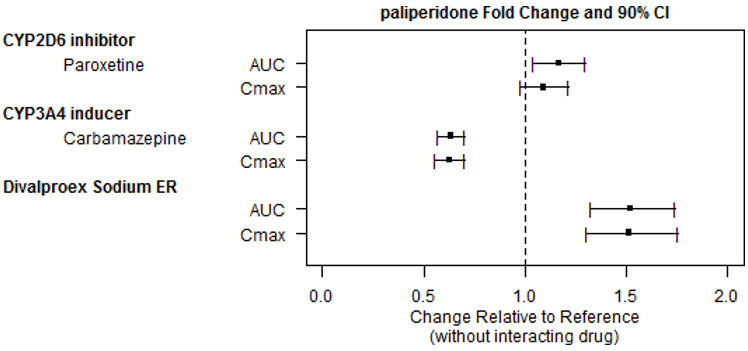
Clinically meaningful pharmacokinetic interaction between paliperidone and valproate (including valproic acid and divalproex sodium) is not expected. Oral administration of divalproex sodium extended-release tablets (two 500 mg tablets once daily at steady-state) with oral paliperidone extended-release tablets resulted in an increase of approximately 50% in the C maxand AUC of paliperidone.
After oral administration of paliperidone, the steady-state C maxand AUC of divalproex sodium extended-release tablets were not affected in 13 patients stabilized on divalproex sodium extended- release tablets. In a clinical study, subjects on stable doses of divalproex sodium extended-release tablets had comparable valproate average plasma concentrations when oral paliperidone extended- release tablets 3-15 mg/day was added to their existing divalproex sodium extended-release tablets treatment [see Drug Interactions (7.2)] .
In vitrostudies indicate that CYP2D6 and CYP3A4 may be involved in paliperidone metabolism, however, there is no evidence in vivothat inhibitors of these enzymes significantly affect the metabolism of paliperidone; they contribute to only a small fraction of total body clearance. In vitrostudies demonstrated that paliperidone is a substrate of P-glycoprotein (P-gp) [see Drug Interactions (7.2)] .
In vitrostudies in human liver microsomes demonstrated that paliperidone does not substantially inhibit the metabolism of drugs metabolized by cytochrome P450 isozymes, including CYP1A2, CYP2A6, CYP2C8/9/10, CYP2D6, CYP2E1, CYP3A4, and CYP3A5. Therefore, paliperidone is not expected to inhibit clearance of drugs that are metabolized by these metabolic pathways in a clinically relevant manner. Paliperidone is also not expected to have enzyme inducing properties.
Paliperidone is a weak inhibitor of P-gp at high concentrations. No in vivodata are available, and the clinical relevance is unknown.
Specific Populations
No pharmacokinetic studies have been performed with ERZOFRI in specific populations. The information is obtained from studies with oral paliperidone or is based on the population pharmacokinetic modeling of oral paliperidone and another PP1M. Exposures of paliperidone in specific populations (renal impairment, hepatic impairment and elderly) are summarized in Figure 2 [see Dosage and Administration (2.4)and Use in Specific Populations (8.6)] .
After oral administration of paliperidone in patients with moderate hepatic impairment, the plasma concentrations of free paliperidone were similar to those of healthy subjects, although total paliperidone exposure decreased because of a decrease in protein binding. Paliperidone has not been studied in patients with severe hepatic impairment [see Use in Specific Populations (8.7)] .
After oral administration of paliperidone in elderly subjects, the C maxand AUC increased 1.2-fold compared to young subjects. However, there may be age-related decreases in creatinine clearance [see Dosage and Administration (2.4)and Use in Specific Populations (8.5)] .
Figure 2 Effects of Intrinsic Factors on Paliperidone Pharmacokinetics
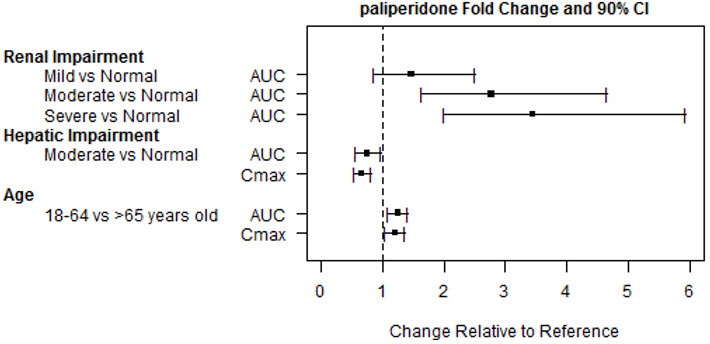
Based on in vitrostudies utilizing human liver enzymes, paliperidone is not a substrate for CYP1A2; smoking should, therefore, not have an effect on the pharmacokinetics of paliperidone.
Slower absorption was observed in females in a population pharmacokinetic analysis. At apparent steady-state with PP1M, the trough concentrations were similar between males and females.
Lower C maxwas observed in overweight and obese subjects. At apparent steady-state PP1M, the trough concentrations were similar among normal, overweight, and obese subjects.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
The carcinogenic potential of intramuscularly injected paliperidone palmitate was assessed in rats. There was an increase in mammary gland adenocarcinomas in female rats at 16, 47, and 94 mg/kg monthly injections, which are 0.6, 2, and 4 times, respectively, the MRHD of 234 mg of another once-a-month paliperidone palmitate extended-release injectable suspension based on body surface area (BSA). A no-effect dose was not established. Male rats showed an increase in mammary gland adenomas, fibroadenomas, and carcinomas at 2 and 4 times the MRHD based on BSA. A carcinogenicity study in mice has not been conducted with paliperidone palmitate.
Carcinogenicity studies with risperidone, which is extensively converted to paliperidone in rats, mice, and humans, were conducted in Swiss albino mice and Wistar rats. Risperidone was administered in the diet at daily doses of 0.63, 2.5, and 10 mg/kg for 18 months to mice and for 25 months to rats. A maximum tolerated dose was not achieved in male mice. There were statistically significant increases in pituitary gland adenomas, endocrine pancreas adenomas, and mammary gland adenocarcinomas. The no-effect dose for these tumors was less than or equal to the MRHD of risperidone based on BSA (see risperidone prescribing information). An increase in mammary, pituitary, and endocrine pancreas neoplasms has been found in rodents after chronic administration of other antipsychotic drugs and is considered to be mediated by prolonged dopamine D 2antagonism and hyperprolactinemia. The relevance of these tumor findings in rodents to human risk is unclear [see Warnings and Precautions (5.7)] .
Mutagenesis
Paliperidone palmitate was not genotoxic in the in vitroAmes bacterial reverse mutation test or the mouse lymphoma assay. Paliperidone was not genotoxic in the in vitroAmes bacterial reverse mutation test, the mouse lymphoma assay, or the in vivorat bone marrow micronucleus test.
Impairment of Fertility
No fertility studies were conducted with paliperidone palmitate.
Paliperidone did not affect fertility in treated female rats at oral doses of up to 2.5 mg/kg/day which is 2 times the MRHD based on BSA. However, pre- and post-implantation loss was increased, and the number of live embryos was slightly decreased, at 2.5 mg/kg, a dose that also caused slight maternal toxicity. These parameters were not affected at a dose of 0.63 mg/kg, which is half of the MRHD based on BSA.
Paliperidone did not affect fertility of treated male rats at oral doses of up to 2 times the MRHD of 12 mg/day based on BSA. However, studies to assess sperm count and sperm viability were not conducted with paliperidone. In a subchronic study in Beagle dogs with risperidone, which is extensively converted to paliperidone in dogs and humans, all doses tested (0.31 mg/kg - 5.0 mg/kg) resulted in decreases in serum testosterone and in sperm motility and concentration (0.6 to 10 times the MRHD of 16 mg/day for risperidone, based on BSA). Serum testosterone and sperm parameters partially recovered, and remained decreased after the last observation at two months after treatment was discontinued.
-
14 CLINICAL STUDIES
14.1 Schizophrenia
The efficacy of ERZOFRI for the treatment of schizophrenia in adults is based upon adequate and well-controlled studies of another once-a-month paliperidone palmitate extended-release injectable suspension (also referred to as "PP1M" in this section). The results of these adequate and well-controlled studies of another PP1M are presented below.
Short-Term Monotherapy (Studies 1, 2, 3, 4)
The efficacy of another PP1M in the acute treatment of schizophrenia was evaluated in four short-term (one 9-week and three 13-week) double-blind, randomized, placebo-controlled, fixed-dose studies of acutely relapsed adult inpatients who met DSM-IV criteria for schizophrenia. The fixed doses of PP1M in these studies were given on days 1, 8, and 36 in the 9-week study, and additionally on Day 64 of the 13-week studies, i.e., at a weekly interval for the initial two doses and then every 4 weeks for maintenance.
Efficacy was evaluated using the total score on the Positive and Negative Syndrome Scale (PANSS). The PANSS is a 30-item scale that measures positive symptoms of schizophrenia (7 items), negative symptoms of schizophrenia (7 items), and general psychopathology (16 items), each rated on a scale of 1 (absent) to 7 (extreme); total PANSS scores range from 30 to 210.
In Study 1 (PSY-3007), a 13-week study (n=636) comparing three fixed doses of PP1M (initial deltoid injection of 234 mg followed by 3 gluteal or deltoid doses of either 39 mg/4 weeks, 156 mg/4 weeks or 234 mg/4 weeks) to placebo, all three doses of PP1M were superior to placebo in improving the PANSS total score.
In Study 2 (PSY-3003), another 13-week study (n=349) comparing three fixed doses of PP1M (78 mg/4 weeks, 156 mg/4 weeks, and 234 mg/4 weeks) to placebo, only 156 mg/4 weeks of PP1M was superior to placebo in improving the PANSS total score.
In Study 3 (PSY-3004), a third 13-week study (n=513) comparing three fixed doses of PP1M (39 mg/4 weeks, 78 mg/4 weeks, and 156 mg/4 weeks) to placebo, all three doses of PP1M were superior to placebo in improving the PANSS total score.
In Study 4 (SCH-201), the 9-week study (n=197) comparing two fixed doses of PP1M (78 mg/4 weeks and 156 mg/4 weeks) to placebo, both doses of PP1M were superior to placebo in improving PANSS total score.
A summary of the mean baseline PANSS scores along with the mean changes from baseline in the four short-term acute schizophrenia studies are provided in Table 13.
Table 13: Schizophrenia Short-term Studies Study Number Treatment Group Primary Efficacy Measure: PANSS Total Score Mean Baseline Score (SD) LS Mean Change from Baseline (SE) Placebo-subtracted Difference *
(95% CI)SD: standard deviation; SE: standard error; LS Mean: least-squares mean; CI: unadjusted confidence interval. - * Difference (drug minus placebo) in least-squares mean change from baseline.
- † p<0.05 (Doses statistically significantly superior to placebo).
- ‡ Because an insufficient number of subjects received the 234 mg/4 weeks dose, results from this group are not included.
Study 1 Once-a-Month Paliperidone Palmitate Extended-Release Injectable Suspension (39 mg/4 weeks) † 86.9 (11.99) -11.2 (1.69) -5.1 (-9.01, -1.10) Once-a-Month Paliperidone Palmitate Extended-Release Injectable Suspension (156 mg/4 weeks) † 86.2 (10.77) -14.8 (1.68) -8.7 (-12.62, -4.78) Once-a-Month Paliperidone Palmitate Extended-Release Injectable Suspension (234 mg/4 weeks) † 88.4 (11.70) -15.9 (1.70) -9.8 (-13.71, -5.85) Placebo 86.8 (10.31) -6.1 (1.69) -- Study 2‡ Once-a-Month Paliperidone Palmitate Extended-Release Injectable Suspension (78 mg/4 weeks) 89.9 (10.78) -6.9 (2.50) -3.5 (-8.73, 1.77) Once-a-Month Paliperidone Palmitate Extended-Release Injectable Suspension (156 mg/4 weeks) † 90.1 (11.66) -10.4 (2.47) -6.9 (-12.12, -1.68) Placebo 92.4 (12.55) -3.5 (2.15) -- Study 3 Once-a-Month Paliperidone Palmitate Extended-Release Injectable Suspension (39 mg/4 weeks) † 90.7 (12.25) -19.8 (2.19) -6.6 (-11.40, -1.73) Once-a-Month Paliperidone Palmitate Extended-Release Injectable Suspension (78 mg/4 weeks) † 91.2 (12.02) -19.2 (2.19) -5.9 (-10.76, -1.07) Once-a-Month Paliperidone Palmitate Extended-Release Injectable Suspension (156 mg/4 weeks) † 90.8 (11.70) -22.5 (2.18) -9.2 (-14.07, -4.43) Placebo 90.7 (12.22) -13.3 (2.21) -- Study 4 Once-a-Month Paliperidone Palmitate Extended-Release Injectable Suspension (78 mg/4 weeks) † 88.0 (12.39) -4.6 (2.43) -11.2 (-16.85, -5.57) Once-a-Month Paliperidone Palmitate Extended-Release Injectable Suspension (156 mg/4 weeks) † 85.2 (11.09) -7.4 (2.45) -14.0 (-19.51, -8.58) Placebo 87.8 (13.90) 6.6 (2.45) -- Maintenance Monotherapy Treatment (Study 5: PSY-3001)
The efficacy of another PP1M in maintaining symptomatic control in schizophrenia was established in a longer-term double-blind, placebo-controlled, flexible-dose study involving adult subjects who met DSM-IV criteria for schizophrenia. This study included a minimum 12-week, fixed-dose stabilization phase, and a randomized, placebo-controlled phase to observe for relapse. During the double-blind phase, patients were randomized to either the same dose of PP1M they received during the stabilization phase, i.e., 39 mg, 78 mg, or 156 mg administered every 4 weeks, or to placebo. A total of 410 stabilized patients were randomized to either PP1M or to placebo until they experienced a relapse of schizophrenia symptoms. Relapse was pre-defined as time to first emergence of one or more of the following: psychiatric hospitalization, ≥ 25% increase (if the baseline score was > 40) or a 10-point increase (if the baseline score was ≤ 40) in total PANSS score on two consecutive assessments, deliberate self-injury, violent behavior, suicidal/homicidal ideation, or a score of ≥ 5 (if the maximum baseline score was ≤ 3) or ≥ 6 (if the maximum baseline score was 4) on two consecutive assessments of the specific PANSS items. The primary efficacy variable was time to relapse. A pre-planned interim analysis showed a statistically significantly longer time to relapse in patients treated with PP1M compared to placebo, and the study was stopped early because maintenance of efficacy was demonstrated. Thirty-four percent (34%) of subjects in the placebo group and 10% of subjects in the PP1M group experienced a relapse event. There was a statistically significant difference between the treatment groups in favor of PP1M. A Kaplan-Meier plot of time to relapse by treatment group is shown in Figure 3. The time to relapse for subjects in the placebo group was statistically significantly shorter than for the PP1M group. An examination of population subgroups did not reveal any clinically significant differences in responsiveness on the basis of gender, age, or race.
Figure 3: Kaplan-Meier Plot of Cumulative Proportion of Subjects with Relapse Over Time (Schizophrenia Study 5)
* median time to relapse for placebo group is 163 days 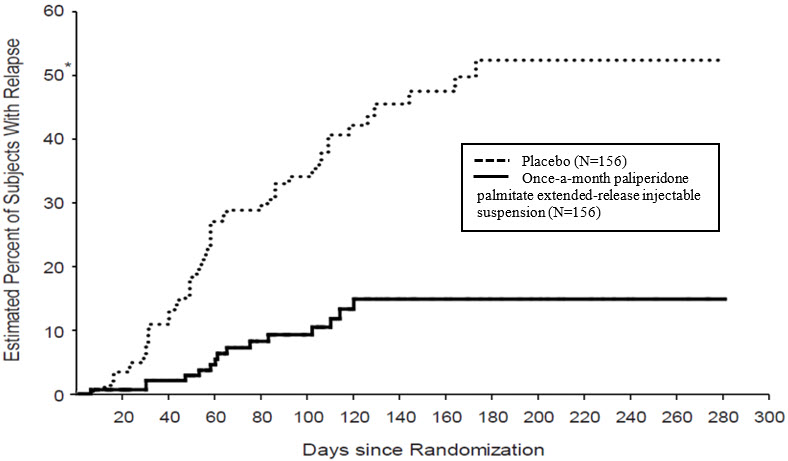
Long-Term Comparative Monotherapy Treatment versus Oral Antipsychotic Therapy (Study 6: SCH-3006)
The efficacy of another PP1M in delaying time to treatment failure compared with selected oral antipsychotic medications was established in a long-term, randomized, flexible-dose study in subjects with schizophrenia and a history of incarceration. Subjects were screened for up to 14 days followed by a 15-month treatment phase during which they were observed for treatment failure.
The primary endpoint was time to first treatment failure. Treatment failure was defined as one of the following: arrest and/or incarceration; psychiatric hospitalization; discontinuation of antipsychotic treatment because of safety or tolerability; treatment supplementation with another antipsychotic because of inadequate efficacy; need for increase in level of psychiatric services to prevent an imminent psychiatric hospitalization; discontinuation of antipsychotic treatment because of inadequate efficacy; or suicide. Treatment failure was determined by an Event Monitoring Board (EMB) that was blinded to treatment assignment. A total of 444 subjects were randomly assigned to either PP1M (N = 226; median dose 156 mg) or one of up to seven pre-specified, flexibly-dosed, commonly prescribed oral antipsychotic medications (N = 218; aripiprazole, haloperidol, olanzapine, paliperidone, perphenazine, quetiapine, or risperidone). The selection of the oral antipsychotic medication was determined to be appropriate for the patient by the investigator. A statistically significantly longer time to first treatment failure was seen for PP1M compared with oral antipsychotic medications. The median time to treatment failure was 416 days and 226 days for PP1M and antipsychotic medications, respectively. A Kaplan-Meier plot of time to first treatment failure is shown in Figure 4. The frequencies of first treatment failure events by type are shown in Table 14. The time to first arrest and/or incarceration or psychiatric hospitalization was also statistically significantly longer for the PP1M group compared to the oral antipsychotic group.
Figure 4: Kaplan-Meier Plot of Time to First Treatment Failure in a Long-Term, Randomized, Flexible-Dose Study in Subjects with Schizophrenia and a History of Incarceration (Schizophrenia Study 6)
* Median time to first treatment failure: 416 days with once-a-month paliperidone palmitate extended-release injectable suspension; 226 days with oral antipsychotics 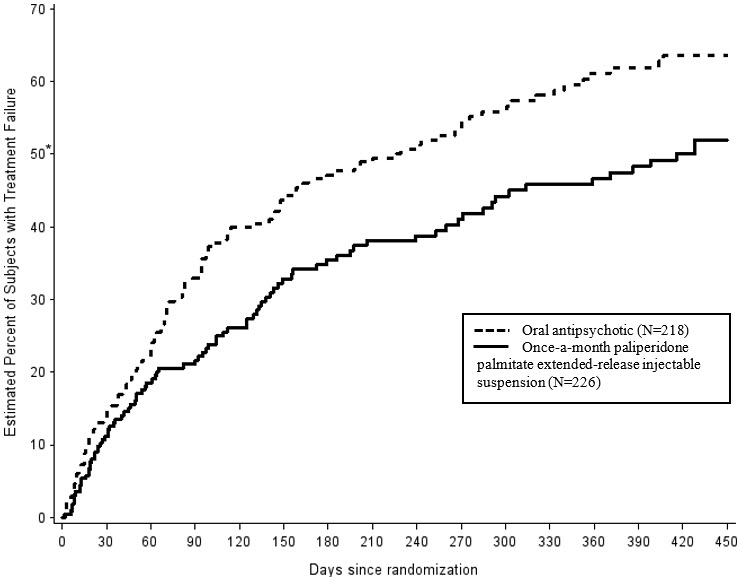
Table 14: Components of Composite Endpoint in a Long-Term, Randomized, Flexible-Dose Study in Subjects with Schizophrenia and a History of Incarceration (Schizophrenia Study 6) Event Type Once-a-Month Paliperidone Palmitate Extended-Release Injectable Suspension
N=226
frequency (%)Oral Antipsychotics
N=218
frequency (%)Hazard Ratio *
[95% CI]- * Hazard ratio of once-a-month paliperidone palmitate extended-release injectable suspension to Oral Antipsychotics based on Cox regression model for time-to-event analysis. Note that the hazard ratio did not appear constant throughout the trial.
- † Analysis results, which incorporated relevant events collected after discontinuation for those who discontinued, were consistent with the results from the pre-specified analysis of this secondary endpoint.
First Treatment Failures 90 (39.8%) 117 (53.7%) 0.70
[0.53, 0.92]First Treatment Failure Component Events - Arrest and/or incarceration
48 (21.2%) 64 (29.4%) - Psychiatric hospitalization
18 (8.0%) 26 (11.9%) - Discontinuation of antipsychotic treatment because of safety or tolerability
15 (6.6%) 8 (3.7%) - Treatment supplementation with another antipsychotic because of inadequate efficacy
5 (2.2%) 6 (2.8%) - Need for increase in level of psychiatric services to prevent an imminent psychiatric hospitalization
3 (1.3%) 4 (1.8%) - Discontinuation of antipsychotic treatment because of inadequate efficacy
1 (0.4%) 9 (4.1%) - Suicide
0 0 Arrest and/or Incarceration or Psychiatric Hospitalization Events, regardless of whether they were first events † 76 (33.6%) 98 (45.0%) 0.70
[0.52, 0.94]14.2 Schizoaffective Disorder
The efficacy of ERZOFRI for the treatment of schizoaffective disorder in adults as monotherapy and as an adjunct to mood stabilizers or antidepressants is based upon an adequate and well-controlled study of another PP1M. The results of the adequate and well-controlled study is presented below.
Maintenance Treatment – Monotherapy and as Adjunct to Mood Stabilizer or Antidepressant (SAff Study 1: SCA-3004)
The efficacy of PP1M in maintaining symptom control in schizoaffective disorder was established in a long-term double-blind, placebo-controlled, flexible-dose randomized-withdrawal study designed to delay relapse in adult subjects who met DSM-IV criteria for schizoaffective disorder, as confirmed by the Structured Clinical Interview for DSM-IV Disorders. The population included subjects with schizoaffective bipolar and depressive types. Subjects received PP1M either as monotherapy or as an adjunct to stable doses of antidepressant or mood stabilizers.
This study included a 13-week, open-label, flexible-dose (PP1M 78 mg, 117 mg, 156 mg, or 234 mg) lead-in period which enrolled a total of 667 subjects who had 1) acute exacerbation of psychotic symptoms; 2) score ≥4 on ≥3 PANSS items of delusions, conceptual disorganization, hallucinatory behavior, excitement, suspiciousness/persecution, hostility, uncooperativeness, tension, and poor impulse control; and 3) prominent mood symptoms ≥16 on the Young Mania Rating Scale (YMRS) and/or the Hamilton Rating Scale for Depression, 21-item version (HAM-D-21). Subjects were 19 to 66 years old (mean 39.5 years) and 53.5% were male. The mean scores at open-label enrollment of PANSS total was 85.8 (range 42 to 128), HAM-D- 21 was 20.4 (range 3 to 43), YMRS was 18.6 (range 0 to 50), and CGI-S-SCA was 4.4 (range 2 to 6).
After the 13-week open-label flexible-dose PP1M treatment, 432 subjects met stabilization criteria (PANSS total score ≤70, YMRS ≤12, and HAM-D-21 ≤12) and continued into the 12-week open-label fixed-dose stabilization period.
A total of 334 subjects who met stabilization criteria for 12 consecutive weeks were randomized (1:1) to continue the same dose of PP1M or to placebo in the 15-month, double- blind, maintenance period. For the 164 subjects who were randomized to PP1M, dose distribution was 78 mg (4.9%), 117 mg (9.8%), 156 mg (47.0%), and 234 mg (38.4%). The primary efficacy variable was time to relapse. Relapse was defined as the first occurrence of one or more of the following: 1) psychiatric hospitalization; 2) intervention employed to avert hospitalization; 3) clinically significant self-injury, suicidal or homicidal ideation or violent behavior; 4) a score of ≥6 (if the score was ≤4 at randomization) of any of the individual PANSS items: delusions, conceptual disorganization, hallucinatory behavior, excitement, suspiciousness/persecution, hostility, uncooperativeness, or poor impulse control; 5) on two consecutive assessments within 7 days: ≥ 25% increase (if the score at randomization was > 45) or ≥ 10-point increase (if the score at randomization was ≤ 45) in total PANSS score; a score of ≥ 5 (if the score was ≤ 3 at randomization) of any of the individual PANSS items: delusions, conceptual disorganization, hallucinatory behavior, excitement, suspiciousness/persecution, hostility, uncooperativeness, or poor impulse control; an increase of ≥ 2 points (if the score was 1 [not ill] to 3 [mildly ill] at randomization) or increase of ≥ 1 point (if the score was ≥ 4 [moderately ill or worse] at randomization) in CGI-S-SCA overall score.
There was a statistically significant difference in time to relapse between the treatment groups in favor of PP1M. A Kaplan-Meier plot of time to relapse by treatment group is shown in Figure 5.
Figure 5: Kaplan-Meier Plot of Cumulative Proportion of Subjects with Relapse Over Time (SAff Study 1)
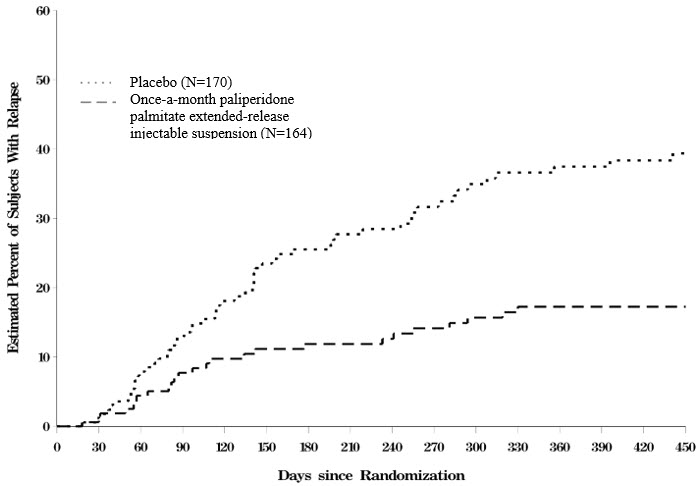
Table 15 summarizes the number of subjects with relapse in the overall population, by subgroup (monotherapy versus adjunctive therapy), and by symptom type at the first occurrence of relapse.
Table 15: Summary of Relapse Rates (SAff Study 1). Number (Percent) of Subjects Who Relapsed Placebo Once-a-Month Paliperidone Palmitate Extended-Release Injectable Suspension N=170 N=164 - * 8 subjects experienced a relapse without psychotic symptoms.
- † 16 subjects experienced a relapse without any mood symptoms.
All Subjects 57 (33.5%) 25 (15.2%) Monotherapy subset N=73
24 (32.9%)N=78
9 (11.5%)Adjunct to Antidepressants or Mood Stabilizer subset N=97
33 (34.0%)N=86
16 (18.6%)Psychotic Symptoms * 53 (31.2%) 21 (12.8%) Mood Symptoms † Any Mood Symptoms 48 (28.2%) 18 (11.0%) Manic 16 (9.4%) 5 (3.0%) Depressive 23 (13.5%) 8 (4.9%) Mixed 9 (5.3%) 5 (3.0%) -
16 HOW SUPPLIED/STORAGE AND HANDLING
How Supplied
ERZOFRI ®is provided as a single-use kit containing a single-dose prefilled syringe with a plunger stopper and tip cap. The kit also contains 2 safety needles (a 1 ½-inch 22 gauge safety needle and a 1-inch 23 gauge safety needle).
ERZOFRI is available as a white to off-white aqueous suspension in the following strengths:
39 mg/0.25 mL paliperidone palmitate kit (NDC: 72526-105-11) 78 mg/0.5 mL paliperidone palmitate kit (NDC: 72526-106-11) 117 mg/0.75 mL paliperidone palmitate kit (NDC: 72526-107-11) 156 mg/mL paliperidone palmitate kit (NDC: 72526-108-11) 234 mg/1.5 mL paliperidone palmitate kit (NDC: 72526-109-11) 351 mg/2.25 mL paliperidone palmitate kit (NDC: 72526-110-11) -
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient Information).
Neuroleptic Malignant Syndrome (NMS)
Counsel patients about a potentially fatal adverse reaction, Neuroleptic Malignant Syndrome (NMS), that has been reported in association with administration of antipsychotic drugs. Advise patients, family members, or caregivers to contact their healthcare provider or report to the emergency room if they experience signs and symptoms of NMS, including hyperpyrexia, muscle rigidity, altered mental status including delirium, and evidence of autonomic instability (irregular pulse or blood pressure, tachycardia, diaphoresis, and cardiac dysrhythmia) [see Warnings and Precautions (5.3)].
Tardive Dyskinesia
Counsel patients on the signs and symptoms of tardive dyskinesia and to contact their healthcare provider if these abnormal movements occur [see Warnings and Precautions (5.5)].
Metabolic Changes
Educate patients about the risk of metabolic changes, how to recognize symptoms of hyperglycemia and diabetes mellitus, and the need for specific monitoring, including blood glucose, lipids, and weight [see Warnings and Precautions (5.6)].
Orthostatic Hypotension
Educate patients about the risk of orthostatic hypotension and syncope, particularly at the time of initiating treatment, re-initiating treatment, or increasing the dose [see Warnings and Precautions (5.7)] .
Leukopenia/Neutropenia
Advise patients with a pre-existing low WBC or a history of drug-induced leukopenia/neutropenia that they should have their CBC monitored while taking ERZOFRI [see Warnings and Precautions (5.9)] .
Hyperprolactinemia
Counsel patients on signs and symptoms of hyperprolactinemia that may be associated with chronic use of ERZOFRI. Advise them to seek medical attention if they experience any of the following: amenorrhea or galactorrhea in females, erectile dysfunction or gynecomastia in males [see Warnings and Precautions (5.10)] .
Potential for Cognitive and Motor Impairment
As ERZOFRI has the potential to impair judgement, thinking or motor skills, caution patients about operating hazardous machinery, including motor vehicles, until they are reasonably certain that ERZOFRI therapy does not affect them adversely [see Warnings and Precautions (5.11)] .
Priapism
Advise patients of the possibility of painful or prolonged penile erections (priapism). Instruct the patient to seek immediate medical attention in the event of priapism [see Warnings and Precautions (5.14)] .
Heat Exposure and Dehydration
Counsel patients regarding appropriate care in avoiding overheating and dehydration [see Warnings and Precautions (5.15)] .
Concomitant Medication
Advise patients to inform their healthcare providers if they are taking, or plan to take any prescription or over-the-counter medications because there is a potential for clinically significant interactions [see Drug Interactions (7)] .
Alcohol
Advise patients to avoid alcohol during treatment with ERZOFRI [see Drug Interactions (7.1)] .
Pregnancy
Advise patients to notify their healthcare provider if they become pregnant or intend to become pregnant during treatment with ERZOFRI. Advise patients that ERZOFRI may cause extrapyramidal and/or withdrawal symptoms in a neonate. Advise patients that there is a pregnancy registry that monitors pregnancy outcomes in women exposed to ERZOFRI during pregnancy [see Use in Specific Populations (8.1)] .
Lactation
Advise breastfeeding women using ERZOFRI to monitor infants for somnolence, failure to thrive, jitteriness, and extrapyramidal symptoms (tremors and abnormal muscle movements) and to seek medical care if they notice these signs [see Use in Specific Populations (8.2)] .
Infertility
Advise females of reproductive potential that ERZOFRI may impair fertility due to an increase in serum prolactin levels. The effects on fertility are reversible [see Use in Specific Populations (8.3)].
-
SPL UNCLASSIFIED SECTION
ERZOFRI ®(paliperidone palmitate) extended-release injectable suspension
Product of China.
Manufactured by:
Shandong Luye Pharmaceutical Co., Ltd.
No.15 Chuangye Road
Yantai, Shandong Province, China 264003Manufactured for:
Luye Innomind Pharma Shijiazhuang Co., Ltd.
Shijiazhuang, Hebei Province, China 050000For patent information: www.luyeusa.com/patents
© 2024 Luye Innomind Pharma Shijiazhuang Co., Ltd.
-
PATIENT PACKAGE INSERT
PATIENT INFORMATION
ERZOFRI ®(er-ZOH-free)
(paliperidone palmitate)
extended-release injectable suspensionThis Patient Information has been approved by the U.S. Food and Drug Administration. Revised: 3/2025 What is the most important information I should know about ERZOFRI? ERZOFRI may cause serious side effects, including: - Increased risk of death in elderly people with dementia-related psychosis. ERZOFRI increases the risk of death in elderly people who have lost touch with reality (psychosis) due to confusion and memory loss (dementia).ERZOFRI is not for the treatment of people with dementia-related psychosis.
What is ERZOFRI? ERZOFRI is a prescription medicine given by injection by a healthcare provider and used to treat: - schizophrenia in adults
- schizoaffective disorder in adults either alone or with other medicines such as mood stabilizers or antidepressants
It is not known if ERZOFRI is safe and effective in children. Who should not receive ERZOFRI? Do not receive ERZOFRI if youare allergic to paliperidone, risperidone, or any of the ingredients in ERZOFRI. See the end of this Patient Information leaflet for a complete list of ingredients in ERZOFRI. Before receiving ERZOFRI, tell your healthcare provider about all your medical conditions, including if you: - have never taken paliperidone or risperidone before
- have had Neuroleptic Malignant Syndrome (NMS)
- have or had heart problems, including a heart attack, heart failure, abnormal heart rhythm, or long QT syndrome
- have or had low levels of potassium or magnesium in your blood
- have or had uncontrolled movements of your tongue, face, mouth, or jaw (tardive dyskinesia)
- have or had kidney or liver problems
- have or had high blood sugar, diabetes or have a family history of diabetes
- have or had high levels of total cholesterol, LDL cholesterol, or triglycerides, or low levels of HDL cholesterol
- have Parkinson's disease or a type of dementia called Lewy Body Dementia
- have or had problems with dizziness or fainting or are being treated for high blood pressure
- have or had a low white blood cell count
- have or had seizures or epilepsy
- are pregnant or plan to become pregnant. It is not known if ERZOFRI will harm your unborn baby.
- If you become pregnant during treatment with ERZOFRI, talk to your healthcare provider about registering with the National Pregnancy Registry for Atypical Antipsychotics. You can register by calling 1-866-961-2388 or visit http://womensmentalhealth.org/clinical-and-research-programs/pregnancyregistry/.
- Babies born to women who are treated with ERZOFRI during their third trimester of pregnancy may experience symptoms such as tremors, irritability, excessive sleepiness, eye twitching, muscle spasms, decreased appetite, difficulty breathing, or abnormal movement of arms and legs. Let your healthcare provider know if these symptoms occur.
- are breastfeeding or plan to breastfeed. ERZOFRI can pass into your breast milk.
- Talk to your healthcare provider about the best way to feed your baby if you receive ERZOFRI.
Tell your healthcare provider about all the medicines you take,including prescription and over-the-counter medicines, vitamins, and herbal supplements. ERZOFRI and certain other medicines may affect each other causing possible serious side effects or affect the way each other works. Know the medicines you take. Keep a list of them to show to your healthcare provider or pharmacist when you get a new medicine. How will I receive ERZOFRI? - Follow your ERZOFRI treatment schedule exactly as your healthcare provider tells you to.
- Your healthcare provider will tell you how much ERZOFRI you will receive and when you will receive it.
- ERZOFRI is given as an injection by your healthcare provider into the muscle (intramuscularly) of your arm or your buttocks 1 time every month. Your first ERZOFRI injection will be in your arm.
- If you miss a dose of ERZOFRI, call your healthcare provider right away to schedule your next injection.
What should I avoid while receiving ERZOFRI? - Do notdrive, operate heavy machinery, or do other dangerous activities until you know how ERZOFRI affects you. ERZOFRI may affect your ability to make decisions, think clearly, or react quickly.
- Avoid getting too hot or becoming dehydrated.
- Do not exercise too much.
- In hot weather, stay inside in a cool place if possible.
- Stay out of the sun.
- Do not wear too much clothing or heavy clothing.
- Drink plenty of water.
- Avoid alcohol during treatment with ERZOFRI.
What are the possible side effects of ERZOFRI? ERZOFRI may cause serious side effects, including: - See " What is the most important information I should know about ERZOFRI"
- Cardiovascular problems (including stroke) in elderly people with dementia-related psychosis that can lead to death.
- Neuroleptic Malignant Syndrome (NMS), a serious condition that can lead to death.Call your healthcare provider right away or go to your nearest emergency room right away if you get any of the following signs or symptoms:
- high fever
- stiff muscles
- confusion
- sweating
- changes in your breathing, pulse, heart rate, or blood pressure
-
Problems with your heartbeat.These heart problems can cause death. Call your healthcare provider right away if you get any of these symptoms:
- passing out or feeling like you will pass out
- dizziness
- feeling as if your heart is pounding or missing beats
- Uncontrolled body movements (tardive dyskinesia).ERZOFRI may cause movements that you cannot control in your face, tongue, or other body parts. Tardive dyskinesia may not go away, even if you stop taking ERZOFRI. Tardive dyskinesia may also start after you stop taking ERZOFRI.
-
Problems with your metabolism such as:
-
High blood sugar (hyperglycemia) and diabetes.Increases in blood sugar can happen in some people who are treated with ERZOFRI. Extremely high blood sugar can lead to coma or death. If you have diabetes or risk factors for diabetes such as being overweight, or a family history of diabetes, your healthcare provider should check your blood sugar before you start treatment and during your treatment with ERZOFRI.
Call your healthcare provider if you get any of these symptoms of high blood sugar during treatment with ERZOFRI:
-
High blood sugar (hyperglycemia) and diabetes.Increases in blood sugar can happen in some people who are treated with ERZOFRI. Extremely high blood sugar can lead to coma or death. If you have diabetes or risk factors for diabetes such as being overweight, or a family history of diabetes, your healthcare provider should check your blood sugar before you start treatment and during your treatment with ERZOFRI.
- feel very thirsty
- feel very hungry
- feel sick to your stomach
- need to urinate more than usual
- feel weak or tired
- feel confused, or your breath smells fruity
- Increased fat levels (cholesterol and triglycerides) in your blood.Your healthcare provider may check your cholesterol and triglyceride levels during treatment with ERZOFRI.
- Weight gain.You and your healthcare provider should check your weight regularly during treatment with ERZOFRI.
- Decreased blood pressure (orthostatic hypotension) and fainting.You may feel lightheaded or faint when you rise too quickly from a sitting or lying position.
- Falls.ERZOFRI may make you sleepy or dizzy, may cause a decrease in your blood pressure when changing position (orthostatic hypotension), and can slow your thinking and motor skills which may lead to falls that can cause fractures or other injuries.
- Low white blood cell counts.Your healthcare provider may do blood tests during treatment with ERZOFRI.
- Increased prolactin levels in your blood (hyperprolactinemia).ERZOFRI may cause a rise in the blood levels of a hormone called prolactin that may cause side effects including missed menstrual periods, a reversible reduction in fertility in females who are able to become pregnant, leakage of milk from the breasts, development of breasts in men, or problems with erection.
- Sleepiness, drowsiness, feeling tired, difficulty thinking and doing normal activities.See " What should I avoid while receiving ERZOFRI?"
- Seizures (convulsions).
- Difficulty swallowingthat can cause food or liquid to get into your lungs.
- Prolonged or painful erection lasting more than 4 hours (priapism).Call your healthcare provider or go to your nearest emergency room right away if you have an erection that lasts more than 4 hours.
- Problems with control of your body temperature so that you feel too warm.See " What should I avoid while receiving ERZOFRI?"
The most common side effects of ERZOFRI include: - injection site reactions
- sleepiness or drowsiness
- dizziness
- feeling restless or like you need to move
- abnormal muscle movements including tremor (shaking), shuffling, uncontrolled involuntary movements, and abnormal movements of your eyes
Tell your healthcare provider if you have any side effect that bothers you or does not go away. These are not all of the possible side effects of ERZOFRI. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. General information about the safe and effective use of ERZOFRI. Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. You can ask your pharmacist or healthcare provider for information about ERZOFRI that is written for health professionals. What are the ingredients in ERZOFRI? Active ingredient: paliperidone palmitate Inactive ingredients:citric acid monohydrate, dibasic sodium phosphate anhydrous, monobasic sodium phosphate monohydrate, polyethylene glycol 4000, polysorbate 20, sodium hydroxide, and water for injection. Manufactured by: Shandong Luye Pharmaceutical Co., Ltd., No.15 Chuangye Road, Yantai, Shandong Province, China 264003 Manufactured for: Luye Innomind Pharma Shijiazhuang Co., Ltd., Shijiazhuang, Hebei Province, China 050000
For more information call 1-800-548-9765. -
PRINCIPAL DISPLAY PANEL - 39 mg/0.25 mL Syringe Kit
NDC: 72526-105-11
Rx OnlyErzofri ®
(paliperidone palmitate)
extended-release injectable suspension39 mg/0.25 mL
For Single Use Only.
Use entire contents of syringe.FOR INTRAMUSCULAR INJECTION ONLY.
Shake before using. Each injection must be administered by a healthcare professional.
-
PRINCIPAL DISPLAY PANEL - 78 mg/0.5 mL Syringe Kit
NDC: 72526-106-11
Rx OnlyErzofri ®
(paliperidone palmitate)
extended-release injectable suspension78 mg/0.5 mL
For Single Use Only.
Use entire contents of syringe.FOR INTRAMUSCULAR INJECTION ONLY.
Shake before using. Each injection must be administered by a healthcare professional.
-
PRINCIPAL DISPLAY PANEL - 117 mg/0.75 mL Syringe Kit
NDC: 72526-107-11
Rx OnlyErzofri ®
(paliperidone palmitate)
extended-release injectable suspension117 mg/0.75 mL
For Single Use Only.
Use entire contents of syringe.FOR INTRAMUSCULAR INJECTION ONLY.
Shake before using. Each injection must be administered by a healthcare professional.
-
PRINCIPAL DISPLAY PANEL - 156 mg/mL Syringe Kit
NDC: 72526-108-11
Rx OnlyErzofri ®
(paliperidone palmitate)
extended-release injectable suspension156 mg/mL
For Single Use Only.
Use entire contents of syringe.FOR INTRAMUSCULAR INJECTION ONLY.
Shake before using. Each injection must be administered by a healthcare professional.
-
PRINCIPAL DISPLAY PANEL - 234 mg/1.5 mL Syringe Kit
NDC: 72526-109-11
Rx OnlyErzofri ®
(paliperidone palmitate)
extended-release injectable suspension234 mg/1.5 mL
For Single Use Only.
Use entire contents of syringe.FOR INTRAMUSCULAR INJECTION ONLY.
Shake before using. Each injection must be administered by a healthcare professional.
-
PRINCIPAL DISPLAY PANEL - 351 mg/2.25 mL Syringe Kit
NDC: 72526-110-11
Rx OnlyErzofri ®
(paliperidone palmitate)
extended-release injectable suspension351 mg/2.25 mL
For Single Use Only.
Use entire contents of syringe.FOR INTRAMUSCULAR INJECTION ONLY.
Shake before using. Each injection must be administered by a healthcare professional.
-
INGREDIENTS AND APPEARANCE
ERZOFRI EXTENDED-RELEASE
paliperidone palmitate injectionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 72526-105 Route of Administration INTRAMUSCULAR Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength PALIPERIDONE PALMITATE (UNII: R8P8USM8FR) (PALIPERIDONE - UNII:838F01T721) PALIPERIDONE PALMITATE 39 mg in 0.25 mL Inactive Ingredients Ingredient Name Strength CITRIC ACID MONOHYDRATE (UNII: 2968PHW8QP) POLYETHYLENE GLYCOL 4000 (UNII: 4R4HFI6D95) POLYSORBATE 20 (UNII: 7T1F30V5YH) SODIUM HYDROXIDE (UNII: 55X04QC32I) SODIUM PHOSPHATE, DIBASIC, ANHYDROUS (UNII: 22ADO53M6F) SODIUM PHOSPHATE, MONOBASIC, MONOHYDRATE (UNII: 593YOG76RN) WATER (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 72526-105-11 1 in 1 KIT 12/10/2024 1 0.25 mL in 1 SYRINGE, GLASS; Type 2: Prefilled Drug Delivery Device/System (syringe, patch, etc.) Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA216352 12/10/2024 ERZOFRI EXTENDED-RELEASE
paliperidone palmitate injectionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 72526-106 Route of Administration INTRAMUSCULAR Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength PALIPERIDONE PALMITATE (UNII: R8P8USM8FR) (PALIPERIDONE - UNII:838F01T721) PALIPERIDONE PALMITATE 78 mg in 0.5 mL Inactive Ingredients Ingredient Name Strength CITRIC ACID MONOHYDRATE (UNII: 2968PHW8QP) POLYETHYLENE GLYCOL 4000 (UNII: 4R4HFI6D95) POLYSORBATE 20 (UNII: 7T1F30V5YH) SODIUM HYDROXIDE (UNII: 55X04QC32I) SODIUM PHOSPHATE, DIBASIC, ANHYDROUS (UNII: 22ADO53M6F) SODIUM PHOSPHATE, MONOBASIC, MONOHYDRATE (UNII: 593YOG76RN) WATER (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 72526-106-11 1 in 1 KIT 12/10/2024 1 0.5 mL in 1 SYRINGE, GLASS; Type 2: Prefilled Drug Delivery Device/System (syringe, patch, etc.) Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA216352 12/10/2024 ERZOFRI EXTENDED-RELEASE
paliperidone palmitate injectionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 72526-107 Route of Administration INTRAMUSCULAR Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength PALIPERIDONE PALMITATE (UNII: R8P8USM8FR) (PALIPERIDONE - UNII:838F01T721) PALIPERIDONE PALMITATE 117 mg in 0.75 mL Inactive Ingredients Ingredient Name Strength CITRIC ACID MONOHYDRATE (UNII: 2968PHW8QP) POLYETHYLENE GLYCOL 4000 (UNII: 4R4HFI6D95) POLYSORBATE 20 (UNII: 7T1F30V5YH) SODIUM HYDROXIDE (UNII: 55X04QC32I) SODIUM PHOSPHATE, DIBASIC, ANHYDROUS (UNII: 22ADO53M6F) SODIUM PHOSPHATE, MONOBASIC, MONOHYDRATE (UNII: 593YOG76RN) WATER (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 72526-107-11 1 in 1 KIT 12/10/2024 1 0.75 mL in 1 SYRINGE, GLASS; Type 2: Prefilled Drug Delivery Device/System (syringe, patch, etc.) Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA216352 12/10/2024 ERZOFRI EXTENDED-RELEASE
paliperidone palmitate injectionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 72526-108 Route of Administration INTRAMUSCULAR Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength PALIPERIDONE PALMITATE (UNII: R8P8USM8FR) (PALIPERIDONE - UNII:838F01T721) PALIPERIDONE PALMITATE 156 mg in 1 mL Inactive Ingredients Ingredient Name Strength CITRIC ACID MONOHYDRATE (UNII: 2968PHW8QP) POLYETHYLENE GLYCOL 4000 (UNII: 4R4HFI6D95) POLYSORBATE 20 (UNII: 7T1F30V5YH) SODIUM HYDROXIDE (UNII: 55X04QC32I) SODIUM PHOSPHATE, DIBASIC, ANHYDROUS (UNII: 22ADO53M6F) SODIUM PHOSPHATE, MONOBASIC, MONOHYDRATE (UNII: 593YOG76RN) WATER (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 72526-108-11 1 in 1 KIT 12/10/2024 1 1 mL in 1 SYRINGE, GLASS; Type 2: Prefilled Drug Delivery Device/System (syringe, patch, etc.) Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA216352 12/10/2024 ERZOFRI EXTENDED-RELEASE
paliperidone palmitate injectionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 72526-109 Route of Administration INTRAMUSCULAR Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength PALIPERIDONE PALMITATE (UNII: R8P8USM8FR) (PALIPERIDONE - UNII:838F01T721) PALIPERIDONE PALMITATE 234 mg in 1.5 mL Inactive Ingredients Ingredient Name Strength CITRIC ACID MONOHYDRATE (UNII: 2968PHW8QP) POLYETHYLENE GLYCOL 4000 (UNII: 4R4HFI6D95) POLYSORBATE 20 (UNII: 7T1F30V5YH) SODIUM HYDROXIDE (UNII: 55X04QC32I) SODIUM PHOSPHATE, DIBASIC, ANHYDROUS (UNII: 22ADO53M6F) SODIUM PHOSPHATE, MONOBASIC, MONOHYDRATE (UNII: 593YOG76RN) WATER (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 72526-109-11 1 in 1 KIT 12/10/2024 1 1.5 mL in 1 SYRINGE, GLASS; Type 2: Prefilled Drug Delivery Device/System (syringe, patch, etc.) Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA216352 12/10/2024 ERZOFRI EXTENDED-RELEASE
paliperidone palmitate injectionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 72526-110 Route of Administration INTRAMUSCULAR Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength PALIPERIDONE PALMITATE (UNII: R8P8USM8FR) (PALIPERIDONE - UNII:838F01T721) PALIPERIDONE PALMITATE 351 mg in 2.25 mL Inactive Ingredients Ingredient Name Strength CITRIC ACID MONOHYDRATE (UNII: 2968PHW8QP) POLYETHYLENE GLYCOL 4000 (UNII: 4R4HFI6D95) POLYSORBATE 20 (UNII: 7T1F30V5YH) SODIUM HYDROXIDE (UNII: 55X04QC32I) SODIUM PHOSPHATE, DIBASIC, ANHYDROUS (UNII: 22ADO53M6F) SODIUM PHOSPHATE, MONOBASIC, MONOHYDRATE (UNII: 593YOG76RN) WATER (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 72526-110-11 1 in 1 KIT 12/10/2024 1 2.25 mL in 1 SYRINGE, GLASS; Type 2: Prefilled Drug Delivery Device/System (syringe, patch, etc.) 2 NDC: 72526-110-21 1 in 1 KIT 03/20/2025 2 2.25 mL in 1 SYRINGE, GLASS; Type 2: Prefilled Drug Delivery Device/System (syringe, patch, etc.) Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA216352 12/10/2024 Labeler - Shandong Luye Pharmaceutical Co., Ltd. (544705452) Establishment Name Address ID/FEI Business Operations Shandong Luye Pharmaceutical Co., Ltd. 544705452 manufacture(72526-105, 72526-106, 72526-107, 72526-108, 72526-109, 72526-110) , analysis(72526-105, 72526-106, 72526-107, 72526-108, 72526-109, 72526-110) , pack(72526-105, 72526-106, 72526-107, 72526-108, 72526-109, 72526-110) , label(72526-105, 72526-106, 72526-107, 72526-108, 72526-109, 72526-110) Establishment Name Address ID/FEI Business Operations Interquim, S.A. 460009442 api manufacture(72526-105, 72526-106, 72526-107, 72526-108, 72526-109, 72526-110) Establishment Name Address ID/FEI Business Operations Curia Spain, S.A.U. 563371111 api manufacture(72526-105, 72526-106, 72526-107, 72526-108, 72526-109, 72526-110) , particle size reduction(72526-105, 72526-106, 72526-107, 72526-108, 72526-109, 72526-110) , analysis(72526-105, 72526-106, 72526-107, 72526-108, 72526-109, 72526-110)
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.