TOPIRAMATE tablet, film coated
topiramate by
Drug Labeling and Warnings
topiramate by is a Prescription medication manufactured, distributed, or labeled by Unichem Pharmaceuticals (USA), Inc.. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use TOPIRAMATE TABLETS safely and effectively. See full prescribing information for TOPIRAMATE TABLETS.
TOPIRAMATE tablets, for oral use
Initial U.S. Approval: 1996
INDICATIONS AND USAGE
Topiramate tablets are indicated for:
- Epilepsy: initial monotherapy for the treatment of partial-onset or primary generalized tonic-clonic seizures in patients 2 years of age and older (1.1); adjunctive therapy for the treatment of partial-onset seizures, primary generalized tonic-clonic seizures, or seizures associated with Lennox-Gastaut syndrome in patients 2 years of age and older (1.2)
- Preventive treatment of migraine in patients 12 years of age and older (1.3)
DOSAGE AND ADMINISTRATION
Topiramate tablets initial dose, titration, and recommended maintenance dose varies by indication and age group. See Full Prescribing Information for recommended dosage, and dosing considerations in patients with renal impairment, geriatric patients, and patients undergoing hemodialysis (2.1, 2.2, 2.3, 2.4, 2.5, 2.6)
DOSAGE FORMS AND STRENGTHS
- Tablets: 25 mg, 50 mg, 100 mg, and 200 mg (3)
CONTRAINDICATIONS
None (4)
WARNINGS AND PRECAUTIONS
- Acute myopia and secondary angle closure glaucoma: can lead to permanent visual loss; discontinue topiramate as soon as possible (5.1)
- Visual field defects: consider discontinuation of topiramate (5.2)
- Oligohidrosis and hyperthermia: monitor decreased sweating and increased body temperature, especially in pediatric patients (5.3)
- Metabolic acidosis: baseline and periodic measurement of serum bicarbonate is recommended; consider dose reduction or discontinuation of topiramate if clinically appropriate (5.4)
- Suicidal behavior and ideation: antiepileptic drugs increase the risk of suicidal behavior or ideation (5.5)
- Cognitive/neuropsychiatric adverse reactions: use caution when operating machinery including cars; depression and mood problems may occur (5.6)
- Fetal Toxicity: use during pregnancy can cause cleft lip and/or palate and being small for gestational age (5.7)
- Withdrawal of AEDs: withdraw topiramate gradually (5.8)
- Hyperammonemia/encephalopathy: measure ammonia if encephalopathic symptoms occur (5.9)
- Kidney stones: avoid use with other carbonic anhydrase inhibitors, drugs causing metabolic acidosis, or in patients on a ketogenic diet (5.10)
- Hypothermia has been reported with and without hyperammonemia during topiramate treatment with concomitant valproic acid use (5.11)
ADVERSE REACTIONS
Epilepsy: Most common (≥10% more frequent than placebo or low-dose topiramate) adverse reactions in adult and pediatric patients were: paresthesia, anorexia, weight loss, speech disorders/related speech problems, fatigue, dizziness, somnolence, nervousness, psychomotor slowing, abnormal vision and fever (6.1)
Migraine: Most common (≥5% more frequent than placebo) adverse reactions in adult and pediatric patients were: paresthesia, anorexia, weight loss, difficulty with memory, taste perversion, diarrhea, hypoesthesia, nausea, abdominal pain and upper respiratory tract infection (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Unichem Pharmaceuticals (USA), Inc., at 1-866-562-4616 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide.
Revised: 5/2019
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
1.1 Monotherapy Epilepsy
1.2 Adjunctive Therapy Epilepsy
1.3 Migraine
2 DOSAGE AND ADMINISTRATION
2.1 Dosing in Monotherapy Epilepsy
2.2 Dosing in Adjunctive Therapy Epilepsy
2.3 Dosing for the Preventive Treatment of Migraine
2.4 Administration Information
2.5 Dosing in Patients with Renal Impairment
2.6 Dosing in Patients Undergoing Hemodialysis
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Acute Myopia and Secondary Angle Closure Glaucoma
5.2 Visual Field Defects
5.3 Oligohidrosis and Hyperthermia
5.4 Metabolic Acidosis
5.5 Suicidal Behavior and Ideation
5.6 Cognitive/Neuropsychiatric Adverse Reactions
5.7 Fetal Toxicity
5.8 Withdrawal of Antiepileptic Drugs
5.9 Hyperammonemia and Encephalopathy (Without and With Concomitant Valproic Acid Use)
5.10 Kidney Stones
5.11 Hypothermia with Concomitant Valproic Acid Use
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
6.2 Postmarketing Experience
7 DRUG INTERACTIONS
7.1 Antiepileptic Drugs
7.2 Other Carbonic Anhydrase Inhibitors
7.3 CNS Depressants
7.4 Oral Contraceptives
7.5 Hydrochlorothiazide (HCTZ)
7.6 Pioglitazone
7.7 Lithium
7.8 Amitriptyline
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.3 Females and Males of Reproductive Potential
8.4 Pediatric Use
8.5 Geriatric Use
8.6 Renal Impairment
8.7 Patients Undergoing Hemodialysis
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
14.1 Monotherapy Epilepsy
14.2 Adjunctive Therapy Epilepsy
14.3 Preventive Treatment of Migraine
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 How Supplied.
16.2 Storage and Handling.
17 PATIENT COUNSELING INFORMATION
- * Sections or subsections omitted from the full prescribing information are not listed.
-
1 INDICATIONS AND USAGE
1.1 Monotherapy Epilepsy
Topiramate tablets are indicated as initial monotherapy for the treatment of partial-onset or primary generalized tonic-clonic seizures in patients 2 years of age and older.
-
2 DOSAGE AND ADMINISTRATION
2.1 Dosing in Monotherapy Epilepsy
Adults and Pediatric Patients 10 Years of Age and Older
The recommended dose for topiramate tablets monotherapy in adults and pediatric patients 10 years of age and older is 400 mg/day in two divided doses. The dose should be achieved by titration according to the following schedule (Table 1):
Table 1: Monotherapy Titration Schedule for Adults and Pediatric Patients 10 years and older Morning Dose
Evening Dose
Week 1
25 mg
25 mg
Week 2
50 mg
50 mg
Week 3
75 mg
75 mg
Week 4
100 mg
100 mg
Week 5
150 mg
150 mg
Week 6
200 mg
200 mg
Pediatric Patients 2 to 9 Years of Age
Dosing in patients 2 to 9 years of age is based on weight. During the titration period, the initial dose of topiramate tablets is 25 mg/day nightly for the first week. Based upon tolerability, the dosage can be increased to 50 mg/day (25 mg twice daily) in the second week. Dosage can be increased by 25 to 50 mg/day each subsequent week as tolerated. Titration to the minimum maintenance dose should be attempted over 5 to 7 weeks of the total titration period. Based upon tolerability and clinical response, additional titration to a higher dose (up to the maximum maintenance dose) can be attempted at 25 to 50 mg/day weekly increments. The total daily dose should not exceed the maximum maintenance dose for each range of body weight (Table 2).
Table 2: Monotherapy Target Total Daily Maintenance Dosing for Patients 2 to 9 Years of Age Weight (kg)
Total Daily Dose (mg/day)*
Minimum Maintenance Dose
Total Daily Dose (mg/day)*
Maximum Maintenance Dose
Up to 11
150
250
12 to 22
200
300
23 to 31
200
350
32 to 38
250
350
Greater than 38
250
400
* Administered in two equally divided doses
2.2 Dosing in Adjunctive Therapy Epilepsy
Adults (17 Years of Age and Older)
The recommended total daily dose of topiramate tablets as adjunctive therapy in adults with partial-onset seizures or Lennox-Gastaut Syndrome is 200 to 400 mg/day in two divided doses, and 400 mg/day in two divided doses as adjunctive treatment in adults with primary generalized tonic-clonic seizures. Topiramate tablets should be initiated at 25 to 50 mg/day, followed by titration to an effective dose in increments of 25 to 50 mg/day every week. Titrating in increments of 25 mg/day every week may delay the time to reach an effective dose. Doses above 400 mg/day have not been shown to improve responses in adults with partial-onset seizures.
Pediatric Patients 2 to 16 Years of Age
The recommended total daily dose of topiramate tablets as adjunctive therapy for pediatric patients 2 to 16 years of age with partial-onset seizures, primary generalized tonic-clonic seizures, or seizures associated with Lennox-Gastaut syndrome is approximately 5 to 9 mg/kg/day in two divided doses. Titration should begin at 25 mg/day (or less, based on a range of 1 to 3 mg/kg/day) nightly for the first week. The dosage should then be increased at 1- or 2-week intervals by increments of 1 to 3 mg/kg/day (administered in two divided doses), to achieve optimal clinical response. Dose titration should be guided by clinical outcome. The total daily dose should not exceed 400 mg/day
2.3 Dosing for the Preventive Treatment of Migraine
The recommended total daily dose of topiramate tablets as treatment for patients 12 years of age and older for the preventive treatment of migraine is 100 mg/day administered in two divided doses (Table 3). The recommended titration rate for topiramate tablets for the preventive treatment of migraine is as follows:
Table 3: Preventive Treatment of Migraine Titration Schedule for Patients 12 Years of Age and Older Morning Dose
Evening Dose
Week 1
None
25 mg
Week 2
25 mg
25 mg
Week 3
25 mg
50 mg
Week 4
50 mg
50 mg
Dose and titration rate should be guided by clinical outcome. If required, longer intervals between dose adjustments can be used.
2.4 Administration Information
Topiramate tablets can be taken without regard to meals.
Topiramate Tablets
Because of the bitter taste, tablets should not be broken.
2.5 Dosing in Patients with Renal Impairment
In patients with renal impairment (creatinine clearance less than 70 mL/min/1.73 m2), one-half of the usual adult dose of topiramate tablets is recommended [see Use in Specific Populations 8.5 8.6), Clinical Pharmacology (12.3)].
2.6 Dosing in Patients Undergoing Hemodialysis
To avoid rapid drops in topiramate plasma concentration during hemodialysis, a supplemental dose of topiramate tablets may be required. The actual adjustment should take into account 1) the duration of dialysis period, 2) the clearance rate of the dialysis system being used, and 3) the effective renal clearance of topiramate in the patient being dialyzed [see Use in Specific Populations (8.7), Clinical Pharmacology (12.3)].
-
3 DOSAGE FORMS AND STRENGTHS
Topiramate tablets, USP are available as round, biconvex, film-coated tablets in the following strengths and colors:
25 mg: Light yellow with 'U' debossed on one side and '115' debossed on other side.
50 mg: White to off-white, bevel edged with 'U' debossed on one side and '116' debossed on other side.
100 mg: Salmon, bevel edged with 'U' debossed on one side and '117' debossed on other side.
200 mg: Yellow, bevel edged with 'U' debossed on one side and "118' debossed on other side.
- 4 CONTRAINDICATIONS
-
5 WARNINGS AND PRECAUTIONS
5.1 Acute Myopia and Secondary Angle Closure Glaucoma
A syndrome consisting of acute myopia associated with secondary angle closure glaucoma has been reported in patients receiving topiramate. Symptoms include acute onset of decreased visual acuity and/or ocular pain. Ophthalmologic findings can include myopia, anterior chamber shallowing, ocular hyperemia (redness), and increased intraocular pressure. Mydriasis may or may not be present. This syndrome may be associated with supraciliary effusion resulting in anterior displacement of the lens and iris, with secondary angle closure glaucoma. Symptoms typically occur within 1 month of initiating topiramate therapy. In contrast to primary narrow angle glaucoma, which is rare under 40 years of age, secondary angle closure glaucoma associated with topiramate has been reported in pediatric patients as well as adults. The primary treatment to reverse symptoms is discontinuation of topiramate as rapidly as possible, according to the judgment of the treating physician. Other measures, in conjunction with discontinuation of topiramate, may be helpful.
Elevated intraocular pressure of any etiology, if left untreated, can lead to serious sequelae including permanent vision loss.
5.2 Visual Field Defects
Visual field defects (independent of elevated intraocular pressure) have been reported in clinical trials and in postmarketing experience in patients receiving topiramate. In clinical trials, most of these events were reversible after topiramate discontinuation. If visual problems occur at any time during topiramate treatment, consideration should be given to discontinuing the drug.
5.3 Oligohidrosis and Hyperthermia
Oligohidrosis (decreased sweating), infrequently resulting in hospitalization, has been reported in association with topiramate use. Decreased sweating and an elevation in body temperature above normal characterized these cases. Some of the cases were reported after exposure to elevated environmental temperatures.
The majority of the reports have been in pediatric patients. Patients (especially pediatric patients) treated with topiramate should be monitored closely for evidence of decreased sweating and increased body temperature, especially in hot weather. Caution should be used when topiramate is given with other drugs that predispose patients to heat-related disorders; these drugs include, but are not limited to, other carbonic anhydrase inhibitors and drugs with anticholinergic activity.
5.4 Metabolic Acidosis
Topiramate can cause hyperchloremic, non-anion gap, metabolic acidosis (i.e., decreased serum bicarbonate below the normal reference range in the absence of chronic respiratory alkalosis). This metabolic acidosis is caused by renal bicarbonate loss due to carbonic anhydrase inhibition by topiramate. Topiramate-induced metabolic acidosis can occur at any time during treatment. Bicarbonate decrements are usually mild-moderate (average decrease of 4 mEq/L at daily doses of 400 mg in adults and at approximately 6 mg/kg/day in pediatric patients); rarely, patients can experience severe decrements to values below 10 mEq/L. Conditions or therapies that predispose patients to acidosis (such as renal disease, severe respiratory disorders, status epilepticus, diarrhea, ketogenic diet, or specific drugs) may be additive to the bicarbonate lowering effects of topiramate.
Metabolic acidosis was commonly observed in adult and pediatric patients treated with topiramate in clinical trials. The incidence of decreased serum bicarbonate in pediatric trials, for adjunctive treatment of Lennox-Gastaut syndrome or refractory partial-onset seizures was as high as 67% for topiramate (at approximately 6 mg/kg/day), and 10% for placebo. The incidence of a markedly abnormally low serum bicarbonate (i.e., absolute value < 17 mEq/L and >5 mEq/L decrease from pretreatment) in these trials was up to 11%, compared to < 2% for placebo.
Manifestations of acute or chronic metabolic acidosis may include hyperventilation, nonspecific symptoms such as fatigue and anorexia, or more severe sequelae including cardiac arrhythmias or stupor. Chronic, untreated metabolic acidosis may increase the risk for nephrolithiasis or nephrocalcinosis, and may also result in osteomalacia (referred to as rickets in pediatric patients) and/or osteoporosis with an increased risk for fractures [see Warnings and Precautions (5.10)]. Chronic metabolic acidosis in pediatric patients may also reduce growth rates, which may decrease the maximal height achieved. The effect of topiramate on growth and bone-related sequelae has not been systematically investigated in long-term, placebo-controlled trials. Long-term, open-label treatment of pediatric patients 1 to 24 months old with intractable partial epilepsy, for up to 1 year, showed reductions from baseline in length, weight, and head circumference compared to age and sex-matched normative data, although these patients with epilepsy are likely to have different growth rates than normal 1 to 24 month old pediatrics. Reductions in length and weight were correlated to the degree of acidosis [see Use in Specific Populations (8.4)]. Topiramate treatment that causes metabolic acidosis during pregnancy can possibly produce adverse effects on the fetus and might also cause metabolic acidosis in the neonate from possible transfer of topiramate to the fetus [see Warnings and Precautions (5.7), Use in Specific Populations (8.1)].
Measurement of Serum Bicarbonate in Epilepsy and Migraine Patients
Measurement of baseline and periodic serum bicarbonate during topiramate treatment is recommended. If metabolic acidosis develops and persists, consideration should be given to reducing the dose or discontinuing topiramate (using dose tapering). If the decision is made to continue patients on topiramate in the face of persistent acidosis, alkali treatment should be considered.
5.5 Suicidal Behavior and Ideation
Antiepileptic drugs (AEDs), including topiramate, increase the risk of suicidal thoughts or behavior in patients taking these drugs for any indication. Patients treated with any AED for any indication should be monitored for the emergence or worsening of depression, suicidal thoughts or behavior, and/or any unusual changes in mood or behavior.
Pooled analyses of 199 placebo-controlled clinical trials (mono- and adjunctive therapy) of 11 different AEDs showed that patients randomized to one of the AEDs had approximately twice the risk (adjusted Relative Risk 1.8, 95% CI:1.2, 2.7) of suicidal thinking or behavior compared to patients randomized to placebo. In these trials, which had a median treatment duration of 12 weeks, the estimated incidence rate of suicidal behavior or ideation among 27,863 AED-treated patients was 0.43%, compared to 0.24% among 16,029 placebo-treated patients, representing an increase of approximately one case of suicidal thinking or behavior for every 530 patients treated. There were four suicides in drug-treated patients in the trials and none in placebo-treated patients, but the number is too small to allow any conclusion about drug effect on suicide.
The increased risk of suicidal thoughts or behavior with AEDs was observed as early as one week after starting drug treatment with AEDs and persisted for the duration of treatment assessed. Because most trials included in the analysis did not extend beyond 24 weeks, the risk of suicidal thoughts or behavior beyond 24 weeks could not be assessed.
The risk of suicidal thoughts or behavior was generally consistent among drugs in the data analyzed. The finding of increased risk with AEDs of varying mechanisms of action and across a range of indications suggests that the risk applies to all AEDs used for any indication. The risk did not vary substantially by age (5 to 100 years) in the clinical trials analyzed.
Table 4 shows absolute and relative risk by indication for all evaluated AEDs.
Table 4: Risk by Indication for Antiepileptic Drugs in the Pooled Analysis Indication
Placebo Patients with Events per 1000 Patients
Drug Patients with Events per 1000 Patients
Relative Risk: Incidence of Events in Drug Patients/
Incidence in Placebo Patients
Risk Difference: Additional Drug Patients with Events per 1000 Patients
Epilepsy
1.0
3.4
3.5
2.4
Psychiatric
5.7
8.5
1.5
2.9
Other
1.0
1.8
1.9
0.9
Total
2.4
4.3
1.8
1.9
The relative risk for suicidal thoughts or behavior was higher in clinical trials for epilepsy than in clinical trials for psychiatric or other conditions, but the absolute risk differences were similar for the epilepsy and psychiatric indications.
Anyone considering prescribing topiramate or any other AED must balance the risk of suicidal thoughts or behavior with the risk of untreated illness. Epilepsy and many other illnesses for which AEDs are prescribed are themselves associated with morbidity and mortality and an increased risk of suicidal thoughts and behavior. Should suicidal thoughts and behavior emerge during treatment, the prescriber needs to consider whether the emergence of these symptoms in any given patient may be related to the illness being treated.
5.6 Cognitive/Neuropsychiatric Adverse Reactions
Topiramate can cause cognitive/neuropsychiatric adverse reactions. The most frequent of these can be classified into three general categories: 1) Cognitive-related dysfunction (e.g., confusion, psychomotor slowing, difficulty with concentration/attention, difficulty with memory, speech or language problems, particularly word-finding difficulties); 2) Psychiatric/behavioral disturbances (e.g., depression or mood problems); and 3) Somnolence or fatigue.
Adult Patients
Cognitive-Related Dysfunction
Rapid titration rate and higher initial dose were associated with higher incidences of cognitive-related dysfunction.
In adult epilepsy adjunctive controlled trials, which used rapid titration (100 to 200 mg/day weekly increments), and target topiramate doses of 200 mg to 1000 mg/day, 56% of patients in the 800 mg/day and 1000 mg/day dose groups experienced cognitive-related dysfunction compared to approximately 42% of patients in the 200 to 400 mg/day groups and 14% for placebo. In this rapid titration regimen, these dose-related adverse reactions began in the titration or in the maintenance phase, and in some patients these events began during titration and persisted into the maintenance phase.
In the monotherapy epilepsy controlled trial, the proportion of patients who experienced one or more cognitive-related adverse reactions was 19% for topiramate 50 mg/day and 26% for 400 mg/day.
In the 6-month controlled trials for the preventive treatment of migraine, which used a slower titration regimen (25 mg/day weekly increments), the proportion of patients who experienced one or more cognitive-related adverse reactions was 19% for topiramate 50 mg/day, 22% for 100 mg/day (the recommended dose), 28% for 200 mg/day, and 10% for placebo. Cognitive adverse reactions most commonly developed during titration and sometimes persisted after completion of titration.
Psychiatric/Behavioral Disturbances
Psychiatric/behavioral disturbances (e.g., depression, mood) were dose-related for both the adjunctive epilepsy and migraine populations [see Warnings and Precautions (5.5)].
Somnolence/Fatigue
Somnolence and fatigue were the adverse reactions most frequently reported during clinical trials of topiramate for adjunctive epilepsy. For the adjunctive epilepsy population, the incidence of fatigue, appeared dose related. For the monotherapy epilepsy population, the incidence of somnolence was dose-related. For the migraine population, the incidences of both fatigue and somnolence were dose-related and more common in the titration phase.
Pediatric Patients
In pediatric epilepsy trials (adjunctive and monotherapy), the incidence of cognitive/neuropsychiatric adverse reactions was generally lower than that observed in adults. These reactions included psychomotor slowing, difficulty with concentration/attention; speech disorders/related speech problems, and language problems. The most frequently reported cognitive/neuropsychiatric reactions in pediatric epilepsy patients during adjunctive therapy double-blind studies were somnolence and fatigue. The most frequently reported cognitive/neuropsychiatric reactions in pediatric epilepsy patients in the 50 mg/day and 400 mg/day groups during the monotherapy double-blind study were headache, dizziness, anorexia, and somnolence.
In pediatric migraine patients, the incidence of cognitive/neuropsychiatric adverse reactions was increased in topiramate-treated patients compared to placebo.
The risk for cognitive/neuropsychiatric adverse reactions was dose-dependent, and was greatest at the highest dose (200 mg). This risk for cognitive/neuropsychiatric adverse reactions was also greater in younger patients (6 to 11 years of age) than in older patients (12 to 17 years of age). The most common cognitive/neuropsychiatric adverse reaction in these trials was difficulty with concentration/attention. Cognitive adverse reactions most commonly developed during titration and sometimes persisted for various durations after completion of titration.
The Cambridge Neuropsychological Test Automated Battery (CANTAB) was administered to adolescents (12 to 17 years) to assess the effects of topiramate on cognitive function at baseline and at the end of the Study 13 [see Clinical Studies (14.3)]. Mean change from baseline in certain CANTAB tests suggests that topiramate treatment may result in psychomotor slowing and decreased verbal fluency.
5.7 Fetal Toxicity
Topiramate can cause fetal harm when administered to a pregnant woman. Data from pregnancy registries indicate that infants exposed to topiramate in utero have an increased risk for cleft lip and/or cleft palate (oral clefts) and for being small for gestational age (SGA). When multiple species of pregnant animals received topiramate at clinically relevant doses, structural malformations, including craniofacial defects, and reduced fetal weights occurred in offspring [see Use in Specific Populations (8.1)].
Consider the benefits and the risks of topiramate when administering this drug in women of childbearing potential, particularly when topiramate is considered for a condition not usually associated with permanent injury or death [see Use in Specific Populations (8.1), Patient Counseling Information (17)]. Topiramate should be used during pregnancy only if the potential benefit outweighs the potential risk. If this drug is used during pregnancy, or if the patient becomes pregnant while taking this drug, the patient should be apprised of the potential hazard to a fetus [see Use in Specific Populations (8.1).
5.8 Withdrawal of Antiepileptic Drugs
In patients with or without a history of seizures or epilepsy, antiepileptic drugs, including topiramate, should be gradually withdrawn to minimize the potential for seizures or increased seizure frequency [see Clinical Studies (14)]. In situations where rapid withdrawal of topiramate is medically required, appropriate monitoring is recommended.
5.9 Hyperammonemia and Encephalopathy (Without and With Concomitant Valproic Acid Use)
Topiramate treatment can cause hyperammonemia with or without encephalopathy [see Adverse Reactions (6.2)]. The risk for hyperammonemia with topiramate appears dose-related. Hyperammonemia has been reported more frequently when topiramate is used concomitantly with valproic acid. Postmarketing cases of hyperammonemia with or without encephalopathy have been reported with topiramate and valproic acid in patients who previously tolerated either drug alone [see Drug Interactions (7.1)].
Clinical symptoms of hyperammonemic encephalopathy often include acute alterations in level of consciousness and/or cognitive function with lethargy and/or vomiting. In most cases, hyperammonemic encephalopathy abated with discontinuation of treatment.
The incidence of hyperammonemia in pediatric patients 12 to 17 years of age in the preventive treatment of migraine trials was 26% in patients taking topiramate monotherapy at 100 mg/day, and 14% in patients taking topiramate at 50 mg/day, compared to 9% in patients taking placebo. There was also an increased incidence of markedly increased hyperammonemia at the 100 mg dose.
Dose-related hyperammonemia was also seen in pediatric patients 1 to 24 months of age treated with topiramate and concomitant valproic acid for partial-onset epilepsy and this was not due to a pharmacokinetic interaction.
In some patients, hyperammonemia can be asymptomatic.
Monitoring for Hyperammonemia
Patients with inborn errors of metabolism or reduced hepatic mitochondrial activity may be at an increased risk for hyperammonemia with or without encephalopathy. Although not studied, topiramate treatment or an interaction of concomitant topiramate and valproic acid treatment may exacerbate existing defects or unmask deficiencies in susceptible persons.
In patients who develop unexplained lethargy, vomiting or changes in mental status associated with any topiramate treatment, hyperammonemic encephalopathy should be considered and an ammonia level should be measured.
5.10 Kidney Stones
Topiramate increases the risk of kidney stones. During adjunctive epilepsy trials, the risk for kidney stones in topiramate-treated adults was 1.5%, an incidence about 2 to 4 times greater than expected in a similar, untreated population. As in the general population, the incidence of stone formation among topiramate-treated patients was higher in men. Kidney stones have also been reported in pediatric patients taking topiramate for epilepsy or migraine. During long-term (up to 1 year) topiramate treatment in an open-label extension study of 284 pediatric patients 1-24 months old with epilepsy, 7% developed kidney or bladder stones. Topiramate is not approved for treatment of epilepsy in pediatric patients less than 2 years old [see Use in Specific Populations (8.4)].
Topiramate is a carbonic anhydrase inhibitor. Carbonic anhydrase inhibitors can promote stone formation by reducing urinary citrate excretion and by increasing urinary pH [see Warnings and Precautions (5.4)]. The concomitant use of topiramate with any other drug producing metabolic acidosis, or potentially in patients on a ketogenic diet, may create a physiological environment that increases the risk of kidney stone formation, and should therefore be avoided.
Increased fluid intake increases the urinary output, lowering the concentration of substances involved in stone formation. Hydration is recommended to reduce new stone formation.
5.11 Hypothermia with Concomitant Valproic Acid Use
Hypothermia, defined as a drop in body core temperature to <35°C (95°F), has been reported in association with topiramate use with concomitant valproic acid both in conjunction with hyperammonemia and in the absence of hyperammonemia. This adverse reaction in patients using concomitant topiramate and valproate can occur after starting topiramate treatment or after increasing the daily dose of topiramate [see Drug Interactions (7.1)]. Consideration should be given to stopping topiramate or valproate in patients who develop hypothermia, which may be manifested by a variety of clinical abnormalities including lethargy, confusion, coma, and significant alterations in other major organ systems such as the cardiovascular and respiratory systems. Clinical management and assessment should include examination of blood ammonia levels.
-
6 ADVERSE REACTIONS
The following serious adverse reactions are discussed in more detail in other sections of the labeling:
- Acute Myopia and Secondary Angle Closure Glaucoma [see Warnings and Precautions (5.1)]
- Visual Field Defects [see Warnings and Precautions (5.2)]
- Oligohidrosis and Hyperthermia [see Warnings and Precautions (5.3)]
- Metabolic Acidosis [see Warnings and Precautions (5.4)]
- Suicidal Behavior and Ideation [see Warnings and Precautions (5.5)]
- Cognitive/Neuropsychiatric Adverse Reactions [see Warnings and Precautions (5.6)]
- Hyperammonemia and Encephalopathy (Without and With Concomitant Valproic Acid [VPA] Use) [see Warnings and Precautions (5.9)]
- Kidney Stones [see Warnings and Precautions (5.10)]
- Hypothermia with Concomitant Valproic Acid (VPA) Use [see Warnings and Precautions (5.11)]
The data described in the following sections were obtained using topiramate tablets.
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, the incidence of adverse reactions observed in the clinical trials of a drug cannot be directly compared to the incidence of adverse reactions in the clinical trials of another drug, and may not reflect the incidence of adverse reactions observed in practice.
Monotherapy Epilepsy
Adults 16 Years of Age and Older
The most common adverse reactions in the controlled clinical trial (Study 1) that occurred in adults in the 400 mg/day topiramate group and at an incidence higher (≥ 10 %) than in the 50 mg/day group were: paresthesia, weight loss and anorexia (see Table 5).
Approximately 21% of the 159 adult patients in the 400 mg/day group who received topiramate as monotherapy in study 1 discontinued therapy due to adverse reactions. The most common (≥ 2% more frequent than low-dose 50 mg/day topiramate) adverse reactions causing discontinuation were difficulty with memory, fatigue, asthenia, insomnia, somnolence, and paresthesia.
Pediatric Patients 6 to 15 Years of Age
The most common adverse reactions in the controlled clinical trial (Study 1) that occurred in pediatric patients in the 400 mg/day topiramate group and at an incidence higher (≥10%) than in the 50 mg/day group were fever and weight loss (see Table 5).
Approximately 14% of the 77 pediatric patients in the 400 mg/day group who received topiramate as monotherapy in the controlled clinical trial discontinued therapy due to adverse reactions. The most common (≥2% more frequent than low-dose 50 mg/day topiramate) adverse reactions resulting in discontinuation were difficulty with concentration/attention, fever, flushing, and confusion.
Table 5 presents the incidence of adverse reactions occurring in at least 3% of adult and pediatric patients treated with 400 mg/day topiramate and occurring with greater incidence than 50 mg/day topiramate.
Table 5: Adverse Reactions in the High Dose Group As Compared to the Low Dose Group, in Monotherapy Epilepsy Trials (Study 1) in Adult and Pediatric Patients Body System
Adverse Reaction
Age Group
Pediatric (6 to 15 Years)
Adult (Age ≥16 Years)
Topiramate Daily Dosage Group (mg/day)
50
400
50
400
(N = 74)
(N = 77)
(N = 160)
(N = 159)
%*
%*
%*
%*
Body as a Whole-General Disorders
Asthenia
0
3
4
6
Fever
1
12
Leg pain
2
3
Central & Peripheral Nervous System Disorders
Paresthesia
3
12
21
40
Dizziness
13
14
Ataxia
3
4
Hypoesthesia
4
5
Hypertonia
0
3
Involuntary muscle contractions
0
3
Vertigo
0
3
Gastro-Intestinal System Disorders
Constipation
1
4
Diarrhea
8
9
Gastritis
0
3
Dry mouth
1
3
Liver and Biliary System Disorders
Increase in Gamma-GT
1
3
Metabolic and Nutritional Disorders
Weight loss
7
17
6
17
Platelet, Bleeding & Clotting Disorders
Epistaxis
0
4
Psychiatric Disorders
Anorexia
4
14
Anxiety
4
6
Cognitive problems
1
6
1
4
Confusion
0
3
Depression
0
3
7
9
Difficulty with concentration or attention
7
10
7
8
Difficulty with memory
1
3
6
11
Insomnia
8
9
Descrease in libido
0
3
Mood problems
1
8
2
5
Personality disorder (behaviour problems)
0
3
Psychomotor slowing
3
5
Somnolence
10
15
Red Blood Cell Disorders
Anemia
1
3
Reproductive Disorders, Female
Intermenstrual bleeding
0
3
Vaginal hemorrhage
0
3
Resistance Mechanism Disorders
Infection
3
8
2
3
Viral infection
3
6
6
8
Respiratory System Disorders
Bronchitis
1
5
3
4
Upper respiratory tract infection
16
18
Rhinitis
5
6
2
4
Sinusitis
1
4
Skin and Appendages Disorders
Alopecia
1
4
3
4
Pruritus
1
4
Rash
3
4
1
4
Acne
2
3
Special Senses Other, Disorders
Taste perversion
3
5
Urinary System Disorders
Cystitis
1
3
Micturition frequency
0
3
Renal calculus
0
3
Urinary incontinence
1
3
Vascular (Extracardiac) Disorders
Flushing
0
5
Adults 16 Years of Age and Older
In pooled controlled clinical trials in adults with partial-onset seizures, primary generalized tonic-clonic seizures, or Lennox-Gastaut syndrome, 183 patients received adjunctive therapy with topiramate at dosages of 200 to 400 mg/day (recommended dosage range) and 291 patients received placebo. Patients in these trials were receiving 1 to 2 concomitant antiepileptic drugs in addition to topiramate or placebo.
The most common adverse reactions in the controlled clinical trial that occurred in adult patients in the 200 to 400 mg/day topiramate group with an incidence higher (≥ 10 %) than in the placebo group were: dizziness, speech disorders/related speech problems, somnolence, nervousness, psychomotor slowing, and vision abnormal (Table 6).
Table 6 presents the incidence of adverse reactions occurring in at least 3% of adult patients treated with 200 to 400 mg/day topiramate and was greater than placebo incidence. The incidence of some adverse reactions (e.g., fatigue, dizziness, paresthesia, language problems, psychomotor slowing, depression, difficulty with concentration/attention, mood problems) was dose-related and much greater at higher than recommended topiramate dosing (i.e., 600 mg to 1000 mg daily) compared to the incidence of these adverse reactions at the recommended dosing (200 mg to 400 mg daily) range.
Table 6: Most Common Adverse Reactions in Pooled Placebo-Controlled, Adjunctive Epilepsy Trials in Adultsa Body System/
Adverse Reaction
Placebo
(N = 291)
Topiramate Dosage
(mg/day)
200-400
(N = 183)
Body as a Whole-General Disorders
Fatigue
13
15
Asthenia
1
6
Back pain
4
5
Chest pain
3
4
Influenza-like symptoms
2
3
Central & Peripheral Nervous System Disorders
Dizziness
15
25
Ataxia
7
16
Speech disorders/ Related speech problems
2
13
Paresthesia
4
11
Nystagmus
7
10
Tremor
6
9
Language problems
1
6
Coordination abnormal
2
4
Gait abnormal
1
3
Gastro-Intestinal System Disorders
Nausea
8
10
Dyspepsia
6
7
Abdominal pain
4
6
Constipation
2
4
Metabolic and Nutritional Disorders
Weight loss
3
9
Psychiatric Disorders
Somnolence
12
29
Nervousness
6
16
Psychomotor slowing
2
13
Difficulty with memory
3
12
Confusion
5
11
Anorexia
4
10
Difficulty with concentration/attention
2
6
Mood problems
2
4
Agitation
2
3
Aggressive reaction
2
3
Emotional lability
1
3
Cognitive problems
1
3
Reproductive Disorders
Breast pain
2
4
Respiratory System Disorders
Rhinitis
6
7
Pharyngitis
2
6
Sinusitis
4
5
Vision Disorders
Vision abnormal
2
13
Diplopia
5
10
a = Patients in these adjunctive trials were receiving 1 to 2 concomitant antiepileptic drugs in addition to topiramate or placebo
In controlled clinical trials in adults, 11% of patients receiving topiramate 200 to 400 mg/day as adjunctive therapy discontinued due to adverse reactions. This rate appeared to increase at dosages above 400 mg/day. Adverse reactions associated with discontinuing topiramate included somnolence, dizziness, anxiety, difficulty with concentration or attention, fatigue, and paresthesia and increased at dosages above 400 mg/day.
Pediatric Patients 2 to 15 Years of Age
In pooled, controlled clinical trials in pediatric patients (2 to 15 years of age) with partial-onset seizures, primary generalized tonic-clonic seizures, or Lennox-Gastaut syndrome, 98 patients received adjunctive therapy with topiramate at dosages of 5 to 9 mg/kg/day (recommended dose range) and 101 patients received placebo.
The most common adverse reactions in the controlled clinical trial that occurred in pediatric patients in the 5 mg to 9 mg/kg/day topiramate group with an incidence higher (≥ 10 %) than in the placebo group were: fatigue and somnolence (Table 7).
Table 7 presents the incidence of adverse reactions that occurred in at least 3% of pediatric patients 2 to 15 years of age receiving 5 mg to 9 mg/kg/day (recommended dose range) of topiramate and was greater than placebo incidence
Table 7: Adverse Reactions in Pooled Placebo-Controlled, Adjunctive Epilepsy Trials in Pediatric Patients 2 to 15 Years of Agea, b Body System /
Adverse Reaction
Placebo
(N=101)
%
Topiramate
(N=98)
%
Body as a Whole - General Disorders
Fatigue
5
16
Injury
13
14
Central & Peripheral Nervous System Disorders
Gait abnormal
5
8
Ataxia
2
6
Hyperkinesia
4
5
Dizziness
2
4
Speech disorders/Related speech problems
2
4
Gastro-Intestinal System Disorders
Nausea
5
6
Saliva increased
4
6
Constipation
4
5
Gastroenteritis
2
3
Metabolic and Nutritional Disorders
Weight loss
1
9
Platelet, Bleeding, & Clotting Disorders
Purpura
4
8
Epistaxis
1
4
Psychiatric Disorders
Somnolence
16
26
Anorexia
15
24
Nervousness
7
14
Personality disorder (behavior problems)
9
11
Difficulty with concentration/attention
2
10
Aggressive reaction
4
9
Insomnia
7
8
Difficulty with memory
0
5
Confusion
3
4
Psychomotor slowing
2
3
Resistance Mechanism Disorders
Infection viral
3
7
Respiratory System Disorders
Pneumonia
1
5
Skin and Appendages Disorders
Skin disorder
2
3
Urinary System Disorders
Urinary incontinence
2
4
a = Patients in these adjunctive trials were receiving 1 to 2 concomitant antiepileptic drugs in addition to topiramate or placebo.
b = Values represent the percentage of patients reporting a given adverse reaction. Patients may have reported more than one adverse reaction during the study and can be included in more than one adverse reaction category.
None of the pediatric patients who received topiramate adjunctive therapy at 5 to 9 mg/kg/day in controlled clinical trials discontinued due to adverse reactions.
Migraine
Adults
In the four multicenter, randomized, double-blind, placebo-controlled, parallel group migraine clinical trials for the preventive treatment of migraine (which included 35 pediatric patients 12 to 15 years of age), most adverse reactions occurred more frequently during the titration period than during the maintenance period.
The most common adverse reactions with topiramate 100 mg in the clinical trials for the preventive treatment of migraine of predominantly adults that were seen at an incidence higher (≥ 5 %) than in the placebo group were: paresthesia, anorexia, weight loss, taste perversion, diarrhea, difficulty with memory, hypoesthesia, and nausea (see Table 8).
Table 8 includes those adverse reactions that occurred in the placebo-controlled trials where the incidence in any topiramate treatment group was at least 3% and was greater than that for placebo patients. The incidence of some adverse reactions (e.g., fatigue, dizziness, somnolence, difficulty with memory, difficulty with concentration/attention) was dose-related and greater at higher than recommended topiramate dosing (200 mg daily) compared to the incidence of these adverse reactions at the recommended dosing (100 mg daily).
Table 8: Adverse Reactions in Pooled, Placebo-Controlled, Migraine Trials in Adultsa,b Body System / Adverse Reaction
Placebo
(N=445)
%
Topiramate Dosage (mg/day)
50
(N=235)
%
100
(N=386)
%
Body as a Whole-General Disorders
Fatigue
11
14
15
Injury
7
9
6
Central & Peripheral Nervous System Disorders
Paresthesia
6
35
51
Dizziness
10
8
9
Hypoesthesia
2
6
7
Language problems
2
7
6
Gastro-Intestinal System Disorders
Nausea
8
9
13
Diarrhea
4
9
11
Abdominal pain
5
6
6
Dyspepsia
3
4
5
Dry mouth
2
2
3
Gastroenteritis
1
3
3
Metabolic and Nutritional Disorders
Weight loss
1
6
9
Musculoskeletal System Disorders
Arthralgia
2
7
3
Psychiatric Disorders
Anorexia
6
9
15
Somnolence
5
8
7
Difficulty with memory
2
7
7
Insomnia
5
6
7
Difficulty with concentration/attention
2
3
6
Mood problems
2
3
6
Anxiety
3
4
5
Depression
4
3
4
Nervousness
2
4
4
Confusion
2
2
3
Psychomotor slowing
1
3
2
Reproductive Disorders, Female
Menstrual disorder
2
3
2
Reproductive Disorders, Male
Ejaculation premature
0
3
0
Resistance Mechanism Disorders
Viral infection
3
4
4
Respiratory System Disorders
Upper respiratory tract infection
12
13
14
Sinusitis
6
10
6
Pharyngitis
4
5
6
Coughing
2
2
4
Bronchitis
2
3
3
Dyspnea
2
1
3
Skin and Appendages Disorders
Pruritis
2
4
2
Special Sense Other, Disorders
Taste perversion
1
15
8
Urinary System Disorders
Urinary tract infection
2
4
2
Vision Disorders
Blurred visionc
2
4
2
a = Includes 35 adolescent patients age 12 to 15 years.
b = Values represent the percentage of patients reporting a given adverse reaction. Patients may have reported more than one adverse reaction during the study and can be included in more than one adverse reaction category.
c = Blurred vision was the most common term considered as vision abnormal. Blurred vision was an included term that accounted for >50% of reactions coded as vision abnormal, a preferred term.
Of the 1,135 patients exposed to topiramate in the adult placebo-controlled studies, 25% of topiramate-treated patients discontinued due to adverse reactions, compared to 10% of the 445 placebo-treated patients. The adverse reactions associated with discontinuing therapy in the topiramate -treated patients included paresthesia (7%), fatigue (4%), nausea (4%), difficulty with concentration/attention (3%), insomnia (3%), anorexia (2%), and dizziness (2%).
Patients treated with topiramate experienced mean percent reductions in body weight that were dose-dependent. This change was not seen in the placebo group. Mean changes of 0%, -2%, -3%, and -4% were seen for the placebo group, topiramate 50, 100, and 200 mg groups, respectively.
Pediatric Patients 12 to 17 Years of Age
In five, randomized, double-blind, placebo-controlled, parallel group clinical trials for the preventive treatment of migraine, most adverse reactions occurred more frequently during the titration period than during the maintenance period. Among adverse reactions with onset during titration, approximately half persisted into the maintenance period.
In four, fixed-dose, double-blind clinical trials for the preventive treatment of migraine in topiramate-treated pediatric patients 12 to 17 years of age, the most common adverse reactions with topiramate 100 mg that were seen at an incidence higher (≥5%) than in the placebo group were: paresthesia, upper respiratory tract infection, anorexia, and abdominal pain (see Table 9). Table 9 shows adverse reactions from the pediatric trial (Study 13 [see Clinical Studies (14.3)]) in which 103 pediatric patients were treated with placebo or 50 mg or 100 mg of topiramate, and three predominantly adult trials in which 49 pediatric patients (12 to 17 years of age) were treated with placebo or 50 mg, 100 mg or 200 mg of topiramate. Table 9 also shows adverse reactions in pediatric patients in the controlled migraine trials when the incidence in a topiramate dose group was at least 5 % or higher and greater than the incidence of placebo. Many adverse reactions shown in Table 9 indicate a dose-dependent relationship. The incidence of some adverse reactions (e.g., allergy, fatigue, headache, anorexia, insomnia, somnolence, and viral infection) was dose-related and greater at higher than recommended topiramate dosing (200 mg daily) compared to the incidence of these adverse reactions at the recommended dosing (100 mg daily).
Table 9: Adverse Reactions in Pooled Double-Blind Migraine Prophylaxis Studies for the Preventive Treatment of Migraine in Pediatric Patients 12 to 17 Years of Agea,b,c Topiramate Dosage
Body System /
Adverse Reaction
Placebo
(N=45)
%
50 mg/day
(N=46)
%
100 mg/day
(N=48)
%
Body as a Whole – General Disorders
Fatigue
7
7
8
Fever
2
4
6
Central & Peripheral Nervous System Disorders
Paresthesia
7
20
19
Dizziness
4
4
6
Gastrointestinal System Disorders
Abdominal pain
9
7
15
Nausea
4
4
8
Metabolic and Nutritional Disorders
Weight loss
2
7
4
Psychiatric Disorders
Anorexia
4
9
10
Somnolence
2
2
6
Insomnia
2
9
2
Resistance Mechanism Disorders
Infection viral
4
4
8
Respiratory System Disorders
Upper respiratory tract infection
11
26
23
Rhinitis
2
7
6
Sinusitis
2
9
4
Coughing
0
7
2
Special Senses Other, Disorders
Taste perversion
2
2
6
Vision Disorders
Conjunctivitis
4
7
4
a = 35 adolescent patients aged 12 to <16 years were also included in adverse reaction assessment for adults
(Tables 10 and 11)
b = Incidence is based on the number of subjects experiencing at least 1 adverse event, not the number of events.
c = Included studies MIG-3006, MIGR-001, MIGR-002 and MIGR-003
In the double-blind placebo-controlled studies, adverse reactions led to discontinuation of treatment in 8% of placebo patients compared with 6% of topiramate-treated patients. Adverse reactions associated with discontinuing therapy that occurred in more than one topiramate-treated patient were fatigue (1%), headache (1%), and somnolence (1%).
Increased Risk for Bleeding
Topiramate is associated with an increased risk for bleeding. In a pooled analysis of placebo-controlled studies of approved and unapproved indications, bleeding was more frequently reported as an adverse reaction for topiramate than for placebo (4.5% versus 3.0% in adult patients, and 4.4% versus 2.3% in pediatric patients). In this analysis, the incidence of serious bleeding events for topiramate and placebo was 0.3% versus 0.2% for adult patients, and 0.4% versus 0% for pediatric patients.
Adverse bleeding reactions reported with topiramate ranged from mild epistaxis, ecchymosis, and increased menstrual bleeding to life-threatening hemorrhages. In patients with serious bleeding events, conditions that increased the risk for bleeding were often present, or patients were often taking drugs that cause thrombocytopenia (other antiepileptic drugs) or affect platelet function or coagulation (e.g., aspirin, nonsteroidal anti-inflammatory drugs, selective serotonin reuptake inhibitors, or warfarin or other anticoagulants).
Other Adverse Reactions Observed During Clinical Trials
Other adverse reactions seen during clinical trials were: abnormal coordination, eosinophilia, gingival bleeding, hematuria, hypotension, myalgia, myopia, postural hypotension, scotoma, suicide attempt, syncope, and visual field defect.
Laboratory Test Abnormalities
Adult Patients
In addition to changes in serum bicarbonate (i.e., metabolic acidosis), sodium chloride and ammonia, topiramate was associated with changes in several clinical laboratory analytes in randomized, double-blind, placebo-controlled studies [see Warnings and Precautions (5.4, 5.9)]. Controlled trials of adjunctive topiramate treatment of adults for partial-onset seizures showed an increased incidence of markedly decreased serum phosphorus (6% topiramate versus 2% placebo), markedly increased serum alkaline phosphatase (3% topiramate versus 1% placebo), and decreased serum potassium (0.4 % topiramate versus 0.1 % placebo).
Pediatric Patients
In pediatric patients (1-24 months) receiving adjunctive topiramate for partial-onset seizures, there was an increased incidence for an increased result (relative to normal analyte reference range) associated with topiramate (vs placebo) for the following clinical laboratory analytes: creatinine, BUN, alkaline phosphatase, and total protein, The incidence was also increased for a decreased result for bicarbonate (i.e., metabolic acidosis), and potassium with topiramate (vs placebo) [see Use in Specific Populations (8.4)]. Topiramate is not indicated for partial onset seizures in pediatric patients less than 2 years of age.
In pediatric patients (ranging from 6-17 years of age) receiving topiramate for the preventive treatment of migraine, there was an increased incidence for an increased result (relative to normal analyte reference range) associated with topiramate (vs placebo) for the following clinical laboratory analytes: creatinine, BUN, uric acid, chloride, ammonia, alkaline phosphatase, total protein, platelets, and eosinophils, The incidence was also increased for a decreased result for phosphorus, bicarbonate, total white blood count, and neutrophils [see Use in Specific Populations (8.4)]. Topiramate is not indicated for the preventive treatment of migraine in pediatric patients less than 12 years of age.
6.2 Postmarketing Experience
The following adverse reactions have been identified during post approval use of topiramate. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Body as a Whole-General Disorders: oligohydrosis and hyperthermia [see Warnings and Precautions (5.3)], hyperammonemia, hyperammonemic encephalopathy [see Warnings and Precautions (5.9)], hypothermia with concomitant valproic acid [see Warnings and Precautions (5.11)]
Gastrointestinal System Disorders: hepatic failure (including fatalities), hepatitis, pancreatitis
Skin and Appendage Disorders: bullous skin reactions (including erythema multiforme, Stevens- Johnson syndrome, toxic epidermal necrolysis), pemphigus
Urinary System Disorders: kidney stones, nephrocalcinosis [see Warnings and Precautions (5.4, 5.10)]
Vision Disorders: acute myopia, secondary angle closure glaucoma [see Warnings and Precautions (5.1)], maculopathy.
Hematological Disorders: decrease of the International Normalized Ratio (INR) or prothrombin time when given concomitantly with vitamin K antagonist anticoagulant medications such as warfarin.
-
7 DRUG INTERACTIONS
7.1 Antiepileptic Drugs
Concomitant administration of phenytoin or carbamazepine with topiramate resulted in a clinically significant decrease in plasma concentrations of topiramate when compared to topiramate given alone. A dosage adjustment may be needed [see Dosage and Administration (2.1), Clinical Pharmacology (12.3).]
Concomitant administration of valproic acid and topiramate has been associated with hypothermia and hyperammonemia with and without encephalopathy. Examine blood ammonia levels in patients in whom the onset of hypothermia has been reported [see Warnings and Precautions (5.9, 5.11), Clinical Pharmacology (12.3)].
7.2 Other Carbonic Anhydrase Inhibitors
Concomitant use of topiramate, a carbonic anhydrase inhibitor, with any other carbonic anhydrase inhibitor (e.g., zonisamide or acetazolamide) may increase the severity of metabolic acidosis and may also increase the risk of kidney stone formation. Therefore, patients given topiramate concomitantly with another carbonic anhydrase inhibitor should be monitored particularly closely for the appearance or worsening of metabolic acidosis [see Clinical Pharmacology (12.3)].
7.3 CNS Depressants
Concomitant administration of topiramate and alcohol or other CNS depressant drugs has not been evaluated in clinical studies. Because of the potential of topiramate to cause CNS depression, as well as other cognitive and/or neuropsychiatric adverse reactions, topiramate should be used with extreme caution if used in combination with alcohol and other CNS depressants.
7.4 Oral Contraceptives
The possibility of decreased contraceptive efficacy and increased breakthrough bleeding may occur in patients taking combination oral contraceptive products with topiramate. Patients taking estrogen-containing contraceptives should be asked to report any change in their bleeding patterns. Contraceptive efficacy can be decreased even in the absence of breakthrough bleeding [see Clinical Pharmacology (12.3)].
7.5 Hydrochlorothiazide (HCTZ)
Topiramate Cmax and AUC increased when HCTZ was added to topiramate. The clinical significance of this change is unknown. The addition of HCTZ to topiramate may require a decrease in the topiramate dose [see Clinical Pharmacology (12.3).
7.6 Pioglitazone
A decrease in the exposure of pioglitazone and its active metabolites were noted with the concurrent use of pioglitazone and topiramate in a clinical trial. The clinical relevance of these observations is unknown; however, when topiramate is added to pioglitazone therapy or pioglitazone is added to topiramate therapy, careful attention should be given to the routine monitoring of patients for adequate control of their diabetic disease state [see Clinical Pharmacology (12.3)].
7.7 Lithium
An increase in systemic exposure of lithium following topiramate doses of up to 600 mg/day can occur. Lithium levels should be monitored when co-administered with high-dose topiramate [see Clinical Pharmacology (12.3)].
7.8 Amitriptyline
Some patients may experience a large increase in amitriptyline concentration in the presence of topiramate and any adjustments in amitriptyline dose should be made according to the patient's clinical response and not on the basis of plasma levels [see Clinical Pharmacology (12.3)].
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
There is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to topiramate during pregnancy. Patients should be encouraged to enroll in the North American Antiepileptic Drug (NAAED) Pregnancy Registry if they become pregnant. This registry is collecting information about the safety of antiepileptic drugs during pregnancy. To enroll, patients can call the toll-free number 1-888-233-2334. Information about the North American Drug Pregnancy Registry can be found at http://www.aedpregnancyregistry.org/.
Risk Summary
Topiramate can cause fetal harm when administered to a pregnant woman. Data from pregnancy registries indicate that infants exposed to topiramate in utero have an increased risk for cleft lip and/or cleft palate (oral clefts) and for being SGA [see Human Data]. SGA has been observed at all doses and appears to be dose-dependent. The prevalence of SGA is greater in infants of women who received higher doses of topiramate during pregnancy. In addition, the prevalence of SGA in infants of women who continued topiramate use until later in pregnancy is higher compared to the prevalence in infants of women who stopped topiramate use before the third trimester.
In multiple animal species, topiramate produced developmental toxicity, including increased incidences of fetal malformations, in the absence of maternal toxicity at clinically relevant doses [see Animal Data].
In the U.S. general population, the estimated background risks of major birth defects and miscarriage in clinically recognized pregnancies are 2-4% and 15-20%, respectively.
Clinical Considerations
Fetal/Neonatal Adverse Reactions
Consider the benefits and risks of topiramate when prescribing this drug to women of childbearing potential, particularly when topiramate is considered for a condition not usually associated with permanent injury or death. Because of the risk of oral clefts to the fetus, which occur in the first trimester of pregnancy, all women of childbearing potential should be informed of the potential risk to the fetus from exposure to topiramate. Women who are planning a pregnancy should be counseled regarding the relative risks and benefits of topiramate use during pregnancy, and alternative therapeutic options should be considered for these patients.
Labor or Delivery
Although the effect of topiramate on labor and delivery in humans has not been established, the development of topiramate-induced metabolic acidosis in the mother and/or in the fetus might affect the fetus' ability to tolerate labor.
Topiramate treatment can cause metabolic acidosis [see Warnings and Precautions (5.4)]. The effect of topiramate-induced metabolic acidosis has not been studied in pregnancy; however, metabolic acidosis in pregnancy (due to other causes) can cause decreased fetal growth, decreased fetal oxygenation, and fetal death, and may affect the fetus' ability to tolerate labor. Pregnant patients should be monitored for metabolic acidosis and treated as in the nonpregnant state [see Warnings and Precautions (5.4)]. Newborns of mothers treated with topiramate should be monitored for metabolic acidosis because of transfer of topiramate to the fetus and possible occurrence of transient metabolic acidosis following birth.
Based on limited information, topiramate has also been associated with pre-term labor and premature delivery.
Data
Human Data
Data from pregnancy registries indicate an increased risk of oral clefts in infants exposed to topiramate during the first trimester of pregnancy. In the NAAED pregnancy registry, the prevalence of oral clefts among topiramate-exposed infants (1.1%) was higher than the prevalence of infants exposed to a reference AED (0.36%) or the prevalence of infants in mothers without epilepsy and without exposure to AEDs (0.12%). It was also higher than the background prevalence in United States (0.17%) as estimated by the Centers for Disease Control and Prevention (CDC). The relative risk of oral clefts in topiramate-exposed pregnancies in the NAAED Pregnancy Registry was 9.6 (95% Confidence Interval [CI] 4.0 to 23.0) as compared to the risk in a background population of untreated women. The UK Epilepsy and Pregnancy Register reported a prevalence of oral clefts among infants exposed to topiramate monotherapy (3.2%) that was 16 times higher than the background rate in the UK (0.2%).
Data from the NAAED pregnancy registry and a population-based birth registry cohort indicate that exposure to topiramate in utero is associated with an increased risk of SGA newborns (birth weight <10th percentile). In the NAAED pregnancy registry, 19.7% of topiramate-exposed newborns were SGA compared to 7.9% of newborns exposed to a reference AED and 5.4% of newborns of mothers without epilepsy and without AED exposure. In the Medical Birth Registry of Norway (MBRN), a population-based pregnancy registry, 25% of newborns in the topiramate monotherapy exposure group were SGA compared to 9 % in the comparison group unexposed to AEDs. The long-term consequences of the SGA findings are not known.
When topiramate (0, 20, 100, or 500 mg/kg/day) was administered to pregnant mice during the period of organogenesis, incidences of fetal malformations (primarily craniofacial defects) were increased at all doses. Fetal body weights and skeletal ossification were reduced at the highest dose tested in conjunction with decreased maternal body weight gain. A no-effect dose for embryofetal developmental toxicity in mice was not identified. The lowest dose tested, which was associated with increased malformations, is less than the maximum recommended human dose (MRHD) for epilepsy (400 mg/day) or migraine (100 mg/day) on a body surface area (mg/m2) basis.
In pregnant rats administered topiramate (0, 20, 100, and 500 mg/kg/day or 0, 0.2, 2.5, 30, and 400 mg/kg/day) orally during the period of organogenesis, the frequency of limb malformations (ectrodactyly, micromelia, and amelia) was increased in fetuses at 400 and 500 mg/kg/day. Embryotoxicity (reduced fetal body weights, increased incidences of structural variations) was observed at doses as low as 20 mg/kg/day. Clinical signs of maternal toxicity were seen at 400 mg/kg/day and above, and maternal body weight gain was reduced at doses of 100 mg/kg/day or greater. The no-effect dose (2.5 mg/kg/day) for embryofetal developmental toxicity in rats is less than the MRHD for epilepsy or migraine on a mg/m2 basis.
In pregnant rabbits administered topiramate (0, 20, 60, and 180 mg/kg/day or 0, 10, 35, and 120 mg/kg/day) orally during organogenesis, embryofetal mortality was increased at 35 mg/kg/day, and increased incidences of fetal malformations (primarily rib and vertebral malformations) were observed at 120 mg/kg/day. Evidence of maternal toxicity (decreased body weight gain, clinical signs, and/or mortality) was seen at 35 mg/kg/day and above. The no-effect dose (20 mg/kg/day) for embryofetal developmental toxicity in rabbits is equivalent to the MRHD for epilepsy and approximately 4 times the MRHD for migraine on a mg/m2 basis.
When topiramate (0, 0.2, 4, 20, and 100 mg/kg/day or 0, 2, 20, and 200 mg/kg/day) was administered orally to female rats during the latter part of gestation and throughout lactation, offspring exhibited decreased viability and delayed physical development at 200 mg/kg/day and reductions in pre-and/or postweaning body weight gain at 2 mg/kg/day and above. Maternal toxicity (decreased body weight gain, clinical signs) was evident at 100 mg/kg/day or greater. In a rat embryofetal development study which included postnatal assessment of offspring, oral administration of topiramate (0, 0.2, 2.5, 30, and 400 mg/kg) to pregnant animals during the period of organogenesis resulted in delayed physical development in offspring at 400 mg/kg/day and persistent reductions in body weight gain in offspring at 30 mg/kg/day and higher. The no-effect dose (0.2 mg/kg/day) for pre-and postnatal developmental toxicity in rats is less than the MRHD for epilepsy or migraine on a mg/m2 basis.
8.2 Lactation
Topiramate is excreted in human milk [see Data]. The effects of topiramate on milk production are unknown. Diarrhea and somnolence have been reported in breastfed infants whose mothers receive topiramate treatment.
The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for topiramate and any potential adverse effects on the breastfed infant from topiramate or from the underlying maternal condition.
Human Data
Limited data from 5 women with epilepsy treated with topiramate during lactation showed drug levels in milk similar to those in maternal plasma.
8.3 Females and Males of Reproductive Potential
Women of childbearing potential who are not planning a pregnancy should use effective contraception because of the risks of oral clefts and SGA [see Drug Interactions (7.4) and Use in Specific Populations 8.1].
8.4 Pediatric Use
Adjunctive Treatment for Partial-Onset Epilepsy in Pediatric Patients 1 to 24 months
Safety and effectiveness in patients below the age of 2 years have not been established for the adjunctive therapy treatment of partial-onset seizures, primary generalized tonic-clonic seizures, or seizures associated with Lennox-Gastaut syndrome. In a single randomized, double-blind, placebo-controlled investigational trial, the efficacy, safety, and tolerability of topiramate oral liquid and sprinkle formulations as an adjunct to concurrent antiepileptic drug therapy in pediatric patients 1 to 24 months of age with refractory partial-onset seizures were assessed. After 20 days of double-blind treatment, topiramate (at fixed doses of 5, 15, and 25 mg/kg/day) did not demonstrate efficacy compared with placebo in controlling seizures.
In general, the adverse reaction profile for topiramate in this population was similar to that of older pediatric patients, although results from the above controlled study and an open-label, long-term extension study in these pediatric patients 1 to 24 months old suggested some adverse reactions/toxicities (not previously observed in older pediatric patients and adults; i.e., growth/length retardation, certain clinical laboratory abnormalities, and other adverse reactions/toxicities that occurred with a greater frequency and/or greater severity than had been recognized previously from studies in older pediatric patients or adults for various indications.
These very young pediatric patients appeared to experience an increased risk for infections (any topiramate dose 12%, placebo 0%) and of respiratory disorders (any topiramate dose 40%, placebo 16%). The following adverse reactions were observed in at least 3% of patients on topiramate and were 3% to 7% more frequent than in patients on placebo: viral infection, bronchitis, pharyngitis, rhinitis, otitis media, upper respiratory infection, cough, and bronchospasm. A generally similar profile was observed in older pediatric patients [see Adverse Reactions (6)].
Topiramate resulted in an increased incidence of patients with increased creatinine (any topiramate dose 5%, placebo 0%), BUN (any topiramate dose 3%, placebo 0%), and protein (any topiramate dose 34%, placebo 6%), and an increased incidence of decreased potassium (any topiramate dose 7%, placebo 0%). This increased frequency of abnormal values was not dose-related. Creatinine was the only analyte showing a noteworthy increased incidence (topiramate 25 mg/kg/day 5%, placebo 0%) of a markedly abnormal increase. The significance of these findings is uncertain.
Topiramate treatment also produced a dose-related increase in the percentage of patients who had a shift from normal at baseline to high/increased (above the normal reference range) in total eosinophil count at the end of treatment. The incidence of these abnormal shifts was 6 % for placebo, 10% for 5 mg/kg/day, 9% for 15 mg/kg/day, 14% for 25 mg/kg/day, and 11% for any topiramate dose. There was a mean dose-related increase in alkaline phosphatase. The significance of these findings is uncertain.
Topiramate produced a dose-related increased incidence of hyperammonemia [see Warnings and Precautions (5.9)].
Treatment with topiramate for up to 1 year was associated with reductions in Z SCORES for length, weight, and head circumference [see Warnings and Precautions (5.4), Adverse Reactions (6)].
In open-label, uncontrolled experience, increasing impairment of adaptive behavior was documented in behavioral testing over time in this population. There was a suggestion that this effect was dose-related. However, because of the absence of an appropriate control group, it is not known if this decrement in function was treatment-related or reflects the patient's underlying disease (e.g., patients who received higher doses may have more severe underlying disease) [see Warnings and Precautions (5.6)].
In this open-label, uncontrolled study, the mortality was 37 deaths/1000 patient years. It is not possible to know whether this mortality rate is related to topiramate treatment, because the background mortality rate for a similar, significantly refractory, young pediatric population (1-24 months) with partial epilepsy is not known.
Monotherapy Treatment in Partial-Onset Epilepsy in Patients <2 Years Old
Safety and effectiveness in patients below the age of 2 years have not been established for the monotherapy treatment of epilepsy.
Preventive Treatment of Migraine in Pediatric Patients 12 to 17 Years of Age
Safety and effectiveness of topiramate for the preventive treatment of migraine was studied in 5 double-blind, randomized, placebo-controlled, parallel-group trials in a total of 219 pediatric patients, at doses of 50 to 200 mg/day, or 2 to 3 mg/kg/day. These comprised a fixed dose study in 103 pediatric patients 12 to 17 years of age [see Clinical Studies (14.3)], a flexible dose (2 to 3 mg/kg/day), placebo-controlled study in 157 pediatric patients 6 to 16 years of age (including 67 pediatric patients 12 to 16 years of age), and a total of 49 pediatric patients 12 to 17 years of age in 3 studies for the preventive treatment of migraine primarily in adults. Open-label extension phases of 3 studies enabled evaluation of long-term safety for up to 6 months after the end of the double-blind phase.
Efficacy of topiramate for the preventive treatment of migraine in pediatric patients 12 to 17 years of age is demonstrated for a 100 mg daily dose in Study 13 [see Clinical Studies (14.3)]. Efficacy of topiramate (2 to 3 mg/kg/day) for the preventive treatment of migraine was not demonstrated in a placebo- controlled trial of 157 pediatric patients (6 to 16 years of age) that included treatment of 67 pediatric patients (12 to 16 years of age) for 20 weeks.
In the pediatric trials (12 to 17 years of age) in which patients were randomized to placebo or a fixed daily dose of topiramate, the most common adverse reactions with topiramate that were seen at an incidence higher (≥5%) than in the placebo group were: paresthesia, upper respiratory tract infection, anorexia, and abdominal pain [see Adverse Reactions (6)].
The most common cognitive adverse reaction in pooled double-blind studies in pediatric patients 12 to 17 years of age was difficulty with concentration/attention [see Warnings and Precautions (5.6)].
Markedly abnormally low serum bicarbonate values indicative of metabolic acidosis were reported in topiramate-treated pediatric migraine patients [see Warnings and Precautions (5.4)].
In topiramate-treated pediatric patients (12 to 17 years of age) compared to placebo-treated patients, abnormally increased results were more frequent for creatinine, BUN, uric acid, chloride, ammonia, total protein, and platelets. Abnormally decreased results were observed with topiramate vs placebo treatment for phosphorus and bicarbonate [see Clinical Trials Experience (6.1)].
Notable changes (increases and decreases) from baseline in systolic blood pressure, diastolic blood pressure, and pulse were observed occurred more commonly in pediatric patients treated with topiramate compared to pediatric patients treated with placebo [see Clinical Pharmacology (12.2)].
Preventive treatment of Migraine in Pediatric Patients 6 to 11 Years of Age
Safety and effectiveness in pediatric patients below the age of 12 years have not been established for the preventive treatment of migraine.
In a double-blind study in 90 pediatric patients 6 to 11 years of age (including 59 topiramate-treated and 31 placebo patients), the adverse reaction profile was generally similar to that seen in pooled double-blind studies of pediatric patients 12 to 17 years of age. The most common adverse reactions that occurred in topiramate-treated pediatric patients 6 to 11 years of age, and at least twice as frequently than placebo, were gastroenteritis (12% topiramate, 6% placebo), sinusitis (10% topiramate, 3% placebo), weight loss (8% topiramate, 3% placebo) and paresthesia (7% topiramate, 0% placebo). Difficulty with concentration/attention occurred in 3 topiramate-treated patients (5%) and 0 placebo-treated patients.
The risk for cognitive adverse reaction was greater in younger patients (6 to 11 years of age) than in older patients (12 to 17 years of age) [see Warnings and Precautions (5.6)].
Juvenile Animal Studies
When topiramate (0, 30, 90, and 300 mg/kg/day) was administered orally to rats during the juvenile period of development (postnatal days 12 to 50), bone growth plate thickness was reduced in males at the highest dose. The no-effect dose (90 mg/kg/day) for adverse development effects is approximately 2 times the maximum recommended pediatric dose (9 mg/kg/day) on a body surface area (mg/m2) basis.
8.5 Geriatric Use
In clinical trials, 3% of patients were over age 60. No age-related differences in effectiveness or adverse effects were evident. However, clinical studies of topiramate did not include sufficient numbers of subjects age 65 and over to determine whether they respond differently than younger subjects. Dosage adjustment may be necessary for elderly with age-related renal impairment (creatinine clearance rate <70 mL/min/1.73 m2) resulting in reduced clearance [see Dosage and Administration (2.5), Clinical Pharmacology (12.3)].
8.6 Renal Impairment
The clearance of topiramate is reduced in patients with moderate (creatinine clearance 30 to 69 mL/min/1.73 m2) and severe (creatinine clearance <30 mL/min/1.73 m2) renal impairment. A dosage adjustment is recommended in patients with moderate or severe renal impairment [see Dosage and Administration (2.5), Clinical Pharmacology (12.3)].
-
10 OVERDOSAGE
Overdoses of topiramate have been reported. Signs and symptoms included convulsions, drowsiness, speech disturbance, blurred vision, diplopia, impaired mentation, lethargy, abnormal coordination, stupor, hypotension, abdominal pain, agitation, dizziness and depression. The clinical consequences were not severe in most cases, but deaths have been reported after overdoses involving topiramate.
Topiramate overdose has resulted in severe metabolic acidosis [see Warnings and Precautions (5.4)].
A patient who ingested a dose of topiramate between 96 and 110 g was admitted to a hospital with a coma lasting 20 to 24 hours followed by full recovery after 3 to 4 days.
In the event of overdose, topiramate tablets should be discontinued and general supportive treatment given until clinical toxicity has been diminished or resolved. Hemodialysis is an effective means of removing topiramate from the body.
-
11 DESCRIPTION
Topiramate USP is a sulfamate-substituted monosaccharide. Topiramate tablets, USP are available as 25 mg, 50 mg, 100 mg, and 200 mg round shaped tablets for oral administration.
Topiramate USP is a white crystalline powder with a bitter taste. Topiramate USP is most soluble in alkaline solutions containing sodium hydroxide or sodium phosphate and having a pH of 9 to 10. It is freely soluble in acetone, chloroform, dimethylsulfoxide, and ethanol. The solubility in water is 9.8 mg/mL. Its saturated solution has a pH of 6.3. Topiramate USP has the molecular formula C12H21NO8S and a molecular weight of 339.36. Topiramate USP is designated chemically as 2,3:4,5-Di-O-isopropylidene-β-D-fructopyranose sulfamate and has the following structural formula:
Topiramate tablets, USP contain the following inactive ingredients: lactose monohydrate, pregelatinized corn starch, microcrystalline cellulose, sodium starch glycolate Type A (Potato), magnesium stearate, hypromellose, polysorbate 80, polyethylene glycol, and titanium dioxide. In addition the 25 mg, 100 mg and 200 mg tablets also contain yellow iron oxide; the 25 mg and 100 mg tablets also contain red iron oxide.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
The precise mechanisms by which topiramate exerts its anticonvulsant and preventive migraine effects are unknown; however, preclinical studies have revealed four properties that may contribute to topiramate's efficacy for epilepsy and the preventive treatment of migraine. Electrophysiological and biochemical evidence suggests that topiramate, at pharmacologically relevant concentrations, blocks voltage-dependent sodium channels, augments the activity of the neurotransmitter gamma-aminobutyrate at some subtypes of the GABA-A receptor, antagonizes the AMPA/kainate subtype of the glutamate receptor, and inhibits the carbonic anhydrase enzyme, particularly isozymes II and IV.
12.2 Pharmacodynamics
Topiramate has anticonvulsant activity in rat and mouse maximal electroshock seizure (MES) tests. Topiramate is only weakly effective in blocking clonic seizures induced by the GABAA receptor antagonist, pentylenetetrazole. Topiramate is also effective in rodent models of epilepsy, which include tonic and absence-like seizures in the spontaneous epileptic rat (SER) and tonic and clonic seizures induced in rats by kindling of the amygdala or by global ischemia.
Changes (increases and decreases) from baseline in vital signs (systolic blood pressure-SBP, diastolic blood pressure-DBP, pulse) occurred more frequently in pediatric patients (6 to 17 years) treated with various daily doses of topiramate (50 mg, 100 mg, 200 mg, 2 to 3 mg/kg) than in patients treated with placebo in controlled trials for preventive treatment of migraine. The most notable changes were SBP <90 mm Hg, DBP <50 mm Hg, SBP or DBP increases or decreases ≥20 mm Hg, and pulse increases or decreases ≥30 beats per minute. These changes were often dose-related, and were most frequently associated with the greatest treatment difference at the 200 mg dose level. Systematic collection of orthostatic vital signs has not been conducted. The clinical significance of these various changes in vital signs has not been clearly established.
12.3 Pharmacokinetics
Absorption of topiramate is rapid, with peak plasma concentrations occurring at approximately 2 hours following a 400 mg oral dose. The relative bioavailability of topiramate from the tablet formulation is about 80% compared to a solution. The bioavailability of topiramate is not affected by food.
The pharmacokinetics of topiramate are linear with dose proportional increases in plasma concentration over the dose range studied (200 to 800 mg/day). The mean plasma elimination half-life is 21 hours after single or multiple doses. Steady-state is thus reached in about 4 days in patients with normal renal function. Topiramate is 15% to 41% bound to human plasma proteins over the blood concentration range of 0.5 to 250 μg/mL. The fraction bound decreased as blood concentration increased.
Carbamazepine and phenytoin do not alter the binding of topiramate. Sodium valproate, at 500 μg/mL (a concentration 5 to 10 times higher than considered therapeutic for valproate) decreased the protein binding of topiramate from 23% to 13%. Topiramate does not influence the binding of sodium valproate.
Metabolism and Excretion
Topiramate is not extensively metabolized and is primarily eliminated unchanged in the urine (approximately 70% of an administered dose). Six metabolites have been identified in humans, none of which constitutes more than 5% of an administered dose. The metabolites are formed via hydroxylation, hydrolysis, and glucuronidation. There is evidence of renal tubular reabsorption of topiramate. In rats, given probenecid to inhibit tubular reabsorption, along with topiramate, a significant increase in renal clearance of topiramate was observed. This interaction has not been evaluated in humans. Overall, oral plasma clearance (CL/F) is approximately 20 to 30 mL/min in adults following oral administration.
Specific Populations
Renal Impairment
The clearance of topiramate was reduced by 42% in subjects with moderate renal impairment (creatinine clearance 30 to 69 mL/min/1.73 m2) and by 54% in subjects with severe renal impairment (creatinine clearance <30 mL/min/1.73 m2) compared to subjects with normal renal function (creatinine clearance >70 mL/min/1.73 m2) [see Dosage and Administration (2.4) and (2.5)].
Hemodialysis
Topiramate is cleared by hemodialysis. Using a high-efficiency, counterflow, single pass-dialysate hemodialysis procedure, topiramate dialysis clearance was 120 mL/min with blood flow through the dialyzer at 400 mL/min. This high clearance (compared to 20 to 30 mL/min total oral clearance in healthy adults) will remove a clinically significant amount of topiramate from the patient over the hemodialysis treatment period [see Dosage and Administration (2.6), Use in Specific Populations (8.7)].
Hepatic Impairment
Plasma clearance of topiramate decreased a mean of 26% in patients with moderate to severe hepatic impairment.
Age, Gender, and Race
The pharmacokinetics of topiramate in elderly subjects (65 to 85 years of age, N=16) were evaluated in a controlled clinical study. The elderly subject population had reduced renal function (creatinine clearance [-20%]) compared to young adults. Following a single oral 100 mg dose, maximum plasma concentration for elderly and young adults was achieved at approximately 1 to 2 hours. Reflecting the primary renal elimination of topiramate, topiramate plasma and renal clearance were reduced 21% and 19%, respectively, in elderly subjects, compared to young adults. Similarly, topiramate half-life was longer (13%) in the elderly. Reduced topiramate clearance resulted in slightly higher maximum plasma concentration (23%) and AUC (25%) in elderly subjects than observed in young adults. Topiramate clearance is decreased in the elderly only to the extent that renal function is reduced [see Dosage and Administration (2.4) and Use in Specific Populations (8.5)].
Clearance of topiramate in adults was not affected by gender or race.
Pediatric Pharmacokinetics
Pharmacokinetics of topiramate were evaluated in patients age 2 to <16 years. Patients received either no or a combination of other antiepileptic drugs. A population pharmacokinetic model was developed on the basis of pharmacokinetic data from relevant topiramate clinical studies. This dataset contained data from 1217 subjects including 258 pediatric patients age 2 to <16 years (95 pediatric patients <10 years of age).
Pediatric patients on adjunctive treatment exhibited a higher oral clearance (L/h) of topiramate compared to patients on monotherapy, presumably because of increased clearance from concomitant enzyme-inducing antiepileptic drugs. In comparison, topiramate clearance per kg is greater in pediatric patients than in adults and in young pediatric patients (down to 2 years) than in older pediatric patients. Consequently, the plasma drug concentration for the same mg/kg/day dose would be lower in pediatric patients compared to adults and also in younger pediatric patients compared to older pediatric patients. Clearance was independent of dose.
As in adults, hepatic enzyme-inducing antiepileptic drugs decrease the steady state plasma concentrations of topiramate.
Drug Interactions
In vitro studies indicate that topiramate does not inhibit CYP1A2, CYP2A6, CYP2B6, CYP2C9, CYP2D6, CYP2E1, or CYP3A4/5 isozymes. In vitro studies indicate that topiramate is a mild inhibitor of CYP2C19 and a mild inducer of CYP3A4.
Antiepileptic Drugs
Potential interactions between topiramate and standard AEDs were assessed in controlled clinical pharmacokinetic studies in patients with epilepsy. The effects of these interactions on mean plasma AUCs are summarized in Table 10.
In Table 10, the second column (AED concentration) describes what happens to the concentration of the co-administered AED listed in the first column when topiramate is added. The third column (topiramate concentration) describes how the co-administration of a drug listed in the first column modifies the concentration of topiramate when compared to topiramate given alone.
Table 10 : Summary of AED Interactions with Topiramate AED
Co-administered
AED
Concentration
Topiramate
Concentration
Phenytoin
NC or 25% increasea
48% decrease
Carbamazepine (CBZ)
NC
40% decrease
CBZ epoxideb
NC
NE
Valproic acid
11% decrease
14% decrease
Phenobarbital
NC
NE
Primidone
NC
NE
Lamotrigine
NC at TPM doses up to 400 mg/day
13% decrease
a = Plasma concentration increased 25% in some patients, generally those on a twice a day dosing regimen of phenytoin.
b = Is not administered but is an active metabolite of carbamazepine.
NC = Less than 10% change in plasma concentration.
AED = Antiepileptic drug.
NE = Not Evaluated.
TPM = Topiramate
In a pharmacokinetic interaction study in healthy volunteers with a concomitantly administered combination oral contraceptive product containing 1 mg norethindrone (NET) plus 35 mcg ethinyl estradiol (EE), topiramate, given in the absence of other medications at doses of 50 to 200 mg/day, was not associated with statistically significant changes in mean exposure (AUC) to either component of the oral contraceptive. In another study, exposure to EE was statistically significantly decreased at doses of 200, 400, and 800 mg/day (18%, 21%, and 30%, respectively) when given as adjunctive therapy in patients taking valproic acid. In both studies, topiramate (50 mg/day to 800 mg/day) did not significantly affect exposure to NET and there was no significant dose-dependent change in EE exposure for doses of 50 to 200 mg/day. The clinical significance of the changes observed is not known [see Drug Interactions (7.4).
Digoxin
In a single-dose study, serum digoxin AUC was decreased by 12% with concomitant topiramate administration. The clinical relevance of this observation has not been established.
Hydrochlorothiazide
A drug interaction study conducted in healthy volunteers evaluated the steady-state pharmacokinetics of hydrochlorothiazide (HCTZ) (25 mg every 24 hours) and topiramate (96 mg every 12 hours) when administered alone and concomitantly. The results of this study indicate that topiramate Cmax increased by 27% and AUC increased by 29% when HCTZ was added to topiramate. The clinical significance of this change is unknown. The steady-state pharmacokinetics of HCTZ were not significantly influenced by the concomitant administration of topiramate. Clinical laboratory results indicated decreases in serum potassium after topiramate or HCTZ administration, which were greater when HCTZ and topiramate were administered in combination.
Metformin
A drug interaction study conducted in healthy volunteers evaluated the steady-state pharmacokinetics of metformin (500 mg every 12 hours) and topiramate in plasma when metformin was given alone and when metformin and topiramate (100 mg every 12 hours) were given simultaneously. The results of this study indicated that the mean metformin Cmax and AUC0-12h increased by 18% and 25%, respectively, when topiramate was added. Topiramate did not affect metformin tmax. The clinical significance of the effect of topiramate on metformin pharmacokinetics is not known. Oral plasma clearance of topiramate appears to be reduced when administered with metformin. The clinical significance of the effect of metformin on topiramate pharmacokinetics is unclear.
Pioglitazone
A drug interaction study conducted in healthy volunteers evaluated the steady-state pharmacokinetics of topiramate and pioglitazone when administered alone and concomitantly. A 15% decrease in the AUCt,ss of pioglitazone with no alteration in Cmax,ss was observed. This finding was not statistically significant. In addition, a 13% and 16% decrease in Cmax,ss and AUCt,ss respectively, of the active hydroxy-metabolite was noted as well as a 60% decrease in Cmax,ss and AUCt,ss of the active keto-metabolite. The clinical significance of these findings is not known.
Glyburide
A drug-drug interaction study conducted in patients with type 2 diabetes evaluated the steady-state pharmacokinetics of glyburide (5 mg/day) alone and concomitantly with topiramate (150 mg/day). There was a 22% decrease in Cmax and a 25% reduction in AUC24 for glyburide during topiramate administration. Systemic exposure (AUC) of the active metabolites, 4-trans-hydroxy-glyburide (M1) and 3-cis-hydroxyglyburide (M2), was also reduced by 13% and 15%, and Cmax was reduced by 18% and 25%, respectively. The steady-state pharmacokinetics of topiramate were unaffected by concomitant administration of glyburide.
Lithium
In patients, the pharmacokinetics of lithium were unaffected during treatment with topiramate at doses of 200 mg/day; however, there was an observed increase in systemic exposure of lithium (27% for Cmax and 26% for AUC) following topiramate doses up to 600 mg/day [see Drug Interactions (7.7).
Haloperidol
The pharmacokinetics of a single dose of haloperidol (5 mg) were not affected following multiple dosing of topiramate (100 mg every 12 hr) in 13 healthy adults (6 males, 7 females).
Amitriptyline
There was a 12% increase in AUC and Cmax for amitriptyline (25 mg per day) in 18 healthy subjects (9 males, 9 females) receiving 200 mg/day of topiramate.
Sumatriptan
Multiple dosing of topiramate (100 mg every 12 hours) in 24 healthy volunteers (14 males, 10 females) did not affect the pharmacokinetics of single-dose sumatriptan either orally (100 mg) or subcutaneously (6 mg).
Risperidone
When administered concomitantly with topiramate at escalating doses of 100, 250, and 400 mg/day, there was a reduction in risperidone systemic exposure (16% and 33% for steady-state AUC at the 250 and 400 mg/day doses of topiramate). No alterations of 9-hydroxyrisperidone levels were observed. Co-administration of topiramate 400 mg/day with risperidone resulted in a 14% increase in Cmax and a 12% increase in AUC12 of topiramate.There were no clinically significant changes in the systemic exposure of risperidone plus 9-hydroxyrisperidone or of topiramate; therefore, this interaction is not likely to be of clinical significance.
Propranolol
Multiple dosing of topiramate (200 mg/day) in 34 healthy volunteers (17 males, 17 females) did not affect the pharmacokinetics of propranolol following daily 160 mg doses. Propranolol doses of 160 mg/day in 39 volunteers (27 males, 12 females) had no effect on the exposure to topiramate, at a dose of 200 mg/day of topiramate.
Dihydroergotamine
Multiple dosing of topiramate (200 mg/day) in 24 healthy volunteers (12 males, 12 females) did not affect the pharmacokinetics of a 1 mg subcutaneous dose of dihydroergotamine. Similarly, a 1 mg subcutaneous dose of dihydroergotamine did not affect the pharmacokinetics of a 200 mg/day dose of topiramate in the same study.
Diltiazem
Co-administration of diltiazem (240 mg Cardizem CD®) with topiramate (150 mg/day) resulted in a 10% decrease in Cmax and a 25% decrease in diltiazem AUC, a 27% decrease in Cmax and an 18% decrease in des-acetyl diltiazem AUC, and no effect on N-desmethyl diltiazem. Co-administration of topiramate with diltiazem resulted in a 16% increase in Cmax and a 19% increase in AUC12 of topiramate.
Venlafaxine
Multiple dosing of topiramate (150 mg/day) in healthy volunteers did not affect the pharmacokinetics of venlafaxine or O-desmethyl venlafaxine. Multiple dosing of venlafaxine (150 mg) did not affect the pharmacokinetics of topiramate.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
An increase in urinary bladder tumors was observed in mice given topiramate (0, 20, 75, and 300 mg/kg/day) in the diet for 21 months. The increase in the incidence of bladder tumors in males and females receiving 300 mg/kg/day was primarily due to the increased occurrence of a smooth muscle tumor considered histomorphologically unique to mice. The higher of the doses not associated with an increase in tumors (75 mg/kg/day) is equivalent to the maximum recommended human dose (MRHD) for epilepsy (400 mg), and approximately 4 times the MRHD for migraine (100 mg) on a mg/m2 basis. The relevance of this finding to human carcinogenic risk is uncertain. No evidence of carcinogenicity was seen in rats following oral administration of topiramate for 2 years at doses up to 120 mg/kg/day (approximately 3 times the MRHD for epilepsy and 12 times the MRHD for migraine on a mg/m2 basis).
Mutagenesis
Topiramate did not demonstrate genotoxic potential when tested in a battery of in vitro and in vivo assays. Topiramate was not mutagenic in the Ames test or the in vitro mouse lymphoma assay; it did not increase unscheduled DNA synthesis in rat hepatocytes in vitro; and it did not increase chromosomal aberrations in human lymphocytes in vitro or in rat bone marrow in vivo.
Impairment of Fertility
No adverse effects on male or female fertility were observed in rats administered topiramate orally at doses up to 100 mg/kg/day (2.5 times the MRHD for epilepsy and 10 times the MRHD for migraine on a mg/m2 basis) prior to and during mating and early pregnancy.
-
14 CLINICAL STUDIES
The studies described in the following sections were conducted using topiramate tablets.
14.1 Monotherapy Epilepsy
Patients with Partial-Onset or Primary Generalized Tonic-Clonic Seizures
Adults and Pediatric Patients 10 Years of Age and Older
The effectiveness of topiramate as initial monotherapy in adults and pediatric patients 10 years of age and older with partial-onset or primary generalized tonic-clonic seizures was established in a multicenter, randomized, double-blind, parallel-group trial (Study 1).
Study 1 was conducted in 487 patients diagnosed with epilepsy (6 to 83 years of age) who had 1 or 2 well-documented seizures during the 3-month retrospective baseline phase who then entered the study and received topiramate 25 mg/day for 7 days in an open-label fashion. Forty-nine percent of patients had no prior AED treatment and 17% had a diagnosis of epilepsy for greater than 24 months. Any AED therapy used for temporary or emergency purposes was discontinued prior to randomization. In the double-blind phase, 470 patients were randomized to titrate up to 50 mg/day or 400 mg/day. If the target dose could not be achieved, patients were maintained on the maximum tolerated dose. Fifty-eight percent of patients achieved the maximal dose of 400 mg/day for >2 weeks, and patients who did not tolerate 150 mg/day were discontinued.
The primary efficacy assessment was a between-group comparison of time to first seizure during the double-blind phase. Comparison of the Kaplan-Meier survival curves of time to first seizure favored the topiramate 400 mg/day group over the topiramate 50 mg/day group (Figure 1). The treatment effects with respect to time to first seizure were consistent across various patient subgroups defined by age, sex, geographic region, baseline body weight, baseline seizure type, time since diagnosis, and baseline AED use.
Figure 1: Kaplan-Meier Estimates of Cumulative Rates for Time to First Seizure in Study 1
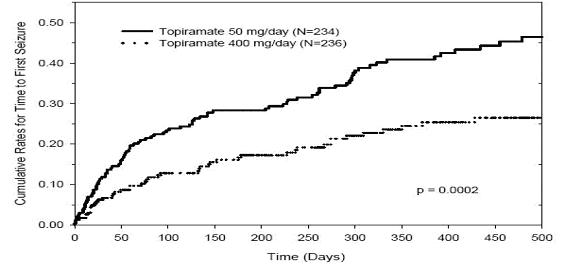
Pediatric Patients 2 to 9 Years of Age
The conclusion that topiramate is effective as initial monotherapy in pediatric patients 2 to 9 years of age with partial-onset or primary generalized tonic-clonic seizures was based on a pharmacometric bridging approach using data from the controlled epilepsy trials described in labeling. This approach consisted of first showing a similar exposure response relationship between pediatric patients down to 2 years of age and adults when topiramate was given as adjunctive therapy. Similarity of exposure-response was also demonstrated in pediatric patients 6 to less than 16 years of age and adults when topiramate was given as initial monotherapy. Specific dosing in pediatric patients 2 to 9 years of age was derived from simulations utilizing plasma exposure ranges observed in pediatric and adult patients treated with topiramate initial monotherapy [see Dosage and Administration (2.1)].
14.2 Adjunctive Therapy Epilepsy
Adult Patients With Partial Onset Seizures
The effectiveness of topiramate as an adjunctive treatment for adults with partial-onset seizures was established in six multicenter, randomized, double-blind, placebo-controlled trials (Studies 2, 3, 4, 5, 6 and 7), two comparing several dosages of topiramate and placebo and four comparing a single dosage with placebo, in patients with a history of partial-onset seizures, with or without secondarily generalized seizures.
Patients in these studies were permitted a maximum of two antiepileptic drugs (AEDs) in addition to topiramate tablets or placebo. In each study, patients were stabilized on optimum dosages of their concomitant AEDs during baseline phase lasting between 4 and 12 weeks. Patients who experienced a pre-specified minimum number of partial onset seizures, with or without secondary generalization, during the baseline phase (12 seizures for 12-week baseline, 8 for 8-week baseline or 3 for 4-week baseline) were randomly assigned to placebo or a specified dose of topiramate tablets in addition to their other AEDs.
Following randomization, patients began the double-blind phase of treatment. In five of the six studies, patients received active drug beginning at 100 mg per day; the dose was then increased by 100 mg or 200 mg/day increments weekly or every other week until the assigned dose was reached, unless intolerance prevented increases. In the sixth study (Study 7), the 25 or 50 mg/day initial doses of topiramate were followed by respective weekly increments of 25 or 50 mg/day until the target dose of 200 mg/day was reached. After titration, patients entered a 4, 8 or 12-week stabilization period. The numbers of patients randomized to each dose and the actual mean and median doses in the stabilization period are shown in Table 11.
Pediatric Patients 2 to 16 Years of Age with Partial-Onset Seizures
The effectiveness of topiramate as an adjunctive treatment for pediatric patients 2 to 16 years of age with partial-onset seizures was established in a multicenter, randomized, double-blind, placebo-controlled trial (Study 8), comparing topiramate and placebo in patients with a history of partial-onset seizures, with or without secondarily generalized seizures (see Table 12).
Patients in this study were permitted a maximum of two antiepileptic drugs (AEDs) in addition to topiramate tablets or placebo. In this study, patients were stabilized on optimum dosages of their concomitant AEDs during an 8-week baseline phase. Patients who experienced at least six partial-onset seizures, with or without secondarily generalized seizures, during the baseline phase were randomly assigned to placebo or topiramate tablets in addition to their other AEDs.
Following randomization, patients began the double-blind phase of treatment. Patients received active drug beginning at 25 or 50 mg/day; the dose was then increased by 25 mg to 150 mg/day increments every other week until the assigned dosage of 125, 175, 225, or 400 mg/day based on patients' weight to approximate a dosage of 6 mg/kg/day was reached, unless intolerance prevented increases. After titration, patients entered an 8-week stabilization period.
Patients With Primary Generalized Tonic-Clonic Seizures
The effectiveness of topiramate as an adjunctive treatment for primary generalized tonic- clonic seizures in patients 2 years of age and older was established in a multicenter, randomized, double-blind, placebo-controlled trial (Study 9), comparing a single dosage of topiramate and placebo (see Table 12).
Patients in study 9 were permitted a maximum of two antiepileptic drugs (AEDs) in addition to topiramate or placebo. Patients were stabilized on optimum dosages of their concomitant AEDs during an 8-week baseline phase. Patients who experienced at least three primary generalized tonic-clonic seizures during the baseline phase were randomly assigned to placebo or topiramate in addition to their other AEDs.
Following randomization, patients began the double-blind phase of treatment. Patients received active drug beginning at 50 mg/day for four weeks; the dose was then increased by 50 mg to 150 mg/day increments every other week until the assigned dose of 175, 225, or 400 mg/day based on patients' body weight to approximate a dosage of 6 mg/kg/day was reached, unless intolerance prevented increases. After titration, patients entered a 12-week stabilization period.
Patients With Lennox-Gastaut Syndrome
The effectiveness of topiramate as an adjunctive treatment for seizures associated with Lennox-Gastaut syndrome was established in a multicenter, randomized, double-blind, placebo-controlled trial (Study 10) comparing a single dosage of topiramate with placebo in patients 2 years of age and older (see Table 12).
Patients in Study 10 were permitted a maximum of two antiepileptic drugs (AEDs) in addition to topiramate or placebo. Patients who were experiencing at least 60 seizures per month before study entry were stabilized on optimum dosages of their concomitant AEDs during a 4-week baseline phase. Following baseline, patients were randomly assigned to placebo or topiramate in addition to their other AEDs. Active drug was titrated beginning at 1 mg/kg/day for a week; the dose was then increased to 3 mg/kg/day for one week, then to 6 mg/kg/day. After titration, patients entered an 8-week stabilization period.
The primary measures of effectiveness were the percent reduction in drop attacks and a parental global rating of seizure severity.
Table 11: Topiramate Dose Summary During the Stabilization Periods of Each of Six Double-Blind, Placebo-Controlled, Adjunctive Trials in Adults with Partial-Onset Seizuresa Study
S tabilization Dose
Placebo b
Target topiramate Dosage (mg/day)
200
400
600
800
1,000
2
N
42
42
40
41
--
--
Mean Dose
5.9
200
390
556
--
--
Median Dose
6.0
200
400
600
--
--
3
N
44
--
--
40
45
40
Mean Dose
9.7
--
--
544
739
796
Median Dose
10.0
--
--
600
800
1,000
4
N
23
--
19
--
--
--
Mean Dose
3.8
--
395
--
--
--
Median Dose
4.0
--
400
--
--
--
5
N
30
--
--
28
--
--
Mean Dose
5.7
--
--
522
--
--
Median Dose
6.0
--
--
600
--
--
6
N
28
--
--
--
25
--
Mean Dose
7.9
--
--
--
568
--
Median Dose
8.0
--
--
--
600
--
7
N
90
157
--
--
--
--
Mean Dose
8
200
--
--
--
--
Median Dose
8
200
--
--
--
--
a Dose-response studies were not conducted for other indications or pediatric partial-onset
seizures.
b Placebo dosages are given as the number of tablets. Placebo target dosages were as follows: Protocol 3 4 tablets/day; Protocols 1 and 4, 6 tablets/day; Protocols 5 and 6, 8 tablets/day; Protocol 2, 10 tablets/day.
In all adjunctive trials, the reduction in seizure rate from baseline during the entire double-blind phase was measured. The median percent reductions in seizure rates and the responder rates (fraction of patients with at least a 50% reduction) by treatment group for each study are shown below in Table 12. As described above, a global improvement in seizure severity was also assessed in the Lennox-Gastaut trial.
Table 12: Efficacy Results in Double-Blind, Placebo-Controlled, Adjunctive Epilepsy Trials Target topiramate Dosage (mg/day)
Study
#
#
Placebo
200
400
600
800
1,000
6 mg/
k g /day*
Partial-Onset Seizures Studies in Adults
2
N
45
45
45
46
--
--
--
Median % Reduction
12
27a
48b
45c
--
--
--
% Responders
18
24
44d
46d
--
--
--
3
N
47
--
--
48
48
47
--
Median % Reduction
2
--
--
41c
41c
36c
--
% Responders
9
--
--
40c
41c
36d
--
4
N
24
--
23
--
--
--
--
Median % Reduction
1
--
41e
--
--
--
--
% Responders
8
--
35d
--
--
--
--
5
N
30
--
--
30
--
--
--
Median % Reduction
-12
--
--
46f
--
--
--
% Responders
10
--
--
47c
--
--
--
6
N
28
--
--
--
28
--
--
Median % Reduction
-21
--
--
--
24c
--
--
% Responders
0
--
--
--
43c
--
--
7
N
91
168
--
--
--
--
--
Median % Reduction
20
44c
--
--
--
--
--
% Responders
24
45c
--
--
--
--
--
Partial-Onset Seizures Studies in Pediatric Patients
8
N
45
--
--
--
--
--
41
Median % Reduction
11
--
--
--
--
--
33d
% Responders
20
--
--
--
--
--
39
Primary Generalized Tonic-Clonich
9
N
40
--
--
--
--
--
39
Median % Reduction
9
--
--
--
--
--
57d
% Responders
20
--
--
--
--
--
56c
Lennox-Gastaut Syndromei
10
N
49
--
--
--
--
--
46
Median % Reduction
-5
--
--
--
--
--
15d
% Responders
14
--
--
--
--
--
28g
Improvement in Seizure Severityj
28
--
--
--
--
--
52d
Comparisons with placebo: a p=0.080; b p≤0.010; c p≤0.001; d p≤0.050; e p=0.065; f p≤0.005; g p=0.071;
h Median % reduction and % responders are reported for PGTC Seizures;
i Median % reduction and % responders for drop attacks, i.e., tonic or atonic seizures;
j Percentage of subjects who were minimally, much, or very much improved from baseline
* For Studies 8 and 9, specified target dosages (<9.3 mg/kg/day) were assigned based on subject's weight to approximate a dosage of 6 mg/kg per day; these dosages corresponded to mg/day dosages of 125, 175, 225, and 400 mg/day.
Subset analyses of the antiepileptic efficacy of topiramate tablets in these studies showed no differences as a function of gender, race, age, baseline seizure rate, or concomitant AED.
In clinical trials for epilepsy, daily dosages were decreased in weekly intervals by 50 to 100 mg/day in adults and over a 2- to 8- week period in pediatric patients; transition was permitted to a new antiepileptic regimen when clinically indicated.
14.3 Preventive Treatment of Migraine
The results of 2 multicenter, randomized, double-blind, placebo-controlled, parallel-group clinical trials established the effectiveness of topiramate in the preventive treatment of migraine. The design of both trials (Study 11 was conducted in the U.S. and Study 12 was conducted in the U.S. and Canada) was identical, enrolling patients with a history of migraine, with or without aura, for at least 6 months, according to the International Headache Society (IHS) diagnostic criteria. Patients with a history of cluster headaches or basilar, ophthalmoplegic, hemiplegic, or transformed migraine headaches were excluded from the trials. Patients were required to have completed up to a 2-week washout of any prior migraine preventive medications before starting the baseline phase.
Patients who experienced 3 to 12 migraine headaches over the 4 weeks in the baseline phase were randomized to either topiramate 50 mg/day, 100 mg/day, 200 mg/day, or placebo and treated for a total of 26 weeks (8-week titration period and 18-week maintenance period). Treatment was initiated at 25 mg/day for one week, and then the daily dosage was increased by 25 mg increments each week until reaching the assigned target dose or maximum tolerated dose (administered twice daily).
Effectiveness of treatment was assessed by the reduction in migraine headache frequency, as measured by the change in 4-week migraine rate (according to migraines classified by IHS criteria) from the baseline phase to double-blind treatment period in each topiramate treatment group compared to placebo in the Intent-To-Treat (ITT) population.
In Study 11, a total of 469 patients (416 females, 53 males), ranging in age from 13 to 70 years, were randomized and provided efficacy data. Two hundred sixty-five patients completed the entire 26-week double-blind phase. The median average daily dosages were 48 mg/day,
88 mg/day and 132 mg/day in the target dose groups of topiramate 50, 100, and 200 mg/day, respectively.
The mean migraine headache frequency rate at baseline was approximately 5.5 migraine headaches/28 days and was similar across treatment groups. The change in the mean 4-week migraine headache frequency from baseline to the double-blind phase was -1.3, -2.1, and -2.2 in the topiramate 50, 100, and 200 mg/day groups, respectively, versus -0.8 in the placebo group (see Figure 2). The treatment differences between the topiramate 100 and 200 mg/day groups versus placebo were similar and statistically significant (p<0.001 for both comparisons).
In Study 12, a total of 468 patients (406 females, 62 males), ranging in age from 12 to 65 years, were randomized and provided efficacy data. Two hundred fifty-five patients completed the entire 26-week double-blind phase. The median average daily dosages were 47 mg/day, 86 mg/day, and 150 mg/day in the target dose groups of topiramate 50, 100, and 200 mg/day, respectively.
The mean migraine headache frequency rate at baseline was approximately 5.5 migraine headaches/28 days and was similar across treatment groups. The change in the mean 4-week migraine headache period frequency from baseline to the double-blind phase was -1.4, -2.1, and -2.4 in the topiramate 50, 100, and 200 mg/day groups, respectively, versus -1.1 in the placebo group (see Figure 2). The differences between the topiramate 100 and 200 mg/day groups versus placebo were similar and statistically significant (p=0.008 and p <0.001, respectively).
In both studies, there were no apparent differences in treatment effect within age or gender subgroups. Because most patients were Caucasian, there were insufficient numbers of patients from different races to make a meaningful comparison of race.
For patients withdrawing from topiramate, daily dosages were decreased in weekly intervals by 25 to 50 mg/day.
Figure 2: Reduction in 4-Week Migraine Headache Frequency
(Studies 11 and 12 for Adults and Adolescents)
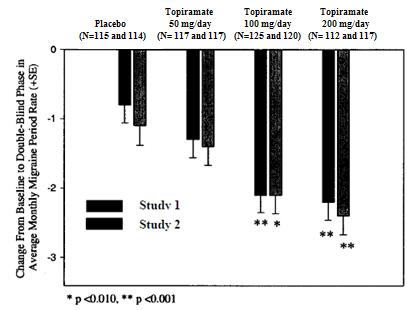
Pediatric Patients 12 to 17 Years of Age
The effectiveness of topiramate for the preventive treatment of migraine in pediatric patients 12 to 17 years of age was established in a multicenter, randomized, double-blind, parallel-group trial (Study 13). The study enrolled 103 patients (40 male, 63 female) 12 to 17 years of age with episodic migraine headaches with or without aura. Patient selection was based on IHS criteria for migraines (using proposed revisions to the 1988 IHS pediatric migraine criteria [IHS-R criteria]).
Patients who experienced 3 to 12 migraine attacks (according to migraines classified by patient reported diaries) and ≤14 headache days (migraine and non-migraine) during the 4-week prospective baseline period were randomized to either topiramate 50 mg/day, 100 mg/day, or placebo and treated for a total of 16 weeks (4-week titration period followed by a 12-week maintenance period). Treatment was initiated at 25 mg/day for one week, and then the daily dosage was increased by 25 mg increments each week until reaching the assigned target dose or maximum tolerated dose (administered twice daily). Approximately 80% or more patients in each treatment group completed the study. The median average daily dosages were 45 and 79 mg/day in the target dose groups of topiramate 50 and 100 mg/day, respectively.
Effectiveness of treatment was assessed by comparing each topiramate treatment group to placebo (ITT population) for the percent reduction from baseline to the last 12 weeks of the double-blind phase in the monthly migraine attack rate (primary endpoint). The percent reduction from baseline to the last 12 weeks of the double-blind phase in average monthly migraine attack rate is shown in Table 13. The 100 mg topiramate dose produced a statistically significant treatment difference relative to placebo of 28% reduction from baseline in the monthly migraine attack rate.
The mean reduction from baseline to the last 12 weeks of the double-blind phase in average monthly attack rate, a key secondary efficacy endpoint in Study 13 (and the primary efficacy endpoint in Studies 11 and 12, of adults) was 3.0 for 100 mg topiramate dose and 1.7 for placebo. This 1.3 treatment difference in mean reduction from baseline of monthly migraine rate was statistically significant (p = 0.0087).
Table 13: Percent Reduction from Baseline to the Last 12 Weeks of Double-Blind Phase in Average Monthly Attack Rate: Study 13 (Intent-to-Treat Analysis Set)
Category
Placebo
(N=33)
Topiramate
50 mg/day
(N=35)
Topiramate
100 mg/day
(N=35)
Baseline
Median
3.6
4.0
4.0
Last 12 Weeks of Double-Blind Phase
Median
2.3
2.3
1.0
Percent Reduction (%)
Median
44.4
44.6
72.2
P-value versus Placeboa,b
0.7975
0.0164 c
a = P-values (two-sided) for comparisons relative to placebo are generated by applying an ANCOVA model on ranks that includes subject's stratified age at baseline, treatment group, and analysis center as factors and monthly migraine attack rate during baseline period as a covariate.
b = P-values for the dose groups are the adjusted p-value according to the Hochberg multiple comparison procedure.
c = Indicates p-value is <0.05 (two-sided).
-
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 How Supplied.
Topiramate Tablets, USP are available as:
25 mg Tablet:
Light yellow, round, biconvex, film-coated tablets with 'U' debossed on one side and '115' debossed on other side.
Bottles of 60: NDC: 29300-115-16
Bottles of 100: NDC: 29300-115-01
Bottles of 500: NDC: 29300-115-05
Bottles of 1000: NDC: 29300-115-10
50 mg Tablet:
White to off-white, round, bevel edged, biconvex, film-coated tablets with 'U' debossed on one side and '116' debossed on other side.
Bottles of 60: NDC: 29300-116-16
Bottles of 100: NDC: 29300-116-01
Bottles of 500: NDC: 29300-116-05
Bottles of 1000: NDC: 29300-116-10
100 mg Tablet:
Salmon, round, bevel edged, biconvex, film-coated tablets with 'U' debossed on one side and '117' debossed on other side.
Bottles of 60: NDC: 29300-117-16
Bottles of 100: NDC: 29300-117-01
Bottles of 500: NDC: 29300-117-05
Bottles of 1000: NDC: 29300-117-10
200 mg Tablet:
Yellow, round, bevel edged, biconvex, film-coated tablets with 'U' debossed on one side and '118' debossed on other side.
Bottles of 60: NDC: 29300-118-16
Bottles of 100: NDC: 29300-118-01
Bottles of 500: NDC: 29300-118-05
Bottles of 1000: NDC: 29300-118-10
-
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Medication Guide).
Additional Medication Guides can be obtained by calling Unichem at 1-866-562-4616
Eye Disorders
Instruct patients taking topiramate to seek immediate medical attention if they experience blurred vision, visual disturbances, or periorbital pain [see Warnings and Precautions (5.1, 5.2)].
Oligohidrosis and Hyperthermia
Closely monitor topiramate-treated patients, especially pediatric patients, for evidence of decreased sweating and increased body temperature, especially in hot weather. Counsel patients to contact their healthcare professionals immediately if they develop a high or persistent fever, or decreased sweating [see Warnings and Precautions (5.3)].
Metabolic Acidosis
Warn patients about the potential significant risk for metabolic acidosis that may be asymptomatic and may be associated with adverse effects on kidneys (e.g., kidney stones, nephrocalcinosis), bones (e.g., osteoporosis, osteomalacia, and/or rickets in children), and growth (e.g., growth delay/retardation) in pediatric patients, and on the fetus [see Warnings and Precautions (5.4), Use in Specific Populations (8.1)].
Suicidal Behavior and Ideation
Counsel patients, their caregivers, and families that AEDs, including topiramate, may increase the risk of suicidal thoughts and behavior, and advise of the need to be alert for the emergence or worsening of the signs and symptoms of depression, any unusual changes in mood or behavior or the emergence of suicidal thoughts, or behavior or thoughts about self-harm. Instruct patients to immediately report behaviors of concern to their healthcare providers [see Warnings and Precautions (5.5)].
Interference with Cognitive and Motor Performance
Warn patients about the potential for somnolence, dizziness, confusion, difficulty concentrating, or visual effects, and advise patients not to drive or operate machinery until they have gained sufficient experience on topiramate to gauge whether it adversely affects their mental performance, motor performance, and/or vision [see Warnings and Precautions (5.6)].
Even when taking topiramate or other anticonvulsants, some patients with epilepsy will continue to have unpredictable seizures. Therefore, advise all patients taking topiramate for epilepsy to exercise appropriate caution when engaging in any activities where loss of consciousness could result in serious danger to themselves or those around them (including swimming, driving a car, climbing in high places, etc.). Some patients with refractory epilepsy will need to avoid such activities altogether. Discuss the appropriate level of caution with patients, before patients with epilepsy engage in such activities.
Fetal Toxicity
Inform pregnant women and women of childbearing potential that use of topiramate during pregnancy can cause fetal harm, including an increased risk for cleft lip and/or cleft palate (oral clefts), which occur early in pregnancy before many women know they are pregnant. Also inform patients that infants exposed to topiramate monotherapy in utero may be SGA [see Use in Specific Populations (8.1)]. There may also be risks to the fetus from chronic metabolic acidosis with use of topiramate during pregnancy [see Warnings and Precautions (5.7), Use in Specific Populations (8.1]. When appropriate, counsel pregnant women and women of childbearing potential about alternative therapeutic options.
Advise women of childbearing potential who are not planning a pregnancy to use effective contraception while using topiramate, keeping in mind that there is a potential for decreased contraceptive efficacy when using estrogen-containing birth control with topiramate [see Drug Interactions (7.4)].
Encourage pregnant women using topiramate, to enroll in the North American Antiepileptic Drug (NAAED) Pregnancy Registry. The registry is collecting information about the safety of antiepileptic drugs during pregnancy [see Use in Specific Populations (8.1)].
Hyperammonemia and Encephalopathy
Warn patients about the possible development of hyperammonemia with or without encephalopathy. Although hyperammonemia may be asymptomatic, clinical symptoms of hyperammonemic encephalopathy often include acute alterations in level of consciousness and/or cognitive function with lethargy and/or vomiting. This hyperammonemia and encephalopathy can develop with topiramate treatment alone or with topiramate treatment with concomitant valproic acid (VPA).
Instruct patients to contact their physician if they develop unexplained lethargy, vomiting, or changes in mental status [see Warnings and Precautions (5.9)].
Kidney Stones
Instruct patients, particularly those with predisposing factors, to maintain an adequate fluid intake in order to minimize the risk of kidney stone formation [see Warnings and Precautions (5.10)].
Instructions for a Missing Dose
Instruct patients that if they miss a single dose of topiramate, it should be taken as soon as possible. However, if a patient is within 6 hours of taking the next scheduled dose, tell the patient to wait until then to take the usual dose of topiramate, and to skip the missed dose. Tell patients that they should not take a double dose in the event of a missed dose. Advise patients to contact their healthcare provider if they have missed more than one dose.
11-R-05/2019
-
MEDICATION GUIDE
MEDICATION GUIDE
Topiramate Tablets, USP
(toe pir' a mate), for oral use
What is the most important information I should know about topiramate tablets?
Topiramate tablets may cause eye problems. Serious eye problems include:
any sudden decrease in vision with or without eye pain and redness,
a blockage of fluid in the eye causing increased pressure in the eye (secondary angle closure glaucoma).
These eye problems can lead to permanent loss of vision if not treated.
You should call your healthcare provider right away if you have any new eye symptoms, including any new problems with your vision.
Topiramate tablets may cause decreased sweating and increased body temperature (fever). People, especially children, should be watched for signs of decreased sweating and fever, especially in hot temperatures. Some people may need to be hospitalized for this condition. If a high fever, a fever that does not go away, or decreased sweating develops, call your healthcare provider right away.
Topiramate tablets can increase the level of acid in your blood (metabolic acidosis). If left untreated, metabolic acidosis can cause brittle or soft bones (osteoporosis, osteomalacia, osteopenia), kidney stones, can slow the rate of growth in children, and may possibly harm your baby if you are pregnant. Metabolic acidosis can happen with or without symptoms.
Sometimes people with metabolic acidosis will:
feel tired
not feel hungry (loss of appetite)
feel changes in heartbeat
have trouble thinking clearly
Your healthcare provider should do a blood test to measure the level of acid in your blood before and during your treatment with topiramate tablets. If you are pregnant, you should talk to your healthcare provider about whether you have metabolic acidosis.
Like other antiepileptic drugs, topiramate tablets may cause suicidal thoughts or actions in a very small number of people, about 1 in 500.
Call a healthcare provider right away if you have any of these symptoms, especially if they are new, worse, or worry you:
thoughts about suicide or dying
attempts to commit suicide
new or worse depression
new or worse anxiety
feeling agitated or restless
panic attacks
trouble sleeping (insomnia)
new or worse irritability
acting aggressive, being angry, or violent
acting on dangerous impulses
an extreme increase in activity and talking (mania)
other unusual changes in behavior or mood
Do not stop topiramate tablets without first talking to a healthcare provider.
Stopping topiramate tablets suddenly can cause serious problems.
Suicidal thoughts or actions can be caused by things other than medicines. If you have suicidal thoughts or actions, your healthcare provider may check for other causes.
How can I watch for early symptoms of suicidal thoughts and actions?
Pay attention to any changes, especially sudden changes, in mood, behaviors, thoughts, or feelings.
Keep all follow-up visits with your healthcare provider as scheduled.
Call your healthcare provider between visits as needed, especially if you are worried about symptoms.
Topiramate tablets can harm your unborn baby.
If you take topiramate tablets during pregnancy, your baby has a higher risk for birth defects called cleft lip and cleft palate. These defects can begin early in pregnancy, even before you know you are pregnant.
Cleft lip and cleft palate may happen even in children born to women who are not taking any medicines and do not have other risk factors.
There may be other medicines to treat your condition that have a lower chance of birth defects.
All women of childbearing age should talk to their healthcare providers about using other possible treatments instead of topiramate tablets. If the decision is made to use topiramate tablets, you should use effective birth control (contraception) unless you are planning to become pregnant. You should talk to your doctor about the best kind of birth control to use while you are taking topiramate tablets.
Tell your healthcare provider right away if you become pregnant while taking topiramate tablets. You and your healthcare provider should decide if you will continue to take topiramate tablets while you are pregnant.
If you take topiramate tablets during pregnancy, your baby may be smaller than expected at birth. The long-term effects of this are not known. Talk to your healthcare provider if you have questions about this risk during pregnancy.
Metabolic acidosis may have harmful effects on your baby. Talk to your healthcare provider if topiramate tablets have caused metabolic acidosis during your pregnancy.
Pregnancy Registry: If you become pregnant while taking topiramate tablets, talk to your healthcare provider about registering with the North American Antiepileptic Drug Pregnancy Registry. You can enroll in this registry by calling 1-888-233-2334. The purpose of this registry is to collect information about the safety of topiramate and other antiepileptic drugs during pregnancy.
What are topiramate tablets?
Topiramate tablets are a prescription medicine used:
to treat certain types of seizures (partial-onset seizures and primary generalized tonic-clonic seizures) in adults and children 2 years and older,
with other medicines to treat certain types of seizures (partial-onset seizures, primary generalized tonic-clonic seizures, and seizures associated with Lennox-Gastaut syndrome) in adults and children 2 years and older,
to prevent migraine headaches in adults and adolescents 12 years and older.
Before taking topiramate tablets, tell your healthcare provider about all of your medical conditions, including if you:
have or have had depression, mood problems, or suicidal thoughts or behavior.
have kidney problems, have kidney stones, or are getting kidney dialysis.
have a history of metabolic acidosis (too much acid in the blood).
have liver problems.
have weak, brittle, or soft bones (osteomalacia, osteoporosis, osteopenia, or decreased bone density).
have lung or breathing problems.
have eye problems, especially glaucoma.
have diarrhea.
have a growth problem.
are on a diet high in fat and low in carbohydrates, which is called a ketogenic diet.
are having surgery.
are pregnant or plan to become pregnant.
are breastfeeding or plan to breastfeed. Topiramate passes into breast milk. Breastfed babies may be sleepy or have diarrhea. It is not known if the topiramate that passes into breast milk can cause other serious harm to your baby. Talk to your healthcare provider about the best way to feed your baby if you take topiramate tablets.
Tell your healthcare provider about all the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. Topiramate tablets and other medicines may affect each other causing side effects.
Especially tell your healthcare provider if you take:
Valproic acid (such as DEPAKENE or DEPAKOTE).
any medicines that impair or decrease your thinking, concentration, or muscle coordination
birth control pills. Topiramate tablets may make your birth control pills less effective. Tell your healthcare provider if your menstrual bleeding changes while you are taking birth control pills and topiramate tablets.
Ask your healthcare provider if you are not sure if your medicine is listed above.
Know the medicines you take. Keep a list of them to show your healthcare provider and pharmacist each time you get a new medicine. Do not start a new medicine without talking with your healthcare provider.
How should I take topiramate tablets?
Take topiramate tablets exactly as prescribed.
Your healthcare provider may change your dose. Do not change your dose without talking to your healthcare provider.
Take Topiramate tablets whole. Do not chew the tablets. They may leave a bitter taste.
Topiramate tablets can be taken before, during, or after a meal. Drink plenty of fluids during the day. This may help prevent kidney stones while taking topiramate tablets.
If you take too much topiramate tablets, call your healthcare provider right away or go to the nearest emergency room.
If you miss a single dose of topiramate tablets, take it as soon as you can. However, if you are within 6 hours of taking your next scheduled dose, wait until then to take your usual dose of topiramate tablets, and skip the missed dose. Do not double your dose. If you have missed more than one dose, you should call your healthcare provider for advice.
Do not stop taking topiramate tablets without talking to your healthcare provider. Stopping topiramate tablets suddenly may cause serious problems. If you have epilepsy and you stop taking topiramate tablets suddenly, you may have seizures that do not stop. Your healthcare provider will tell you how to stop taking topiramate tablets slowly.
Your healthcare provider may do blood tests while you take topiramate tablets.
What should I avoid while taking topiramate tablets?
You should not drink alcohol while taking topiramate tablets. Topiramate tablets and alcohol can affect each other causing side effects such as sleepiness and dizziness.
Do not drive a car or operate machinery until you know how topiramate tablets affect you. Topiramate tablets can slow your thinking and motor skills, and may affect vision.
What are the possible side effects of topiramate tablets?
Topiramate tablets may cause serious side effects including :
See "What is the most important information I should know about topiramate tablets?"
High blood ammonia levels. High ammonia in the blood can affect your mental activities, slow your alertness, make you feel tired, or cause vomiting. This has happened when topiramate tablets is taken with a medicine called valproic acid (DEPAKENE and DEPAKOTE).
Effects on thinking and alertness. Topiramate tablets may affect how you think and cause confusion, problems with concentration, attention, memory, or speech. topiramate tablets may cause depression or mood problems, tiredness, and sleepiness.
Dizziness or loss of muscle coordination.
Kidney stones. Drink plenty of fluids when taking topiramate tablets to decrease your chances of getting kidney stones.
Low body temperature. Taking topiramate tablets when you are also taking valproic acid can cause a drop in body temperature to less than 95°F, or can cause tirednessfeeling tired, confusion, or coma.
Call your healthcare provider right away if you have any of the symptoms above.
The most common side effects of topiramate tablets include:
tingling of the arms and legs (paresthesia)
not feeling hungry
nausea
a change in the way foods taste
diarrhea
weight loss
nervousness
upper respiratory tract infection
speech problems
tiredness
dizziness
sleepiness/drowsiness
slow reactions
difficulty with memory
pain in the abdomen
fever
abnormal vision
decreased feeling or sensitivity, especially in the skin
Tell your healthcare provider about any side effect that bothers you or that does not go away. These are not all the possible side effects of topiramate tablets. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
You may also report side effects to Unichem Pharmaceuticals (USA), Inc., at 1-866-562-4616
How should I store topiramate tablets?
Store topiramate tablets at 20° to 25°C (68° to 77°F).
Keep topiramate tablets in a tightly closed container.
Keep topiramate tablets dry and away from moisture.
Keep topiramate tablets and all medicines out of the reach of children.
General information about the safe and effective use of topiramate tablets.
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use topiramate tablets for a condition for which it was not prescribed. Do not give topiramate tablets to other people, even if they have the same symptoms that you have. It may harm them.
You can ask your pharmacist or healthcare provider for information about topiramate tablets that is written for health professionals.
What are the ingredients in topiramate tablets?
Active ingredient: Topiramate USP
Inactive ingredients: lactose monohydrate, pregelatinized corn starch, microcrystalline cellulose, sodium starch glycolate Type A (Potato), magnesium stearate, hypromellose, polysorbate 80, polyethylene glycol, and titanium dioxide. In addition the 25 mg, 100 mg, and 200 mg tablets also contain yellow iron oxide; the 25 mg and 100 mg tablets also contain red iron oxide
Trademarks are the property of their respective owners.
Additional Medication Guides can be obtained by calling Unichem at 1-866-562-4616
Manufactured by:
UNICHEM LABORATORIES LTD.
Ind Area, Meerut Road, Ghaziabad – 201 003, India
Manufactured for:

East Brunswick, NJ 08816
11-R-05/2019
13011565
This Medication Guide has been approved by the U.S. Food and Drug Administration Revised: 05/2019
- PACKAGE LABEL.PRINCIPAL DISPLAY PANEL
-
INGREDIENTS AND APPEARANCE
TOPIRAMATE
topiramate tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 29300-115 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength TOPIRAMATE (UNII: 0H73WJJ391) (TOPIRAMATE - UNII:0H73WJJ391) TOPIRAMATE 25 mg Inactive Ingredients Ingredient Name Strength CELLULOSE, MICROCRYSTALLINE (UNII: OP1R32D61U) FERRIC OXIDE RED (UNII: 1K09F3G675) FERRIC OXIDE YELLOW (UNII: EX438O2MRT) HYPROMELLOSE 2910 (6 MPA.S) (UNII: 0WZ8WG20P6) LACTOSE MONOHYDRATE (UNII: EWQ57Q8I5X) MAGNESIUM STEARATE (UNII: 70097M6I30) POLYETHYLENE GLYCOL 6000 (UNII: 30IQX730WE) POLYSORBATE 80 (UNII: 6OZP39ZG8H) SODIUM STARCH GLYCOLATE TYPE A POTATO (UNII: 5856J3G2A2) STARCH, PREGELATINIZED CORN (UNII: O8232NY3SJ) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) Product Characteristics Color YELLOW (Light Yellow) Score no score Shape ROUND Size 6mm Flavor Imprint Code U;115 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 29300-115-16 60 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 07/01/2013 2 NDC: 29300-115-01 100 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 07/01/2013 3 NDC: 29300-115-05 500 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 07/01/2013 4 NDC: 29300-115-10 1000 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 07/01/2013 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA090162 07/01/2013 TOPIRAMATE
topiramate tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 29300-116 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength TOPIRAMATE (UNII: 0H73WJJ391) (TOPIRAMATE - UNII:0H73WJJ391) TOPIRAMATE 50 mg Inactive Ingredients Ingredient Name Strength CELLULOSE, MICROCRYSTALLINE (UNII: OP1R32D61U) HYPROMELLOSE 2910 (6 MPA.S) (UNII: 0WZ8WG20P6) LACTOSE MONOHYDRATE (UNII: EWQ57Q8I5X) MAGNESIUM STEARATE (UNII: 70097M6I30) POLYETHYLENE GLYCOL 6000 (UNII: 30IQX730WE) POLYSORBATE 80 (UNII: 6OZP39ZG8H) SODIUM STARCH GLYCOLATE TYPE A POTATO (UNII: 5856J3G2A2) STARCH, PREGELATINIZED CORN (UNII: O8232NY3SJ) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) Product Characteristics Color WHITE Score no score Shape ROUND Size 8mm Flavor Imprint Code U;116 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 29300-116-16 60 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 07/01/2013 2 NDC: 29300-116-01 100 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 07/01/2013 3 NDC: 29300-116-05 500 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 07/01/2013 4 NDC: 29300-116-10 1000 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 07/01/2013 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA090162 07/01/2013 TOPIRAMATE
topiramate tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 29300-117 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength TOPIRAMATE (UNII: 0H73WJJ391) (TOPIRAMATE - UNII:0H73WJJ391) TOPIRAMATE 100 mg Inactive Ingredients Ingredient Name Strength CELLULOSE, MICROCRYSTALLINE (UNII: OP1R32D61U) FERRIC OXIDE RED (UNII: 1K09F3G675) FERRIC OXIDE YELLOW (UNII: EX438O2MRT) HYPROMELLOSE 2910 (6 MPA.S) (UNII: 0WZ8WG20P6) LACTOSE MONOHYDRATE (UNII: EWQ57Q8I5X) MAGNESIUM STEARATE (UNII: 70097M6I30) POLYETHYLENE GLYCOL 6000 (UNII: 30IQX730WE) POLYSORBATE 80 (UNII: 6OZP39ZG8H) SODIUM STARCH GLYCOLATE TYPE A POTATO (UNII: 5856J3G2A2) STARCH, PREGELATINIZED CORN (UNII: O8232NY3SJ) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) Product Characteristics Color RED (Salmon) Score no score Shape ROUND Size 10mm Flavor Imprint Code U;117 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 29300-117-16 60 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 07/01/2013 2 NDC: 29300-117-01 100 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 07/01/2013 3 NDC: 29300-117-05 500 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 07/01/2013 4 NDC: 29300-117-10 1000 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 07/01/2013 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA090162 07/01/2013 TOPIRAMATE
topiramate tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 29300-118 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength TOPIRAMATE (UNII: 0H73WJJ391) (TOPIRAMATE - UNII:0H73WJJ391) TOPIRAMATE 200 mg Inactive Ingredients Ingredient Name Strength CELLULOSE, MICROCRYSTALLINE (UNII: OP1R32D61U) FERRIC OXIDE YELLOW (UNII: EX438O2MRT) HYPROMELLOSE 2910 (6 MPA.S) (UNII: 0WZ8WG20P6) LACTOSE MONOHYDRATE (UNII: EWQ57Q8I5X) MAGNESIUM STEARATE (UNII: 70097M6I30) POLYETHYLENE GLYCOL 6000 (UNII: 30IQX730WE) POLYSORBATE 80 (UNII: 6OZP39ZG8H) SODIUM STARCH GLYCOLATE TYPE A POTATO (UNII: 5856J3G2A2) STARCH, PREGELATINIZED CORN (UNII: O8232NY3SJ) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) Product Characteristics Color YELLOW Score no score Shape ROUND Size 13mm Flavor Imprint Code U;118 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 29300-118-16 60 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 07/01/2013 2 NDC: 29300-118-01 100 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 07/01/2013 3 NDC: 29300-118-05 500 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 07/01/2013 4 NDC: 29300-118-10 1000 in 1 BOTTLE, PLASTIC; Type 0: Not a Combination Product 07/01/2013 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA090162 07/01/2013 Labeler - Unichem Pharmaceuticals (USA), Inc. (181620514)
![Topiramate Tablets, USP 25 mg [60T]](https://fda.report/DailyMed/6ee00e82-799d-445e-b658-a9712c49a28e/725edb08-469b-42f5-9b5a-e3e72554b5cb-04.jpg)
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.