Moxidectin by Medicines Development for Global Health MOXIDECTIN tablet
Moxidectin by
Drug Labeling and Warnings
Moxidectin by is a Prescription medication manufactured, distributed, or labeled by Medicines Development for Global Health. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use
MOXIDECTIN safely and effectively.
See full prescribing information for MOXIDECTIN.
MOXIDECTIN tablets, for oral use
Initial U.S. Approval: 2018INDICATIONS AND USAGE
MOXIDECTIN tablets, for oral use
Initial U.S. Approval: 2018 (1)(1)
(1)
Moxidectin is an anthelmintic indicated for the treatment of onchocerciasis due to Onchocerca volvulus in patients aged 12 years and older. (1) (1)
Limitations of Use: (1)- Moxidectin Tablets do not kill adult
O. volvulus parasites.
Follow-up is advised. - The safety and efficacy of repeat administration of Moxidectin Tablets in patients with O. volvulus has not been studied.These highlights do not include all the information needed to use Moxidectin Tablets. See full prescribing information for Moxidectin Tablets Initial U.S. Approval.
DOSAGE AND ADMINISTRATION
Patients aged 12 years and older: Take 8 mg (four 2 mg tablets) as a
single oral dose, with or without food. (2.1) (2)DOSAGE FORMS AND STRENGTHS
Tablets: 2 mg. (3) (3)
CONTRAINDICATIONS
None. (4) (4)
WARNINGS AND PRECAUTIONS
Cutaneous, Ophthalmological and/or Systemic Adverse Reactions of Varying Severity (Mazzotti Reaction): This may occur in patients with onchocerciasis following treatment with Moxidectin Tablets. Monitor patients for symptoms, including symptomatic orthostatic hypotension. (5.1) (5)
(5)
Symptomatic Orthostatic Hypotension: Episodes of symptomatic orthostatic hypotension including inability to stand without support may occur in patients following treatment with Moxidectin Tablets. (5.2) (5)
(5)
Encephalopathy in Loa loa co-infected patients: Serious or even fatal encephalopathy following treatment with Moxidectin Tablets may occur in patients co-infected with Loa loa. Assess patients for loiasis in Loa loa endemic areas prior to treatment. (5.3) (5)
(5)
Edema and Worsening of Onchodermatitis: Patients with hyper-reactive onchodermatitis (sowda) may be more likely than others to experience severe edema and aggravation of onchodermatitis. (5.4) (5)
ADVERSE REACTIONS
The most common adverse reactions (incidence > 10%) were:
eosinophilia, pruritus, musculoskeletal pain, headache, lymphopenia,
tachycardia, rash, abdominal pain, hypotension, pyrexia, leukocytosis,
influenza-like illness, neutropenia, cough, lymph node pain, dizziness,
diarrhea, hyponatremia and peripheral swelling. (6) (6)(6)
To report SUSPECTED ADVERSE REACTIONS, contact
Medicines Development for Global Health at 1-800-MDGH-456 or
FDA at 1-800-FDA-1088 or www.fda.gov/medwatch. (6)Revised: 6/2018
- Moxidectin Tablets do not kill adult
O. volvulus parasites.
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
6 ADVERSE REACTIONS
7 DRUG INTERACTIONS
8 USE IN SPECIFIC POPULATIONS
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
13 NONCLINICAL TOXICOLOGY
14 CLINICAL STUDIES
16 HOW SUPPLIED/STORAGE AND HANDLING
- * Sections or subsections omitted from the full prescribing information are not listed.
-
1 INDICATIONS AND USAGE
Moxidectin Tablets are indicated for the treatment of onchocerciasis due to Onchocerca volvulus in patients aged 12 years and older [see Clinical Studies (14)].
Limitations of Use:
Moxidectin Tablets do not kill adult O. volvulus. Follow-up evaluation is advised.
The safety and efficacy of repeat administration of Moxidectin Tablets in patients with O. volvulus has not been studied.
- 2 DOSAGE AND ADMINISTRATION
- 3 DOSAGE FORMS AND STRENGTHS
- 4 CONTRAINDICATIONS
-
5 WARNINGS AND PRECAUTIONS
5.1 Cutaneous, Ophthalmological and/or Systemic Adverse Reactions
Treatment with Moxidectin Tablets may cause cutaneous, ophthalmological and/or systemic reactions of
varying severity (Mazzotti reaction). These adverse reactions are due to allergic and inflammatory host
responses to the death of microfilariae [ see Adverse Reactions (6.1)]. There is a trend toward an increased
incidence of these adverse reactions in patients with higher microfilarial burden.The clinical manifestations of Mazzotti reaction includes pruritus, headache, pyrexia, rash, urticaria,
hypotension (including symptomatic orthostatic hypotension and dizziness) [ see Warnings and
Precautions (5.2 )], tachycardia, edema, lymphadenopathy, arthralgia, myalgia, chills, paresthesia and
asthenia. Ophthalmological manifestations include conjunctivitis, eye pain, eye pruritus, eyelid swelling, blurred
vision, photophobia, changes in visual acuity, hyperemia, ocular discomfort and watery eyes. These adverse
reactions generally occur and resolve in the first week post-treatment. Laboratory changes include
eosinophilia, eosinopenia, lymphocytopenia, neutropenia, and increases in alanine aminotransferase (ALT),
aspartate aminotransferase (AST), gamma glutamyl transferase (GGT) and lactate dehydrogenase (LDH).
Proteinuria has also been reported.Treatment of severe Mazzotti reactions has not been evaluated in controlled clinical trials. Symptomatic
treatments such as oral hydration, recumbency, intravenous normal saline, and/or parenteral corticosteroids
have been used to treat orthostatic hypotension. Antihistamines and/or analgesics have been used for most
mild to moderate cases.5.2 Symptomatic Orthostatic Hypotension
An increased number of patients who received Moxidectin Tablets developed symptomatic orthostatic
hypotension with inability to stand without support after lying down for 5 minutes (in an orthostatic hypotension
provocation test); 47/978 (5%) compared with 8/494 (2%) who received ivermectin. The decreases in blood
pressure were transient, managed by resumption of recumbency and most commonly occurred on Days 1 and
2 post-treatment. Advise patients that if they feel dizzy or light-headed after taking Moxidectin Tablets, they
should lie down until the symptoms resolve.5.3 Encephalopathy in Loa loa Co-infected Patients
Patients with onchocerciasis who are also infected with Loa loa may develop a serious or even fatal
encephalopathy following treatment with Moxidectin Tablets.Moxidectin Tablets have not been studied in patients co-infected with Loa loa. Therefore, it is recommended
that individuals who warrant treatment with Moxidectin Tablets and have had exposure to Loa loa-endemic
areas undergo diagnostic screening for loiasis prior to treatment.5.4 Edema and Worsening of Onchodermatitis
Patients with hyper-reactive onchodermatitis (sowda) may be more likely than others to experience severe
edema and worsening of onchodermatitis following the use of Moxidectin Tablets. Symptomatic treatment has
been used to manage patients who have experienced edema and worsening of onchodermatitis. -
6 ADVERSE REACTIONS
The following clinically significant adverse reactions are described in greater detail in other labeling sections:
Cutaneous, Ophthalmological and/or Systemic Adverse Reactions [see Warnings and
Precautions (5.1)]
Symptomatic Orthostatic Hypotension [ see Warnings and Precautions (5.2)]
Encephalopathy in Loa loa Co-infection [ see Warnings and Precautions (5.3)]
Edema and Worsening of Onchodermatitis [ see Warnings and Precautions (5.4)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under varying controlled conditions, adverse reaction rates observed in
one clinical trial cannot be directly compared to rates observed in the clinical trials of another drug and may not
reflect the rates observed in clinical practice.
The safety of Moxidectin Tablets was evaluated in two randomized, double-blind, active-controlled studies
(Trial 1 and Trial 2) [ see Clinical Studies (14)]. In Trial 1, 978 patients received Moxidectin Tablets as a single
oral dose of 8 mg and 494 patients received ivermectin as a single oral dose of approximately 150 mcg/kg. In
Trial 2, 127 patients received Moxidectin Tablets as a single oral dose ranging from 2 mg (this is not an
approved dose) to 8 mg (38 received the recommended 8 mg dose) and 45 patients received ivermectin as a
single oral dose of approximately 150 mcg/kg.
Most Common Adverse Reactions
No patients withdrew from either trial due to adverse reactions. Adverse Reactions reported in Trial 1 in > 10%
of patients are summarized in Table 1. Most were related to physical, vital signs and laboratory changes
associated with Mazzotti reaction [ see Warnings and Precautions (5.1)].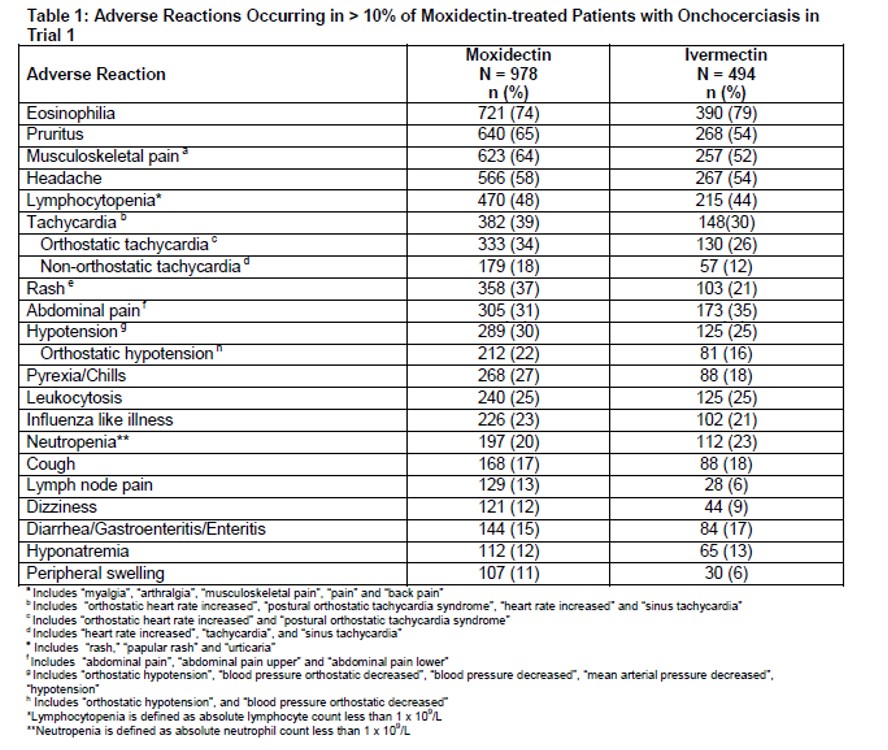
The most common adverse reactions in patients (n = 38) treated with 8 mg moxidectin in Trial 2 were similar to
the adverse reactions noted in Trial 1 described in Table 1 above.
Other Adverse Reactions Reported in Clinical Trials
The following adverse reactions occurred in less than 10% of subjects receiving Moxidectin Tablets in Trial 1:
Ocular Adverse Reactions: In Trial 1, the most common ocular adverse reactions (occurring in ≥ 0.5% of
patients) is shown in Table 2.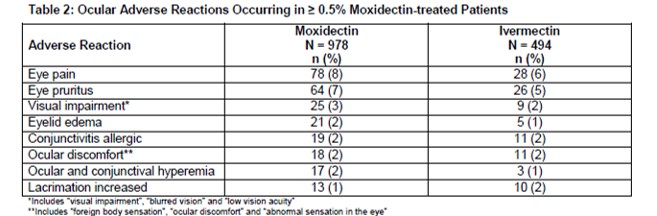
Hepatobiliary Adverse Reactions
More patients in the moxidectin arm experienced elevation in bilirubin above the upper limit of normal and
elevation in transaminases > 5x upper limit of normal. Twenty-seven (2.8%) patients in the moxidectin arm and
3 (0.6%) patients in the ivermectin arm had hyperbilirubinemia. Most of the patients had single measurements
of hyperbilirubinemia without concurrent elevation in transaminases.
Nine (1%) patients in the moxidectin arm and 2 (0.4%) patients in the ivermectin arm had elevation in ALT of
more than 5x upper limit of normal; ten (1%) patients in the moxidectin arm and 3 (0.6%) patients in the
ivermectin arm had elevation in AST to more than 5x upper limit of normal.
Laboratory Abnormalities
Laboratory abnormalities occurring in at least 1% of patients in the Trial 1 are described in Table 3.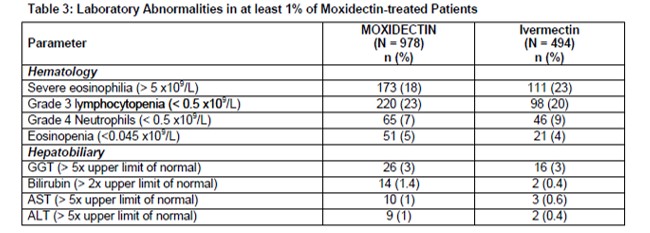
- 7 DRUG INTERACTIONS
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
Limited available data on the use of Moxidectin Tablets in pregnant women are insufficient to establish whether
there is a moxidectin-associated risk for major birth defects and miscarriage. Moxidectin administered orally to
pregnant rats during the period of organogenesis (Gestation Days (GD) 6 to 15), was not associated with
significant embryo-fetal developmental effects at doses of approximately 15 times the recommended human
dose based on body surface area. When moxidectin was dosed orally to pregnant rabbits during the period of
organogenesis (GD 7 - 19), no embryo-fetal developmental effects were observed at oral doses of moxidectin
up to 24 times the recommended human dose based on body surface area [ see Data].
Daily parental oral administration of dietary moxidectin to rats prior to mating, and through mating, gestation,
and lactation was associated with decreased survival and body weights for first-generation offspring without
maternal toxicity at moxidectin doses less than 2-times the recommended human dose based on body surface
area comparison. Daily dietary moxidectin did not produce maternal toxicity or adverse effects for first- and
second-generation offspring at doses approximately equivalent to the recommended human dose based on body surface area comparison.
Offspring were assessed for survival, body weights, and fertility.
Developmental milestones were not assessed in this study.
The estimated background risk of major birth defects and miscarriage for the indicated population is unknown.
All pregnancies have a background risk of birth defect, loss or other adverse outcomes. In the U.S. general
population, the estimated background risk of major birth defects and miscarriage in clinically recognized
pregnancies is 2% to 4% and 15% to 20%, respectively.
Data
Animal Data
In a rat embryo-fetal development study, daily oral administration of moxidectin at 12 mg/kg/day (approximately
15 times the recommended human dose of 8 mg based on body surface area comparison) during Gestation
Days (GDs) 6 to 15 significantly increased the fetal incidence, but not the litter incidence of cleft palate and the
fetal and litter incidence of a skeletal variation, wavy ribs, at a maternally toxic dose. Mean maternal food
consumption, body weights, and body weight gain were significantly decreased at moxidectin doses of 10 and
12 mg/kg/day compared to control values. The no observed adverse effect level (NOAEL) value for maternal
and fetal toxicity was considered to be 5 and 10 mg/kg/day respectively (approximately 6 and 12 times,
respectively, the recommended human dose based on body surface area comparison). In the rabbit, daily oral
administration of moxidectin at ≥ 5 mg/kg/day from GD7 to GD19 was not associated with fetal weight loss or
malformations but resulted in significantly decreased maternal food consumption and body weight gains. The
NOAEL value for maternal and fetal toxicity in the rabbit was 1 mg/kg/day and 10 mg/kg/day respectively
(approximately 2 times and 24 times, respectively, the recommended human dose based on body surface area
comparison). In a pre-postnatal study in rats, parental oral administration of dietary moxidectin prior to mating,
through mating, gestation, and lactation did not produce adverse effects in first-generation or secondgeneration
offspring at a maternal NOAEL dose of 0.824 mg/kg/day (approximately equivalent to the
recommended human dose based on body surface area comparison). However, at moxidectin doses
≥ 1.1 mg/kg/day (approximately equivalent to 1.3 times the recommended human dose based on body surface
area comparison), the survival and body weights of first-generation offspring were significantly decreased
during the lactation period, and the number of live fetuses at birth was significantly decreased with a maternal
moxidectin dose of 11 mg/kg/day (approximately equivalent to 13 times the recommended human dose based
on body surface area comparison). In this study, offspring were assessed for survival, body weights, and
fertility, and developmental milestones were not assessed.
8.2 Lactation
Risk Summary
Moxidectin was detected in the milk of lactating women following a single 8 mg dose of Moxidectin Tablets
[ see Data]. There are no data on the effects of Moxidectin Tablets on the breast-fed infant or milk production.
The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical
need for Moxidectin Tablets and any potential adverse effects on the breastfed child from Moxidectin Tablets
or from the underlying maternal condition.Data
A pharmacokinetic study in twelve healthy adult lactating women who were 21 to 100 weeks post partum
evaluated the concentrations of moxidectin in plasma and breast milk collected over a period of 28 days
following a single 8 mg dose of Moxidectin Tablets. The mean (± SD) exposure ratio of moxidectin present in
human breast milk to that of human plasma was approximately 1.77 (± 0.66) over a collection period of
28 days. The estimated mean (± SD) total infant dose, assuming the infants would consume all the breast milk
collected during the study, was 0.056 mg (± 0.024 mg), which would be approximately 0.70% (± 0.30%) of the
maternal dose. The effects of moxidectin or its metabolites on the breast-fed child or milk production were not
evaluated.
8.4 Pediatric Use
The safety and effectiveness of Moxidectin Tablets have been established in pediatric patients 12 years of age
and older. In Trial 1, (n = 53 patients aged 12 to 17 years), the safety and effectiveness was similar to that
observed in adults [ see Adverse Reactions (6.1), and Clinical Studies (14)]. The safety and effectiveness of
Moxidectin Tablets in pediatric patients under 12 years of age has not been established.
8.5 Geriatric Use
Of the total number of patients included in Trial 1 that were treated with Moxidectin Tablets, 83 were aged
65 and over. No overall differences in safety or effectiveness were observed between these patients and
younger patients, and other reported clinical experience has not identified differences in responses between
the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out [ see
Clinical Studies (14) and Clinical Pharmacology (12.3)].
8.6 Renal Impairment
No dose adjustment of Moxidectin Tablets is necessary for patients with mild (creatinine clearance (CrCL)
60 to 89 mL/min) to moderate (CrCL 30 to 59 mL/min) renal impairment. The safety of Moxidectin Tablets in
patients with severe renal impairment (CrCL 15 to 29 mL/min) or end stage renal disease, is unknown [ see
Clinical Pharmacology (12.3)]. -
10 OVERDOSAGE
No specific antidote is available for overdose with Moxidectin Tablets. If overdose occurs, the patient should be
monitored for evidence of toxicity. Treatment of overdose with Moxidectin Tablets consists of general
supportive measures including monitoring of vital signs as well as observation of the clinical status of the
patient. Supportive therapy, if indicated, should include parenteral fluids and electrolytes, respiratory support
(oxygen and mechanical ventilation if necessary) and pressor agents if clinically significant hypotension is
present. -
11 DESCRIPTION
Moxidectin Tablets contain moxidectin, an anthelmintic drug and a macrocyclic lactone of the milbemycin class
derived from the actinomycete Streptomyces cyanogriseus.
The chemical name of moxidectin is (2aE,4E,5'R,6R,6'S,8E,11R,13S,15S,17aR,20R,20aR,20bS)-6'-[(E)-1,3-
dimethyl-1-butenyl]-5',6,6',7,10,11,14,15,17a,20,20a,20b-dodecahydro-20,20b-dihydroxy-5',6,8,19-
tetramethylspiro[11,15-methano-2H,13H,17H-furo[4,3,2-pq][2,6]benzodioxacyclooctadecin-13,2'-[2H]pyran]-
4',17(3'H)-dione 4'-(E)-(O-methyloxime). The structural formula is: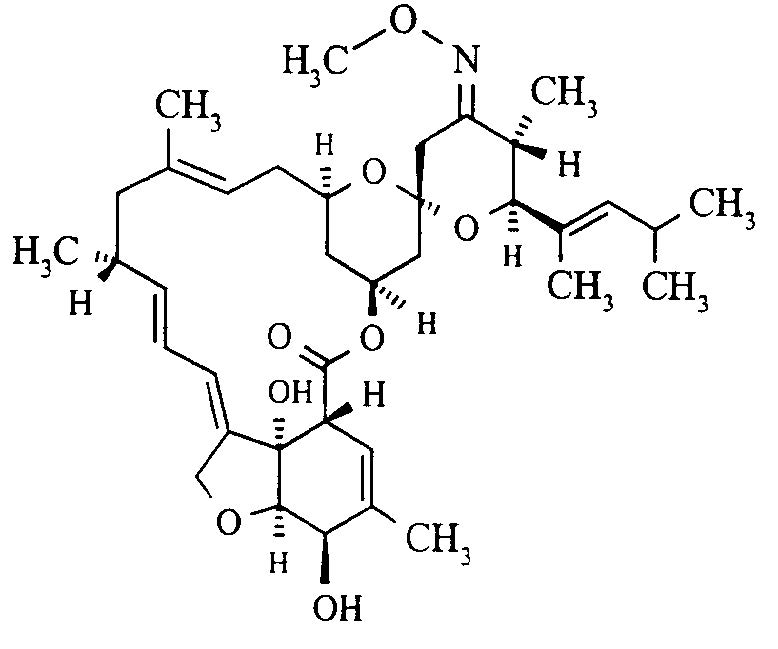
Figure 1: Moxidectin Structure
Moxidectin is a white or pale-yellow, amorphous powder. The empirical formula is C37H53NO8 and the
molecular weight is 639.82 Dalton. Moxidectin is readily soluble in organic solvents such as methylene chloride, diethyl ether, ethanol, acetonitrile, and ethyl acetate. It is only slightly soluble in water (0.51 mg/L) and
the melting point range for moxidectin powder is 145°C to 154°C.
Moxidectin Tablets are for oral administration. Each tablet contains 2 mg of moxidectin. The tablets are
uncoated and include the following inactive ingredients: colloidal silicon dioxide, croscarmellose sodium,
lactose anhydrous, magnesium stearate, microcrystalline cellulose and sodium lauryl sulfate. -
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Moxidectin, a macrocyclic lactone, is an anthelmintic drug [ see Microbiology (12.4)].
12.2 Pharmacodynamics
Cardiac Electrophysiology
At a dose 4.5 times the approved recommended dose, moxidectin does not prolong the QT interval to any
clinically relevant extent.
12.3 Pharmacokinetics
The pharmacokinetic parameters of moxidectin following a single 8 mg oral dose of Moxidectin Tablets to
healthy subjects and patients with onchocerciasis under fasted conditions are shown in Table 4. Mean
moxidectin C max and AUC increased approximately proportionally to dose over a dose range of 2 to 36 mg
(0.25 to 4.5 times the approved recommended dose) in healthy subjects under fasted conditions.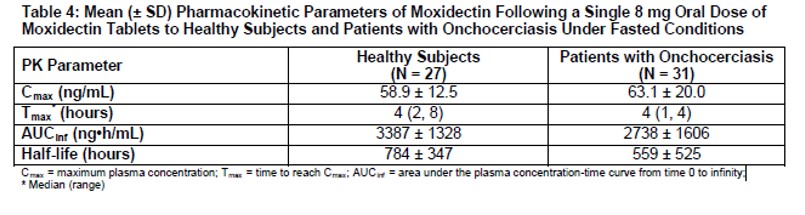
Absorption
Effect of Food
Moxidectin mean C max and AUC increased on average by 34% and 39%, respectively, when administered with
a standard high fat meal (900 calories, with a nutritional distribution of approximately 55% fat,
31% carbohydrates and 14% protein), compared to fasted conditions [see Dosage and Administration (2.1)].
Distribution
The apparent mean ± SD volume of distribution of moxidectin is 2421 ± 1658 L in patients with onchocerciasis.
The plasma protein binding in humans is unknown.
Elimination
The mean terminal half-life of moxidectin in patients with onchocerciasis is 23.3 days (559 hours) following a
single 8 mg dose of Moxidectin Tablets.
The apparent mean ± SD total clearance of moxidectin is approximately 3.50 ± 1.23 L/hour in patients with
onchocerciasis.Metabolism
The hepatic metabolism of moxidectin is minimal.
Excretion
Following administration of a single 8 mg oral dose of Moxidectin Tablets to healthy subjects, 2% of the dose is
eliminated unchanged in the feces within the first 72 hours. Renal elimination of intact drug is negligible.
Specific Populations
In clinical studies, no clinically significant differences in the pharmacokinetics of moxidectin were observed
based on age (18 to 60 years), sex, weight (42.7 to 107.2 kg), or renal impairment (creatinine clearance (CrCL)
47 to 89 mL/min, estimated by Cockcroft-Gault). The pharmacokinetics of moxidectin in patients with CrCL less
than 47 mL/min is unknown. The pharmacokinetics of moxidectin in patients with hepatic impairment is
unknown.
Patients with Renal Impairment
Based on a population pharmacokinetic analysis and the fact that renal elimination of intact drug is negligible,
mild (creatinine clearance (CrCL), estimated by Cockcroft-Gault of 60 to 89 mL/min) and moderate (CrCL 30 to
59 mL/min) renal impairment is not likely to have an impact on the exposure of moxidectin. The effect of severe
renal impairment (CrCL 15 to 29 mL/min) or of end-stage renal disease on the pharmacokinetics of moxidectin
is unknown.
Drug Interaction Studies
Clinical Study with Midazolam (CYP3A4 substrate)
Co-administration of a single 8 mg dose of Moxidectin Tablets with a single oral 7.5 mg dose of midazolam (a
sensitive CYP3A substrate) to healthy subjects (n = 37) did not affect the pharmacokinetics of midazolam or its
major metabolite, 1-hydroxy midazolam.
In Vitro Studies
CYP Enzymes: Moxidectin is not a substrate or inhibitor of CYP enzymes.
Uridine 5'-diphospho-glucuronosyltransferases (UGTs): Moxidectin is not a UGT substrate.
Transporter Systems: Moxidectin is not a substrate of P-glycoprotein (P-gp) nor breast cancer resistance
protein 1 (BCRP1).12.4 Microbiology
Mechanism of Action
The mechanism by which moxidectin exhibits its effect against O. volvulus is not known. Studies with other
nematodes suggest that moxidectin binds to glutamate-gated chloride channels (GluCl), gamma-aminobutyric
acid (GABA) receptors and/or ATP-binding cassette (ABC) transporters. This leads to increased permeability,
influx of chloride ions, hyperpolarization and muscle paralysis. Additionally, there is a reduction in motility of all
stages of the parasite, excretion of immunomodulatory proteins, and the fertility of both male and female adult
worms.
Antimicrobial activity
Moxidectin is active against the microfilariae of O. volvulus [ see Clinical Studies (14)].
Studies suggest that moxidectin is not effective in killing the adult worms, however, it inhibits intra-uterine
embryogenesis and release of microfilariae from the adult worms.
Resistance
Studies in vitro and infected animals suggest a potential for development of resistance to moxidectin and
cross-resistance with other macrocyclic lactones, such as ivermectin. However, the clinical relevance of these
findings is not known.The mechanism of resistance may be multifactorial that include alteration in the target GluCl, GABA receptors
and/or ABC transporters. -
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Moxidectin was shown to be negative for genotoxicity in a battery of in vitro assays including a bacterial mutagenicity assay, mouse lymphoma cell mutagenicity assay, unscheduled DNA synthesis assay, and a chromosome aberration assay, as well as in vivo in a micronucleus assay in mice and a chromosome aberration assay in rats.
Two-year carcinogenicity studies in mice and rats were conducted with moxidectin. Mice were administered a mean dietary dose of 8.7 mg/kg/day moxidectin which is approximately equivalent to 5 times the recommended human dose based on body surface area comparison. Rats were administered a mean dietary dose of 6.1 mg/kg/day moxidectin which is approximately equivalent to 7 times the recommended human dose based on body surface area comparison. There was no evidence of tumorigenicity in either study.
In fertility evaluations, male and female mating and fertility indices were not inhibited by oral-dietary moxidectin doses of approximately 0.86 mg/kg/day which is approximately equivalent to the recommended human dose based on body surface area comparison.
13.2 Animal Toxicology and/or Pharmacology
Moxidectin was associated with transient CNS-related clinical signs. In rats, a single dose of 20 mg/kg
(equivalent to approximately 24 times the recommended human dose based on body surface area
comparison) moxidectin was associated with piloerection, reduced arousal and body tone, abnormal gait,
slowed breathing, and impaired righting reflex. In dogs, repeated doses of 1.6 mg/kg/day moxidectin
(equivalent to approximately 7 times the recommended human dose based on body surface area comparison)
was associated with lacrimation, languid appearance, tremors, slight salivation, and slight ataxia. -
14 CLINICAL STUDIES
The assessment of the safety and efficacy of Moxidectin Tablets 8 mg in the treatment of onchocerciasis is
based on data from two randomized, double-blind, active-controlled trials in patients with O. volvulus infection,
Trial 1 in 1472 patients (NCT 00790998), and Trial 2, a dose-ranging trial (NCT 00300768). Patients in the
trials received a single oral dose of moxidectin or ivermectin, the active control medication.
Efficacy was assessed by skin microfilarial density (microfilariae/mg skin) from the mean of 4 skin snips per
person per time point up to 18 months post-treatment.
Trial 1 recruited adult and adolescent patients ≥ 12 years with a body weight ≥ 30 kg and ≥ 10 microfilariae/mg
skin. Mean (± SD) age was 42.5 (± 16.3) years, height 1.59 (± 0.09) meters, weight 51.6 (± 8.2) kg; 36.1%
were female and 100% were black. Mean (± SD) pretreatment skin microfilarial density was 39.5 (± 30.7),
69.6% had ≥ 20 microfilariae/mg skin and 39.7% had at least one ocular microfilaria.
Patients who were not previously exposed to ivermectin community directed treatment programs were
recruited from the sub-Saharan African region (Democratic Republic of Congo, Liberia, and Ghana). Table 5
reports mean skin microfilarial density and the proportion of patients with undetectable skin microfilariae at
Months 1, 6, and 12.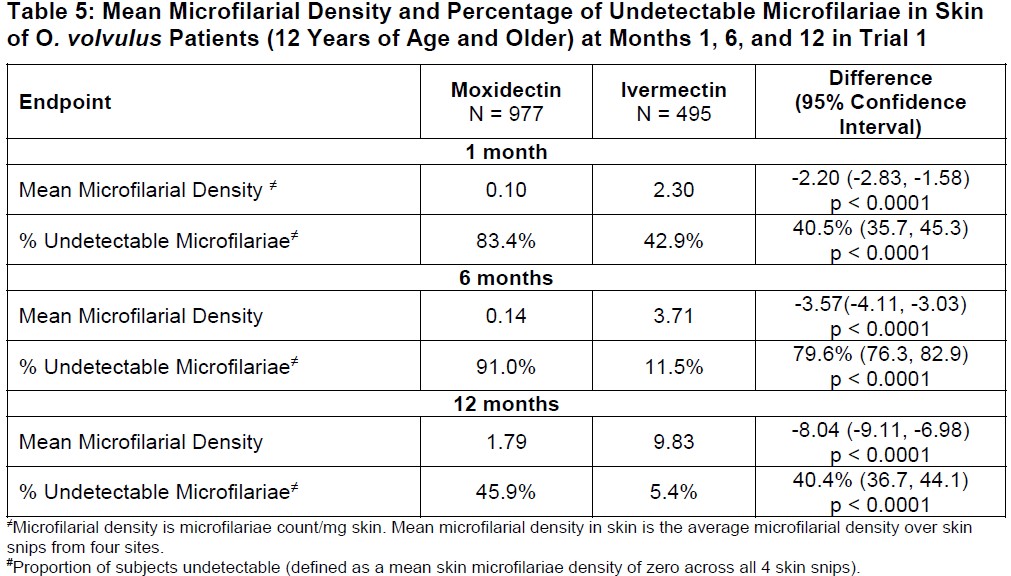
Additionally, safety and efficacy was assessed in a smaller single ascending dose trial (Trial 2, NCT 00300768)
comparing 2 mg (n = 44), 4 mg (n = 45) (2 mg and 4 mg are not approved doses) and 8 mg (n = 38) single
doses of moxidectin to ivermectin. Trial 2 was conducted in Ghana in adults aged ≥ 18 to ≤ 60 years with
O. volvulus infection. Analysis of the baseline-to-12-month change in skin microfilarial density for the proposed
moxidectin 8 mg dose showed statistically significant superiority to ivermectin, p < 0.001. -
16 HOW SUPPLIED/STORAGE AND HANDLING
Moxidectin Tablets containing 2 mg moxidectin are white to pale yellow uncoated oval-shaped tablets,
debossed on one side with “AKKA”. Each high-density polyethylene bottle contains 500 tablets
(NDC: 71705-050-01), a silica gel desiccant and polyester coil.
Store below 30°C (86°F).
Protect from light.
Once open, the full contents of the container should be used within 24 hours with any unused content
discarded. -
17 PATIENT COUNSELING INFORMATION
Signs and Symptoms Associated with Microfilarial Death
Advise patients that they are likely to have flu like symptoms including malaise, myalgia, headache,
tachycardia, hypotension and pruritus, most commonly during the first week after treatment.
Symptomatic Orthostatic Hypotension
Advise patients that if they feel dizzy, faint or light-headed after taking Moxidectin Tablets, they should lie down
until the symptoms resolve.
Absence of Macrofilarial Activity
Advise patients that treatment with Moxidectin Tablets does not kill adult O. volvulus and that follow up
evaluation is usually required.
Edema and Worsening of Onchodermatitis
Advise patients with hyper-reactive onchodermatitis that they may be more likely to experience severe adverse
reactions.
Encephalopathy in Loa loa Co-infected Patients
Advise patients to report any symptoms of encephalopathy to their healthcare provider. - PRINCIPAL DISPLAY PANEL
-
INGREDIENTS AND APPEARANCE
MOXIDECTIN
moxidectin tabletProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 71705-050 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength MOXIDECTIN (UNII: NGU5H31YO9) (MOXIDECTIN - UNII:NGU5H31YO9) MOXIDECTIN 2 mg in 1 mg Product Characteristics Color white (White to pale yellow) Score no score Shape OVAL Size 8mm Flavor Imprint Code Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 71705-050-01 1000 mg in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 12/02/2019 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA210867 12/02/2019 Labeler - Medicines Development Limited (trading as Medicines Development for Global Health) (754191398)
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.