SYMLINPEN- pramlintide acetate injection
SymlinPen by
Drug Labeling and Warnings
SymlinPen by is a Prescription medication manufactured, distributed, or labeled by AstraZeneca Pharmaceuticals LP, AstraZeneca PLC. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use SYMLIN safely and effectively. See full prescribing information for SYMLIN.
SYMLIN® (pramlintide acetate) injection for subcutaneous use
Initial U.S. Approval: 2005WARNING: SEVERE HYPOGLYCEMIA
See full prescribing information for complete boxed warning.
INDICATIONS AND USAGE
SYMLIN is an amylin analog indicated for patients with type 1 or type 2 diabetes who use mealtime insulin and have failed to achieve desired glycemic control despite optimal insulin therapy (1).
DOSAGE AND ADMINISTRATION
- Upon initiation of SYMLIN, reduce mealtime insulin dose by 50%. Monitor glucoses frequently and individualize subsequent insulin dose adjustments (2.1).
- Type 1 Diabetes: Start at 15 mcg subcutaneously before major meals. Increase in 15 mcg increments to a maximum premeal dose of 30 or 60 mcg; if not tolerated, reduce to 30 mcg, as tolerated (2.2).
- Type 2 Diabetes: Start at 60 mcg subcutaneously before major meals then increase to 120 mcg before meals, as tolerated (2.2).
- Wait at least 3 days between dose titrations to minimize nausea (2.1).
DOSAGE FORMS AND STRENGTHS
CONTRAINDICATIONS
WARNINGS AND PRECAUTIONS
- Severe hypoglycemia: Increased risk particularly for type 1 diabetes. Upon initiation of SYMLIN, reduce mealtime insulin dose by 50% and frequently monitor blood glucoses (5.2).
- Never share a SymlinPen between patients, even if the needle is changed (5.3).
- Do not mix SYMLIN and insulin: Mixing can alter the pharmacokinetics of both products. Administer as separate injections (5.4, 7.1).
- Slows gastric emptying: Administer concomitant oral medications at least 1 hour before or 2 hours after SYMLIN if rapid onset or threshold concentration is critical (5.6, 7.2).
ADVERSE REACTIONS
- Most common adverse reactions (incidence ≥5% and higher incidence than placebo): nausea, vomiting, anorexia, headache (6.1).
To report SUSPECTED ADVERSE REACTIONS, contact AstraZeneca at 1-800-236-9933 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide.
Revised: 12/2019
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
WARNING: SEVERE HYPOGLYCEMIA
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Important Considerations Pertaining to SYMLIN and Insulin Dose Adjustments
2.2 Patients with Type 2 Diabetes Using Mealtime Insulin
2.3 Patients with Type 1 Diabetes
2.4 Administration
2.5 Discontinuation of Therapy
2.6 Preparation and Handling
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Patient Selection
5.2 Hypoglycemia
5.3 Never Share a SymlinPen Between Patients
5.4 Never Mix SYMLIN and Insulin
5.5 Concomitantly Administered Oral Medications
5.6 Medications that Affect Gastrointestinal Motility
5.7 Allergy
6 ADVERSE REACTIONS
6.1 Clinical Trial Experience
6.2 Postmarketing Experience
7 DRUG INTERACTIONS
7.1 Insulin
7.2 Oral Medications
7.3 Drugs Affecting Gastrointestinal Motility
7.4 Drugs Affecting Glucose Metabolism
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.4 Pediatric Use
8.5 Geriatric Use
8.6 Renal Impairment
8.7 Hepatic Impairment
8.8 Gender
8.9 Race/Ethnicity
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
14.1 Type 1 Diabetes
14.2 Type 2 Diabetes
16 HOW SUPPLIED/STORAGE AND HANDLING
Storage and Handling
17 PATIENT COUNSELING INFORMATION
SymlinPen® (SĬM-lĭnPεn) 120
- * Sections or subsections omitted from the full prescribing information are not listed.
-
BOXED WARNING
(What is this?)
WARNING: SEVERE HYPOGLYCEMIA
SYMLIN use with insulin increases the risk of severe hypoglycemia, particularly in patients with type 1 diabetes. When severe hypoglycemia occurs, it is seen within 3 hours following a SYMLIN injection. Serious injuries may occur if severe hypoglycemia occurs while operating a motor vehicle, heavy machinery, or while engaging in other high-risk activities. Appropriate patient selection, careful patient instruction, and insulin dose reduction are critical elements for reducing this risk.
- 1 INDICATIONS AND USAGE
-
2 DOSAGE AND ADMINISTRATION
2.1 Important Considerations Pertaining to SYMLIN and Insulin Dose Adjustments
SYMLIN dosage differs depending on whether the patient has type 1 or type 2 diabetes [see Dosage and Administration (2.2, 2.3)].
SYMLIN should be used only in patients who can fully understand and adhere to proper insulin adjustments and glucose monitoring.
Insulin and SYMLIN dose adjustments should be made only as directed by a healthcare professional skilled in the use of insulin.
When initiating SYMLIN, reduce mealtime insulin doses, including premixed insulins, by 50% to reduce the risk of hypoglycemia.
To reduce the risk of nausea, wait at least 3 days before titrating SYMLIN to the next dose increment.
Monitor blood glucoses frequently, including pre- and post-meals and at bedtime, particularly when initiating SYMLIN or increasing the SYMLIN dose. After the initial 50% reduction in mealtime insulin dose, individualize insulin dose adjustments based on glycemic control and tolerability (e.g., if nausea occurs it may affect the dose of insulin required). An increased frequency of mild-to-moderate hypoglycemia should be viewed as a warning sign of increased risk for severe hypoglycemia.
If SYMLIN therapy is discontinued for any reason (e.g., surgery or illnesses), the same initiation protocol should be followed when SYMLIN therapy is reinstituted [see Dosage and Administration (2.2)].
2.2 Patients with Type 2 Diabetes Using Mealtime Insulin
Reduce mealtime insulin doses (including premixed insulins) by 50%, then initiate SYMLIN at 60 mcg subcutaneously, injecting immediately prior to each major meal.
Increase the SYMLIN dose from 60 to 120 mcg prior to each major meal when no clinically significant nausea has occurred for at least 3 days.
If significant nausea persists at the 120 mcg dose, the SYMLIN dose should be decreased to 60 mcg.
2.3 Patients with Type 1 Diabetes
Reduce mealtime insulin doses by 50%, then initiate SYMLIN at 15 mcg subcutaneously, injecting immediately prior to each major meal.
Increase the SYMLIN dose to the next increment (30, 45, or 60 mcg) when no clinically significant nausea has occurred for at least 3 days.
If significant nausea persists at the 45 or 60 mcg dose level, the SYMLIN dose should be decreased to 30 mcg. If the 30 mcg dose is not tolerated, discontinuation of SYMLIN therapy should be considered.
2.4 Administration
SYMLIN should be administered subcutaneously immediately prior to each major meal (≥250 kcal or containing ≥30 grams of carbohydrate).
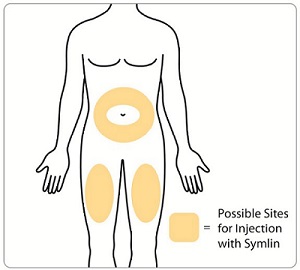
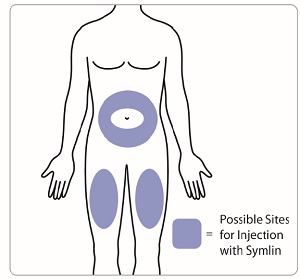
SYMLIN should be at room temperature before injecting to reduce potential injection site reactions. Each SYMLIN dose should be administered subcutaneously into the abdomen or thigh. Administration into the arm is not recommended because of variable absorption. Injection sites should be rotated so that the same site is not used repeatedly. The injection site selected should also be distinct from the site chosen for any concomitant insulin injection.
SYMLIN and insulin should always be administered as separate injections.
SYMLIN should not be mixed with any type of insulin.
If a SYMLIN dose is missed, wait until the next scheduled dose and administer the usual amount.
2.5 Discontinuation of Therapy
SYMLIN therapy should be discontinued if there is:
- recurrent unexplained hypoglycemia that requires medical assistance.
- persistent clinically significant nausea.
- noncompliance with self-monitoring of blood glucose concentrations.
- noncompliance with insulin dose adjustments.
- noncompliance with scheduled healthcare provider contacts or recommended clinic visits.
- 3 DOSAGE FORMS AND STRENGTHS
- 4 CONTRAINDICATIONS
-
5 WARNINGS AND PRECAUTIONS
5.1 Patient Selection
Proper patient selection is critical to the safe and effective use of SYMLIN. Before initiating SYMLIN, the patient's HbA1c, recent blood glucose monitoring data, history of insulin-induced hypoglycemia, current insulin regimen, and body weight should be reviewed. SYMLIN therapy should only be considered in patients with type 1 diabetes or patients with type 2 diabetes using mealtime insulin who fulfill the following criteria:
- have failed to achieve adequate glycemic control despite individualized insulin management.
- are receiving ongoing care under the guidance of a healthcare professional skilled in the use of insulin and supported by the services of diabetes educator(s).
Patients meeting any of the following criteria should NOT be considered for SYMLIN therapy:
- poor compliance with current insulin regimen.
- poor compliance with prescribed self blood glucose monitoring.
- have a HbA1c >9%.
- recurrent severe hypoglycemia requiring assistance during the past 6 months.
- presence of hypoglycemia unawareness.
- confirmed diagnosis of gastroparesis.
- require the use of drugs that stimulate gastrointestinal motility.
- pediatric patients.
SYMLIN should be prescribed with caution to persons with visual or dexterity impairment.
5.2 Hypoglycemia
SYMLIN alone does not cause hypoglycemia. However, SYMLIN is indicated to be coadministered with mealtime insulin therapy, and in this setting there is an increased risk of severe hypoglycemia, particularly in patients with type 1 diabetes. If severe hypoglycemia associated with SYMLIN occurs, it is usually seen within the first 2 to 3 hours following a SYMLIN injection. If severe hypoglycemia occurs while operating a motor vehicle, heavy machinery, or while engaging in other high-risk activities, serious injuries or death may occur. Therefore, when introducing SYMLIN therapy, appropriate precautions need to be taken to avoid increasing the risk for severe hypoglycemia. These precautions include frequent monitoring of pre- and post-meal glucose combined with an initial 50% reduction in doses of mealtime insulin [see Dosage and Administration (2.1, 2.2)].
Early warning symptoms of hypoglycemia may be different or less pronounced under certain conditions, such as longstanding diabetes; diabetic neuropathy; use of medications such as beta-blockers, clonidine, guanethidine, or reserpine; or intensified glycemic control.
The addition of any anti-diabetic medication, such as SYMLIN, to an existing regimen of one or more anti-diabetic medications (e.g., sulfonylurea), or other medications that can increase the risk of hypoglycemia may necessitate further insulin dose adjustments and particularly close monitoring of blood glucose.
5.3 Never Share a SymlinPen Between Patients
SymlinPen must never be shared between patients, even if the needle is changed. Pen-sharing poses a risk for transmission of blood-borne pathogens.
5.4 Never Mix SYMLIN and Insulin
Mixing SYMLIN and insulin can alter the pharmacokinetics of both products which may result in inadequate glucose control or hypoglycemia. Therefore, SYMLIN and insulin must always be administered as separate injections and should never be mixed [see Drug Interactions (7.1) and Clinical Pharmacology (12.3)].
5.5 Concomitantly Administered Oral Medications
SYMLIN slows gastric emptying, which may delay the absorption of concomitantly administered oral medications. Administer the concomitant oral medication at least 1 hour prior to SYMLIN injection or 2 hours after SYMLIN injection if the rapid onset or threshold concentration of the concomitant medication is a critical determinant of its effectiveness (such as with analgesics, antibiotics, and oral contraceptives) [see Drug Interactions (7.2) and Clinical Pharmacology (12.3)].
5.6 Medications that Affect Gastrointestinal Motility
SYMLIN slows gastric emptying. SYMLIN is not recommended for patients taking other medications that alter gastrointestinal motility [see Drug Interactions (7.3)].
5.7 Allergy
Local Allergy
Patients may experience erythema, edema, or pruritus at the site of injection. These minor reactions usually resolve in a few days to a few weeks. In some instances, these reactions may be related to factors other than SYMLIN, such as irritants in a skin cleansing agent or improper injection technique.
-
6 ADVERSE REACTIONS
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
6.1 Clinical Trial Experience
Adverse Reactions (Excluding Hypoglycemia)
Adverse reactions (excluding hypoglycemia, which is discussed separately below) commonly associated with SYMLIN when coadministered with a fixed dose of insulin in the 26- to 52-week, placebo-controlled trials in patients with type 1 diabetes and patients with type 2 diabetes on mealtime insulin are presented in Table 1 and Table 2, respectively.
Table 1: Patients with Type 1 Diabetes: Common Adverse Reactions (Incidence ≥5% and Greater Incidence with SYMLIN Compared to Placebo) in 3 Pooled Placebo-Controlled Trials Long-Term, Placebo-Controlled Studies SYMLIN 30 or 60 mcg
3 Times Daily + InsulinPlacebo + Insulin (N=716)
%(N=538)
%- * Examples of inflicted injury included among others, abrasions, bruises, burns, fractures, lacerations, and muscle strains.
Nausea
48
17
Anorexia
17
2
Inflicted Injury*
14
10
Vomiting
11
7
Arthralgia
7
5
Fatigue
7
4
Allergic Reaction
6
5
Dizziness
5
4
Table 2: Patients with Type 2 Diabetes on Insulin: Common Adverse Reactions (Incidence ≥5% and Greater Incidence with SYMLIN Compared to Placebo) in 2 Pooled Placebo-Controlled Trials Long-Term, Placebo-Controlled Studies SYMLIN 120 mcg
2 Times Daily + InsulinPlacebo + Insulin (N=292)
%(N=284)
%Nausea
28
12
Headache
13
7
Anorexia
9
2
Vomiting
8
4
Abdominal pain
8
7
Fatigue
7
4
Dizziness
6
4
Cough
6
4
Pharyngitis
5
2
Most adverse reactions were gastrointestinal in nature. The incidence of nausea is higher at the beginning of SYMLIN treatment and decreases with time in most patients. Gradual titration of the SYMLIN dose minimizes the incidence and severity of nausea [see Dosage and Administration (2)].
Severe Hypoglycemia
Coadministration of SYMLIN with mealtime insulin increases the risk of severe hypoglycemia, particularly in patients with type 1 diabetes [see Boxed Warning and Warnings and Precautions (5.1)].
Two definitions of severe hypoglycemia were used in the SYMLIN clinical trials. Patient-ascertained severe hypoglycemia was defined as an episode of hypoglycemia requiring the assistance of another individual (including help administering oral carbohydrate) or requiring the administration of glucagon, intravenous glucose, or other medical intervention. Medically-assisted severe hypoglycemia was defined as an episode of hypoglycemia that was classified as a serious event by the investigator or that required glucagon, intravenous glucose, hospitalization, paramedic assistance or an emergency room visit. The incidence of severe hypoglycemia during the SYMLIN clinical development program is summarized in Table 3 and Table 4.
Table 3: Incidence and Event Rate of Severe Hypoglycemia in Six-Month, Placebo-Controlled Trials and Dose Titration Trial in Patients with Type 1 Diabetes Long-Term, Placebo-Controlled Studies
(No Insulin Dose-Reduction During Initiation)Placebo-Controlled Dose Titration Study SYMLIN + Insulin Placebo + Insulin SYMLIN + Insulin Placebo + Insulin Severe Hypoglycemia 0 to 3 Months
(n=716)>3 to 6 Months
(n=576)0 to 3 Months
(n=538)>3 to 6 Months
(n=470)0 to 3 Months
(n=148)>3 to 6 Months
(n=133)0 to 3 Months
(n=147)>3 to 6 Months
(n=138)- * Patient-ascertained severe hypoglycemia: Requiring the assistance of another individual (including help ingesting oral carbohydrate) and/or requiring the administration of glucagon injection, intravenous glucose, or other medical intervention.
- † Medically-assisted severe hypoglycemia: Requiring glucagon, intravenous glucose, hospitalization, paramedic assistance, emergency room visit, and/or assessed as a serious adverse event by the investigator.
Patient-Ascertained*
Event Rate (events/patient-year)
1.55
0.82
1.33
1.06
0.69
0.49
0.28
0.3
Subject Incidence (%)
16.8
11.1
10.8
8.7
13.5
10.5
6.1
5.8
Medically-Assisted†
Event Rate (events/patient-year)
0.50
0.27
0.19
0.24
0.14
0.20
0.08
0.15
Subject Incidence (%)
7.3
5.2
3.3
4.3
3.4
4.5
2.0
2.9
Table 4: Incidence and Event Rate of Severe Hypoglycemia in Six-Month, Placebo-Controlled Trials in Patients with Type 2 Diabetes Using Insulin Long-Term, Placebo-Controlled Studies
(No Insulin Dose-Reduction During Initiation)SYMLIN + Insulin Placebo + Insulin Severe Hypoglycemia 0 to 3 Months
(n=292)>3 to 6 Months
(n=255)0 to 3 Months
(n=284)>3 to 6 Months
(n=251)- * Patient-ascertained severe hypoglycemia: Requiring the assistance of another individual (including help ingesting oral carbohydrate) and/or requiring the administration of glucagon injection, intravenous glucose, or other medical intervention.
- † Medically-assisted severe hypoglycemia: Requiring glucagon, intravenous glucose, hospitalization, paramedic assistance, emergency room visit, and/or assessed as a serious adverse event by the investigator.
Patient-Ascertained*
Event Rate (events/patient-year)
0.45
0.39
0.24
0.13
Subject Incidence (%)
8.2
4.7
2.1
2.4
Medically-Assisted†
Event Rate (events/patient-year)
0.09
0.02
0.06
0.07
Subject Incidence (%)
1.7
0.4
0.7
1.2
6.2 Postmarketing Experience
The following adverse reactions have been identified during post-approval use of SYMLIN. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
- Injection site reactions
- Pancreatitis
-
7 DRUG INTERACTIONS
7.1 Insulin
The pharmacokinetic parameters of pramlintide are altered when SYMLIN is mixed in the same syringe with regular, NPH, and 70/30 premixed formulations of recombinant human insulin. SYMLIN and insulin must not be mixed and must be administered as separate injections [see Dosage and Administration (2.4), Warnings and Precautions (5.4), and Clinical Pharmacology (12.3)].
7.2 Oral Medications
SYMLIN has the potential to delay the absorption of concomitantly administered oral medications. When the rapid onset or threshold concentration of a concomitant orally administered medication is a critical determinant of effectiveness (such as with analgesics, antibiotics, and oral contraceptives), the medication should be administered at least 1 hour prior to SYMLIN injection or 2 hours after SYMLIN injection [see Warnings and Precautions (5.5) and Clinical Pharmacology (12.3)].
7.3 Drugs Affecting Gastrointestinal Motility
Due to its effects on gastric emptying, SYMLIN should not be considered for patients taking medications that alter gastrointestinal motility (e.g., anticholinergic agents such as atropine) or medications that slow the intestinal absorption of nutrients (e.g., alpha-glucosidase inhibitors). Patients using these medications have not been studied in SYMLIN clinical trials [see Warnings and Precautions (5.6)].
7.4 Drugs Affecting Glucose Metabolism
The following are examples of medications that may increase the susceptibility to hypoglycemia when administered with SYMLIN: anti-diabetic products, angiotensin converting enzyme (ACE) inhibitors, disopyramide, fibrates, fluoxetine, monoamine oxidase inhibitors, pentoxifylline, salicylates, somatostatin analogs, and sulfonamide antibiotics. SYMLIN and these drugs should be coadministered with caution.
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
Available data from a small number of reports in the manufacturer’s safety database on SYMLIN use in pregnant women are not sufficient to determine a drug-associated risk for major birth defects, miscarriage, or other adverse maternal or fetal outcomes. There are risks to the mother and fetus associated with poorly controlled diabetes in pregnancy (see Clinical Considerations).
Ex-vivo studies using term perfused human, rabbit, and rat placentas indicate that SYMLIN has low potential to cross the maternal/fetal placental barrier. In animal reproduction studies, congenital abnormalities were observed in fetuses of pregnant rats but not in fetuses of pregnant rabbits exposed during organogenesis to pramlintide at 10 times the clinical dose of 360 mcg/day, based on exposure (see Data).
The estimated background risk of major birth defects is 6-10% in women with pre-gestational diabetes with an HbA1c >7 and has been reported to be as high as 20-25% in women with HbA1c >10. The estimated background risk of miscarriage for the indicated population is unknown. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2-4% and 15-20%, respectively.
Clinical Considerations
Disease-associated maternal and/or embryo/fetal risk
Poorly controlled diabetes in pregnancy increases the maternal risk for diabetic ketoacidosis, preeclampsia, spontaneous abortions, preterm delivery, and delivery complications. Poorly controlled diabetes increases the fetal risk for major birth defects, stillbirth, and macrosomia related morbidity.
Data
Animal Data
Developmental and reproductive toxicity studies with SYMLIN were performed in pregnant rats and rabbits. Increases in congenital abnormalities (neural tube defect, cleft palate, exencephaly) were observed in fetuses of pregnant rats administered pramlintide subcutaneously during organogenesis at 0.3 and 1 mg/kg/day (10 and 47 times the human dose of 360 mcg/day based on AUC, respectively), but not at 3mg/kg/day. Administration of pramlintide to pregnant rabbits during organogenesis resulted in maternal toxicity but did not increase fetal malformations at doses up to 0.3 mg/kg/day (9 times the human dose of 360 mcg/day based on AUC).
8.2 Lactation
Risk Summary
There is no data on the presence of pramlintide in human milk, the effects on the breastfed infant, or the effects on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for SYMLIN and any potential adverse effects on the breastfed child from SYMLIN or from the underlying maternal condition.
8.4 Pediatric Use
Safety and effectiveness of SYMLIN in pediatric patients have not been established.
8.5 Geriatric Use
SYMLIN has been studied in patients ranging in age from 15 to 84 years of age, including 769 patients ≥65 to 75 years of age and 87 patients ≥75 years of age. No consistent differences in the efficacy and safety of SYMLIN have been observed in older patients, but greater sensitivity in some older individuals cannot be ruled out. As is recommended for all patients, SYMLIN and insulin regimens should be carefully managed to minimize the risk of severe hypoglycemia.
8.6 Renal Impairment
The dosing requirements for SYMLIN are not altered in patients with mild (creatinine clearance [ClCr] 60-89 mL/min), moderate (ClCr 30-59 mL/min) or severe renal impairment (ClCr 15-29 mL/min). SYMLIN has not been studied in patients with end-stage renal disease [see Clinical Pharmacology (12.3)].
8.7 Hepatic Impairment
SYMLIN use has not been studied in patients with hepatic impairment [see Clinical Pharmacology (12.3)].
8.8 Gender
No consistent differences in the efficacy and safety of SYMLIN have been observed between men and women in SYMLIN clinical trials (n=2799 for male and n=2085 for female).
8.9 Race/Ethnicity
No consistent differences in the efficacy and safety of SYMLIN have been observed among patients of differing race/ethnicity in SYMLIN clinical trials (n=4257 for Caucasian, n=229 for black, n=337 for Hispanic or Latino, and n=61 for Asian and one or more races) although the smaller sample sizes for non-Caucasians, particularly Asians, limit conclusions.
-
10 OVERDOSAGE
Single 10 mg doses of SYMLIN (83 times the maximum recommended dose of 120 mcg for patients with type 2 diabetes) were administered to 3 healthy volunteers. All 3 individuals reported severe nausea associated with vomiting, diarrhea, vasodilatation, and dizziness. No hypoglycemia was reported. Pramlintide has a short half-life (approximately 48 minutes in healthy individuals). Initiate supportive measures in the case of overdose.
-
11 DESCRIPTION
SYMLIN® (pramlintide acetate) injection is an anti-diabetic medication for use in patients with diabetes treated with insulin. Pramlintide is a synthetic analog of human amylin, a naturally occurring neuroendocrine hormone synthesized by pancreatic beta cells that contributes to glucose control during the postprandial period. Pramlintide is provided as an acetate salt of the synthetic 37-amino acid polypeptide, which differs in amino acid sequence from human amylin by replacement with proline at positions 25 (alanine), 28 (serine), and 29 (serine).
The structural formula of pramlintide acetate is shown below:
Pramlintide acetate is a white powder that has a molecular formula of C171H267N51O53S2 × C2H4O2 (3≤ × ≤8); the molecular weight is 3949.4. Pramlintide acetate is soluble in water.
SYMLIN is formulated as a clear, isotonic, sterile solution for subcutaneous administration. The disposable multidose SymlinPen® pen-injector contains 1000 mcg/mL of pramlintide (as acetate). The formulation contains 2.25 mg/mL of metacresol as a preservative, D-mannitol as a tonicity modifier, acetic acid, sodium acetate as pH modifiers, and water for injection. SYMLIN has a pH of approximately 4.0.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Pramlintide is an analog of human amylin. Amylin is colocated with insulin in secretory granules and cosecreted with insulin by pancreatic beta cells in response to food intake. Amylin and insulin show similar fasting and postprandial patterns in healthy individuals (Figure 1).
Figure 1: Secretion Profile of Amylin and Insulin in Healthy Adults
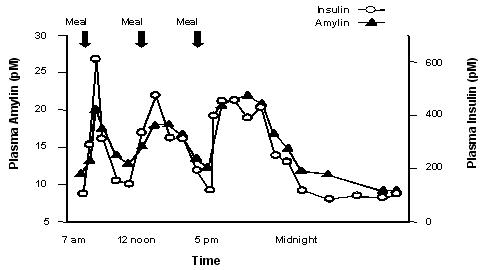
In patients with type 1 and type 2 diabetes, there is reduced secretion from pancreatic beta cells of both insulin and amylin in response to food.
Amylin affects the rate of postprandial glucose appearance through a variety of mechanisms, as determined by nonclinical studies. Amylin slows gastric emptying (i.e., the rate at which food is released from the stomach to the small intestine) without altering the overall absorption of nutrients. In addition, amylin suppresses glucagon secretion (not normalized by insulin alone), which leads to suppression of endogenous glucose output from the liver. Amylin also regulates food intake due to centrally-mediated modulation of appetite.
In human studies, pramlintide, acting as an amylin analog, slows gastric emptying, reduces the postprandial rise in plasma glucagon, and modulates satiety leading to decreased caloric intake.
12.2 Pharmacodynamics
In clinical studies in patients with type 1 diabetes and patients with type 2 diabetes using mealtime insulin, SYMLIN reduced mean postprandial glucose concentrations, reduced glucose fluctuations, and reduced food intake.
Reduction in Postprandial Glucose Concentrations
In a randomized, single-blind, placebo-controlled, crossover study, 19 subjects with type 2 diabetes using insulin lispro, 19 subjects with type 1 diabetes using regular human insulin, and 21 subjects with type 1 diabetes using insulin lispro underwent mixed-meal tests. SYMLIN administered subcutaneously immediately prior to a meal reduced plasma glucose concentrations following the meal when used with mealtime insulin (rapid-acting insulin analogs or regular human insulin) (Figure 2). When rapid-acting insulin analogs were used, plasma glucose concentrations tended to rise during the interval between 150 minutes following SYMLIN injection and the next meal [see Dosage and Administration (2)].
Figure 2: Postprandial Plasma Glucose Profiles in Patients with Type 1 Diabetes or Type 2 Diabetes Receiving SYMLIN and Insulin Compared to Those Receiving Insulin Alone
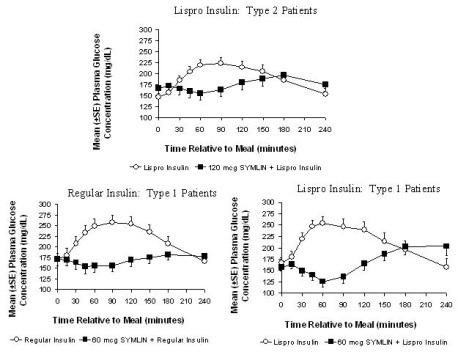
While SYMLIN reduces postprandial glucose, clinical studies employing a controlled hypoglycemic challenge have demonstrated that SYMLIN does not alter the counter-regulatory hormonal response to insulin-induced hypoglycemia. Likewise, in SYMLIN-treated patients, the perception of hypoglycemic symptoms was not altered with plasma glucose concentrations as low as 45 mg/dL. In a separate clinical trial pramlintide also reduced the 24-hour glucose fluctuations based upon 24-hour glucose monitoring.
Reduced Food Intake
A single, subcutaneous dose of 30 mcg of SYMLIN to patients with type 1 diabetes and 120 mcg of SYMLIN to patients with type 2 diabetes administered 1 hour prior to an unlimited buffet meal was associated with reductions in total caloric intake (placebo-subtracted mean changes of ~21% and 23%, respectively), which occurred without decreases in meal duration.
12.3 Pharmacokinetics
Absorption
The absolute bioavailability of pramlintide following a single subcutaneous dose of SYMLIN is approximately 30% to 40%. Subcutaneous administration of different doses of SYMLIN into the abdominal area or thigh of healthy individuals showed a linear, dose-dependent increase in maximum plasma concentrations (Cmax) and overall exposure (AUC) (Table 5).
Table 5: Mean Pharmacokinetic Parameters Following Administration of Single Subcutaneous Doses of SYMLIN Subcutaneous Dose
(mcg)AUC (0-∞)
(pmol*min/L)Cmax
(pmol/L)Tmax
(min)Elimination t½
(min)30
3750
39
21
55
60
6778
79
20
49
90
8507
102
19
51
120
11970
147
21
48
Injection of SYMLIN into the arm in obese patients with type 1 or type 2 diabetes showed higher overall exposure (20%-36%) with greater variability (% CV for AUC: 73%-106%), compared with exposure after injection of SYMLIN into the abdominal area or thigh.
Relative bioavailability of pramlintide was not significantly different between obese and non-obese patients and based on BMI or skin fold thickness. Injections administered with 6.0-mm and 12.7-mm needles yielded similar bioavailability.
Distribution
SYMLIN does not extensively bind to red blood cells or albumin (approximately 40% of the drug is unbound in plasma).
Metabolism and Elimination
In healthy individuals, the half-life of pramlintide is approximately 48 minutes. The primary metabolite, Des-lys1 pramlintide (2-37 pramlintide), is biologically active in vitro. Overall exposure (AUC) to pramlintide is relatively constant with repeat dosing of SYMLIN, indicating no bioaccumulation.
Specific Populations
Renal Impairment
No studies have been conducted in patients with end-stage renal disease. In a single-dose pharmacokinetic study in patients with type 1 diabetes, 60 mcg of SYMLIN was administered to 4 patients with normal renal function (ClCr >90 mL/min), 9 patients with mild renal impairment (ClCr 60-89 mL/min), 5 patients with moderate renal impairment (ClCr 30-59 mL/min) and 3 patients with severe renal impairment (ClCr 15-29 mL/min). No statistically significant differences were noted in total (AUC0-∞) and peak (Cmax) exposure of pramlintide for mild, moderate, and severe renal impairment categories in comparison to patients with normal renal function; although, inter-patient variability in pharmacokinetic parameters was high.
Hepatic Impairment
Pharmacokinetic studies have not been conducted in patients with hepatic impairment.
Geriatric
Pharmacokinetic studies have not been conducted in the geriatric population [see Use in Specific Populations (8.5)].
Pediatric
The efficacy and safety of SYMLIN have not been established in the pediatric population. The use of SYMLIN is not recommended in pediatric patients due to the risk of severe hypoglycemia [see Warnings and Precautions (5.1, 5.2)].
Drug Interactions
Effect of Pre-Mixing SYMLIN with Insulin
Pharmacokinetic profiles of pramlintide and insulins after coadministration of 30 mcg SYMLIN with different insulins (regular, NPH, and 70/30 premixed formulations of recombinant human insulin) as one subcutaneous injection, premixed in one syringe, were compared to those observed after the coadministration of SYMLIN and different insulins given as separate subcutaneous injections. The effects of premixing on pramlintide pharmacokinetics varied across the different insulin products with a maximum decrease of 40% in pramlintide Cmax and a maximum increase of 36% in pramlintide AUC0-∞. Similarly, effects of premixing on insulin pharmacokinetics varied across different insulin products with a maximum increase of 15% in insulin Cmax and up to a 20% increase in insulin AUC0-600min. Always administer SYMLIN and insulin as separate injections and never mix [see Warnings and Precautions (5.4)].
Acetaminophen
When 1000 mg acetaminophen was given within 0, 1, and 2 hours after a 120 mcg SYMLIN injection in patients with type 2 diabetes (n=24), acetaminophen Cmax decreased by 29%, 23%, and 20%, respectively compared to placebo. The time to maximum plasma concentration or Tmax increased by 72, 48, and 48 minutes, respectively. SYMLIN did not significantly affect acetaminophen Tmax or Cmax when acetaminophen was administered 1 to 2 hours before SYMLIN injection. SYMLIN did not affect acetaminophen AUC regardless of the time of acetaminophen administration in relation to SYMLIN injection.
Oral Contraceptives
When a single dose of a combination oral contraceptive product, containing 30 mcg ethinyl estradiol and 300 mcg norgestrel, was administered 15 minutes after SYMLIN injection (90 mcg dose) in healthy female subjects, there was no statistically significant change in the Cmax and AUC of ethinyl estradiol. However, the norgestrel Cmax was reduced by about 30% and Tmax was delayed by 45 minutes; there was no effect on norgestrel AUC. The clinical relevance of this change is unknown.
Ampicillin
The effect of concomitant administration of SYMLIN and ampicillin was evaluated in healthy volunteers. The administration of a single oral 500 mg dose of ampicillin 15 minutes after a single dose of SYMLIN (90 mcg) did not alter the Cmax or AUC for ampicillin. However, the Tmax for ampicillin was delayed by approximately 60 minutes.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
A two-year carcinogenicity study was conducted in CD-1 mice with doses of 0.2, 0.5, and 1.2 mg/kg/day of pramlintide (32, 67, and 159 times the exposure resulting from the human dose of 360 mcg/day based on area under the plasma concentration curve or AUC, respectively). No drug-induced tumors were observed. A two-year carcinogenicity study was conducted in Sprague-Dawley rats with doses of 0.04, 0.2, and 0.5 mg/kg/day of pramlintide (3, 9, and 25 times the exposure resulting from the human dose of 360 mcg/day based on AUC, respectively). No drug-induced tumors were observed in any organ.
Mutagenesis
Pramlintide was not mutagenic in the Ames test and did not increase chromosomal aberration in the human lymphocytes assay. Pramlintide was not clastogenic in the in vivo mouse micronucleus test or in the chromosomal aberration assay utilizing Chinese hamster ovary cells.
Impairment of Fertility
Administration of 0.3, 1, or 3 mg/kg/day of pramlintide (up to 140 times the human dose of 360 mcg/day based on exposure) prior to and during mating had no significant effects on fertility in male or female rats. The highest dose of 3 mg/kg/day resulted in dystocia in 8/12 female rats secondary to maternal toxicity and significant decreases in serum calcium levels.
-
14 CLINICAL STUDIES
A total of 2333 patients with type 1 diabetes and 1852 patients with type 2 diabetes received SYMLIN in controlled clinical trials.
14.1 Type 1 Diabetes
The efficacy and safety of SYMLIN were evaluated in 3 (26-52-week), randomized, double-blind, placebo-controlled trials in patients with type 1 diabetes. In these studies, insulin adjustments were minimized in order to isolate the SYMLIN effect with insulin adjustments allowed, at the investigator's discretion, when excessive hypoglycemia was encountered. Patients participating in these 3 trials had a mean age of 40 years, a mean duration of diabetes of 17 years, and a mean body mass index of 25.9 kg/m2.
Table 6 summarizes the 6-month results for those patients assigned to the 30 or 60 mcg dose of SYMLIN or placebo.
Table 6: Mean (SE) Change in HbA1c and Insulin at 6 Months in the Double-Blind, Placebo-Controlled Studies in Patients with Type 1 Diabetes for the Intent-to-Treat Population Trial 1 Trial 2 Trial 3 Variable SYMLIN
(30/60 mcg)Placebo SYMLIN
(60 mcg)Placebo SYMLIN
(60 mcg TID)SYMLIN
(60 mcg QID)Placebo N=243 N=237 N=148 N=147 N=164 N=161 N=154 - * Statistically significant reduction compared to placebo (p-value <0.05).
Baseline HbA1c (%) (SD)
8.7
(1.33)8.9
(1.46)9.0
(1.12)9.1
(1.08)8.9
(1.1)8.9
(1.0)9.0
(1.1)LSM Change in HbA1c at 6 Months Relative to Baseline (%) (SE)
–0.58
(0.07)*–0.25
(0.07)–0.24
(0.09)*+0.08
(0.09)–0.44
(0.07)*–0.44
(–0.07)–0.19
(0.08)Placebo-
Subtracted LSM change in HbA1c at 6 Months (%)–0.34*
NA
–0.32*
NA
–0.25*
–0.25*
NA
Mean Insulin Doses at Baseline: Mealtime/Bolus (U) (SE)
NM
NM
29.5
(1.4)28.5
(1.1)19.9
(1.2)19.8
(2.2)19.8
(1.3)Mean Change in Insulin Doses (U) at 6 Months: Mealtime/Bolus (SE)
NM
NM
–2.0
(0.5)*+0.3
(0.4)+0.6
(0.8)–0.8
(0.7)+0.3
(1.4)Mean Insulin Doses at Baseline: Basal (U) (SE)
NM
NM
21.0
(1.1)21.0
(1.1)33.1
(1.7)33.7
(1.6)31.9
(1.8)Mean Change in Insulin Doses (U) at 6 Months: Basal (SE)
NM
NM
+0.2
(0.3)–0.3
(0.4)–0.1
(0.9)
–0.6
(0.7)+0.6
(0.7)SD: standard deviation; LSM: least squares mean; SE: standard error; U: Units; NM: not measured; TID: 3 times a day; QID: 4 times a day.
In the three studies, from a mean baseline body weight of 75.3 kg, 73.3 kg, and 76.6 kg, respectively, after randomization there were corresponding mean reductions of –0.8 kg, –1.6 kg, and –1.3 kg (60 mcg TID) and –0.8 kg (60 mcg QID) in the SYMLIN treatment group compared to mean increases of +0.8 kg, +0.4 kg, and +0.7 kg in the placebo treatment group.
SYMLIN Dose-Titration Study
A dose-titration study of SYMLIN was conducted in patients with type 1 diabetes who had a mean age of 41 years, a mean duration of diabetes of 20 years, and a mean body mass index of 28 kg/m2. Patients with a mean baseline HbA1c of 8.1% (range 6.5%-10.7%) were randomized to receive either SYMLIN or placebo, both administered before major meals as add-on to insulin therapy. SYMLIN was initiated at a dose of 15 mcg and titrated upward at weekly intervals in 15 mcg increments to maintenance doses of 30 or 60 mcg, based on whether patients experienced nausea. Upon initiation of SYMLIN, the insulin dose (mostly the mealtime insulin) was reduced by 30% to 50% in order to minimize the occurrence of hypoglycemia. Once the maintenance dose of SYMLIN was reached, insulin dose adjustments were made according to standard clinical practice, based on pre- and post-meal blood glucose monitoring.
Table 7 summarizes the 6-month results for the dose-titration study.
Table 7: Mean (SE) Change in HbA1c and Insulin at 6 Months in the Dose-Titration Study in Patients with Type 1 Diabetes for Intent-to-Treat Population Variable SYMLIN
(all doses)Placebo N=148 N=147 - * Statistically significant reduction compared to placebo (p-value <0.05).
Mean Baseline HbA1c (%), (SD)
8.1 (0.8)
8.1 (0.8)
LSM Change in HbA1c at Week 29 Relative to Baseline (%)
–0.47 (0.07)
–0.49 (0.07)
Placebo-Subtracted LSM change in HbA1c at 6 Months (%) (SE)
0.03 (0.10)
NA
Mean Insulin Doses at Baseline: Mealtime/Bolus (U) (SD)
26.5 (14.2)
28.4 (16.3)
Mean Percent Change in Insulin Doses (U) at 6 Months: Mealtime/Bolus (SE)
–7.1 (0.9)*
–2.4 (1.2)
Mean Insulin Doses at Baseline: Basal (U) (SD)
29.4 (19.6)
28.1 (17.5)
Mean Change in Insulin Doses (U) at 6 Months: Basal (SE)
+1.4 (0.9)
+2.6 (1.2)
SD: standard deviation; LSM: least squares mean; SE: standard error; U: Units.
In the dose titration study, from mean baseline body weight of 81.5 kg, after randomization there was a mean reduction of –1.33 kg in the SYMLIN treatment group compared to a mean increase of +1.25 kg in the placebo treatment group.
14.2 Type 2 Diabetes
The efficacy and safety of SYMLIN were evaluated in 2 (a 26-week and a 52-week) randomized, double-blind, placebo-controlled trials in patients with type 2 diabetes. These trials enrolled patients with inadequate glycemic control (HbA1c >8%) on fixed dose insulin. In both trials, SYMLIN or placebo was added to existing insulin therapies. Concomitant use of a sulfonylurea and/or metformin was permitted. Insulin doses were to be kept as stable as possible throughout the treatment period to isolate the SYMLIN effect.
Patients participating in these 2 trials had a mean age of 57 years and a mean duration of diabetes of 13 years. Mean body mass index was 32.9 kg/m2 for SYMLIN and 32.2 kg/m2 for placebo.
Table 8 summarizes the 6-month results for each trial for those patients assigned to the 120 mcg dose of SYMLIN and placebo.
Table 8: Mean (SE) Change in HbA1c and Insulin at 6 Months in the Double-Blind, Placebo-Controlled Studies in Patients with Type 2 Diabetes for the Intent-to-Treat Population Trial 1 Trial 2 Variable SYMLIN
(120 mcg)Placebo SYMLIN
(120 mcg)Placebo N=166 N=161 N=126 N=123 - * dStatistically significant reduction compared to placebo (p-value <0.05).
Baseline HbA1c (%) (SD)
9.0 (0.08)
9.3 (0.10)
9.3 (1.1)
9.5 (1.4)
LSM Change in HbA1c at 6 Months Relative to Baseline (%) (SE)
–0.66 (0.08)*
–0.32 (0.09)
–0.36 (0.10)*
–0.06 (0.10)
Placebo-Subtracted LSM change in HbA1c at 6 Months (%)
–0.34*
NA
–0.30*
NA
Insulin Dose at Baseline: Mealtime/Bolus (U) (SE)
20.7 (1.6)
21.4 (1.5)
22.2 (1.8)
22.0 (1.6)
Mean Change in Insulin Doses (U) at 6 Months: Mealtime/Bolus (SE)
–0.7 (0.5)
–0.3 (0.6)
–0.0 (0.8)*
+1.6 (0.7)
Insulin Dose at Baseline: Basal (U) (SE)
48.0 (1.9)
52.4 (2.1)
33.2 (1.4)
30.9 (1.6)
Mean Change in Insulin Doses (U) at 6 Months: Basal (SE)
+0.01 (0.8)
+1.1 (1.0)
–1.2 (0.8)
+1.3 (0.7)
SD: standard deviation; LSM: least squares mean; SE: standard error; U: Units.
In both studies, from a mean baseline body weight of 96.7 kg, and 85.6 kg, respectively, after randomization there were corresponding mean reductions of –1.4 kg, and –1.6 kg in the SYMLIN treatment group compared to mean increases of +0.3 kg, and +0.1 kg in the placebo treatment group.
-
16 HOW SUPPLIED/STORAGE AND HANDLING
SYMLIN Injection is available in the following package sizes:
-
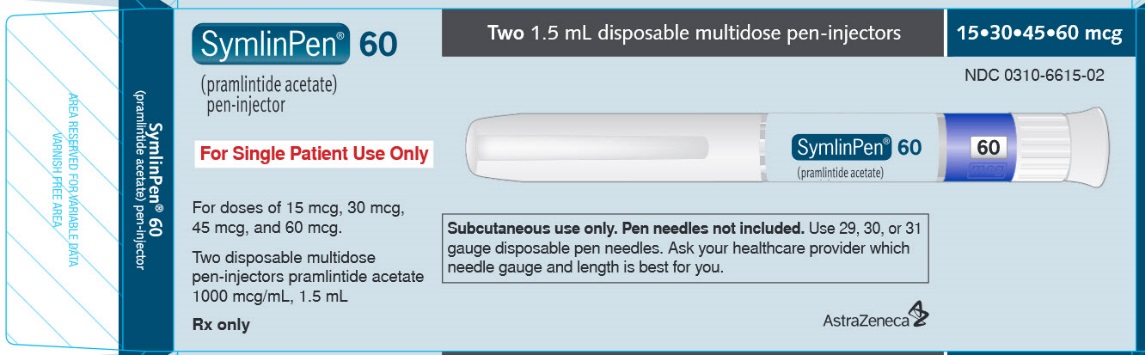
SymlinPen® 60 pen-injector, containing 1000 mcg/mL pramlintide (as acetate)
Two 1.5 mL disposable multidose pen-injectors
(NDC: 0310-6615-02) -
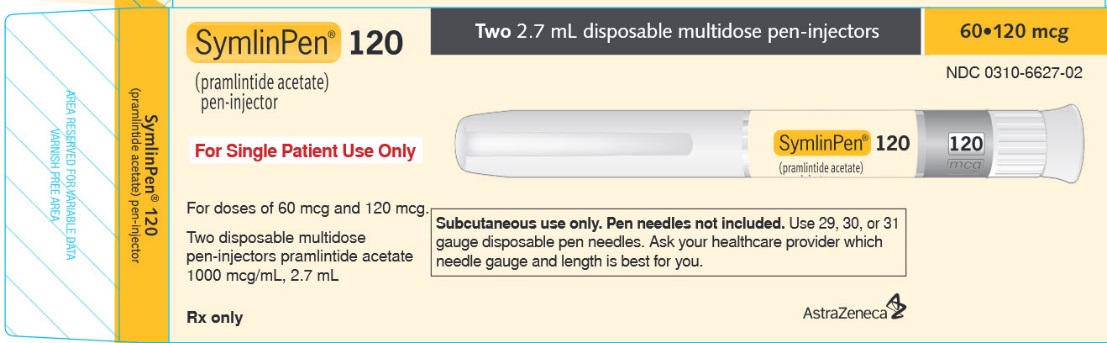
SymlinPen® 120 pen-injector, containing 1000 mcg/mL pramlintide (as acetate)
Two 2.7 mL disposable multidose pen-injectors
(NDC: 0310-6627-02)
Storage and Handling
SYMLIN pen-injectors not in use: Refrigerate (2°C to 8°C; 36°F to 46°F), and protect from light. Do not freeze. Do not use if product has been frozen. Unused SYMLIN (opened or unopened) should not be used after the expiration (EXP) date printed on the carton and the label.
SYMLIN pen-injectors in use: After first use, refrigerate or keep at a temperature not greater than 86°F (30°C) for 30 days. Use within 30 days, whether or not refrigerated.
Storage conditions are summarized in Table 9.
Table 9: Storage Conditions Dosage Form Unopened (not in use)
RefrigeratedOpen (in use)
Refrigerated or Temperature up to 86°F (30°C)1.5 mL pen-injector
Until Expiration Date
Use Within 30 Days
2.7 mL pen-injector
-
SymlinPen® 60 pen-injector, containing 1000 mcg/mL pramlintide (as acetate)
-
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Medication Guide).
Risk of Hypoglycemia
Discuss the risk and consequences of hypoglycemia and approaches to minimize its occurrence. Inform patients about the importance of self-management practices including glucose monitoring and timing of dosing. In addition, reinforce the importance of adherence to meal planning, physical activity, recognition and management of hypoglycemia and hyperglycemia, and assessment of diabetes complications.
Never Share a SymlinPen Between Patients
Advise patients that they must never share a SymlinPen with another person, even if the needle is changed, because doing so carries a risk for transmission of blood-borne pathogens.
Never Mix SYMLIN and Insulin
Inform patients that SYMLIN and insulin should always be administered as separate injections and never be mixed.
Show patients how to administer SYMLIN using the pen-injector. Advise patients to use a new needle for each injection.
Instructions
Instruct patients on the proper injection technique and proper storage of SYMLIN. Refer patients to the SYMLIN Medication Guide and Patient Instructions for Use for additional information.
Distributed by:
AstraZeneca Pharmaceuticals LP
Wilmington, DE 19850SYMLIN and SymlinPen are registered trademarks of the AstraZeneca group of companies.
-
MEDICATION GUIDE
SYMLIN® (SĬM-lĭn)
(pramlintide acetate)injection for subcutaneous use
Read this Medication Guide and Instructions for Use that come with your SYMLIN before you start using it and each time you get a refill. There may be new information. This Medication Guide does not take the place of talking to your healthcare provider about your medical condition or treatment.
What is the most important information I should know about SYMLIN?
SYMLIN can cause serious side effects, including:
-
severe low blood sugar (hypoglycemia). Even when SYMLIN is carefully added to your mealtime insulin therapy, your blood sugar may drop too low, especially if you have type 1 diabetes. If this severe low blood sugar (hypoglycemia) happens, it is seen within 3 hours after a SYMLIN injection. Symptoms of severe low blood sugar and low blood sugar include:
- o lightheadedness
- o dizziness
- o shakiness
- o sweating
- o hunger
- o fast heartbeat
- o trouble concentrating or confusion
- o change in vision
- o headache
- o irritability
- o drowsiness
People who have severely low blood sugar have had injuries while driving their car, operating heavy machinery or doing other dangerous activities. You and your healthcare provider should talk about a plan to treat low blood sugar. You should have fast-acting sugar (such as hard candy, glucose tablets, juice) or glucagon for injection with you at all times. Call your healthcare provider if you have severe low blood sugar or if you have low blood sugar more often than normal.
-
You have a higher chance of getting severe low blood sugar if you:
- o do not follow your healthcare provider’s instructions to reduce your insulin use before meals
- o use more SYMLIN or insulin than prescribed by your healthcare provider
- o change your insulin dose without checking your blood sugar
- o eat less food than your usual meal
- o are sick and cannot eat
- o are more active than usual
- o have a low blood sugar level before eating
- o drink alcohol
- SYMLIN is used with insulin to lower blood sugar, especially high blood sugar that happens after meals.
- SYMLIN is taken at mealtimes. The use of SYMLIN does not replace your daily insulin but may lower the amount of insulin you need, especially before meals.
Do not share your SymlinPen with other people, even if the needle has been changed. You may give other people a serious infection, or get a serious infection from them.
What is SYMLIN?
SYMLIN is an injectable prescription medicine used to treat adults with type 1 and type 2 diabetes to control blood sugar. SYMLIN is used when your mealtime insulin dose has not controlled your blood sugar well enough.
It is not known if SYMLIN is safe and effective in children.
Who should not use SYMLIN?
Do not use SYMLIN if you:
- are allergic to SYMLIN or any ingredients in SYMLIN. See the end of this Medication Guide for a complete list of ingredients in SYMLIN.
- cannot tell when your blood sugar is low (hypoglycemia unawareness)
- have a stomach problem called gastroparesis. This is when your stomach does not empty as fast as it should.
What should I tell my healthcare provider before using SYMLIN?
Before you use SYMLIN, tell your healthcare provider about all of your medical conditions, including if you:
- are pregnant or plan to become pregnant. It is not known if SYMLIN will harm your unborn baby. You and your healthcare provider should decide how to best control your blood sugar levels during pregnancy.
- are breastfeeding or plan to breastfeed. It is not known if SYMLIN passes into your breast milk. You and your healthcare provider should decide about the best way to feed your baby if you are using SYMLIN.
Tell your healthcare provider about all the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. SYMLIN slows stomach emptying and can affect medicines that need to pass through the stomach quickly.
How should I use SYMLIN?
- Read the “Instructions for Use” and the Medication Guide and that come with your SYMLIN for information about the right way to use SYMLIN.
- Use SYMLIN exactly as your healthcare provider tells you to use it.
- Your healthcare provider will tell you how much SYMLIN to use and when to use it.
- Your healthcare provider may change your dose if needed.
- If you stop taking SYMLIN for any reason, such as surgery or illness, talk to your healthcare provider about how to re-start SYMLIN.
- To reduce the risk of hypoglycemia, it is important that you plan your meals and physical activity every day while you use SYMLIN. Plan for what you will eat and when you will eat your meals.
- The amount of SYMLIN you use will depend on whether you have type 1 or type 2 diabetes.
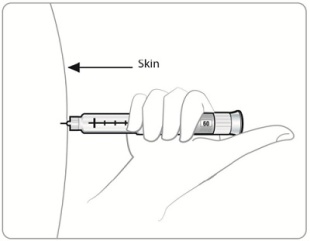
- The way you inject SYMLIN is similar to the way you inject insulin. Inject SYMLIN under the skin of your stomach area (abdomen) or upper leg (thigh). Inject SYMLIN at a site that is more than 2 inches away from your insulin injection. Do not inject SYMLIN and insulin in the same site.
- To help reduce the chances of getting a reaction at the injection site, allow SYMLIN to come to room temperature before injecting.
- Use a new needle for each SYMLIN injection. Do not reuse or share your needles with other people. You may give other people a serious infection, or get a serious infection from them.
- Never mix SYMLIN and insulin. Insulin can affect SYMLIN when they are mixed together.
- Do not use SYMLIN if the liquid looks cloudy.
- If you take more than your prescribed dose of SYMLIN, you may get nauseous or vomit, and may not be able to eat the amount of food you usually eat. If you take more SYMLIN than your prescribed dose, pay careful attention to the amount of insulin you use because you may be at more risk for low blood sugar. Contact your healthcare provider for guidance.
- If you miss or forget a dose of SYMLIN, wait until the next meal and take your usual dose of SYMLIN at that meal. Do not take more than your usual dose of SYMLIN.
- Do not share your SymlinPen with other people, even if the needle is changed.You may give other people a serious infection or get a serious infection from them.
Using SYMLIN and insulin with type 1 diabetes:
- When starting SYMLIN, you will need to reduce your dose of mealtime insulin. Your healthcare provider will tell you how to reduce your dose of mealtime insulin the right way.
- You must check your blood sugar as often as your healthcare provider tells you to, which may include before and after every meal and at bedtime.
- The usual starting dose of SYMLIN for people who have type 1 diabetes is 15 micrograms (mcg) injected under your skin.
- Inject SYMLIN under your skin (subcutaneously) just before a major meal. A major meal must have at least 250 calories or 30 grams of carbohydrate.
- If you have not had any nausea for 3 days or more after your dose of SYMLIN is changed, your healthcare provider may tell you to slowly increase your dose of SYMLIN. Do not increase your dose of SYMLIN unless your healthcare provider tells you to.
- Tell your healthcare provider right away if you have nausea or low blood sugar after your dose of SYMLIN is changed. Your healthcare provider will tell you what to do.
- Your healthcare provider may make changes to your insulin dose to better control your blood sugar. Your healthcare provider should tell you what the right dose of insulin is for you.
Using SYMLIN and insulin with type 2 diabetes:
- When starting SYMLIN, you will need to reduce your dose of mealtime insulin. Your healthcare provider will tell you how to reduce your dose of mealtime insulin the right way.
- You must check your blood sugar as often as your healthcare provider advises you to, which may include before and after every meal and at bedtime.
- The usual starting dose of SYMLIN for people who have type 2 diabetes is 60 micrograms (mcg) injected under your skin.
- Inject SYMLIN under your skin (subcutaneously) just before a major meal. A major meal must have at least 250 calories or 30 grams of carbohydrate.
- If you have not had any nausea for 3 days or more after your dose of SYMLIN is changed, your healthcare provider may tell you to increase your dose of SYMLIN. Do not increase your dose of SYMLIN unless your healthcare provider tells you to.
- Tell your healthcare provider right away if you have nausea or low blood sugar after your dose of SYMLIN is changed. Your healthcare provider will tell you what to do.
- Your healthcare provider may make changes to your insulin dose to better control your blood sugar. Your healthcare provider should tell you what the right dose of insulin is for you.
What should I avoid while taking SYMLIN?
- See “What is the most important information I should know about SYMLIN?”
- Do not drive, operate machinery, or do other dangerous activities until you know how SYMLIN affects you. Talk to your healthcare provider about the activities you should avoid.
- Alcohol. Drinking alcohol may increase your chances of getting severe low blood sugar.
What are the possible side effects of SYMLIN?
SYMLIN may cause serious side effects, including:
- See “What is the most important information I should know about SYMLIN?”
- injection site reactions. SYMLIN may cause bruising, swelling, or itching at the injection site.
The most common side effects of SYMLIN include:
- nausea
- vomiting
- decreased appetite
- stomach pain
- headache
Tell your healthcare provider if you have any side effect that bothers you or that does not go away.
These are not all the possible side effects of SYMLIN. For more information, ask your healthcare provider or pharmacist.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
How should I store SYMLIN?
Unopened SYMLIN:
- Keep SYMLIN in the refrigerator between 36°F to 46°F (2°C to 8°C), until you are ready to use it.
- Do not freeze. Do not use SYMLIN if it has been frozen.
- Keep unopened SYMLIN out of the light.
Opened SYMLIN:
- Keep SYMLIN either in the refrigerator or at room temperature between 36°F to 86°F (2°C to 30°C) for up to 30 days.
- Throw away used SYMLIN after 30 days of use, even if the pen still has medicine in it.
- Do not use SYMLIN (opened or unopened) after the expiration (EXP) date printed on the carton and the label.
Keep SYMLIN and all medicines out of the reach of children.
General information about the safe and effective use of SYMLIN:
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use SYMLIN for a condition for which it was not prescribed. Do not give SYMLIN to other people, even if they have the same symptoms that you have. It may harm them.
This Medication Guide summarizes the most important information about SYMLIN. If you would like more information, talk with your healthcare provider. You can ask your pharmacist or healthcare provider for information about SYMLIN that is written for health professionals.
More information, go to www.SYMLIN.com or call 1-800-236-9933.
What are the ingredients in SYMLIN?
Active ingredient: pramlintide acetate
Inactive ingredients: metacresol, D-mannitol, acetic acid, and sodium acetate
This Medication Guide has been approved by the U.S. Food and Drug Administration.
SYMLIN and SymlinPen are registered trademarks of the AstraZeneca group of companies.
Distributed by:
AstraZeneca Pharmaceuticals LP
Wilmington, DE 19850
Revised: February 2015
-
severe low blood sugar (hypoglycemia). Even when SYMLIN is carefully added to your mealtime insulin therapy, your blood sugar may drop too low, especially if you have type 1 diabetes. If this severe low blood sugar (hypoglycemia) happens, it is seen within 3 hours after a SYMLIN injection. Symptoms of severe low blood sugar and low blood sugar include:
-
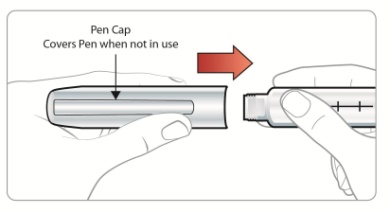
Instructions for Use
SymlinPen® (SĬM-lĭnPεn) 120
(pramlintide acetate)
Pen-InjectorRead the Medication Guide and these Instructions for Use before you start using SYMLIN and each time you get a refill. There may be new information.
Do not share your SymlinPen with other people, even if the needle has been changed. You may give other people a serious infection, or get a serious infection from them.
Important:
- Ask your healthcare provider about your dose of SYMLIN and how to inject SYMLIN the right way before you inject it for the first time.
- Use a new needle for each SYMLIN injection. Do not reuse or share your needles with other people.You may give other people a serious infection, or get a serious infection from them.
- This SymlinPen is not recommended for use by the blind or visually impaired without the assistance of a person trained in the proper use of this SymlinPen.
- Check SYMLIN before you use it. SYMLIN should be clear and colorless. Do not use SYMLIN if the liquid looks cloudy or colored or has lumps or particles in it.
- Your SymlinPen may look empty because SYMLIN is a clear and colorless liquid.
- Small bubbles will not hurt you or affect your dose of SYMLIN.
- Do not transfer SYMLIN from your SymlinPen into a syringe.
-
Do not inject your dose of SYMLIN if you:
- ∘ have low blood sugar (hypoglycemia)
- ∘ do not plan to eat. Do not inject SYMLIN if you skip a meal. Wait until the next meal and take your usual dose of SYMLIN at that meal.
- ∘ plan to eat a meal with less than 250 calories or 30 grams of carbohydrate
- ∘ are sick and cannot eat your usual meal
- ∘ are having surgery or a medical test where you cannot eat
- If you take more than your prescribed dose of SYMLIN, you may get nauseous or vomit, and may not be able to eat the amount of food you usually eat. If you take more SYMLIN than your prescribed dose, pay careful attention to the amount of insulin you use because you may be at more risk for low blood sugar. Contact your healthcare provider for guidance.
Supplies you will need to give each injection of SYMLIN:
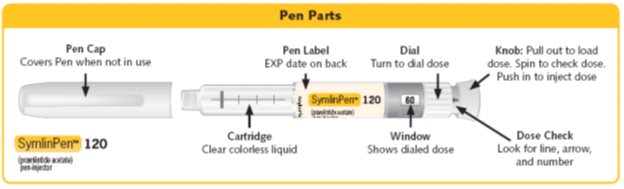
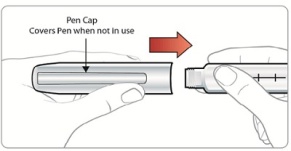
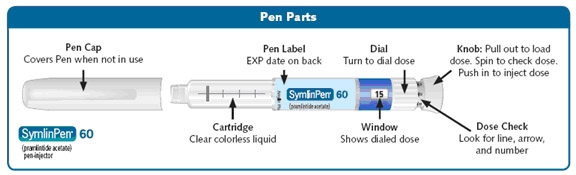
- SymlinPen® 120 Pen-Injector (Pen) (See Figure A)
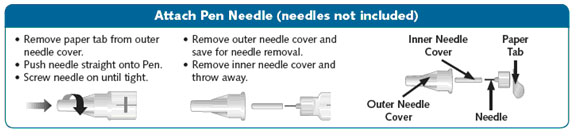
- a new SymlinPen compatible needle (See Figure B). Pen needles are not included. Use 29, 30, or 31 gauge disposable pen needles. Ask your healthcare provider which needle gauge and length is best for you.
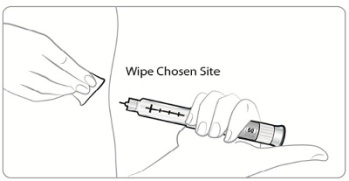
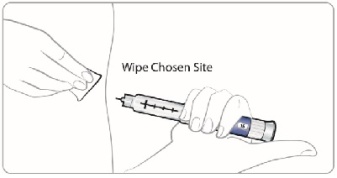
- alcohol swab
- 1 sharps container for throwing away used SymlinPens and needles. See “Disposing of used SymlinPens and needles” at the end of these Instructions for Use.
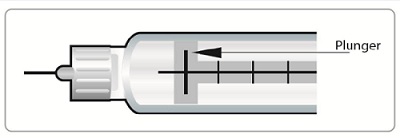
(Figure A)
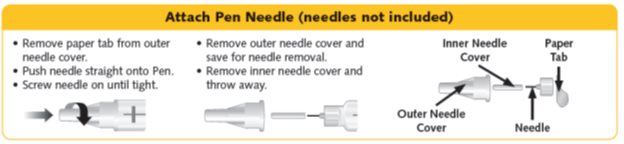
(Figure B)
Preparing your SymlinPen:
- Wash your hands with soap and water.
- Check the SymlinPen label before each use to make sure you have the right SymlinPen.
- Check the expiration date (EXP) on the SymlinPen label (See Figure A). Do not use the SymlinPen past the expiration date printed on the label.
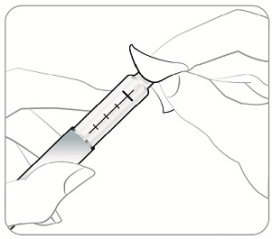
-
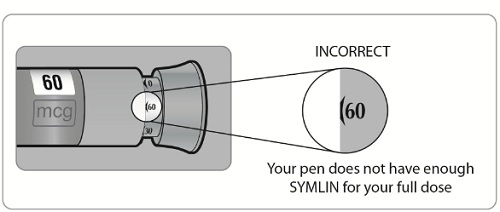
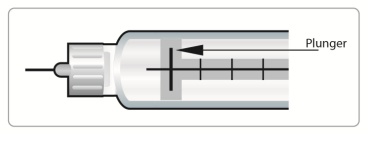
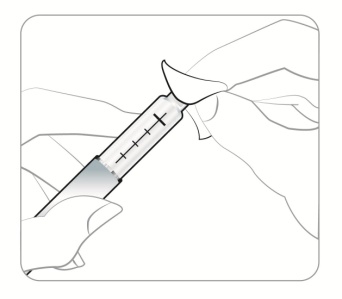
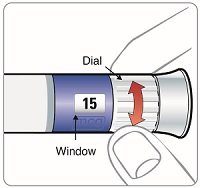
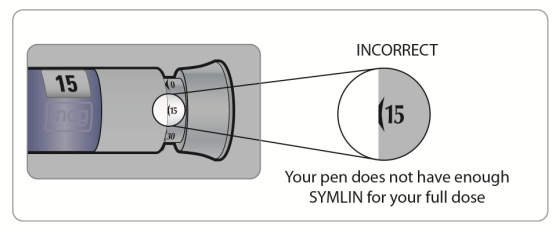
Check the liquid in your SymlinPen to make sure you have enough SYMLIN left in your SymlinPen to load your correct dose.
- ∘ The lines on the cartridge show about how much SYMLIN is left in your SymlinPen. When the top of the plunger is at the thickest line on the cartridge, your SymlinPen is almost empty (See Figure C).
(Figure C)
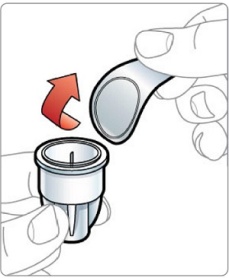
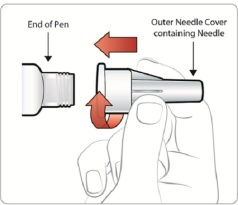
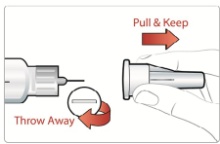
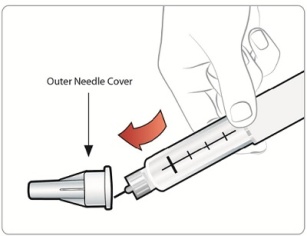
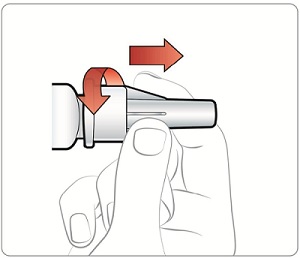
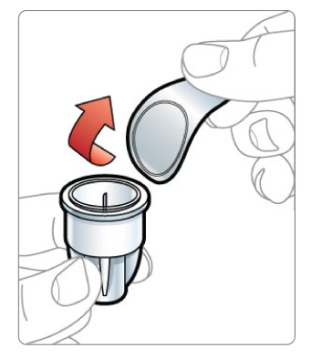
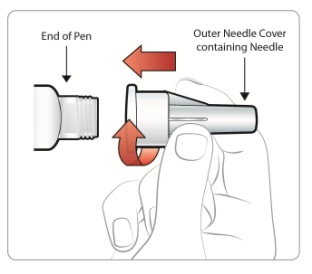
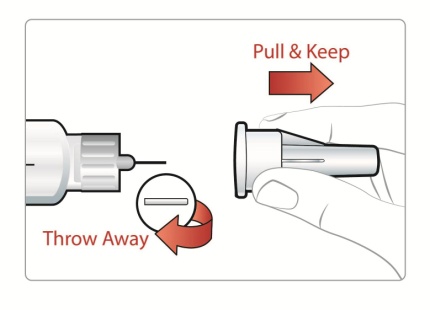
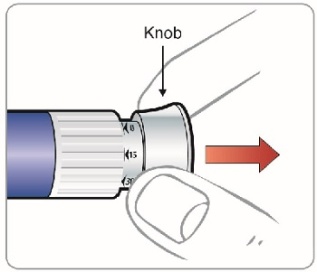
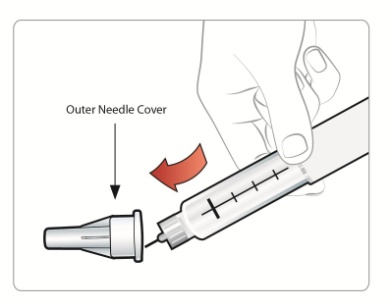
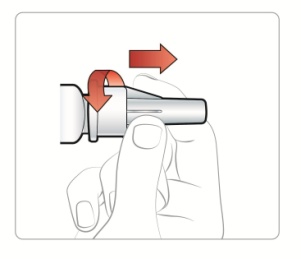
Attaching a Needle:
New Pen Setup - Priming your SymlinPen:
Note:
-
Steps 5 through 7 are only required if you are using your SymlinPen for the first time. Do not repeat Step 1 through 4 before each dose.
- ∘ If you have already primed your SymlinPen, go to Step 8 for instructions about giving your scheduled dose.
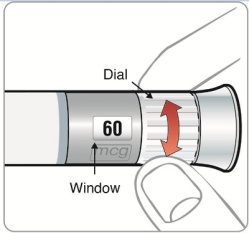
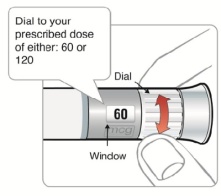
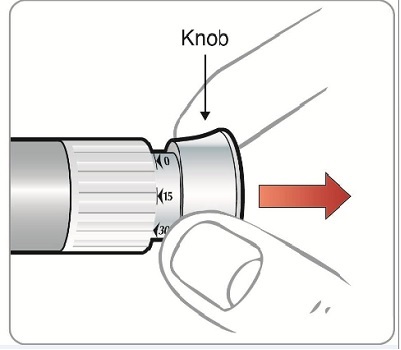
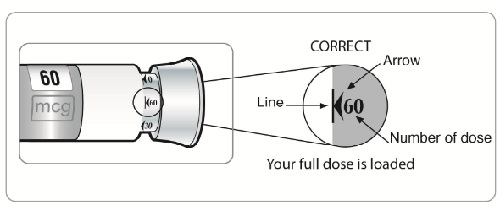
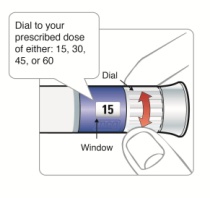
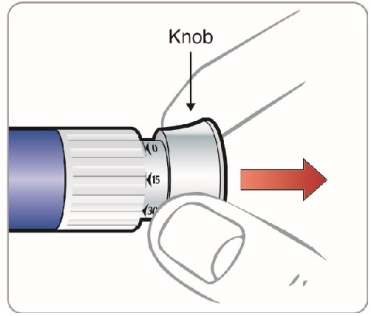
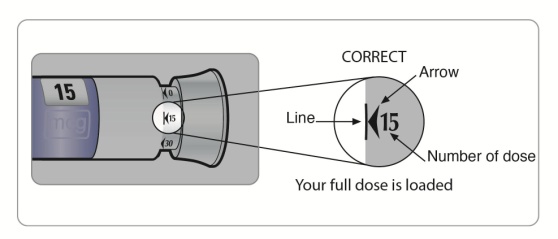
Selecting your routine dose:
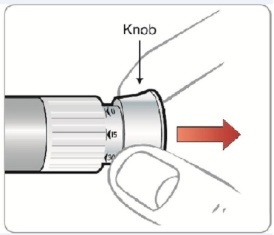
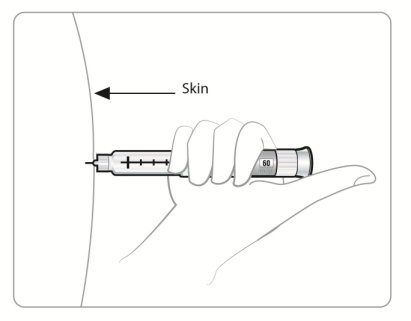
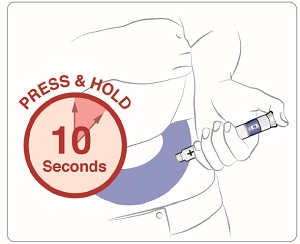
Giving your SYMLIN injection:
- Inject your SYMLIN exactly as your doctor has shown you.
- Change (rotate) injection sites for SYMLIN. Inject SYMLIN at a site that is more than 2 inches away from your insulin injection. Do not inject SYMLIN and insulin in the same site.
- To help reduce the chances of getting a reaction at the injection site, let SYMLIN come to room temperature before you inject it.
After your injection:
-
Put your used needles and SymlinPen in an FDA-cleared sharps disposal container right away after use. Do not throw away (dispose of) loose needles and syringes in your household trash.
- ∘
If you do not have an FDA-cleared sharps disposal container, you may use a household container that is:
- ▪ made of a heavy-duty plastic,
- ▪ can be closed with a tight-fitting, puncture-resistant lid, without sharps being able to come out,
- ▪ upright and stable during use,
- ▪ leak-resistant, and
- ▪ properly labeled to warn of hazardous waste inside the container.
- ∘ When your sharps disposal container is almost full, you will need to follow your community guidelines for the right way to dispose of your sharps disposal container. There may be state or local laws about how you should throw away used needles and SymlinPen. For more information about safe sharps disposal, and for specific information about sharps disposal in the state that you live in, go to the FDA’s website at: http://www.fda.gov/safesharpsdisposal
- ∘ Do not dispose of your used sharps disposal container in your household trash unless your community guidelines permit this. Do not recycle your used sharps disposal container.
- ∘
If you do not have an FDA-cleared sharps disposal container, you may use a household container that is:
How should I store my SymlinPen?
Unused SymlinPens:
- Keep SYMLIN in the refrigerator between 36°F to 46°F (2°C to 8°C), until you are ready to use it.
- Do not freeze. Do not use SYMLIN if it has been frozen.
- Keep unopened SYMLIN out of the light.
Used SymlinPens:
- Store SymlinPens in the refrigerator or at room temperature between 36°F to 86°F (2°C to 30°C) for up to 30 days.
- Throw away used SymlinPens after 30 days of use, even if a used SymlinPen still has medicine in it.
- Do not use SymlinPens (opened or unopened) after the expiration (EXP) date printed on the carton and the label.
General information about the safe and effective use of SymlinPens.
- If you drop your SymlinPen, you should prime it before you use it to make sure your SymlinPen works.
- Do not use your SymlinPen if any part looks broken or damaged.
- Keep SYMLIN and all medicines out of the reach of children.
- It is not known if SYMLIN is safe and effective in children.
If you are having problems using your SymlinPen, go to www.SYMLIN.com or call Information Support at 1-800-236-9933.
These Instructions for Use have been approved by the U.S. Food and Drug Administration.
SYMLIN and SymlinPen are registered trademarks of the AstraZeneca group of companies.
Distributed by:
AstraZeneca Pharmaceuticals LP
Wilmington, DE 19850
Revised: March 2015
-
Instructions for Use
SymlinPen® (SĬM-lĭnPεn) 60
(pramlintide acetate)
Pen-InjectorRead the Medication Guide and these Instructions for Use before you start using SYMLIN and each time you get a refill. There may be new information.
Do not share your SymlinPen with other people, even if the needle has been changed. You may give other people a serious infection, or get a serious infection from them.
Important:
- Ask your healthcare provider about your dose of SYMLIN and how to inject SYMLIN the right way before you inject it for the first time.
- Use a new needle for each SYMLIN injection. Do not reuse or share your needles with other people. You may give other people a serious infection, or get a serious infection from them.
- This SymlinPen is not recommended for use by the blind or visually impaired without the assistance of a person trained in the proper use of this SymlinPen.
- Check SYMLIN before you use it. SYMLIN should be clear and colorless. Do not use SYMLIN if the liquid looks cloudy or colored or has lumps or particles in it.
- Your SymlinPen may look empty because SYMLIN is a clear and colorless liquid.
- Small bubbles will not hurt you or affect your dose of SYMLIN.
- Do not transfer SYMLIN from your SymlinPen into a syringe.
-
Do not inject your dose of SYMLIN if you:
- ∘ have low blood sugar (hypoglycemia)
- ∘ do not plan to eat. Do not inject SYMLIN if you skip a meal. Wait until the next meal and take your usual dose of SYMLIN at that meal.
- ∘ plan to eat a meal with less than 250 calories or 30 grams of carbohydrate
- ∘ are sick and cannot eat your usual meal
- ∘ are having surgery or a medical test where you cannot eat
- If you take more than your prescribed dose of SYMLIN, you may get nauseous or vomit, and may not be able to eat the amount of food you usually eat. If you take more SYMLIN than your prescribed dose, pay careful attention to the amount of insulin you use because you may be at more risk for low blood sugar. Contact your healthcare provider for guidance.
Supplies you will need to give each injection of SYMLIN:
- SymlinPen® 60 Pen-Injector (Pen) (See Figure A)
- a new SymlinPen compatible needle (See Figure B). Pen needles are not included. Use 29, 30, or 31 gauge disposable pen needles. Ask your healthcare provider which needle gauge and length is best for you.
- alcohol swab
- 1 sharps container for throwing away used SymlinPens and needles. See “Disposing of used SymlinPens and needles” at the end of these Instructions for Use.
(Figure A)
(Figure B)
Preparing your SymlinPen:
- Wash your hands with soap and water.
- Check the SymlinPen label before each use to make sure you have the right SymlinPen.
- Check the expiration date (EXP) on the SymlinPen label (See Figure A). Do not use the SymlinPen past the expiration date printed on the label.
-
Check the liquid in your SymlinPen to make sure you have enough SYMLIN left in your SymlinPen to load your correct dose.
- ∘ The lines on the cartridge show about how much SYMLIN is left in your SymlinPen. When the top of the plunger is at the thickest line on the cartridge, your SymlinPen is almost empty (See Figure C).
(Figure C)
Attaching a Needle:
New Pen Setup - Priming your SymlinPen:
Note:
- Steps 5 through 7 are only required if you are using your SymlinPen for the first time. Do not repeat Step 1 through 4 before each dose.
- If you have already primed your SymlinPen, go to Step 8 for instructions about giving your scheduled dose.
Selecting your routine dose:
Giving your SYMLIN injection:
- Inject your SYMLIN exactly as your doctor has shown you.
- Change (rotate) injection sites for SYMLIN. Inject SYMLIN at a site that is more than 2 inches away from your insulin injection. Do not inject SYMLIN and insulin in the same site.
- To help reduce the chances of getting a reaction at the injection site, let SYMLIN come to room temperature before you inject it.
After your injection:
-
Put your used needles and SymlinPen in an FDA-cleared sharps disposal container right away after use. Do not throw away (dispose of) loose needles and syringes in your household trash.
- ∘
If you do not have an FDA-cleared sharps disposal container, you may use a household container that is:
- ▪ made of a heavy-duty plastic,
- ▪ can be closed with a tight-fitting, puncture-resistant lid, without sharps being able to come out,
- ▪ upright and stable during use,
- ▪ leak-resistant, and
- ▪ properly labeled to warn of hazardous waste inside the container.
- ∘ When your sharps disposal container is almost full, you will need to follow your community guidelines for the right way to dispose of your sharps disposal container. There may be state or local laws about how you should throw away used needles and SymlinPen. For more information about safe sharps disposal, and for specific information about sharps disposal in the state that you live in, go to the FDA’s website at: http://www.fda.gov/safesharpsdisposal
- ∘ Do not dispose of your used sharps disposal container in your household trash unless your community guidelines permit this. Do not recycle your used sharps disposal container.
- ∘
If you do not have an FDA-cleared sharps disposal container, you may use a household container that is:
How should I store my SymlinPen?
Unused SymlinPens:
- Keep SYMLIN in the refrigerator between 36°F to 46°F (2°C to 8°C), until you are ready to use it.
- Do not freeze. Do not use SYMLIN if it has been frozen.
- Keep unopened SYMLIN out of the light.
Used SymlinPens:
- Store SymlinPens in the refrigerator or at room temperature between 36°F to 86°F (2°C to 30°C) for up to 30 days.
- Throw away used SymlinPens after 30 days of use, even if a used SymlinPen still has medicine in it.
- Do not use SymlinPens (opened or unopened) after the expiration (EXP) date printed on the carton and the label.
General information about the safe and effective use of SymlinPens.
- If you drop your SymlinPen, you should prime it before you use it to make sure your SymlinPen works.
- Do not use your SymlinPen if any part looks broken or damaged.
- Keep SYMLIN and all medicines out of the reach of children.
- It is not known if SYMLIN is safe and effective in children.
- If you are having problems using your SymlinPen, go to www.SYMLIN.com or call Information Support at 1-800-236-9933.
These Instructions for Use have been approved by the U.S. Food and Drug Administration.
SYMLIN and SymlinPen are registered trademarks of the AstraZeneca group of companies.
Distributed by:
AstraZeneca Pharmaceuticals LP
Wilmington, DE 19850
Revised: March 2015
-
PACKAGE/LABEL PRINCIPAL DISPLAY PANEL – 1.5 mL pen-injector
SymlinPen® 60
(pramlintide acetate)
pen-injector
For Single Patient Use Only
For doses of 15 mcg, 30 mcg, 45 mcg, and 60 mcg.
Two disposable multidose pen-injectors pramlintide acetate 1000 mcg/mL, 1.5 mL
Subcutaneous use only. Pen needles not included. Use 29, 30, or 31 gauge disposable pen needles. Ask your healthcare provider which needle gauge and length is best for you.
Rx Only AstraZeneca
-
PACKAGE/LABEL PRINCIPAL DISPLAY PANEL – 2.7 mL pen-injector
SymlinPen® 120
(pramlintide acetate)
pen-injector
Two 2.7 mL disposable multidose pen-injectors 60120 mcg NDC: 0310-6627-02
For Single Patient Use Only
For doses of 60 mcg and 120 mcg.
Two disposable multidose pen-injectors pramlintide acetate 1000 mcg/mL, 2.7 mL
Subcutaneous use only. Pen needles not included. Use 29, 30, or 31 gauge disposable pen needles. Ask your healthcare provider which needle gauge and length is best for you.
Rx Only AstraZeneca
-
INGREDIENTS AND APPEARANCE
SYMLINPEN
pramlintide acetate injectionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 0310-6615 Route of Administration SUBCUTANEOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength pramlintide acetate (UNII: 726I6TE06G) (pramlintide - UNII:D3FM8FA78T) pramlintide 1000 ug in 1 mL Inactive Ingredients Ingredient Name Strength metacresol (UNII: GGO4Y809LO) 2.25 mg in 1 mL mannitol (UNII: 3OWL53L36A) acetic acid (UNII: Q40Q9N063P) sodium acetate (UNII: 4550K0SC9B) water (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 0310-6615-02 2 in 1 CARTON 02/02/2015 1 1.5 mL in 1 CARTRIDGE; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA021332 01/08/2015 SYMLINPEN
pramlintide acetate injectionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 0310-6627 Route of Administration SUBCUTANEOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength pramlintide acetate (UNII: 726I6TE06G) (pramlintide - UNII:D3FM8FA78T) pramlintide 1000 ug in 1 mL Inactive Ingredients Ingredient Name Strength metacresol (UNII: GGO4Y809LO) 2.25 mg in 1 mL mannitol (UNII: 3OWL53L36A) acetic acid (UNII: Q40Q9N063P) sodium acetate (UNII: 4550K0SC9B) water (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 0310-6627-02 2 in 1 CARTON 01/08/2015 1 2.7 mL in 1 CARTRIDGE; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA021332 01/08/2015 Labeler - AstraZeneca Pharmaceuticals LP (054743190) Registrant - AstraZeneca PLC (230790719)




Trademark Results [SymlinPen]
Mark Image Registration | Serial | Company Trademark Application Date |
|---|---|
 SYMLINPEN 78301872 3419705 Live/Registered |
AMYLIN PHARMACEUTICALS, LLC 2003-09-17 |
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.