Cephalexin by Denton Pharma, Inc. DBA Northwind Pharmaceuticals CEPHALEXIN capsule
Cephalexin by
Drug Labeling and Warnings
Cephalexin by is a Prescription medication manufactured, distributed, or labeled by Denton Pharma, Inc. DBA Northwind Pharmaceuticals. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use CEPHALEXIN CAPSULES safely and effectively. See full prescribing information for CEPHALEXIN CAPSULES.
CEPHALEXIN capsules, for oral use
Initial U.S. Approval: 1971INDICATIONS AND USAGE
Cephalexin is a cephalosporin antibacterial drug indicated for the treatment of the following infections caused by susceptible isolates of designated bacteria:
- Respiratory tract infection (
1.1)
- Otitis media (
1.2)
- Skin and skin structure infections (
1.3)
- Bone infections (
1 . 4 )
- Genitourinary tract infections (
1.5)
To reduce the development of drug-resistant bacteria and maintain the effectiveness of cephalexin and other antibacterial drugs, Cephalexin should be used only to treat infections that are proven or strongly suspected to be caused by bacteria. (1.6)
DOSAGE AND ADMINISTRATION
Adults and patients at least 15 years of age T he usual dose is 250 mg every 6 hours, but a dose of 5 00 mg every 12 hours may be administered ( 2. 1)
Pediatric patients (over 1 year of age)
DOSAGE FORMS AND STRENGTHS
Capsules: 250 m g, 333mg, 500 mg and 750 mg ( 3)
CONTRAINDICATIONS
Patients with known hypersensitivity to cephalexin or other members of the cephalosporin class of antibacterial drugs. ( 4) (4)
WARNINGS AND PRECAUTIONS
- Serious hypersensitivity (anaphylactic) reactions: Prior to use, inquire regarding history of hypersensitivity to beta-lactam antibacterial drugs. Discontinue the drug if signs or symptoms of an allergic reaction occur and institute supportive measures. ( 5 .1)
-
Clostridium difficile-associated diarrhea (CDAD): Evaluate if diarrhea occurs. (
5. 2)
-
Direct Coomb’s Test Seroconversion: If anemia develops during or after cephalexin therapy, evaluate for drug-induced hemolytic anemia. (
5. 3 )
-
Seizure Potential: Use lower dose in patients with renal impairment. (
5.4)
ADVERSE REACTIONS
The most common adverse reactions associated with cephalexin include diarrhea, nausea, vomiting, dyspepsia and abdominal pain. ( 6)
To report SUSPECTED ADVERSE REACTIONS, contact Ascend Laboratories, LLC at 1-877-ASC-RX01 (877-272-7901) or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
- Metformin: increased metformin concentrations. Monitor for hypoglycemia. ( 7.1)
- Probenecid- The renal excretion of cephalexin is inhibited by probenecid. Co-administration of probenecid with cephalexin is not recommended. (
7.2)
- Administration of cephalexin may result in a false-positive reaction for glucose in the urine. ( 7.3)
See 17 for PATIENT COUNSELING INFORMATION.
Revised: 4/2020
- Respiratory tract infection (
1.1)
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS & USAGE
1.1 Respiratory Tract Infections
1.2 Otitis Media
1.3 Skin and Skin Structure Infections
1.4 Bone Infections
1.5 Genitourinary Tract Infections
1.6 Usage
2 DOSAGE & ADMINISTRATION
2.1 Adults and Pediatric Patients at Least 15 Years of Age
2.2 Pediatric Patients (over 1 year of age)
2.3 Dosage Adjustments in Adult and Pediatric Patients at Least 15 Years of Age With Renal Impairment
3 DOSAGE FORMS & STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Hypersensitivity Reactions
5.2 Clostridium difficile-Associated Diarrhea
5.3 Direct Coombs’ Test Seroconversion
5.4 Seizure Potential
5.5 Prolonged Prothrombin Time
5.6 Development of Drug-Resistant Bacteria
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
7 DRUG INTERACTIONS
7.1 Metformin
7.2 Probenecid
7.3 Interaction With Laboratory or Diagnostic Testing
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.3 Nursing Mothers
8.4 Pediatric Use
8.5 Geriatric Use
8.6 Renal Impairment
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.3 Pharmacokinetics
12.4 Microbiology
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis & Mutagenesis & Impairment Of Fertility
15 REFERENCES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- * Sections or subsections omitted from the full prescribing information are not listed.
-
1 INDICATIONS & USAGE
1.1 Respiratory Tract Infections
Cephalexin is indicated for the treatment of respiratory tract infections caused by susceptible isolates of Streptococcus pneumoniae and Streptococcuspyogenes.
1.2 Otitis Media
Cephalexin is indicated for the treatment of otitis media caused by susceptible isolates of Streptococcuspneumoniae, Haemophilus infl uenz ae, Staphylococcus aureus, Streptococcuspyogenes, and Mo raxella catarrhalis.
1.3 Skin and Skin Structure Infections
Cephalexin is indicated for the treatment of skin and skin structure infections caused by susceptible isolates of the following Gram-positive bacteria: Staphylococcus aureus and Streptococcus pyogenes.
1.4 Bone Infections
Cephalexin is indicated for the treat ment of bone infections caused by susceptible isolates of Staphylococcusaureus and Proteus mi rabilis.
1.5 Genitourinary Tract Infections
Cephalexin is indicated for the treatment of genitourinary tract infections, including acute prostatitis, caused by susceptible isolates of Escheric hia c oli, Proteus mirabilis, and Klebsiella pneumonia e.
1.6 Usage
To reduce the development of drug-resistant bacteria and maintain the effectiveness of cephalexin and other antibacterial drugs, Cephalexin should be used only to treat infections that are proven or strongly suspected to be caused by susceptible bacteria. When culture and susceptibility information is available, this information should be considered in selecting or modifying antibacterial therapy. In the absence of such data, local epidemiology and susceptibility patterns may contribute to the empiric selection of therapy.
-
2 DOSAGE & ADMINISTRATION
2.1 Adults and Pediatric Patients at Least 15 Years of Age
The usual dose of oral Cephalexin capsule, USP is 250 mg every 6 hours, but a dose of 500 mg every 12 hours may be administered. Treatment is administered for 7 to 14 days.
For more severe infections larger doses of oral Cephalexin capsules, USP may be needed, up to 4 grams daily in two to four equally divided doses.
2.2 Pediatric Patients (over 1 year of age)
The recommended total daily doseof oral Cephalexin capsules, USP for pediatric patients is 25 to 50 mg/kg givenin equally divided doses for 7 to 14 days. In the treatment of β-hemolyticstreptococcal infections, duration of at least 10 days is recommended. Insevere infections, a total daily dose of 50 to 100 mg/kg may be administered inequally divided doses.
For thetreatment of otitis media, the recommended daily dose is 75 to 100 mg/kg givenin equally divided doses.
2.3 Dosage Adjustments in Adult and Pediatric Patients at Least 15 Years of Age With Renal Impairment
Administer the following dosing regimens for Cephalexin capsules, USP to patients with impaired renal function [see War nin gsand Precautions (5.4) and Use inSpecific Populations (8.6 )].
Table 1. Recommended Dose Regimen for Patients with Renal Impairment
Renal Function Dose regimen recommendation Creatinine cleartance ≥ 60mL/min. No dose adjustment
Creatinine clearance 30 to 59 mL / min
No dose adjustment; maximum daily dose should not exceed 1 g
Creati nine clearance 15 to 29 mL / min
250 mg, every 8 hours or every 12 hours
Creati nine clearance 5 to 14 mL / min not yet on dialysis*
250 mg, every 24 hours
Creati nine clearance 1 to 4 mL / min not yet on dialysis*
250 mg, every 48 hours or every 60 hours
*There is insufficient information to make dose adjustment recommendations in patients on hemodialysis.
-
3 DOSAGE FORMS & STRENGTHS
250 mg capsules: a white to off white powder filled into size 2 capsules (dark green cap and dark green body) that are imprinted with “220” on the both cap and body in edible black ink.
500 mg capsules: a white to off white powder filled into size 0 capsules (light green cap and light green body) that are imprinted with “219” on the both cap and body in edible black ink.
333 mg capsules: a white to off white powder filled into size 1 capsules (light green cap and light green body) that are imprinted “CEP” on cap and “333” on body in edible black ink.
750 mg capsules: a white to off white powder filled into size '00 Elongated' capsules (dark green cap and dark green body) that are imprinted “CEP” on cap and “750” on body in edible white ink.
- 4 CONTRAINDICATIONS
-
5 WARNINGS AND PRECAUTIONS
5.1 Hypersensitivity Reactions
Allergic reactions in the form of rash, urticaria, angioedema, anaphylaxis, erythema multiforme, Stevens- Johnson syndrome, or toxic epidermal necrolysis have been reported with the use of cephalexin. Before therapy with cephalexin is instituted, inquire whether the patient has a history of hypersensitivity reactions to cephalexin, cephalosporins, penicillins, or other drugs. Cross-hypersensitivity among beta-lactam antibacterial drugs may occur in up to 10% of patients with a history of penicillin allergy.
If an allergic reaction to cephalexin occurs, discontinue the drug and institute appropriate treatment.5.2 Clostridium difficile-Associated Diarrhea
Clostridium difficile-associated diarrhea (CDAD) has been reported with use of nearly all antibacterial agents, including cephalexin, and may range in severity from mild diarrhea to fatal colitis. Treatment with antibacterial agents alters the normal flora of the colon leading to overgrowth of C. difficile.
C. difficile produces toxins A and B, which contribute to the development of CDAD. Hypertoxin-producing strains of C. difficile cause increased morbidity and mortality, as these infections can be refractory to antimicrobial therapy and may require colectomy. CDAD must be considered in all patients who present with diarrhea following antibiotic use. Careful medical history is necessary since CDAD has been reported to occur over two months after the administration of antibacterial agents.
If CDAD is suspected or confirmed, ongoing antibiotic use not directed against C. difficile may need to be discontinued. Appropriate fluid and electrolyte management, protein supplementation, antibiotic treatment of C. difficile, and surgical evaluation should be instituted as clinically indicated.
5.3 Direct Coombs’ Test Seroconversion
Positive direct Coombs’ tests have been reported during treatment with the cephalosporin antibacterial drugs including cephalexin. Acute intravascular hemolysis induced by cephalexin therapy has been reported. If anemia develops during or after cephalexin therapy, perform a diagnostic work-up for drug-induced hemolytic anemia, discontinue cephalexin and institute appropriate therapy.
5.4 Seizure Potential
Several cephalosporins have been implicated in triggering seizures, particularly in patients with renal impairment when the dosage was not reduced. If seizures occur, discontinue cephalexin. Anticonvulsant therapy can be given if clinically indicated.
5.5 Prolonged Prothrombin Time
Cephalosporins may be associated with prolonged prothrombin time. Those at risk include patients with renal or hepatic impairment, or poor nutritional state, as well as patients receiving a protracted course of antibacterial therapy, and patients receiving anticoagulant therapy. Monitor prothrombin time in patients at risk and manage as indicated.
5.6 Development of Drug-Resistant Bacteria
Prescribing cephalexin in the absence of a proven or strongly suspected bacterial infection is unlikely to provide benefit to the patient and increases the risk of the development of drug-resistant bacteria.
Prolonged use of cephalexin may result in the overgrowth of nonsusceptible organisms. Careful observation of the patient is essential. If superinfection occurs during therapy, appropriate measures should be taken.
-
6 ADVERSE REACTIONS
The following serious events are described in greater detail in the Warning and Precautions section:
- Hypersensitivity reactions [ see Warning and Precautions ( 5.1 ) ]
-
Clostridium difficile-associated diarrhea [
see Warnings and Precautions (
5.2 )
]
- Direct Coombs’ Test Seroconversion [
see Warnings and Precautions (
5.3 )
]
- Seizure Potential [
see Warnings and Precautions (
5.4 )
]
- Effect on Prothrombin Activity [
see Warnings and Precautions (
5.5 )
]
- Development of Drug-Resistant Bacteria [
see Warnings and Precautions (
5.6 )
]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice
In clinical trials, the most frequent adverse reaction was diarrhea. Nausea and vomiting, dyspepsia, gastritis, and abdominal pain have also occurred. As with penicillins and other cephalosporins, transient hepatitis and cholestatic jaundice have been reported.
Other reactions have included hypersensitivity reactions, genital and anal pruritus, genital candidiasis, vaginitis and vaginal discharge, dizziness, fatigue, headache, agitation, confusion, hallucinations, arthralgia, arthritis, and joint disorder. Reversible interstitial nephritis has been reported. Eosinophilia, neutropenia, thrombocytopenia, hemolytic anemia, and slight elevations in aspartate transaminase (AST) and alanine transaminase (ALT) have been reported.
In addition to the adverse reactions listed above that have been observed in patients treated with cephalexin, the following adverse reactions and other altered laboratory tests have been reported for cephalosporin class antibacterial drugs:
Other Adverse Reactions: Fever, colitis, aplastic anemia, hemorrhage, renal dysfunction, and toxic nephropathy.
Altered Laboratory Tests:Prolonged prothrombin time, increased blood urea nitrogen (BUN), increased creatinine, elevated alkaline phosphatase, elevated bilirubin, elevated lactate dehydrogenase (LDH), pancytopenia, leukopenia, and agranulocytosis.
-
7 DRUG INTERACTIONS
7.1 Metformin
Administration of cephalexin with metformin results in increased plasma metformin concentrations and decreased renal clearance of metformin.
Careful patient monitoring and dose adjustment of metformin is recommended in patients concomitantly taking cephalexin and metformin [ see Clinical Pharmacology (12.2) ].
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Category B
There are no adequate and well-controlled studies in pregnant women. Because animal reproduction studies are not always predictive of human response, this drug should be used during pregnancy only if clearly needed.
Reproduction studies have been performed on mice and rats using oral doses of cephalexin monohydrate 0.6 and 1.5 times the maximum daily human dose (66 mg/kg/day) based upon body surface area basis, and have revealed no evidence of impaired fertility or harm to the fetus.
8.3 Nursing Mothers
Cephalexin is excreted in human milk. Caution should be exercised when Cephalexin is administered to a nursing woman.
8.4 Pediatric Use
The safety and effectiveness of cephalexin in pediatric patients was established in clinical trials for the dosages described in the dosage and administration section [see Dosage and Administration ( 2.2 ) ] .
8.5 Geriatric Use
Of the 701 subjects in 3 published clinical studies of cephalexin, 433 (62%) were 65 and over. No overall differences in safety or effectiveness were observed between these subjects and younger subjects, and other reported clinical experience has not identified differences in responses between the elderly and younger patients.
This drug is substantially excreted by the kidney, and the risk of toxic reactions to this drug may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection [ see Warnings and Precautions ( 5.4 ) ].
8.6 Renal Impairment
Cephalexin should be administered with caution in the presence of impaired renal function (creatinine clearance < 30 mL/min, with or without dialysis). Under such conditions, careful clinical observation and laboratory studies renal function monitoring should be conducted because safe dosage may be lower than that usually recommended [see Dosage and Administration ( 2.3 ) ] .
-
10 OVERDOSAGE
Symptoms of oral overdose may include nausea, vomiting, epigastric distress, diarrhea, and hematuria. In the event of an overdose, institute general supportive measures.
Forced diuresis, peritoneal dialysis, hemodialysis, or charcoal hemoperfusion have not been established as beneficial for an overdose of cephalexin.
-
11 DESCRIPTION
Cephalexin capsules, USP is a semisynthetic cephalosporin antibacterial drug intended for oral administration. It is 7-(D-α-Amino-α-phenylacetamido)-3-methyl-3-cephem-4-carboxylic acid monohydrate. Cephalexin has the molecular formula C 16 H 17 N 3O 4SH 2Oand the molecular weight is 365.41.
Cephalexin has the following structural formula: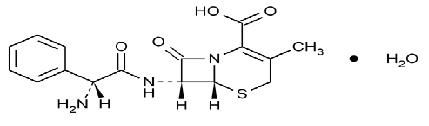
Each capsule contains cephalexin monohydrate equivalent to 250 mg, 333 mg, 500 mg, or 750 mg of cephalexin. The 250 mg, 333 mg, 500 mg and 750 mg capsules contain anhydrous lactose, colloidal silicon dioxide, magnesium stearate, FD & C Blue No. 1, D & C Yellow No. 10, gelatin, sodium lauryl sulphate, titanium dioxide. In addition, the 250 mg capsule contains FD & C Red No. 40; 333 mg and 750 mg Capsules contains FD & C Yellow No. 6. The imprinting ink contains; shellac, propylene glycol, strong ammonia solution and potassium hydroxide. Also black Iron oxide is used in 250mg, 333mg and 500mg and titanium dioxide is used in 750mg.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Cephalexin is a cephalosporin antibacterial drug [seeMicrobiology ( 12.4 ) ] .
12.3 Pharmacokinetics
Absorption:
Cephalexin is acid stable and may be given without regard to meals. Following doses of 250 mg, 500 mg, and 1 g, average peak serum levels of approximately 9, 18, and 32 mcg/mL, respectively, were obtained at 1 hour. Serum levels were detectable 6 hours after administration (at a level of detection of 0.2 mcg/mL).
Distribution:
Cephalexin is approximately 10% to 15% bound to plasma proteins.
Excretion:
Cephalexin is excreted in the urine by glomerular filtration and tubular secretion. Studies showed that over 90% of the drug was excreted unchanged in the urine within 8 hours. During this period, peak urine concentrations following the 250 mg, 500 mg, and 1 g doses were approximately 1000, 2200, and 5000 mcg/mL respectively.
Drug Interactions
In healthy subjects given single 500 mg doses of cephalexin and metformin, plasma metformin mean Cmax and AUC increased by an average of 34% and 24%, respectively, and metformin mean renal clearance decreased by 14%. No information is available about the interaction of cephalexin and metformin following multiple doses of either drug.
12.4 Microbiology
Mechanism of Action
Cephalexin is a bactericidal agent that acts by the inhibition of bacterial cell-wall synthesis.
Resistance
Methicillin-resistant staphylococci and most isolates of enterococci are resistant to cephalexin. Cephalexin is not active against most isolates of Enterobacter spp., Morganella morganii, and Proteus vulgaris. Cephalexin has no activity against Pseudomonas spp., or Acinetobacter calcoaceticus. Penicillin-resistant Streptococcus pneumoniae is usually cross-resistant to beta-lactam antibacterial drugs.
Antimicrobial Activity
Cephalexin has been shown to be active against most isolates of the following bacteria both in vitro and in clinical infections [ see Indications and Usage (1) ].
Gram-positive bacteria
Staphylococcus aureus (methicillin-susceptible isolates only)
Streptococcus pneumoniae (penicillin-susceptible isolates)
Streptococcus pyogenes
Gram-negative bacteria
Escheric h ia coli
Haemophilusinfl uenzae
Klebsiellapneumoniae
Moraxella catarrhalis
Proteusmi rabilis
Susceptibility Tests Methods
When available, the clinical microbiology laboratory should provide the results of in vitro susceptibility test results for antimicrobial drug products used in resident hospitals to the physician as periodic reports that describe the susceptibility profile of nosocomial and community-acquired pathogens. These reports should aid the physician in selecting an antibacterial drug product for treatment.
In cases of uncomplicated urinary tract infection only, susceptibility of E. coli, K. pneumoniae, and P. mirabilis to cephalexin may be inferred by testing cefazolin2.
Dilution Techniques
Quantitative methods are used to determine antimicrobial minimal inhibitory concentrations (MICs). These MICs provide estimates of the susceptibility of bacteria to antimicrobial compounds. The MICs should be determined using a standardized test methods (broth or agar)1,2.
Diffusion Techniques
Quantitative methods that require measurement of zone diameters also provide reproducible estimates of the susceptibility of bacteria to antimicrobial compounds. The zone size provides an estimate of the susceptibility of bacteria to antimicrobial compounds. The zone size should be determined using a standardized test method2,3.
A report of Susceptible (S) indicates that the antimicrobial drug is likely to inhibit growth of the pathogen if the antimicrobial drug reaches the concentration usually achievable at the site of infection. A report of Intermediate (I) indicates that the result should be considered equivocal, and if the microorganism is not fully susceptible to alternative clinically feasible drugs, the test should be repeated. This category implies possible clinical applicability in body sites where the drug is physiologically concentrated or in situations where a high dosage of the drug can be used. This category also provides a buffer zone that prevents small uncontrolled technical factors from causing major discrepancies in interpretation. A report of Resistant (R) indicates that the antimicrobial drug is not likely to inhibit growth of the pathogen if the antimicrobial drug reaches the concentrations usually achievable at the infection site; other therapy should be selected.
Quality Co n t r ol
Standardized susceptibility test procedures require the use of laboratory controls to monitor and ensure the accuracy and precision of supplies and reagents used in the assay, and the techniques of the individual performing the test 1,2,3,.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis & Mutagenesis & Impairment Of Fertility
Lifetime studies in animals have not been performed to evaluate the carcinogenic potential of cephalexin. Tests to determine the mutagenic potential of cephalexin have not been performed. In male and female rats, fertility and reproductive peLifetime studies in animals have not been performed to evaluate the carcinogenic potential of cephalexin. Tests to determine the mutagenic potential of cephalexin have not been performed. In male and female rats, fertility and reproductive performance were not affected by cephalexin oral doses up to 1.5 times the highest recommended human dose based upon body surface area.rformance were not affected by cephalexin oral doses up to 1.5 times the highest recommended human dose based upon mg/m2.
-
15 REFERENCES
1. Clinical and Laboratory Standards Institute (CLSI). Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria that Grow Aerobically; Approved Standard - Tenth Edition. CLSI document M07-A10, Clinical and Laboratory Standards Institute, 950 West Valley Road, Suite 2500, Wayne, Pennsylvania 19087, USA, 2015.
2. Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobials Susceptibility Tests; Twenty-Fifth Informational Supplement. CLSI document M100-S25, Clinical and Laboratory Standards Institute, 950 West Valley Road, Suite 2500, Wayne, Pennsylvania 19087, USA, 2015.
3. Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Disk Susceptibility Tests; Approved Standard - Twelfth Edition. CLSI document M02-A12, Clinical and Laboratory Standards Institute, 950 West Valley Road, Suite 2500, Wayne, Pennsylvania 19087, USA, 2015. -
16 HOW SUPPLIED/STORAGE AND HANDLING
Cephalexin capsules, USP, are supplied as follows:
The 500 mg capsules are a white to off white powder filled into size 0 capsules (light green cap and light green body) that are imprinted with “219” on the both cap and body in edible black ink. They are available as follows:
Bottles of 10 NDC: 70934-040-10
Bottles of 14 NDC: 70934-040-14
Bottles of 20 NDC: 70934-040-20
Bottles of 21 NDC: 70934-040-21
Bottles of 28 NDC: 70934-040-28
Bottles of 30 NDC: 70934-040-30
Bottles of 40 NDC: 70934-040-40
Bottles of 56 NDC: 70934-040-56
30 Capsules (1 x 30 Dosepack) NDC: 70934-040-94
Store at 20°C to 25°C (68°F to77°F); excursions permitted to 15 to 30°C (59 to 86°F) [see USP Controlled Room Temperature]. -
17 PATIENT COUNSELING INFORMATION
- Advise patients that allergic reactions, including serious allergic reactions, could occur and that serious reactions require immediate treatment. Ask the patient about any previous hypersensitivity reactions to cephalexin, other beta-lactams (including cephalosporins) or other allergens (5.1)
- Advise patients that diarrhea is a common problem caused by antibacterial drugs and usually resolves when the drug is discontinued. Sometimes, frequent watery or bloody diarrhea may occur and may be a sign of a more serious intestinal infection. If severe watery or bloody diarrhea develops, advise patients to contact their healthcare provider
- Counsel patients that antibacterial drugs including cephalexin, should only be used to treat bacterial infections. They do not treat viral infections (e.g., the common cold). When cephalexin is prescribed to treat a bacterial infection, tell patients that although it is common to feel better early in the course of therapy, the medication should be taken exactly as directed. Skipping doses or not completing the full course of therapy may (1) decrease the effectiveness of the immediate treatment and (2) increase the likelihood that bacteria will develop resistance and will not be treatable by cephalexin or other antibacterial drugs in the future.
Manufactured by:
Alkem Laboratories ltd.
Mumbai - 400 013, India
Distributed by:
Ascend Laboratories, LLC
Parsippany, NJ 07054
Revised: July 2016
PT 1199-08
- PACKAGE LABEL.PRINCIPAL DISPLAY PANEL
-
INGREDIENTS AND APPEARANCE
CEPHALEXIN
cephalexin capsuleProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 70934-040(NDC:67877-219) Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength CEPHALEXIN (UNII: OBN7UDS42Y) (CEPHALEXIN ANHYDROUS - UNII:5SFF1W6677) CEPHALEXIN ANHYDROUS 500 mg Inactive Ingredients Ingredient Name Strength AMMONIA (UNII: 5138Q19F1X) POTASSIUM HYDROXIDE (UNII: WZH3C48M4T) FERROSOFERRIC OXIDE (UNII: XM0M87F357) SHELLAC (UNII: 46N107B71O) ANHYDROUS LACTOSE (UNII: 3SY5LH9PMK) MAGNESIUM STEARATE (UNII: 70097M6I30) FD&C BLUE NO. 1 (UNII: H3R47K3TBD) D&C YELLOW NO. 10 (UNII: 35SW5USQ3G) GELATIN (UNII: 2G86QN327L) SODIUM LAURYL SULFATE (UNII: 368GB5141J) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) SILICON DIOXIDE (UNII: ETJ7Z6XBU4) PROPYLENE GLYCOL (UNII: 6DC9Q167V3) Product Characteristics Color green (light green cap and body) Score no score Shape CAPSULE Size 22mm Flavor Imprint Code 219 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 70934-040-14 14 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 10/30/2017 2 NDC: 70934-040-20 20 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 10/30/2017 3 NDC: 70934-040-21 21 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 10/30/2017 4 NDC: 70934-040-28 28 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 10/30/2017 5 NDC: 70934-040-30 30 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 10/30/2017 6 NDC: 70934-040-40 40 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 10/30/2017 7 NDC: 70934-040-10 10 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 03/01/2018 8 NDC: 70934-040-94 30 in 1 DOSE PACK; Type 0: Not a Combination Product 01/22/2018 9 NDC: 70934-040-56 56 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 07/19/2018 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA090836 10/30/2017 Labeler - Denton Pharma, Inc. DBA Northwind Pharmaceuticals (080355546) Registrant - Denton Pharma, Inc. DBA Northwind Pharmaceuticals (080355546) Establishment Name Address ID/FEI Business Operations Denton Pharma, Inc. DBA Northwind Pharmaceuticals 080355546 repack(70934-040)

© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.