ZANAFLEX- tizanidine hydrochloride capsule ZANAFLEX- tizanidine hydrochloride tablet
Zanaflex by
Drug Labeling and Warnings
Zanaflex by is a Prescription medication manufactured, distributed, or labeled by Legacy Pharma USA, Inc., Patheon Manufacturing Services LLC, Patheon Inc.. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use ZANAFLEX ®safely and effectively. See full prescribing information for ZANAFLEX.
ZANAFLEX ®(tizanidine) capsules, for oral use
ZANAFLEX ®(tizanidine) tablets, for oral use
Initial U.S. Approval: 1996RECENT MAJOR CHANGES
INDICATIONS AND USAGE
Zanaflex is a central alpha-2-adrenergic agonist indicated for the treatment of spasticity. ( 1)
DOSAGE AND ADMINISTRATION
- Monitoring of aminotransferase levels is recommended at baseline and 1 month after maximum dose is achieved. ( 2.1)
- Recommended starting dose: 2 mg by mouth every 6 to 8 hours, as needed, up to a maximum of 3 doses in 24 hours ( 2.2)
- Dosage can be increased by 2 mg to 4 mg per dose every 1 to 4 days; maximum total daily dosage is 36 mg ( 2.2)
- Tizanidine pharmacokinetics differs between tablets and capsules, and when taken with or without food. These differences could result in a change in tolerability and control of symptoms. Consistent administration with respect to food is recommended. If substitution between dosage forms is necessary, take into consideration these pharmacokinetic differences. ( 2.2, 2.6, 12.3)
- Patients with renal impairment (creatinine clearance <25 mL/min) or hepatic impairment: use lower individual doses during titration. If higher doses are required, individual doses rather than dosing frequency should be increased. ( 2.3, 2.4)
- To discontinue Zanaflex, decrease dose slowly to minimize the risk of withdrawal adverse reactions ( 2.5)
CONTRAINDICATIONS
WARNINGS AND PRECAUTIONS
- Hypotension: monitor for signs and symptoms of hypotension, in particular in patients receiving concurrent antihypertensives; Zanaflex should not be used with other α 2-adrenergic agonists ( 5.1, 7.7)
- Risk of liver injury: monitor ALTs; discontinue Zanaflex if liver injury occurs ( 5.2)
- Sedation: Zanaflex may interfere with everyday activities; sedative effects of Zanaflex, alcohol, and other central nervous system (CNS) depressants are additive ( 5.3, 7.4)
- Hallucinations: consider discontinuation of Zanaflex ( 5.4)
ADVERSE REACTIONS
The most common adverse reactions (greater than 10% of patients taking tizanidine and greater than in patients taking placebo) were dry mouth, somnolence, asthenia, and dizziness. ( 6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Legacy Pharma Inc. at 1-8007277151 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
USE IN SPECIFIC POPULATIONS
See 17 for PATIENT COUNSELING INFORMATION.
Revised: 11/2024
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Evaluation and Testing Before and After Initiating Zanaflex
2.2 Recommended Dosage
2.3 Recommended Dosage in Patients with Renal Impairment
2.4 Recommended Dosage in Patients with Hepatic Impairment
2.5 Discontinuation of Zanaflex
2.6 Switching Between With/Without Food and Different Tizanidine Dosage Forms
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Hypotension
5.2 Liver Injury
5.3 Sedation
5.4 Hallucinosis/Psychotic-Like Symptoms
5.5 Hypersensitivity Reactions
5.6 Withdrawal Adverse Reactions
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
6.2 Postmarketing Experience
7 DRUG INTERACTIONS
7.1 Strong CYP1A2 Inhibitors
7.2 Moderate or Weak CYP1A2 Inhibitors
7.3 Oral Contraceptives
7.4 Alcohol and Other CNS Depressants
7.5 α 2-Adrenergic Agonists
7.6 Antihypertensive Medications
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.3 Females and Males of Reproductive Potential
8.4 Pediatric Use
8.5 Geriatric Use
8.6 Renal Impairment
8.7 Hepatic Impairment
9 DRUG ABUSE AND DEPENDENCE
9.1 Controlled Substance
9.2 Abuse
9.3 Dependence
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 How Supplied
16.2 Storage and Handling
17 PATIENT COUNSELING INFORMATION
- * Sections or subsections omitted from the full prescribing information are not listed.
- 1 INDICATIONS AND USAGE
-
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Evaluation and Testing Before and After Initiating Zanaflex
Monitoring of aminotransferase levels is recommended at baseline and 1 month after maximum dose is achieved [see Warnings and Precautions ( 5.2)] .
2.2 Recommended Dosage
The recommended starting dose is 2 mg by mouth every 6 to 8 hours, as needed, to a maximum of three doses in 24 hours.
Dosage can be gradually increased every 1 to 4 days by 2 mg to 4 mg at each dose based on clinical response and tolerability. The maximum total daily dosage is 36 mg. Single doses greater than 16 mg have not been studied.
There are pharmacokinetic differences when administering Zanaflex between the fed or fasted state [see Clinical Pharmacology ( 12.3)] . Zanaflex may be taken with or without food; however, consistent administration with respect to food is recommended to reduce variability in tizanidine plasma exposure.
Because of the short duration of therapeutic effect, treatment with Zanaflex should be reserved for those daily activities and times when relief of spasticity is most important.
2.3 Recommended Dosage in Patients with Renal Impairment
In patients with creatinine clearance < 25 mL/min, use lower individual doses during titration. If higher doses are required, the individual doses rather than dosing frequency should be increased [see Use in Specific Populations ( 8.6) and Clinical Pharmacology ( 12.3)] .
2.4 Recommended Dosage in Patients with Hepatic Impairment
In patients with hepatic impairment, use lower individual doses during titration. If higher doses are required, individual doses rather than dosing frequency should be increased [see Use in Specific Populations ( 8.7) and Clinical Pharmacology ( 12.3)] .
2.5 Discontinuation of Zanaflex
When discontinuing Zanaflex, particularly in patients who have been receiving high doses for long periods or who may be on concomitant treatment with narcotics, decrease the dosage by 2 mg to 4 mg per day to minimize the risk of withdrawal adverse reactions [see Drug Abuse and Dependence ( 9.3)] .
2.6 Switching Between With/Without Food and Different Tizanidine Dosage Forms
There are pharmacokinetic differences when:
- switching between administration of Zanaflex with or without food
- switching between dosage forms if being administered with food.
If these situations occur, monitor patients for therapeutic effect or adverse reactions [see Dosage and Administration ( 2.2) and Clinical Pharmacology ( 12.3)] .
-
3 DOSAGE FORMS AND STRENGTHS
Capsules
2 mg: Light blue opaque body with a light blue opaque cap with “2 MG” printed on the cap
4 mg: White opaque body with a blue opaque cap with “4 MG” printed on the cap
6 mg: Blue opaque body with a white stripe and blue opaque cap with “6 MG” printed on the cap
Tablets
4 mg white, uncoated tablets with a quadrisecting score on one side and debossed with “A594” on the other side
- 4 CONTRAINDICATIONS
-
5 WARNINGS AND PRECAUTIONS
5.1 Hypotension
Zanaflex is an α 2-adrenergic agonist that can produce hypotension [see Adverse Reactions ( 6.1) and Drug Interactions ( 7.5)] . Syncope has been reported in patients treated with tizanidine in the postmarketing setting. The risk of hypotension may be minimized by dose titration; monitoring for signs and symptoms of hypotension prior to dosage increase may minimize the risks associated with hypotension. In addition, patients moving from a supine to fixed upright position may be at increased risk for hypotension and orthostatic effects.
Monitor for hypotension when Zanaflex is used in patients receiving concurrent antihypertensive therapy. It is not recommended that Zanaflex be used with other α 2-adrenergic agonists. Clinically significant hypotension (decreases in both systolic and diastolic pressure) has been reported with concomitant administration of tizanidine and strong CYP1A2 inhibitors [see Clinical Pharmacology ( 12.3)] . Therefore, concomitant use of Zanaflex with strong CYP1A2 inhibitors is contraindicated [see Contraindications ( 4) and Drug Interactions ( 7.1)] .
5.2 Liver Injury
Zanaflex may cause hepatocellular liver injury. Liver function test abnormality and hepatotoxicity have been observed with Zanaflex [see Adverse Reactions ( 6.1, 6.2)] . Monitoring of aminotransferase levels is recommended at baseline and 1 month after maximum dose is achieved, or if hepatic injury is suspected [see Dosage and Administration ( 2.1) and Use in Specific Populations ( 8.7)] .
5.3 Sedation
Zanaflex can cause sedation, which may interfere with everyday activity. In the multiple dose studies of Zanaflex, the prevalence of patients with sedation peaked following the first week of titration and then remained stable for the duration of the maintenance phase of the study [see Adverse Reactions ( 6.1)] . The CNS depressant effects of Zanaflex with alcohol and other CNS depressants (e.g., benzodiazepines, opioids, tricyclic antidepressants) may be additive [see Drug Interactions ( 7.4)] . Monitor patients who take Zanaflex with another CNS depressant for symptoms of excess sedation.
5.4 Hallucinosis/Psychotic-Like Symptoms
Zanaflex use has been associated with hallucinations. Formed, visual hallucinations or delusions were reported in 5 of 170 patients (3%) in two North American controlled clinical studies. Most of the patients were aware that the events were unreal. One patient developed psychosis in association with the hallucinations. One patient among these 5 continued to have problems for at least 2 weeks following discontinuation of tizanidine. Hallucinations have also been reported with tizanidine use in the postmarketing setting. Consider discontinuing Zanaflex in patients who develop hallucinations.
5.5 Hypersensitivity Reactions
Zanaflex can cause anaphylaxis. Signs and symptoms of hypersensitivity, including respiratory compromise, urticaria, and angioedema of the throat and tongue, have been reported. Zanaflex is contraindicated in patients with a history of hypersensitivity reactions to tizanidine [see Contraindications ( 4)] .
5.6 Withdrawal Adverse Reactions
Zanaflex can cause withdrawal adverse reactions, which include rebound hypertension, tachycardia, and hypertonia. To minimize the risk of these reactions, particularly in patients who have been receiving high doses of Zanaflex (20 to 28 mg daily) for long periods of time (9 weeks or more) or who may be on concomitant treatment with narcotics, the Zanaflex dosage should be decreased slowly [see Dosage and Administration ( 2.5)] .
-
6 ADVERSE REACTIONS
The following clinically significant adverse reactions are described elsewhere in other sections of the prescribing information:
- Hypotension [see Warnings and Precautions ( 5.1)]
- Liver Injury [see Warnings and Precautions ( 5.2)]
- Sedation [see Warnings and Precautions ( 5.3)]
- Hallucinosis/Psychotic-Like Symptoms [see Warnings and Precautions ( 5.4)]
- Hypersensitivity Reactions [see Warnings and Precautions ( 5.5)]
- Withdrawal Adverse Reactions [see Warnings and Precautions ( 5.6)]
6.1 Clinical Trials Experience
Because clinical studies are conducted under widely varying conditions, adverse reaction rates observed in the clinical studies of a drug cannot be directly compared to rates in the clinical studies of another drug and may not reflect the rates observed in clinical practice.
The safety of Zanaflex has been evaluated in three double-blind, randomized, placebo-controlled clinical studies [see Clinical Studies ( 14)] . Two studies were conducted in patients with multiple sclerosis and one in patients with spinal cord injury. Each study had a 13-week active treatment period which included a 3-week titration phase to the maximum tolerated dose up to 36 mg/day in three divided doses, a 9-week plateau phase where the dose of tizanidine was held constant and a 1-week dose tapering period. In all, 264 patients received tizanidine and 261 patients received placebo. Across the three studies approximately 51% of patients were women, and the median dose during the plateau phase ranged from 20 to 28 mg/day.
The most common adverse reactions (>10% of patients treated with Zanaflex) reported in multiple dose, placebo-controlled clinical studies involving 264 patients with spasticity were dry mouth, somnolence/sedation, asthenia (weakness, fatigue and/or tiredness), and dizziness. Three-quarters of the patients rated the reactions as mild to moderate and one-quarter of the patients rated the reactions as being severe. These adverse reactions appeared to be dose related.
Table 1lists adverse reactions that were reported in greater than 2% of patients in three multiple dose, placebo-controlled studies who received Zanaflex where the frequency in the Zanaflex group was greater than the placebo group.
Table 1: Multiple Dose, Placebo-Controlled Studies-Adverse Reactions Reported in >2% of Patients Treated with Zanaflex Tablets and Incidence Greater than Placebo - * includes weakness, fatigue, and/or tiredness
Adverse Reaction
Placebo
N = 261
%Zanaflex Tablet
N = 264
%Dry mouth
10
49
Somnolence
10
48
Asthenia *
16
41
Dizziness
4
16
UTI
7
10
Infection
5
6
Liver test abnormality
2
6
Constipation
1
4
Vomiting
0
3
Speech disorder
0
3
Amblyopia (blurred vision)
<1
3
Urinary frequency
2
3
Flu syndrome
2
3
Dyskinesia
0
3
Nervousness
<1
3
Pharyngitis
1
3
Rhinitis
2
3
In the single dose, placebo-controlled study involving 142 patients with spasticity due to multiple sclerosis (Study 1) [see Clinical Studies ( 14)] , the patients were specifically asked if they had experienced any of the four most common adverse reactions: dry mouth, somnolence (drowsiness), asthenia (weakness, fatigue and/or tiredness), and dizziness. In addition, hypotension and bradycardia were observed. The occurrence of these reactions is summarized in Table 2. Other events were, in general, reported at a rate of 2% or less.
Table 2: Single Dose, Placebo-Controlled Study-Common Adverse Reactions Reported - * includes weakness, fatigue, and/or tiredness
Adverse Reaction
Placebo
N = 48
%Zanaflex Tablet,
8mg, N = 45
%Zanaflex Tablet,
16 mg, N = 49
%Somnolence
31
78
92
Dry mouth
35
76
88
Asthenia *
40
67
78
Dizziness
4
22
45
Hypotension
0
16
33
Bradycardia
0
2
10
6.2 Postmarketing Experience
The following adverse reactions have been identified during post approval use of Zanaflex. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Cardiac Disorders: Ventricular tachycardia, decreased blood pressure
Hepatobiliary Disorders: Hepatotoxicity [see Warnings and Precautions ( 5.2)] , hepatitis
Musculoskeletal and Connective Tissue Disorders: arthralgia
Nervous System Disorders: Convulsion, paresthesia, tremor, muscle spasms
Psychiatric Disorders: Hallucinations [see Warnings and Precautions ( 5.4)] , depression
Skin and Subcutaneous Tissue Disorders: Stevens Johnson Syndrome, anaphylactic reaction [see Warnings and Precautions ( 5.5)] , exfoliative dermatitis, rash
-
7 DRUG INTERACTIONS
7.1 Strong CYP1A2 Inhibitors
Concomitant use of Zanaflex with strong cytochrome P450 1A2 (CYP1A2) inhibitors (e.g., fluvoxamine, ciprofloxacin) is contraindicated. Changes in pharmacokinetics of tizanidine when administered with a strong CYP1A2 inhibitor resulted in significantly decreased blood pressure, increased drowsiness, and increased psychomotor impairment [see Contraindications ( 4) and Clinical Pharmacology ( 12.3)] .
7.2 Moderate or Weak CYP1A2 Inhibitors
Concomitant use of Zanaflex with moderate or weak CYP1A2 inhibitors (e.g., zileuton, antiarrhythmics [amiodarone, mexiletine, propafenone, and verapamil], cimetidine, famotidine, oral contraceptives, acyclovir, and ticlopidine) should be avoided. If concomitant use is clinically necessary, and adverse reactions such as hypotension, bradycardia, or excessive drowsiness occur, reduce Zanaflex dosage or discontinue Zanaflex therapy [see Clinical Pharmacology ( 12.3)] .
7.3 Oral Contraceptives
Concomitant use of Zanaflex with oral contraceptives is not recommended. However, if concomitant use is clinically necessary and adverse reactions such as hypotension, bradycardia, or excessive drowsiness occur, reduce or discontinue Zanaflex therapy [see Clinical Pharmacology ( 12.3)] .
7.4 Alcohol and Other CNS Depressants
Alcohol increases the exposure of tizanidine after administration of Zanaflex. This was associated with an increase in adverse reactions of Zanaflex.
Concomitant use of Zanaflex with CNS depressants (e.g., alcohol, benzodiazepines, opioids, tricyclic antidepressants) may cause additive CNS depressant effects, including sedation. Monitor patients who take Zanaflex with another CNS depressant for symptoms of excess sedation [see Clinical Pharmacology ( 12.3)] .
7.5 α 2-Adrenergic Agonists
Concomitant use of Zanaflex with other α2-adrenergic agonists is not recommended because hypotensive effects may be cumulative [see Warnings and Precautions ( 5.1)] .
7.6 Antihypertensive Medications
Concomitant use of Zanaflex with antihypertensive medications may cause additive hypotensive effects [see Warnings and Precautions ( 5.1)] . Monitor patients who take Zanaflex with antihypertensive medications for hypotension.
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
There are no adequate data on the developmental risk associated with use of Zanaflex in pregnant women. In animal studies, administration of tizanidine during pregnancy resulted in developmental toxicity (embryofetal and postnatal offspring mortality and growth deficits) at doses less than those used clinically, which were not associated with maternal toxicity (see Animal Data).
In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% - 4% and 15% - 20%, respectively. The background risk of major birth defects and miscarriage for the indicated population is unknown.
Data
Animal Data
Oral administration of tizanidine (0.3 to 100 mg/kg/day) to pregnant rats during the period of organogenesis resulted in embryofetal and postnatal offspring mortality and reductions in body weight at doses of 30 mg/kg/day and above. Maternal toxicity was observed at the highest dose tested. The no-effect dose for embryofetal developmental toxicity in rats (3 mg/kg/day) is similar to the maximum recommended human dose (MRHD) of 36 mg/day on a body surface area (mg/m 2) basis.
Oral administration of tizanidine (1 to 100 mg/kg/day) to pregnant rabbits during the period of organogenesis resulted in embryofetal and postnatal offspring mortality at all doses. Maternal toxicity was observed at the highest dose tested. Oral administration of tizanidine (10 and 30 mg/kg/day) during the perinatal period of pregnancy (2-6 days prior to delivery) resulted in increased postnatal offspring mortality at both doses. A no-effect dose for embryofetal developmental toxicity in rabbit was not identified. The lowest dose tested (1 mg/kg/day) is less than the MRHD on a mg/m 2basis.
In a pre- and postnatal development study in rats, oral administration of tizanidine (3 to 30 mg/kg/day) resulted in increased postnatal offspring mortality. A no-effect dose for pre- and postnatal developmental toxicity was not identified. The lowest dose tested (3 mg/kg/day) is similar to the MRHD on a mg/m 2basis, respectively.
8.2 Lactation
Risk Summary
There are no data on the presence of tizanidine in human milk, the effects on the breastfed infant, or the effects on human milk production. Animal studies have reported the presence of tizanidine in the milk of lactating animals.
The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for Zanaflex and any potential adverse effects on the breastfed infant from Zanaflex or from the underlying maternal condition.
8.3 Females and Males of Reproductive Potential
There are no adequate and well-controlled studies in humans on the effect of Zanaflex on female or male reproductive potential. Oral administration of tizanidine to male and female rats resulted in adverse effects on fertility [see Nonclinical Toxicology ( 13.1)].
8.4 Pediatric Use
Safety and effectiveness in pediatric patients have not been established.
Juvenile Animal Toxicity Data
Oral administration of tizanidine (0, 1, 3, and 10 mg/kg/day) to juvenile rats from postnatal day (PND) 7 through PND 70 resulted in delayed sexual maturation in males at all doses, reduced body weight gain, delayed sexual maturation in females, and bilateral corneal crystals at the mid and high doses. Corneal crystals were still observed at the mid and high doses after a three-week recovery period. Neurobehavioral deficits were observed on a learning and memory task at the high dose. A no-effect dose for adverse effects on postnatal development not identified.
8.5 Geriatric Use
Zanaflex is known to be substantially excreted by the kidney, and the risk of adverse reactions to this drug may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function.
Clinical studies of Zanaflex did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently than younger subjects. Pharmacokinetic data showed that younger subjects cleared tizanidine faster than the elderly subjects [see Clinical Pharmacology ( 12.3)] . In elderly patients with renal insufficiency (creatinine clearance <25 mL/min), tizanidine clearance is reduced compared to healthy elderly subjects; this would be expected to lead to a longer duration of clinical effect. During titration, the individual doses should be reduced. If higher doses are required, individual doses rather than dosing frequency should be increased. Monitor elderly patients because they may have an increased risk for adverse reactions associated with Zanaflex.
8.6 Renal Impairment
In patients with renal insufficiency (creatinine clearance <25 mL/min), clearance of tizanidine was reduced [see Clinical Pharmacology ( 12.3)] . In these patients, dosage reduction is recommended [see Dosage and Administration ( 2.3)] .Because the risk of adverse reactions to Zanaflex may be greater in patients with impaired renal function, monitor these patients closely for the onset or increase in severity of common adverse reactions [see Adverse Reactions ( 6.1)]
8.7 Hepatic Impairment
Zanaflex should be used with caution in patients with hepatic impairment. The influence of hepatic impairment on the pharmacokinetics of tizanidine has not been evaluated. Because tizanidine is extensively metabolized in the liver, hepatic impairment would be expected to have significant effects on pharmacokinetics of tizanidine. [see Warnings and Precautions ( 5.2), and Clinical Pharmacology ( 12.3)] . In patients with hepatic impairment, dosage reduction is recommended [see Dosage and Administration ( 2.4)]
-
9 DRUG ABUSE AND DEPENDENCE
9.2 Abuse
Abuse is the intentional, non-therapeutic use of a drug, even once, for its desirable psychological or physiological effects. Abuse potential was not evaluated in human studies. Rats were able to distinguish tizanidine from saline in a standard discrimination paradigm, after training, but failed to generalize the effects of morphine, cocaine, diazepam, or phenobarbital to tizanidine.
9.3 Dependence
Physical dependence is a state that develops as a result of physiological adaptation in response to repeated drug use, manifested by withdrawal signs and symptoms after abrupt discontinuation or a significant dose reduction of a drug. Tizanidine is closely related to clonidine, which is often abused in combination with narcotics and is known to cause symptoms of rebound upon abrupt withdrawal. Cases of rebound symptoms on sudden withdrawal of tizanidine have been reported. The case reports suggest that these patients were also misusing narcotics. Withdrawal symptoms included hypertension, tachycardia, hypertonia, tremor, and anxiety. Withdrawal symptoms are more likely to occur in cases where high doses are used, especially for prolonged periods, or with concomitant use of narcotics. If therapy needs to be discontinued, the dose should be decreased slowly to minimize the risk of withdrawal symptoms [see Dosage and Administration ( 2.5)] .
Monkeys were shown to self-administer tizanidine in a dose-dependent manner, and abrupt cessation of tizanidine produced transient signs of withdrawal at doses >35 times the maximum recommended human dose on a mg/m 2basis. These transient withdrawal signs (increased locomotion, body twitching, and aversive behavior toward the observer) were not reversed by naloxone administration.
-
10 OVERDOSAGE
A review of the safety surveillance database revealed cases of intentional and accidental Zanaflex overdose. Some of the cases resulted in fatality and many of the intentional overdoses were with multiple drugs, including CNS depressants. The clinical manifestations of tizanidine overdose were consistent with its known pharmacology. In the majority of cases, a decrease in sensorium was observed including lethargy, somnolence, confusion, and coma. Depressed cardiac function is also observed including most often bradycardia and hypotension. Respiratory depression is another common feature of tizanidine overdose.
Should overdose occur, ensure the adequacy of an airway and monitor cardiovascular and respiratory function. Dialysis is not likely to be an efficient method of removing tizanidine from the body [see Description ( 11)] . In general, symptoms resolve within one to three days following discontinuation of tizanidine and administration of appropriate therapy. Because of the similar mechanism of action, symptoms and management of tizanidine overdose are similar to that following clonidine overdose. For the most recent information concerning the management of overdose, contact a poison control center.
-
11 DESCRIPTION
Zanaflex ®contains tizanidine hydrochloride as the active ingredient, which is a central alpha 2-adrenergic agonist. Its chemical name is 5-chloro-4-(2-imidazolin-2-ylamino)-2,1,3-benzothiadiazole monohydrochloride. It has a molecular formula of C 9H 8ClN 5S-HCl and a molecular weight of 290.2. Its structural formula is:
Tizanidine hydrochloride is a white to off-white, fine crystalline powder, which is odorless or with a faint characteristic odor. Tizanidine hydrochloride is slightly soluble in water and methanol; solubility in water decreases as the pH increases.
Zanaflex capsules are for oral administration and contain 2, 4, or 6 mg tizanidine (equivalent to 2.29 mg, 4.58 mg, and 6.87 mg tizanidine hydrochloride, respectively), and the inactive ingredients colorants, gelatin, hypromellose, silicon dioxide, sugar spheres, and titanium dioxide.
Zanaflex tablets are for oral administration and contain 4 mg tizanidine (equivalent to 4.58 mg tizanidine hydrochloride), and the inactive ingredients anhydrous lactose, colloidal silicon dioxide, microcrystalline cellulose, and stearic acid.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Tizanidine is a central alpha-2-adrenergic receptor agonist and presumably reduces spasticity by increasing presynaptic inhibition of motor neurons. The effects of tizanidine are greatest on polysynaptic pathways. The overall effect of these actions is thought to reduce facilitation of spinal motor neurons.
12.2 Pharmacodynamics
The CNS depressant effects of tizanidine and alcohol are additive [see Warnings and Precautions ( 5.3) and Drug Interactions ( 7.4)]
12.3 Pharmacokinetics
Tizanidine has linear pharmacokinetics over the doses studied in clinical development [1 mg (half the recommended dosage) to 20 mg].
Zanaflex capsules and tablets are bioequivalent to each other under fasting conditions, but not under fed conditions (see Absorption, Effect of Food).
Absorption
Following oral administration, tizanidine is essentially completely absorbed. The absolute oral bioavailability of tizanidine is approximately 40% (CV = 24%), due to extensive first-pass hepatic metabolism.
Effect of Food
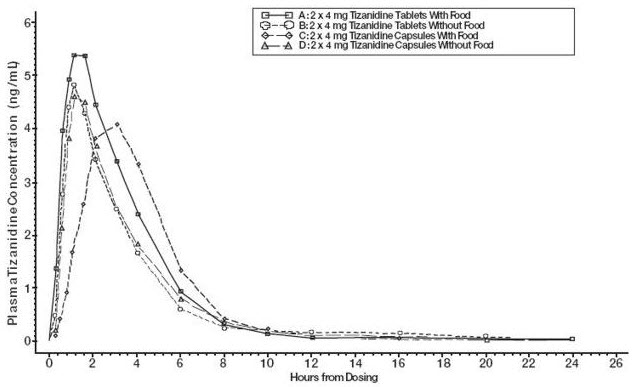
There are pharmacokinetic differences between Zanaflex capsules and Zanaflex tablets with respect to administration with food.
A single dose of either two 4 mg tablets or two 4 mg capsules was administered under fed and fasting conditions in an open-label, four-period, randomized crossover study in 96 volunteers, of whom 81 were eligible for the statistical analysis. Pharmacokinetics under fed conditions were different than under fasting conditions and vary by dosage form.
Tablets or Capsules - Fasting
- T maxwas 1.0 hours after dosing
- T 1/2was approximately 2 hours.
Tablets - Fed
- Mean C maxwas increased by approximately 30%
- Median T maxwas increased by 25 minutes, to 1 hour and 25 minutes.
- Extent of absorption was increased approximately 30%
Capsules - Fed
- Mean C maxwas decreased by 20% (consequently, approximately 66% the Cmax for the tablet when administered with food)
- Median T maxwas increased 2 to 3 hours
- Extent of absorption was increased approximately 10% (consequently, approximately 80% of the amount absorbed from the tablet administered with food)
Capsule Content Sprinkled on Applesauce
Compared to administration of an intact capsule while fasting:
- C maxand AUC was increased 15%–20%
- T maxwas decreased 15 minutes
Figure 1: Mean Tizanidine Concentration vs. Time Profiles For Zanaflex Tablets and Capsules (2 × 4 mg) Under Fasted and Fed Conditions
Distribution
Tizanidine is extensively distributed throughout the body with a mean steady state volume of distribution of 2.4 L/kg (CV = 21%) following intravenous administration in healthy adult volunteers. Tizanidine is approximately 30% bound to plasma proteins.
Elimination
Metabolism
Tizanidine has a half-life of approximately 2.5 hours (CV=33%). Approximately 95% of an administered dose is metabolized. The primary cytochrome P450 isoenzyme involved in tizanidine metabolism is CYP1A2. Tizanidine metabolites are not known to be active; their half-lives range from 20 to 40 hours.
Excretion
Following single and multiple oral dosing of 14C-tizanidine, an average of 60% and 20% of total radioactivity was recovered in the urine and feces, respectively.
Specific Populations
Geriatric Patients
No specific pharmacokinetic study was conducted to investigate age effects. Cross study comparison of pharmacokinetic data following single dose administration of 6 mg Zanaflex showed that younger subjects cleared the drug four times faster than the elderly subjects [see Use in Specific Populations ( 8.5)] .
Patients with Hepatic Impairment
The influence of hepatic impairment on the pharmacokinetics of tizanidine has not been evaluated. Because tizanidine is extensively metabolized in the liver, hepatic impairment would be expected to have significant effects on pharmacokinetics of tizanidine [see Use in Specific Populations ( 8.7)] .
Patients with Renal Impairment
Tizanidine clearance is reduced by more than 50% in elderly patients with renal insufficiency (creatinine clearance <25 mL/min) compared to healthy elderly subjects; this would be expected to lead to a longer duration of clinical effect [see Use in Specific Populations ( 8.6)] .
Gender Effects
No specific pharmacokinetic study was conducted to investigate gender effects. Retrospective analysis of pharmacokinetic data following single and multiple dose administration of 4 mg Zanaflex, however, showed that gender had no effect on the pharmacokinetics of tizanidine.
Drug Interactions
CYP1A2 Inhibitors
The effects of coadministration of fluvoxamine or ciprofloxacin, both strong CYP1A2 inhibitors, on the pharmacokinetics of a single 4 mg dose of Zanaflex was studied in 10 healthy subjects. The Cmax, AUC, and half-life of tizanidine increased by 12-fold, 33-fold, and 3-fold, respectively, with coadministration of fluvoxamine. The C maxand AUC of tizanidine increased by 7-fold and 10-fold, respectively, with coadministration of ciprofloxacin [see Contraindications ( 4)] .
There have been no clinical studies evaluating the effects of other CYP1A2 inhibitors on tizanidine [see Drug Interactions ( 7.2)] .
In vitro studies of cytochrome P450 isoenzymes using human liver microsomes indicate that neither tizanidine nor the major metabolites are likely to affect the metabolism of other drugs metabolized by cytochrome P450 isoenzymes.
Oral Contraceptives
No specific pharmacokinetic study was conducted to investigate interaction between oral contraceptives and Zanaflex. Retrospective analysis of population pharmacokinetic data following single and multiple dose administration of 4 mg Zanaflex, however, showed that women concurrently taking oral contraceptives had 50% lower clearance of tizanidine compared to women not on oral contraceptives [see Drug Interactions ( 7.3))] .
Acetaminophen
Tizanidine delayed the T maxof acetaminophen by 16 minutes. Acetaminophen did not affect the pharmacokinetics of tizanidine.
Alcohol
Alcohol increased the AUC and C maxof tizanidine by approximately 20% and 15%, respectively [see Drug Interactions ( 7.4)] .
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Tizanidine was administered to mice for 78 weeks at oral doses up to 16 mg/kg/day, which is 2 times the maximum recommended human dose (MRHD) of 36 mg/day on a body surface area (mg/m 2) basis. Tizanidine was administered to rats for 104 weeks at oral doses up to 9 mg/kg/day, which is 2.5 times the MRHD on a mg/m 2basis. There was no increase in tumors in either species.
Mutagenesis
Tizanidine was negative in in vitro(bacterial reverse mutation [Ames], mammalian gene mutation, and chromosomal aberration test in mammalian cells) and in vivo(bone marrow micronucleus, and cytogenetics) assay.
Impairment of Fertility
Oral administration of tizanidine to rats prior to and during mating and continuing during early pregnancy in females resulted in reduced fertility in male and female rats at doses of 30 and 10 mg/kg/day, respectively. No effect on fertility was observed at doses of 10 (male) and 3 (female) mg/kg/day, which are approximately 3 times and similar to the MRHD, respectively, on a mg/m 2basis.
-
14 CLINICAL STUDIES
The efficacy of Zanaflex for the treatment of spasticity was demonstrated in two adequate and well-controlled studies in patients with multiple sclerosis or spinal cord injury (Studies 1 and 2).
Single-Dose Study in Patients with Multiple Sclerosis with Spasticity
In Study 1, 140 patients with spasticity caused by multiple sclerosis were randomized to receive single oral doses of 8 mg or 16 mg of Zanaflex, or placebo. Patients and assessors were blinded to treatment assignment and efforts were made to reduce the likelihood that assessors would become aware indirectly of treatment assignment (e.g., they did not provide direct care to patients and were prohibited from asking questions about side effects).
Response was assessed by physical examination; muscle tone was rated on a 5-point scale (Ashworth score) as follows:
- 0 = normal muscle tone
- 1 = slight spastic catch
- 2 = more marked muscle resistance
- 3 = considerable increase in tone, making passive movement difficult
- 4 = a muscle immobilized by spasticity
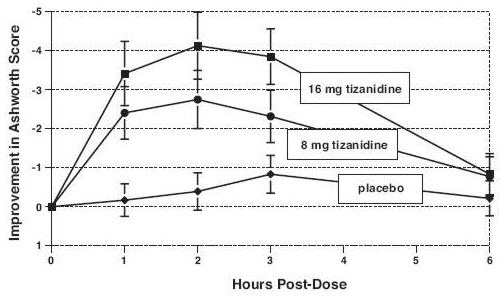
Spasm counts were also collected. Assessments were made at 1, 2, 3 and 6 hours after treatment. A statistically significant reduction of the Ashworth score for Zanaflex compared to placebo was detected at 1, 2, and 3 hours after treatment. Figure 2below shows a comparison of the mean change in muscle tone from baseline as measured by the Ashworth scale. The greatest reduction in muscle tone was 1 to 2 hours after treatment. By 6 hours after treatment, muscle tone in the 8 mg and 16 mg Zanaflex groups was indistinguishable from muscle tone in patients who received placebo. Within a given patient, improvement in muscle tone was correlated with plasma concentration. Plasma concentrations were variable from patient to patient at a given dose. Although 16 mg produced a larger effect, adverse reactions including hypotension were more common and more severe than in the 8 mg group. There were no differences in the number of spasms occurring in each group.
Figure 2: Single Dose Study—Mean Change in Muscle Tone from Baseline as Measured by the Ashworth Scale ± 95% Confidence Interval (A Negative Ashworth Score Signifies an Improvement in Muscle Tone from Baseline)
Seven-Week Study in Patients with Spinal Cord Injury with Spasticity
In a 7-week study (Study 2), 118 patients with spasticity secondary to spinal cord injury were randomized to either placebo or Zanaflex. Steps similar to those taken in the first study were employed to ensure the integrity of blinding.
Patients were titrated over 3 weeks up to a maximum tolerated dose or 36 mg daily given in three unequal doses (e.g., 10 mg given in the morning and afternoon and 16 mg given at night). Patients were then maintained on their maximally tolerated dose for 4 additional weeks (i.e., maintenance phase). Throughout the maintenance phase, muscle tone was assessed on the Ashworth scale within a period of 2.5 hours following either the morning or afternoon dose. The number of daytime spasms was recorded daily by patients.
At endpoint (the protocol-specified time of outcome assessment), there was a statistically significant reduction in muscle tone and frequency of spasms in the Zanaflex treated group compared to placebo. The reduction in muscle tone was not associated with a reduction in muscle strength (a desirable outcome), but also did not lead to any consistent advantage of Zanaflex treated patients on measures of activities of daily living. Figure 3below shows a comparison of the mean change in muscle tone from baseline as measured by the Ashworth scale.
Figure 3: Seven Week Study-Mean Change in Muscle Tone 0.5–2.5 Hours After Dosing as Measured by the Ashworth Scale ± 95% Confidence Interval (A Negative Ashworth Score Signifies an Improvement in Muscle Tone from Baseline)
-
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 How Supplied
Zanaflex Capsules
Zanaflex (tizanidine) capsules are two-piece hard gelatin shells containing 2 mg, 4 mg, or 6 mg tizanidine in bottles of 150 capsules available as follows.
- The 2 mg capsules have a light blue opaque body with a light blue opaque cap with “2 MG” printed on the cap: NDC: 83107-001-15
- The 4 mg capsules have a white opaque body with a blue opaque cap with “4 MG” printed on the cap: NDC: 83107-002-15
- The 6 mg capsules have a blue opaque body with a white stripe and blue opaque cap with “6 MG” printed on the capsules: NDC: 83107-003-15
Zanaflex Tablets
Zanaflex (tizanidine) tablets are uncoated containing 4 mg tizanidine in bottles of 150 tablets. The tablets have a quadrisecting score on one side and are debossed with “A594” on the other side: NDC: 83107-004-15.
-
17 PATIENT COUNSELING INFORMATION
Serious Drug Interactions
Advise patients they should not take Zanaflex if they are taking fluvoxamine or ciprofloxacin because of the increased risk of serious adverse reactions including severe lowering of blood pressure and sedation. Instruct patients to inform their healthcare providers when they start or stop taking any medication because of the risks associated with interaction between Zanaflex and other medicines [see Contraindications ( 4) and Drug Interactions ( 7)]. .
Zanaflex Dosing and Administration
Tell patients to take Zanaflex exactly as prescribed (consistently either with or without food) and not to switch between tablets and capsules [see Dosage and Administration ( 2)] . Inform patients that they should not take more Zanaflex than prescribed because of the risk of adverse events at single doses greater than 8 mg or total daily doses greater than 36 mg. Tell patients that they should not suddenly discontinue Zanaflex, because rebound hypertension and tachycardia may occur [see Warnings and Precautions ( 5.6)].
Hypotension
Warn patients that they may experience hypotension and to be careful when changing from a lying or sitting to a standing position [see Warnings and Precautions ( 5.1)] .
Sedation
Tell patients that Zanaflex may cause them to become sedated or somnolent and they should be careful when performing activities that require alertness, such as driving a vehicle or operating machinery [see Warnings and Precautions ( 5.3)] . Tell patients that the sedation may be additive when Zanaflex is taken in conjunction with drugs (baclofen, benzodiazepines) or substances (e.g., alcohol) that act as CNS depressants.
Remind patients that if they depend on their spasticity to sustain posture and balance in locomotion, or whenever spasticity is utilized to obtain increased function, that Zanaflex decreases spasticity and caution should be used.
Hypersensitivity Reactions
Inform patients of the signs and symptoms of severe allergic reactions and instruct them to discontinue Zanaflex and seek immediate medical care should these signs and symptoms occur [see Warnings and Precautions ( 5.5)] .
Zanaflex ®capsules is a registered trademark of Legacy Pharma Inc. Zanaflex ®tablets is a registered trademark of Legacy Pharma Inc.
Manufactured for:
Legacy Pharma Inc.
Georgetown, Grand Cayman
KY1-9012
- PRINCIPAL DISPLAY PANEL
- PRINCIPAL DISPLAY PANEL
- PRINCIPAL DISPLAY PANEL
- PRINCIPAL DISPLAY PANEL
-
INGREDIENTS AND APPEARANCE
ZANAFLEX
tizanidine hydrochloride capsuleProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 83107-001 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength TIZANIDINE HYDROCHLORIDE (UNII: B53E3NMY5C) (TIZANIDINE - UNII:6AI06C00GW) TIZANIDINE 2 mg Inactive Ingredients Ingredient Name Strength SILICON DIOXIDE (UNII: ETJ7Z6XBU4) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) GELATIN, UNSPECIFIED (UNII: 2G86QN327L) HYPROMELLOSE, UNSPECIFIED (UNII: 3NXW29V3WO) Product Characteristics Color blue (light blue opaque) Score no score Shape CAPSULE Size 16mm Flavor Imprint Code 2;MG Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 83107-001-15 150 in 1 BOTTLE; Type 0: Not a Combination Product 08/01/2018 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA021447 08/01/2018 ZANAFLEX
tizanidine hydrochloride capsuleProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 83107-002 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength TIZANIDINE HYDROCHLORIDE (UNII: B53E3NMY5C) (TIZANIDINE - UNII:6AI06C00GW) TIZANIDINE 4 mg Inactive Ingredients Ingredient Name Strength SILICON DIOXIDE (UNII: ETJ7Z6XBU4) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) GELATIN, UNSPECIFIED (UNII: 2G86QN327L) HYPROMELLOSE, UNSPECIFIED (UNII: 3NXW29V3WO) Product Characteristics Color white (white opaque) , blue (blue opaque) Score no score Shape CAPSULE Size 16mm Flavor Imprint Code 4;MG Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 83107-002-15 150 in 1 BOTTLE; Type 0: Not a Combination Product 08/01/2018 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA021447 08/01/2018 ZANAFLEX
tizanidine hydrochloride capsuleProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 83107-003 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength TIZANIDINE HYDROCHLORIDE (UNII: B53E3NMY5C) (TIZANIDINE - UNII:6AI06C00GW) TIZANIDINE 6 mg Inactive Ingredients Ingredient Name Strength SILICON DIOXIDE (UNII: ETJ7Z6XBU4) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) GELATIN, UNSPECIFIED (UNII: 2G86QN327L) HYPROMELLOSE, UNSPECIFIED (UNII: 3NXW29V3WO) Product Characteristics Color blue (blue opaque body with white stripe) , blue (blue opaque) Score no score Shape CAPSULE Size 18mm Flavor Imprint Code 6;MG Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 83107-003-15 150 in 1 BOTTLE; Type 0: Not a Combination Product 08/01/2018 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA021447 08/01/2018 ZANAFLEX
tizanidine hydrochloride tabletProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 83107-004 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength TIZANIDINE HYDROCHLORIDE (UNII: B53E3NMY5C) (TIZANIDINE - UNII:6AI06C00GW) TIZANIDINE 4 mg Inactive Ingredients Ingredient Name Strength SILICON DIOXIDE (UNII: ETJ7Z6XBU4) STEARIC ACID (UNII: 4ELV7Z65AP) MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) ANHYDROUS LACTOSE (UNII: 3SY5LH9PMK) Product Characteristics Color white Score 4 pieces Shape ROUND Size 9mm Flavor Imprint Code A594 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 83107-004-15 150 in 1 BOTTLE; Type 0: Not a Combination Product 08/01/2018 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA020397 08/01/2018 Labeler - Legacy Pharma USA, Inc. (118831776)


Trademark Results [Zanaflex]
Mark Image Registration | Serial | Company Trademark Application Date |
|---|---|
 ZANAFLEX 75186534 2383531 Live/Registered |
COVIS PHARMA B.V. 1996-10-15 |
 ZANAFLEX 74400930 1906277 Dead/Cancelled |
ELAN PHARMACEUTICALS, INC. 1993-06-09 |
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.