BAVENCIO- avelumab injection, solution, concentrate
BAVENCIO by
Drug Labeling and Warnings
BAVENCIO by is a Prescription medication manufactured, distributed, or labeled by EMD Serono, Inc.. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use BAVENCIO safely and effectively. See full prescribing information for BAVENCIO.
BAVENCIO® (avelumab) injection, for intravenous use
Initial U.S. Approval: 2017RECENT MAJOR CHANGES
INDICATIONS AND USAGE
BAVENCIO is a programmed death ligand-1 (PD-L1) blocking antibody indicated for:
- Adults and pediatric patients 12 years and older with metastatic Merkel cell carcinoma (MCC).a (1.1)
- Patients with locally advanced or metastatic urothelial carcinoma (UC) who:
- First-line treatment, in combination with axitinib of patients with advanced renal cell carcinoma (RCC). (1.3, 14.3)
a This indication is approved under accelerated approval based on tumor response rate and duration of response. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials.
DOSAGE AND ADMINISTRATION
- Premedicate for the first 4 infusions and subsequently as needed. (2.1)
- Merkel Cell Carcinoma: 800 mg every 2 weeks (2.2)
- Urothelial Carcinoma; 800 mg every 2 weeks. (2.3)
- Renal Cell Carcinoma: 800 mg every 2 weeks in combination with axitinib 5 mg orally twice daily. (2.4)
Administer BAVENCIO as an intravenous infusion over 60 minutes
DOSAGE FORMS AND STRENGTHS
Injection: 200 mg/10 mL (20 mg/mL) solution in single-dose vial. (3)
CONTRAINDICATIONS
None. (4)
WARNINGS AND PRECAUTIONS
- Immune-mediated pneumonitis: Withhold for moderate pneumonitis; permanently discontinue for severe, life-threatening, or recurrent moderate pneumonitis. (5.1)
- Hepatotoxicity and immune-mediated hepatitis: Monitor for changes in liver function. Withhold for moderate hepatitis; permanently discontinue for severe or life-threatening hepatitis. (5.2)
- Immune-mediated colitis: Withhold for moderate or severe colitis; permanently discontinue for life-threatening or recurrent severe colitis. (5.3)
- Immune-mediated endocrinopathies: Withhold for severe or life-threatening endocrinopathies (5.4)
- Immune-mediated nephritis and renal dysfunction: Withhold for moderate or severe nephritis and renal dysfunction; permanently discontinue for life-threatening nephritis or renal dysfunction. (5.5)
- Infusion-related reactions: Interrupt or slow the rate of infusion for mild or moderate infusion-related reactions. Stop the infusion and permanently discontinue BAVENCIO for severe or life-threatening infusion-related reactions. (5.7)
- Major adverse cardiovascular events: Optimize management of cardiovascular risk factors. Discontinue BAVENCIO in combination with axitinib for Grade 3-4 events. (5.8)
- Embryo-fetal toxicity: BAVENCIO can cause fetal harm. Advise of potential risk to a fetus and use of effective contraception. (5.9, 8.1, 8.3)
ADVERSE REACTIONS
Most common adverse reactions (≥ 20%) were:
BAVENCIO in patients with metastatic Merkel cell carcinoma: fatigue, musculoskeletal pain, diarrhea, nausea, infusion-related reaction, rash, decreased appetite, and peripheral edema. (6.1)
BAVENCIO in patients with locally advanced or metastatic urothelial carcinoma: fatigue, infusion-related reaction, musculoskeletal pain, nausea, decreased appetite, and urinary tract infection. (6.1)
BAVENCIO with axitinib in patients with RCC: diarrhea, fatigue, hypertension, musculoskeletal pain, nausea, mucositis, palmar-plantar erythrodysesthesia, dysphonia, decreased appetite, hypothyroidism, rash, hepatotoxicity, cough, dyspnea, abdominal pain, and headache. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact EMD Serono at 1-800-283-8088 ext. 5563 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide.
Revised: 5/2019
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
1.1 Metastatic Merkel Cell Carcinoma
1.2 Locally Advanced or Metastatic Urothelial Carcinoma
1.3 Advanced Renal Cell Carcinoma
2 DOSAGE AND ADMINISTRATION
2.1 Premedication
2.2 Recommended Dosage for MCC
2.3 Recommended Dosage for UC
2.4 Recommended Dosage for RCC
2.5 Dose Modifications
2.6 Preparation and Administration
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Immune-Mediated Pneumonitis
5.2 Hepatotoxicity and Immune-Mediated Hepatitis
5.3 Immune-Mediated Colitis
5.4 Immune-Mediated Endocrinopathies
5.5 Immune-Mediated Nephritis and Renal Dysfunction
5.6 Other Immune-Mediated Adverse Reactions
5.7 Infusion-Related Reactions
5.8 Major Adverse Cardiovascular Events (MACE)
5.9 Embryo-Fetal Toxicity
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
6.2 Immunogenicity
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.3 Females and Males of Reproductive Potential
8.4 Pediatric Use
8.5 Geriatric Use
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
13.2 Animal Toxicology and/or Pharmacology
14 CLINICAL STUDIES
14.1 Metastatic Merkel Cell Carcinoma
14.2 Locally Advanced or Metastatic Urothelial Carcinoma
14.3 Advanced Renal Cell Carcinoma
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- * Sections or subsections omitted from the full prescribing information are not listed.
-
1 INDICATIONS AND USAGE
1.1 Metastatic Merkel Cell Carcinoma
BAVENCIO (avelumab) is indicated for the treatment of adults and pediatric patients 12 years and older with metastatic Merkel cell carcinoma (MCC).
This indication is approved under accelerated approval based on tumor response rate and duration of response. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials [see Clinical Studies (14.1)].
1.2 Locally Advanced or Metastatic Urothelial Carcinoma
BAVENCIO is indicated for the treatment of patients with locally advanced or metastatic urothelial carcinoma (UC) who:
- Have disease progression during or following platinum-containing chemotherapy
- Have disease progression within 12 months of neoadjuvant or adjuvant treatment with platinum-containing chemotherapy
This indication is approved under accelerated approval based on tumor response rate and duration of response. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials [see Clinical Studies (14.2)].
1.3 Advanced Renal Cell Carcinoma
BAVENCIO in combination with axitinib is indicated for the first-line treatment of patients with advanced renal cell carcinoma (RCC) [see Clinical Studies (14.3)].
-
2 DOSAGE AND ADMINISTRATION
2.1 Premedication
Premedicate patients with an antihistamine and with acetaminophen prior to the first 4 infusions of BAVENCIO. Premedication should be administered for subsequent BAVENCIO doses based upon clinical judgment and presence/severity of prior infusion reactions [see Dosage and Administration (2.5) and Warnings and Precautions (5.7)].
2.2 Recommended Dosage for MCC
The recommended dose of BAVENCIO is 800 mg administered as an intravenous infusion over 60 minutes every 2 weeks until disease progression or unacceptable toxicity.
2.3 Recommended Dosage for UC
The recommended dose of BAVENCIO is 800 mg administered as an intravenous infusion over 60 minutes every 2 weeks until disease progression or unacceptable toxicity.
2.4 Recommended Dosage for RCC
The recommended dose of BAVENCIO is 800 mg administered as an intravenous infusion over 60 minutes every 2 weeks in combination with axitinib 5 mg orally taken twice daily (12 hours apart) with or without food until disease progression or unacceptable toxicity.
When axitinib is used in combination with BAVENCIO, dose escalation of axitinib above the initial 5 mg dose may be considered at intervals of two weeks or longer. Review the Full Prescribing Information for axitinib prior to initiation.
2.5 Dose Modifications
Recommended dose modifications of BAVENCIO for adverse reactions are provided in Table 1. Detailed information regarding clinical and laboratory monitoring guidelines for early detection of adverse reactions of BAVENCIO and recommended management (immunosuppressant treatment guidelines) are described in Warnings and Precautions (5).
Table 1: Recommended Dose Modifications of BAVENCIO for Adverse Reactions Treatment-Related Adverse Reaction Severity of Adverse Reactions* Dose Modification - * Toxicity was graded per National Cancer Institute Common Terminology Criteria for Adverse Events. Version 4.0 (NCI CTCAE v4)
- † Observed with BAVENCIO or with other anti-PD-1/PD-L1 monoclonal antibodies
Pneumonitis [see Warnings and Precautions (5.1)] Grade 2 pneumonitis Withhold BAVENCIO.
Resume BAVENCIO in patients with complete or partial resolution (Grade 0 to 1) of pneumonitis after corticosteroid taper.Grade 3 or 4 pneumonitis or recurrent Grade 2 pneumonitis Permanently discontinue. Hepatitis [see Warnings and Precautions (5.2)]
For BAVENCIO in combination with axitinib, see below.Aspartate aminotransferase (AST)/or alanine aminotransferase (ALT) more than 3 and up to 5 times the upper limit of normal or total bilirubin more than 1.5 and up to 3 times the upper limit of normal Withhold BAVENCIO.
Resume BAVENCIO in patients with complete or partial resolution (Grade 0 to 1) of hepatitis after corticosteroid taper.AST or ALT more than 5 times the upper limit of normal or total bilirubin more than 3 times the upper limit of normal Permanently discontinue. Colitis [see Warnings and Precautions (5.3)] Grade 2 or 3 diarrhea or colitis Withhold BAVENCIO.
Resume BAVENCIO in patients with complete or partial resolution (Grade 0 to 1) of colitis or diarrhea after corticosteroid taper.Grade 4 diarrhea or colitis or recurrent Grade 3 diarrhea or colitis Permanently discontinue. Endocrinopathies (including but not limited to hypothyroidism, hyperthyroidism, adrenal insufficiency, hyperglycemia) [see Warnings and Precautions (5.4)] Grade 3 or 4 Withhold BAVENCIO.
Resume BAVENCIO in patients with complete or partial resolution (Grade 0 to 1) of endocrinopathies after corticosteroid taper.Nephritis and Renal Dysfunction [see Warnings and Precautions (5.5)] Serum creatinine more than 1.5 and up to 6 times the upper limit of normal Withhold BAVENCIO.
Resume BAVENCIO in patients with complete or partial resolution (Grade 0 to 1) of nephritis and renal dysfunction after corticosteroid taper.Serum creatinine more than 6 times the upper limit of normal Permanently discontinue. Other immune-mediated adverse reactions (including but not limited to myocarditis, pancreatitis, myositis, psoriasis, arthritis, exfoliative dermatitis, erythema multiforme, pemphigoid, hypopituitarism, uveitis, Guillain-Barré syndrome, bullous dermatitis, Stevens Johnson Syndrome (SJS)/toxic epidermal necrolysis (TEN), rhabdomyolysis, myasthenia gravis, histiocytic necrotizing lymphadenitis, demyelination, vasculitis, hemolytic anemia, hypophysitis, iritis, and encephalitis)† [see Warnings and Precautions (5.6)] For any of the following: - Moderate or severe clinical signs or symptoms of an immune-mediated adverse reaction not described above
- Grade 3 or 4 endocrinopathies
Withhold BAVENCIO pending clinical evaluation.
Resume BAVENCIO in patients with complete or partial resolution (Grade 0 to 1) of other immune-mediated adverse reactions after corticosteroid taper.For any of the following: - Life-threatening adverse reaction (excluding endocrinopathies)
- Recurrent severe immune-mediated adverse reaction
- Requirement for 10 mg per day or greater prednisone or equivalent for more than 12 weeks
- Persistent Grade 2 or 3 immune-mediated adverse reactions lasting 12 weeks or longer
Permanently discontinue. Infusion-related reaction [see Warnings and Precautions (5.7)] Grade 1 or 2 Interrupt or slow the rate of infusion. Grade 3 or 4 Permanently discontinue. In patients with RCC being treated with BAVENCIO in combination with axitinib:
- If ALT or AST ≥ 3 times ULN but < 5 times ULN or total bilirubin ≥ 1.5 times ULN but < 3 times ULN, withhold both BAVENCIO and axitinib until these adverse reactions recover to Grades 0-1. If persistent (greater than 5 days), consider corticosteroid therapy [initial dose of 0.5 to 1 mg/kg/day] prednisone or equivalent followed by a taper. Consider rechallenge with a single drug or sequential rechallenge with both drugs after recovery. Dose reduce per the axitinib Full Prescribing Information if rechallenging with axitinib.
- If ALT or AST ≥ 5 times ULN or > 3 times ULN with concurrent total bilirubin ≥ 2 times ULN or total bilirubin ≥ 3 times ULN, permanently discontinue both BAVENCIO and axitinib and consider corticosteroid therapy [initial dose 1 to 2 mg/kg/day prednisone or equivalent followed by a taper].
When BAVENCIO is administered in combination with axitinib, review the axitinib Full Prescribing Information for recommended dose modifications for axitinib.
2.6 Preparation and Administration
Preparation
- Visually inspect vial for particulate matter and discoloration. BAVENCIO is a clear, colorless to slightly yellow solution. Discard vial if the solution is cloudy, discolored, or contains particulate matter.
- Withdraw the required volume of BAVENCIO from the vial(s) and inject it into a 250 mL infusion bag containing either 0.9% Sodium Chloride Injection or 0.45% Sodium Chloride Injection.
- Gently invert the bag to mix the diluted solution and avoid foaming or excessive shearing.
- Inspect the solution to ensure it is clear, colorless, and free of visible particles.
- Discard any partially used or empty vials.
Storage of diluted BAVENCIO solution
Protect from light.
Store diluted BAVENCIO solution:
- At room temperature up to 77°F (25°C) for no more than 4 hours from the time of dilution.
Or
- Under refrigeration at 36°F to 46°F (2°C to 8°C) for no more than 24 hours from the time of dilution. If refrigerated, allow the diluted solution to come to room temperature prior to administration.
Do not freeze or shake diluted solution.
- 3 DOSAGE FORMS AND STRENGTHS
- 4 CONTRAINDICATIONS
-
5 WARNINGS AND PRECAUTIONS
5.1 Immune-Mediated Pneumonitis
BAVENCIO can cause immune-mediated pneumonitis, including fatal cases [see Adverse Reactions (6.1)]. Monitor patients for signs and symptoms of pneumonitis and evaluate patients with suspected pneumonitis with radiographic imaging. Administer corticosteroids (initial dose of 1 to 2 mg/kg/day prednisone or equivalent, followed by a corticosteroid taper) for Grade 2 or greater pneumonitis. Withhold BAVENCIO for moderate (Grade 2) pneumonitis, and permanently discontinue for severe (Grade 3), life-threatening (Grade 4), or recurrent moderate (Grade 2) pneumonitis [see Dosage and Administration (2.5)].
Pneumonitis occurred in 1.2% of patients receiving BAVENCIO including one (0.1%) patient with Grade 5, one (0.1%) with Grade 4, and five (0.3%) with Grade 3 pneumonitis. Immune-mediated pneumonitis led to permanent discontinuation of BAVENCIO in 0.3% of patients. Among the 21 patients with immune-mediated pneumonitis, the median time to onset was 2.5 months (range: 3 days to 11 months) and the median duration of pneumonitis was 7 weeks (range: 4 days to 4+ months). All 21 patients were treated with systemic corticosteroids; 17 (81%) of the 21 patients received high-dose corticosteroids for a median of 8 days (range: 1 day to 2.3 months). Resolution of pneumonitis occurred in 12 (57%) of the 21 patients at the time of data cut-off.
5.2 Hepatotoxicity and Immune-Mediated Hepatitis
BAVENCIO can cause immune-mediated hepatitis including fatal cases [see Adverse Reactions (6.1)]. Monitor patients for abnormal liver tests prior to and periodically during treatment. Administer corticosteroids (initial dose of 1 to 2 mg/kg/day prednisone or equivalent, followed by a corticosteroid taper) for Grade 2 or greater hepatitis. Withhold BAVENCIO for moderate (Grade 2) immune-mediated hepatitis until resolution and permanently discontinue for severe (Grade 3) or life-threatening (Grade 4) immune-mediated hepatitis [see Dosage and Administration (2.5)].
BAVENCIO as a Single Agent
Immune-mediated hepatitis occurred in 0.9% of patients receiving BAVENCIO including two (0.1%) patients with Grade 5 and 11 (0.6 %) patients with Grade 3 immune-mediated hepatitis. Immune-mediated hepatitis led to permanent discontinuation of BAVENCIO in 0.5% of patients. Among the 16 patients with immune-mediated hepatitis, the median time to onset was 3.2 months (range: 1 week to 15 months), and the median duration of hepatitis was 2.5 months (range: 1 day to 7.4+ months). All 16 patients were treated with corticosteroids; 15 (94%) of the 16 patients received high-dose corticosteroids for a median of 14 days (range: 1 day to 2.5 months). Resolution of hepatitis occurred in nine (56%) of the 16 patients at the time of data cut-off.
BAVENCIO with Axitinib
BAVENCIO in combination with axitinib can cause hepatotoxicity with higher than expected frequencies of Grade 3 and 4 ALT and AST elevation. Consider more frequent monitoring of liver enzymes as compared to when the drugs are used as monotherapy. Withhold BAVENCIO and axitinib for moderate (Grade 2) hepatotoxicity and permanently discontinue the combination for severe or life-threatening (Grade 3 or 4) hepatotoxicity. Administer corticosteroids as needed [see Dosage and Administration (2.5)].
In patients treated with BAVENCIO in combination with axitinib in the advanced RCC trials, Grades 3 and 4 increased ALT and increased AST were reported in 9% and 7% of patients, respectively. In patients with ALT ≥ 3 times ULN (Grades 2-4, n=82), ALT resolved to Grades 0-1 in 92%. Among the 73 patients who were rechallenged with either BAVENCIO (59%) or axitinib (85%) monotherapy or with both (55%), 66% had no recurrence of ALT ≥ 3 times ULN. Immune-mediated hepatitis was reported in 7% of patients including 4.9% with Grade 3 or 4 immune-mediated hepatitis. Hepatotoxicity led to permanent discontinuation in 6.5% and immune-mediated hepatitis led to permanent discontinuation of either BAVENCIO or axitinib in 5.3% of patients. Among the 35 patients with immune-mediated hepatitis, the median time to onset was 2.8 months (range: 2.1 weeks to 14.5 months) and the median duration of hepatitis was 15 days (range: 2 days to 9 months). Thirty-four patients were treated with corticosteroids and one patient was treated with a non-steroidal immunosuppressant; 33 patients received high-dose corticosteroids for a median of 21 days (range: 4 days to 3 months). Resolution of hepatitis occurred in 31 of the 35 patients at the time of data cut-off.
5.3 Immune-Mediated Colitis
BAVENCIO can cause immune-mediated colitis [see Adverse Reactions (6.1)]. Monitor patients for signs and symptoms of colitis. Administer corticosteroids (initial dose of 1 to 2 mg/kg/day prednisone or equivalent followed by a corticosteroid taper) for Grade 2 or greater colitis. Withhold BAVENCIO for moderate or severe (Grade 2 or 3) colitis until resolution. Permanently discontinue BAVENCIO for life-threatening (Grade 4) or for recurrent (Grade 3) colitis upon re-initiation of BAVENCIO [see Dosage and Administration (2.5)].
Immune-mediated colitis occurred in 1.5% of patients receiving BAVENCIO including seven (0.4%) patients with Grade 3 colitis. Immune-mediated colitis led to permanent discontinuation of BAVENCIO in 0.5% of patients. Among the 26 patients with immune-mediated colitis, the median time to onset was 2.1 months (range: 2 days to 11 months) and the median duration of colitis was 6 weeks (range: 1 day to 14+ months). All 26 patients were treated with corticosteroids; 15 (58%) of the 26 patients received high-dose corticosteroids for a median of 19 days (range: 1 day to 2.3 months). Resolution of colitis occurred in 18 (70%) of the patients at the time of data cut-off.
5.4 Immune-Mediated Endocrinopathies
BAVENCIO can cause immune-mediated endocrinopathies [see Adverse Reactions (6.1)].
Adrenal Insufficiency
Monitor patients for signs and symptoms of adrenal insufficiency during and after treatment. Administer corticosteroids as appropriate for adrenal insufficiency. Withhold BAVENCIO for severe (Grade 3) or life-threatening (Grade 4) adrenal insufficiency [see Dosage and Administration (2.5)].
Adrenal insufficiency occurred in 0.5% of patients receiving BAVENCIO including one patient (0.1%) with Grade 3 adrenal insufficiency. Immune-mediated adrenal insufficiency led to permanent discontinuation of BAVENCIO in 0.1% of patients. Among the 8 patients with immune-mediated adrenal insufficiency, the median time to onset was 2.5 months (range: 1 day to 8 months). All eight patients were treated with corticosteroids; four (50%) of the eight patients received high-dose corticosteroids for a median of 1 day (range: 1 day to 24 days).
Thyroid Disorders (Hypothyroidism/Hyperthyroidism)
BAVENCIO can cause immune-mediated thyroid disorders. Thyroid disorders can occur at any time during treatment. Monitor patients for changes in thyroid function at the start of treatment, periodically during treatment, and as indicated based on clinical evaluation. Manage hypothyroidism with hormone-replacement therapy. Initiate medical management for control of hyperthyroidism. Withhold BAVENCIO for severe (Grade 3) or life-threatening (Grade 4) thyroid disorders [see Dosage and Administration (2.5)].
Immune-mediated thyroid disorders occurred in 6% of patients receiving BAVENCIO including 3 (0.2%) Grade 3 immune-mediated thyroid disorders. Immune-mediated thyroid disorders led to discontinuation of BAVENCIO in 0.1% of patients. Hypothyroidism occurred in 90 (5%) patients; hyperthyroidism in seven (0.4%) patients; and thyroiditis in four (0.2%) patients treated with BAVENCIO. Among the 98 patients with immune-mediated thyroid disorders, the median time to onset was 2.8 months (range: 2 weeks to 13 months) and the median duration was not estimable (range: 6 days to more than 26 months). Immune-mediated thyroid disorders resolved in seven (7%) of the 98 patients.
Type 1 Diabetes Mellitus
BAVENCIO can cause type 1 diabetes mellitus, including diabetic ketoacidosis. Monitor patients for hyperglycemia or other signs and symptoms of diabetes. Withhold BAVENCIO and administer anti-hyperglycemics or insulin in patients with severe or life-threatening (Grade ≥ 3) hyperglycemia. Resume treatment with BAVENCIO when metabolic control is achieved on insulin replacement or anti-hyperglycemics [see Dosage and Administration (2.5)].
Type 1 diabetes mellitus without an alternative etiology occurred in 0.1% of patients including two cases of Grade 3 hyperglycemia that led to permanent discontinuation of BAVENCIO.
5.5 Immune-Mediated Nephritis and Renal Dysfunction
BAVENCIO can cause immune-mediated nephritis [see Adverse Reactions (6.1)]. Monitor patients for elevated serum creatinine prior to and periodically during treatment. Administer corticosteroids (initial dose of 1 to 2 mg/kg/day prednisone or equivalent followed by a corticosteroid taper) for Grade 2 or greater nephritis. Withhold BAVENCIO for moderate (Grade 2) or severe (Grade 3) nephritis until resolution to ≤ Grade 1. Permanently discontinue BAVENCIO for life-threatening (Grade 4) nephritis [see Dosage and Administration (2.5)].
Immune-mediated nephritis occurred in 0.1% of patients receiving BAVENCIO; BAVENCIO was permanently discontinued in this patient.
5.6 Other Immune-Mediated Adverse Reactions
BAVENCIO can result in severe and fatal immune-mediated adverse reactions [see Adverse Reactions (6.1)]. These immune-mediated reactions may involve any organ system. Most immune-mediated reactions initially manifest during treatment with BAVENCIO; however, immune-mediated adverse reactions can occur after discontinuation of BAVENCIO.
For suspected immune-mediated adverse reactions, evaluate to confirm or rule out an immune-mediated adverse reaction and to exclude other causes. Depending upon the severity of the adverse reaction, withhold or permanently discontinue BAVENCIO, administer high dose corticosteroids, and if appropriate, initiate hormone replacement therapy. Upon improvement to Grade 1 or less, initiate corticosteroid taper. Resume BAVENCIO when the immune-mediated adverse reaction remains at Grade 1 or less following corticosteroid taper. Permanently discontinue BAVENCIO for any severe (Grade 3) immune-mediated adverse reaction that recurs and for any life-threatening immune-mediated adverse reaction [see Dosage and Administration (2.5)].
The following clinically significant, immune-mediated adverse reactions occurred at an incidence of less than 1% of patients who received BAVENCIO as a single agent or in 489 patients who received BAVENCIO in combination with axitinib: immune-mediated myocarditis including fatal cases, pancreatitis including fatal cases, immune-mediated myositis, psoriasis, arthritis, exfoliative dermatitis, erythema multiforme, pemphigoid, hypopituitarism, uveitis, Guillain-Barré syndrome, and systemic inflammatory response. The following clinically significant, immune-mediated adverse reactions have been reported with other products in this class: bullous dermatitis, Stevens Johnson Syndrome (SJS)/toxic epidermal necrolysis (TEN), rhabdomyolysis, myasthenia gravis, histiocytic necrotizing lymphadenitis, demyelination, vasculitis, hemolytic anemia, hypophysitis, iritis, and encephalitis.
5.7 Infusion-Related Reactions
BAVENCIO can cause severe or life-threatening infusion-related reactions [see Adverse Reactions (6.1)]. Premedicate with antihistamine and acetaminophen prior to the first 4 infusions. Monitor patients for signs and symptoms of infusion-related reactions including pyrexia, chills, flushing, hypotension, dyspnea, wheezing, back pain, abdominal pain, and urticaria. Interrupt or slow the rate of infusion for mild or moderate infusion-related reactions. Stop the infusion and permanently discontinue BAVENCIO for severe (Grade 3) or life-threatening (Grade 4) infusion-related reactions [see Dosage and Administration (2.5) and Adverse Reactions (6.1)].
Infusion-related reactions occurred in 25% of patients treated with BAVENCIO including three (0.2%) Grade 4 and nine (0.5%) Grade 3 infusion-related reactions. Ninety-three percent of patients received premedication with antihistamine and acetaminophen. Eleven (92%) of the 12 patients with Grade ≥ 3 reactions were treated with intravenous corticosteroids. Fourteen percent of patients had infusion-related reactions that occurred after the BAVENCIO infusion was completed.
5.8 Major Adverse Cardiovascular Events (MACE)
BAVENCIO in combination with axitinib can cause severe and fatal cardiovascular events. Consider baseline and periodic evaluations of left ventricular ejection fraction. Monitor for signs and symptoms of cardiovascular events. Optimize management of cardiovascular risk factors, such as hypertension, diabetes, or dyslipidemia. Discontinue BAVENCIO and axitinib for Grade 3-4 cardiovascular events.
MACE occurred in 7% of patients with advanced RCC treated with BAVENCIO in combination with axitinib compared to 3.4% treated with sunitinib in a randomized trial, JAVELIN Renal 101. These events included death due to cardiac events (1.4%), Grade 3-4 myocardial infarction (2.8%), and Grade 3-4 congestive heart failure (1.8%). Median time to onset of MACE was 4.2 months (range: 2 days to 24.5 months).
5.9 Embryo-Fetal Toxicity
Based on its mechanism of action, BAVENCIO can cause fetal harm when administered to a pregnant woman. Animal studies have demonstrated that inhibition of the PD-1/PD-L1 pathway can lead to increased risk of immune-mediated rejection of the developing fetus resulting in fetal death. If this drug is used during pregnancy, or if the patient becomes pregnant while taking BAVENCIO, inform the patient of the potential risk to a fetus. Advise females of childbearing potential to use effective contraception during treatment with BAVENCIO and for at least one month after the last dose of BAVENCIO [see Use in Specific Populations (8.1, 8.3)].
-
6 ADVERSE REACTIONS
The following adverse reactions are described elsewhere in the label:
- Immune-mediated pneumonitis [see Warnings and Precautions (5.1)]
- Hepatotoxicity and immune-mediated hepatitis [see Warnings and Precautions (5.2)]
- Immune-mediated colitis [see Warnings and Precautions (5.3)]
- Immune-mediated endocrinopathies [see Warnings and Precautions (5.4)]
- Immune-mediated nephritis and renal dysfunction [see Warnings and Precautions (5.5)]
- Other immune-mediated adverse reactions [see Warnings and Precautions (5.6)]
- Infusion-related reactions [see Warnings and Precautions (5.7)]
- Major adverse cardiovascular events [see Warnings and Precautions (5.8)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The data described in the WARNINGS AND PRECAUTIONS section reflect exposure to BAVENCIO 10 mg/kg intravenously every 2 weeks as a single agent in 1738 patients enrolled in the JAVELIN Merkel 200 and JAVELIN Solid Tumor trials and to BAVENCIO 10 mg/kg intravenously every 2 weeks in combination with axitinib 5 mg orally twice daily in 489 patients enrolled in the JAVELIN Renal 100 and JAVELIN Renal 101 trials. In the BAVENCIO monotherapy population, 24% of patients were exposed for ≥ 6 months and 7% were exposed for ≥ 12 months. The population characteristics of BAVENCIO in combination with axitinib are shown below. When BAVENCIO was used in combination with axitinib, 70% of patients were exposed for ≥ 6 months and 31% were exposed for ≥ 12 months. The following criteria were used to classify an adverse reaction as immune-mediated: onset within 90 days after last dose of BAVENCIO, no spontaneous resolution within 7 days of onset, treatment with corticosteroids or other immunosuppressant or hormone replacement therapy, biopsy consistent with immune-mediated reaction, and no other clear etiology.
Metastatic Merkel Cell Carcinoma
The data described below reflect exposure to BAVENCIO 10 mg/kg intravenously every 2 weeks in 88 patients with metastatic MCC enrolled in the JAVELIN Merkel 200 trial. Patients with any of the following were excluded: autoimmune disease; medical conditions requiring systemic immunosuppression; prior organ or allogeneic stem cell transplantation; prior treatment with anti-PD-1, anti-PD-L1, or anti-CTLA-4 antibodies; central nervous system (CNS) metastases; infection with HIV, hepatitis B, or hepatitis C; or ECOG performance score ≥ 2.
The median duration of exposure to BAVENCIO was 4 months (range: 2 weeks to 21 months). Forty percent of patients received BAVENCIO for more than 6 months and 14% were treated for more than one year [see Clinical Studies (14.1)]. The study population characteristics were: median age of 73 years (range: 33 to 88), 74% male, 92% White, ECOG performance score of 0 (56%) or 1 (44%), and 65% of patients had one prior anti-cancer therapy for metastatic MCC and 35% had two or more prior therapies.
BAVENCIO was permanently discontinued for adverse reactions in six (7%) patients; adverse reactions resulting in permanent discontinuation were ileus, Grade 3 transaminitis, Grade 3 creatine kinase elevation, tubulointerstitial nephritis, and Grade 3 pericardial effusion. BAVENCIO was temporarily discontinued in 21 (24%) patients for adverse events, excluding temporary dose interruption for infusion-related reactions where infusion was restarted the same day. The most common adverse reaction requiring dose interruption was anemia. Serious adverse reactions that occurred in more than one patient were acute kidney injury, anemia, abdominal pain, ileus, asthenia, and cellulitis. The most common adverse reactions (≥ 20%) were fatigue, musculoskeletal pain, diarrhea, nausea, infusion-related reaction, rash, decreased appetite, and peripheral edema.
Table 2 and Table 3 summarize the incidence of adverse reactions and laboratory abnormalities, respectively, that occurred in patients receiving BAVENCIO.
Table 2: Adverse Reactions in ≥ 10% of Patients Receiving BAVENCIO in the JAVELIN Merkel 200 Trial Adverse Reactions BAVENCIO
(N=88)All Grades
%Grade 3-4
%- * Fatigue is a composite term that includes fatigue and asthenia
- † Infusion-related reaction is a composite term that includes drug hypersensitivity, hypersensitivity, chills, pyrexia, back pain, and hypotension
- ‡ Peripheral edema is a composite term that includes peripheral edema and peripheral swelling
- § Musculoskeletal pain is a composite term that includes back pain, myalgia, neck pain, pain in extremity
- ¶ Abdominal pain is a composite term that includes abdominal pain and abdominal pain upper
- # Rash is a composite term that includes rash maculo-papular, erythema, and dermatitis bullous
- Þ Pruritus is a composite term that includes pruritus and pruritus generalized
- ß Dyspnea is a composite term that includes dyspnea and dyspnea exertional
General Disorders Fatigue* 50 2 Infusion-related reaction† 22 0 Peripheral edema‡ 20 0 Musculoskeletal and Connective Tissue Disorders Musculoskeletal pain§ 32 2 Arthralgia 16 1 Gastrointestinal Disorders Diarrhea 23 0 Nausea 22 0 Constipation 17 1 Abdominal pain¶ 16 2 Vomiting 13 0 Skin and Subcutaneous Tissue Disorders Rash# 22 0 PruritusÞ 10 0 Metabolism and Nutrition Disorders Decreased appetite 20 2 Decreased weight 15 0 Respiratory, Thoracic and Mediastinal Disorders Cough 18 0 Dyspneaß 11 1 Nervous System Disorders Dizziness 14 0 Headache 10 0 Vascular Disorders Hypertension 13 6 Table 3: Selected Treatment-Emergent* Laboratory Abnormalities in Patients Receiving BAVENCIO in the JAVELIN Merkel 200 Trial Laboratory Tests Any Grade
(N=88)
%Grade 3-4
(N=88)
%- * Treatment emergent consists of new onset of laboratory abnormality or worsening of baseline laboratory abnormality
- † Hyperglycemia limited to Grade ≥ 3 events since fasting measurements were not obtained routinely
Chemistry Increased aspartate aminotransferase (AST) 34 1 Increased alanine aminotransferase (ALT) 20 5 Increased lipase 14 4 Increased amylase 8 1 Increased bilirubin 6 1 Hyperglycemia† - 7 Hematology Anemia 35 9 Lymphopenia 49 19 Thrombocytopenia 27 1 Neutropenia 6 1 Locally Advanced or Metastatic Urothelial Carcinoma
Table 4 describes adverse reactions reported in 242 patients with locally advanced or metastatic UC receiving BAVENCIO at 10 mg/kg every 2 weeks in the UC cohorts of the JAVELIN Solid Tumor trial. Patients received pre-medication with an anti-histamine and acetaminophen prior to each infusion. The median duration of exposure to BAVENCIO was 12 weeks (range: 2 weeks to 92 weeks) [see Clinical Studies (14.2)].
Fourteen patients (6%) who were treated with BAVENCIO experienced either pneumonitis, respiratory failure, sepsis/urosepsis, cerebrovascular accident, or gastrointestinal adverse events, which led to death.
BAVENCIO was permanently discontinued for Grade 1-4 adverse reactions in 30 (12%) patients. The adverse reaction that resulted in permanent discontinuation in > 1% of patients was fatigue. BAVENCIO was temporarily discontinued in 29% of patients for adverse reactions, excluding temporary dose interruption for infusion-related reactions where infusion was restarted the same day. The adverse reactions that resulted in temporary discontinuation in > 1% of patients were diarrhea, fatigue, dyspnea, urinary tract infection, and rash.
Grade 1-4 serious adverse reactions were reported in 41% of patients. The most frequent serious adverse reactions reported in ≥ 2% of patients were urinary tract infection/urosepsis, abdominal pain, musculoskeletal pain, creatinine increased/renal failure, dehydration, hematuria/urinary tract hemorrhage, intestinal obstruction/small intestine obstruction, and pyrexia.
The most common Grade 3 and 4 adverse reactions (≥ 3%) were anemia, fatigue, hyponatremia, hypertension urinary tract infection, and musculoskeletal pain.
The most common adverse reactions (≥ 20%) were fatigue, infusion-related reaction, musculoskeletal pain, nausea, decreased appetite, and urinary tract infection.
Eleven (4.5%) patients received an oral prednisone dose equivalent to ≥ 40 mg daily for an immune-mediated adverse reaction [see Warnings and Precautions (5)].
Table 4 summarizes the adverse reactions that occurred in at least 10% of patients with locally advanced or metastatic UC receiving BAVENCIO while Table 5 summarizes selected Grade 3-4 laboratory abnormalities that occurred in ≥ 1% of patients treated with BAVENCIO.
Table 4: All Grade Adverse Reactions in ≥ 10% of Patients with Locally Advanced or Metastatic UC in the JAVELIN Solid Tumor Trial Adverse Reactions BAVENCIO
(N=242)All Grades
(%)Grade 3-4
(%)- * Includes abdominal discomfort, abdominal pain upper and lower, and gastrointestinal pain
- † Includes asthenia and malaise
- ‡ Infusion-related reaction is a composite term that includes chills, pyrexia, back pain, flushing, dyspnea, and hypotension
- § Includes edema, generalized edema, and peripheral swelling
- ¶ Includes urosepsis, cystitis, kidney infection, pyuria, and urinary tract infection due to fungus, bacterial, and enterococcus
- # Includes back pain, myalgia, neck pain, and pain in extremity
- Þ Includes acute kidney injury and glomerular filtration rate decreased
- ß Includes dermatitis acneiform, eczema, erythema, erythema multiforme, erythematous, macular, maculo-papular, papular, and pruritic rash
Any 98 59 Gastrointestinal Disorders Nausea 24 1 Abdominal pain* 19 2 Diarrhea 18 2 Constipation 18 1 Vomiting/Retching 14 1 General Disorders and Administration Site Conditions Fatigue† 41 7 Infusion-related reaction‡ 30 0.4 Peripheral edema§ 17 0.4 Pyrexia/Temperature increased 16 1 Infections Urinary tract infection¶ 21 5 Investigations Weight decreased 19 0 Metabolism and Nutrition Disorders Decreased appetite/Hypophagia 21 2 Musculoskeletal and Connective Tissue Disorders Musculoskeletal pain# 25 3 Renal Disorders Creatinine increased/Renal failureÞ 16 3 Respiratory, Thoracic and Mediastinal Disorders Dyspnea/Exertional dyspnea 17 2 Cough/Productive cough 14 0 Skin and Subcutaneous Tissue Disorders Rashß 15 0.4 Pruritus/Generalized pruritus 10 0.4 Vascular Disorders Hypertension/Hypertensive crisis 10 5 Table 5: Selected Laboratory Abnormalities* (Grade 3-4) in ≥ 1% of Patients with Locally Advanced or Metastatic UC Receiving BAVENCIO in the JAVELIN Solid Tumor Trial Laboratory Tests Grade 3-4
(N=242)†
%- * Including Grade 3 and 4 lab abnormalities worsening from and unchanged since baseline.
- † The number of patients with on study available laboratories varies between 188 and 235.
- ‡ Increased alanine aminotransferase (ALT) was reported in 0.9% (Grade 3-4) of platinum-pretreated patients with locally advanced or metastatic UC.
Chemistry Hyponatremia 16 GGT increased 12 Hyperglycemia 9 Increased alkaline phosphatase 7 Increased lipase 6 Hyperkalemia 3 Increased aspartate aminotransferase (AST)‡ 3 Increased creatinine 2 Increased amylase 2 Increased bilirubin 1 Hematology Lymphopenia 11 Anemia 6 Advanced Renal Cell Carcinoma
The safety of BAVENCIO was evaluated in JAVELIN Renal 101. Patients with autoimmune disease other than type I diabetes mellitus, vitiligo, psoriasis, or thyroid disorders not requiring immunosuppressive treatment were excluded. Patients received BAVENCIO 10 mg/kg every 2 weeks administered in combination with axitinib 5 mg twice daily (N=434) or sunitinib 50 mg once daily for 4 weeks followed by 2 weeks off (N=439).
In the BAVENCIO plus axitinib arm, 70% were exposed to BAVENCIO for ≥ 6 months and 29% were exposed for ≥ 1 year in JAVELIN Renal 101 [see Clinical Studies (14.3)].
The median age of patients treated with BAVENCIO in combination with axitinib was 62 years (range: 29 to 83), 38% of patients were 65 years or older, 71% were male, 75% were White, and the ECOG performance score was 0 (64%) or 1 (36%).
Fatal adverse reactions occurred in 1.8% of patients receiving BAVENCIO in combination with axitinib. These included sudden cardiac death (1.2%), stroke (0.2%), myocarditis (0.2%), and necrotizing pancreatitis (0.2%).
Serious adverse reactions occurred in 35% of patients receiving BAVENCIO in combination with axitinib. Serious adverse reactions in ≥ 1% of patients included diarrhea (2.5%), dyspnea (1.8%), hepatotoxicity (1.8%), venous thromboembolic disease (1.6%), acute kidney injury (1.4%), and pneumonia (1.2%).
Permanent discontinuation due to an adverse reaction of either BAVENCIO or axitinib occurred in 22% of patients: 19% BAVENCIO only, 13% axitinib only, and 8% both drugs. The most common adverse reactions (> 1%) resulting in permanent discontinuation of BAVENCIO or the combination were hepatotoxicity (6%) and infusion-related reaction (1.8%).
Dose interruptions or reductions due to an adverse reaction, excluding temporary interruptions of BAVENCIO infusions due to infusion-related reactions, occurred in 76% of patients receiving BAVENCIO in combination with axitinib. This includes interruption of BAVENCIO in 50% of patients. Axitinib was interrupted in 66% and dose reduced in 19% of patients. The most common adverse reaction (> 10%) resulting in interruption of BAVENCIO was diarrhea (10%) and the most common adverse reactions resulting in either interruption or dose reduction of axitinib were diarrhea (19%), hypertension (18%), palmar-plantar erythrodysesthesia (18%), and hepatotoxicity (10%).
The most common adverse reactions (≥ 20%) in patients receiving BAVENCIO in combination with axitinib were diarrhea, fatigue, hypertension, musculoskeletal pain, nausea, mucositis, palmar-plantar erythrodysesthesia, dysphonia, decreased appetite, hypothyroidism, rash, hepatotoxicity, cough, dyspnea, abdominal pain, and headache.
Forty-eight (11%) of patients treated with BAVENCIO in combination with axitinib received an oral prednisone dose equivalent to ≥ 40 mg daily for an immune-mediated adverse reaction [see Warnings and Precautions (5)].
Table 6 summarizes adverse reactions that occurred in ≥ 20% of BAVENCIO in combination with axitinib-treated patients.
Table 6: Adverse Reactions (≥ 20%) of Patients Receiving BAVENCIO in Combination with Axitinib (JAVELIN Renal 101 Trial)* Adverse Reactions BAVENCIO plus Axitinib
(N=434)Sunitinib
(N=439)All Grades
%Grade 3-4
%All Grades
%Grade 3-4
%Toxicity was graded per National Cancer Institute Common Terminology Criteria for Adverse Events. Version 4.03 (NCI CTCAE v4). - * The trial was not designed to demonstrate a statistically significant difference in the incidence of adverse reactions between BAVENCIO in combination with axitinib and sunitinib.
- † Diarrhea is a composite term that includes diarrhea, autoimmune colitis, and colitis
- ‡ Mucositis is a composite term that includes mucosal inflammation and stomatitis
- § Hepatotoxicity is a composite term that includes ALT increased, AST increased, autoimmune hepatitis, bilirubin conjugated, bilirubin conjugated increased, blood bilirubin increased, drug-induced liver injury, hepatic enzyme increased, hepatic function abnormal, hepatitis, hepatitis fulminant, hepatocellular injury, hepatotoxicity, hyperbilirubinemia, immune-mediated hepatitis, liver function test increased, liver disorder, liver injury, and transaminases increased
- ¶ Abdominal pain is a composite term that includes abdominal pain, flank pain, abdominal pain upper, and abdominal pain lower
- # Fatigue is a composite term that includes fatigue and asthenia
- Þ Hypertension is a composite term that includes hypertension and hypertensive crisis
- ß Musculoskeletal pain is a composite term that includes musculoskeletal pain, musculoskeletal chest pain, myalgia, back pain, bone pain, musculoskeletal discomfort, neck pain, spinal pain, and pain in extremity
- à Rash is a composite term that includes rash, rash generalized, rash macular, rash maculo-papular, rash pruritic, rash erythematous, rash papular, and rash pustular
- è Dyspnea is a composite term that includes dyspnea, dyspnea exertional and dyspnea at rest
Gastrointestinal Disorders Diarrhea† 62 8 48 2.7 Nausea 34 1.4 39 1.6 Mucositis‡ 34 2.8 35 2.1 Hepatotoxicity§ 24 9 18 3.6 Abdominal pain¶ 22 1.4 19 2.1 General Disorders and Administration Site Conditions Fatigue# 53 6 54 6 Vascular Disorders HypertensionÞ 50 26 36 17 Musculoskeletal and Connective Tissue Disorders Musculoskeletal painß 40 3.2 33 2.7 Skin and Subcutaneous Tissue Disorders Palmar-plantar erythrodysesthesia 33 6 34 4 Rashà 25 0.9 16 0.5 Respiratory, Thoracic and Mediastinal Disorders Dysphonia 31 0.5 3.2 0 Dyspneaè 23 3.0 16 1.8 Cough 23 0.2 19 0 Metabolism and Nutrition Disorders Decreased appetite 26 2.1 29 0.9 Endocrine Disorders Hypothyroidism 25 0.2 14 0.2 Nervous System Disorders Headache 21 0.2 16 0.2 Other clinically important adverse reactions that occurred in less than 20% of patients in JAVELIN Renal 101 included arthralgia, weight decreased, and chills.
Patients received pre-medication with an anti-histamine and acetaminophen prior to each infusion. Infusion-related reactions occurred in 12% (Grade 3: 1.6%; no Grade 4) of patients treated with BAVENCIO in combination with axitinib.
Table 7 summarizes selected laboratory abnormalities that occurred in ≥ 20% of BAVENCIO in combination with axitinib-treated patients.
Table 7: Selected Laboratory Abnormalities Worsening from Baseline Occurring in ≥ 20% of Patients Receiving BAVENCIO in Combination with Axitinib (JAVELIN Renal 101 Trial)* Laboratory Abnormality BAVENCIO plus Axitinib† Sunitinib† Any Grade
%Grade 3-4
%Any Grade
%Grade 3-4
%- * The trial was not designed to demonstrate a statistically significant difference in the incidence of laboratory abnormalities between BAVENCIO in combination with axitinib and sunitinib.
- † Each test incidence is based on the number of patients who had both baseline and at least one on-study laboratory measurement available: BAVENCIO in combination with axitinib group (range: 413 to 428 patients) and sunitinib group (range: 405 to 433 patients).
Chemistry Blood triglycerides increased 71 13 48 5 Blood creatinine increased 62 2.3 68 1.4 Blood cholesterol increased 57 1.9 22 0.7 Alanine aminotransferase increased (ALT) 50 9 46 3.2 Aspartate aminotransferase increased (AST) 47 7 57 3.2 Blood sodium decreased 38 9 37 10 Lipase increased 37 14 25 7 Blood potassium increased 35 3.0 28 3.9 Blood bilirubin increased 21 1.4 23 1.4 Hematology Platelet count decreased 27 0.7 80 15 Hemoglobin decreased 21 2.1 65 8 6.2 Immunogenicity
As with all therapeutic proteins, there is potential for immunogenicity. The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assay may be influenced by several factors including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of antibodies to avelumab in the studies described below with the incidence of antibodies in other studies or to other products may be misleading.
Of the 1738 patients treated with BAVENCIO 10 mg/kg as an intravenous infusion every 2 weeks, 1558 were evaluable for treatment-emergent anti-drug antibodies (ADA) and 64 (4.1%) tested positive. The development of treatment-emergent ADA against avelumab did not appear to alter the pharmacokinetic profile or risk of infusion-related reactions.
Of the 480 patients treated with BAVENCIO 10 mg/kg as an intravenous infusion every 2 weeks in combination with axitinib 5 mg twice daily, 453 were evaluable for treatment-emergent anti-drug antibodies (ADA) and 66 (15%) tested positive. A new ADA method with improved sensitivity was used in the RCC population. Patients who tested positive for treatment-emergent ADA had decreased systemic BAVENCIO exposure [see Clinical Pharmacology (12.3)]. The development of treatment-emergent ADA against avelumab did not appear to alter the risk of infusion-related reactions.
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
Based on its mechanism of action, BAVENCIO can cause fetal harm when administered to a pregnant woman. There are no available data on the use of BAVENCIO in pregnant women [see Clinical Pharmacology (12.1)]. Animal studies have demonstrated that inhibition of the PD-1/PD-L1 pathway can lead to increased risk of immune-mediated rejection of the developing fetus resulting in fetal death [see Data]. Human IgG1 immunoglobulins (IgG1) are known to cross the placenta. Therefore, BAVENCIO has the potential to be transmitted from the mother to the developing fetus. If this drug is used during pregnancy, or if the patient becomes pregnant while taking this drug, advise the patient of the potential risk to a fetus.
In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Data
Animal Data
Animal reproduction studies have not been conducted with BAVENCIO to evaluate its effect on reproduction and fetal development. A central function of the PD-1/PD-L1 pathway is to preserve pregnancy by maintaining maternal immune tolerance to the fetus. In murine models of pregnancy, blockade of PD-L1 signaling has been shown to disrupt tolerance to the fetus and to result in an increase in fetal loss; therefore, potential risks of administering BAVENCIO during pregnancy include increased rates of abortion or stillbirth. As reported in the literature, there were no malformations related to the blockade of PD-1/PD-L1 signaling in the offspring of these animals; however, immune-mediated disorders occurred in PD-1 and PD-L1 knockout mice. Based on its mechanism of action, fetal exposure to BAVENCIO may increase the risk of developing immune-related disorders or altering the normal immune response.
8.2 Lactation
Risk Summary
There is no information regarding the presence of avelumab in human milk, the effects on the breastfed infant, or the effects on milk production. Since many drugs including antibodies are excreted in human milk, advise a lactating woman not to breastfeed during treatment and for at least one month after the last dose of BAVENCIO due to the potential for serious adverse reactions in breastfed infants.
8.3 Females and Males of Reproductive Potential
Contraception
Based on its mechanism of action, BAVENCIO can cause fetal harm when administered to a pregnant woman [see Use in Specific Populations (8.1)]. Advise females of reproductive potential to use effective contraception during treatment with BAVENCIO and for at least 1 month after the last dose of BAVENCIO.
8.4 Pediatric Use
The safety and effectiveness of BAVENCIO have been established in pediatric patients aged 12 years and older for metastatic MCC. Use of BAVENCIO in this age group is supported by evidence from adequate and well-controlled studies of BAVENCIO in adults with additional population pharmacokinetic data demonstrating that age and body weight had no clinically meaningful effect on the steady state exposure of avelumab, that drug exposure is generally similar between adults and pediatric patients age 12 years and older for monoclonal antibodies, and that the course of MCC is sufficiently similar in adult and pediatric patients to allow extrapolation of data in adults to pediatric patients. The recommended dose in pediatric patients 12 years of age or greater is the same as that in adults [see Dosage and Administration (2.2), Clinical Pharmacology (12.3), and Clinical Studies (14)].
Safety and effectiveness of BAVENCIO have not been established in pediatric patients less than 12 years of age.
8.5 Geriatric Use
Metastatic Merkel Cell Carcinoma
Clinical studies of BAVENCIO in MCC did not include sufficient numbers of patients aged 65 and over to determine whether they respond differently from younger patients.
Locally Advanced or Metastatic Urothelial Carcinoma
Of the 226 patients with locally advanced or metastatic UC treated with BAVENCIO, 68% were 65 years or over and 29% were 75 years or over. Among patients 65 years or over who were followed for at least 13 weeks, 14% (22/153) responded to BAVENCIO and 58% (89/153) developed a Grade 3-4 adverse reaction. No overall differences in safety or efficacy were reported between elderly patients and younger patients.
Advanced Renal Cell Carcinoma
Of the 434 patients randomized to BAVENCIO 10 mg/kg administered in combination with axitinib 5 mg twice daily in the JAVELIN Renal 101 trial, 38% were 65 years or older and 8% were 75 years or older. No overall difference in safety or efficacy were reported between elderly patients and younger patients.
-
11 DESCRIPTION
Avelumab is a programmed death ligand1 (PD-L1) blocking antibody. Avelumab- is a human IgG1 lambda monoclonal antibody produced in Chinese hamster ovary cells and has a molecular weight of approximately 147 kDa.
BAVENCIO (avelumab) Injection for intravenous use is a sterile, preservative-free, non-pyrogenic, clear, colorless to slightly yellow solution. Each single-dose vial contains 200 mg avelumab in 10 mL (20 mg/mL). Each mL contains 20 mg avelumab, D-mannitol (51 mg), glacial acetic acid (0.6 mg), polysorbate 20 (0.5 mg), sodium hydroxide (0.3 mg), and Water for Injection. The pH range of the solution is 5.0 – 5.6.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
PD-L1 may be expressed on tumor cells and tumor-infiltrating immune cells and can contribute to the inhibition of the anti-tumor immune response in the tumor microenvironment. Binding of PD-L1 to the PD-1 and B7.1 receptors found on T cells and antigen presenting cells suppresses cytotoxic T-cell activity, T-cell proliferation, and cytokine production. Avelumab binds PD-L1 and blocks the interaction between PD-L1 and its receptors PD-1 and B7.1. This interaction releases the inhibitory effects of PD-L1 on the immune response resulting in the restoration of immune responses, including anti-tumor immune responses. Avelumab has also been shown to induce antibody-dependent cell-mediated cytotoxicity (ADCC) in vitro. In syngeneic mouse tumor models, blocking PD-L1 activity resulted in decreased tumor growth.
12.2 Pharmacodynamics
Based on exposure efficacy and exposure safety relationships, there are no expected clinically meaningful differences in the safety or efficacy of BAVENCIO administered every 2 weeks at 800 mg or 10 mg/kg in patients with metastatic Merkel cell carcinoma, in patients with urothelial carcinoma and in patients with advanced renal cell carcinoma.
12.3 Pharmacokinetics
Avelumab pharmacokinetics (PK) was assessed using a population PK approach for both single-agent BAVENCIO and BAVENCIO in combination with axitinib. There are no expected clinically meaningful differences in exposure of avelumab administered every 2 weeks at 800 mg or 10 mg/kg in both settings.
BAVENCIO as a single agent
The pharmacokinetics of avelumab as a single agent was studied in 1629 patients who received doses ranging from 1 to 20 mg/kg every 2 weeks. The data showed that the exposure of avelumab increased dose-proportionally in the dose range of 10 to 20 mg/kg every 2 weeks. Steady-state concentrations of avelumab were reached after approximately 4 to 6 weeks (2 to 3 cycles) of repeated dosing, and the systemic accumulation was approximately 1.25-fold. The geometric mean volume of distribution at steady state for a subject receiving 10 mg/kg was 4.72 L. The primary elimination mechanism of avelumab is proteolytic degradation. Based on population pharmacokinetic analyses in patients with solid tumors, the total systemic clearance was 0.59 L/day and the terminal half-life was 6.1 days in patients receiving 10 mg/kg. In a post hoc analysis, avelumab clearance was found to decrease over time in patients with MCC, with a mean maximal reduction (% coefficient of variation [CV%]) from baseline value of approximately 32.1% (36.2%), which is not considered clinically important. There was no evidence to suggest a change of avelumab clearance over time in patients with UC.
BAVENCIO with axitinib
When BAVENCIO 10 mg/kg was administered in combination with axitinib 5 mg, the respective exposures of avelumab and axitinib were comparable to the single agents. There was no evidence to suggest a clinically relevant change of avelumab clearance over time in patients with advanced RCC.
Specific Populations
Body weight was positively correlated with total systemic clearance in population pharmacokinetic analyses. No clinically meaningful differences in pharmacokinetics were observed in the clearance of avelumab based on age; sex; race; PD-L1 status; tumor burden; mild [calculated creatinine clearance (CLcr) 60 to 89 mL/min, n=623 as estimated by the Cockcroft-Gault formula], moderate [CLcr 30 to 59 mL/min, n=320], or severe [CLcr 15 to 29 mL/min, n=4] renal impairment; and mild [bilirubin less than or equal to ULN and AST greater than ULN or bilirubin between 1 and 1.5 times ULN, n=217] or moderate [bilirubin between 1.5 and 3 times ULN, n=4] hepatic impairment. There are limited data from patients with severe hepatic impairment [bilirubin greater than 3 times ULN, n=1], and the effect of severe hepatic impairment on the pharmacokinetics of avelumab is unknown. In patients with advanced RCC, BAVENCIO clearance in patients who tested positive for treatment-emergent ADA was 15% higher as compared to clearance in patients who tested negative for treatment-emergent ADA.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
No studies have been conducted to assess the potential of avelumab for genotoxicity or carcinogenicity.
Fertility studies have not been conducted with avelumab; however, an assessment of male and female reproductive organs was included in 3-month repeat-dose toxicity study in Cynomolgus monkeys. Weekly administration of avelumab did not result in any notable effects in the male and female reproductive organs.
13.2 Animal Toxicology and/or Pharmacology
In animal models, inhibition of PD-L1/PD-1 signaling increased the severity of some infections and enhanced inflammatory responses. M. tuberculosis-infected PD-1 knockout mice exhibit markedly decreased survival compared with wild-type controls, which correlated with increased bacterial proliferation and inflammatory responses in these animals. PD-L1 and PD-1 knockout mice and mice receiving PD-L1 blocking antibody have also shown decreased survival following infection with lymphocytic choriomeningitis virus.
-
14 CLINICAL STUDIES
14.1 Metastatic Merkel Cell Carcinoma
The efficacy and safety of BAVENCIO was demonstrated in the JAVELIN Merkel 200 trial (NCT02155647), an open-label, single-arm, multi-center study conducted in patients with histologically confirmed metastatic MCC whose disease had progressed on or after chemotherapy administered for distant metastatic disease. The trial excluded patients with autoimmune disease; medical conditions requiring systemic immunosuppression; prior organ or allogeneic stem cell transplantation; prior treatment with anti-PD-1, anti-PD-L1, or anti-CTLA-4 antibodies; CNS metastases; infection with HIV, hepatitis B, or hepatitis C; or ECOG performance score ≥ 2.
Patients received BAVENCIO 10 mg/kg as an intravenous infusion over 60 minutes every 2 weeks until disease progression or unacceptable toxicity. Patients with radiological disease progression not associated with significant clinical deterioration, defined as no new or worsening symptoms, no change in performance status for greater than 2 weeks, and no need for salvage therapy, could continue treatment. Tumor response assessments were performed every 6 weeks. The major efficacy outcome measures were confirmed overall response rate (ORR) according to Response Evaluation Criteria in Solid Tumors (RECIST) v1.1 as assessed by a blinded independent central review committee (IRC) and IRC-assessed duration of response. The efficacy analysis was conducted when the last patient enrolled had completed 12 months of follow-up.
A total of 88 patients were enrolled. Baseline patient characteristics were a median age of 73 years (range: 33 to 88), 74% of patients were male, 92% were White, and the ECOG performance score was 0 (56%) or 1 (44%). Seventy-five percent of patients were 65 years or older, 35% were 75 or older, and 3% were 85 or older. Sixty-five percent of patients were reported to have had one prior anti-cancer therapy for metastatic MCC and 35% had two or more prior therapies. Fifty-three percent of patients had visceral metastases. All patients had tumor samples evaluated for PD-L1 expression; of these, 66% were PD-L1-positive (≥ 1% of tumor cells), 18% were PD-L1 negative, and 16% had non-evaluable results by an investigational immunohistochemistry assay. Archival tumor samples were evaluated for Merkel cell polyomavirus (MCV) using an investigational assay; of the 77 patients with evaluable results, 52% had evidence of MCV.
Efficacy results are presented in Table 8. Responses were observed in patients regardless of tumor PD-L1 expression or presence of MCV.
Table 8: Efficacy Results of the JAVELIN Merkel 200 Trial Efficacy Endpoints Results
(N=88)CI: Confidence interval Overall Response Rate (ORR) Overall response rate, (95% CI) 33.0% (23.3%, 43.8%) Complete response (CR) rate, (95% CI) 11.4% (6.6%, 19.9%) Partial response (PR) rate, (95% CI) 21.6% (13.5%, 31.7%) Duration of Response (DOR) N=29 Range in months 2.8 to 23.3+ Patients with DOR ≥ 6 months, n (%) 25 (86%) Patients with DOR ≥ 12 months, n (%) 13 (45%) 14.2 Locally Advanced or Metastatic Urothelial Carcinoma
The efficacy and safety of BAVENCIO was demonstrated in the UC cohorts of the JAVELIN Solid Tumor trial, an open-label, single-arm, multi-center study that included 242 patients with locally advanced or metastatic urothelial carcinoma (UC) with disease progression on or after platinum-containing chemotherapy or who had disease progression within 12 months of treatment with a platinum-containing neoadjuvant or adjuvant chemotherapy regimen. Patients with active or history of central nervous system metastasis; other malignancies within the last 5 years; organ transplant; conditions requiring therapeutic immune suppression; or active infection with HIV, hepatitis B, or hepatitis C were excluded. Patients with autoimmune disease, other than type 1 diabetes, vitiligo, psoriasis, or thyroid disease that did not require immunosuppressive treatment, were excluded. Patients were included regardless of their PD-L1 status.
Patients received BAVENCIO at a dose of 10 mg/kg intravenously every 2 weeks until radiographic or clinical progression or unacceptable toxicity. Tumor response assessments were performed every 6 weeks. Efficacy outcome measures included confirmed overall response rate (ORR), as assessed by an Independent Endpoint Review Committee (IERC) using Response Evaluation Criteria in Solid Tumors (RECIST) v1.1, and duration of response (DOR). Efficacy was evaluated in patients who were followed for a minimum of both 13 weeks and 6 months at the time of data cut-off.
Baseline demographic and disease characteristics for the 226 patients with a minimum of 13 weeks of follow-up were median age 68 years (range: 30 to 89), 72% male, 80% White, and 34% and 66% of patients had an ECOG performance status 0 and 1, respectively. Forty-four percent of patients had non-bladder urothelial carcinoma including 23% of patients with upper tract disease, and 83% of patients had visceral metastases (baseline target and/or non-target lesions present outside of the lymph nodes). Nine (4%) patients had disease progression following prior platinum-containing neoadjuvant or adjuvant therapy only. Forty-seven percent of patients only received prior cisplatin-based regimens, 32% received only prior carboplatin-based regimens, and 20% received both cisplatin and carboplatin-based regimens. At baseline, 17% of patients had a hemoglobin < 10 g/dL and 34% of patients had liver metastases.
Efficacy results are presented in Table 9. The median time to response was 2.0 months (range: 1.3 to 11.0) among patients followed for either ≥ 13 weeks or ≥ 6 months. Using a clinical trial assay to assess PD-L1 staining, with 16% of patients not evaluable, there were no clear differences in response rates based on PD-L1 tumor expression. Among the total 30 responding patients followed for ≥ 13 weeks, 22 patients (73%) had an ongoing response of 6 months or longer and 4 patients (13%) had ongoing responses of 12 months or longer. Among the total 26 responding patients followed for ≥ 6 months, 22 patients (85%) had ongoing responses of 6 months or longer and 4 patients (15%) had ongoing responses of 12 months or longer.
Table 9: Efficacy Results of the UC Cohorts in the JAVELIN Solid Tumor Trial Efficacy Endpoints ≥ 13 Weeks Follow-Up
(N=226)≥ 6 Months Follow-Up
(N=161)CI: Confidence interval; NE: Not estimable; + denotes a censored value Confirmed Overall Response Rate (ORR) Overall Response Rate n (%) 30 (13.3%) 26 (16.1%) (95% CI) (9.1, 18.4) (10.8, 22.8) Complete Response (CR) n (%) 9 (4.0%) 9 (5.6%) Partial Response (PR) n (%) 21 (9.3%) 17 (10.6%) Duration of Response (DOR) Median, months (range) NE (1.4+ to 17.4+) NE (1.4+ to 17.4+) 14.3 Advanced Renal Cell Carcinoma
The efficacy and safety of BAVENCIO in combination with axitinib was demonstrated in the JAVELIN Renal 101 trial (NCT02684006), a randomized, multicenter, open-label, study of BAVENCIO in combination with axitinib in 886 patients with untreated advanced RCC regardless of tumor PD-L1 expression [intent-to-treat (ITT) population]. Patients with autoimmune disease or conditions requiring systemic immunosuppression were excluded.
Randomization was stratified according to Eastern Cooperative Oncology Group (ECOG) Performance Status (PS) (0 vs. 1) and region (United States vs. Canada/Western Europe vs. the rest of the world). Patients were randomized (1:1) to one of the following treatment arms:
- BAVENCIO 10 mg/kg intravenous infusion every 2 weeks in combination with axitinib 5 mg twice daily orally (N=442). Patients who tolerated axitinib 5 mg twice daily without Grade 2 or greater axitinib-related adverse events for 2 consecutive weeks could increase to 7 mg and then subsequently to 10 mg twice daily. Axitinib could be interrupted or reduced to 3 mg twice daily and subsequently to 2 mg twice daily to manage toxicity.
- Sunitinib 50 mg once daily orally for 4 weeks followed by 2 weeks off (N=444) until radiographic or clinical progression or unacceptable toxicity.
Treatment with BAVENCIO and axitinib continued until RECIST v1.1-defined progression of disease by Blinded Independent Central Review (BICR) assessment or unacceptable toxicity. Administration BAVENCIO and axitinib was permitted beyond RECIST-defined disease progression if the patient was clinically stable and considered to be deriving clinical benefit by the investigator. Assessment of tumor status was performed at baseline, after randomization at 6 weeks, then every 6 weeks thereafter up to 18 months after randomization, and every 12 weeks thereafter until documented confirmed disease progression by BICR.
Baseline characteristics were a median age of 61 years (range: 27 to 88), 38% of patients were 65 years or older, 75% were male, 75% were White, and the ECOG PS was 0 (63%) or 1 (37%), respectively. Patient distribution by International Metastatic Renal Cell Carcinoma Database (IMDC) risk groups was 21% favorable, 62% intermediate, and 16% poor.
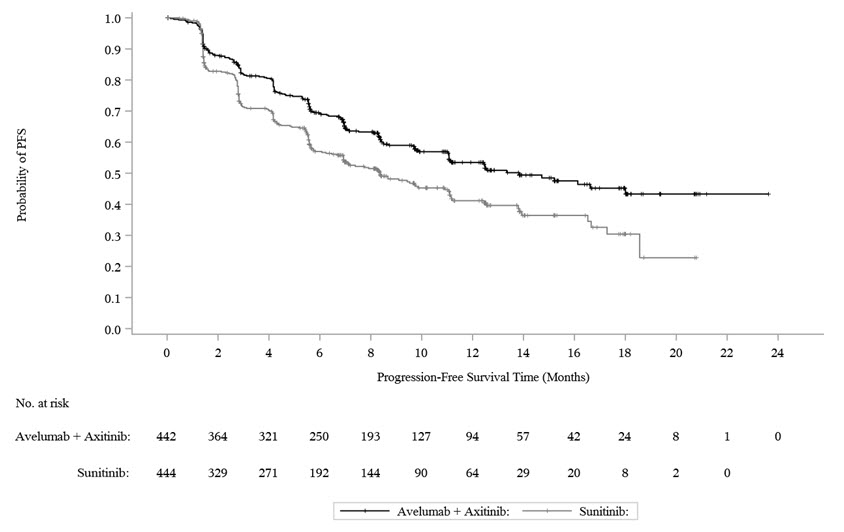
The major efficacy outcome measures were progression-free survival (PFS), as assessed by an BICR using RECIST v1.1 and overall survival (OS) in patients with PD-L1-positive tumors using a clinical trial assay (PD-L1 expression level ≥ 1%). Since PFS was statistically significant in patients with PD-L1-positive tumors [HR 0.61 (95% CI: 0.48, 0.79)], it was then tested in the ITT population and a statistically significant improvement in PFS in the ITT population was also demonstrated.
With a median overall survival follow-up of 19 months, overall survival data were immature with 27% deaths in the ITT population.
Efficacy results are presented in Table 10 and Figure 1.
Table 10: Efficacy Results from JAVELIN Renal 101 Trial - ITT Efficacy Endpoints
(Based on BICR Assessment)BAVENCIO plus Axitinib
(N=442)Sunitinib
(N=444)BICR: Blinded Independent Central Review; CI: Confidence interval; NE: Not estimable. - * p-value based on stratified log-rank.
Progression-Free Survival (PFS) Events (%) 180 (41) 216 (49) Median in months (95% CI) 13.8 (11.1, NE) 8.4 (6.9, 11.1) Hazard ratio (95% CI) 0.69 (0.56, 0.84) 2-sided p-value* 0.0002 Confirmed Objective Response Rate (ORR) Objective Response Rate n (%) 227 (51.4) 114 (25.7) (95% CI) (46.6, 56.1) (21.7, 30.0) Complete Response (CR) n (%) 15 (3.4) 8 (1.8) Partial Response (PR) n (%) 212 (48) 106 (24) Figure 1: K-M Estimates for PFS based on BICR Assessment – ITT
-
16 HOW SUPPLIED/STORAGE AND HANDLING
BAVENCIO (avelumab) Injection is a sterile, preservative-free, and clear, colorless to slightly yellow solution for intravenous infusion supplied as a single-dose vial of 200 mg/10 mL (20 mg/mL), individually packed into a carton (NDC: 44087-3535-1).
-
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Medication Guide).
Immune-Mediated Adverse Reactions
Inform patients of the risk of immune-mediated adverse reactions requiring corticosteroids or hormone replacement therapy, including, but not limited to:
- Pneumonitis: Advise patients to contact their healthcare provider immediately for new or worsening cough, chest pain, or shortness of breath [see Warnings and Precautions (5.1)].
- Hepatitis: Advise patients to contact their healthcare provider immediately for jaundice, severe nausea or vomiting, pain on the right side of abdomen, lethargy, or easy bruising or bleeding [see Warnings and Precautions (5.2)].
- Colitis: Advise patients to contact their healthcare provider immediately for diarrhea or severe abdominal pain [see Warnings and Precautions (5.3)].
- Endocrinopathies: Advise patients to contact their healthcare provider immediately for signs or symptoms of adrenal insufficiency, hypothyroidism, hyperthyroidism, and diabetes mellitus [see Warnings and Precautions (5.4)].
- Nephritis and Renal Dysfunction: Advise patients to contact their healthcare provider immediately for signs or symptoms of nephritis including decreased urine output, blood in urine, swelling in ankles, loss of appetite, and any other symptoms of renal dysfunction [see Warnings and Precautions (5.5)].
Infusion-Related Reactions
Advise patients to contact their healthcare provider immediately for signs or symptoms of potential infusion-related reactions [see Warnings and Precautions (5.7)].
Major Adverse Cardiovascular Events
Advise patients receiving BAVENCIO in combination with axitinib to contact their healthcare provider immediately for signs or symptoms of cardiovascular events including but not limited to new or worsening chest discomfort, dyspnea, or peripheral edema [see Warnings and Precautions (5.8).
Embryo-Fetal Toxicity
Advise females of reproductive potential that BAVENCIO can cause fetal harm. Instruct females of reproductive potential to use effective contraception during and for at least one month after the last dose of BAVENCIO [see Warnings and Precautions (5.9) and Use in Specific Populations (8.1, 8.3)].
Lactation
Advise nursing mothers not to breastfeed while taking BAVENCIO and for at least one month after the final dose [see Use in Specific Populations (8.2)].
- SPL UNCLASSIFIED SECTION
-
MEDICATION GUIDE
-
PRINCIPAL DISPLAY PANEL - 10 mL Vial Carton
NDC: 44087-3535-1
BAVENCIO®
(avelumab)
Injection200 mg/10 mL
(20 mg/mL)For intravenous infusion
after dilution
Single-dose vial
Discard unused portion.Dispense the enclosed
Medication Guide to each
patient.1 vial
Rx onlyEMD
SERONOPfizer
-
INGREDIENTS AND APPEARANCE
BAVENCIO
avelumab injection, solution, concentrateProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 44087-3535 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength avelumab (UNII: KXG2PJ551I) (avelumab - UNII:KXG2PJ551I) avelumab 20 mg in 1 mL Inactive Ingredients Ingredient Name Strength MANNITOL (UNII: 3OWL53L36A) acetic acid (UNII: Q40Q9N063P) polysorbate 20 (UNII: 7T1F30V5YH) sodium hydroxide (UNII: 55X04QC32I) water (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 44087-3535-1 1 in 1 CARTON 03/23/2017 1 10 mL in 1 VIAL, SINGLE-DOSE; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA761049 03/23/2017 Labeler - EMD Serono, Inc. (088514898)
Trademark Results [BAVENCIO]
Mark Image Registration | Serial | Company Trademark Application Date |
|---|---|
 BAVENCIO 86663701 5083111 Live/Registered |
MERCK KGAA 2015-06-16 |
 BAVENCIO 85499483 not registered Dead/Abandoned |
Pfizer Inc. 2011-12-20 |
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.