BALFAXAR (prothrombin complex concentrate- human powder, for solution
Balfaxar by
Drug Labeling and Warnings
Balfaxar by is a Other medication manufactured, distributed, or labeled by Octapharma USA Inc. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use BALFAXAR safely and effectively. See full prescribing information for BALFAXAR.
BALFAXAR (prothrombin complex concentrate, human-lans)
lyophilized powder for solution, for intravenous use
Initial U.S. Approval: 2023WARNING: ARTERIAL and VENOUS THROMBOEMBOLIC COMPLICATIONS
See full prescribing information for complete boxed warning .
Patients being treated with Vitamin K antagonists (VKA) therapy have underlying disease states that predispose them to thromboembolic events. Potential benefits of reversing VKA should be weighed against the potential risks of thromboembolic events, especially in patients with the history of a thromboembolic event. Resumption of anticoagulation should be carefully considered as soon as the risk of thromboembolic events outweighs the risk of acute bleeding.
Both fatal and non-fatal arterial and venous thromboembolic complications have been reported with BALFAXAR in clinical trials and post marketing surveillance. Monitor patients receiving BALFAXAR for signs and symptoms of thromboembolic events. ( 5.2 )
BALFAXAR may not be suitable in patients with thromboembolic events in the prior 3 months. ( 5.2 )
INDICATIONS AND USAGE
BALFAXAR (prothrombin complex concentrate, human-lans) is a blood coagulation factor replacement product indicated for the urgent reversal of acquired coagulation factor deficiency induced by Vitamin K antagonist (VKA, e.g., warfarin) therapy in adult patients with need for an urgent surgery/invasive procedure. ( 1 )
DOSAGE AND ADMINISTRATION
For intravenous use after reconstitution only.
BALFAXAR dosing should be individualized based on the patient’s baseline International Normalized Ratio (INR) value, and body weight. ( 2.1 )
Administer Vitamin K concurrently to patients receiving BALFAXAR to maintain factor levels once the effects of BALFAXAR have diminished. ( 14 )
The safety and effectiveness of repeat dosing have not been established and it is not recommended. ( 2.1 )
Administer reconstituted BALFAXAR at a rate of 0.12 mL/kg/min (~3 units/kg/min) up to a maximum rate of 8.4 mL/min (~210 units/min). ( 2.3 )
Pre-treatment INR 2-< 4 4-6 > 6 Dose# of BALFAXAR (units† of Factor IX) / kg body weight 25 35 50 Maximum dose‡ (units of Factor IX) Not to exceed 2500 Not to exceed 3500 Not to exceed 5000 # Dosing is based on body weight. Dose based on actual potency is stated on the vial, which will vary from 20-32 Factor IX units/mL after reconstitution.
The actual potency for a 500 unit vial ranges from 400-640 units/vial. The actual potency for a 1000 unit vial ranges from 800-1280 units/vial.
† Units refer to International Units.
‡ Dose is based on body weight up to but not exceeding 100 kg. For patients weighing more than 100 kg, maximum dose should not be exceeded. ( 2.2 )
DOSAGE FORMS AND STRENGTHS
BALFAXAR is available as a white to ice-blue lyophilized powder for reconstitution for intravenous use in a single-dose vial, provided in a nominal strength of 500 Factor IX units in 20 mL reconstitution volume and 1000 Factor IX units in 40 mL reconstitution volume per vial. BALFAXAR contains the coagulation factors II, VII, IX, and X and antithrombotic Proteins C and S. ( 3 )
CONTRAINDICATIONS
WARNINGS AND PRECAUTIONS
Discontinue infusion if allergic or anaphylactic-type reactions occur. Initiate appropriate treatment. ( 5.1 )
Arterial and venous thromboembolic complications have been reported in patients receiving BALFAXAR. Monitor patients receiving BALFAXAR for signs and symptoms of thromboembolic events. ( 5.2 )
BALFAXAR is made from human plasma; therefore, may carry the risk of transmitting infectious agents, e.g., viruses, the variant Creutzfeldt-Jakob disease (vCJD) agent, and theoretically, the Creutzfeldt-Jakob disease (CJD) agent. ( 5.3 )
ADVERSE REACTIONS
The most common adverse reactions observed in ≥ 3% of subjects were procedural pain, wound complications, asthenia, anemia, dysuria, procedural vomiting and catheter site related reaction. ( 6 )
To report SUSPECTED ADVERSE REACTIONS, contact Octapharma USA Inc. at 1-866-766-4860 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
_________________________________________________________________________________________________________________________
See 17 for PATIENT COUNSELING INFORMATION.
Revised: 7/2023
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
WARNING: ARTERIAL AND VENOUS THROMBOEMBOLIC COMPLICATIONS
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Dosage
2.2 Preparation and Reconstitution
2.3 Administration
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Hypersensitivity Reactions
5.2 Thromboembolic Risk/Complications
5.3 Transmissible Infectious Agents
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
6.2 Postmarketing Experience
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.4 Pediatric Use
8.5 Geriatric Use
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
15 REFERENCES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- * Sections or subsections omitted from the full prescribing information are not listed.
- SPL UNCLASSIFIED SECTION
-
BOXED WARNING
(What is this?)
WARNING: ARTERIAL AND VENOUS THROMBOEMBOLIC COMPLICATIONS
Patients being treated with Vitamin K antagonist (VKA) therapy have underlying disease states that predispose them to thromboembolic events. Potential benefits of reversing VKA should be weighed against the potential risks of thromboembolic events, especially in patients with the history of a thromboembolic event. Resumption of anticoagulation should be carefully considered as soon as the risk of thromboembolic events outweighs the risk of acute bleeding.
- Both fatal and non-fatal arterial and venous thromboembolic complications have been reported with BALFAXAR in clinical trials and post marketing surveillance. Monitor patients receiving BALFAXAR for signs and symptoms of thromboembolic events. [see Warnings and Precautions ( 5.2 )].
- BALFAXAR may not be suitable in patients with thromboembolic events in the prior 3 months. [see Warnings and Precautions ( 5.2 )].
-
1 INDICATIONS AND USAGE
BALFAXAR (prothrombin complex concentrate, human-lans) is a blood coagulation factor replacement product indicated for the urgent reversal of acquired coagulation factor deficiency induced by Vitamin K antagonist (VKA, e.g., warfarin) therapy in adult patients with need for an urgent surgery/invasive procedure.
-
2 DOSAGE AND ADMINISTRATION
For intravenous use after reconstitution only .
2.1 Dosage
- Measurement of INR prior to treatment and close to the time of dosing is important because coagulation factors may be unstable in patients with need for an urgent surgery and other invasive procedures.
- Individualize BALFAXAR dosing based on the patient’s current pre-dose International Normalized Ratio (INR) value, and body weight (see Table 1 ).
- The actual potency per vial of Factor IX is stated on the carton. The potencies of Factors II, VII, IX and X, Proteins C and S are indicated as ranges.
- Administer Vitamin K concurrently to patients receiving BALFAXAR. Vitamin K is administered to maintain Vitamin K-dependent clotting factor levels once the effects of BALFAXAR have diminished.
- The safety and effectiveness of repeat dosing have not been established and it is not recommended.
- Dose ranging within pre-treatment INR groups has not been studied in randomized clinical trials of BALFAXAR.
Table 1 Dosage Required for Reversal of VKA Anticoagulation in Patients with Need for an Urgent Surgery/Invasive Procedure
Pre-treatment INR 2-< 4 4-6 > 6 Dose* of BALFAXAR (units † of Factor IX) / kg body weight 25 35 50 Maximum dose ‡ (units of Factor IX) Not to exceed
2500Not to exceed
3500Not to exceed
5000* Dosing is based on body weight. Dose based on actual potency is stated on the vial, which will vary from 20-32 Factor IX units/mL after reconstitution. The actual potency for a 500 unit vial ranges from 400-640 units/vial. The actual potency for a 1000 unit vial ranges from 800-1280 units/vial.
† Units refer to International Units.
‡ Dose is based on body weight up to but not exceeding 100 kg. For patients weighing more than 100 kg, maximum dose should not be exceeded.
Example dosing calculation for 80 kg patient:
For example, an 80 kg patient with a baseline of INR of 5.0, the dose would be 2,800 Factor IX units of BALFAXAR, calculated as follows based on INR range of 4-6, see Table 1 :
35 units of Factor IX/kg x 80 kg = 2,800 units of Factor IX required*
* For a vial with an actual potency of 30 units/mL Factor IX, 93 mL would be given (2,800 U/30 U per mL = 93 mL).
Monitor INR and clinical response during and after treatment. In clinical trials, BALFAXAR decreased the INR to ≤1.5 within 30 minutes in most subjects. The relationship between this or other INR values and clinical hemostasis in patients has not been established [see Clinical Studies ( 14 )] .
2.2 Preparation and Reconstitution
BALFAXAR is provided with a transfer device (Nextaro ® ) for reconstitution of the lyophilized powder in diluent (sterile Water for Injection (sWFI)).
BALFAXAR is for single dose only. Do not re-use any of the components.
Inspect all components for physical integrity prior to use. Do not use products or components that appear damaged or broken.
Reconstitute BALFAXAR using aseptic technique for the procedure described below.
The product reconstitutes quickly (1 to 5 minutes) at room temperature (20°C to 25°C; 68°F to 77°F). As BALFAXAR contains no preservatives, the solution should be administered immediately after reconstitution, or within 8 hours, provided sterility is maintained. The reconstituted solution can be stored for up to 8 hours at room temperature (20°C to 25°C; 68°F to 77°F).
Instructions for Reconstitution:
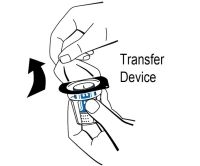
Figure 11. Ensure that the lyophilized powder and diluent vials are at room temperature (20°C to 25°C, 68°F to 77°F). This temperature should be maintained during reconstitution.
2. Remove the flip caps from the lyophilized powder and diluent vials and disinfect the rubber stoppers with an alcohol swab and allow to dry.
3. Open the transfer device package by peeling off the lid ( Figure 1 ). To maintain sterility, do not remove the transfer device from the blister package and do not touch the spike.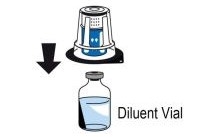
Figure 24. Place the diluent vial on an even, clean surface and hold it firmly. Without removing the blister package, place the blue part of the transfer device on top of the diluent vial and press straight and firmly down until it snaps into place ( Figure 2 ). Do not twist while attaching. 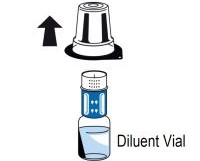
Figure 35. While holding onto the diluent vial, carefully remove the blister package from the transfer device by pulling vertically upwards. Make sure to leave the transfer device attached firmly to the diluent vial ( Figure 3 ). 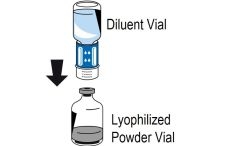
Figure 46. Place the lyophilized powder vial on an even, clean surface and hold it firmly. Take the diluent vial with the attached transfer device and turn it upside down. Place the white part of the transfer device connector on top of the powder vial and press firmly down until it snaps into place ( Figure 4 ). Do not twist while attaching. The diluent will flow automatically into the powder vial.
Note: The transfer device must be attached to the diluent vial first and then to the lyophilized powder vial. Otherwise, loss of vacuum occurs, and transfer of the diluent does not take place. If diluent is not completely transferred to the lyophilized powder vial during this process, contact your Octapharma representative.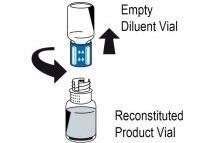
Figure 57. With both vials still attached, gently swirl the product vial until the product is fully dissolved. To avoid foam formation, do not shake the vial. BALFAXAR dissolves quickly at room temperature (20°C to 25°C; 68°F to 77°F) and is a clear solution that may be colorless to slightly blue. Unscrew the transfer device counterclockwise into two parts ( Figure 5 ). Do not touch the luer lock connector.
8. Dispose of the empty diluent vial together with the blue part of the transfer device.
Reconstituted products should be inspected visually for particulate matter. Do not use solutions that are cloudy or have deposits.
If the lyophilized powder fails to dissolve completely or an aggregate is formed, do not use the preparation.
After reconstitution, administration should begin promptly or within 8 hours, provided sterility is maintained.
If the same patient is to receive more than one vial, you may pool the contents of multiple vials, provided sterility is maintained. Use a separate unused transfer device for the reconstitution of each product vial.
2.3 Administration
BALFAXAR is for intravenous use after reconstitution only.
Do not mix with other medicinal products; administer through a separate infusion line. The infusion line may be flushed with normal saline before and after administration of BALFAXAR.
Instructions for Infusion:
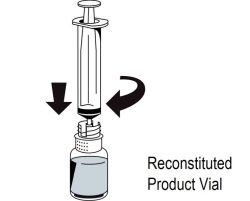
Figure 61. Attach a syringe to the luer lock outlet on the white part of the transfer device (Figure 6). 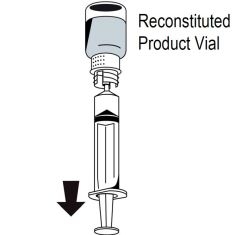
Figure 72. Turn the vial upside down and draw the solution into the syringe ( Figure 7 ). 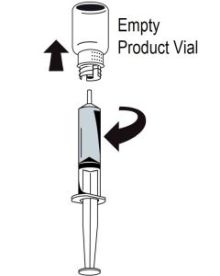
Figure 83. Once the solution has been transferred, firmly hold the barrel of the syringe (keeping the syringe plunger facing down) and remove the syringe from the transfer device ( Figure 8 ).
4. Dispose of the white part of the transfer device together with the empty vial.
5.Attach a suitable administration set to the luer adapter of the syringe.
6.Disinfect the intended injection site appropriately.
7.Administer by intravenous infusion at a rate of 0.12 mL/kg/min (~3 units/kg/min), up to a maximum rate of 8.4 mL/min (~210 units/min). No blood should enter the syringe due to the risk of fibrin clot formation.
Any unused product or waste material should be disposed of immediately in accordance with local requirements.
-
3 DOSAGE FORMS AND STRENGTHS
BALFAXAR is a sterile, white to ice-blue lyophilized powder for reconstitution for intravenous use. It is provided in a single-dose vial with a nominal strength of 500 Factor IX units in 20 mL reconstitution volume and 1000 Factor IX units in 40 mL reconstitution volume per vial. BALFAXAR contains the coagulation factors II, VII, IX, and X and antithrombotic Proteins C and S.
-
4 CONTRAINDICATIONS
- Known anaphylactic or severe systemic reactions to BALFAXAR or any of the components of the product. For a complete listing of ingredients, [ see Description ( 11 ) ].
- Known allergy to heparin or history of heparin-induced thrombocytopenia (HIT).
- IgA deficient patients with known antibodies against IgA.
-
5 WARNINGS AND PRECAUTIONS
5.1 Hypersensitivity Reactions
If severe allergic or anaphylactic-type reactions occur, immediately discontinue administration of BALFAXAR and initiate appropriate treatment. Therapeutic measures depend on the type and severity of the undesirable effect.
5.2 Thromboembolic Risk/Complications
There is a risk of thrombosis or disseminated intravascular coagulation when patients with acquired deficiency are treated with human prothrombin complex. [ 1 ] Patients given human prothrombin complex should be observed closely for signs or symptoms of disseminated intravascular coagulation or thrombosis. Because of the risk of thromboembolic complications, monitoring of signs and symptoms should be exercised when administering human prothrombin complex to patients with a history of coronary heart disease, patients with liver disease, or to patients at risk of thromboembolic events or disseminated intravascular coagulation. The potential benefit of treatment should be weighed against the risk of complications. BALFAXAR may not be suitable in patients with thrombotic or thromboembolic events in the prior 3 months, as it has not been studied in these patients. Resumption of anticoagulation should be carefully considered following administration of BALFAXAR and vitamin K once the risk of thromboembolic events outweighs the risk of bleeding.
5.3 Transmissible Infectious Agents
Standard measures to prevent infections resulting from the use of medicinal products prepared from human blood or plasma include selection of donors, screening of individual donations and plasma pools for specific markers of infection and the inclusion of effective manufacturing steps for the inactivation/removal of viruses.
Despite this, when medicinal products prepared from human blood or plasma are administered, the possibility of transmitting infectious agents e.g., viruses, the vCJD agent, and theoretically, CJD agent, cannot be completely eliminated. This also applies to unknown or emerging viruses and other pathogens.
The measures taken are considered effective for enveloped viruses such as human immunodeficiency virus (HIV), hepatitis B virus (HBV) and hepatitis C virus (HCV). The measures taken may be of limited value against non-enveloped viruses such as hepatitis A virus (HAV) and human parvovirus B19 (B19V).
B19V infections may be serious for pregnant women (fetal infection) and for individuals with immunodeficiency or increased erythropoiesis, e.g., hemolytic anemia.
All suspected infections thought by a physician to have been possibly transmitted by this product should be reported by the physician or other healthcare provider to Octapharma USA Inc. at 1-866-766-4860.
-
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
In a prospective, randomized, controlled, double-blind, multicenter non-inferiority trial, 208 subjects who required reversal of vitamin K antagonist induced anticoagulation due to the need for urgent surgery were enrolled; 105 received BALFAXAR and 103 Kcentra. Subjects ranged in age from 31 years to 92 years. Adverse reactions for BALFAXAR and the comparator are described below.
Adverse Reactions
The most common adverse reactions observed in ≥ 3% subjects receiving BALFAXAR were procedural pain, wound complications, asthenia, anemia, dysuria, procedural vomiting and catheter site related reaction.
In the post-surgical setting, serious adverse reactions in BALFAXAR treatment arm included cerebral infarction, and pulmonary embolism as well as hemorrhage, acute respiratory failure, shock, subdural hemorrhage. One subject experienced one serious adverse reaction, unstable angina assessed as related to BALFAXAR.
Adverse reactions are summarized for BALFAXAR and Kcentra in the following table:
Table 2 Adverse Reactions Reported in More Than 3% Subjects Following BALFAXAR or Kcentra Administration
System Organ Class
Preferred TermBALFAXAR Subjects (N=105)
n (%)Kcentra Subjects (N=103)
n (%)Blood and lymphatic system disorders Anemia 6 (5.7%) 6 (5.8%) Gastrointestinal disorders Abdominal pain 3 (2.9%) 5 (4.9%) General disorders and administration site conditions Asthenia 13 (12.4%) 18 (17.5%) Catheter site related reaction 4 (3.8%) 2 (1.9%) Injury, poisoning and procedural complications Postoperative wound complication 15 (14.3%) 15 (14.6%) Procedural pain 50 (47.6%) 50 (48.5%) Procedural vomiting 4 (3.8%) 0 Suture related complication 2 (1.9%) 4 (3.9%) Investigations Blood pressure increased 0 5 (4.9%) Body temperature increased 0 4 (3.9%) Renal and urinary disorders Dysuria 5 (4.8%) 2 (1.9%)
Deaths
There were a total of four deaths (3.8%) in the BALFAXAR group between 22 and 45 days post surgery, with one (1%) additional death occurring on day 47 just after completion of the study reporting period and one (1%) death in the Kcentra group 10 days after treatment. No deaths were considered to be related to study treatment.
Thromboembolic Events
There were three subjects (2.9%) with BALFAXAR who experienced four thromboembolic events in the randomized controlled trial in urgent surgery; cerebral infarction, pulmonary embolism, unstable angina and myocardial ischemia. The number of thromboembolic adverse reactions assessed as at least possibly related to study treatment was one (1%) with BALFAXAR (unstable angina). There were no thromboembolic events observed in the Kcentra treatment arm.
The following serious adverse reactions are described below and/or elsewhere in the labeling:
- Hypersensitivity Reactions [ see Warnings and Precautions ( 5.1 ) ]
- Arterial and venous thromboembolic complications [ see Boxed Warning and Warning s and Precautions ( 5.2 ) ]
- Possible Transmission of Infectious Agents [ see Warnings and Precautions ( 5.3 ) ]
6.2 Postmarketing Experience
Because post-marketing reporting of adverse reactions is voluntary and from a population of uncertain size, it is not always possible to reliably estimate the frequency of these reactions or establish a causal relationship to product exposure.
The following adverse reactions have been reported during postmarketing use of BALFAXAR outside the US since 2003:
Table 3 Adverse Reactions Reported During Post-Marketing Use of BALFAXAR
Immune system disorders
Anaphylactic shock, anaphylactic reaction, anaphylactoid reaction, hypersensitivity reactionNervous system disorders
Cerebrovascular accident, headache, paresthesia, tremorCardiac disorders
Bradycardia, tachycardia, cardiac arrestVascular disorders
Thromboembolic events, circulatory collapse, hypotension, hypertensionRespiratory, thoracic and mediastinal disorders
Dyspnea, respiratory failureGastrointestinal disorders
NauseaSkin and subcutaneous tissue disorders
Urticaria, rash, pruritusGeneral disorders and administration site conditions
Fever, chills
To report SUSPECTED ADVERSE REACTIONS, contact Octapharma USA Inc. at 1-866-766-4860 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
There are no data with BALFAXAR use in pregnancy to inform on drug-associated risk. Animal reproduction studies have not been conducted with BALFAXAR. It is not known whether BALFAXAR can cause fetal harm when administered to a pregnant woman or can affect reproduction capacity. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2-4% and 15-20%, respectively.
8.2 Lactation
Risk Summary
There is no information regarding the excretion of BALFAXAR in human milk, the effect on the breastfed infant, or the effects on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for BALFAXAR and any potential adverse effects on the breastfed child from BALFAXAR or from the underlying maternal condition.
8.4 Pediatric Use
The efficacy and safety of BALFAXAR have not been evaluated in pediatric patients.
8.5 Geriatric Use
Of the total number of subjects (105) with need for an urgent surgery/invasive procedure treated with BALFAXAR to reverse VKA anticoagulation, 59% were 65 years old or greater and 20% were 75 years old or greater. There is no evidence to suggest that BALFAXAR use in the geriatric population is associated with differences in safety or effectiveness.
-
11 DESCRIPTION
BALFAXAR is a human plasma-derived, purified, virus inactivated and nanofiltered non-activated Prothrombin Complex Concentrate (PCC) containing the coagulation factors II, VII, IX, and X and antithrombotic Proteins C and S. BALFAXAR is supplied as a lyophilized powder for reconstitution for intravenous use. The actual potency printed on the vial label represents the potency of Factor IX. BALFAXAR is sterile, endotoxin-free, and does not contain preservatives. No albumin is added as a stabilizer, and the excipients are heparin and sodium citrate. The diluent for reconstitution of the lyophilized powder is sterile Water for Injection.
The composition of BALFAXAR is as follows:
Component Potency Range for 500 IU vial Potency Range for 1000 IU vial Human Coagulation Factor II 340-500 IU 680-1000 IU Human Coagulation Factor VII 240-400 IU 480-800 IU Human Coagulation Factor IX 400-640 IU 800-1280 IU Human Coagulation Factor X 300-540 IU 600-1080 IU Protein C 320-560 IU 640-1120 IU Protein S 240-600 IU 480-1200 IU Heparin 80-384 IU 160-768 IU Sodium Citrate 16.8-23.4 mmol/L 16.8-23.4 mmol/L
All human plasma used in the manufacture of BALFAXAR is obtained from U.S. donors, collected in FDA-approved blood and plasma establishments, and tested by FDA-licensed serological tests for viral markers (Hepatitis B surface antigen (HBsAg), antibodies to HIV-1/2 and HCV). The plasma is tested with Nucleic Acid Testing (NAT) for HCV, HIV-1, HAV, and HBV, and found to be non-reactive (negative), and the plasma is also tested by NAT for B19V to exclude donations with high titers. The limit for the titer of B19V DNA in the manufacturing pool is set not to exceed 10 4 IU/mL. Only plasma that passed virus screening is used for production.
The BALFAXAR manufacturing process has the capability to clear viruses by a solvent/detergent (S/D) virus inactivation step and a virus removal nanofiltration step. The mean cumulative virus reduction factors of these steps are summarized in Table 4 .
Table 4 Virus Reduction During BALFAXAR Manufacturing
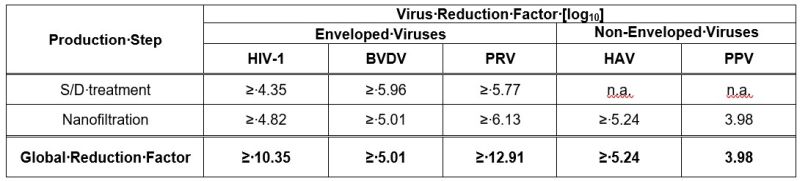
n.a.: not applicable
BVDV: Bovine Viral Diarrhea Virus, model for HCV
PRV: Pseudorabies Virus, model for large enveloped DNA viruses, e.g., HBV
PPV: Porcine Parvovirus, model for B19V
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
The administration of BALFAXAR provides a rapid increase in plasma levels of the vitamin K-dependent coagulation factors (FII, FVII, FIX, FX) and antithrombotic proteins C and S. Together they are referred to/known as the prothrombin complex. [ 2 ; 3 ] BALFAXAR can temporarily correct the coagulation defect of patients with deficiency of one or several of these factors.
12.2 Pharmacodynamics
In the randomized controlled trial in urgent surgery, the INR was determined at varying time points after the end of infusion. The median INR was 3.0 prior to the infusion and dropped to a median value of 1.30 by the 30-minute time point after the end of infusion. After 24 hours it was 1.25 in the BALFAXAR group (see Table 5 ).
The relationship between these or other INR values and clinical hemostasis in patients has not been established [see Clinical Studies ( 14 )].
Table 5 Median INR (Min-Max) After End of Infusion in Urgent Surgery RCT
Treatment Baseline 30 min 2 hr 4 hr 12 hr 24 hr BALFAXAR (N=105) 3.05
(2.0 - 21.1)1.30
(1.0 – 3.1)1.28
(1.0 - 2.5)1.30
(1.0 - 2.0)1.30
(0.9 - 2.7)1.25
(0.8 - 3.4)
12.3 Pharmacokinetics
Since BALFAXAR is given intravenously, bioavailability is proportional to the dose administered. BALFAXAR is distributed, metabolized, and excreted in the same manner as the endogenous proteins (see Table 6 ).
Table 6 Pharmacokinetic Parameters and Recovery of Coagulation Factors, Protein C and Protein S
Parameter FII FVII FIX FX Protein C Protein S C max (%) 62.42/1.33(37.00-118.00) 30.58/1.55(13.00-81.00) 57.57/1.55(27.00-130.00) 51.03/1.41(30.00-120.00) 59.95/1.35(38.00-109.00) 63.20/1.39(30.00-115.00) C max,norm (%/IU/kg) 2.38/1.23(1.38-2.96) 1.16/1.51(0.48-2.11) 2.19/1.65(0.84-4.71) 1.94/1.26(1.08-2.74) 2.28/1.31(1.17-3.45) 2.41/1.41(0.90-3.95) Incremental Recovery** (%/IU/kg) 1.73/1.33(0.81-2.42) 0.68/1.88(0.11-1.62) 1.17/1.83(0.26-2.52) 1.47/1.34(0.73-2.38) 1.25/0.54*(0.00-2.22) 1.47/1.52(0.59-2.35) Absolute Recovery*** (%) 75.70/1.34(32.65-116.98) 29.64/1.90(4.45-78.35) 51.36/1.82(13.54-115.58) 64.39/1.37(29.68-114.8) 54.95/24.60*(0.00-107.04) 64.26/1.55(23.74-113.66) t max 0.17(0.17-3.00) 0.17(0.17-1.00) 0.50(0.17-3.00) 0.17(0.17-3.00) 0.17(0.00-3.00) 0.17(0.17-3.00) Note: Values reported as geometric mean/geometric SDs (range), except for t max which is reported as median (min-max)
*Mean values SD (due to zero values, the geometric mean could not be calculated)
**The incremental recovery is defined as the rise in the plasma concentrations (%) achieved with 1 IU BALFAXAR/kg BW.
***The absolute recovery is defined as the rise in the plasma concentrations (%) achieved by the dose.
- 13 NONCLINICAL TOXICOLOGY
-
14 CLINICAL STUDIES
The efficacy of BALFAXAR was assessed in a randomized, double-blind, multicenter study in comparison to Kcentra, for the reversal of vitamin K antagonist induced anticoagulation in patients needing urgent surgery. A total of 208 subjects with acquired coagulation factor deficiency due to oral Vitamin K antagonist therapy were randomized to a single dose of BALFAXAR (n=105) or Kcentra (n=103). The doses of BALFAXAR and Kcentra based on the nominal Factor IX content (25 units/kg, 35 units/kg, or 50 units/kg) were calculated according to the patient’s baseline INR (2-< 4, 4-6, >6, respectively). The observation period lasted for 45 days post-surgery. The primary endpoint was hemostatic efficacy rating at the end of the surgery assessed by the Independent Endpoint Adjudication Board (IEAB). The study was stopped early due to statistically significant efficacy results at the pre-specified interim analysis, where 94.6% (88/93) of the subjects in the BALFAXAR group and 93.5% (86/92) of the subjects in the Kcentra group achieved effective hemostasis ( Table7 ). The non-inferiority analysis for the proportion difference (98% CI) of 1.1% (-9.2%, 11.5%) was statistically significant (p<0.001) indicating that BALFAXAR was non-inferior to Kcentra. The lower bound of the CI was above the pre-specified noninferiority margin of -15%, indicating that BALFAXAR was non-inferior to Kcentra. At the conclusion of the study, the updated proportions of subjects with effective hemostasis were 94.3% (99/105) in the BALFAXAR group and 94.2% (97/103) in the Kcentra group ( Table 7 ), resulting in a difference (95% CI) of 0.1% (-8.0%, 8.2%).
Table 7 Rating of Hemostatic Efficacy in Urgent Surgery RCT
Effective hemostasis No. (%) of subjects Proportion difference BALFAXAR Kcentra BALFAXAR vs. Kcentra Interim analysis 88/93 (94.6%) 86/92 (93.5%) 1.1%, 98% CI: (-9.2%, 11.5%)* Final analysis** 99/105 (94.3%) 97/103 (94.2%) 0.1%, 95% CI: (-8.0%, 8.2%) CI = confidence interval N = number of subjects
* Met pre-specified non-inferiority criterion (Margin used -15% and p<0.001, statistically significant at pre-specified alpha level of 0.01)
** Descriptive analysis of all subjects in the study including an overrun of subjects during the decision making at the interim analysis.
Mean (SD) baseline (i.e., within 3 hours prior to BALFAXAR or Kcentra infusion) INR was 3.96 (2.77) in the BALFAXAR group and 3.56 (1.82) in the Kcentra group. The proportion of patients achieving an INR ≤1.5 as measured 30 minutes after the end of the infusion was 78.1% in the BALFAXAR group versus 71.8% in the Kcentra group (proportion difference of 6.3%; 95% CI: 5.5%, 18.0%). Overall, 72.1% of patients had vitamin K administered, with a median dose of 10 mg in both groups ( Table 8 ).
Table 8 Decrease of INR (to 1.5 or Less at 30 Minutes after End of Infusion) in Urgent Surgery RCT
Rating No. (%) of subjects Proportion difference
BALFAXAR vs Kcentra
(95% CI for difference)BALFAXAR (N=105) Kcentra (N=103) Decrease of INR to ≤ 1.5 at 30 min 82 (78.1) 74 (71.8) 6.3% (5.5%, 18.0%)
The median dose of BALFAXAR/ Kcentra was 25 IU of Factor IX/kg body weight in both treatment groups, ranging from 16 IU/kg to 50 IU/kg in the BALFAXAR group and 15 IU/kg to 50 IU/kg in the Kcentra group. The median duration of the infusion was 12 minutes in the BALFAXAR group (ranging from 8 to 50 minutes) and 13 minutes (ranging from 7 to 30 minutes) in the Kcentra group.
-
15 REFERENCES
- Koehler M: Thrombogenicity of prothrombin complex concentrates. Thrombosis Research 1999;95:S13-S17.
- Warkentin TE, Crowther MA: Reversing anticoagulants both old and new. Can.J. Anaesth. 2002;49:S11-S25.
- Ansell J, Hirsh J, Poller L, et al: The pharmacology and management of the vitamin K antagonists: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 2004;126:204S-233S.
-
16 HOW SUPPLIED/STORAGE AND HANDLING
BALFAXAR is supplied in single-dose vials.
Carton
NDC NumberContainer (Vial)
NDC NumberSize Color coding 68982-261-01
68982-261-0268982-261-81
68982-261-82500 IU Range FIX in 20 mL
1000 IU Range FIX in 40 mLpurple
green- BALFAXAR is supplied in a package with a single-dose vial of lyophilized powder and a vial of diluent (sterile Water for Injection), together with a transfer device.
- Components used in the packaging of BALFAXAR are not made with natural rubber latex.
- Store BALFAXAR for up to 36 months at 2°C to 25°C (36°F to 77°F) from the date of manufacture. Do not freeze.
- Do not use beyond the expiration date on the vial label and carton.
- Store the vial in the original package to protect it from light.
- Reconstitute the BALFAXAR powder only directly before use. Use the solution immediately after reconstitution. However, if it is not administered immediately, the reconstituted solution can be stored for up to 8 hours at room temperature (20°C to 25°C; 68°F to 77°F), provided sterility of the stored product is maintained. Discard partially used vials.
-
17 PATIENT COUNSELING INFORMATION
- Inform patients of the signs and symptoms of allergic hypersensitivity reactions, such as urticaria, rash, tightness of the chest, wheezing, hypotension and/or anaphylaxis experienced during or after injection of BALFAXAR. [ see Warnings and Precautions ( 5.1 ) ].
- Inform patients of signs and symptoms of thrombosis, such as limb or abdomen swelling and/or pain, chest pain or pressure, shortness of breath, loss of sensation or motor power, altered consciousness, vision, or speech. [ see Warnings and Precautions ( 5.2 ) ].
- Inform patients that, because BALFAXAR is made from human blood, it may carry a risk of transmitting infectious agents, e.g., viruses, the variant Creutzfeldt-Jakob disease (vCJD) agent, and theoretically, the Creutzfeldt-Jakob disease (CJD) agent. [ see Warnings and Precautions ( 5.3 ), Description ( 11 ) ].
Manufactured by:
Octapharma Pharmazeutika Produktionsges.m.b.H.
Oberlaaer Strasse 235
1100 Vienna, Austria
U.S. License No. 1646
Distributed by:
Octapharma USA Inc.
117 W Century Road
Paramus, NJ 07652
-
PACKAGE LABEL - PRINCIPAL DISPLAY PANEL
Prothrombin Complex Concentrate (Human)
BALFAXAR
500 IU Range FIX in 20 mL
NDC: 68982-261-01
BALFAXAR
1000 IU Range FIX in 40 mL
NDC: 68982-261-01
-
INGREDIENTS AND APPEARANCE
BALFAXAR
prothrombin complex concentrate (human) powder, for solutionProduct Information Product Type PLASMA DERIVATIVE Item Code (Source) NDC: 68982-261 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength COAGULATION FACTOR IX HUMAN (UNII: 6U90Y1795T) (COAGULATION FACTOR IX HUMAN - UNII:6U90Y1795T) COAGULATION FACTOR IX HUMAN 25.5 [iU] in 1 mL PROTHROMBIN (UNII: 8FB1K07F16) (Prothrombin - UNII:8FB1K07F16) PROTHROMBIN 26 [iU] in 1 mL COAGULATION FACTOR VII HUMAN (UNII: 4156XVB4QD) (COAGULATION FACTOR VII HUMAN - UNII:4156XVB4QD) COAGULATION FACTOR VII HUMAN 16.5 [iU] in 1 mL COAGULATION FACTOR X HUMAN (UNII: 0P94UQE6SY) (COAGULATION FACTOR X HUMAN - UNII:0P94UQE6SY) COAGULATION FACTOR X HUMAN 24 [iU] in 1 mL PROTEIN C (UNII: 3Z6S89TXPW) (PROTEIN C - UNII:3Z6S89TXPW) PROTEIN C 22 [iU] in 1 mL PROTEIN S HUMAN (UNII: 90J3F6N5FN) (PROTEIN S HUMAN - UNII:90J3F6N5FN) PROTEIN S HUMAN 22 [iU] in 1 mL Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 68982-261-01 1 in 1 CARTON 1 NDC: 68982-261-81 20 mL in 1 VIAL, GLASS; Type 9: Other Type of Part 3 Combination Product (e.g., Drug/Device/Biological Product) 2 NDC: 68982-261-02 1 in 1 CARTON 2 NDC: 68982-261-82 40 mL in 1 VIAL, GLASS; Type 9: Other Type of Part 3 Combination Product (e.g., Drug/Device/Biological Product) Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA125776 11/30/2023 Labeler - Octapharma USA Inc (606121163)
Trademark Results [Balfaxar]
Mark Image Registration | Serial | Company Trademark Application Date |
|---|---|
 BALFAXAR 87648328 5593557 Live/Registered |
Octapharma AG 2017-10-17 |
 BALFAXAR 86125467 not registered Dead/Abandoned |
Octapharma AG 2013-11-21 |
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.