LANSOPRAZOLE capsule, delayed release pellets
lansoprazole by
Drug Labeling and Warnings
lansoprazole by is a Prescription medication manufactured, distributed, or labeled by NuCare Pharmaceuticals, Inc.. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use LANSOPRAZOLE DELAYED-RELEASE CAPSULES safely and effectively. See full prescribing information for LANSOPRAZOLE DELAYED-RELEASE CAPSULES.
LANSOPRAZOLE delayed-release capsules, for oral use
Initial U.S. Approval: 1995INDICATIONS AND USAGE
Lansoprazole delayed-release capsules are a proton pump inhibitor (PPI) indicated for:
- Short-Term Treatment of Active Duodenal Ulcer ( 1.1)
- H. pylori Eradication to Reduce the Risk of Duodenal Ulcer Recurrence ( 1.2)
- Maintenance of Healed Duodenal Ulcers ( 1.3)
- Short-Term Treatment of Active Benign Gastric Ulcer ( 1.4)
- Healing of nonsteroidal anti-inflammatory drugs (NSAID)-Associated Gastric Ulcer ( 1.5)
- Risk Reduction of NSAID-Associated Gastric Ulcer ( 1.6)
- Gastroesophageal Reflux Disease (GERD) ( 1.7)
- Maintenance of Healing of Erosive Esophagitis (EE) ( 1.8)
- Pathological Hypersecretory Conditions Including Zollinger-Ellison Syndrome (ZES) ( 1.9)
DOSAGE AND ADMINISTRATION
Indication
Dose
Frequency
- * Studied for 12 months
Duodenal Ulcers ( 1.1, 1.3)
Short-Term Treatment
15 mg
Once daily for 4 wks
Maintenance of Healed
15 mg
Once daily
H. pylori Eradication to Reduce Recurrence of Duodenal Ulcer ( 1.2)
Triple Therapy:
Lansoprazole
Amoxicillin
Clarithromycin
30 mg
1 gram
500 mg
Twice daily for 10 or 14 days
Dual Therapy:
Lansoprazole
Amoxicillin
30 mg
1 gram
Three times daily for 14 days
Benign Gastric Ulcer ( 1.4) Short-Term Treatment 30 mg
Once daily up to 8 wks
NSAID-associated Gastric Ulcer ( 1.6)
Healing
Risk Reduction
30 mg
15 mg
Once daily for 8 wks
Once daily up to 12 wks
GERD ( 1.7)
Short-Term Treatment of Symptomatic GERD
15 mg
Once daily up to 8 wks
Short-Term Treatment of EE
30 mg
Once daily up to 8 wks
Pediatric ( 8.4)
(1 to 11 years of age) Short-Term Treatment of Symptomatic GERD and Short-Term Treatment of EE
≤ 30 kg
15 mg
Once daily up to 12 wks
> 30 kg
30 mg
Once daily up to 12 wks
(12 to 17 years of age) Short-Term Treatment of Symptomatic GERD
Nonerosive GERD
15 mg
Once daily up to 8 wks
EE
30 mg
Once daily up to 8 wks
Maintenance of Healing of EE ( 1.8)* 15 mg
Once daily *
Pathological Hypersecretory Conditions (i.e., ZES) ( 1.9) 60 mg
Once daily
DOSAGE FORMS AND STRENGTHS
Capsules: 15 mg and 30 mg. ( 3)
CONTRAINDICATIONS
Contraindicated in patients with known severe hypersensitivity to any component of the lansoprazole formulation. ( 4)
WARNINGS AND PRECAUTIONS
Gastric Malignancy: In adults, symptomatic response with lansoprazole does not preclude the presence of gastric malignancy. Consider additional follow-up and diagnostic testing ( 5.1)
Acute Interstitial Nephritis: Acute interstitial nephritis has been observed in patients taking PPIs. ( 5.2)
Clostridium difficile- Associated Diarrhea: PPI therapy may be associated with increased risk of Clostridium difficile associated diarrhea. ( 5.3)
Bone Fracture: Long-term and multiple daily dose PPI therapy may be associated with an increased risk for osteoporosis-related fractures of the hip, wrist or spine. ( 5.4)
- Cutaneous and Systemic Lupus Erythematosus: Mostly cutaneous; new onset or exacerbation of existing disease; discontinue lansoprazole and refer to specialist for evaluation. ( 5.5)
- Cyanocobalamin (Vitamin B-12) Deficiency: Daily long-term use (e.g., longer than 3 years) may lead to malabsorption or a deficiency of cyanocobalamin. ( 5.6)
- Hypomagnesemia: Hypomagnesemia has been reported rarely with prolonged treatment with PPIs. ( 5.7)
ADVERSE REACTIONS
Most commonly reported adverse reactions (≥ 1%): diarrhea, abdominal pain, nausea and constipation. ( 6)
To report SUSPECTED ADVERSE REACTIONS, contact Zydus Pharmaceuticals USA Inc. at 1-877-993-8779 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
- Atazanavir and Nelfinavir: Do not coadminister with lansoprazole because atazanavir and nelfinavir systemic concentrations may be substantially decreased. ( 7.1)
- Drugs with pH-Dependent Absorption: May interfere with the absorption of drugs where gastric pH is important for bioavailability (e.g. ampicillin esters, digoxin, iron salts, erlotinib, ketoconazole, atazanavir, nelfinavir, and mycophenolate mofetil). ( 7.1)
- Warfarin: Concomitant warfarin use may require monitoring for increases in INR and prothrombin time. ( 7.2)
- Tacrolimus: Concomitant tacrolimus use may increase tacrolimus whole blood concentrations. ( 7.3)
- Theophylline: Titration of theophylline dosage may be required when concomitant lansoprazole use is started or stopped. ( 7.4)
- Methotrexate: Lansoprazole may increase serum levels of methotrexate. ( 7.6)
USE IN SPECIFIC POPULATIONS
See 17 for Medication Guide.
Revised: 11/2016
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
RECENT MAJOR CHANGES
1 INDICATIONS AND USAGE
1.1 Short-Term Treatment of Active Duodenal Ulcer
1.2 H. pylori Eradication to Reduce the Risk of Duodenal Ulcer Recurrence
1.3 Maintenance of Healed Duodenal Ulcers
1.4 Short-Term Treatment of Active Benign Gastric Ulcer
1.5 Healing of NSAID-Associated Gastric Ulcer
1.6 Risk Reduction of NSAID-Associated Gastric Ulcer
1.7 Gastroesophageal Reflux Disease (GERD)
1.8 Maintenance of Healing of Erosive Esophagitis (EE)
1.9 Pathological Hypersecretory Conditions Including Zollinger-Ellison Syndrome(ZES)
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dose
2.2 Special Populations
2.3 Important Administration Information
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Presence of Gastric Malignancy
5.2 Acute Interstitial Nephritis
5.3 Clostridium difficile-Associated Diarrhea
5.4 Bone Fracture
5.5 Cutaneous and Systemic Lupus Erythematosus
5.6 Cyanocobalamin (Vitamin B-12) Deficiency
5.7 Hypomagnesemia
5.8 Concomitant Use of Lansoprazole with Methotrexate
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
6.2 Postmarketing Experience
6.3 Combination Therapy with Amoxicillin and Clarithromycin
6.4 Laboratory Values
7 DRUG INTERACTIONS
7.1 Drugs with pH-Dependent Absorption
7.2 Warfarin
7.3 Tacrolimus
7.4 Theophylline
7.5 Clopidogrel
7.6 Methotrexate
7.7 Combination Therapy with Clarithromycin
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.3 Nursing Mothers
8.4 Pediatric Use
8.5 Geriatric Use
8.6 Renal Impairment
8.7 Hepatic Impairment
8.8 Gender
8.9 Race
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
13.2 Animal Toxicology and/or Pharmacology
14 CLINICAL STUDIES
15 REFERENCES
16 HOW SUPPLIED/STORAGE AND HANDLING
- * Sections or subsections omitted from the full prescribing information are not listed.
-
1 INDICATIONS AND USAGE
1.1 Short-Term Treatment of Active Duodenal Ulcer
Lansoprazole delayed-release capsules are indicated for short-term treatment (for four weeks) for healing and symptom relief of active duodenal ulcer [ see Clinical Studies ( 14) ].
1.2 H. pylori Eradication to Reduce the Risk of Duodenal Ulcer Recurrence
Triple Therapy: Lansoprazole/amoxicillin/clarithromycin
Lansoprazole in combination with amoxicillin plus clarithromycin as triple therapy is indicated for the treatment of patients with H. pylori infection and duodenal ulcer disease (active or one-year history of a duodenal ulcer) to eradicate H. pylori. Eradication of H. pylori has been shown to reduce the risk of duodenal ulcer recurrence [see Clinical Studies ( 14) ].
Please refer to the full prescribing information for amoxicillin and clarithromycin.
Dual Therapy: Lansoprazole/amoxicillin
Lansoprazole in combination with amoxicillin as dual therapy is indicated for the treatment of patients with H. pylori infection and duodenal ulcer disease (active or one-year history of a duodenal ulcer) who are either allergic or intolerant to clarithromycin or in whom resistance to clarithromycin is known or suspected (see the clarithromycin prescribing information, MICROBIOLOGY section). Eradication of H. pylori has been shown to reduce the risk of duodenal ulcer recurrence [see Clinical Studies ( 14) ].
Please refer to the full prescribing information for amoxicillin.
1.3 Maintenance of Healed Duodenal Ulcers
Lansoprazole delayed-release capsules are indicated to maintain healing of duodenal ulcers. Controlled studies do not extend beyond 12 months [ see Clinical Studies ( 14) ].
1.4 Short-Term Treatment of Active Benign Gastric Ulcer
Lansoprazole delayed-release capsules are indicated for short-term treatment (up to eight weeks)for healing and symptom relief of active benign gastric ulcer [ see Clinical Studies ( 14) ].
1.5 Healing of NSAID-Associated Gastric Ulcer
Lansoprazole delayed-release capsules are indicated for the treatment of NSAID-associated gastric ulcer in patients who continue NSAID use. Controlled studies did not extend beyond eight weeks [ see Clinical Studies ( 14) ].
1.6 Risk Reduction of NSAID-Associated Gastric Ulcer
Lansoprazole delayed-release capsules are indicated for reducing the risk of NSAID-associated gastric ulcers in patients with a history of a documented gastric ulcer who require the use of an NSAID. Controlled studies did not extend beyond 12 weeks [ see Clinical Studies ( 14) ].
1.7 Gastroesophageal Reflux Disease (GERD)
Short-Term Treatment of Symptomatic GERD
Lansoprazole delayed-release capsules are indicated for the treatment of heartburn and other symptoms associated with GERD for up to eight weeks [ see Clinical Studies ( 14) ].
Short-Term Treatment of Erosive Esophagitis
Lansoprazole delayed-release capsules are indicated for short-term treatment (up to eight weeks) for healing and symptom relief of all grades of erosive esophagitis. For patients who do not heal with Lansoprazole for eight weeks (5 to 10%), it may be helpful to give an additional eight weeks of treatment. If there is a recurrence of erosive esophagitis an additional eight week course of Lansoprazole may be considered [ see Clinical Studies ( 14) ].
1.8 Maintenance of Healing of Erosive Esophagitis (EE)
Lansoprazole delayed-release capsules are indicated to maintain healing of erosive esophagitis. Controlled studies did not extend beyond 12 months [ see Clinical Studies ( 14) ].
1.9 Pathological Hypersecretory Conditions Including Zollinger-Ellison Syndrome(ZES)
Lansoprazole delayed-release capsules are indicated for the long-term treatment of pathological hypersecretory conditions, including Zollinger-Ellison syndrome [ see Clinical Studies ( 14) ].
-
2 DOSAGE AND ADMINISTRATION
Lansoprazole is available as a capsule in 15 mg and 30 mg strengths. Direction for use specific to the route and available methods of administration of this dosage form is presented below. Lansoprazole should be taken before eating. Lansoprazole delayed-release capsules SHOULD NOT BE CRUSHED OR CHEWED. In the clinical trials, antacids were used concomitantly.
2.1 Recommended Dose
*Please refer to amoxicillin and clarithromycin full prescribing information for CONTRAINDICATIONS and WARNINGS, and for information regarding dosing in elderly and renally-impaired patients.
† Controlled studies did not extend beyond indicated duration.
‡ For patients who do not heal with lansoprazole for eight weeks (5 to 10%), it may be helpful to give an additional eight weeks of treatment. If there is a recurrence of erosive esophagitis, an additional eight week course of lansoprazole may be considered.
§The lansoprazole dose was increased (up to 30 mg twice daily) in some pediatric patients after two or more weeks of treatment if they remained symptomatic. For pediatric patients unable to swallow an intact capsule please see Administration Options.
¶Varies with individual patient. Recommended adult starting dose is 60 mg once daily. Doses should be adjusted to individual patient needs and should continue for as long as clinically indicated. Dosages up to 90 mg twice daily have been administered. Daily dose of greater than 120 mg should be administered in divided doses. Some patients with Zollinger-Ellison Syndrome have been treated continuously with lansoprazole for more than four years.
#Controlled studies did not extend beyond 12 months.
Indication
Recommended Dose
Frequency
Duodenal Ulcers
Short-Term Treatment
15 mg
Once daily for 4 weeks
Maintenance of Healed
15 mg
Once daily
H. pylori Eradication to
Reduce the Risk of
Duodenal Ulcer Recurrence*
Triple Therapy:
Lansoprazole
30 mg
Twice daily (q12h) for 10 or 14 days
Amoxicillin
1 gram
Twice daily (q12h) for 10 or 14 days
Clarithromycin
500 mg
Twice daily (q12h) for 10 or 14 days
Dual Therapy:
Lansoprazole
30 mg
Three times daily (q8h) for 14 days
Amoxicillin
1 gram
Three times daily (q8h) for 14 days
Benign Gastric Ulcer
Short-Term Treatment
30 mg
Once daily for up to 8 weeks
NSAID-associated Gastric Ulcer
Healing
30 mg
Once daily for 8 weeks †
Risk Reduction
15 mg
Once daily for up to 12 weeks †
Gastroesophageal Reflux Disease (GERD)
Short-Term Treatment of Symptomatic GERD
15 mg
Once daily for up to 8 weeks
Short-Term
Treatment of Erosive Esophagitis
30 mg
Once daily for up to 8 weeks ‡
Pediatric
(1 to 11 years of age)
Short-Term Treatment of Symptomatic GERD and Short-Term Treatment of Erosive Esophagitis
≤ 30 kg
15 mg
Once daily for up to 12 weeks §
> 30 kg
30 mg
Once daily for up to 12 weeks §
(12 to 17 year of age)
Short-Term Treatment of Symptomatic GERD
Nonerosive GERD
15 mg
Once daily for up to 8 weeks
Erosive Esophagitis
30 mg
Once daily for up to 8 weeks
Maintenance of Healing of Erosive Esophagitis
15 mg
Once daily
Pathological Hypersecretory Conditions including Zollinger-Ellison Syndrome
60 mg
Once daily ¶
Patients should be instructed that if a dose is missed, it should be taken as soon as possible. However, if the next scheduled dose is due, the patient should not take the missed dose, and should be instructed to take the next dose on time. Patients should be instructed not to take two doses at one time to make up for a missed dose.
2.2 Special Populations
Renal impairment patients and geriatric patients do not require dosage adjustment. However, consider dose adjustment in patients with severe liver impairment [see Use in Specific Populations ( 8.5, 8.6 and 8.7) ].
2.3 Important Administration Information
Lansoprazole Delayed-release Capsules – Oral Administration
- Lansoprazole delayed-release capsules should be swallowed whole.
- Alternatively, for patients who have difficulty swallowing capsules, lansoprazole delayed-release capsules can be opened and administered as follows:
о Sprinkle intact granules on one tablespoon of either applesauce, ENSURE pudding, cottage cheese, yogurt or strained pears.
о Swallow immediately.
- Lansoprazole delayed-release capsules may also be emptied into a small volume of either apple juice, orange juice or tomato juice and administered as follows:
о Sprinkle intact granules into a small volume of either apple juice, orange juice or tomato juice (60 mL – approximately two ounces).
о Mix briefly.
о Swallow immediately.
о To ensure complete delivery of the dose, the glass should be rinsed with two or more volumes of juice and the contents swallowed immediately.
Lansoprazole delayed-release capsules - Nasogastric Tube (≥ 16 French) Administration
- For patients who have a nasogastric tube in place, lansoprazole delayed-release capsules can be administered as follows:
о Mix intact granules into 40 mL of apple juice. DO NOT USE OTHER LIQUIDS.
о Inject through the nasogastric tube into the stomach.
о Flush with additional apple juice to clear the tube.
USE IN OTHER FOODS AND LIQUIDS HAS NOT BEEN STUDIED CLINICALLY AND IS THEREFORE NOT RECOMMENDED.
-
3 DOSAGE FORMS AND STRENGTHS
- 15 mg capsules are enteric coated pellets filled in size ‘3’ hard gelatin capsules with standard pink opaque colored cap printed with "ZA -50" in black ink and white opaque body printed with "15mg" in black ink
- 30 mg capsules are enteric coated pellets filled in size ‘1’ hard gelatin capsules with standard pink opaque colored cap printed with "ZA -51" in black ink and white opaque body printed with "30 mg" in black ink
-
4 CONTRAINDICATIONS
Lansoprazole is contraindicated in patients with known severe hypersensitivity to any component of the formulation. Hypersensitivity reactions may include anaphylaxis, anaphylactic shock, angioedema, bronchospasm, acute interstitial nephritis, and urticaria [see Adverse Reactions ( 6) ].
For information about contraindications of antibacterial agents (clarithromycin and amoxicillin) indicated in combination with lansoprazole, refer to the CONTRAINDICATIONS section of their prescribing information.
-
5 WARNINGS AND PRECAUTIONS
5.1 Presence of Gastric Malignancy
In adults, symtomatic response to therapy with lansoprazole does not preclude the presence of gastric malignancy. Consider additional follow-up and diagnostic testing in adult patients who have a suboptimal response or an early symptomatic relapse after completing treatment with a PPI. In older patients, also consider an endoscopy.
5.2 Acute Interstitial Nephritis
Acute interstitial nephritis has been observed in patients taking PPIs including lansoprazole. Acute interstitial nephritis may occur at any point during PPI therapy and is generally attributed to an idiopathic hypersensitivity reaction. Discontinue lansoprazole if acute interstitial nephritis develops [see Contraindications ( 4) ].
5.3 Clostridium difficile-Associated Diarrhea
Published observational studies suggest that proton pump inhibitor (PPI) therapy like lansoprazole may be associated with an increased risk of Clostridium difficile associated diarrhea (CDAD), especially in hospitalized patients. This diagnosis should be considered for diarrhea that does not improve [see Adverse Reactions ( 6.2) ].
Patients should use the lowest dose and shortest duration of PPI therapy appropriate to the condition being treated.
CDAD has been reported with use of nearly all antibacterial agents. For more information specific to antibacterial agents (clarithromycin and amoxicillin) indicated for use in combination with lansoprazole, refer to WARNINGS and PRECAUTIONS sections of those prescribing information.
5.4 Bone Fracture
Several published observational studies suggest that PPI therapy may be associated with an increased risk for osteoporosis-related fractures of the hip, wrist or spine. The risk of fracture was increased in patients who received high-dose, defined as multiple daily doses, and long-term PPI therapy (a year or longer). Patients should use the lowest dose and shortest duration of PPI therapy appropriate to the condition being treated. Patients at risk for osteoporosis-related fractures should be managed according to established treatment guidelines [see Dosage and Administration ( 2) and Adverse Reactions ( 6.2) ].
5.5 Cutaneous and Systemic Lupus Erythematosus
Cutaneous lupus erythematosus (CLE) and systemic lupus erythematosus (SLE) have been reported in patients taking PPIs, including lansoprazole. These events have occurred as both new onset and an exacerbation of existing autoimmune disease. The majority of PPI-induced lupus erythematosus cases were CLE.
The most common form of CLE reported in patients treated with PPIs was subacute CLE (SCLE) and occurred within weeks to years after continuous drug therapy in patients ranging from infants to the elderly. Generally, histological findings were observed without organ involvement.
Systemic lupus erythematosus (SLE) is less commonly reported than CLE in patients receiving PPIs. PPI associated SLE is usually milder than non-drug induced SLE. Onset of SLE typically occurred within days to years after initiating treatment primarily in patients ranging from young adults to the elderly. The majority of patients presented with rash; however, arthralgia and cytopenia were also reported.
Avoid administration of PPIs for longer than medically indicated. If signs or symptoms consistent with CLE or SLE are noted in patients receiving lansoprazole, discontinue the drug and refer the patient to the appropriate specialist for evaluation. Most patients improve with discontinuation of the PPI alone in four to 12 weeks. Serological testing (e.g., ANA) may be positive and elevated serological test results may take longer to resolve than clinical manifestations.
5.6 Cyanocobalamin (Vitamin B-12) Deficiency
Daily treatment with any acid-suppressing medications over a long period of time (e.g., longer than three years) may lead to malabsorption of cyanocobalamin (Vitamin B-12) caused by hypo- or achlorhydria. Rare reports of cyanocobalamin deficiency occurring with acid-suppressing therapy have been reported in the literature. This diagnosis should be considered if clinical symptoms consistent with cyanocobalamin deficiency are observed.
5.7 Hypomagnesemia
Hypomagnesemia, symptomatic and asymptomatic, has been reported rarely in patients treated with PPIs for at least three months, in most cases after a year of therapy. Serious adverse events include tetany, arrhythmias, and seizures. In most patients, treatment of hypomagnesemia required magnesium replacement and discontinuation of the PPI.
For patients expected to be on prolonged treatment or who take PPIs with medications such as digoxin or drugs that may cause hypomagnesemia (e.g., diuretics), health care professionals may consider monitoring magnesium levels prior to initiation of PPI treatment and periodically [see Adverse Reactions ( 6.2) ].
5.8 Concomitant Use of Lansoprazole with Methotrexate
Literature suggests that concomitant use of PPIs with methotrexate (primarily at high dose; see methotrexate prescribing information) may elevate and prolong serum levels of methotrexate and/or its metabolite, possibly leading to methotrexate toxicities. In high-dose methotrexate administration, a temporary withdrawal of the PPI may be considered in some patients [see Drug Interactions ( 7.6) and Clinical Pharmacology ( 12.3) ].
-
6 ADVERSE REACTIONS
The following serious adverse reactions are described below and elsewhere in labeling:
- Acute Interstitial Nephritis [see Warnings and Precautions ( 5.2 )]
- Clostridium difficile-Associated Diarrhea [see Warnings and Precautions ( 5.3)]
- Bone Fracture [see Warnings and Precautions ( 5.4) ]
- Cutaneous and Systemic Lupus Erythematosus [see Warnings and Precautions ( 5.5) ]
- Cyanocobalamin (Vitamin B-12) Deficiency [see Warnings and Precautions ( 5.6) ]
- Hypomagnesemia [see Warnings and Precautions ( 5.7) ]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
Worldwide, over 10,000 patients have been treated with lansoprazole in Phase 2 or Phase 3 clinical trials involving various dosages and durations of treatment. In general, lansoprazole treatment has been well-tolerated in both short-term and long-term trials.
The following adverse reactions were reported by the treating physician to have a possible or probable relationship to drug in 1% or more of lansoprazole-treated patients and occurred at a greater rate in lansoprazole-treated patients than placebo-treated patients in Table 1.
Table 1Incidence of Possibly or Probably Treatment-Related Adverse Reactions in Short-Term, Placebo-Controlled Lansoprazole Studies Body System/Adverse Event
Lansoprazole
(N= 2768)
%
Placebo
(N= 1023)
%
Body as a Whole
Abdominal Pain
2.1
1.2
Digestive System
Constipation
Diarrhea
Nausea
1
3.8
1.3
0.4
2.3
1.2
Headache was also seen at greater than 1% incidence but was more common on placebo. The incidence of diarrhea was similar between patients who received placebo and patients who received 15 mg and 30 mg of lansoprazole, but higher in the patients who received 60 mg of lansoprazole (2.9%, 1.4%, 4.2%, and 7.4%, respectively).
The most commonly reported possibly or probably treatment-related adverse event during maintenance therapy was diarrhea.
In the risk reduction study of lansoprazole for NSAID-associated gastric ulcers, the incidence of diarrhea for patients treated with lansoprazole, misoprostol, and placebo was 5%, 22%, and 3%, respectively.
Another study for the same indication, where patients took either a COX-2 inhibitor or lansoprazole and naproxen, demonstrated that the safety profile was similar to the prior study. Additional reactions from this study not previously observed in other clinical trials with lansoprazole included contusion, duodenitis, epigastric discomfort, esophageal disorder, fatigue, hunger, hiatal hernia, hoarseness, impaired gastric emptying, metaplasia, and renal impairment.
Additional adverse experiences occurring in less than 1% of patients or subjects who received lansoprazole in domestic trials are shown below:
Body as a Whole - abdomen enlarged, allergic reaction, asthenia, back pain, candidiasis, carcinoma, chest pain (not otherwise specified), chills, edema, fever, flu syndrome, halitosis, infection (not otherwise specified), malaise, neck pain, neck rigidity, pain, pelvic pain
Cardiovascular System - angina, arrhythmia, bradycardia, cerebrovascular accident/cerebral infarction, hypertension/hypotension, migraine, myocardial infarction, palpitations, shock (circulatory failure), syncope, tachycardia, vasodilation
Digestive System - abnormal stools, anorexia, bezoar, cardiospasm, cholelithiasis, colitis, dry mouth, dyspepsia, dysphagia, enteritis, eructation, esophageal stenosis, esophageal ulcer, esophagitis, fecal discoloration, flatulence, gastric nodules/fundic gland polyps, gastritis, gastroenteritis, gastrointestinal anomaly, gastrointestinal disorder, gastrointestinal hemorrhage, glossitis, gum hemorrhage, hematemesis, increased appetite, increased salivation, melena, mouth ulceration, nausea and vomiting, nausea and vomiting and diarrhea, gastrointestinal moniliasis, rectal disorder, rectal hemorrhage, stomatitis, tenesmus, thirst, tongue disorder, ulcerative colitis, ulcerative stomatitis
Endocrine System - diabetes mellitus, goiter, hypothyroidism
Hemic and Lymphatic System - anemia, hemolysis, lymphadenopathy
Metabolism and Nutritional Disorders - avitaminosis, gout, dehydration, hyperglycemia/hypoglycemia, peripheral edema, weight gain/loss
Musculoskeletal System - arthralgia, arthritis, bone disorder, joint disorder, leg cramps, musculoskeletal pain, myalgia, myasthenia, ptosis, synovitis
Nervous System - abnormal dreams, agitation, amnesia, anxiety, apathy, confusion, convulsion, dementia, depersonalization, depression, diplopia, dizziness, emotional lability, hallucinations, hemiplegia, hostility aggravated, hyperkinesia, hypertonia, hypesthesia, insomnia, libido decreased/increased, nervousness, neurosis, paresthesia, sleep disorder, somnolence, thinking abnormality, tremor, vertigo
Respiratory System - asthma, bronchitis, cough increased, dyspnea, epistaxis, hemoptysis, hiccup, laryngeal neoplasia, lung fibrosis, pharyngitis, pleural disorder, pneumonia, respiratory disorder, upper respiratory inflammation/infection, rhinitis, sinusitis, stridor
Skin and Appendages - acne, alopecia, contact dermatitis, dry skin, fixed eruption, hair disorder, maculopapular rash, nail disorder, pruritus, rash, skin carcinoma, skin disorder, sweating, urticaria
Special Senses - abnormal vision, amblyopia, blepharitis, blurred vision, cataract, conjunctivitis, deafness, dry eyes, ear/eye disorder, eye pain, glaucoma, otitis media, parosmia, photophobia, retinal degeneration/disorder, taste loss, taste perversion, tinnitus, visual field defect
Urogenital System - abnormal menses, breast enlargement, breast pain, breast tenderness, dysmenorrhea, dysuria, gynecomastia, impotence, kidney calculus, kidney pain, leukorrhea, menorrhagia, menstrual disorder, penis disorder, polyuria, testis disorder, urethral pain, urinary frequency, urinary retention, urinary tract infection, urinary urgency, urination impaired, vaginitis.
6.2 Postmarketing Experience
Additional adverse experiences have been reported since lansoprazole has been marketed. The majority of these cases are foreign-sourced and a relationship to lansoprazole has not been established. Because these reactions were reported voluntarily from a population of unknown size, estimates of frequency cannot be made. These events are listed below by COSTART body system.
Body as a Whole - anaphylactic/anaphylactoid reactions, systemic lupus erythematosus;
Digestive System - hepatotoxicity, pancreatitis, vomiting
Hemic and Lymphatic System - agranulocytosis, aplastic anemia, hemolytic anemia, leukopenia, neutropenia, pancytopenia, thrombocytopenia, and thrombotic thrombocytopenic purpura
Infections and Infestations - Clostridium difficile associated diarrhea
Metabolism and Nutritional Disorders - hypomagnesemia
Musculoskeletal System - bone fracture, myositis
Skin and Appendages - severe dermatologic reactions including erythema multiforme, Stevens-Johnson syndrome, toxic epidermal necrolysis (some fatal), cutaneous lupus erythematosus
Special Senses - speech disorder
Urogenital System - interstitial nephritis, urinary retention
6.3 Combination Therapy with Amoxicillin and Clarithromycin
In clinical trials using combination therapy with lansoprazole plus amoxicillin and clarithromycin, and lansoprazole plus amoxicillin, no adverse reactions peculiar to these drug combinations were observed. Adverse reactions that have occurred have been limited to those that had been previously reported with lansoprazole, amoxicillin, or clarithromycin.
Triple Therapy: Lansoprazole /amoxicillin/clarithromycin
The most frequently reported adverse reactions for patients who received triple therapy for 14 days were diarrhea (7%), headache (6%), and taste perversion (5%). There were no statistically significant differences in the frequency of reported adverse reactions between the 10- and 14-day triple therapy regimens. No treatment-emergent adverse reactions were observed at significantly higher rates with triple therapy than with any dual therapy regimen.
Dual Therapy: Lansoprazole/amoxicillin
The most frequently reported adverse reactions for patients who received lansoprazole three times daily plus amoxicillin three times daily dual therapy were diarrhea (8%) and headache (7%). No treatment-emergent adverse reactions were observed at significantly higher rates with lansoprazole three times daily plus amoxicillin three times daily dual therapy than with lansoprazole alone.
For information about adverse reactions with antibacterial agents (amoxicillin and clarithromycin) indicated in combination with lansoprazole, refer to the ADVERSE REACTIONS section of their prescribing information.
6.4 Laboratory Values
The following changes in laboratory parameters in patients who received lansoprazole were reported as adverse reactions:
Abnormal liver function tests, increased SGOT (AST), increased SGPT (ALT), increased creatinine, increased alkaline phosphatase, increased globulins, increased GGTP, increased/decreased/abnormal WBC, abnormal AG ratio, abnormal RBC, bilirubinemia, blood potassium increased, blood urea increased, crystal urine present, eosinophilia, hemoglobin decreased, hyperlipemia, increased/decreased electrolytes, increased/decreased cholesterol, increased glucocorticoids, increased LDH, increased/decreased/abnormal platelets, increased gastrin levels and positive fecal occult blood. Urine abnormalities such as albuminuria, glycosuria, and hematuria were also reported. Additional isolated laboratory abnormalities were reported.
In the placebo-controlled studies, when SGOT (AST) and SGPT (ALT) were evaluated, 0.4% (4/978) and 0.4% (11/2677) patients, who received placebo and lansoprazole, respectively, had enzyme elevations greater than three times the upper limit of normal range at the final treatment visit. None of these patients who received lansoprazole reported jaundice at any time during the study.
In clinical trials using combination therapy with lansoprazole plus amoxicillin and clarithromycin, and lansoprazole plus amoxicillin, no increased laboratory abnormalities particular to these drug combinations were observed.
For information about laboratory value changes with antibacterial agents (amoxicillin and clarithromycin) indicated in combination with lansoprazole, refer to the ADVERSE REACTIONS section of their prescribing information.
-
7 DRUG INTERACTIONS
7.1 Drugs with pH-Dependent Absorption
Due to its effects on gastric acid secretion, lansoprazole can reduce the absorption of drugs where gastric pH is an important determinant of their bioavailability. As with other drugs that decrease the intragastric acidity, the absorption of drugs such as ampicillin esters, ketoconazole, atazanavir, nelfinavir, iron salts, erlotinib, and mycophenolate mofetil (MMF) can decrease, while the absorption of drugs such as digoxin can increase during treatment with lansoprazole [see Clinical Pharmacology ( 12.3) ].
Lansoprazole is likely to substantially decrease the systemic concentrations of HIV protease inhibitors, such as atazanavir and nelfinavir, which are dependent upon the presence of gastric acid for absorption, and may result in a loss of therapeutic effect of atazanavir or nelfinavirand the development of HIV resistance. Therefore, lansoprazole should not be coadministered with atazanavir or nelfinavir [see Clinical Pharmacology ( 12.3) ].
Coadministration of PPIs in healthy subjects and in transplant patients receiving MMF has been reported to reduce the exposure to the active metabolite, mycophenolic acid (MPA), possibly due to a decrease in MMF solubility at an increased gastric pH. The clinical relevance of reduced MPA exposure on organ rejection has not been established in transplant patients receiving PPIs and MMF. Use lansoprazole with caution in transplant patients receiving MMF.
7.2 Warfarin
In a study of healthy subjects, coadministration of single or multiple 60 mg doses of lansoprazole and warfarin did not affect the pharmacokinetics of warfarin nor prothrombin time [see Clinical Pharmacology ( 12.3) ]. However, there have been reports of increased INR and prothrombin time in patients receiving PPIs and warfarin concomitantly. Increases in INR and prothrombin time may lead to abnormal bleeding and even death. Patients treated with PPIs and warfarin concomitantly may need to be monitored for increases in INR and prothrombin time [see Clinical Pharmacology ( 12.3) ].
7.3 Tacrolimus
Concomitant administration of lansoprazole and tacrolimus may increase whole blood levels of tacrolimus, especially in transplant patients who are intermediate or poor metabolizers of CYP2C19.
7.4 Theophylline
A minor increase (10%) in the clearance of theophylline was observed following the administration of lansoprazole concomitantly with theophylline. Although the magnitude of the effect on theophylline clearance is small, individual patients may require additional titration of their theophylline dosage when lansoprazole is started or stopped to ensure clinically effective blood levels [see Clinical Pharmacology ( 12.3) ].
7.5 Clopidogrel
Concomitant administration of lansoprazole and clopidogrel in healthy subjects had no clinically important effect on exposure to the active metabolite of clopidogrel or clopidogrel-induced platelet inhibition [see Clinical Pharmacology ( 12.3) ]. No dose adjustment of clopidogrel is necessary when administered with an approved dose of lansoprazole.
7.6 Methotrexate
Case reports, published population pharmacokinetic studies, and retrospective analyses suggest that concomitant administration of PPIs and methotrexate (primarily at high dose; see methotrexate prescribing information) may elevate and prolong serum levels of methotrexate and/or its metabolite hydroxymethotrexate. However, no formal drug interaction studies of high dose methotrexate with PPIs have been conducted [see Warnings and Precautions ( 5.8) ].
In a study of rheumatoid arthritis patients receiving low-dose methotrexate, lansoprazole and naproxen, no effect on pharmacokinetics of methotrexate was observed [see Clinical Pharmacology ( 12.3) ].
7.7 Combination Therapy with Clarithromycin
Concomitant administration of clarithromycin with other drugs can lead to serious adverse reactions due to drug interactions [see Warnings and Precautions in prescribing information for clarithromycin]. Because of these drug interactions, clarithromycin is contraindicated for coadministration with certain drugs [see Contraindications in prescribing information for clarithromycin].
For information about drug interactions of antibacterial agents (amoxicillin and clarithromycin) indicated in combination with lansoprazole, refer to the DRUG INTERACTIONS section of their prescribing information.
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Category B
Reproduction studies have been performed in pregnant rats at oral doses up to 40 times the recommended human dose and in pregnant rabbits at oral doses up to 16 times the recommended human dose and have revealed no evidence of impaired fertility or harm to the fetus due to lansoprazole. There are, however, no adequate or well-controlled studies in pregnant women. Because animal reproduction studies are not always predictive of human response, this drug should be used during pregnancy only if clearly needed [see Nonclinical Toxicology ( 13.2) ].
See full prescribing information for clarithromycin before using in pregnant women.
8.3 Nursing Mothers
Lansoprazole or its metabolites are excreted in the milk of rats. It is not known whether lansoprazole is excreted in human milk. Because many drugs are excreted in human milk, because of the potential for serious adverse reactions in nursing infants from lansoprazole, and because of the potential for tumorigenicity shown for lansoprazole in rat carcinogenicity studies, a decision should be made whether to discontinue nursing or to discontinue lansoprazole, taking into account the importance of lansoprazole to the mother.
8.4 Pediatric Use
The safety and effectiveness of lansoprazole have been established in pediatric patients one to 17 years of age for short-term treatment of symptomatic GERD and erosive esophagitis, however, lansoprazole was not effective in patients with symptomatic GERD one month to less than one year of age in a multicenter, double-blind, placebo-controlled study.
Neonate to less than one year of age
The pharmacokinetics of lansoprazole were studied in pediatric patients with GERD aged less than 28 days and one to 11 months. Compared to healthy adults receiving 30 mg, neonates had higher exposure (mean weight-based normalized AUC values 2.04- and 1.88-fold higher at doses of 0.5 mg/kg/day and 1 mg/kg/day, respectively). Infants aged ≤ 10 weeks had clearance and exposure values that were similar to neonates. Infants aged greater than 10 weeks who received 1 mg/kg/day had mean AUC values that were similar to adults who received a 30 mg dose.
Lansoprazole was not found to be effective in a U.S. and Polish four week multicenter, double-blind, placebo-controlled, parallel-group study of 162 patients between one month and less than 12 months of age with symptomatic GERD based on a medical history of crying/fussing/irritability associated with feedings who had not responded to conservative GERD management (i.e., nonpharmacologic intervention) for seven to 14 days. Patients received lansoprazole as a suspension daily (0.2 to 0.3 mg/kg/day in infants ≤ 10 weeks of age or 1 to 1.5 mg/kg/day in infants greater than 10 weeks or placebo) for up to four weeks of double-blind treatment.
The primary efficacy endpoint was assessed by greater than 50% reduction from baseline in either the percent of feedings with a crying/fussing/irritability episode or the duration (minutes) of a crying/fussing/irritability episode within one hour after feeding.
There was no difference in the percentage of responders between the lansoprazole pediatric suspension group and placebo group (54% in both groups).
There were no adverse events reported in pediatric clinical studies (one month to less than 12 months of age) that were not previously observed in adults.
Based on the results of the Phase 3 efficacy study, lansoprazole was not shown to be effective. Therefore, these results do not support the use of lansoprazole in treating symptomatic GERD in infants.
One to 11 years of age
In an uncontrolled, open-label, U.S. multicenter study, 66 pediatric patients (one to 11 years of age) with GERD were assigned, based on body weight, to receive an initial dose of either lansoprazole 15 mg daily if ≤ 30 kg or lansoprazole 30 mg daily if greater than 30 kg administered for eight to 12 weeks. The lansoprazole dose was increased (up to 30 mg twice daily) in 24 of 66 pediatric patients after two or more weeks of treatment if they remained symptomatic. At baseline 85% of patients had mild to moderate overall GERD symptoms (assessed by investigator interview), 58% had non-erosive GERD and 42% had erosive esophagitis (assessed by endoscopy).
After eight to 12 weeks of lansoprazole treatment, the intent-to-treat analysis demonstrated an approximate 50% reduction in frequency and severity of GERD symptoms.
Twenty-one of 27 erosive esophagitis patients were healed at eight weeks and 100% of patients were healed at 12 weeks by endoscopy (Table 2).
Table 2GERD Symptom Improvement and Erosive Esophagitis Healing Rates in Pediatric Patients Age 1 to 11 GERD
Final Visit * % (n/N)
- * At Week 8 or Week 12
- † Symptoms assessed by patients diary kept by caregiver.
- ‡ No data were available for 4 pediatric patients.
Symptomatic GERD
Improvement in Overall GERD Symptoms †
76% (47/62 ‡)
Erosive Esophagitis
Improvement in Overall GERD Symptoms †
81% (22/27)
Healing Rate
100% (27/27)
In a study of 66 pediatric patients in the age group one year to 11 years old after treatment with lansoprazole given orally in doses of 15 mg daily to 30 mg twice daily, increases in serum gastrin levels were similar to those observed in adult studies. Median fasting serum gastrin levels increased 89% from 51 pg/mL at baseline to 97 pg/mL [interquartile range (25 th to 75 thpercentile) of 71 to 130 pg/mL] at the final visit.
The pediatric safety of lansoprazole delayed-release capsules has been assessed in 66 pediatric patients aged one to 11 years of age. Of the 66 patients with GERD 85% (56/66) took lansoprazole for 8 weeks and 15% (10/66) took it for 12 weeks.
The most frequently reported (two or more patients) treatment-related adverse reactions in patients one to 11 years of age (N=66) were constipation (5%) and headache (3%).
Twelve to 17 years of age
In an uncontrolled, open-label, U.S. multicenter study, 87 adolescent patients (12 to 17 years of age) with symptomatic GERD were treated with lansoprazole for 8 to 12 weeks. Baseline upper endoscopies classified these patients into two groups: 64 (74%) nonerosive GERD and 23 (26%) erosive esophagitis (EE). The nonerosive GERD patients received lansoprazole 15 mg daily for eight weeks and the EE patients received lansoprazole 30 mg daily for eight to 12 weeks. At baseline, 89% of these patients had mild to moderate overall GERD symptoms (assessed by investigator interviews). During 8 weeks of lansoprazole treatment, adolescent patients experienced a 63% reduction in frequency and a 69% reduction in severity of GERD symptoms based on diary results.
Twenty-one of 22 (95.5%) adolescent erosive esophagitis patients were healed after eight weeks of lansoprazole treatment. One patient remained unhealed after 12 weeks of treatment (Table 3).
Table 3GERD Symptom Improvement and Erosive Esophagitis Healing Rates in Pediatric Patients Age 12 to 17 GERD
Final Visit % (n/N)
- * Symptoms assessed by patient diary (parents/caregivers as necessary).
- † No data available for five patients.
- ‡ Data from one healed patient was excluded from this analysis due to timing of final endoscopy.
Symptomatic GERD (All Patients)
Improvement in Overall GERD Symptoms *
73.2% (60/82) †
Nonerosive GERD
Improvement in Overall GERD Symptoms *
71.2% (42/59) †
Erosive Esophagitis
Improvement in Overall GERD Symptoms *
78.3% (18/23)
Healing Rate ‡
95.5% (21/22) ‡
In these 87 adolescent patients, increases in serum gastrin levels were similar to those observed in adult studies, median fasting serum gastrin levels increased 42% from 45 pg/mL at baseline to 64 pg/mL [interquartile range (25 thto 75 thpercentile) of 44 to 88 pg/mL] at the final visit. (Normal serum gastrin levels are 25 to 111 pg/mL. )
The safety of lansoprazole delayed-release capsules has been assessed in these 87 adolescent patients. Of the 87 adolescent patients with GERD, 6% (5/87) took lansoprazole for less than six weeks, 93% (81/87) for six to 10 weeks, and 1% (1/87) for greater than 10 weeks.
The most frequently reported (at least 3%) treatment-related adverse reactions in these patients were headache (7%), abdominal pain (5%), nausea (3%) and dizziness (3%). Treatment-related dizziness, reported in this prescribing information as occurring in less than 1% of adult patients, was reported in this study by three adolescent patients with nonerosive GERD, who had dizziness concurrently with other reactions (such as migraine, dyspnea, and vomiting).
8.5 Geriatric Use
No dosage adjustment of lansoprazole is necessary in geriatric patients. The incidence rates of adverse reactions and laboratory test abnormalities are similar to those seen in younger patients [see Clinical Pharmacology ( 12.3) ].
8.6 Renal Impairment
No dosage adjustment of lansoprazole is necessary in patients with renal impairment. The pharmacokinetics of lansoprazole in patients with various degrees of renal impairment were not substantially different compared to those in subjects with normal renal function [see Clinical Pharmacology ( 12.3) ].
8.7 Hepatic Impairment
In patients with various degrees of chronic hepatic impairment, an increase in the mean AUC of up to 500% was observed at steady state compared to healthy subjects. Consider dose reduction in patients with severe hepatic impairment [see Clinical Pharmacology ( 12.3) ].
8.8 Gender
Over 4,000 women were treated with lansoprazole. Ulcer healing rates in females were similar to those in males. The incidence rates of adverse reactions in females were similar to those seen in males [see Clinical Pharmacology ( 12.3) ].
8.9 Race
The pooled mean pharmacokinetic parameters of lansoprazole from twelve U.S. Phase 1 studies (N=513) were compared to the mean pharmacokinetic parameters from two Asian studies (N=20). The mean AUCs of lansoprazole in Asian subjects were approximately twice those seen in pooled U.S. data; however, the inter-individual variability was high. The C max values were comparable.
-
10 OVERDOSAGE
Lansoprazole is not removed from the circulation by hemodialysis. In one reported overdose, a patient consumed 600 mg of lansoprazole with no adverse reaction. Oral lansoprazole doses up to 5000 mg/kg in rats [approximately 1300 times the 30 mg human dose based on body surface area (BSA)] and in mice (about 675.7 times the 30 mg human dose based on BSA) did not produce deaths or any clinical signs.
-
11 DESCRIPTION
The active ingredient in lansoprazole delayed-release capsules is lansoprazole, a substituted benzimidazole, 2-[[[3-methyl-4-(2,2,2-trifluoroethoxy)-2-pyridyl] methyl] sulfinyl] benzimidazole, a compound that inhibits gastric acid secretion. Its molecular formula is C 16H 14F 3N 3O 2S with a molecular weight of 369.37. Lansoprazole has the following structure:
Lansoprazole, USP is a white to brownish-white powder which melts with decomposition at approximately 166°C. Lansoprazole is freely soluble in dimethylformamide; and practically insoluble in water.
Lansoprazole is stable when exposed to light for up to two months. The rate of degradation of the compound in aqueous solution increases with decreasing pH. The degradation half-life of the drug substance in aqueous solution at 25°C is approximately 0.5 hour at pH 5 and approximately 18 hours at pH 7.
Each lansoprazole delayed-release capsule, USP intended for oral administration contains 15 mg or 30 mg of lansoprazole. In addition, each capsule contains the following inactive ingredients: corn starch, D&C red # 28, FD&C blue # 1, FD&C red # 40, gelatin, hydroxypropyl cellulose, hypromellose, low substituted hydroxypropyl cellulose, magnesium carbonate heavy powder, methacrylic acid copolymer dispersion, polyethylene glycol, polysorbate 80, sucrose, sugar spheres, talc and titanium dioxide. The capsule shell is printed with black pharmaceutical ink which contains following ingredients: black iron oxide, butyl alcohol, dehydrated alcohol, isopropyl alcohol, potassium hydroxide, propylene glycol, purified water, shellac and strong ammonia solution.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Lansoprazole belongs to a class of antisecretory compounds, the substituted benzimidazoles, that suppress gastric acid secretion by specific inhibition of the (H +, K +)-ATPase enzyme system at the secretory surface of the gastric parietal cell. Because this enzyme system is regarded as the acid (proton) pump within the parietal cell, lansoprazole has been characterized as a gastric acid-pump inhibitor, in that it blocks the final step of acid production. This effect is dose-related and leads to inhibition of both basal and stimulated gastric acid secretion irrespective of the stimulus. Lansoprazole does not exhibit anticholinergic or histamine type-2 antagonist activity.
12.2 Pharmacodynamics
After oral administration, lansoprazole was shown to significantly decrease the basal acid output and significantly increase the mean gastric pH and percent of time the gastric pH was greater than three and greater than four. Lansoprazole also significantly reduced meal-stimulated gastric acid output and secretion volume, as well as pentagastrin-stimulated acid output. In patients with hypersecretion of acid, lansoprazole significantly reduced basal and pentagastrin-stimulated gastric acid secretion. Lansoprazole inhibited the normal increases in secretion volume, acidity and acid output induced by insulin.
The intragastric pH results of a five-day, pharmacodynamic, crossover study of 15 mg and 30 mg of once daily lansoprazole are presented in Table 4:
Table 4Mean Antisecretory Effects After Single and Multiple Daily Lansoprazole Dosing
Lansoprazole
Parameter
Baseline Value
15 mg
30 mg
NOTE: An intragastric pH of greater than 4 reflects a reduction in gastric acid by 99%.
* (p < 0.05) versus baseline only.
†(p < 0.05) versus baseline and lansoprazole 15 mg.
Day 1
Day 5
Day 1
Day 5
Mean 24 Hour pH
2.1
2.7 *
4 *
3.6 †
4.9 †
Mean Nighttime pH
1.9
2.4
3 *
2.6
3.8 †
% Time Gastric pH > 3
18
33 *
59 *
51 †
72 †
% Time Gastric pH > 4
12
22 *
49 *
41 †
66 †
After the initial dose in this study, increased gastric pH was seen within one to two hours with 30 mg of lansoprazole and two to three hours with 15 mg of lansoprazole. After multiple daily dosing, increased gastric pH was seen within the first hour post-dosing with 30 mg of lansoprazole and within one to two hours post-dosing with 15 mg of lansoprazole.
Acid suppression may enhance the effect of antimicrobials in eradicating Helicobacter pylori ( H. pylori). The percentage of time gastric pH was elevated above five and six was evaluated in a crossover study of lansoprazole given daily, twice daily and three times daily (Table 5).
Table 5Mean Antisecretory Effects After Five Days of Twice Daily and Three Times Daily Dosing - * (p < 0.05) versus lansoprazole 30 mg daily
- † (p < 0.05) versus lansoprazole 30 mg daily, 15 mg twice daily and 30 mg twice daily.
Lansoprazole
Parameter
30 mg
daily
15 mg
twice daily
30 mg
twice daily
30 mg
three times daily
% Time Gastric pH > 5
43
47
59 *
77 †
% Time Gastric pH > 6
20
23
28
45 †
The inhibition of gastric acid secretion as measured by intragastric pH gradually returned to normal over two to four days after multiple doses. There was no indication of rebound gastric acidity.
Enterochromaffin-like (ECL) Cell Effects
During lifetime exposure of rats with up to 150 mg/kg/day of lansoprazole dosed seven days per week, marked hypergastrinemia was observed followed by ECL cell proliferation and formation of carcinoid tumors, especially in female rats. Gastric biopsy specimens from the body of the stomach from approximately 150 patients treated continuously with lansoprazole for at least one year did not show evidence of ECL cell effects similar to those seen in rat studies. Longer term data are needed to rule out the possibility of an increased risk of the development of gastric tumors in patients receiving long-term therapy with lansoprazole [see Nonclinical Toxicology ( 13.1) ].
Other Gastric Effects in Humans
Lansoprazole did not significantly affect mucosal blood flow in the fundus of the stomach. Due to the normal physiologic effect caused by the inhibition of gastric acid secretion, a decrease of about 17% in blood flow in the antrum, pylorus, and duodenal bulb was seen. Lansoprazole significantly slowed the gastric emptying of digestible solids. Lansoprazole increased serum pepsinogen levels and decreased pepsin activity under basal conditions and in response to meal stimulation or insulin injection. As with other agents that elevate intragastric pH, increases in gastric pH were associated with increases in nitrate-reducing bacteria and elevation of nitrite concentration in gastric juice in patients with gastric ulcer. No significant increase in nitrosamine concentrations was observed.
Serum Gastrin Effects
In over 2100 patients, median fasting serum gastrin levels increased 50% to 100% from baseline but remained within normal range after treatment with 15 to 60 mg of oral lansoprazole. These elevations reached a plateau within two months of therapy and returned to pretreatment levels within four weeks after discontinuation of therapy.
Endocrine Effects
Human studies for up to one year have not detected any clinically significant effects on the endocrine system. Hormones studied include testosterone, luteinizing hormone (LH), follicle stimulating hormone (FSH), sex hormone binding globulin (SHBG), dehydroepiandrosterone sulfate (DHEA-S), prolactin, cortisol, estradiol, insulin, aldosterone, parathormone, glucagon, thyroid stimulating hormone (TSH), triiodothyronine (T3), thyroxine (T4), and somatotropic hormone (STH). Lansoprazole in oral doses of 15 to 60 mg for up to one year had no clinically significant effect on sexual function. In addition, lansoprazole in oral doses of 15 to 60 mg for two to eight weeks had no clinically significant effect on thyroid function. In 24 month carcinogenicity studies in Sprague-Dawley rats with daily lansoprazole dosages up to 150 mg/kg, proliferative changes in the Leydig cells of the testes, including benign neoplasm, were increased compared to control rats.
Other Effects
No systemic effects of lansoprazole on the central nervous system, lymphoid, hematopoietic, renal, hepatic, cardiovascular, or respiratory systems have been found in humans. Among 56 patients who had extensive baseline eye evaluations, no visual toxicity was observed after lansoprazole treatment (up to 180 mg/day) for up to 58 months. After lifetime lansoprazole exposure in rats, focal pancreatic atrophy, diffuse lymphoid hyperplasia in the thymus, and spontaneous retinal atrophy were seen.
Microbiology
Lansoprazole, clarithromycin and/or amoxicillin have been shown to be active against most strains of Helicobacter pylori in vitro and in clinical infections as described in the INDICATIONS AND USAGE section [see Indications and Usage ( 1.2) ].
Helicobacter pylori Pretreatment Resistance
Clarithromycin pretreatment resistance (≥ 2 mcg/mL) was 9.5% (91/960) by E-test and 11.3% (12/106) by agar dilution in the dual and triple therapy clinical trials (M93 to 125, M93 to 130, M93 to 131, M95 to 392, and M95 to 399).
Amoxicillin pretreatment susceptible isolates (≤ 0.25 mcg/mL) occurred in 97.8% (936/957) and 98% (98/100) of the patients in the dual and triple therapy clinical trials by E-test and agar dilution, respectively. Twenty-one of 957 patients (2.2%) by E-test, and two of 100 patients (2%) by agar dilution, had amoxicillin pretreatment MICs of greater than 0.25 mcg/mL. One patient on the 14 day triple therapy regimen had an unconfirmed pretreatment amoxicillin minimum inhibitory concentration (MIC) of greater than 256 mcg/mL by E-test and the patient was eradicated of H. pylori (Table 6) .
Table 6 Clarithromycin Susceptibility Test Results and Clinical/Bacteriological Outcomes * Clarithromycin Pretreatment Results
Clarithromycin Post-treatment Results - * Includes only patients with pretreatment clarithromycin susceptibility test results
- † Susceptible (S) MIC ≤ 0.25 mcg/mL, Intermediate (I) MIC 0.5 to 1 mcg/mL, Resistant (R) MIC ≥ 2 mcg/mL
H. pylori negative – eradicated H. pylori positive –not eradicated
Post-treatment susceptibility resultsS † I † R † No MIC Triple Therapy 14 Day (lansoprazole 30 mg twice daily/amoxicillin 1 g twice daily/clarithromycin 500 mg twice daily)
(M95 to 399, M93 to 131, M95 to 392)
Susceptible †
112 105 7 Intermediate †
3 3 Resistant † 17 6 7 4 Triple Therapy 10-Day (lansoprazole 30 mg twice daily/amoxicillin 1 gm twice daily /clarithromycin 500 mg twice daily)
(M95-399)
Susceptible † 42 40 1 1 Intermediate †
Resistant † 4 1 3
Patients not eradicated of H. pylori following lansoprazole/amoxicillin/clarithromycin triple therapy will likely have clarithromycin resistant H. pylori. Therefore, for those patients who fail therapy, clarithromycin susceptibility testing should be done when possible. Patients with clarithromycin resistant H. pylori should not be treated with lansoprazole/amoxicillin/clarithromycin triple therapy or with regimens which include clarithromycin as the sole antimicrobial agent.
Amoxicillin Susceptibility Test Results and Clinical/Bacteriological Outcomes
In the dual and triple therapy clinical trials, 82.6% (195/236) of the patients that had pretreatment amoxicillin susceptible MICs (≤ 0.25 mcg/mL) were eradicated of H. pylori. Of those with pretreatment amoxicillin MICs of greater than 0.25 mcg/mL, three of six had the H. pylori eradicated. A total of 30% (21/70) of the patients failed lansoprazole 30 mg three times daily/amoxicillin 1 g three times daily dual therapy and a total of 12.8% (22/172) of the patients failed the 10 and 14 day triple therapy regimens. Post-treatment susceptibility results were not obtained on 11 of the patients who failed therapy. Nine of the 11 patients with amoxicillin post-treatment MICs that failed the triple therapy regimen also had clarithromycin resistant H. pylori isolates.
Susceptibility Test for Helicobacter pylori
For susceptibility testing information about Helicobacter pylori, see Microbiology section in prescribing information for clarithromycin and amoxicillin.
12.3 Pharmacokinetics
Lansoprazole delayed-release capsules contain an enteric-coated granule formulation of lansoprazole. Absorption of lansoprazole begins only after the granules leave the stomach. Absorption is rapid, with mean peak plasma levels of lansoprazole occurring after approximately 1.7 hours. After a single-dose administration of 15 mg to 60 mg of oral lansoprazole, the peak plasma concentrations (C max) of lansoprazole and the area under the plasma concentration curves (AUCs) of lansoprazole were approximately proportional to the administered dose. Lansoprazole does not accumulate and its pharmacokinetics are unaltered by multiple dosing.
Absorption
The absorption of lansoprazole is rapid, with the mean C max occurring approximately 1.7 hours after oral dosing, and the absolute bioavailability is over 80%. In healthy subjects, the mean (±SD) plasma half-life was 1.5 (±1) hours. Both the C max and AUC are diminished by about 50% to 70% if lansoprazole is given 30 minutes after food, compared to the fasting condition. There is no significant food effect if lansoprazole is given before meals.
Distribution
Lansoprazole is 97% bound to plasma proteins. Plasma protein binding is constant over the concentration range of 0.05 to 5 mcg/mL.
Metabolism
Lansoprazole is extensively metabolized in the liver. Two metabolites have been identified in measurable quantities in plasma (the hydroxylated sulfinyl and sulfone derivatives of lansoprazole). These metabolites have very little or no antisecretory activity. Lansoprazole is thought to be transformed into two active species which inhibit acid secretion by blocking the proton pump [(H +, K +)-ATPase enzyme system] at the secretory surface of the gastric parietal cell. The two active species are not present in the systemic circulation. The plasma elimination half-life of lansoprazole is less than two hours while the acid inhibitory effect lasts more than 24 hours. Therefore, the plasma elimination half-life of lansoprazole does not reflect its duration of suppression of gastric acid secretion.
Elimination
Following single-dose oral administration of lansoprazole, virtually no unchanged lansoprazole was excreted in the urine. In one study, after a single oral dose of 14C-lansoprazole, approximately one-third of the administered radiation was excreted in the urine and two-thirds was recovered in the feces. This implies a significant biliary excretion of the lansoprazole metabolites.
Pediatric Use
One to 17 years of age
The pharmacokinetics of lansoprazole were studied in pediatric patients with GERD aged one to 11 years and 12 to 17 years in two separate clinical studies. In children aged one to 11 years, lansoprazole was dosed 15 mg daily for subjects weighing ≤ 30 kg and 30 mg daily for subjects weighing greater than 30 kg. Mean C max and AUC values observed on Day 5 of dosing were similar between the two dose groups and were not affected by weight or age within each weight-adjusted dose group used in the study. In adolescent subjects aged 12 to 17 years, subjects were randomized to receive lansoprazole at 15 mg or 30 mg daily. Mean C max and AUC values of lansoprazole were not affected by body weight or age; and nearly dose-proportional increases in mean C max and AUC values were observed between the two dose groups in the study. Overall, lansoprazole pharmacokinetics in pediatric patients aged 1 to 17 years were similar to those observed in healthy adult subjects.
Neonate to less than one year of age
Refer to Section 8.4 for the pharmacokinetics of lansoprazole in pediatric patients with GERD aged less than 28 days and one to 11 months.
Geriatric Use
The clearance of lansoprazole is decreased in the elderly, with elimination half-life increased approximately 50% to 100%. Because the mean half-life in the elderly remains between 1.9 to 2.9 hours, repeated once daily dosing does not result in accumulation of lansoprazole. Peak plasma levels were not increased in the elderly. No dosage adjustment is necessary in the elderly [see Use in Specific Populations ( 8.5) ].
Renal Impairment
In patients with severe renal impairment, plasma protein binding decreased by 1% to 1.5% after administration of 60 mg of lansoprazole. Patients with renal impairment had a shortened elimination half-life and decreased total AUC (free and bound). The AUC for free lansoprazole in plasma, however, was not related to the degree of renal impairment; and the C max and T max (time to reach the maximum concentration) were not different than the C max and T max from subjects with normal renal function. No dosage adjustment is necessary in patients with renal impairment [see Use in Specific Populations ( 8.6) ].
Hepatic Impairment
In patients with various degrees of chronic hepatic impairment, the mean plasma half-life of lansoprazole was prolonged from 1.5 hours to 3.2 to 7.2 hours. An increase in the mean AUC of up to 500% was observed at steady state in hepatically-impaired patients compared to healthy subjects. Consider dose reduction in patients with severe hepatic impairment [see Use in Specific Populations ( 8.7) ].
Gender
In a study comparing 12 male and six female human subjects who received lansoprazole, no gender differences were found in pharmacokinetics and intragastric pH results [see Use in Specific Populations ( 8.8) ].
Lansoprazole may interfere with the absorption of other drugs where gastric pH is an important determinant of bioavailability (e.g., ketoconazole, ampicillin esters, iron salts, digoxin).
Lansoprazole is metabolized through the cytochrome P450 system, specifically through the CYP3A and CYP2C19 isozymes. Studies have shown that lansoprazole does not have clinically significant interactions with other drugs metabolized by the cytochrome P 450 system, such as warfarin, antipyrine, indomethacin, ibuprofen, phenytoin, propranolol, prednisone, diazepam, or clarithromycin in healthy subjects. These compounds are metabolized through various cytochrome P 450 isozymes including CYP1A2, CYP2C9, CYP2C19, CYP2D6, and CYP3A.
Atazanavir and Nelfinavir
Lansoprazole causes long-lasting inhibition of gastric acid secretion. Lansoprazole substantially decreases the systemic concentrations of HIV protease inhibitors, such as atazanavir and nelfinavir, which are dependent upon the presence of gastric acid for absorption, and may result in a loss of therapeutic effect of atazanavir or nelfinavir and the development of HIV resistance. Therefore, lansoprazole, or other proton pump inhibitors, should not be coadministered with atazanavir or nelfinavir.
Theophylline
When lansoprazole was administered concomitantly with theophylline (CYP1A2, CYP3A), a minor increase (10%) in the clearance of theophylline was seen. Because of the small magnitude and the direction of the effect on theophylline clearance, this interaction is unlikely to be of clinical concern. Nonetheless, individual patients may require additional titration of their theophylline dosage when lansoprazole is started or stopped to ensure clinically effective blood levels.
Warfarin
In a study of healthy subjects neither the pharmacokinetics of warfarin enantiomers nor prothrombin time were affected following single or multiple 60 mg doses of lansoprazole. However, there have been reports of increased International Normalized Ratio (INR) and prothrombin time in patients receiving proton pump inhibitors, including lansoprazole, and warfarin concomitantly. Increases in INR and prothrombin time may lead to abnormal bleeding and even death. Patients treated with proton pump inhibitors and warfarin concomitantly may need to be monitored for increases in INR and prothrombin time.
Methotrexate and 7-hydromethotrexate
In an open-label, single-arm, eight-day, pharmacokinetic study of 28 adult rheumatoid arthritis patients (who required the chronic use of 7.5 to 15 mg of methotrexate given weekly), administration of seven days of naproxen 500 mg twice daily and lansoprazole 30 mg daily had no effect on the pharmacokinetics of methotrexate and 7-hydroxymethotrexate. While this study was not designed to assess the safety of this combination of drugs, no major adverse reactions were noted. However, this study was conducted with low doses of methotrexate. A drug interaction study with high doses of methotrexate has not been conducted.
Amoxicillin
Lansoprazole has also been shown to have no clinically significant interaction with amoxicillin.
Sucralfate
In a single-dose crossover study examining lansoprazole 30 mg and omeprazole 20 mg each administered alone and concomitantly with sucralfate 1 gram, absorption of the proton pump inhibitors was delayed and their bioavailability was reduced by 17% and 16%, respectively, when administered concomitantly with sucralfate. Therefore, proton pump inhibitors should be taken at least 30 minutes prior to sucralfate. In clinical trials, antacids were administered concomitantly with lansoprazole and there was no evidence of a change in the efficacy of lansoprazole.
Clopidogrel
Clopidogrel is metabolized to its active metabolite in part by CYP2C19. A study of healthy subjects who were CYP2C19 extensive metabolizers, receiving once daily administration of clopidogrel 75 mg alone or concomitantly with lansoprazole 30 mg (n=40), for nine days was conducted. The mean AUC of the active metabolite of clopidogrel was reduced by approximately 14 % (mean AUC ratio was 86 %, with 90 % CI of 80 to 92 %) when lansoprazole was coadministered compared to administration of clopidogrel alone. Pharmacodynamic parameters were also measured and demonstrated that the change in inhibition of platelet aggregation (induced by 5 mcM ADP) was related to the change in the exposure to clopidogrel active metabolite. The clinical significance of this finding is not clear.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
In two 24 month carcinogenicity studies, Sprague-Dawley rats were treated with oral lansoprazole doses of five to 150 mg/kg/day, about one to 40 times the exposure on a body surface (mg/m 2) basis of a 50 kg person of average height [1.46 m 2body surface area (BSA)] given the recommended human dose of 30 mg/day. Lansoprazole produced dose-related gastric enterochromaffin-like (ECL) cell hyperplasia and ECL cell carcinoids in both male and female rats. It also increased the incidence of intestinal metaplasia of the gastric epithelium in both sexes. In male rats, lansoprazole produced a dose-related increase of testicular interstitial cell adenomas. The incidence of these adenomas in rats receiving doses of 15 to 150 mg/kg/day (four to 40 times the recommended human dose based on BSA) exceeded the low background incidence (range = 1.4 to 10%) for this strain of rat.
In a 24 month carcinogenicity study, CD-1 mice were treated with oral lansoprazole doses of 15 to 600 mg/kg/day, two to 80 times the recommended human dose based on BSA. Lansoprazole produced a dose-related increased incidence of gastric ECL cell hyperplasia. It also produced an increased incidence of liver tumors (hepatocellular adenoma plus carcinoma). The tumor incidences in male mice treated with 300 and 600 mg/kg/day (40 to 80 times the recommended human dose based on BSA) and female mice treated with 150 to 600 mg/kg/day (20 to 80 times the recommended human dose based on BSA) exceeded the ranges of background incidences in historical controls for this strain of mice. Lansoprazole treatment produced adenoma of rete testis in male mice receiving 75 to 600 mg/kg/day (10 to 80 times the recommended human dose based on BSA).
A 26 week p53 (+/-) transgenic mouse carcinogenicity study was not positive.
Lansoprazole was positive in the Ames test and the in vitro human lymphocyte chromosomal aberration assay. Lansoprazole was not genotoxic in the ex vivo rat hepatocyte unscheduled DNA synthesis (UDS) test, the in vivo mouse micronucleus test, or the rat bone marrow cell chromosomal aberration test.
Lansoprazole at oral doses up to 150 mg/kg/day (40 times the recommended human dose based on BSA) was found to have no effect on fertility and reproductive performance of male and female rats.
13.2 Animal Toxicology and/or Pharmacology
Reproductive Toxicology Studies
Reproduction studies have been performed in pregnant rats at oral lansoprazole doses up to 150 mg/kg/day [40 times the recommended human dose (30 mg/day) based on body surface area (BSA)] and pregnant rabbits at oral lansoprazole doses up to 30 mg/kg/day (16 times the recommended human dose based on BSA) and have revealed no evidence of impaired fertility or harm to the fetus due to lansoprazole.
-
14 CLINICAL STUDIES
In a U.S. multicenter, double-blind, placebo-controlled, dose-response (15, 30, and 60 mg of lansoprazole once daily) study of 284 patients with endoscopically documented duodenal ulcer, the percentage of patients healed after two and four weeks was significantly higher with all doses of lansoprazole than with placebo. There was no evidence of a greater or earlier response with the two higher doses compared with lansoprazole 15 mg. Based on this study and the second study described below, the recommended dose of lansoprazole in duodenal ulcer is 15 mg per day (Table 7).
Table 7Duodenal Ulcer Healing Rates
Lansoprazole Placebo
*(p ≤ 0.001) versus placebo.
Week 15 mg daily
(N=68)30 mg daily
(N=74)60 mg daily
(N=70)(N=72) 2 42.4% * 35.6% * 39.1% *
11.3% 4 89.4% * 91.7% * 89.9% *
46.1% Lansoprazole 15 mg was significantly more effective than placebo in relieving day and nighttime abdominal pain and in decreasing the amount of antacid taken per day.
In a second U.S. multicenter study, also double-blind, placebo-controlled, dose-comparison (15 and 30 mg of lansoprazole once daily), and including a comparison with ranitidine, in 280 patients with endoscopically documented duodenal ulcer, the percentage of patients healed after four weeks was significantly higher with both doses of lansoprazole than with placebo. There was no evidence of a greater or earlier response with the higher dose of lansoprazole. Although the 15 mg dose of lansoprazole was superior to ranitidine at four weeks, the lack of significant difference at two weeks and the absence of a difference between 30 mg of lansoprazole and ranitidine leaves the comparative effectiveness of the two agents undetermined (Table 8) [see Indications and Usage ( 1.1) ].
Table 8 Duodenal Ulcer Healing Rates
Lansoprazole
Ranitidine
Placebo
- * (p ≤ 0.05) versus placebo and ranitidine.
- † (p ≤ 0.05) versus placebo.
Week 15 mg daily
(N=80)30 mg daily
(N=77)300 mg h.s.
(N=82)
(N=41)
2 35% 44.2%
30.5%
34.2% 4 92.3% * 80.3% † 70.5% †
47.5%
H. pylori Eradication to Reduce the Risk of Duodenal Ulcer Recurrence
Randomized, double-blind clinical studies performed in the U.S. in patients with H. pylori and duodenal ulcer disease (defined as an active ulcer or history of an ulcer within one year) evaluated the efficacy of lansoprazole in combination with amoxicillin capsules and clarithromycin tablets as triple 14 day therapy or in combination with amoxicillin capsules as dual 14 day therapy for the eradication of H. pylori. Based on the results of these studies, the safety and efficacy of two different eradication regimens were established:
Triple therapy: Lansoprazole 30 mg twice daily/amoxicillin 1 g twice daily/clarithromycin 500 mg twice daily
Dual therapy: Lansoprazole 30 mg three times daily/amoxicillin 1 g three times daily
All treatments were for 14 days. H. pylori eradication was defined as two negative tests (culture and histology) at four to six weeks following the end of treatment.
Triple therapy was shown to be more effective than all possible dual therapy combinations. Dual therapy was shown to be more effective than both monotherapies. Eradication of H. pylori has been shown to reduce the risk of duodenal ulcer recurrence.
A randomized, double-blind clinical study performed in the U.S. in patients with H. pylori and duodenal ulcer disease (defined as an active ulcer or history of an ulcer within one year) compared the efficacy of lansoprazole triple therapy for 10 and 14 days. This study established that the 10 day triple therapy was equivalent to the 14 day triple therapy in eradicating H. pylori (Tables 9 and 10) [see Indications and Usage ( 1.2) ].
Table 9 H. pylori Eradication Rates – Triple Therapy (lansoprazole/amoxicillin/clarithromycin) Percent of Patients Cured [95% Confidence Interval] (Number of patients) Study
Duration
Triple Therapy Evaluable Analysis*
Triple Therapy
Intent-to-Treat Analysis†
*Based on evaluable patients with confirmed duodenal ulcer (active or within one year) and H. pylori infection at baseline defined as at least two of three positive endoscopic tests from CLOtest ®, histology and/or culture. Patients were included in the analysis if they completed the study. Additionally, if patients dropped out of the study due to an adverse event related to the study drug, they were included in the evaluable analysis as failures of therapy.
†Patients were included in the analysis if they had documented H. pylori infection at baseline as defined above and had a confirmed duodenal ulcer (active or within one year). All dropouts were included as failures of therapy.
‡(p < 0.05) versus lansoprazole/amoxicillin and lansoprazole/clarithromycin dual therapy.
§(p < 0.05) versus clarithromycin/amoxicillin dual therapy.
¶The 95% confidence interval for the difference in eradication rates, 10 day minus 14 day is (-10.5, 8.1) in the evaluable analysis and (-9.7, 9.1) in the intent-to-treat analysis.
M93 to 131
14 days
92 ‡
[80 to 97.7]
(N=48)
86 ‡
[73.3 to 93.5]
(N=55)
M95 to 392
14 days
86 §
[75.7 to 93.6]
(N=66)
83 §
[72 to 90.8]
(N=70)
M95 to 399 ¶
14 days
85
[77 to 91]
(N=113)
82
[73.9 to 88.1]
(N=126)
10 days
84
[76 to 89.8]
(N=123)
81
[73.9 to 87.6]
(N=135)
Table 10 H. pylori Eradication Rates – 14 Day Dual Therapy (lansoprazole/amoxicillin) Percent of Patients Cured [95% Confidence Interval] (Number of patients) *Based on evaluable patients with confirmed duodenal ulcer (active or within one year) and H. pylori infection at baseline defined as at least two of three positive endoscopic tests from CLOtest ®, histology and/or culture. Patients were included in the analysis if they completed the study. Additionally, if patients dropped out of the study due to an adverse event related to the study drug, they were included in the analysis as failures of therapy.
†Patients were included in the analysis if they had documented H. pylori infection at baseline as defined above and had a confirmed duodenal ulcer (active or within one year). All dropouts were included as failures of therapy.
‡ (p < 0.05) versus lansoprazole alone.
§ (p < 0.05) versus lansoprazole alone or amoxicillin alone.
Study
Dual Therapy Evaluable Analysis*
Dual Therapy Intent-to-Treat Analysis†
M93 to 131
77 ‡[62.5 to 87.2]
(N=51)
70 ‡[56.8 to 81.2]
(N=60)
M93 to 125
66 §[51.9 to 77.5]
(N=58)
61 §[48.5 to 72.9]
(N=67)
Long-Term Maintenance Treatment of Duodenal Ulcers
Lansoprazole has been shown to prevent the recurrence of duodenal ulcers. Two independent, double-blind, multicenter, controlled trials were conducted in patients with endoscopically confirmed healed duodenal ulcers. Patients remained healed significantly longer and the number of recurrences of duodenal ulcers was significantly less in patients treated with lansoprazole than in patients treated with placebo over a 12 month period (Table 11) [see Indications and Usage ( 1.3) ].
Table 11 Endoscopic Remission Rates Trial
Drug
No. of Pts.
Percent in Endoscopic Remission
%=Life Table Estimate
*(p ≤ 0.001) versus placebo.
0 to 3
mo.
0 to 6
mo.
0 to 12
mo.
#1
Lansoprazole 15 mg daily
86
90% *
87% *
84% *
Placebo
83
49%
41%
39%
#2
Lansoprazole 30 mg daily
18
94% *
94% *
85% *
Lansoprazole 15 mg daily
15
87% *
79% *
70% *
Placebo
15
33%
0%
0%
In trial #2, no significant difference was noted between lansoprazole 15 mg and 30 mg in maintaining remission.
Gastric Ulcer
In a U.S. multicenter, double-blind, placebo-controlled study of 253 patients with endoscopically documented gastric ulcer, the percentage of patients healed at four and eight weeks was significantly higher with lansoprazole 15 mg and 30 mg once a day than with placebo (Table 12) [see Indications and Usage ( 1.4) ].
Table 12Gastric Ulcer Healing Rates
Lansoprazole
Week
15 mg daily
30 mg daily
60 mg daily
Placebo
- * (p ≤ 0.05) versus placebo.
(N=65)
(N=63)
(N=61)
(N=64)
4
64.6% *
58.1% *
53.3% *
37.5%
8
92.2% *
96.8% *
93.2% *
76.7%
Patients treated with any lansoprazole dose reported significantly less day and night abdominal pain along with fewer days of antacid use and fewer antacid tablets used per day than the placebo group.
Independent substantiation of the effectiveness of lansoprazole 30 mg was provided by a meta-analysis of published and unpublished data.
Healing of NSAID-Associated Gastric Ulcer
In two U.S. and Canadian multicenter, double-blind, active-controlled studies in patients with endoscopically confirmed NSAID-associated gastric ulcer who continued their NSAID use, the percentage of patients healed after eight weeks was statistically significantly higher with 30 mg of lansoprazole than with the active control. A total of 711 patients were enrolled in the study, and 701 patients were treated. Patients ranged in age from 18 to 88 years (median age 59 years), with 67% female patients and 33% male patients. Race was distributed as follows: 87% Caucasian, 8% Black, 5% Other. There was no statistically significant difference between lansoprazole 30 mg daily and the active control on symptom relief (i.e., abdominal pain) (Table 13) [see Indications and Usage ( 1.5) ].
Table 13NSAID-Associated Gastric Ulcer Healing Rates * - * Actual observed ulcer(s) healed at time points ± 2 days
- † Dose for healing of gastric ulcer
- ‡ (p ≤ 0.05) versus the active control
Study #1
Lansoprazole 30 mg daily
Active Control †
Week 4
60% (53/88) ‡
28% (23/83)
Week 8
79% (62/79) ‡
55% (41/74)
Study #2
Lansoprazole 30 mg daily
Active Control †
Week 4
53% (40/75)
38% (31/82)
Week 8
77% (47/61) ‡
50% (33/66)
Risk Reduction of NSAID-Associated Gastric Ulcer
In one large U.S., multicenter, double-blind, placebo- and misoprostol-controlled (misoprostol blinded only to the endoscopist) study in patients who required chronic use of an NSAID and who had a history of an endoscopically documented gastric ulcer, the proportion of patients remaining free from gastric ulcer at four, eight, and 12 weeks was significantly higher with 15 or 30 mg of lansoprazole than placebo. A total of 537 patients were enrolled in the study, and 535 patients were treated. Patients ranged in age from 23 to 89 years (median age 60 years), with 65% female patients and 35% male patients. Race was distributed as follows: 90% Caucasian, 6% Black, 4% other. The 30 mg dose of lansoprazole demonstrated no additional benefit in risk reduction of the NSAID-associated gastric ulcer than the 15 mg dose (Table 14) [see Indications and Usage ( 1.6) ].
Table 14Proportion of Patients Remaining Free of Gastric Ulcers * Week
Lansoprazole
15 mg daily
(N=121)
Lansoprazole
30 mg daily
(N=116)
Misoprostol
200 mcg four times daily
(N=106)
Placebo
(N=112)
*% = Life Table Estimate
(p < 0.001) lansoprazole 15 mg daily versus placebo; lansoprazole 30 mg daily versus placebo; and misoprostol 200 mcg four times daily versus placebo.
(p < 0.05) Misoprostol 200 mcg four times daily versus lansoprazole 15 mg daily; and misoprostol 200 mcg four times daily versus lansoprazole 30 mg daily.
4
90%
92%
96%
66%
8
86%
88%
95%
60%
12
80%
82%
93%
51%
Gastroesophageal Reflux Disease (GERD)
Symptomatic GERD
In a U.S. multicenter, double-blind, placebo-controlled study of 214 patients with frequent GERD symptoms, but no esophageal erosions by endoscopy, significantly greater relief of heartburn associated with GERD was observed with the administration of lansoprazole 15 mg once daily up to eight weeks than with placebo. No significant additional benefit from lansoprazole 30 mg once daily was observed.
The intent-to-treat analyses demonstrated significant reduction in frequency and severity of day and night heartburn. Data for frequency and severity for the eight week treatment period are presented in Table 15 and in Figures 1 and 2:
Table 15Frequency of Heartburn Variable
Placebo
(n=43)
Lansoprazole 15 mg
(n=80)
Lansoprazole 30 mg (n=86)
- * (p < 0.01) versus placebo.
Median
% of Days without Heartburn
Week 1
0%
71% *
46% *
Week 4
11%
81% *
76% *
Week 8
13%
84% *
82% *
% of Nights without Heartburn
Week 1
17%
86% *
57% *
Week 4
25%
89% *
73% *
Week 8
36%
92% *
80% *
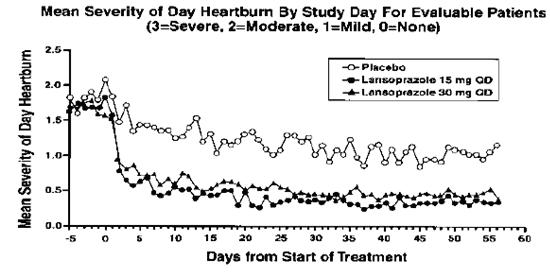
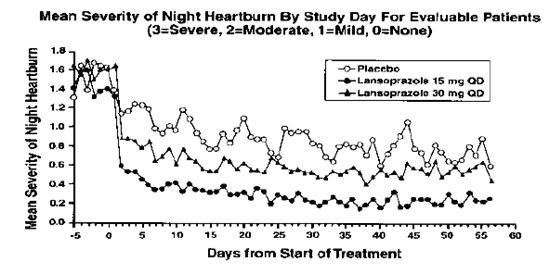
In two U.S., multicenter double-blind, ranitidine-controlled studies of 925 total patients with frequent GERD symptoms, but no esophageal erosions by endoscopy, lansoprazole 15 mg was superior to ranitidine 150 mg (twice daily) in decreasing the frequency and severity of day and night heartburn associated with GERD for the eight week treatment period. No significant additional benefit from lansoprazole 30 mg once daily was observed [see Indications and Usage ( 1.7) ].
Erosive Esophagitis
In a U.S. multicenter, double-blind, placebo-controlled study of 269 patients entering with an endoscopic diagnosis of esophagitis with mucosal grading of two or more and grades three and four signifying erosive disease, the percentages of patients with healing are presented in Table 16:
Table 16 Erosive Esophagitis Healing Rates
Lansoprazole
Placebo
- * (p ≤ 0.001) versus placebo.
- † (p ≤ 0.05) versus lansoprazole 15 mg.
15 mg daily
30 mg daily
60 mg daily
Week
(N=69)
(N=65)
(N=72)
(N=63)
4
67.6% *
81.3% *†
80.6% *†
32.8%
6
87.7% *
95.4% *
94.3% *
52.5%
8
90.9% *
95.4% *
94.4% *
52.5%
In this study, all lansoprazole groups reported significantly greater relief of heartburn and less day and night abdominal pain along with fewer days of antacid use and fewer antacid tablets taken per day than the placebo group.
Although all doses were effective, the earlier healing in the higher two doses suggests 30 mg daily as the recommended dose.
Lansoprazole was also compared in a U.S. multicenter, double-blind study to a low dose of ranitidine in 242 patients with erosive reflux esophagitis. Lansoprazole at a dose of 30 mg was significantly more effective than ranitidine 150 mg twice daily as shown below (Table 17).
Table 17Erosive Esophagitis Healing Rates Week
Lansoprazole
30 mg daily
(N=115)
Ranitidine
150 mg twice daily
(N=127)
- * (p ≤ 0.001) versus ranitidine.
2
66.7% *
38.7%
4
82.5% *
52%
6
93% *
67.8%
8
92.1% *
69.9%
In addition, patients treated with lansoprazole reported less day and nighttime heartburn and took less antacid tablets for fewer days than patients taking ranitidine 150 mg twice daily.
Although this study demonstrates effectiveness of lansoprazole in healing erosive esophagitis, it does not represent an adequate comparison with ranitidine because the recommended ranitidine dose for esophagitis is 150 mg four times daily, twice the dose used in this study.
In the two trials described and in several smaller studies involving patients with moderate to severe erosive esophagitis, lansoprazole produced healing rates similar to those shown above.
In a U.S. multicenter, double-blind, active-controlled study, 30 mg of lansoprazole was compared with ranitidine 150 mg twice daily in 151 patients with erosive reflux esophagitis that was poorly responsive to a minimum of 12 weeks of treatment with at least one H 2-receptor antagonist given at the dose indicated for symptom relief or greater, namely, cimetidine 800 mg/day, ranitidine 300 mg/day, famotidine 40 mg/day or nizatidine 300 mg/day. Lansoprazole 30 mg was more effective than ranitidine 150 mg twice daily in healing reflux esophagitis, and the percentage of patients with healing were as follows. This study does not constitute a comparison of the effectiveness of histamine H 2-receptor antagonists with lansoprazole, as all patients had demonstrated unresponsiveness to the histamine H 2-receptor antagonist mode of treatment. It does indicate, however, that lansoprazole may be useful in patients failing on a histamine H 2-receptor antagonist (Table 18) [see Indications and Usage ( 1.7) ].
Table 18Reflux Esophagitis Healing Rates in Patients Poorly Responsive to Histamine H 2-Receptor Antagonist Therapy Week
Lansoprazole
30 mg daily
(N=100)
Ranitidine
150 mg twice daily
(N=51)
- * (p ≤ 0.001) versus ranitidine.
4
8
74.7% *
83.7% *
42.6%
32%
Long-Term Maintenance Treatment of Erosive Esophagitis
Two independent, double-blind, multicenter, controlled trials were conducted in patients with endoscopically confirmed healed esophagitis. Patients remained in remission significantly longer and the number of recurrences of erosive esophagitis was significantly less in patients treated with lansoprazole than in patients treated with placebo over a 12 month period (Table 19)
Table 19 Endoscopic Remission Rates
Percent in Endoscopic Remission
%=Life Table Estimate
- * (p ≤ 0.001) versus placebo.
Trial
Drug
No. of Pts.
0 to 3 mo.
0 to 6 mo.
0 to 12 mo.
#1
Lansoprazole 15 mg daily
59
83% *
81% *
79% *
Lansoprazole 30 mg daily
56
93% *
93% *
90% *
Placebo
55
31%
27%
24%
#2
Lansoprazole 15 mg daily
50
74% *
72% *
67% *
Lansoprazole 30 mg daily
49
75% *
72% *
55% *
Placebo
47
16%
13%
13%
Regardless of initial grade of erosive esophagitis, lansoprazole 15 mg and 30 mg were similar in maintaining remission.
In a U.S., randomized, doubleblind, study, lansoprazole 15 mg daily (n = 100) was compared with ranitidine 150 mg twice daily (n = 106), at the recommended dosage, in patients with endoscopically-proven healed erosive esophagitis over a 12 month period. Treatment with lansoprazole resulted in patients remaining healed (Grade 0 lesions) of erosive esophagitis for significantly longer periods of time than those treated with ranitidine (p < 0.001). In addition, lansoprazole was significantly more effective than ranitidine in providing complete relief of both daytime and nighttime heartburn. Patients treated with lansoprazole remained asymptomatic for a significantly longer period of time than patients treated with ranitidine [see Indications and Usage ( 1.8) ].
Pathological Hypersecretory Conditions Including Zollinger-Ellison Syndrome
In open studies of 57 patients with pathological hypersecretory conditions, such as Zollinger-Ellison syndrome (ZES) with or without multiple endocrine adenomas, lansoprazole significantly inhibited gastric acid secretion and controlled associated symptoms of diarrhea, anorexia and pain. Doses ranging from 15 mg every other day to 180 mg per day maintained basal acid secretion below 10 mEq/hr in patients without prior gastric surgery and below 5 mEq/hr in patients with prior gastric surgery.
Initial doses were titrated to the individual patient need, and adjustments were necessary with time in some patients [see Dosage and Administration ( 2.1) ]. Lansoprazole was well tolerated at these high dose levels for prolonged periods (greater than four years in some patients). In most ZES patients, serum gastrin levels were not modified by lansoprazole. However, in some patients, serum gastrin increased to levels greater than those present prior to initiation of lansoprazole therapy [see Indications and Usage ( 1.9) ].
- 15 REFERENCES
-
16 HOW SUPPLIED/STORAGE AND HANDLING
Lansoprazole Delayed-release Capsules USP, 30 mg are enteric-coated pellets filled in size '1' hard gelatin capsules with standard pink opaque colored cap printed with "ZA -51" in black ink and white opaque body printed with "30 mg" in black ink and are supplied as follows:
NDC: 68071-3019-3 bottle of 30
NDC: 68071-3019-7 bottle of 7
NDC: 68071-3019-6 bottle of 60
Storage
Store at 20 ο to 25 οC (68 ο to 77 οF) [See USP Controlled Room Temperature]. Protect from moisture.
Dispense in a tight container.
-
MEDICATION GUIDE
Advise the patient to read the FDA-approved patient labeling (Medication Guide and Instructions for Use).
Adverse Reactions
Advise patients to report to their healthcare provider if they experience any signs or symptoms consistent with:
- Hypersensitivity Reactions [see Contraindications
- Acute Interstitial Nephritis [see Warnings and Precautions > ]
-
Clostridium difficile-Associated Diarrhea [see
Warnings and
- Bone Fracture [see Warnings and Precautions ( ]
-
Cutaneous and Systemic Lupus Erythematosus [see
Warnings and
-
Cyanocobalamin (Vitamin B-12) Deficiency [see
Warnings and Precautions
- Hypomagnesemia [see Warnings and Precautions ( 5.7) ]
-
Cyanocobalamin (Vitamin B-12) Deficiency [see
Warnings and Precautions
Lansoprazole is available as capsules in 15 mg and 30 mg strengths. Direction for use specific to the route and available methods of administration of this dosage form is presented below [see Dosage and Administration ( 2.3) ].
- Lansoprazole should be taken before eating.
- Lansoprazole delayed-release capsules SHOULD NOT BE CRUSHED OR CHEWED.
Lansoprazole Delayed-release Capsules – Oral Administration
- Lansoprazole delayed-release capsules should be swallowed whole.
- Alternatively, for patients who have difficulty swallowing capsules, lansoprazole delayed-release capsules can be opened and administered as follows:
о Sprinkle intact granules on one tablespoon of either applesauce, ENSURE pudding, cottage cheese, yogurt or strained pears.
о Swallow immediately.
- Lansoprazole delayed-release capsules may also be emptied into a small volume of either apple juice, orange juice or tomato juice and administered as follows:
о Sprinkle intact granules into a small volume of either apple juice, orange juice or tomato juice (60 mL – approximately two ounces).
о Mix briefly.
о Swallow immediately.
о To ensure complete delivery of the dose, the glass should be rinsed with two or more volumes of juice and the contents swallowed immediately.
Lansoprazole delayed-release capsules - Nasogastric Tube (≥ 16 French) Administration
- For patients who have a nasogastric tube in place, lansoprazole delayed-release capsules can be administered as follows:
о Mix intact granules into 40 mL of apple juice. DO NOT USE OTHER LIQUIDS.
о Inject through the nasogastric tube into the stomach.
о Flush with additional apple juice to clear the tube.
USE IN OTHER FOODS AND LIQUIDS HAS NOT BEEN STUDIED CLINICALLY AND IS THEREFORE NOT RECOMMENDED.
@CLOtest ® is a registered trademark of Delta West Ltd., Bentley, Australia.
- SPL UNCLASSIFIED SECTION
-
PATIENT PACKAGE INSERT
Lansoprazole
(lan-SO-pruh-zole)
Delayed-release Capsules, USP
Read this Medication Guide before you start taking lansoprazole delayed-release capsules and each time you get a refill. There may be new information. This information does not take the place of talking to your doctor about your medical condition or your treatment.
What is the most important information that I should know about lansoprazole delayed-release capsules?
Lansoprazole delayed-release capsules may help your acid-related symptoms, but you could still have serious stomach problems. Talk with your doctor.
Lansoprazole delayed-release capsules can cause serious side effects, including:
- A type of kidney problem (acute interstitial nephritis). Some people who take proton pump inhibitor (PPI) medicines, including lansoprazole, may develop a kidney problem called acute interstitial nephritis, that can happen at any time during treatment with PPI medicines. Call your doctor right away if you have a decrease in the amount that you urinate or if you have blood in your urine.
- Diarrhea. Lansoprazole delayed-release capsules may increase your risk of getting severe diarrhea. This diarrhea may be caused by an infection ( Clostridium difficile ) in your intestines. Call your doctor right away if you have watery stool, stomach pain, and fever that does not go away.
- Bone fractures. People who take multiple daily doses of PPI medicines for a long period of time (a year or longer) may have an increased risk of fractures of the hip, wrist or spine. You should take lansoprazole delayed-release capsules exactly as prescribed, at the lowest dose possible for your treatment and for the shortest time needed. Talk to your doctor about your risk of bone fracture if you take lansoprazole delayed-release capsules.
- Certain types of lupus erythematosus . Lupus erythematosus is an autoimmune disorder (the body's immune cells attack other cells or organs in the body). Some people who take PPI medicines, including lansoprazole, may develop certain types of lupus erythematosus or have worsening of the lupus they already have. Call your doctor right away if you have new or worsening joint pain or a rash on your cheeks or arms that gets worse in the sun.
Lansoprazole delayed-release capsules can have other serious side effects. See "What are the possible side effects of lansoprazole delayed-release capsules?"
What is lansoprazole delayed-release capsule?
Lansoprazole delayed-release capsule is a prescription medicine called a proton pump inhibitor (PPIs). Lansoprazole delayed-release capsule reduces the amount of acid in your stomach.
Lansoprazole delayed-release capsule is used in adults:
- for 4 weeks for the healing and symptom relief of duodenal ulcers. The duodenal area is the area where food passes when it leaves the stomach.
- with certain antibiotics to treat an infection called H. pylori . Sometimes H. pylori bacteria can cause duodenal ulcers. The infection needs to be treated to prevent ulcers from coming back.
- for continued healing of duodenal ulcers.
- for up to 8 weeks to heal stomach ulcers.
- for up to 8 weeks to heal stomach ulcers in some people taking pain medicines called non-steroidal anti-inflammatory drugs (NSAIDs).
- for reducing the risk of stomach ulcers in some people taking NSAIDs.
- for up to 8 weeks for the relief of heartburn and other symptoms of gastroesophageal reflux disease (GERD).
GERD happens when acid in your stomach backs up into the tube (esophagus) that connects your mouth to your stomach. This may cause a burning feeling in your chest or throat, sour taste or burping.
- for 8 weeks to heal the acid-related damage to the lining of the esophagus (called erosive esophagitis) and to relieve symptoms. If needed, your doctor may prescribe another 8 weeks of lansoprazole delayed-release capsules.
- for continued healing of erosive esophagitis.
- for the long-term treatment of conditions where your stomach makes too much acid. This includes a condition called Zollinger-Ellison syndrome.
Lansoprazole delayed-release capsule is used in children and adolescents (ages 1 to 17):
- for up to 12 weeks to treat GERD and erosive esophagitis in children 1 to 11 years old.
- for up to 8 weeks to treat GERD and erosive esophagitis in adolescents 12 to 17 years old.
Lansoprazole delayed-release capsule is not effective for symptoms of GERD in children under the age of 1 year.
Who should not take lansoprazole delayed-release capsules?
- Do not take lansoprazole delayed-release capsules if you are allergic to lansoprazole or any of the other ingredients in lansoprazole delayed-release capsules. See the end of this Medication Guide for a complete list of ingredients in lansoprazole delayed release capsules.
What should I tell my doctor before taking lansoprazole delayed-release capsules?
Before you take lansoprazole delayed-release capsules, tell your doctor if you:
- have been told that you have low magnesium levels in your blood.
- have liver problems
- have any other medical conditions
- are pregnant or plan to become pregnant. It is not known if lansoprazole delayedrelease capsules will harm your unborn baby.
- are breastfeeding or plan to breastfeed. It is not known if lansoprazole passes into your breast milk. You and your doctor should decide if you will take lansoprazole delayed-release capsules or breastfeed. You should not do both. Talk to your doctor about the best way to feed your baby if you take lansoprazole delayed-release capsules.
Tell your doctor about all the medicines you take, including prescription and nonprescription drugs, vitamins, and herbal supplements. Lansoprazole delayed-release capsules may affect how other medicines work, and other medicines may affect how lansoprazole delayed-release capsules work.
Especially tell your doctor if you take:
- atazanavir (Reyataz ®$)
- nelfinavir (Viracept ®$)
- erlotinib (Tarceva ®$)
- digoxin (Lanoxin ®$)
- a product that contains iron
- ketoconazole (Nizoral ®$)
- warfarin (Coumadin ®$, Jantoven ®$)
- tacrolimus (Prograf ®$)
- theophylline (Theo-24 ®$, Elixophyllin ®$, Theochron ®$, Theolair ®$)
- an antibiotic that contains ampicillin or clarithromycin
- methotrexate
- mycophenolate mofetil (Cellcept ®$)
Ask your doctor or pharmacist for a list of these medicines if you are not sure.
Know the medicines that you take. Keep a list of them to show your doctor and pharmacist when you get a new medicine.
How should I take lansoprazole delayed-release capsules?
- Take lansoprazole delayed-release capsules exactly as prescribed by your doctor.
- Do not change your dose or stop taking lansoprazole delayed-release capsules without talking to your doctor.
- You should take lansoprazole delayed-release capsules before eating.
- Lansoprazole Delayed-Release Capsules:
○ You should swallow lansoprazole delayed-release capsules whole.
○ Do not crush or chew lansoprazole delayed-release capsules.
○ If you have trouble swallowing a whole capsule, you can open the capsule and take the contents with certain foods or juices. See the "Instructions for Use" at the end of this Medication Guide for instructions on how to take lansoprazole delayed-release capsules with certain foods and juices.
○ See the "Instructions for Use" at the end of this Medication Guide for instructions on how to mix and give lansoprazole delayed-release capsules through a nasogastric tube.
- If you miss a dose, take it as soon as you remember. If it is almost time for your next dose, skip the missed dose. Just take the next dose at your regular time. Do not take 2 doses at the same time.
- If you take too much lansoprazole, call your doctor right away.
What are the possible side effects of lansoprazole delayed-release capsules?
Lansoprazole delayed-release capsules can cause serious side effects, including:
- See "What is the most important information that I should know about lansoprazole delayed-release capsules?"
- Vitamin B-12 deficiency. Lansoprazole delayed-release capsules reduce the amount of acid in your stomach. Stomach acid is needed to absorb vitamin B-12 properly. Talk with your doctor about the possibility of vitamin B-12 deficiency if you have been on lansoprazole delayed-release capsules for a long time (more than 3 years).
- Low magnesium levels in your body. This problem can be serious. Low magnesium can happen in some people who take a PPI medicine for at least 3 months. If low magnesium levels happen, it is usually after a year of treatment. You may or may not have symptoms of low magnesium.
Tell your doctor right away if you develop any of these symptoms:
- seizures
- dizziness
- abnormal or fast heartbeat
- jitteriness
- jerking movements or shaking (tremors)
- muscle weakness
- spasms of the hands and feet
- cramps or muscle aches
- spasm of the voice box
Your doctor may check the level of magnesium in your body before you start taking lansoprazole delayed-release capsules, or during treatment; if you will be taking lansoprazole delayed-release capsules for a long period of time. The most common side effects of lansoprazole delayed-release capsules in adults and children include:
- diarrhea
- stomach pain
- nausea
- constipation
- headache
- Serious allergic reactions. Tell your doctor if you get any of the following symptoms with lansoprazole delayed-release capsules.
- rash
- face swelling
- throat tightness
- difficulty breathing
Your doctor may stop lansoprazole delayed-release capsules if these symptoms happen.
Tell your doctor if you have any side effect that bothers you or that does not go away.
These are not all the possible side effects of lansoprazole delayed-release capsules. For more information, ask your doctor or pharmacist.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
How should I store lansoprazole delayed-release capsules?
- Store at 20° to 25°C (68° to 77°F) Protect from moisture.
Keep lansoprazole delayed-release capsules and all medicines out of the reach of children.
General information about lansoprazole delayed-release capsules
Medicines are sometimes prescribed for conditions other than those listed in a Medication Guide. Do not use lansoprazole delayed-release capsules for conditions for which it was not prescribed. Do not give lansoprazole delayed-release capsules to other people, even if they have the same symptoms you have. It may harm them.
This Medication Guide summarizes the most important information about lansoprazole delayed-release capsules. If you would like more information, talk with your doctor. You can ask your doctor or pharmacist for information about lansoprazole delayed-release capsules that is written for healthcare professionals.
Please address medical inquiries to, (MedicalAffairs@zydususa.com) Tel.: 1-877-993-8779.
What are the ingredients in Lansoprazole Delayed-release Capsules?
Active ingredient: lansoprazole, USP
Inactive ingredients:
Corn starch, D&C red # 28, FD&C blue # 1, FD&C red # 40, gelatin, hydroxypropyl cellulose, hypromellose, low substituted hydroxypropyl cellulose, magnesium carbonate heavy powder, methacrylic acid copolymer dispersion, polyethylene glycol, polysorbate 80, sucrose, sugar spheres, talc and titanium dioxide. The capsule shell is printed with black pharmaceutical ink which contains following ingredients: black iron oxide, butyl alcohol, dehydrated alcohol, isopropyl alcohol, potassium hydroxide, propylene glycol, purified water, shellac and strong ammonia solution.
This Medication Guide has been approved by the U.S. Food and Drug Administration.
Manufactured by:
Cadila Healthcare Ltd.
Ahmedabad, India
Distributed by:
Zydus Pharmaceuticals USA Inc.
Pennington, NJ 08534
Rev.: 11/16
Lansoprazole Delayed-release Capsules, USP
Lansoprazole Delayed-release Capsules, USP
- Swallow lansoprazole delayed-release capsules whole. Do not crush or chew them.
- You should take lansoprazole before eating.
- Lansoprazole Delayed-release Capsule with certain food
You can only use applesauce, ENSURE pudding, cottage cheese, yogurt or strained pears.
- Open the capsule.
- Sprinkle the granules on one tablespoon of either applesauce, ENSURE pudding, cottage cheese, yogurt or strained pears.
- Swallow right away.
- Lansoprazole Delayed-release Capsule with certain juices
You can only use apple juice, orange juice or tomato juice.
- Open the capsule.
- Sprinkle the granules into 60 mL (about ¼ cup) of either apple juice, orange juice or tomato juice.
- Stir.
- Swallow right away.
- To make sure that the entire dose is taken, rinse the glass with 1/2 cup or more of juice to get out any leftover granules. Swallow the juice right away.
Lansoprazole Delayed-release Capsules through a nasogastric tube (NG tube) 16 French or larger, as prescribed by your doctor
You can only use apple juice.
- Open the capsule and empty the granules into a syringe.
- Do not break or crush the granules.
- Mix with 40 mL of apple juice. Do not use other liquids.
- Attach the syringe to the NG tube and give the medicine in the syringe through the NG tube into the stomach.
- After giving the granules, flush the NG tube with more apple juice to clear the tube.
Lansoprazole should not be used in foods or liquids not listed above.
How should I store lansoprazole?
- Store at 20 οto 25 οC (68 οto 77 οF) Protect from moisture.
Keep lansoprazole and all medicines out of the reach of children.
This Instruction for Use has been approved by the U.S. Food and Drug Administration.
$ are the registered trademark of their respective owners.
This product's package insert may have been updated. For current package insert, please visit www.zydususa.com.
- SPL UNCLASSIFIED SECTION
- PRINCIPAL DISPLAY PANEL
-
INGREDIENTS AND APPEARANCE
LANSOPRAZOLE
lansoprazole capsule, delayed release pelletsProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 68071-3019(NDC:68382-544) Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength LANSOPRAZOLE (UNII: 0K5C5T2QPG) (LANSOPRAZOLE - UNII:0K5C5T2QPG) LANSOPRAZOLE 30 mg Inactive Ingredients Ingredient Name Strength GELATIN (UNII: 2G86QN327L) SUCROSE (UNII: C151H8M554) TALC (UNII: 7SEV7J4R1U) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) POTASSIUM HYDROXIDE (UNII: WZH3C48M4T) HYDROXYPROPYL CELLULOSE, LOW SUBSTITUTED (UNII: 2165RE0K14) STARCH, CORN (UNII: O8232NY3SJ) ALCOHOL (UNII: 3K9958V90M) AMMONIA (UNII: 5138Q19F1X) BUTYL ALCOHOL (UNII: 8PJ61P6TS3) D&C RED NO. 28 (UNII: 767IP0Y5NH) FD&C BLUE NO. 1 (UNII: H3R47K3TBD) FD&C RED NO. 40 (UNII: WZB9127XOA) FERROSOFERRIC OXIDE (UNII: XM0M87F357) HYDROXYPROPYL CELLULOSE (1600000 WAMW) (UNII: RFW2ET671P) HYPROMELLOSES (UNII: 3NXW29V3WO) ISOPROPYL ALCOHOL (UNII: ND2M416302) SHELLAC (UNII: 46N107B71O) MAGNESIUM CARBONATE (UNII: 0E53J927NA) METHACRYLIC ACID (UNII: 1CS02G8656) POLYETHYLENE GLYCOL, UNSPECIFIED (UNII: 3WJQ0SDW1A) POLYSORBATE 80 (UNII: 6OZP39ZG8H) PROPYLENE GLYCOL (UNII: 6DC9Q167V3) WATER (UNII: 059QF0KO0R) Product Characteristics Color pink (PINK) , white (WHITE) Score no score Shape CAPSULE (CAPSULE) Size 20mm Flavor Imprint Code ZA;51;30mg Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 68071-3019-6 60 in 1 BOTTLE; Type 0: Not a Combination Product 03/03/2017 2 NDC: 68071-3019-7 7 in 1 BOTTLE; Type 0: Not a Combination Product 03/03/2017 3 NDC: 68071-3019-3 30 in 1 BOTTLE; Type 0: Not a Combination Product 03/03/2017 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA202366 08/23/2013 Labeler - NuCare Pharmaceuticals, Inc. (010632300) Establishment Name Address ID/FEI Business Operations NuCare Pharmaceuticals, Inc. 010632300 repack(68071-3019)
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.