AFSTYLA ANTIHEMOPHILIC FACTOR (RECOMBINANT), SINGLE CHAIN- antihemophilic factor, human recombinant kit
AFSTYLA by
Drug Labeling and Warnings
AFSTYLA by is a Other medication manufactured, distributed, or labeled by CSL Behring Recombinant facility AG, CSL Behring GmbH, CSL Behring LLC. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use AFSTYLA safely and effectively. See full prescribing information for AFSTYLA.
AFSTYLA®, Antihemophilic Factor (Recombinant), Single Chain Lyophilized Powder for Solution for Intravenous Injection
Initial U.S. Approval: 2016RECENT MAJOR CHANGES
Warnings and Precautions (5.2) 12/2019 INDICATIONS AND USAGE
AFSTYLA, Antihemophilic Factor (Recombinant), Single Chain, is a recombinant, antihemophilic factor indicated in adults and children with hemophilia A (congenital Factor VIII deficiency) for:
- On-demand treatment and control of bleeding episodes,
- Routine prophylaxis to reduce the frequency of bleeding episodes,
- Perioperative management of bleeding.
Limitation of Use
AFSTYLA is not indicated for the treatment of von Willebrand disease (1).
DOSAGE AND ADMINISTRATION
For intravenous use after reconstitution only.
- Each vial of AFSTYLA is labeled with the amount of recombinant Factor VIII in international units (IU or unit). One unit per kilogram body weight will raise the Factor VIII level by 2 IU/dL. (2.1)
- Plasma Factor VIII levels can be monitored using either a chromogenic assay or a one-stage clotting assay – routinely used in US clinical laboratories. If the one-stage clotting assay is used, multiply the result by a conversion factor of 2 to determine the patient's Factor VIII activity level. (2.1, 5.3)
Calculating Required Dose: (2.1)
Dose (IU) = Body Weight (kg) × Desired Factor VIII Rise (IU/dL or % of normal) × 0.5 (IU/kg per IU/dL)
Routine Prophylaxis: (2.1)
- Adults and adolescents (≥12 years): The recommended starting regimen is 20 to 50 IU per kg of AFSTYLA administered 2 to 3 times weekly.
- Children (<12 years): The recommended starting regimen is 30 to 50 IU per kg of AFSTYLA administered 2 to 3 times weekly. More frequent or higher doses may be required in children <12 years of age to account for the higher clearance in this age group.
- The regimen may be adjusted based on patient response.
Perioperative Management: (2.1)
- Ensure the appropriate Factor VIII activity level is achieved and maintained.
DOSAGE FORMS AND STRENGTHS
AFSTYLA is available as a white or slightly yellow lyophilized powder supplied in single-use vials containing nominally 250, 500, 1000, 1500, 2000, 2500, or 3000 International Units (IU). (3)
CONTRAINDICATIONS
Do not use in patients who have had life-threatening hypersensitivity reactions, including anaphylaxis to AFSTYLA or its excipients, or hamster proteins. (4)
WARNINGS AND PRECAUTIONS
- Hypersensitivity reactions, including anaphylaxis, are possible. Should symptoms occur, immediately discontinue AFSTYLA and administer appropriate treatment. (5.1)
- Development of Factor VIII neutralizing antibodies (inhibitors) has been reported with AFSTYLA. If expected plasma Factor VIII activity levels are not attained, or if bleeding is not controlled with an appropriate dose, perform an assay that measures Factor VIII inhibitor concentration. (5.2)
- If the one-stage clotting assay is used, multiply the result by a conversion factor of 2 to determine the patient's Factor VIII activity level. (5.3)
ADVERSE REACTIONS
- The most common adverse reactions reported in clinical trials (>0.5% of subjects) were dizziness and hypersensitivity. (6)
To report SUSPECTED ADVERSE REACTIONS, contact the CSL Behring Pharmacovigilance Department at 1-866-915-6958 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
USE IN SPECIFIC POPULATIONS
- Pediatric: Clearance (based on per kg body weight) is higher in pediatric patients 0 to <12 years of age. Higher and/or more frequent dosing may be needed. (8.4)
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.
Revised: 12/2019
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Dosing Guidelines
2.2 Preparation and Reconstitution
2.3 Administration
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Hypersensitivity Reactions
5.2 Neutralizing Antibodies
5.3 Monitoring Laboratory Tests
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
6.2 Immunogenicity
6.3 Postmarketing Experience
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.4 Pediatric Use
8.5 Geriatric Use
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
15 REFERENCES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- * Sections or subsections omitted from the full prescribing information are not listed.
-
1 INDICATIONS AND USAGE
AFSTYLA, Antihemophilic Factor (Recombinant), Single Chain is a recombinant, antihemophilic factor indicated in adults and children with hemophilia A (congenital Factor VIII deficiency) for:
- On-demand treatment and control of bleeding episodes,
- Routine prophylaxis to reduce the frequency of bleeding episodes,
- Perioperative management of bleeding.
-
2 DOSAGE AND ADMINISTRATION
For intravenous use after reconstitution only.
2.1 Dosing Guidelines
- Dose and duration of treatment depend on the severity of the Factor VIII deficiency, the location and extent of bleeding, and the patient's clinical condition.
- Each vial of AFSTYLA states the actual amount of Factor VIII activity in International Units (IU) as determined by chromogenic assay. One IU corresponds to the activity of Factor VIII contained in 1 milliliter (mL) of normal human plasma.
- Plasma Factor VIII levels can be monitored using either a chromogenic assay or a one-stage clotting assay – routinely used in US clinical laboratories. If the one-stage clotting assay is used, multiply the result by a conversion factor of 2 to determine the patient's Factor VIII activity level [see Warnings and Precautions (5.3)].
Calculating Required Dose
- The calculation of the required dose of Factor VIII is based on the empirical finding that 1 IU Factor VIII per kg body weight raises the plasma Factor VIII level by 2 IU/dL.
The expected in vivo peak increase in Factor VIII level expressed as IU/dL (or % of normal) is estimated using the following formula:
Estimated Increment of Factor VIII (IU/dL or % of normal) = [Total Dose (IU)/body weight (kg)] × 2 (IU/dL per IU/kg)
The dose to achieve a desired in vivo peak increase in Factor VIII level may be calculated using the following formula:
Dose (IU) = body weight (kg) × Desired Factor VIII rise (IU/dL or % of normal) × 0.5 (IU/kg per IU/dL)
- The amount of AFSTYLA to be administered and the frequency of administration should always be oriented to the clinical effectiveness in the individual case.
On-demand Treatment and Control of Bleeding Episodes
A guide for dosing AFSTYLA in the treatment and control of bleeding episodes is provided in Table 1. Consideration should be given to maintaining a Factor VIII activity at or above the target range.
Table 1. Dosing for On-demand Treatment and Control of Bleeding Episodes Type of Bleeding Episode Factor VIII Activity Level Required
(% or IU/dL)Frequency of Doses (hours) Minor
Uncomplicated hemarthrosis, minor muscle bleeding or oral bleeding20-40 Repeat injection every 12-24 hours until the bleeding is resolved. Moderate
Muscle bleeding (except iliopsoas), hemarthrosis, or mild trauma30-60 Repeat injection every 12-24 hours until the bleeding is resolved. Major/Life-threatening
Limb threatening hemorrhage, deep muscle bleeding (including iliopsoas), intracranial and retropharyngeal bleeding, fractures or head trauma60-100 Repeat injection every 8-24 hours until bleed is resolved. Routine Prophylaxis
- Adults and adolescents (≥12 years): The recommended starting regimen is 20 to 50 IU per kg of AFSTYLA administered 2 to 3 times weekly.
- Children (<12 years): The recommended starting regimen is 30 to 50 IU per kg of AFSTYLA administered 2 to 3 times weekly. More frequent or higher doses may be required in children <12 years of age to account for the higher clearance in this age group [see Clinical Pharmacology (12.3)].
- The regimen may be adjusted based on patient response.
Perioperative Management of Bleeding
A guide for dosing AFSTYLA during surgery (perioperative management of bleeding) is provided in Table 2. Consideration should be given to maintaining a Factor VIII activity at or above the target range.
Table 2. Target Factor VIII Activity Levels for Perioperative Management of Bleeding Type of Surgery Factor VIII Activity Level Required
(% or IU/dL)Frequency of Doses (hours) / Duration of Therapy (days) Minor
(including tooth extraction)30-60 Repeat injection every 24 hours for at least 1 day, until healing is achieved. Major
(intracranial, intra-abdominal, intrathoracic, or joint-replacement)80-100 Repeat injection every 8-24 hours until adequate wound healing, then continue therapy for at least another 7 days to maintain a Factor VIII activity of 30-60% (IU/dL). 2.2 Preparation and Reconstitution
- Reconstitute AFSTYLA using aseptic technique with diluent provided in the kit.
- Visually inspect the reconstituted solution for particulate matter prior to administration. The solution should be free from visible particles. Do not use if particulate matter is observed.
The procedures provided below are general guidelines for the preparation and reconstitution of AFSTYLA.
AFSTYLA Reconstitution Instructions
- Ensure that the AFSTYLA vial and diluent vial are at room temperature. Prepare and administer using aseptic technique.
- Place the AFSTYLA vial, diluent vial, and Mix2Vial® transfer set on a flat surface.
- Remove AFSTYLA and diluent vial flip caps. Wipe the stoppers with the sterile alcohol swab provided and allow the stoppers to dry prior to opening the Mix2Vial transfer set package.
- Open the Mix2Vial transfer set package by peeling away the lid (Fig. 1). Leave the Mix2Vial transfer set in the clear package.

Fig. 1
- Place the diluent vial on a flat surface and hold the vial tightly. Grip the Mix2Vial transfer set together with the clear package and push the plastic spike at the blue end of the Mix2Vial transfer set firmly through the center of the stopper of the diluent vial (Fig. 2).

Fig. 2
- Carefully remove the clear package from the Mix2Vial transfer set. Make sure that you pull up only the clear package, not the Mix2Vial transfer set (Fig. 3).

Fig. 3
- With the AFSTYLA vial placed firmly on a flat surface, invert the diluent vial with the Mix2Vial transfer set attached and push the plastic spike of the transparent adapter firmly through the center of the stopper of the AFSTYLA vial (Fig. 4). The diluent will automatically transfer into the AFSTYLA vial.

Fig. 4
- With the diluent and AFSTYLA vial still attached to the Mix2Vial transfer set, gently swirl the AFSTYLA vial to ensure that the AFSTYLA is fully dissolved (Fig. 5). Do not shake the vial.
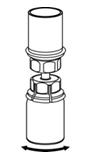
Fig. 5
- With one hand, grasp the AFSTYLA side of the Mix2Vial transfer set and with the other hand grasp the blue diluent-side of the Mix2Vial transfer set, and unscrew the set into two pieces. (Fig. 6).

Fig. 6
- Draw air into an empty, sterile syringe. While the AFSTYLA vial is upright, screw the syringe to the Mix2Vial transfer set. Inject air into the AFSTYLA vial. While keeping the syringe plunger pressed, invert the system upside down and draw the concentrate into the syringe by pulling the plunger back slowly. (Fig. 7).
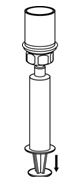
Fig. 7
- Now that the concentrate has been transferred into the syringe, firmly grasp the barrel of the syringe (keeping the plunger facing down) and unscrew the syringe from the Mix2Vial transfer set (Fig. 8).

Fig. 8
- After reconstitution, infuse immediately or within 4 hours. Reconstituted AFSTYLA may be stored at room temperature, not to exceed 25°C (77°F), for up to 4 hours. Do not freeze. Protect from direct sunlight.
- Record treatment – Remove the peel-off portion of the label from each vial used, and affix it to the patient's treatment diary/log book or scan the vial if recording the infusion electronically.
- If the dose requires more than one vial, use a separate, unused Mix2Vial® transfer set for each product vial. Repeat step 10 to pool the contents of the vial into one syringe.
2.3 Administration
- Use aseptic technique when administering AFSTYLA.
- Do not mix AFSTYLA with other medicinal products.
- Administer by intravenous injection. The rate of administration should be determined by the patient's comfort level. Do not exceed infusion rate of 10 mL per minute.
- Administer AFSTYLA at room temperature within 4 hours after reconstitution.
- AFSTYLA is for single use only. Following administration, discard any unused solution and all administration equipment in an appropriate manner as per local requirements.
- If a central venous access device (CVAD) is required, risk of CVAD-related complications including local infections, bacteremia and catheter site thrombosis should be considered.
- 3 DOSAGE FORMS AND STRENGTHS
-
4 CONTRAINDICATIONS
AFSTYLA is contraindicated in patients who have had life-threatening hypersensitivity reactions, including anaphylaxis to AFSTYLA or its excipients (e.g., polysorbate 80) [see Description (11)], or hamster proteins [see Warnings and Precautions (5.1)].
-
5 WARNINGS AND PRECAUTIONS
5.1 Hypersensitivity Reactions
Allergic-type hypersensitivity reactions, including anaphylaxis, are possible with AFSTYLA. Inform patients of the early signs of hypersensitivity reactions that may progress to anaphylaxis (including hives, generalized urticaria, tightness of the chest, wheezing, hypotension and pruritus). Immediately discontinue administration and initiate appropriate treatment if hypersensitivity reactions occur.
For patients with previous hypersensitivity reactions, consider premedication with antihistamines.
5.2 Neutralizing Antibodies
Formation of neutralizing antibodies (inhibitors) to Factor VIII has been reported following administration of AFSTYLA; previously untreated patients (PUPs) are at greatest risk. Monitor patients for the development of neutralizing antibodies (inhibitors) by appropriate clinical observations and laboratory tests. If expected plasma Factor VIII activity levels are not attained, or if bleeding is not controlled after AFSTYLA administration, the presence of an inhibitor (neutralizing antibody) should be suspected [see Warnings and Precautions (5.3)].
Contact a specialized hemophilia treatment center if a patient develops an inhibitor.
5.3 Monitoring Laboratory Tests
- Monitor plasma Factor VIII activity in patients receiving AFSTYLA using either the chromogenic assay or the one-stage clotting assay, which is routinely used in US clinical laboratories. The chromogenic assay result most accurately reflects the clinical hemostatic potential of AFSTYLA and is preferred. The one-stage clotting assay result underestimates the Factor VIII activity level compared to the chromogenic assay result by approximately one-half. If the one-stage clotting assay is used, multiply the result by a conversion factor of 2 to determine the patient's Factor VIII activity level. Incorrect interpretation of the Factor VIII activity obtained by the one-stage clotting assay could lead to unnecessary additional dosing, higher chronic dosing, or investigations for an inhibitor.
- Monitor for the development of Factor VIII inhibitors. Perform a Bethesda inhibitor assay if expected plasma Factor VIII activity levels are not attained or if bleeding is not controlled with the expected dose of AFSTYLA. Use Bethesda Units (BU) to report inhibitor levels.
-
6 ADVERSE REACTIONS
The most common adverse reactions (>0.5% of subjects) reported in clinical trials were dizziness and hypersensitivity.
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of one drug cannot be directly compared to rates in clinical trials of another drug and may not reflect the rates observed in practice.
The safety, efficacy and pharmacokinetics of AFSTYLA have been evaluated in 258 previously treated patients (PTPs) with severe hemophilia A (<1% endogenous Factor VIII activity) who received at least one dose of AFSTYLA as part of either routine prophylaxis, on-demand treatment of bleeding episodes or perioperative management in two completed clinical trials (an adult/adolescent study [≥12 to 65 years of age] and a pediatric study [<12 years of age]), and an ongoing extension study (0 to ≤65 years of age). Patients with a history of, or current FVIII inhibitors, or any first order family history of FVIII inhibitors, patients with known hypersensitivity (allergic reaction or anaphylaxis) to any FVIII product or hamster protein, and patients with evidence of thrombosis, including deep vein thrombosis, stroke, pulmonary embolism, myocardial infarction and arterial embolus within 3 months prior to Day 1 of the study were excluded from study participation.
Eighty-four (32.6%) subjects were children <12 years of age (35 [13.6%] 0 to <6 years and 49 [19.0%] ≥6 to <12 years), 14 (5.4%) were adolescents (≥12 to <18 years), and 160 (62.0%) were adults (≥18 to ≤65 years). There have been a total of 28,418 exposure days (EDs), with at least 28,492 injections of AFSTYLA administered. In the completed studies, a total of 185 subjects achieved at least 50 EDs, of whom 60 subjects achieved ≥100 EDs.
Adverse reactions (ARs) (summarized in Table 3) were reported for 14 of 258 (5.4%) subjects in all studies. An adverse reaction of hypersensitivity resulted in the withdrawal of one subject. No subject developed neutralizing antibodies (inhibitors) to Factor VIII or antibodies to host cell proteins. No events of anaphylaxis or thrombosis were reported.
Table 3. Adverse Reactions Reported for AFSTYLA (N=258) MedDRA System Organ Class Adverse Reactions Number of Subjects
n (%)Immune system disorders Hypersensitivity 4 (1.6) Nervous system disorders Dizziness 2 (0.8) Paresthesia 1 (0.4) Skin and subcutaneous tissue disorders Rash 1 (0.4) Erythema 1 (0.4) Pruritus 1 (0.4) General disorders and administration site conditions Pyrexia 1 (0.4) Injection-site pain 1 (0.4) Chills 1 (0.4) Feeling hot 1 (0.4) 6.2 Immunogenicity
All subjects were monitored for inhibitory and binding antibodies to AFSTYLA, and binding antibodies to chinese hamster ovary (CHO) host cell proteins prior to the first infusion of AFSTYLA, at defined intervals during the studies and at the end of study visit.
Preliminary data from an actively enrolling clinical trial in previously untreated patients (PUPs) aged ≤5 years indicate that 6 of 15 treated subjects (40% with a 95% confidence interval of 16%, 68%) developed an inhibitor. Of these, 3 subjects (20%) had peak inhibitor values in the high titer range, and 3 subjects (20%) had peak values in the low titer range. Of the 6 subjects who tested positive for inhibitors, 5 subjects have remained in the trial and have continued treatment with AFSTYLA; 3 now have titer values in the low titer range and 2 experienced successful eradication of the inhibitor.
No PTPs developed neutralizing antibodies (inhibitors) to Factor VIII or antibodies against CHO host cell proteins at any time during the completed clinical studies. Four subjects in the adult/adolescent study and 10 subjects in the pediatric study were negative for non-neutralizing anti-drug antibodies (ADAs) at screening and turned positive during the clinical study. Two of the adult/adolescent subjects and 3 of the pediatric subjects who developed ADAs were negative at end of study visit. No adverse events were associated with the development of ADAs. The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of antibody positivity in an assay may be influenced by several factors, including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, it may be misleading to compare the incidence of antibodies to AFSTYLA with the incidence of antibodies to other products.
6.3 Postmarketing Experience
The following adverse reaction has been identified during post-approval use of AFSTYLA. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Blood and lymphatic systems disorders: Factor VIII inhibitor development
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
There are no data with AFSTYLA use in pregnant women to inform on drug-associated risk. No developmental or animal reproduction toxicity studies were conducted with AFSTYLA. Thus, the risk of developmental toxicity including, structural abnormalities, embryo-fetal and/or infant mortality, functional impairment, and alterations to growth is not known. In the US general population, the estimated background risk of major birth defects occurs in 2-4% of the general population and miscarriage occurs in 15-20% of clinically recognized pregnancies.
8.2 Lactation
Risk Summary
There is no information regarding the excretion of AFSTYLA in human milk, the effect on the breastfed infant, or the effects on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for AFSTYLA and any potential adverse effects on the breastfed infant from AFSTYLA or from the underlying maternal condition.
8.4 Pediatric Use
Safety and efficacy studies with AFSTYLA have been performed in 98 previously treated pediatric patients <18 years of age. Fourteen adolescent subjects ≥12 to <18 years were enrolled in the adult/adolescent safety and efficacy study. Thirty-five subjects 0 to <6 years and 49 subjects ≥6 to <12 years were enrolled in a pediatric safety and efficacy study [see Adverse Reactions (6.1), Clinical Pharmacology (12.3), and Clinical Studies (14)]. Because clearance (based on per kg body weight) has been shown to be higher in the pediatric population 0 to <12 years, more frequent or higher doses of AFSTYLA based on body weight may be needed [see Clinical Pharmacology (12.3)].
-
11 DESCRIPTION
AFSTYLA is a single-chain recombinant Factor VIII produced in chinese hamster ovary (CHO) cells. It is a construct where the B-domain occurring in wild type full-length Factor VIII has been truncated and 4 amino acids of the adjacent acidic a3 domain were removed (amino acids 765 to 1652 of full-length Factor VIII). AFSTYLA is expressed as a single-chain Factor VIII molecule with covalent linkage between heavy and light chains; thereby keeping the molecule in the single-chain form resulting in increased stability and increased von Willebrand Factor (VWF) affinity. Except for a new N-glycosylation site at the junction between heavy and light chains, the post-translational modifications are comparable to endogenous Factor VIII.
AFSTYLA is purified by a controlled multi-step process including two virus reduction steps complementing each other in their mode of action. No human or animal derived proteins are used in the purification or formulation processes.
AFSTYLA is a preservative-free, sterile, non-pyrogenic, lyophilized powder to be reconstituted with sterile water for injection (sWFI) for intravenous injection. AFSTYLA is available in single-use vials containing the labeled amount of Factor VIII activity, expressed in IU. Each vial contains nominally 250, 500, 1000, 1500, 2000, 2500, or 3000 IU of AFSTYLA. The actual potency is labeled on each AFSTYLA vial and carton. After reconstitution of the lyophilized powder, all dosage strengths yield an almost colorless to slightly opalescent solution. The concentrations of excipients based on the vial size, as well as the amount of sWFI for reconstitution are provided in Table 4 below.
Table 4. Nominal Composition after Reconstitution with sWFI Ingredient 250 IU vial 500 IU vial 1000 IU vial 1500 IU vial 2000 IU vial 2500 IU vial 3000 IU vial rVIII-Single Chain 100 IU/mL 200 IU/mL 400 IU/mL 300 IU/mL 400 IU/mL 500 IU/mL 600 IU/mL L-Histidine 3.1 mg/mL 3.1 mg/mL 3.1 mg/mL 3.1 mg/mL 3.1 mg/mL 3.1 mg/mL 3.1 mg/mL Polysorbate 80 0.2 mg/mL 0.2 mg/mL 0.2 mg/mL 0.2 mg/mL 0.2 mg/mL 0.2 mg/mL 0.2 mg/mL Calcium chloride 0.4 mg/mL 0.4 mg/mL 0.4 mg/mL 0.4 mg/mL 0.4 mg/mL 0.4 mg/mL 0.4 mg/mL Sodium chloride 16.4 mg/mL 16.4 mg/mL 16.4 mg/mL 16.4 mg/mL 16.4 mg/mL 16.4 mg/mL 16.4 mg/mL Sucrose 6 mg/mL 6 mg/mL 6 mg/mL 6 mg/mL 6 mg/mL 6 mg/mL 6 mg/mL Water for Injection 2.5 mL 2.5 mL 2.5 mL 5 mL 5 mL 5 mL 5 mL The number of units of Factor VIII administered is expressed in IU, which are related to the current WHO standard for Factor VIII products. One IU of Factor VIII activity in plasma is equivalent to that quantity of Factor VIII in 1 mL of normal plasma. Factor VIII activity in plasma is expressed either as a percentage (relative to normal human plasma) or in IU (relative to an International Standard for Factor VIII in plasma).
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
AFSTYLA is a recombinant protein that replaces the missing Coagulation Factor VIII needed for effective hemostasis. AFSTYLA is a single polypeptide chain with a truncated B-domain that allows for a covalent bridge to link the Factor VIII heavy and light chains. AFSTYLA has demonstrated a higher VWF affinity relative to full-length rFVIII.1 VWF stabilizes Factor VIII and protects it from degradation. Activated AFSTYLA has an amino acid sequence identical to endogenous FVIIIa.
12.2 Pharmacodynamics
Hemophilia A is an X-linked hereditary disorder of blood coagulation due to decreased levels of Factor VIII and results in bleeding into joints, muscles or internal organs, either spontaneously or as result of accidental or surgical trauma. Replacement therapy increases the plasma levels of Factor VIII enabling a temporary correction of the factor deficiency and correction of the bleeding tendencies.
12.3 Pharmacokinetics
Subjects ≥12 years
The pharmacokinetics (PK) of AFSTYLA were evaluated in 91 (81 adults ≥18 years and 10 adolescents ≥12 to <18 years) previously treated subjects following an intravenous injection of a single dose of 50 IU/kg.
The PK parameters (Table 5) were based on plasma Factor VIII activity measured by the chromogenic assay after the first dose (initial PK assessment). The PK profile obtained 3 to 6 months after the initial PK assessment was comparable with the PK profile obtained after the first dose.
Table 5. Pharmacokinetic Parameters (Arithmetic Mean, Coefficient of Variation [CV%]) in Adults and Adolescents Following a Single Injection of 50 IU/kg of AFSTYLA - Chromogenic Assay PK Parameters ≥18 years
(N=81)≥12 to <18 years
(N=10)IR = incremental recovery recorded at 30 minutes after injection; Cmax = observed maximum plasma concentration; AUC0-inf = area under the Factor VIII activity time curve extrapolated to infinity; t1/2 = half-life; MRT = mean residence time; CL = body weight adjusted clearance; Vss = body weight adjusted volume of distribution at steady-state. IR (IU/dL)/(IU/kg) 2.00 (20.8) 1.69 (24.8) Cmax (IU/dL) 106 (18.1) 89.7 (24.8) AUC0-inf (IU*h/dL) 1960 (33.1) 1540 (36.5) t1/2 (h) 14.2 (26.0) 14.3 (33.3) MRT (h) 20.4 (25.8) 20.0 (32.2) CL (mL/h/kg) 2.90 (34.4) 3.80 (46.9) Vss (mL/kg) 55.2 (20.8) 68.5 (29.9) Children <12 years
Pharmacokinetic parameters of AFSTYLA were evaluated in 39 previously treated children (0 to <12 years) in open-label, multicenter studies following a 50 IU/kg intravenous injection of AFSTYLA.
Table 6 summarizes the PK parameters calculated from the pediatric data. These parameters were estimated based on the plasma Factor VIII activity over time profile.
Table 6. Comparison of Pharmacokinetic Parameters in Children by Age Category (Arithmetic Mean, Coefficient of Variation [CV%]) Following a Single Injection of 50 IU/kg of AFSTYLA - Chromogenic Assay PK Parameters 0 to <6 years
(N=20)≥6 to <12 years
(N=19)IR = incremental recovery recorded at 30 minutes after injection for subjects 12 to <18 years and at 60 minutes after injection for subjects 1 to <12 years; Cmax = observed maximum plasma concentration; AUC = area under the Factor VIII activity time curve extrapolated to infinity; t1/2 = half-life; MRT = mean residence time; CL = body weight adjusted clearance; Vss = body weight adjusted volume of distribution at steady-state. IR (IU/dL)/(IU/kg) 1.60 (21.1) 1.66 (19.7) Cmax (IU/dL) 80.2 (20.6) 83.5 (19.5) AUC0-inf (IU*h/dL) 1080 (31.0) 1170 (26.3) t1/2 (h) 10.4 (28.7) 10.2 (19.4) MRT (h) 12.4 (25.0) 12.3 (16.8) CL (mL/h/kg) 5.07 (29.6) 4.63 (29.5) Vss (mL/kg) 71.0 (11.8) 67.1 (22.3) - 13 NONCLINICAL TOXICOLOGY
-
14 CLINICAL STUDIES
The safety and efficacy of AFSTYLA were evaluated in two studies: an Open-label, Multicenter, Crossover Safety, Efficacy and Pharmacokinetic Study in adults/adolescents as well as in an Open Label Pharmacokinetic, Efficacy and Safety study in children. These studies characterized the PK of AFSTYLA and determined hemostatic efficacy in the control of bleeding events, the prevention of bleeding events in prophylaxis and in the adult/adolescent study determined hemostatic efficacy during perioperative management of bleeding in subjects undergoing surgical procedures.
The adult/adolescent study enrolled a total of 175 previously treated male subjects with severe hemophilia A (<1% endogenous Factor VIII activity). Subjects ranged in age from 12 to 65 years, including 14 adolescent subjects (≥12 to <18 years). Of the 175 enrolled subjects, 174 received at least one dose of AFSTYLA and 173 (99%) were evaluable for efficacy. A total of 161 subjects (92.5%) completed the study. A total of 120 (69.0%) subjects were treated for at least 50 EDs and 52 (29.9%) of those subjects were treated for at least 100 EDs. Subjects received a total of 14,592 injections with a median of 67.0 (range 1 to 395) injections per subject.
The pediatric study enrolled 84 previously treated male subjects with severe hemophilia A (35 subjects 0 to <6 years and 49 subjects ≥6 to <12 years). Of the 84 enrolled subjects, all received at least one dose of AFSTYLA and 83 (99%) were evaluable for efficacy. A total of 65 (77.4%) subjects were treated for at least 50 EDs and 8 (9.5%) of those subjects were treated for at least 100 EDs. Subjects received a total of 5,313 injections with a median of 59 (range 4 to 145) injections per subject.
On-demand Treatment and Control of Bleeding Episodes
In the adult/adolescent study a total of 848 bleeding episodes were treated with AFSTYLA and 835 received an efficacy assessment by the investigator. The majority of the bleeding episodes occurred in joints. The median dose per injection used to treat a bleeding episode was 31.7 IU/kg (range 6 to 84 IU/kg). Of the 848 bleeding episodes, 686 (81%) were controlled with a single AFSTYLA injection and another 107 (13%) were controlled with 2 injections. Fifty-five (6%) of the 848 bleeding episodes required 3 or more injections. For 94% of bleeding episodes the hemostatic efficacy rating by the investigator was either excellent or good.
In the pediatric study a total of 347 bleeding episodes were treated with AFSTYLA all of which received an efficacy assessment by the investigator. The majority of the bleeding episodes occurred in joints. The median dose per injection used to treat a bleeding episode was 27.3 IU/kg (range 16 to 76 IU/kg). Of the 347 bleeding episodes, 298 (86%) were controlled with a single AFSTYLA injection and another 34 (10%) were controlled with 2 injections. Fifteen (4%) of the 347 bleeding episodes required 3 or more injections. For 96% of bleeding episodes the hemostatic efficacy rating by the investigator was either excellent or good.
Assessment of response to treatment of bleeds by the investigator was as follows:
Excellent: Pain relief and/or improvement in signs of bleeding (i.e., swelling, tenderness, and/or increased range of motion in the case of musculoskeletal hemorrhage) within approximately 8 hours after the first infusion
Good: Pain relief and/or improvement in signs of bleeding at approximately 8 hours after the first infusion, but requires two infusions for complete resolution
Moderate: Probable or slight beneficial effect within approximately 8 hours after the first infusion; requires more than two infusions for complete resolution
No response: No improvement at all or condition worsens (i.e., signs of bleeding) after the first infusion and additional hemostatic intervention is required with another FVIII product, cryoprecipitate, or plasma for complete resolution.
Efficacy in control of bleeding episodes in both studies is summarized in Table 7.
Table 7. Efficacy of AFSTYLA in Control of Bleeding Bleeding Episodes Treated Adult and Adolescent
(≥12 to 65 years of age)
(N=848)Pediatric
(0 to <12 years of age)
(N=347)Number of injections 1 injection, n (%) 686 (81%) 298 (85.9%) 2 injections, n (%) 107 (13%) 34 (9.8%) 3 injections, n (%) 29 (3%) 8 (2.3%) >3 injections, n (%) 26 (3%) 7 (2.0%) Efficacy evaluation by investigator (N=835) (N=347) Excellent or Good, n (%) 783 (94%) 334 (96.3%) Moderate, n (%) 52 (6%) 12 (3.5%) No response, n (%) 0 1 (0.3%) Routine Prophylaxis
Adult and Adolescent Study
In the adult/adolescent and pediatric studies, subjects received prophylaxis in a regimen that was determined by the investigator, taking into account the subject's Factor VIII treatment regimen used prior to enrollment and the subject's bleeding phenotype.
In the adult/adolescent study, 54% of the 146 subjects on prophylaxis received AFSTYLA 3 times weekly; 32% of subjects received AFSTYLA 2 times weekly; 6% received AFSTYLA every other day, and 8% of subjects received other regimens.
The annualized bleeding rate (ABR) was comparable between subjects on a 3 times weekly regimen (median ABR of 1.53) and those on a 2 times weekly regimen (median ABR of 0.00). The annualized spontaneous bleeding rate (AsBR) was also comparable between subjects on a 3 times weekly regimen (median AsBR of 0.0) and those on a 2 times weekly regimen (median AsBR of 0.0). The number of subjects who needed dose adjustments was comparable between the two groups (34.2% [27 subjects] for three times weekly and 27.7% [13 subjects] for twice weekly).
The median prescribed dose for subjects on a 3 times weekly prophylaxis regimen was 30 IU/kg (12 to 50 IU/kg). The median prescribed dose for subjects on a 2 times weekly regimen was 35 IU/kg (17 to 50 IU/kg).
The ABR in prophylaxis (median of 1.14) was significantly lower (p <0.0001) than the ABR that was observed in subjects treated on-demand (median of 19.64). Sixty-three of 146 subjects (43%) experienced no bleeding episodes while on prophylaxis. There were no severe or life-threatening bleeds (e.g., intracranial hemorrhage) in subjects receiving prophylaxis.
Pediatric Study
In the pediatric study, 54% of the 80 subjects on prophylaxis received AFSTYLA 2 times a week; 30% of subjects received AFSTYLA 3 times a week; 4% received AFSTYLA every other day; and 12% of subjects received other regimens.
Twenty-one of 80 subjects (26%) experienced no bleeding episodes while on prophylaxis. There was one severe bleed (hip joint hemorrhage) in the pediatric study that was successfully treated.
For subjects on prophylaxis the overall ABR was 3.69, with a median ABR of 2.30 for subjects on a 3 times a week regimen and 4.37 for subjects on a 2 times a week regimen. The median AsBR (0.00) was identical between subjects on the 3 times a week and 2 times a week regimens.
The median prescribed dose for subjects on a 3 times a week regimen was 32 IU/kg (19 to 50 IU/kg) and for subjects on a 2 times a week regimen was 35 IU/kg (20 to 57 IU/kg).
The ABRs for prophylaxis and on-demand in both studies are summarized in Table 8.
Table 8. Summary of Annualized Bleeding Rate (ABR) by AFSTYLA Treatment Regimen Phase I/III Adult/Adolescent Study Phase III Pediatric Study Prophylaxis
(N=146)On-demand
(N=27)Prophylaxis
(N=80)On-demand
(N=3)- * IQR = interquartile range, 25th percentile to 75th percentile
Overall ABR
Median (IQR*)
1.14 (0–4.2)
19.64 (6.2–46.5)3.69 (0–7.2) 78.56 (35.1–86.6) Annualized Spontaneous Bleeding Rate (AsBR)
Median (IQR*)0 (0–2.4) 11.73 (2.8–36.5) 0 (0–2.2) 31.76 (0–42.7) Number of subjects with zero bleeding episodes
63 (43.2%)
1 (3.7%)
21 (26.3%)
0Perioperative Management of Bleeding
Thirteen subjects in the adult/adolescent study underwent a total of 16 surgical procedures. Overall, investigators assessed hemostatic efficacy of AFSTYLA in perioperative management of bleeding as excellent in 15 of 16 surgeries and as good in 1 of 16 surgeries (see Table 9). Median factor consumption pre- and intra-operatively was 89.4 IU/kg (range 40.5 to 108.6 IU/kg).
Assessment of hemostasis during surgical procedures by the investigator was as follows:
Excellent: Hemostasis clinically not significantly different from normal (e.g., achieved hemostasis comparable to that expected during similar surgery in a non-factor deficient patient) in the absence of other hemostatic intervention and estimated blood loss during surgery is not more than 20% higher than the predicted blood loss for the intended surgery
Good: Normal or mildly abnormal hemostasis in terms of quantity and/or quality (e.g., slight oozing, prolonged time to hemostasis with somewhat increased bleeding compared to a non-factor deficient patient in the absence of other hemostatic intervention) or estimated blood loss is >20%, but ≤30% higher than the predicted blood loss for intended surgery
Moderate: Moderately abnormal hemostasis in terms of quantity and/or quality (e.g., moderate hemorrhage that is difficult to control) with estimated blood loss greater than what is defined as good
Poor/No Response: Severely abnormal hemostasis in terms of quantity and/or quality (e.g., severe hemorrhage that is difficult to control) and/or additional hemostatic intervention required with another FVIII product, cryoprecipitate, or plasma for complete resolution.
Table 9. Efficacy of AFSTYLA in Perioperative Management of Bleeding Procedure Efficacy Evaluation Factor Consumption (IU/kg)
(pre- and intra-operatively)Extraction of wisdom teeth Excellent 51.09 Abdominal hernia repair Excellent 47.89 Elbow replacement Excellent 108.58 Ankle arthroplasty Excellent 76.83 Knee replacement (5) Excellent (4), Good (1) 92.49
100.9
67.26
105.79
86.09Cholecystectomy
and
Lengthening of the Achilles tendon combined with: Straightening of the right toesExcellent
Excellent105.95 Circumcision (3) Excellent (3) 99.04
92.74
81.5Open reduction internal fixation (ORIF) right ankle Excellent 89.36 Hardware removal, Right ankle Excellent 40.45 - 15 REFERENCES
-
16 HOW SUPPLIED/STORAGE AND HANDLING
AFSTYLA is supplied in a kit containing a lyophilized powder in a single-use vial labeled with the amount of Factor VIII activity, expressed in international units (IU). Actual Factor VIII activity in International Units (IU) is stated on the AFSTYLA carton and vial label.
AFSTYLA is packaged with Sterile Water for Injection, USP (2.5 mL for reconstitution of 250, 500 or 1000 IU or 5 mL for reconstitution of 1500, 2000, 2500, or 3000 IU AFSTYLA), one Mix2Vial filter transfer set, and one sterile alcohol swab. Components are not made of natural rubber latex.
Table 10. How Supplied Nominal Strength Fill Size Color Indicator Kit NDC 250 IU Orange 69911-474-02 500 IU Blue 69911-475-02 1000 IU Green 69911-476-02 1500 IU Turquoise 69911-480-02 2000 IU Purple 69911-477-02 2500 IU Cool Grey 69911-481-02 3000 IU Yellow 69911-478-02 Storage and Handling
- Store AFSTYLA in the original package to protect the AFSTYLA vials from light.
- Store AFSTYLA in powder form at 2°C to 8°C (36°F to 46°F). Do not freeze to avoid damage to the diluent vial. AFSTYLA can be stored at room temperature, not to exceed 25°C (77°F), for a single period of up to 3 months, within the expiration date printed on the carton and vial labels.
- Record the starting date of room temperature on the unopened product carton. Once stored at room temperature, do not return the product to the refrigerator. The shelf-life then expires after storage at room temperature for 3 months, or after the expiration date on the product vial, whichever is earlier.
- Do not use AFSTYLA after the expiration date indicated on the vial.
- The reconstituted product (after mixing dry product with diluent) can be stored at 2°C to 8°C (36°F to 46°F), or at room temperature, not to exceed 25°C (77°F), for up to 4 hours.
- Protect from direct sunlight.
- After reconstitution, if the product is not used within 4 hours, it must be discarded.
- Do not use AFSTYLA if the reconstituted solution is cloudy or has particulate matter.
- Discard any unused AFSTYLA.
-
17 PATIENT COUNSELING INFORMATION
Advise patients to:
- Read the FDA-approved Patient Labeling (Patient Product Information and Instructions for Use).
- Discontinue use of AFSTYLA in case of a hypersensitivity reaction and contact their healthcare provider and/or seek emergency care, depending on the severity of the reaction. Early signs of hypersensitivity reactions may include hives, itching, facial swelling, tightness of the chest, and wheezing [see Warnings and Precautions (5.1)].
- Contact their healthcare provider or hemophilia treatment facility for further treatment and/or assessment if they experience a lack of a clinical response to Factor VIII replacement therapy, as in some cases this may be a manifestation of an inhibitor [see Warnings and Precautions (5.2)].
- Report any adverse reactions or problems following AFSTYLA administration to their healthcare provider.
-
SPL UNCLASSIFIED SECTION
Manufactured by:
CSL Behring GmbH
35041 Marburg, Germanyfor:
CSL Behring Lengnau AG
Industriestrasse 11
2543 Lengnau, Switzerland
US License No. 2009Distributed by:
CSL Behring LLC
Kankakee, IL 60901 USAMix2Vial® is a registered trademark of West Pharma. Services IL, Ltd., a subsidiary of West Pharmaceuticals Services, Inc.
-
PATIENT PACKAGE INSERT
FDA-Approved Patient Labeling – Patient Product Information (PPI)
AFSTYLA / af sty̆ ̍lah /
Antihemophilic Factor (Recombinant), Single Chain
Freeze-Dried Powder for Reconstitution
This leaflet summarizes important information about AFSTYLA. Please read it carefully before using AFSTYLA. This information does not take the place of talking with your healthcare provider, and it does not include all of the important information about AFSTYLA. If you have any questions after reading this, ask your healthcare provider.
What is the most important information I need to know about AFSTYLA?
- Your healthcare provider or hemophilia treatment center will instruct you on how to do an infusion on your own.
- Carefully follow your healthcare provider's instructions regarding the dose and schedule for infusing this medicine.
What is AFSTYLA?
- AFSTYLA, Antihemophilic Factor (Recombinant), Single Chain is a medicine used to replace clotting Factor VIII that is missing in patients with hemophilia A.
- Hemophilia A is an inherited bleeding disorder that prevents blood from clotting normally.
- Does not contain human plasma-derived proteins or albumin.
- Your healthcare provider may give you this medicine when you have surgery.
- Is used to treat and control bleeding in all patients with hemophilia A.
- Can reduce the number of bleeding episodes when used regularly (prophylaxis) and reduce the risk of joint damage due to bleeding.
- Is not used to treat von Willebrand disease.
Who should not use AFSTYLA?
You should not use AFSTYLA if you:
- Have had a life-threatening allergic reaction to it in the past.
- Are allergic to its ingredients or hamster proteins.
Tell your healthcare provider if you are pregnant or breastfeeding because AFSTYLA may not be right for you.
What should I tell my healthcare provider before using AFSTYLA?
Tell your healthcare provider if you:
- Have or have had any medical problems.
- Take any medicines, including prescription and non-prescription medicines, such as over-the-counter medicines, supplements or herbal remedies.
- Have any allergies, including allergies to hamster proteins.
- Are pregnant or planning to become pregnant. It is not known if AFSTYLA may harm your unborn baby.
- Are breastfeeding. It is not known if AFSTYLA passes into the milk or if it can harm your baby.
- Have been told you have inhibitors to Factor VIII (because this medicine may not work for you).
How should I use AFSTYLA?
- Administer directly into the bloodstream.
- Use as ordered by your healthcare provider.
- You should be trained on how to do intravenous injections by your healthcare provider or hemophilia treatment center. Once trained, many patients with hemophilia A are able to inject this medicine by themselves or with the help of a family member.
- Your healthcare provider will tell you how much to use based on your weight, the severity of your hemophilia A, and where you are bleeding.
- You may need to have blood tests done after getting AFSTYLA to be sure that your blood level of Factor VIII is high enough to clot your blood.
- Call your healthcare provider right away if your bleeding does not stop after taking this medicine.
What are the possible side effects of AFSTYLA?
- Allergic reactions may occur. Immediately stop treatment and call your healthcare provider right away if you get a rash or hives, itching, tightness of the chest or throat, difficulty breathing, light-headedness, dizziness, nausea, or decrease in blood pressure.
- Your body may form inhibitors to Factor VIII. An inhibitor is a part of the body's defense system. If you form inhibitors, it may stop this medicine from working properly. The greatest risk of this occurring is in previously untreated patients. Your healthcare provider may need to test your blood for inhibitors from time to time.
- Common side effects are dizziness and allergic reactions.
- These are not the only side effects possible. Tell your healthcare provider about any side effect that bothers you or does not go away.
What are the AFSTYLA dosage strengths?
AFSTYLA comes in seven different dosage strengths: 250, 500, 1000, 1500, 2000, 2500, or 3000 International Units (IU) as provided in Table 1. The actual strength is printed on the carton and vial label.
Table 1. AFSTYLA Dosage Strengths Fill Size Color Indicator Strengths Orange Dosage strength of approximately 250 IU per vial Blue Dosage strength of approximately 500 IU per vial Green Dosage strength of approximately 1000 IU per vial Turquoise Dosage strength of approximately 1500 IU per vial Purple Dosage strength of approximately 2000 IU per vial Cool Grey Dosage strength of approximately 2500 IU per vial Yellow Dosage strength of approximately 3000 IU per vial Always check the actual dosage strength printed on the label to make sure you are using the strength prescribed by your healthcare provider.
How should I store AFSTYLA?
- Store this medicine in the original package to protect the vials from light.
- Store this medicine in powder form at 2°C to 8°C (36°F to 46°F). Do not freeze to avoid damage to the diluent vial. It can be stored at room temperature, not to exceed 25°C (77°F), for a single period of up to 3 months, within the expiration date printed on the carton and vial labels.
- If stored at room temperature, record the date that this medicine is removed from refrigeration on the top flap of the carton in the area provided. After storage at room temperature, do not return the product to the refrigerator. The powder form for the product then expires after storage at room temperature for 3 months, or after the expiration date on the product vial, whichever is earlier.
- The reconstituted product (after mixing dry product with diluent) can be stored for 4 hours at a temperature not to exceed 25°C (77°F). Protect from direct sunlight. After reconstitution, if the product is not used within 4 hours, it must be discarded.
What else should I know about AFSTYLA?
- Medicines are sometimes prescribed for purposes other than those listed here. Do not use this medicine for a condition for which it is not prescribed. Do not share with other people, even if they have the same symptoms that you have.
Instructions for Use of AFSTYLA
For intravenous use after reconstitution only
This medicine is infused into a vein. Your healthcare provider or hemophilia treatment center should teach you how to do infusions on your own.
Always follow the specific instructions given by your healthcare provider. The steps listed below are general guidelines for using AFSTYLA. If you are unsure of the instructions, call your healthcare provider before using AFSTYLA. Call your healthcare provider right away if bleeding is not controlled after using AFSTYLA. Your healthcare provider will prescribe the dose that you should take. You may need to take blood tests from time to time. Talk to your healthcare provider before traveling. Dispose of all unused solution, empty vial(s), and other used medical supplies in an appropriate medical waste container.
- Always work on a clean flat surface and wash your hands before performing the reconstitution procedures.
- Use only the components for reconstitution that are provided with each package.
- If a package is opened or damaged, do not use and contact your healthcare provider.
- Do not use AFSTYLA beyond the expiration date on the vial and carton labels. If stored at room temperature, the dry product (prior to reconstitution) expires after storage at room temperature for 3 months or after the expiration date on the product vial, whichever is earlier.
- Look at the mixed (reconstituted) solution. Do not use AFSTYLA if the reconstituted solution is cloudy, contains any particles, or is discolored.
- AFSTYLA is for single use only and contains no preservatives. Discard partially used vials.
AFSTYLA Reconstitution Instructions
- Ensure that the AFSTYLA vial and diluent vial are at room temperature.
- Place the AFSTYLA vial, diluent vial, and Mix2Vial® transfer set on a flat surface.
- Remove AFSTYLA and diluent vial flip caps. Wipe the stoppers with the sterile alcohol swab provided and allow the stoppers to dry prior to opening the Mix2Vial transfer set package.
- Open the Mix2Vial transfer set package by peeling away the lid (Fig. 1). Leave the Mix2Vial transfer set in the clear package.
Fig. 1
- Place the diluent vial on a flat surface and hold the vial tightly. Grip the Mix2Vial transfer set together with the clear package and push the plastic spike at the blue end of the Mix2Vial transfer set firmly through the center of the stopper of the diluent vial (Fig. 2).

Fig. 2
- Carefully remove the clear package from the Mix2Vial transfer set. Make sure that you pull up only the clear package, not the Mix2Vial transfer set (Fig. 3).

Fig. 3
- With the AFSTYLA vial placed firmly on a flat surface, invert the diluent vial with the Mix2Vial transfer set attached and push the plastic spike of the transparent adapter firmly through the center of the stopper of the AFSTYLA vial (Fig. 4). The diluent will automatically transfer into the AFSTYLA vial.
Fig. 4
- With the diluent and AFSTYLA vial still attached to the Mix2Vial transfer set, gently swirl the AFSTYLA vial to ensure that the AFSTYLA is fully dissolved (Fig. 5). Do not shake the vial.
Fig. 5
- With one hand, grasp the AFSTYLA side of the Mix2Vial transfer set and with the other hand grasp the blue diluent-side of the Mix2Vial transfer set, and unscrew the set into two pieces. (Fig. 6).
Fig. 6
- Draw air into an empty, sterile syringe. While the AFSTYLA vial is upright, screw the syringe to the Mix2Vial transfer set. Inject air into the AFSTYLA vial. While keeping the syringe plunger pressed, invert the system upside down and draw the concentrate into the syringe by pulling the plunger back slowly. (Fig. 7).
Fig. 7
- Now that the concentrate has been transferred into the syringe, firmly grasp the barrel of the syringe (keeping the plunger facing down) and unscrew the syringe from the Mix2Vial transfer set (Fig. 8).

Fig. 8
- After reconstitution, infuse immediately or within 4 hours. The mixed (reconstituted) solution may be stored at room temperature, not to exceed 25°C (77°F), for up to 4 hours. Do not freeze. Protect from direct sunlight.
- Record treatment – Remove the peel-off portion of the label from each vial used, and affix it to the patient's treatment diary/log book or scan the vial if recording the infusion electronically.
- If the dose requires more than one vial, use a separate unused Mix2Vial transfer set for each product vial. Repeat step 10 to pool the contents into one syringe.
Administration (intravenous injection)
- Do not mix AFSTYLA in the same tubing or container with other medicinal products.
- Attach the syringe containing the mixed (reconstituted) solution to a sterile infusion set and give an injection as directed by your healthcare provider or hemophilia treatment center.
- Administer intravenously. Do not exceed infusion rate of 10 mL per minute.
-
SPL UNCLASSIFIED SECTION
Resources at CSL Behring available to the patient:
For Adverse Reaction Reporting contact:
CSL Behring Pharmacovigilance Department at 1-866-915-6958Contact CSL Behring to receive more product information:
Patient Support Hotline at 1-800-676-4266For more information, visit www.AFSTYLA.com
Manufactured by:
CSL Behring GmbH
35041 Marburg, Germanyfor:
CSL Behring Lengnau AG
Industriestrasse 11
2543 Lengnau, Switzerland
US License No. 2009Distributed by:
CSL Behring LLC
Kankakee, IL 60901 USAMix2Vial® is a registered trademark of West Pharma. Services IL, Ltd., a subsidiary of West Pharmaceuticals Services, Inc.
Revised: 12/2019
-
PRINCIPAL DISPLAY PANEL - Kit Carton - 250 IU
NDC: 69911-474-02
250 IU Range
AFSTYLA®
Antihemophilic Factor (Recombinant),
Single ChainOne single-use vial containing lyophilized powder for reconstitution.
For Intravenous Administration Only
CSL Behring
-
PRINCIPAL DISPLAY PANEL - Kit Carton - 500 IU
NDC: 69911-475-02
500 IU Range
AFSTYLA®
Antihemophilic Factor (Recombinant),
Single ChainOne single-use vial containing lyophilized powder for reconstitution.
For Intravenous Administration Only
CSL Behring
-
PRINCIPAL DISPLAY PANEL - Kit Carton - 1000 IU
NDC: 69911-476-02
1000 IU Range
AFSTYLA®
Antihemophilic Factor (Recombinant),
Single ChainOne single-use vial containing lyophilized powder for reconstitution.
For Intravenous Administration Only
CSL Behring
-
PRINCIPAL DISPLAY PANEL - Kit Carton - 2000 IU
NDC: 69911-477-02
2000 IU Range
AFSTYLA®
Antihemophilic Factor (Recombinant),
Single ChainOne single-use vial containing lyophilized powder for reconstitution.
For Intravenous Administration Only
CSL Behring
-
PRINCIPAL DISPLAY PANEL - Kit Carton - 3000 IU
NDC: 69911-478-02
3000 IU Range
AFSTYLA®
Antihemophilic Factor (Recombinant),
Single ChainOne single-use vial containing lyophilized powder for reconstitution.
For Intravenous Administration Only
CSL Behring
-
PRINCIPAL DISPLAY PANEL - Kit Carton - 1500 IU
NDC: 69911-480-02
1500 IU Range
AFSTYLA®
Antihemophilic Factor (Recombinant),
Single ChainOne single-use vial containing lyophilized powder for reconstitution.
For Intravenous Administration Only
CSL Behring
-
PRINCIPAL DISPLAY PANEL - Kit Carton - 2500 IU
NDC: 69911-481-02
2500 IU Range
AFSTYLA®
Antihemophilic Factor (Recombinant),
Single ChainOne single-use vial containing lyophilized powder for reconstitution.
For Intravenous Administration Only
CSL Behring
-
INGREDIENTS AND APPEARANCE
AFSTYLA ANTIHEMOPHILIC FACTOR (RECOMBINANT), SINGLE CHAIN
antihemophilic factor, human recombinant kitProduct Information Product Type PLASMA DERIVATIVE Item Code (Source) NDC: 69911-474 Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 69911-474-02 1 in 1 CARTON Quantity of Parts Part # Package Quantity Total Product Quantity Part 1 1 VIAL, SINGLE-USE 2.5 mL Part 2 1 VIAL, SINGLE-USE 2.5 mL Part 1 of 2 AFSTYLA ANTIHEMOPHILIC FACTOR (RECOMBINANT), SINGLE CHAIN
antihemophilic factor, human recombinant injection, powder, for solutionProduct Information Item Code (Source) NDC: 69911-484 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength LONOCTOCOG ALFA (UNII: VQ723R7O8R) (LONOCTOCOG ALFA - UNII:VQ723R7O8R) LONOCTOCOG ALFA 250 [iU] in 2.5 mL Inactive Ingredients Ingredient Name Strength Histidine (UNII: 4QD397987E) Polysorbate 80 (UNII: 6OZP39ZG8H) Calcium chloride (UNII: M4I0D6VV5M) Sodium chloride (UNII: 451W47IQ8X) Sucrose (UNII: C151H8M554) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 69911-484-01 2.5 mL in 1 VIAL, SINGLE-USE; Type 1: Convenience Kit of Co-Package Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA125591 05/25/2016 Part 2 of 2 STERILE WATER
water injection, solutionProduct Information Item Code (Source) NDC: 69911-765 Route of Administration INTRAVENOUS Inactive Ingredients Ingredient Name Strength water (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 69911-765-83 2.5 mL in 1 VIAL, SINGLE-USE; Type 1: Convenience Kit of Co-Package Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA125591 05/25/2016 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA125591 05/25/2016 AFSTYLA ANTIHEMOPHILIC FACTOR (RECOMBINANT), SINGLE CHAIN
antihemophilic factor, human recombinant kitProduct Information Product Type PLASMA DERIVATIVE Item Code (Source) NDC: 69911-475 Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 69911-475-02 1 in 1 CARTON Quantity of Parts Part # Package Quantity Total Product Quantity Part 1 1 VIAL, SINGLE-USE 2.5 mL Part 2 1 VIAL, SINGLE-USE 2.5 mL Part 1 of 2 AFSTYLA ANTIHEMOPHILIC FACTOR (RECOMBINANT), SINGLE CHAIN
antihemophilic factor, human recombinant injection, powder, for solutionProduct Information Item Code (Source) NDC: 69911-485 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength LONOCTOCOG ALFA (UNII: VQ723R7O8R) (LONOCTOCOG ALFA - UNII:VQ723R7O8R) LONOCTOCOG ALFA 500 [iU] in 2.5 mL Inactive Ingredients Ingredient Name Strength Histidine (UNII: 4QD397987E) Polysorbate 80 (UNII: 6OZP39ZG8H) Calcium chloride (UNII: M4I0D6VV5M) Sodium chloride (UNII: 451W47IQ8X) Sucrose (UNII: C151H8M554) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 69911-485-01 2.5 mL in 1 VIAL, SINGLE-USE; Type 1: Convenience Kit of Co-Package Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA125591 06/13/2016 Part 2 of 2 STERILE WATER
water injection, solutionProduct Information Item Code (Source) NDC: 69911-765 Route of Administration INTRAVENOUS Inactive Ingredients Ingredient Name Strength water (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 69911-765-83 2.5 mL in 1 VIAL, SINGLE-USE; Type 1: Convenience Kit of Co-Package Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA125591 06/13/2016 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA125591 05/25/2016 AFSTYLA ANTIHEMOPHILIC FACTOR (RECOMBINANT), SINGLE CHAIN
antihemophilic factor, human recombinant kitProduct Information Product Type PLASMA DERIVATIVE Item Code (Source) NDC: 69911-476 Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 69911-476-02 1 in 1 CARTON Quantity of Parts Part # Package Quantity Total Product Quantity Part 1 1 VIAL, SINGLE-USE 2.5 mL Part 2 1 VIAL, SINGLE-USE 2.5 mL Part 1 of 2 AFSTYLA ANTIHEMOPHILIC FACTOR (RECOMBINANT), SINGLE CHAIN
antihemophilic factor, human recombinant injection, powder, for solutionProduct Information Item Code (Source) NDC: 69911-486 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength LONOCTOCOG ALFA (UNII: VQ723R7O8R) (LONOCTOCOG ALFA - UNII:VQ723R7O8R) LONOCTOCOG ALFA 1000 [iU] in 2.5 mL Inactive Ingredients Ingredient Name Strength Histidine (UNII: 4QD397987E) Polysorbate 80 (UNII: 6OZP39ZG8H) Calcium chloride (UNII: M4I0D6VV5M) Sodium chloride (UNII: 451W47IQ8X) Sucrose (UNII: C151H8M554) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 69911-486-01 2.5 mL in 1 VIAL, SINGLE-USE; Type 1: Convenience Kit of Co-Package Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA125591 06/13/2016 Part 2 of 2 STERILE WATER
water injection, solutionProduct Information Item Code (Source) NDC: 69911-765 Route of Administration INTRAVENOUS Inactive Ingredients Ingredient Name Strength water (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 69911-765-83 2.5 mL in 1 VIAL, SINGLE-USE; Type 1: Convenience Kit of Co-Package Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA125591 06/13/2016 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA125591 05/25/2016 AFSTYLA ANTIHEMOPHILIC FACTOR (RECOMBINANT), SINGLE CHAIN
antihemophilic factor, human recombinant kitProduct Information Product Type PLASMA DERIVATIVE Item Code (Source) NDC: 69911-477 Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 69911-477-02 1 in 1 CARTON Quantity of Parts Part # Package Quantity Total Product Quantity Part 1 1 VIAL, SINGLE-USE 5 mL Part 2 1 VIAL, SINGLE-USE 5 mL Part 1 of 2 AFSTYLA ANTIHEMOPHILIC FACTOR (RECOMBINANT), SINGLE CHAIN
antihemophilic factor, human recombinant injection, powder, for solutionProduct Information Item Code (Source) NDC: 69911-487 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength LONOCTOCOG ALFA (UNII: VQ723R7O8R) (LONOCTOCOG ALFA - UNII:VQ723R7O8R) LONOCTOCOG ALFA 2000 [iU] in 5 mL Inactive Ingredients Ingredient Name Strength Histidine (UNII: 4QD397987E) Polysorbate 80 (UNII: 6OZP39ZG8H) Calcium chloride (UNII: M4I0D6VV5M) Sodium chloride (UNII: 451W47IQ8X) Sucrose (UNII: C151H8M554) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 69911-487-01 5 mL in 1 VIAL, SINGLE-USE; Type 1: Convenience Kit of Co-Package Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA125591 06/13/2016 Part 2 of 2 STERILE WATER
water injection, solutionProduct Information Item Code (Source) NDC: 69911-765 Route of Administration INTRAVENOUS Inactive Ingredients Ingredient Name Strength water (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 69911-765-84 5 mL in 1 VIAL, SINGLE-USE; Type 1: Convenience Kit of Co-Package Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA125591 06/13/2016 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA125591 05/25/2016 AFSTYLA ANTIHEMOPHILIC FACTOR (RECOMBINANT), SINGLE CHAIN
antihemophilic factor, human recombinant kitProduct Information Product Type PLASMA DERIVATIVE Item Code (Source) NDC: 69911-478 Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 69911-478-02 1 in 1 CARTON Quantity of Parts Part # Package Quantity Total Product Quantity Part 1 1 VIAL, SINGLE-USE 5 mL Part 2 1 VIAL, SINGLE-USE 5 mL Part 1 of 2 AFSTYLA ANTIHEMOPHILIC FACTOR (RECOMBINANT), SINGLE CHAIN
antihemophilic factor, human recombinant injection, powder, for solutionProduct Information Item Code (Source) NDC: 69911-488 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength LONOCTOCOG ALFA (UNII: VQ723R7O8R) (LONOCTOCOG ALFA - UNII:VQ723R7O8R) LONOCTOCOG ALFA 3000 [iU] in 5 mL Inactive Ingredients Ingredient Name Strength Histidine (UNII: 4QD397987E) Polysorbate 80 (UNII: 6OZP39ZG8H) Calcium chloride (UNII: M4I0D6VV5M) Sodium chloride (UNII: 451W47IQ8X) Sucrose (UNII: C151H8M554) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 69911-488-01 5 mL in 1 VIAL, SINGLE-USE; Type 1: Convenience Kit of Co-Package Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA125591 06/13/2016 Part 2 of 2 STERILE WATER
water injection, solutionProduct Information Item Code (Source) NDC: 69911-765 Route of Administration INTRAVENOUS Inactive Ingredients Ingredient Name Strength water (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 69911-765-84 5 mL in 1 VIAL, SINGLE-USE; Type 1: Convenience Kit of Co-Package Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA125591 06/13/2016 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA125591 05/25/2016 AFSTYLA ANTIHEMOPHILIC FACTOR (RECOMBINANT), SINGLE CHAIN
antihemophilic factor, human recombinant kitProduct Information Product Type PLASMA DERIVATIVE Item Code (Source) NDC: 69911-480 Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 69911-480-02 1 in 1 CARTON Quantity of Parts Part # Package Quantity Total Product Quantity Part 1 1 VIAL, SINGLE-USE 5 mL Part 2 1 VIAL, SINGLE-USE 5 mL Part 1 of 2 AFSTYLA ANTIHEMOPHILIC FACTOR (RECOMBINANT), SINGLE CHAIN
antihemophilic factor, human recombinant injection, powder, for solutionProduct Information Item Code (Source) NDC: 69911-490 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength LONOCTOCOG ALFA (UNII: VQ723R7O8R) (LONOCTOCOG ALFA - UNII:VQ723R7O8R) LONOCTOCOG ALFA 1500 [iU] in 5 mL Inactive Ingredients Ingredient Name Strength Histidine (UNII: 4QD397987E) Polysorbate 80 (UNII: 6OZP39ZG8H) Calcium chloride (UNII: M4I0D6VV5M) Sodium chloride (UNII: 451W47IQ8X) Sucrose (UNII: C151H8M554) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 69911-490-01 5 mL in 1 VIAL, SINGLE-USE; Type 1: Convenience Kit of Co-Package Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA125591 03/29/2017 Part 2 of 2 STERILE WATER
water injection, solutionProduct Information Item Code (Source) NDC: 69911-765 Route of Administration INTRAVENOUS Inactive Ingredients Ingredient Name Strength water (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 69911-765-84 5 mL in 1 VIAL, SINGLE-USE; Type 1: Convenience Kit of Co-Package Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA125591 03/29/2017 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA125591 03/28/2017 AFSTYLA ANTIHEMOPHILIC FACTOR (RECOMBINANT), SINGLE CHAIN
antihemophilic factor, human recombinant kitProduct Information Product Type PLASMA DERIVATIVE Item Code (Source) NDC: 69911-481 Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 69911-481-02 1 in 1 CARTON Quantity of Parts Part # Package Quantity Total Product Quantity Part 1 1 VIAL, SINGLE-USE 5 mL Part 2 1 VIAL, SINGLE-USE 5 mL Part 1 of 2 AFSTYLA ANTIHEMOPHILIC FACTOR (RECOMBINANT), SINGLE CHAIN
antihemophilic factor, human recombinant injection, powder, for solutionProduct Information Item Code (Source) NDC: 69911-491 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength LONOCTOCOG ALFA (UNII: VQ723R7O8R) (LONOCTOCOG ALFA - UNII:VQ723R7O8R) LONOCTOCOG ALFA 2500 [iU] in 5 mL Inactive Ingredients Ingredient Name Strength Histidine (UNII: 4QD397987E) Polysorbate 80 (UNII: 6OZP39ZG8H) Calcium chloride (UNII: M4I0D6VV5M) Sodium chloride (UNII: 451W47IQ8X) Sucrose (UNII: C151H8M554) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 69911-491-01 5 mL in 1 VIAL, SINGLE-USE; Type 1: Convenience Kit of Co-Package Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA125591 03/29/2017 Part 2 of 2 STERILE WATER
water injection, solutionProduct Information Item Code (Source) NDC: 69911-765 Route of Administration INTRAVENOUS Inactive Ingredients Ingredient Name Strength water (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 69911-765-84 5 mL in 1 VIAL, SINGLE-USE; Type 1: Convenience Kit of Co-Package Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA125591 03/29/2017 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA125591 03/28/2017 Labeler - CSL Behring Lengnau AG (480217014) Establishment Name Address ID/FEI Business Operations CSL Behring GmbH 326530474 MANUFACTURE(69911-474, 69911-475, 69911-476, 69911-477, 69911-478, 69911-480, 69911-481) Establishment Name Address ID/FEI Business Operations CSL Behring LLC 058268293 LABEL(69911-474, 69911-475, 69911-476, 69911-477, 69911-478, 69911-480, 69911-481)
Trademark Results [AFSTYLA]
Mark Image Registration | Serial | Company Trademark Application Date |
|---|---|
 AFSTYLA 86286410 4754520 Live/Registered |
CSL BEHRING RECOMBINANT FACILITY AG 2014-05-20 |
 AFSTYLA 86279991 not registered Dead/Abandoned |
CSL Limited 2014-05-13 |
 AFSTYLA 79337443 not registered Live/Pending |
CSL Behring Lengnau AG 2022-01-31 |
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.