These highlights do not include all the information needed to use QUETIAPINE FUMARATE EXTENDED-RELEASE TABLETS safely and effectively. See full prescribing information for QUETIAPINE FUMARATE EXTENDED-RELEASE TABLETS. QUETIAPINE FUMARATE EXTENDED-RELEASE tablets, for oral useInitial U.S. Approval: 1997
Quetiapine Fumarate by
Drug Labeling and Warnings
Quetiapine Fumarate by is a Prescription medication manufactured, distributed, or labeled by Par Pharmaceutical Inc., AstraZeneca PLC. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
QUETIAPINE FUMARATE EXTENDED RELEASE- quetiapine fumarate tablet, extended release
Par Pharmaceutical Inc.
----------
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use QUETIAPINE FUMARATE EXTENDED-RELEASE TABLETS safely and effectively. See full prescribing information for QUETIAPINE FUMARATE EXTENDED-RELEASE TABLETS.
QUETIAPINE FUMARATE EXTENDED-RELEASE tablets, for oral use Initial U.S. Approval: 1997 WARNING: INCREASED MORTALITY IN ELDERLY PATIENTS WITH DEMENTIA-RELATED PSYCHOSIS; and SUICIDAL THOUGHTS AND BEHAVIORSSee full prescribing information for complete boxed warning.Increased Mortality in Elderly Patients with Dementia-Related Psychosis
Suicidal Thoughts and Behaviors RECENT MAJOR CHANGESINDICATIONS AND USAGEDOSAGE AND ADMINISTRATION
DOSAGE FORMS AND STRENGTHSExtended-Release Tablets: 50 mg, 150 mg, 200 mg, and 300 mg (3) CONTRAINDICATIONSKnown hypersensitivity to quetiapine fumarate extended-release tablets or any components in the formulation. (4) WARNINGS AND PRECAUTIONS
ADVERSE REACTIONSMost common adverse reactions (incidence ≥5% and twice placebo): Adults: somnolence, dry mouth, constipation, dizziness, increased appetite, dyspepsia, weight gain, fatigue, dysarthria, and nasal congestion (6.1) Children and Adolescents: somnolence, dizziness, fatigue, increased appetite, nausea, vomiting, dry mouth, tachycardia, weight increased (6.1) To report SUSPECTED ADVERSE REACTIONS, contact AstraZeneca at 1-800-236-9933 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch. DRUG INTERACTIONS
USE IN SPECIFIC POPULATIONS
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide. Revised: 10/2019 |
FULL PRESCRIBING INFORMATION
WARNING: INCREASED MORTALITY IN ELDERLY PATIENTS WITH DEMENTIA-RELATED PSYCHOSIS; and SUICIDAL THOUGHTS AND BEHAVIORS
Increased Mortality in Elderly Patients with Dementia-Related Psychosis
Elderly patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk of death [see Warnings and Precautions (5.1)]. Quetiapine fumarate extended-release tablets are not approved for the treatment of patients with dementia-related psychosis [see Warnings and Precautions (5.1)].
Suicidal Thoughts and Behavior
Antidepressants increased the risk of suicidal thoughts and behavior in children, adolescents, and young adults in short-term studies. These studies did not show an increase in the risk of suicidal thoughts and behavior with antidepressant use in patients over age 24; there was a reduction in risk with antidepressant use in patients aged 65 and older [see Warnings and Precautions (5.2)].
In patients of all ages who are started on antidepressant therapy, monitor closely for worsening, and for emergence of suicidal thoughts and behaviors. Advise families and caregivers of the need for close observation and communication with the prescriber [see Warnings and Precautions (5.2)].
Quetiapine fumarate extended-release tablets are not approved for use in pediatric patients under ten years of age [see Use in Specific Populations (8.4)].
1 INDICATIONS AND USAGE
1.1 Schizophrenia
Quetiapine fumarate extended-release tablets are indicated for the treatment of schizophrenia. The efficacy of quetiapine fumarate extended-release tablets in schizophrenia was established in one 6-week and one maintenance trial in adults with schizophrenia. Efficacy was supported by three 6-week trials in adults with schizophrenia and one 6-week trial in adolescents with schizophrenia (13-17 years) treated with quetiapine fumarate tablets [see Clinical Studies (14.1)].
1.2 Bipolar Disorder
Quetiapine fumarate extended-release tablets are indicated for the acute treatment of manic or mixed episodes associated with bipolar I disorder, both as monotherapy and as an adjunct to lithium or divalproex. The efficacy of quetiapine fumarate extended-release tablets in manic or mixed episodes of bipolar I disorder was established in one 3-week trial in adults with manic or mixed episodes associated with bipolar I disorder. Efficacy was supported by two 12-week monotherapy trials and one 3-week adjunctive trial in adults with manic episodes associated with bipolar I disorder as well as one 3-week monotherapy trial in children and adolescents (10-17 years) with manic episodes associated with bipolar I disorder treated with quetiapine fumarate tablets [see Clinical Studies (14.2)].
Quetiapine fumarate extended-release tablets are indicated for the acute treatment of depressive episodes associated with bipolar disorder. The efficacy of quetiapine fumarate extended-release tablets was established in one 8-week trial in adults with bipolar I or II disorder and supported by two 8-week trials in adults with bipolar I or II disorder treated with quetiapine fumarate tablets [see Clinical Studies (14.2)].
Quetiapine fumarate extended-release tablets are indicated for the maintenance treatment of bipolar I disorder, as an adjunct to lithium or divalproex. Efficacy was extrapolated from two maintenance trials in adults with bipolar I disorder treated with quetiapine fumarate tablets. The effectiveness of monotherapy for the maintenance treatment of bipolar I disorder has not been systematically evaluated in controlled clinical trials [see Clinical Studies (14.2)].
1.3 Adjunctive Treatment of Major Depressive Disorder (MDD)
Quetiapine fumarate extended-release tablets are indicated for use as adjunctive therapy to antidepressants for the treatment of MDD. The efficacy of quetiapine fumarate extended-release tablets as adjunctive therapy to antidepressants in MDD was established in two 6-week trials in adults with MDD who had an inadequate response to antidepressant treatment [see Clinical Studies (14.3)].
1.4 Special Considerations in Treating Pediatric Schizophrenia and Bipolar I Disorder
Pediatric schizophrenia and bipolar I disorder are serious mental disorders, however, diagnosis can be challenging. For pediatric schizophrenia, symptom profiles can be variable, and for bipolar I disorder, patients may have variable patterns of periodicity of manic or mixed symptoms. It is recommended that medication therapy for pediatric schizophrenia and bipolar I disorder be initiated only after a thorough diagnostic evaluation has been performed and careful consideration given to the risks associated with medication treatment. Medication treatment for both pediatric schizophrenia and bipolar I disorder is indicated as part of a total treatment program that often includes psychological, educational and social interventions.
2 DOSAGE AND ADMINISTRATION
2.1 Important Administration Instructions
Quetiapine fumarate extended-release tablets should be swallowed whole and not split, chewed, or crushed.
It is recommended that quetiapine fumarate extended-release tablets be taken without food or with a light meal (approximately 300 calories) [see Clinical Pharmacology (12.3)].
Quetiapine fumarate extended-release tablets should be administered once daily, preferably in the evening.
2.2 Recommended Dosing
The recommended initial dose, titration, dose range and maximum quetiapine fumarate extended-release tablets dose for each approved indication is displayed in Table 1 below. After initial dosing, adjustments can be made upwards or downwards, if necessary, depending upon the clinical response and tolerability of the patient [see Clinical Studies (14.1, 14.2 and 14.3)].
|
Indication |
Initial Dose and Titration |
Recommended Dose |
Maximum Dose |
|
Schizophrenia-Adults |
Day 1: 300 mg/day Dose increases can be made at intervals as short as 1 day and in increments of up to 300 mg/day |
400-800 mg/day |
800 mg/day |
|
Schizophrenia-Adolescents (13 to 17 years) |
Day 1: 50 mg/day Day 2: 100 mg/day Day 3: 200 mg/day Day 4: 300 mg/day Day 5: 400 mg/day |
400-800 mg/day |
800 mg/day |
|
Schizophrenia Maintenance-Monotherapy-Adults |
Not applicable |
400-800 mg/day |
800 mg/day |
|
Bipolar I Disorder manic or mixed-Acute monotherapy or adjunct to lithium or divalproex-Adults |
Day 1: 300 mg/day Day 2: 600 mg/day Day 3: between 400 and 800 mg/day |
400-800 mg/day |
800 mg/day |
|
Bipolar I Disorder, manic-Acute monotherapy-Children and Adolescents (10 to 17 years) |
Day 1: 50 mg/day Day 2: 100 mg/day Day 3: 200 mg/day Day 4: 300 mg/day Day 5: 400 mg/day |
400-600 mg/day |
600 mg/day |
|
Bipolar Disorder, Depressive Episodes -Adults |
Day 1: 50 mg/day Day 2: 100 mg/day Day 3: 200 mg/day Day 4: 300 mg/day |
300 mg/day |
300 mg/day |
|
Bipolar I Disorder Maintenance-Adjunct to lithium or divalproex-Adults |
not applicable |
400-800 mg/day |
800 mg/day |
|
Major Depressive Disorder-Adjunctive Therapy with Antidepressants-Adults |
Day 1: 50 mg/day Day 2: 50 mg/day Day 3: 150 mg/day |
150-300 mg/day |
300 mg/day |
Maintenance Treatment for Schizophrenia and Bipolar I Disorder
Maintenance Treatment—Patients should be periodically reassessed to determine the need for maintenance treatment and the appropriate dose for such treatment [see Clinical Studies (14.1, 14.2)].
2.3 Dose Modifications in Elderly Patients
Consideration should be given to a slower rate of dose titration and a lower target dose in the elderly and in patients who are debilitated or who have a predisposition to hypotensive reactions [see Use in Specific Populations (8.5, 8.7), and Clinical Pharmacology (12.3)]. When indicated, dose escalation should be performed with caution in these patients.
Elderly patients should be started on quetiapine fumarate extended-release tablets 50 mg/day and the dose can be increased in increments of 50 mg/day depending on the clinical response and tolerability of the individual patient.
2.4 Dose Modifications in Hepatically Impaired Patients
Patients with hepatic impairment should be started on quetiapine fumarate extended-release tablets 50 mg/day. The dose can be increased daily in increments of 50 mg/day to an effective dose, depending on the clinical response and tolerability of the patient.
2.5 Dose Modifications when used with CYP3A4 Inhibitors
Quetiapine fumarate extended-release tablets dose should be reduced to one sixth of original dose when co-medicated with a potent CYP3A4 inhibitor (e.g., ketoconazole, itraconazole, indinavir, ritonavir, nefazodone, etc.). When the CYP3A4 inhibitor is discontinued, the dose of quetiapine fumarate extended-release tablets should be increased by 6-fold [see Clinical Pharmacology (12.3) and Drug Interactions (7.1)].
2.6 Dose Modifications when used with CYP3A4 Inducers
Quetiapine fumarate extended-release tablets dose should be increased up to 5-fold of the original dose when used in combination with a chronic treatment (e.g., greater than 7-14 days) of a potent CYP3A4 inducer (e.g., phenytoin, carbamazepine, rifampin, avasimibe, St. John’s wort etc.). The dose should be titrated based on the clinical response and tolerance of the individual patient. When the CYP3A4 inducer is discontinued, the dose of quetiapine fumarate extended-release tablets should be reduced to the original level within 7-14 days [see Clinical Pharmacology (12.3) and Drug Interactions (7.1)].
2.7 Re-initiation of Treatment in Patients Previously Discontinued
Although there are no data to specifically address re-initiation of treatment, it is recommended that when restarting therapy of patients who have been off quetiapine fumarate extended-release tablets for more than one-week, the initial dosing schedule should be followed. When restarting patients who have been off quetiapine fumarate extended-release tablets for less than one-week, gradual dose escalation may not be required and the maintenance dose may be re-initiated.
2.8 Switching Patients from Quetiapine Fumarate Tablets to Quetiapine Fumarate Extended-Release Tablets
Patients who are currently being treated with quetiapine fumarate tablets (immediate release formulation) may be switched to quetiapine fumarate extended-release tablets at the equivalent total daily dose taken once daily. Individual dosage adjustments may be necessary.
2.9 Switching from Antipsychotics
There are no systematically collected data to specifically address switching patients from other antipsychotics to quetiapine fumarate extended-release tablets, or concerning concomitant administration with other antipsychotics. While immediate discontinuation of the previous antipsychotic treatment may be acceptable for some patients, more gradual discontinuation may be most appropriate for others. In all cases, the period of overlapping antipsychotic administration should be minimized. When switching patients from depot antipsychotics, if medically appropriate, initiate quetiapine fumarate extended-release tablets therapy in place of the next scheduled injection. The need for continuing existing extrapyramidal syndrome medication should be re-evaluated periodically.
3 DOSAGE FORMS AND STRENGTHS
- 50 mg extended-release tablets are peach, film coated, capsule-shaped, biconvex, intagliated tablet with “XR 50” on one side and plain on the other side
- 150 mg extended-release tablets are white, film-coated, capsule-shaped, biconvex, intagliated tablet with “XR 150” on one side and plain on the other side
- 200 mg extended-release tablets are yellow, film-coated, capsule-shaped, biconvex, intagliated tablet with “XR 200” on one side and plain on the other side
- 300 mg extended-release tablets are pale yellow, film-coated, capsule-shaped, biconvex, intagliated tablet with “XR 300” on one side and plain on the other side
4 CONTRAINDICATIONS
Hypersensitivity to quetiapine or to any excipients in the quetiapine fumarate extended-release tablets formulation. Anaphylactic reactions have been reported in patients treated with quetiapine fumarate extended-release tablets.
5 WARNINGS AND PRECAUTIONS
5.1 Increased Mortality in Elderly Patients with Dementia-Related Psychosis
Elderly patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk of death. Analysis of 17 placebo-controlled trials (modal duration of 10 weeks), largely in patients taking atypical antipsychotic drugs, revealed a risk of death in drug-treated patients of between 1.6 to 1.7 times the risk of death in placebo-treated patients. Over the course of a typical 10-week controlled trial, the rate of death in drug-treated patients was about 4.5%, compared to a rate of about 2.6% in the placebo group. Although the causes of death were varied, most of the deaths appeared to be either cardiovascular (e.g., heart failure, sudden death) or infectious (e.g., pneumonia) in nature. Observational studies suggest that, similar to atypical antipsychotic drugs, treatment with conventional antipsychotic drugs may increase mortality. The extent to which the findings of increased mortality in observational studies may be attributed to the antipsychotic drug as opposed to some characteristic(s) of the patients is not clear. Quetiapine fumarate extended-release tablets are not approved for the treatment of patients with dementia-related psychosis [see Boxed Warning].
5.2 Suicidal Thoughts and Behaviors in Adolescents and Young Adults
Patients with major depressive disorder (MDD), both adult and pediatric, may experience worsening of their depression and/or the emergence of suicidal ideation and behavior (suicidality) or unusual changes in behavior, whether or not they are taking antidepressant medications, and this risk may persist until significant remission occurs. Suicide is a known risk of depression and certain other psychiatric disorders, and these disorders themselves are the strongest predictors of suicide. There has been a long-standing concern, however, that antidepressants may have a role in inducing worsening of depression and the emergence of suicidality in certain patients during the early phases of treatment. Pooled analyses of short-term placebo-controlled trials of antidepressant drugs (SSRIs and others) showed that these drugs increase the risk of suicidal thinking and behavior (suicidality) in children, adolescents, and young adults (ages 18-24) with major depressive disorder (MDD) and other psychiatric disorders. Short-term studies did not show an increase in the risk of suicidality with antidepressants compared to placebo in adults beyond age 24; there was a reduction with antidepressants compared to placebo in adults aged 65 and older.
The pooled analyses of placebo-controlled trials in children and adolescents with MDD, obsessive compulsive disorder (OCD), or other psychiatric disorders included a total of 24 short-term trials of 9 antidepressant drugs in over 4,400 patients. The pooled analyses of placebo-controlled trials in adults with MDD or other psychiatric disorders included a total of 295 short-term trials (median duration of 2 months) of 11 antidepressant drugs in over 77,000 patients. There was considerable variation in risk of suicidality among drugs, but a tendency toward an increase in the younger patients for almost all drugs studied. There were differences in absolute risk of suicidality across the different indications, with the highest incidence in MDD. The risk differences (drug vs. placebo), however, were relatively stable within age strata and across indications. These risk differences (drug-placebo difference in the number of cases of suicidality per 1000 patients treated) are provided in Table 2.
| Age Range | Drug-Placebo Difference in Number of Cases of Suicidality per 1000 Patients Treated |
|---|---|
|
Increases Compared to Placebo |
|
|
<18 |
14 additional cases |
|
18-24 |
5 additional cases |
|
Decreases Compared to Placebo |
|
|
25-64 |
1 fewer case |
|
≥65 |
6 fewer cases |
No suicides occurred in any of the pediatric trials. There were suicides in the adult trials, but the number was not sufficient to reach any conclusion about drug effect on suicide.
It is unknown whether the suicidality risk extends to longer-term use, i.e., beyond several months. However, there is substantial evidence from placebo-controlled maintenance trials in adults with depression that the use of antidepressants can delay the recurrence of depression.
All patients being treated with antidepressants for any indication should be monitored appropriately and observed closely for clinical worsening, suicidality, and unusual changes in behavior, especially during the initial few months of a course of drug therapy, or at times of dose changes, either increases or decreases.
The following symptoms, anxiety, agitation, panic attacks, insomnia, irritability, hostility, aggressiveness, impulsivity, akathisia (psychomotor restlessness), hypomania, and mania, have been reported in adult and pediatric patients being treated with antidepressants for major depressive disorder as well as for other indications, both psychiatric and non-psychiatric. Although a causal link between the emergence of such symptoms and either the worsening of depression and/or the emergence of suicidal impulses has not been established, there is concern that such symptoms may represent precursors to emerging suicidality.
Consideration should be given to changing the therapeutic regimen, including possibly discontinuing the medication, in patients whose depression is persistently worse, or who are experiencing emergent suicidality or symptoms that might be precursors to worsening depression or suicidality, especially if these symptoms are severe, abrupt in onset, or were not part of the patient's presenting symptoms.
Families and caregivers of patients being treated with antidepressants for major depressive disorder or other indications, both psychiatric and non-psychiatric, should be alerted about the need to monitor patients for the emergence of agitation, irritability, unusual changes in behavior, and the other symptoms described above, as well as the emergence of suicidality, and to report such symptoms immediately to healthcare providers. Such monitoring should include daily observation by families and caregivers. Prescriptions for quetiapine fumarate extended-release tablets should be written for the smallest quantity of tablets consistent with good patient management, in order to reduce the risk of overdose.
Screening Patients for Bipolar Disorder: A major depressive episode may be the initial presentation of bipolar disorder. It is generally believed (though not established in controlled trials) that treating such an episode with an antidepressant alone may increase the likelihood of precipitation of a mixed/manic episode in patients at risk for bipolar disorder. Whether any of the symptoms described above represent such a conversion is unknown. However, prior to initiating treatment with an antidepressant, including quetiapine fumarate extended-release tablets, patients with depressive symptoms should be adequately screened to determine if they are at risk for bipolar disorder; such screening should include a detailed psychiatric history, including a family history of suicide, bipolar disorder, and depression.
5.3 Cerebrovascular Adverse Reactions, Including Stroke, in Elderly Patients with Dementia-Related Psychosis
In placebo-controlled trials with risperidone, aripiprazole, and olanzapine in elderly subjects with dementia, there was a higher incidence of cerebrovascular adverse reactions (cerebrovascular accidents and transient ischemic attacks), including fatalities, compared to placebo-treated subjects. Quetiapine fumarate extended-release tablets are not approved for the treatment of patients with dementia-related psychosis [see Boxed Warning and Warnings and Precautions (5.1)].
5.4 Neuroleptic Malignant Syndrome (NMS)
A potentially fatal symptom complex sometimes referred to as Neuroleptic Malignant Syndrome (NMS) has been reported in association with administration of antipsychotic drugs, including quetiapine. Rare cases of NMS have been reported with quetiapine. Clinical manifestations of NMS are hyperpyrexia, muscle rigidity, altered mental status, and evidence of autonomic instability (irregular pulse or blood pressure, tachycardia, diaphoresis, and cardiac dysrhythmia). Additional signs may include elevated creatine phosphokinase, myoglobinuria (rhabdomyolysis), and acute renal failure.
The diagnostic evaluation of patients with this syndrome is complicated. In arriving at a diagnosis, it is important to exclude cases where the clinical presentation includes both serious medical illness (e.g., pneumonia, systemic infection, etc.) and untreated or inadequately treated extrapyramidal signs and symptoms (EPS). Other important considerations in the differential diagnosis include central anticholinergic toxicity, heat stroke, drug fever, and primary central nervous system (CNS) pathology.
The management of NMS should include: 1) immediate discontinuation of antipsychotic drugs and other drugs not essential to concurrent therapy; 2) intensive symptomatic treatment and medical monitoring; and 3) treatment of any concomitant serious medical problems for which specific treatments are available. There is no general agreement about specific pharmacological treatment regimens for NMS.
If a patient requires antipsychotic drug treatment after recovery from NMS, the potential reintroduction of drug therapy should be carefully considered. The patient should be carefully monitored since recurrences of NMS have been reported.
5.5 Metabolic Changes
Atypical antipsychotic drugs have been associated with metabolic changes that include hyperglycemia/diabetes mellitus, dyslipidemia, and body weight gain. While all of the drugs in the class have been shown to produce some metabolic changes, each drug has its own specific risk profile. In some patients, a worsening of more than one of the metabolic parameters of weight, blood glucose, and lipids was observed in clinical studies. Changes in these metabolic profiles should be managed as clinically appropriate.
Hyperglycemia and Diabetes Mellitus
Hyperglycemia, in some cases extreme and associated with ketoacidosis or hyperosmolar coma or death, has been reported in patients treated with atypical antipsychotics, including quetiapine. Assessment of the relationship between atypical antipsychotic use and glucose abnormalities is complicated by the possibility of an increased background risk of diabetes mellitus in patients with schizophrenia and the increasing incidence of diabetes mellitus in the general population. Given these confounders, the relationship between atypical antipsychotic use and hyperglycemia-related adverse reactions is not completely understood. However, epidemiological studies suggest an increased risk of hyperglycemia-related adverse reactions in patients treated with the atypical antipsychotics. Precise risk estimates for hyperglycemia-related adverse reactions in patients treated with atypical antipsychotics are not available.
Patients with an established diagnosis of diabetes mellitus who are started on atypical antipsychotics should be monitored regularly for worsening of glucose control. Patients with risk factors for diabetes mellitus (e.g., obesity, family history of diabetes) who are starting treatment with atypical antipsychotics should undergo fasting blood glucose testing at the beginning of treatment and periodically during treatment. Any patient treated with atypical antipsychotics should be monitored for symptoms of hyperglycemia including polydipsia, polyuria, polyphagia, and weakness. Patients who develop symptoms of hyperglycemia during treatment with atypical antipsychotics should undergo fasting blood glucose testing. In some cases, hyperglycemia has resolved when the atypical antipsychotic was discontinued; however, some patients required continuation of anti-diabetic treatment despite discontinuation of the suspect drug.
Adults:
|
|
||||
|
Laboratory Analyte |
Category Change (At Least Once) from Baseline |
Treatment Arm |
N |
Patients n (%) |
|
Fasting Glucose |
Normal to High (<100 mg/dL to ≥126 mg/dL) |
Quetiapine |
2907 |
71 (2.4%) |
|
Placebo |
1346 |
19 (1.4%) |
||
|
Borderline to High (≥100 mg/dL and <126 mg/dL to ≥126 mg/dL) |
Quetiapine |
572 |
67 (11.7%) |
|
|
Placebo |
279 |
33 (11.8%) |
||
In a 24-week trial (active-controlled, 115 patients treated with quetiapine fumarate tablets) designed to evaluate glycemic status with oral glucose tolerance testing of all patients, at week 24 the incidence of post-glucose challenge glucose level ≥200 mg/dL was 1.7% and the incidence of a fasting blood glucose level ≥126 mg/dL was 2.6%. The mean change in fasting glucose from baseline was 3.2 mg/dL and mean change in 2-hour glucose from baseline was -1.8 mg/dL for quetiapine.
In 2 long-term placebo-controlled randomized withdrawal clinical trials for bipolar I disorder maintenance, mean exposure of 213 days for quetiapine fumarate tablets (646 patients) and 152 days for placebo (680 patients), the mean change in glucose from baseline was +5.0 mg/dL for quetiapine and -0.05 mg/dL for placebo. The exposure-adjusted rate of any increased blood glucose level (≥126 mg/dL) for patients more than 8 hours since a meal (however, some patients may not have been precluded from calorie intake from fluids during fasting period) was 18.0 per 100 patient years for quetiapine fumarate tablets (10.7% of patients; n=556) and 9.5 for placebo per 100 patient years (4.6% of patients; n=581).
Table 4 shows the percentage of patients with shifts in blood glucose to ≥126 mg/dL from normal baseline in MDD adjunct therapy trials by dose.
|
Laboratory Analyte |
Treatment Arm |
N |
Patients n (%) |
|
Blood Glucose ≥126 mg/dL |
Quetiapine fumarate extended-release tablets 150 mg |
280 |
19 (7%) |
|
Quetiapine fumarate extended-release tablets 300 mg |
269 |
32 (12%) |
|
|
Placebo |
277 |
17 (6%) |
Children and Adolescents: Safety and effectiveness of quetiapine fumarate extended-release tablets is supported from studies of quetiapine fumarate tablets in children and adolescent patients 10 to 17 years of age [see Clinical Studies (14.2)]. In a placebo-controlled quetiapine fumarate extended-release tablets monotherapy study (8 weeks duration) of children and adolescent patients (10-17 years of age) with bipolar depression, in which efficacy was not established, the mean change in fasting glucose levels for quetiapine fumarate extended-release tablets (n=60) compared to placebo (n=62) was 1.8 mg/dL versus 1.6 mg/dL. In this study, there were no patients in the quetiapine fumarate extended-release tablets or placebo-treated groups with a baseline normal fasting glucose level (<100 mg/dL) that had an increase in blood glucose level ≥126 mg/dL. There was one patient in the quetiapine fumarate extended-release tablets group with a baseline borderline fasting glucose level (≥100 mg/dL and <126 mg/dL) who had an increase in blood glucose level of >126 mg/dL compared to zero patients in the placebo group.
In a placebo-controlled quetiapine fumarate tablets monotherapy study of adolescent patients (13-17 years of age) with schizophrenia (6 weeks duration), the mean change in fasting glucose levels for quetiapine fumarate tablets (n=138) compared to placebo (n=67) was -0.75 mg/dL versus -1.70 mg/dL. In a placebo-controlled quetiapine fumarate tablets monotherapy study of children and adolescent patients (10-17 years of age) with bipolar mania (3 weeks duration), the mean change in fasting glucose level for quetiapine fumarate tablets (n=170) compared to placebo (n=81) was 3.62 mg/dL versus -1.17 mg/dL. No patient in either study with a baseline normal fasting glucose level (<100 mg/dL) or a baseline borderline fasting glucose level (≥100 mg/dL and <126 mg/dL) had a blood glucose level of ≥126 mg/dL.
Dyslipidemia
Adults:
Table 5 shows the percentage of patients with changes in cholesterol and triglycerides from baseline by indication in clinical trials with quetiapine fumarate extended-release tablets.
|
|
||||
|
Laboratory Analyte |
Indication |
Treatment Arm |
N |
Patients n (%) |
|
Total Cholesterol ≥240 mg/dL |
Schizophrenia* |
Quetiapine fumarate extended-release tablets |
718 |
67 (9%) |
|
Placebo |
232 |
21 (9%) |
||
|
Bipolar Depression† |
Quetiapine fumarate extended-release tablets |
85 |
6 (7%) |
|
|
Placebo |
106 |
3 (3%) |
||
|
Bipolar Mania‡ |
Quetiapine fumarate extended-release tablets |
128 |
9 (7%) |
|
|
Placebo |
134 |
5 (4%) |
||
|
Major Depressive Disorder (Adjunct Therapy)* |
Quetiapine fumarate extended-release tablets |
420 |
67 (16%) |
|
|
Placebo |
213 |
15 (7%) |
||
|
Triglycerides ≥200 mg/dL |
Schizophrenia* |
Quetiapine fumarate extended-release tablets |
659 |
118 (18%) |
|
Placebo |
214 |
11 (5%) |
||
|
Bipolar Depression† |
Quetiapine fumarate extended-release tablets |
84 |
7 (8%) |
|
|
Placebo |
93 |
7 (8%) |
||
|
Bipolar Mania‡ |
Quetiapine fumarate extended-release tablets |
102 |
15 (15%) |
|
|
Placebo |
125 |
8 (6%) |
||
|
Major Depressive Disorder (Adjunct Therapy)* |
Quetiapine fumarate extended-release tablets |
458 |
75 (16%) |
|
|
Placebo |
223 |
18 (8%) |
||
|
LDL-Cholesterol ≥160 mg/dL |
Schizophrenia* |
Quetiapine fumarate extended-release tablets |
691 |
47 (7%) |
|
Placebo |
227 |
17 (8%) |
||
|
Bipolar Depression† |
Quetiapine fumarate extended-release tablets |
86 |
3 (4%) |
|
|
Placebo |
104 |
2 (2%) |
||
|
Bipolar Mania‡ |
Quetiapine fumarate extended-release tablets |
125 |
5 (4%) |
|
|
Placebo |
135 |
2 (2%) |
||
|
Major Depressive Disorder (Adjunct Therapy)* |
Quetiapine fumarate extended-release tablets |
457 |
51 (11%) |
|
|
Placebo |
219 |
21 (10%) |
||
|
HDL-Cholesterol ≤40 mg/dL |
Schizophrenia* |
Quetiapine fumarate extended-release tablets |
600 |
87 (15%) |
|
Placebo |
195 |
23 (12%) |
||
|
Bipolar Depression† |
Quetiapine fumarate extended-release tablets |
78 |
7 (9%) |
|
|
Placebo |
83 |
6 (7%) |
||
|
Bipolar Mania‡ |
Quetiapine fumarate extended-release tablets |
100 |
19 (19%) |
|
|
Placebo |
115 |
15 (13%) |
||
|
Major Depressive Disorder (Adjunct Therapy)* |
Quetiapine fumarate extended-release tablets |
470 |
34 (7%) |
|
|
Placebo |
230 |
19 (8%) |
||
In quetiapine fumarate tablets clinical trials for schizophrenia, the percentage of patients with shifts in cholesterol and triglycerides from baseline to clinically significant levels were 18% (placebo: 7%) and 22% (placebo: 16%). HDL-cholesterol and LDL-cholesterol parameters were not measured in these studies. In quetiapine fumarate tablets clinical trials for bipolar depression, the following percentage of patients had shifts from baseline to clinically significant levels for the four lipid parameters measured: total cholesterol 9% (placebo: 6%); triglycerides 14% (placebo: 9%); LDL-cholesterol 6% (placebo: 5%) and HDL-cholesterol 14% (placebo: 14%). Lipid parameters were not measured in the bipolar mania studies.
Table 6 shows the percentage of patients in MDD adjunctive therapy trials with clinically significant shifts in total-cholesterol, triglycerides, LDL-cholesterol and HDL-cholesterol from baseline by dose.
|
|
|||
|
Laboratory Analyte |
Treatment Arm* |
N |
Patients n (%) |
|
Cholesterol ≥240 mg/dL |
Quetiapine fumarate extended-release tablets 150 mg |
223 |
41 (18%) |
|
Quetiapine fumarate extended-release tablets 300 mg |
197 |
26 (13%) |
|
|
Placebo |
213 |
15 (7%) |
|
|
Triglycerides ≥200 mg/dL |
Quetiapine fumarate extended-release tablets 150 mg |
232 |
36 (16%) |
|
Quetiapine fumarate extended-release tablets 300 mg |
226 |
39 (17%) |
|
|
Placebo |
223 |
18 (8%) |
|
|
LDL-Cholesterol ≥160 mg/dL |
Quetiapine fumarate extended-release tablets 150 mg |
242 |
29 (12%) |
|
Quetiapine fumarate extended-release tablets 300 mg |
215 |
22 (10%) |
|
|
Placebo |
219 |
21 (10%) |
|
|
HDL-Cholesterol ≤40 mg/dL |
Quetiapine fumarate extended-release tablets 150 mg |
238 |
14 (6%) |
|
Quetiapine fumarate extended-release tablets 300 mg |
232 |
20 (9%) |
|
|
Placebo |
230 |
19 (8%) |
|
Children and Adolescents:
Safety and effectiveness of quetiapine fumarate extended-release tablets is supported by studies of quetiapine fumarate tablets in children and adolescent patients 10 to 17 years of age [see Clinical Studies (14.1 and 14.2)].
In a placebo-controlled quetiapine fumarate extended-release tablets monotherapy study (8 weeks duration) of children and adolescent patients (10-17 years of age) with bipolar depression, in which efficacy was not established, the percentage of children and adolescents with shifts in total cholesterol (≥200 mg/dL), triglycerides (≥150 mg/dL), LDL-cholesterol (≥130 mg/dL), and HDL-cholesterol (≤40 mg/dL) from baseline to clinically significant levels were: total cholesterol 8% (7/83) for quetiapine fumarate extended-release tablets vs. 6% (5/84) for placebo; triglycerides 28% (22/80) for quetiapine fumarate extended-release tablets vs. 9% (7/82) for placebo; LDL-cholesterol 2% (2/86) for quetiapine fumarate extended-release tablets vs. 4% (3/85) for placebo and HDL-cholesterol 20% (13/65) for quetiapine fumarate extended-release tablets vs 15% (11/74) for placebo.
Table 7 shows the percentage of children and adolescents with shifts in total cholesterol, triglycerides, LDL-cholesterol, and HDL-cholesterol from baseline to clinically significant levels by indication in clinical trials with quetiapine fumarate tablets in adolescents (13-17 years) with schizophrenia and in children and adolescents (10-17 years) with bipolar mania.
|
|
||||
|
Laboratory Analyte |
Indication |
Treatment Arm |
N |
Patients n (%) |
|
Total Cholesterol ≥200 mg/dL |
Schizophrenia* |
Quetiapine fumarate tablets |
107 |
13 (12%) |
|
Placebo |
56 |
1 (2%) |
||
|
Bipolar Mania† |
Quetiapine fumarate tablets |
159 |
16 (10%) |
|
|
Placebo |
66 |
2 (3%) |
||
|
Triglycerides ≥150 mg/dL |
Schizophrena* |
Quetiapine fumarate tablets |
103 |
17 (17%) |
|
Placebo |
51 |
4 (8%) |
||
|
Bipolar Mania† |
Quetiapine fumarate tablets |
149 |
32 (22%) |
|
|
Placebo |
60 |
8 (13%) |
||
|
LDL-Cholesterol ≥130 mg/dL |
Schizophrenia* |
Quetiapine fumarate tablets |
112 |
4 (4%) |
|
Placebo |
60 |
1 (2%) |
||
|
Bipolar Mania† |
Quetiapine fumarate tablets |
169 |
13 (8%) |
|
|
Placebo |
74 |
4 (5%) |
||
|
HDL-Cholesterol ≤40 mg/dL |
Schizophrenia* |
Quetiapine fumarate tablets |
104 |
16 (15%) |
|
Placebo |
54 |
10 (19%) |
||
|
Bipolar Mania† |
Quetiapine fumarate tablets |
154 |
16 (10%) |
|
|
Placebo |
61 |
4 (7%) |
||
Weight Gain
Increases in weight have been observed in clinical trials. Patients receiving quetiapine should receive regular monitoring of weight.
Adults: Table 8 shows the percentage of adult patients with weight gain of ≥7% of body weight by indication.
|
|
||||
|
Vital sign |
Indication |
Treatment Arm |
N |
Patients n (%) |
|
Weight Gain ≥7% of Body Weight |
Schizophrenia* |
Quetiapine fumarate extended-release tablets |
907 |
90 (10%) |
|
Placebo |
299 |
16 (5%) |
||
|
Bipolar Mania† |
Quetiapine fumarate extended-release tablets |
138 |
7 (5%) |
|
|
Placebo |
150 |
0 (0%) |
||
|
Bipolar Depression‡ |
Quetiapine fumarate extended-release tablets |
110 |
9 (8%) |
|
|
Placebo |
125 |
1 (1%) |
||
|
Major Depressive Disorder (Adjunctive Therapy)* |
Quetiapine fumarate extended-release tablets |
616 |
32 (5%) |
|
|
Placebo |
302 |
5 (2%) |
||
In schizophrenia trials, the proportions of patients meeting a weight gain criterion of ≥7% of body weight were compared in a pool of four 3- to 6-week placebo-controlled clinical trials, revealing a statistically significant greater incidence of weight gain for quetiapine fumarate tablets (23%) compared to placebo (6%).
Table 9 shows the percentage of adult patients with weight gain of ≥7% of body weight for MDD by dose.
|
Vital sign |
|
N |
Patients n (%) |
|
Weight Gain ≥7% of Body Weight in MDD Adjunctive Therapy |
Quetiapine fumarate extended-release tablets
|
309 |
10 (3%) |
|
Quetiapine fumarate extended-release tablets
|
307 |
22 (7%) |
|
|
302 |
5 (2%) |
Children and Adolescents: Safety and effectiveness of quetiapine fumarate extended-release tablets is supported by studies of quetiapine fumarate tablets in children and adolescent patients 10 to 17 years of age [see Clinical Studies (14.1 and 14.2)]. In a clinical trial for quetiapine fumarate extended-release tablets in children and adolescents (10-17 years of age) with bipolar depression, in which efficacy was not established, the percentage of patients with weight gain ≥7% of body weight at any time was 15% (14/92) for quetiapine fumarate extended-release tablets vs. 10% (10/100) for placebo. The mean change in body weight was 1.4 kg in the quetiapine fumarate extended-release tablets group vs. 0.6 kg in the placebo group.
Weight gain was greater in patients 10-12 years of age compared to patients 13-17 years of age. The percentage of patients 10-12 years of age with weight gain ≥7% at any time was 28% (7/25) for quetiapine fumarate extended-release tablets vs. 0% (0/28) for placebo. The percentage of patients 13-17 years of age with weight gain ≥7% at any time was 10.4% (7/67) for quetiapine fumarate extended-release tablets vs. 13.9% (10/72) for placebo.
Table 10 shows the percentage of children and adolescents with weight gain ≥7% of body weight in clinical trials with quetiapine fumarate tablets in adolescents (13-17 years) with schizophrenia and in children and adolescents (10-17 years) with bipolar mania.
|
|
||||
|
Vital sign |
Indication |
Treatment Arm |
N |
Patients n (%) |
|
Weight Gain ≥7% of Body Weight |
Schizophrenia* |
Quetiapine fumarate tablets |
111 |
23 (21%) |
|
Placebo |
44 |
3 (7%) |
||
|
Bipolar Mania† |
Quetiapine fumarate tablets |
157 |
18 (12%) |
|
|
Placebo |
68 |
0 (0%) |
||
The mean change in body weight in the schizophrenia trial was 2.0 kg in the quetiapine fumarate group and -0.4 kg in the placebo group and in the bipolar mania trial it was 1.7 kg in the quetiapine fumarate group and 0.4 kg in the placebo group.
In an open-label study that enrolled patients from the above two pediatric trials, 63% of patients (241/380) completed 26 weeks of therapy with quetiapine fumarate tablets. After 26 weeks of treatment, the mean increase in body weight was 4.4 kg. Forty-five percent of the patients gained ≥7% of their body weight, not adjusted for normal growth. In order to adjust for normal growth over 26 weeks, an increase of at least 0.5 standard deviation from baseline in BMI was used as a measure of a clinically significant change; 18.3% of patients on quetiapine fumarate tablets met this criterion after 26 weeks of treatment.
When treating pediatric patients with quetiapine fumarate tablets for any indication, weight gain should be assessed against that expected for normal growth.
5.6 Tardive Dyskinesia
A syndrome of potentially irreversible, involuntary, dyskinetic movements may develop in patients treated with antipsychotic drugs including quetiapine. Although the prevalence of the syndrome appears to be highest among the elderly, especially elderly women, it is impossible to rely upon prevalence estimates to predict, at the inception of antipsychotic treatment, which patients are likely to develop the syndrome. Whether antipsychotic drug products differ in their potential to cause tardive dyskinesia is unknown.
The risk of developing tardive dyskinesia and the likelihood that it will become irreversible are believed to increase as the duration of treatment and the total cumulative dose of antipsychotic drugs administered to the patient increase. However, the syndrome can develop, although much less commonly, after relatively brief treatment periods at low doses or may even arise after discontinuation of treatment.
Tardive dyskinesia may remit, partially or completely, if antipsychotic treatment is withdrawn. Antipsychotic treatment, itself, however, may suppress (or partially suppress) the signs and symptoms of the syndrome and thereby may possibly mask the underlying process. The effect that symptomatic suppression has upon the long-term course of the syndrome is unknown.
Given these considerations, quetiapine fumarate extended-release tablets should be prescribed in a manner that is most likely to minimize the occurrence of tardive dyskinesia. Chronic antipsychotic treatment should generally be reserved for patients who appear to suffer from a chronic illness that (1) is known to respond to antipsychotic drugs, and (2) for whom alternative, equally effective, but potentially less harmful treatments are not available or appropriate. In patients who do require chronic treatment, the smallest dose and the shortest duration of treatment producing a satisfactory clinical response should be sought. The need for continued treatment should be reassessed periodically.
If signs and symptoms of tardive dyskinesia appear in a patient on quetiapine fumarate extended-release tablets, drug discontinuation should be considered. However, some patients may require treatment with quetiapine despite the presence of the syndrome.
5.7 Hypotension
Quetiapine may induce orthostatic hypotension associated with dizziness, tachycardia and, in some patients, syncope, especially during the initial dose-titration period, probably reflecting its ά1-adrenergic antagonist properties. Syncope was reported in 0.3% (5/1866) of the patients treated with quetiapine fumarate extended-release tablets across all indications, compared with 0.2% (2/928) on placebo. Syncope was reported in 1% (28/3265) of the patients treated with quetiapine fumarate tablets, compared with 0.2% (2/954) on placebo. Orthostatic hypotension, dizziness, and syncope may lead to falls.
Quetiapine should be used with particular caution in patients with known cardiovascular disease (history of myocardial infarction or ischemic heart disease, heart failure, or conduction abnormalities), cerebrovascular disease, or conditions which would predispose patients to hypotension (dehydration, hypovolemia, and treatment with antihypertensive medications). If hypotension occurs during titration to the target dose, a return to the previous dose in the titration schedule is appropriate.
5.8 Falls
Atypical antipsychotic drugs, including quetiapine fumarate extended-release tablets, may cause somnolence, postural hypotension, motor, and sensory instability, which may lead to falls and, consequently, fractures or other injuries. For patients with diseases, conditions, or medications that could exacerbate these effects, complete fall risk assessments when initiating antipsychotic treatment and recurrently for patients on long-term antipsychotic therapy.
5.9 Increases in Blood Pressure (Children and Adolescents)
Safety and effectiveness of quetiapine fumarate extended-release tablets are supported by studies of quetiapine fumarate tablets in children and adolescent patients 10-17 years of age [see Clinical Studies (14.1 and 14.2)].
In a placebo-controlled quetiapine fumarate extended-release tablets clinical trial (8 weeks duration) in children and adolescents (10-17 years of age) with bipolar depression, in which efficacy was not established, the incidence of increases at any time in systolic blood pressure (≥20 mmHg) was 6.5% (6/92) for quetiapine fumarate extended-release tablets and 6.0% (6/100) for placebo; the incidence of increases at any time in diastolic blood pressure (≥10 mmHg) was 46.7% (43/92) for quetiapine fumarate extended-release tablets and 36.0% (36/100) for placebo.
In placebo-controlled trials in children and adolescents with schizophrenia (13-17 years old, 6-week duration) or bipolar mania (10-17 years old, 3-week duration), the incidence of increases at any time in systolic blood pressure (≥20 mmHg) was 15.2% (51/335) for quetiapine fumarate tablets and 5.5% (9/163) for placebo; the incidence of increases at any time in diastolic blood pressure (≥10 mmHg) was 40.6% (136/335) for quetiapine fumarate tablets and 24.5% (40/163) for placebo. In the 26-week open-label clinical trial, one child with a reported history of hypertension experienced a hypertensive crisis. Blood pressure in children and adolescents should be measured at the beginning of, and periodically during treatment.
5.10 Leukopenia, Neutropenia, and Agranulocytosis
In clinical trials and postmarketing experience, events of leukopenia/neutropenia have been reported temporally related to atypical antipsychotic agents, including quetiapine fumarate. Agranulocytosis has also been reported.
Agranulocytosis has been reported with quetiapine, including fatal cases and cases in patients without pre-existing risk factors. Neutropenia should be considered in patients presenting with infection, particularly in the absence of obvious predisposing factor(s), or in patients with unexplained fever, and should be managed as clinically appropriate.
Possible risk factors for leukopenia/neutropenia include pre-existing low white cell count (WBC) and history of drug induced leukopenia/neutropenia. Patients with a pre-existing low WBC or a history of drug induced leukopenia/neutropenia should have their complete blood count (CBC) monitored frequently during the first few months of therapy and should discontinue quetiapine fumarate extended-release tablets at the first sign of a decline in WBC in absence of other causative factors.
Patients with neutropenia should be carefully monitored for fever or other symptoms or signs of infection and treated promptly if such symptoms or signs occur. Patients with severe neutropenia (absolute neutrophil count <1000/mm3) should discontinue quetiapine fumarate extended-release tablets and have their WBC followed until recovery.
5.11 Cataracts
The development of cataracts was observed in association with quetiapine treatment in chronic dog studies [see Nonclinical Toxicology (13.2)]. Lens changes have also been observed in adults, children, and adolescents during long-term quetiapine treatment but a causal relationship to quetiapine use has not been established. Nevertheless, the possibility of lenticular changes cannot be excluded at this time. Therefore, examination of the lens by methods adequate to detect cataract formation, such as slit lamp exam or other appropriately sensitive methods, is recommended at initiation of treatment or shortly thereafter, and at 6-month intervals during chronic treatment.
5.12 QT Prolongation
In clinical trials quetiapine was not associated with a persistent increase in QT intervals. However, the QT effect was not systematically evaluated in a thorough QT study. In post marketing experience there were cases reported of QT prolongation in patients who overdosed on quetiapine [see Overdosage (10.1)], in patients with concomitant illness, and in patients taking medicines known to cause electrolyte imbalance or increase QT interval.
The use of quetiapine should be avoided in combination with other drugs that are known to prolong QTc including Class 1A antiarrythmics (e.g., quinidine, procainamide) or Class III antiarrythmics (e.g., amiodarone, sotalol), antipsychotic medications (e.g., ziprasidone, chlorpromazine, thioridazine), antibiotics (e.g., gatifloxacin, moxifloxacin), or any other class of medications known to prolong the QTc interval (e.g., pentamidine, levomethadyl acetate, methadone).
Quetiapine should also be avoided in circumstances that may increase the risk of occurrence of torsade de pointes and/or sudden death including (1) a history of cardiac arrhythmias such as bradycardia; (2) hypokalemia or hypomagnesemia; (3) concomitant use of other drugs that prolong the QTc interval; and (4) presence of congenital prolongation of the QT interval.
Caution should also be exercised when quetiapine is prescribed in patients with increased risk of QT prolongation (e.g., cardiovascular disease, family history of QT prolongation, the elderly, congestive heart failure, and heart hypertrophy).
5.13 Seizures
During short-term clinical trials with quetiapine fumarate extended-release tablets, seizures occurred in 0.05% (1/1866) of patients treated with quetiapine fumarate extended-release tablets across all indications compared to 0.3% (3/928) on placebo. During clinical trials with quetiapine fumarate, seizures occurred in 0.5% (20/3490) of patients treated with quetiapine fumarate tablets compared to 0.2% (2/954) on placebo. As with other antipsychotics, quetiapine fumarate should be used cautiously in patients with a history of seizures or with conditions that potentially lower the seizure threshold, e.g., Alzheimer’s dementia. Conditions that lower the seizure threshold may be more prevalent in a population of 65 years or older.
5.14 Hypothyroidism
Adults: Clinical trials with quetiapine demonstrated dose-related decreases in thyroid hormone levels. The reduction in total and free thyroxine (T4) of approximately 20% at the higher end of the therapeutic dose range was maximal in the first six weeks of treatment and maintained without adaptation or progression during more chronic therapy. In nearly all cases, cessation of quetiapine treatment was associated with a reversal of the effects on total and free T4, irrespective of the duration of treatment. The mechanism by which quetiapine effects the thyroid axis is unclear. If there is an effect on the hypothalamic-pituitary axis, measurement of TSH alone may not accurately reflect a patient’s thyroid status. Therefore, both TSH and free T4, in addition to clinical assessment, should be measured at baseline and at follow-up.
In quetiapine fumarate extended-release tablets clinical trials across all indications 1.8% (24/1336) of patients on quetiapine fumarate extended-release tablets versus 0.6% (3/530) on placebo experienced decreased free thyroxine (<0.8 LLN) and 1.6% (21/1346) on quetiapine fumarate extended-release tablets vs. 3.4% (18/534) on placebo experienced increased thyroid stimulating hormone (TSH). About 0.7% (26/3489) of quetiapine fumarate tablets patients did experience TSH increases in monotherapy studies. Some patients with TSH increases needed replacement thyroid treatment.
In all quetiapine trials, the incidence of shifts in thyroid hormones and TSH were1: decrease in free T4 (<0.8 LLN), 2.0% (357/17513); decrease in total T4 (<0.8 LLN), 4.0% (75/1861); decrease in free T3 (<0.8 LLN), 0.4% (53/13766); decrease in total T3 (<0.8 LLN), 2.0% (26/1312), and increase in TSH (>5 mIU/L), 4.9% (956/19412). In eight patients, where TBG was measured, levels of TBG were unchanged.
1Based on shifts from normal baseline to potentially clinically important value at anytime post-baseline. Shifts in total T4, free T4, total T3 and free T3 are defined as <0.8 x LLN (pmol/L) and shift in TSH is >5 mIU/L at any time.
Table 11 shows the incidence of these shifts in short term placebo-controlled clinical trials.
|
|
|||||||||
|
Total T4 |
Free T4 |
Total T3 |
Free T3 |
TSH |
|||||
|
Quetiapine |
Placebo |
Quetiapine |
Placebo |
Quetiapine |
Placebo |
Quetiapine |
Placebo |
Quetiapine |
Placebo |
|
3.4% (37/1097) |
0.6% (4/651) |
0.7% (52/7218) |
0.1% (4/3668) |
0.5% (2/369) |
0.0% (0/113) |
0.2% (11/5673) |
0.0% (1/2679) |
3.2% (240/7587) |
2.7% (105/3912) |
In short-term placebo-controlled monotherapy trials, the incidence of reciprocal shifts in T3 and TSH was 0.0 % for both quetiapine (1/4800) and placebo (0/2190) and for T4 and TSH the shifts were 0.1% (7/6154) for quetiapine versus 0.0 % (1/3007) for placebo.
Children and Adolescents: Safety and effectiveness of quetiapine fumarate extended-release tablets are supported by studies of quetiapine fumarate tablets in children and adolescent patients 10-17 years of age [see Clinical Studies (14.1 and 14.2)].
In acute placebo-controlled trials in children and adolescent patients with schizophrenia (6-week duration) or bipolar mania (3-week duration), the incidence of shifts at any time for quetiapine fumarate tablets treated patients and placebo-treated patients for elevated TSH was 2.9% (8/280) vs. 0.7% (1/138), respectively, and for decreased total thyroxine was 2.8% (8/289) vs. 0% (0/145), respectively. Of the quetiapine fumarate tablets treated patients with elevated TSH levels, 1 had simultaneous low free T4 level at end of treatment.
5.15 Hyperprolactinemia
Adults: During clinical trials with quetiapine across all indications, the incidence of shifts in prolactin levels to a clinically significant value occurred in 3.6% (158/4416) of patients treated with quetiapine compared to 2.6% (51/1968) on placebo.
Children and Adolescents: Safety and effectiveness of quetiapine fumarate extended-release tablets are supported by studies of quetiapine fumarate tablets in children and adolescent patients 10-17 years of age [see Clinical Studies (14.1 and 14.2)]. In acute placebo-controlled trials in children and adolescent patients with bipolar mania (3-week duration) or schizophrenia (6-week duration), the incidence of shifts in prolactin levels to a value (>20 µg/L males; >26 µg/L females at any time) was 13.4% (18/134) for quetiapine fumarate tablets compared to 4% (3/75) for placebo in males and 8.7% (9/104) for quetiapine fumarate tablets compared to 0% (0/39) for placebo in females.
Like other drugs that antagonize dopamine D2 receptors, quetiapine fumarate extended-release tablets elevate prolactin levels in some patients and the elevation may persist during chronic administration. Hyperprolactinemia, regardless of etiology, may suppress hypothalamic GnRH, resulting in reduced pituitary gonadotrophin secretion. This, in turn, may inhibit reproductive function by impairing gonadal steroidogenesis in both female and male patients. Galactorrhea, amenorrhea, gynecomastia, and impotence have been reported in patients receiving prolactin-elevating compounds. Long-standing hyperprolactinemia when associated with hypogonadism may lead to decreased bone density in both female and male subjects.
Tissue culture experiments indicate that approximately one-third of human breast cancers are prolactin dependent in vitro, a factor of potential importance if the prescription of these drugs is considered in a patient with previously detected breast cancer. As is common with compounds which increase prolactin release, mammary gland, and pancreatic islet cell neoplasia (mammary adenocarcinomas, pituitary, and pancreatic adenomas) was observed in carcinogenicity studies conducted in mice and rats. Neither clinical studies nor epidemiologic studies conducted to date have shown an association between chronic administration of this class of drugs and tumorigenesis in humans, but the available evidence is too limited to be conclusive [see Nonclinical Toxicology (13.1)].
5.16 Potential for Cognitive and Motor Impairment
Somnolence was a commonly reported adverse reaction reported in patients treated with quetiapine especially during the 3-day period of initial dose titration. In schizophrenia trials, somnolence was reported in 24.7% (235/951) of patients on quetiapine fumarate extended-release tablets compared to 10.3% (33/319) of placebo patients. In a bipolar depression clinical trial, somnolence was reported in 51.8% (71/137) of patients on quetiapine fumarate extended-release tablets compared to 12.9% (18/140) of placebo patients. In a clinical trial for bipolar mania, somnolence was reported in 50.3% (76/151) of patients on quetiapine fumarate extended-release tablets compared to 11.9% (19/160) of placebo patients. Since quetiapine has the potential to impair judgment, thinking, or motor skills, patients should be cautioned about performing activities requiring mental alertness, such as operating a motor vehicle (including automobiles) or operating hazardous machinery until they are reasonably certain that quetiapine therapy does not affect them adversely. Somnolence may lead to falls.
In short-term adjunctive therapy trials for MDD, somnolence was reported in 40% (252/627) of patients on quetiapine fumarate extended-release tablets respectively compared to 9% (27/309) of placebo patients. Somnolence was dose-related in these trials (37% (117/315) and 43% (135/312) for the 150 mg and 300 mg groups, respectively).
5.17 Body Temperature Regulation
Disruption of the body's ability to reduce core body temperature has been attributed to antipsychotic agents. Appropriate care is advised when prescribing quetiapine fumarate extended-release tablets for patients who will be experiencing conditions which may contribute to an elevation in core body temperature, e.g., exercising strenuously, exposure to extreme heat, receiving concomitant medication with anticholinergic activity, or being subject to dehydration.
5.18 Dysphagia
Esophageal dysmotility and aspiration have been associated with antipsychotic drug use. Aspiration pneumonia is a common cause of morbidity and mortality in elderly patients, in particular those with advanced Alzheimer's dementia. Quetiapine fumarate extended-release tablets and other antipsychotic drugs should be used cautiously in patients at risk for aspiration pneumonia.
5.19 Discontinuation Syndrome
Acute withdrawal symptoms, such as insomnia, nausea, and vomiting have been described after abrupt cessation of atypical antipsychotic drugs, including quetiapine fumarate. In short-term placebo-controlled, monotherapy clinical trials with quetiapine fumarate extended-release tablets that included a discontinuation phase which evaluated discontinuation symptoms, the aggregated incidence of patients experiencing one or more discontinuation symptoms after abrupt cessation was 12.1% (241/1993) for quetiapine fumarate extended-release tablets and 6.7% (71/1065) for placebo. The incidence of the individual adverse reactions (i.e., insomnia, nausea, headache, diarrhea, vomiting, dizziness, and irritability) did not exceed 5.3% in any treatment group and usually resolved after 1-week post-discontinuation. Gradual dose reduction is advised [see Use in Specific Populations (8.1)].
5.20 Anticholinergic (antimuscarinic) Effects
Norquetiapine, an active metabolite of quetiapine, has moderate to strong affinity for several muscarinic receptor subtypes. This contributes to anticholinergic adverse reactions when quetiapine fumarate extended-release tablets is used at therapeutic doses, taken concomitantly with other anticholinergic medications, or taken in overdose. quetiapine fumarate extended-release tablets should be used with caution in patients receiving medications having anticholinergic (antimuscarinic) effects [see Overdosage (10.1) and Clinical Pharmacology (12.1)].
Constipation was a commonly reported adverse event in patients treated with quetiapine and represents a risk factor for intestinal obstruction. Intestinal obstruction has been reported with quetiapine, including fatal reports in patients who were receiving multiple concomitant medications that decrease intestinal motility.
Quetiapine fumarate extended-release tablets should be used with caution in patients with a current diagnosis or prior history of urinary retention, clinically significant prostatic hypertrophy, or constipation, or increased intraocular pressure.
6 ADVERSE REACTIONS
The following adverse reactions are discussed in more detail in other sections of the labeling:
- Increased mortality in elderly patients with dementia-related psychosis [see Warnings and Precautions (5.1)]
- Suicidal thoughts and behaviors in adolescents and young adults [see Warnings and Precautions (5.2)]
- Cerebrovascular adverse reactions, including stroke in elderly patients with dementia-related psychosis [see Warnings and Precautions (5.3)]
- Neuroleptic Malignant Syndrome (NMS) [see Warnings and Precautions (5.4)]
- Metabolic changes (hyperglycemia, dyslipidemia, weight gain) [see Warnings and Precautions (5.5)]
- Tardive dyskinesia [see Warnings and Precautions (5.6)]
- Hypotension [see Warnings and Precautions (5.7)]
- Falls [see Warnings and Precautions (5.8)]
- Increases in blood pressure (children and adolescents) [see Warnings and Precautions (5.9)]
- Leukopenia, neutropenia and agranulocytosis [see Warnings and Precautions (5.10)]
- Cataracts [see Warnings and Precautions (5.11)]
- QT Prolongation [see Warnings and Precautions (5.12)]
- Seizures [see Warnings and Precautions (5.13)]
- Hypothyroidism [see Warnings and Precautions (5.14)]
- Hyperprolactinemia [see Warnings and Precautions (5.15)]
- Potential for cognitive and motor impairment [see Warnings and Precautions (5.16)]
- Body temperature regulation [see Warnings and Precautions (5.17)]
- Dysphagia [see Warnings and Precautions (5.18)]
- Discontinuation Syndrome [see Warnings and Precautions (5.19)]
- Anticholinergic (antimuscarinic) Effects [see Warnings and Precautions, (5.20)]
6.1 Clinical Studies Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
Adults
The information below is derived from a clinical trial database for quetiapine fumarate extended-release tablets consisting of approximately 3400 patients exposed to quetiapine fumarate extended-release tablets for the treatment of Schizophrenia, Bipolar Disorder, and Major Depressive Disorder in placebo-controlled trials. This experience corresponds to approximately 1020.1 patient-years. Adverse reactions were assessed by collecting adverse reactions, results of physical examinations, vital signs, body weights, laboratory analyses, and ECG results.
The stated frequencies of adverse reactions represent the proportion of individuals who experienced, at least once, an adverse reaction of the type listed.
Adverse Reactions Associated with Discontinuation of Treatment in Short-Term, Placebo-Controlled Trials.
Schizophrenia: There were no adverse reactions leading to discontinuation that occurred at an incidence of ≥2% for quetiapine fumarate extended-release tablets in schizophrenia trials.
Bipolar I Disorder, Manic or Mixed Episodes:
There were no adverse reactions leading to discontinuation that occurred at an incidence of ≥2% for quetiapine fumarate extended-release tablets in the bipolar mania trial.
Bipolar Disorder, Depressive Episode: In a single clinical trial in patients with bipolar depression, 14% (19/137) of patients on quetiapine fumarate extended-release tablets discontinued due to an adverse reaction compared to 4% (5/140) on placebo. Somnolence was the only adverse reaction leading to discontinuation that occurred at an incidence of ≥2% in quetiapine fumarate extended-release tablets in the bipolar depression trial.
MDD, Adjunctive Therapy: In adjunctive therapy clinical trials in patients with MDD, 12.1% (76/627) of patients on quetiapine fumarate extended-release tablets discontinued due to adverse reaction compared to 1.9% (6/309) on placebo. Somnolence2 was the only adverse reaction leading to discontinuation that occurred at an incidence of ≥2% in quetiapine fumarate extended-release tablets in MDD trials.
2Somnolence combines adverse reaction terms somnolence and sedation
Commonly Observed Adverse Reactions in Short-Term, Placebo-Controlled Trials:
In short-term placebo-controlled studies for schizophrenia the most commonly observed adverse reactions associated with the use of quetiapine fumarate extended-release tablets (incidence of 5% or greater) and observed at a rate on quetiapine fumarate extended-release tablets at least twice that of placebo were somnolence (25%), dry mouth (12%), dizziness (10%), and dyspepsia (5%).
Adverse Reactions Occurring at an Incidence of 2% or More Among Quetiapine Fumarate Extended-Release Tablets Treated Patients in Short-Term, Placebo-Controlled Trials.
Table 12 enumerates the incidence, rounded to the nearest percent, of adverse reactions that occurred during acute therapy of schizophrenia (up to 6 weeks) in 2% or more in patients treated with quetiapine fumarate extended-release tablets (doses ranging from 300 to 800 mg/day) where the incidence in patients treated with quetiapine fumarate extended-release tablets was greater than the incidence in placebo-treated patients.
|
|
||
|
Preferred Term |
Quetiapine fumarate extended-release tablets (N=951) |
Placebo (N=319) |
|
Somnolence* |
25% |
10% |
|
Dry Mouth |
12% |
1% |
|
Dizziness |
10% |
4% |
|
Extrapyramidal Symptoms† |
8% |
5% |
|
Orthostatic Hypotension |
7% |
5% |
|
Constipation |
6% |
5% |
|
Dyspepsia |
5% |
2% |
|
Heart Rate Increased |
4% |
1% |
|
Tachycardia |
3% |
1% |
|
Fatigue |
3% |
2% |
|
Hypotension |
3% |
1% |
|
Vision Blurred |
2% |
1% |
|
Toothache |
2% |
0% |
|
Increased Appetite |
2% |
0% |
|
Muscle Spasms |
2% |
1% |
|
Tremor |
2% |
1% |
|
Akathisia |
2% |
1% |
|
Anxiety |
2% |
1% |
|
Schizophrenia |
2% |
1% |
|
Restlessness |
2% |
1% |
In a 3-week, placebo-controlled study in bipolar mania the most commonly observed adverse reactions associated with the use of quetiapine fumarate extended-release tablets (incidence of 5% or greater) and observed at a rate on quetiapine fumarate extended-release tablets at least twice that of placebo were somnolence (50%), dry mouth (34%), dizziness (10%), constipation (10%), weight gain (7%), dysarthria (5%), and nasal congestion (5%).
Table 13 enumerates the incidence, rounded to the nearest percent, of adverse reactions that occurred during acute therapy of bipolar mania (up to 3 weeks) in 2% or more of patients treated with quetiapine fumarate extended-release tablets (doses ranging from 400 to 800 mg/day) where the incidence in patients treated with quetiapine fumarate extended-release tablets was greater than the incidence in placebo-treated patients.
|
|
||
|
Preferred Term |
Quetiapine fumarate extended-release tablets (N=151) |
Placebo (N=160) |
|
Somnolence* |
50% |
12% |
|
Dry Mouth |
34% |
7% |
|
Dizziness |
10% |
4% |
|
Constipation |
10% |
3% |
|
Dyspepsia |
7% |
4% |
|
Fatigue |
7% |
4% |
|
Weight Gain |
7% |
1% |
|
Extrapyramidal Symptoms† |
7% |
4% |
|
Nasal Congestion |
5% |
1% |
|
Dysarthria |
5% |
0% |
|
Increased Appetite |
4% |
2% |
|
Back Pain |
3% |
2% |
|
Toothache |
3% |
1% |
|
Heart Rate Increased |
3% |
0% |
|
Abnormal Dreams |
3% |
0% |
|
Orthostatic Hypotension |
3% |
0% |
|
Tachycardia |
2% |
1% |
|
Vision Blurred |
2% |
1% |
|
Sluggishness |
2% |
1% |
|
Lethargy |
2% |
1% |
In the 8-week placebo-controlled bipolar depression study in adults, the most commonly observed adverse reactions associated with the use of quetiapine fumarate extended-release tablets (incidence of 5% or greater) and observed at a rate on quetiapine fumarate extended-release tablets at least twice that of placebo were somnolence (52%), dry mouth (37%), increased appetite (12%), weight gain (7%), dyspepsia (7%), and fatigue (6%).
Table 14 enumerates the incidence, rounded to the nearest percent, of adverse reactions that occurred during acute therapy of bipolar depression (up to 8 weeks) in 2% or more of adult patients treated with quetiapine fumarate extended-release tablets 300 mg/day where the incidence in patients treated with quetiapine fumarate extended-release tablets was greater than the incidence in placebo-treated patients.
|
|
||
|
Preferred Term |
Quetiapine fumarate extended-release tablets (N=137) |
Placebo (N=140) |
|
Somnolence* |
52% |
13% |
|
Dry Mouth |
37% |
7% |
|
Dizziness |
13% |
11% |
|
Increased Appetite |
12% |
6% |
|
Constipation |
8% |
6% |
|
Dyspepsia |
7% |
1% |
|
Weight Gain |
7% |
1% |
|
Fatigue |
6% |
2% |
|
Irritability |
4% |
3% |
|
Viral Gastroenteritis |
4% |
1% |
|
Arthralgia |
4% |
1% |
|
Extrapyramidal Symptoms† |
4% |
1% |
|
Paraesthesia |
3% |
2% |
|
Back Pain |
3% |
1% |
|
Muscle Spasms |
3% |
1% |
|
Toothache |
3% |
0% |
|
Abnormal Dreams |
3% |
0% |
|
Ear Pain |
2% |
1% |
|
Seasonal Allergy |
2% |
1% |
|
Sinusitis |
2% |
1% |
|
Decreased Appetite |
2% |
1% |
|
Myalgia |
2% |
1% |
|
Disturbance in Attention |
2% |
1% |
|
Migraine |
2% |
1% |
|
Restless Legs Syndrome |
2% |
1% |
|
Anxiety |
2% |
1% |
|
Sinus Headache |
2% |
1% |
|
Libido Decreased |
2% |
1% |
|
Pollakiuria |
2% |
1% |
|
Sinus Congestion |
2% |
1% |
|
Hyperhidrosis |
2% |
1% |
|
Orthostatic Hypotension |
2% |
1% |
|
Urinary Tract Infection |
2% |
0% |
|
Heart Rate Increased |
2% |
0% |
|
Neck Pain |
2% |
0% |
|
Dysarthria |
2% |
0% |
|
Akathisia |
2% |
0% |
|
Hypersomnia |
2% |
0% |
|
Mental Impairment |
2% |
0% |
|
Confusional State |
2% |
0% |
|
Disorientation |
2% |
0% |
In the 6-week placebo-controlled fixed dose adjunctive therapy clinical trials, for MDD, the most commonly observed adverse reactions associated with the use of quetiapine fumarate extended-release tablets (incidence of 5% or greater and observed at a rate on quetiapine fumarate extended-release tablets and at least twice that of placebo) were somnolence (150 mg: 37%; 300 mg: 43%), dry mouth (150 mg: 27%; 300 mg: 40%), fatigue (150 mg: 14%; 300 mg: 11%), constipation (300 mg only: 11%), and weight increased (300 mg only: 5%).
Table 15 enumerates the incidence, rounded to the nearest percent, of adverse reactions that occurred during short-term adjunctive therapy of MDD (up to 6 weeks) in 2% or more of patients treated with quetiapine fumarate extended-release tablets (at doses of either 150 mg or 300 mg/day) where the incidence in patients treated with quetiapine fumarate extended-release tablets was greater than the incidence in placebo-treated patients.
|
|
|||
|
Preferred Term |
Quetiapine fumarate extended-release tablets 150 mg (N=315) |
Quetiapine fumarate extended-release tablets 300 mg (N=312) |
Placebo (N=309) |
|
Somnolence* |
37% |
43% |
9% |
|
Dry Mouth |
27% |
40% |
8% |
|
Fatigue |
14% |
11% |
4% |
|
Dizziness |
11% |
12% |
7% |
|
Nausea |
7% |
8% |
7% |
|
Constipation |
6% |
11% |
4% |
|
Irritability |
4% |
2% |
3% |
|
Extrapyramidal Symptoms† |
4% |
6% |
4% |
|
Vomiting |
3% |
1% |
1% |
|
Upper Respiratory Tract Infection |
3% |
2% |
2% |
|
Weight Increased |
3% |
5% |
0% |
|
Increased Appetite |
3% |
5% |
3% |
|
Back Pain |
3% |
3% |
1% |
|
Vertigo |
2% |
2% |
1% |
|
Vision Blurred |
2% |
1% |
1% |
|
Dyspepsia |
2% |
3% |
2% |
|
Influenza |
2% |
1% |
0% |
|
Fall |
2% |
0% |
1% |
|
Muscle Spasms |
2% |
1% |
1% |
|
Lethargy |
2% |
1% |
1% |
|
Akathisia |
2% |
2% |
1% |
|
Abnormal Dreams |
2% |
2% |
1% |
|
Anxiety |
2% |
2% |
1% |
|
Depression |
2% |
1% |
1% |
Adverse Reactions in clinical trials with quetiapine and not listed elsewhere in the label
Pyrexia, nightmares, peripheral edema, dyspnea, palpitations, rhinitis, eosinophilia, hypersensitivity, elevations in gamma-GT levels, and elevations in serum creatine phosphokinase (not associated with NMS), somnambulism (and other related events), hypothermia, decreased platelets, galactorrhea, bradycardia (which may occur at or near initiation of treatment and be associated with hypotension and/ or syncope), and priapism.
Extrapyramidal Symptoms (EPS):
Dystonia
Class Effect: Symptoms of dystonia, prolonged abnormal contractions of muscle groups, may occur in susceptible individuals during the first few days of treatment. Dystonic symptoms include: spasm of the neck muscles, sometimes progressing to tightness of the throat, swallowing difficulty, difficulty breathing, and/or protrusion of the tongue. While these symptoms can occur at low doses, they occur more frequently and with greater severity with high potency and at higher doses of first generation antipsychotic drugs. An elevated risk of acute dystonia is observed in males and younger age groups.
Four methods were used to measure EPS: (1) Simpson-Angus total score (mean change from baseline) which evaluates Parkinsonism and akathisia, (2) Barnes Akathisia Rating Scale (BARS) Global Assessment Score, (3) incidence of spontaneous complaints of EPS (akathisia, akinesia, cogwheel rigidity, extrapyramidal syndrome, hypertonia, hypokinesia, neck rigidity, and tremor), and (4) use of anticholinergic medications to treat EPS.
Adults: In placebo-controlled clinical trials with quetiapine, utilizing doses up to 800 mg per day, the incidence of any adverse reactions related to EPS ranged from 8% to 11% for quetiapine and 4% to 11% for placebo.
In three-arm placebo-controlled clinical trials for the treatment of schizophrenia, utilizing doses between 300 mg and 800 mg of quetiapine fumarate extended-release tablets, the incidence of any adverse reactions related to EPS was 8% for quetiapine fumarate extended-release tablets and 8% for quetiapine fumarate tablets (without evidence of being dose related), and 5% in the placebo group. In these studies, the incidence of the individual adverse reactions (akathisia, extrapyramidal disorder, tremor, dyskinesia, dystonia, restlessness, and muscle rigidity) was generally low and did not exceed 3% for any treatment group.
At the end of treatment, the mean change from baseline in SAS total score and BARS Global Assessment score was similar across the treatment groups. The use of concomitant anticholinergic medications was infrequent and similar across the treatment groups. The incidence of extrapyramidal symptoms was consistent with that seen with the profile of quetiapine fumarate tablets in schizophrenia patients.
In Tables 16-19, dystonic event included nuchal rigidity, hypertonia, dystonia, muscle rigidity, oculogyration; parkinsonism included cogwheel rigidity, tremor, drooling, hypokinesia; akathisia included akathisia, psychomotor agitation; dyskinetic event included tardive dyskinesia, dyskinesia, choreoathetosis; and other extrapyramidal event included restlessness, extrapyramidal disorder, movement disorder.
|
Preferred Term |
Quetiapine fumarate extended-release tablets 300 mg/day (N=91) |
Quetiapine fumarate extended-release tablets 400 mg/day (N=227) |
Quetiapine fumarate extended-release tablets 600 mg/day (N=310) |
Quetiapine fumarate extended-release tablets 800 mg/day (N=323) |
All Doses (N=951) |
Placebo (N=319) |
||||||
|
n |
% |
n |
% |
n |
% |
n |
% |
n |
% |
n |
% |
|
|
Dystonic event |
3 |
3.3 |
0 |
0.0 |
4 |
1.3 |
1 |
0.3 |
8 |
0.8 |
0 |
0.0 |
|
Parkinsonism |
1 |
1.1 |
3 |
1.3 |
11 |
3.6 |
7 |
2.2 |
22 |
2.3 |
4 |
1.3 |
|
Akathisia |
0 |
0.0 |
3 |
1.3 |
7 |
2.3 |
7 |
2.2 |
17 |
1.8 |
4 |
1.3 |
|
Dyskinetic event |
2 |
2.2 |
1 |
0.4 |
1 |
0.3 |
1 |
0.3 |
5 |
0.5 |
2 |
0.6 |
|
Other extrapyramidal event |
3 |
3.3 |
4 |
1.8 |
7 |
2.3 |
12 |
3.7 |
26 |
2.7 |
7 |
2.2 |
In a placebo-controlled clinical trial for the treatment of bipolar mania, utilizing the dose range of 400-800 mg/day of quetiapine fumarate extended-release tablets, the incidence of any adverse reactions related to EPS was 6.6% for quetiapine fumarate extended-release tablets and 3.8% in the placebo group. In this study, the incidence of the individual adverse reactions (akathisia, extrapyramidal disorder, tremor, dystonia, restlessness, and cogwheel rigidity) did not exceed 2.0% for any adverse reaction.
|
|
||||
|
Preferred Term* |
Quetiapine fumarate extended-release tablets (N=151) |
Placebo (N=160) |
||
|
n |
% |
n |
% |
|
|
Dystonic event |
1 |
0.7 |
0 |
0.0 |
|
Parkinsonism |
4 |
2.7 |
3 |
1.9 |
|
Akathisia |
2 |
1.3 |
1 |
0.6 |
|
Other extrapyramidal event |
3 |
2.0 |
2 |
1.3 |
In a placebo-controlled clinical trial for the treatment of bipolar depression utilizing 300 mg of quetiapine fumarate extended-release tablets, the incidence of any adverse reactions related to EPS was 4.4% for quetiapine fumarate extended-release tablets and 0.7% in the placebo group. In this study, the incidence of the individual adverse reactions (akathisia, extrapyramidal disorder, tremor, dystonia, hypertonia) did not exceed 1.5% for any individual adverse reaction.
|
|
||||
|
Preferred Term* |
Quetiapine fumarate extended-release tablets (N=137) |
Placebo (N=140) |
||
|
n |
% |
n |
% |
|
|
Dystonic event |
2 |
1.5 |
0 |
0.0 |
|
Parkinsonism |
1 |
0.7 |
1 |
0.7 |
|
Akathisia |
2 |
1.5 |
0 |
0.0 |
|
Other extrapyramidal event |
1 |
0.7 |
0 |
0.0 |
In two placebo-controlled short-term adjunctive therapy clinical trials for the treatment of MDD utilizing between 150 mg and 300 mg of quetiapine fumarate extended-release tablets, the incidence of any adverse reactions related to EPS was 5.1% for quetiapine fumarate extended-release tablets and 4.2% for the placebo group.
Table 19 shows the percentage of patients experiencing adverse reactions associated with EPS in adjunct clinical trials for MDD by dose:
|
Preferred term |
Quetiapine fumarate extended-release tablets 150 mg/day (N=315) |
Quetiapine fumarate extended-release tablets 300 mg/day (N=312) |
All Doses (N=627) |
Placebo (N=309) |
||||
|
n |
% |
n |
% |
n |
% |
n |
% |
|
|
Dystonic event |
1 |
0.3 |
0 |
0.0 |
1 |
0.2 |
0 |
0.0 |
|
Parkinsonism |
3 |
1.0 |
4 |
1.3 |
7 |
1.1 |
5 |
1.6 |
|
Akathisia |
5 |
1.6 |
8 |
2.6 |
13 |
2.1 |
3 |
1.0 |
|
Dyskinetic event |
0 |
0.0 |
1 |
0.3 |
1 |
0.2 |
0 |
0.0 |
|
Other extrapyramidal event |
5 |
1.6 |
7 |
2.2 |
12 |
1.9 |
5 |
1.6 |
Children and Adolescents
The information below is derived from a clinical trial database for quetiapine fumarate tablets consisting of over 1000 pediatric patients. This database includes 677 adolescents (13-17 years old) exposed to quetiapine fumarate tablets for the treatment of schizophrenia and 393 children and adolescents (10-17 years old) exposed to quetiapine fumarate tablets for the treatment of acute bipolar mania.
Adverse Reactions Associated with Discontinuation of Treatment in Short-Term, Placebo-Controlled Trials:
Schizophrenia: The incidence of discontinuation due to adverse reactions for quetiapine-treated and placebo-treated patients was 8.2% and 2.7%, respectively. The adverse reaction leading to discontinuation in 2% or more of patients on quetiapine and at a greater incidence than placebo was somnolence (2.7% and 0% for placebo).
Bipolar I Mania: The incidence of discontinuation due to adverse reactions for quetiapine-treated and placebo-treated patients was 11.4% and 4.4%, respectively. The adverse reactions leading to discontinuation in 2% or more of patients on quetiapine fumarate tablets and at a greater incidence than placebo were somnolence (4.1% vs. 1.1%) and fatigue (2.1% vs. 0%).
Commonly Observed Adverse Reactions in Short-Term, Placebo-Controlled Trials:
In an acute (8-week) quetiapine fumarate extended-release tablets trial in children and adolescents (10-17 years of age) with bipolar depression, in which efficacy was not established, the most commonly observed adverse reactions associated with the use of quetiapine fumarate extended-release tablets (incidence of 5% or greater and at least twice that for placebo) were: dizziness (7%), diarrhea (5%), fatigue (5%) and nausea (5%).
In therapy for schizophrenia (up to 6 weeks), the most commonly observed adverse reactions associated with the use of quetiapine in adolescents (incidence of 5% or greater and quetiapine incidence at least twice that for placebo) were somnolence (34%), dizziness (12%), dry mouth (7%), tachycardia (7%).
In bipolar mania therapy (up to 3 weeks) the most commonly observed adverse reactions associated with the use of quetiapine in children and adolescents (incidence of 5% or greater and quetiapine incidence at least twice that for placebo) were somnolence (53%), dizziness (18%), fatigue (11%), increased appetite (9%), nausea (8%), vomiting (8%), tachycardia (7%), dry mouth (7%), and weight increased (6%).
Adverse Reactions Occurring at an Incidence of ≥2% among Quetiapine Fumarate Tablets Treated Patients in Short-Term, Placebo-Controlled Trials
Schizophrenia (Adolescents, 13-17 years old)
The following findings were based on a 6-week placebo-controlled trial in which quetiapine was administered in either doses of 400 or 800 mg/day.
Table 20 enumerates the incidence, rounded to the nearest percent, of adverse reactions that occurred during therapy (up to 6 weeks) of schizophrenia in 2% or more of patients treated with quetiapine fumarate tablets (doses of 400 or 800 mg/day) where the incidence in patients treated with quetiapine fumarate tablets was greater than the incidence in placebo-treated patients.
Adverse reactions that were potentially dose-related with higher frequency in the 800 mg group compared to the 400 mg group included dizziness (8% vs. 15%), dry mouth (4% vs. 10%), and tachycardia (6% vs. 11%).
|
|
|||
|
Preferred Term |
Quetiapine fumarate tablets 400 mg (N=73) |
Quetiapine fumarate tablets 800 mg (N=74) |
Placebo (N=75) |
|
Somnolence* |
33% |
35% |
11% |
|
Dizziness |
8% |
15% |
5% |
|
Dry Mouth |
4% |
10% |
1% |
|
Tachycardia† |
6% |
11% |
0% |
|
Irritability |
3% |
5% |
0% |
|
Arthralgia |
1% |
3% |
0% |
|
Asthenia |
1% |
3% |
1% |
|
Back Pain |
1% |
3% |
0% |
|
Dyspnea |
0% |
3% |
0% |
|
Abdominal Pain |
3% |
1% |
0% |
|
Anorexia |
3% |
1% |
0% |
|
Tooth Abscess |
3% |
1% |
0% |
|
Dyskinesia |
3% |
0% |
0% |
|
Epistaxis |
3% |
0% |
1% |
|
Muscle Rigidity |
3% |
0% |
0% |
Bipolar I Mania (Children and Adolescents 10 to 17 years old)
The following findings were based on a 3-week placebo-controlled trial in which quetiapine was administered in either doses of 400 or 600 mg/day.
Table 21 enumerates the incidence, rounded to the nearest percent, of adverse reactions that occurred during therapy (up to 3 weeks) of bipolar mania in 2% or more of patients treated with quetiapine fumarate tablets (doses of 400 or 600 mg/day) where the incidence in patients treated with quetiapine fumarate tablets was greater than the incidence in placebo-treated patients.
Adverse reactions that were potentially dose-related with higher frequency in the 600 mg group compared to the 400 mg group included somnolence (50% vs. 57%), nausea (6% vs. 10%), and tachycardia (6% vs. 9%).
|
|
|||
|
Preferred Term |
Quetiapine fumarate tablets 400 mg (N=95) |
Quetiapine fumarate tablets 600 mg (N=98) |
Placebo (N=90) |
|
Somnolence* |
50% |
57% |
14% |
|
Dizziness |
19% |
17% |
2% |
|
Nausea |
6% |
10% |
4% |
|
Fatigue |
14% |
9% |
4% |
|
Increased Appetite |
10% |
9% |
1% |
|
Tachycardia† |
6% |
9% |
0% |
|
Dry Mouth |
7% |
7% |
0% |
|
Vomiting |
8% |
7% |
3% |
|
Nasal Congestion |
3% |
6% |
2% |
|
Weight Increased |
6% |
6% |
0% |
|
Irritability |
3% |
5% |
1% |
|
Pyrexia |
1% |
4% |
1% |
|
Aggression |
1% |
3% |
0% |
|
Musculoskeletal Stiffness |
1% |
3% |
1% |
|
Accidental Overdose |
0% |
2% |
0% |
|
Acne |
3% |
2% |
0% |
|
Arthralgia |
4% |
2% |
1% |
|
Lethargy |
2% |
2% |
0% |
|
Pallor |
1% |
2% |
0% |
|
Stomach Discomfort |
4% |
2% |
1% |
|
Syncope |
2% |
2% |
0% |
|
Vision Blurred |
3% |
2% |
0% |
|
Constipation |
4% |
2% |
0% |
|
Ear Pain |
2% |
0% |
0% |
|
Paresthesia |
2% |
0% |
0% |
|
Sinus Congestion |
3% |
0% |
0% |
|
Thirst |
2% |
0% |
0% |
Extrapyramidal Symptoms:
Safety and effectiveness of quetiapine fumarate extended-release tablets is supported by studies of quetiapine fumarate tablets in children and adolescent patients 10-17 years of age [see Clinical Studies (14.1 and 14.2)].
In a short-term placebo-controlled quetiapine fumarate extended-release tablets monotherapy trial in children and adolescent patients (10-17 years of age) with bipolar depression (8-week duration), in which efficacy was not established, the aggregated incidence of extrapyramidal symptoms was 1.1% (1/92) for quetiapine fumarate extended-release tablets and 0% (0/100) for placebo.
In a short-term placebo-controlled quetiapine fumarate tablets monotherapy trial in adolescent patients (13-17 years of age) with schizophrenia (6-week duration), the aggregated incidence of extrapyramidal symptoms was 12.9% (19/147) for quetiapine fumarate tablets and 5.3% (4/75) for placebo, though the incidence of the individual adverse reactions (e.g., akathisia, tremor, extrapyramidal disorder, hypokinesia, restlessness, psychomotor hyperactivity, muscle rigidity, dyskinesia) did not exceed 4.1% in any treatment group. In a short-term placebo-controlled quetiapine fumarate tablets monotherapy trial in children and adolescent patients (10-17 years of age) with bipolar mania (3-week duration), the aggregated incidence of extrapyramidal symptoms was 3.6% (7/193) for quetiapine fumarate tablets and 1.1% (1/90) for placebo.
In Tables 22 and 23, dystonic events included nuchal rigidity, hypertonia, dystonia, and muscle rigidity; parkinsonism included cogwheel rigidity and tremor; akathisia included akathisia only; dyskinetic event included tardive dyskinesia, dyskinesia and choreoathetosis; and other extrapyramidal event included restlessness and extrapyramidal disorder.
Table 22 below presents a listing of patients with adverse reactions associated with EPS in the short-term placebo-controlled quetiapine fumarate tablets monotherapy trial in adolescent patients with schizophrenia (6-week duration).
|
Preferred Term |
Quetiapine fumarate tablets 400 mg/day (N=73) |
Quetiapine fumarate tablets 800 mg/day (N=74) |
All Quetiapine fumarate tablets (N=147) |
Placebo (N=75) |
||||
|
n |
% |
n |
% |
n |
% |
n |
% |
|
|
Dystonic Event |
2 |
2.7 |
0 |
0.0 |
2 |
1.4 |
0 |
0.0 |
|
Parkinsonism |
4 |
5.5 |
4 |
5.4 |
8 |
5.4 |
2 |
2.7 |
|
Akathisia |
3 |
4.1 |
4 |
5.4 |
7 |
4.8 |
3 |
4.0 |
|
Dyskinetic Event |
2 |
2.7 |
0 |
0.0 |
2 |
1.4 |
0 |
0.0 |
|
Other Extrapyramidal Event |
2 |
2.7 |
2 |
2.7 |
4 |
2.7 |
0 |
0.0 |
Table 23 below presents a listing of patients with adverse reactions associated with EPS in a short-term placebo-controlled monotherapy trial in children and adolescent patients with bipolar mania (3-week duration).
|
|
||||||||
|
Preferred Term* |
Quetiapine fumarate tablets 400 mg/day (N=95) |
Quetiapine fumarate tablets 600 mg/day (N=98) |
All Quetiapine fumarate tablets (N=193) |
Placebo (N=90) |
||||
|
n |
% |
n |
% |
n |
% |
n |
% |
|
|
Parkinsonism |
2 |
2.1 |
1 |
1.0 |
3 |
1.6 |
1 |
1.1 |
|
Akathisia |
1 |
1.0 |
1 |
1.0 |
2 |
1.0 |
0 |
0.0 |
|
Other Extrapyramidal Event |
1 |
1.1 |
1 |
1.0 |
2 |
1.0 |
0 |
0.0 |
Laboratory, ECG and vital sign changes observed in clinical studies
Laboratory Changes:
Neutrophil Counts
Adults: In three-arm quetiapine fumarate extended-release tablets placebo-controlled monotherapy clinical trials, among patients with a baseline neutrophil count ≥1.5 x 109/L, the incidence of at least one occurrence of neutrophil count <1.5 x 109/L was 1.5% in patients treated with quetiapine fumarate extended-release tablets and 1.5% for quetiapine fumarate tablets, compared to 0.8% in placebo-treated patients.
In placebo-controlled monotherapy clinical trials involving 3368 patients on quetiapine fumarate and 1515 on placebo, the incidence of at least one occurrence of neutrophil count <1.0 x 109/L among patients with a normal baseline neutrophil count and at least one available follow up laboratory measurement was 0.3% (10/2967) in patients treated with quetiapine, compared to 0.1% (2/1349) in patients treated with placebo [see Warnings and Precautions (5.10)].
Transaminase Elevations
Adults: Asymptomatic, transient and reversible elevations in serum transaminases (primarily ALT) have been reported. The proportions of adult patients with transaminase elevations of >3 times the upper limits of the normal reference range in a pool of placebo-controlled trials ranged between 1% and 2% for quetiapine fumarate extended-release tablets compared to 2% for placebo. In schizophrenia trials in adults, the proportions of patients with transaminase elevations of >3 times the upper limits of the normal reference range in a pool of 3- to 6-week placebo-controlled trials were approximately 6% (29/483) for quetiapine fumarate tablets compared to 1% (3/194) for placebo. These hepatic enzyme elevations usually occurred within the first 3 weeks of drug treatment and promptly returned to pre-study levels with ongoing treatment with quetiapine.
Decreased Hemoglobin
Adults: In short-term placebo-controlled trials, decreases in hemoglobin to ≤13 g/dL males, ≤12 g/dL females on at least one occasion occurred in 8.3% (594/7155) of quetiapine-treated patients compared to 6.2% (219/3536) of patients treated with placebo. In a database of controlled and uncontrolled clinical trials, decreases in hemoglobin to ≤13 g/dL males, ≤12 g/dL females on at least one occasion occurred in 11% (2277/20729) of quetiapine-treated patients.
Interference with Urine Drug Screens
There have been literature reports suggesting false positive results in urine enzyme immunoassays for methadone and tricyclic antidepressants in patients who have taken quetiapine. Caution should be exercised in the interpretation of positive urine drug screen results for these drugs, and confirmation by alternative analytical technique (e.g., chromatographic methods) should be considered.
ECG Changes:
Adults: 2.5% of quetiapine fumarate extended-release tablets patients, and 2.3% of placebo patients, had tachycardia (>120 bpm) at any time during the trials. Quetiapine fumarate extended-release tablets was associated with a mean increase in heart rate, assessed by ECG, of 6.3 beats per minute compared to a mean increase of 0.4 beats per minute for placebo. This is consistent with the rates for quetiapine fumarate. The incidence of adverse reactions of tachycardia was 1.9% for quetiapine fumarate extended-release tablets compared to 0.5% for placebo. Quetiapine fumarate tablets use was associated with a mean increase in heart rate, assessed by ECG, of 7 beats per minute compared to a mean increase of 1 beat per minute among placebo patients. The slight tendency for tachycardia may be related to quetiapine’s potential for inducing orthostatic changes [see Warnings and Precautions (5.7)].
Children and Adolescents: Safety and effectiveness of quetiapine fumarate extended-release tablets is supported by studies of quetiapine fumarate tablets in children and adolescent patients 10-17 years of age [see Clinical Studies (14.1 and 14.2)].
In an acute (8-week) quetiapine fumarate extended-release tablets trial in children and adolescents (10-17 years of age) with bipolar depression, in which efficacy was not established, increases in heart rate (>110 bpm 10-12 years and 13-17 years) occurred in 0% of patients receiving quetiapine fumarate extended-release tablets and 1.2% of patients receiving placebo. Mean increases in heart rate were 3.4 bpm for quetiapine fumarate extended-release tablets, compared to 0.3 bpm in the placebo group [see Warnings and Precautions (5.7)].
In the acute (6-week) quetiapine fumarate tablets schizophrenia trial in adolescents (13-17 years of age), increases in heart rate (>110 bpm) occurred in 5.2% of patients receiving quetiapine fumarate tablets 400 mg and 8.5% of patients receiving quetiapine fumarate tablets 800 mg compared to 0% of patients receiving placebo. Mean increases in heart rate were 3.8 bpm and 11.2 bpm for quetiapine fumarate tablets 400 mg and 800 mg groups, respectively, compared to a decrease of 3.3 bpm in the placebo group [see Warnings and Precautions (5.7)].
In the acute (3-week) quetiapine fumarate tablets bipolar mania trial in children and adolescents (10-17 years of age), increases in heart rate (>110 bpm) occurred in 1.1% of patients receiving quetiapine fumarate tablets 400 mg and 4.7% of patients receiving quetiapine fumarate tablets 600 mg compared to 0% of patients receiving placebo. Mean increases in heart rate were 12.8 bpm and 13.4 bpm for quetiapine fumarate tablets 400 mg and 600 mg groups, respectively, compared to a decrease of 1.7 bpm in the placebo group [see Warnings and Precautions (5.7)].
6.2 Postmarketing Experience
The following adverse reactions were identified during post approval use of quetiapine fumarate tablets. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Adverse reactions reported since market introduction which were temporally related to quetiapine therapy include anaphylactic reaction, cardiomyopathy, drug reaction with eosinophilia and systemic symptoms (DRESS), hyponatremia, myocarditis, nocturnal enuresis, pancreatitis, retrograde amnesia, rhabdomyolysis, syndrome of inappropriate antidiuretic hormone secretion (SIADH), Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), decreased platelet count, serious liver reactions (including hepatitis, liver necrosis, and hepatic failure), agranulocytosis, intestinal obstruction, ileus, colon ischemia, sleep apnea, and urinary retention.
7 DRUG INTERACTIONS
7.1 Effect of Other Drugs on Quetiapine
The risks of using quetiapine fumarate extended-release tablets in combination with other drugs have not been extensively evaluated in systematic studies. Given the primary CNS effects of quetiapine fumarate extended-release tablets, caution should be used when it is taken in combination with other centrally acting drugs. Quetiapine potentiated the cognitive and motor effects of alcohol in a clinical trial in subjects with selected psychotic disorders, and alcoholic beverages should be limited while taking quetiapine.
Quetiapine exposure is increased by the prototype CYP3A4 inhibitors (e.g., ketoconazole, itraconazole, indinavir, ritonavir, nefazodone, etc.) and decreased by the prototype of CYP3A4 inducers (e.g., phenytoin, carbamazepine, rifampin, avasimibe, St. John’s wort etc.). Dose adjustment of quetiapine will be necessary if it is co-administered with potent CYP3A4 inducers or inhibitors.
CYP3A4 inhibitors:
Coadministration of ketoconazole, a potent inhibitor of cytochrome CYP3A4, resulted in significant increase in quetiapine exposure. The dose should be reduced to one sixth of the original dose in patients coadministered with a strong CYP3A4 inhibitor [see Dosage and Administration (2.5) and Clinical Pharmacology (12.3)].
CYP3A4 inducers:
Coadministration of quetiapine and phenytoin, a CYP3A4 inducer increased the mean oral clearance of quetiapine by 5-fold. Increased doses of quetiapine fumarate extended-release tablets up to 5 fold may be required to maintain control of symptoms of schizophrenia in patients receiving quetiapine and phenytoin, or other known potent CYP3A4 inducers [see Dosage and Administration (2.6) and Clinical Pharmacology (12.3)]. When the CYP3A4 inducer is discontinued, the dose of quetiapine fumarate extended-release tablets should be reduced to the original level within 7-14 days [see Dosage and Administration (2.6)].
The potential effects of several concomitant medications on quetiapine pharmacokinetics were studied.
7.2 Effect of Quetiapine on Other Drugs
Because of its potential for inducing hypotension, quetiapine fumarate extended-release tablets may enhance the effects of certain antihypertensive agents.
Quetiapine fumarate extended-release tablets may antagonize the effects of levodopa and dopamine agonists.
There are no clinically relevant pharmacokinetic interactions of quetiapine fumarate tablets on other drugs based on the CYP pathway. Quetiapine fumarate tablets and its metabolites are non-inhibitors of major metabolizing CYP’s (1A2, 2C9, 2C19, 2D6, and 3A4).
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Exposure Registry
There is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to atypical antipsychotics, including quetiapine, during pregnancy. Healthcare providers are encouraged to register patients by contacting the National Pregnancy Registry for Atypical Antipsychotics at 1-866-961-2388 or online at http://womensmentalhealth.org/clinical-and-research-programs/pregnancyregistry/
Risk Summary
Neonates exposed to antipsychotic drugs, including quetiapine, during the third trimester are at risk for extrapyramidal and/or withdrawal symptoms following delivery (see Clinical Considerations). Overall available data from published epidemiologic studies of pregnant women exposed to quetiapine have not established a drug-associated risk of major birth defects, miscarriage, or adverse maternal or fetal outcomes (see Data). There are risks to the mother associated with untreated schizophrenia, bipolar I, or major depressive disorder, and with exposure to antipsychotics, including, quetiapine fumarate extended-release tablet during pregnancy (see Clinical Considerations). In animal studies, embryo-fetal toxicity occurred including delays in skeletal ossification at approximately 1 and 2 times the maximum recommended human dose (MRHD) of 800 mg/day in both rats and rabbits, and an increased incidence of carpal/tarsal flexure (minor soft tissue anomaly) in rabbit fetuses at approximately 2 times the MRHD. In addition, fetal weights were decreased in both species. Maternal toxicity (observed as decreased body weights and/or death) occurred at 2 times the MRHD in rats and approximately 1-2 times the MRHD in rabbits.
The estimated background risk of major birth defects and miscarriage for the indicated populations is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2 to 4% and 15 to 20%, respectively.
Clinical Considerations
Disease-associated maternal and/or fetal risk
There is a risk to the mother from untreated schizophrenia, or bipolar I disorder, including increased risk of relapse, hospitalization, and suicide. Schizophrenia and bipolar I disorder are associated with increased adverse perinatal outcomes, including preterm birth. It is not known if this is a direct result of the illness or other comorbid factors.
A prospective, longitudinal study followed 201 pregnant women with a history of major depressive disorder who were euthymic and taking antidepressants at the beginning of pregnancy. The women who discontinued antidepressants during pregnancy were more likely to experience a relapse of major depression than women who continued antidepressants. Consider the risk of untreated depression when discontinuing or changing treatment with antidepressant medication during pregnancy and postpartum.
Fetal/neonatal adverse reactions
Extrapyramidal and/or withdrawal symptoms, including agitation, hypertonia, hypotonia, tremor, somnolence, respiratory distress, and feeding disorder have been reported in neonates who were exposed to antipsychotic drugs, including quetiapine, during the third trimester of pregnancy. These symptoms varied in severity. Monitor neonates for extrapyramidal and/or withdrawal symptoms and manage symptoms appropriately. Some neonates recovered within hours or days without specific treatment; others required prolonged hospitalization.
Data
Human Data
Published data from observational studies, birth registries, and case reports on the use of atypical antipsychotics during pregnancy do not report a clear association with antipsychotics and major birth defects. A retrospective cohort study from a Medicaid database of 9258 women exposed to antipsychotics during pregnancy did not indicate an overall increased risk of major birth defects.
Animal Data
When pregnant rats and rabbits were exposed to quetiapine during organogenesis, there was no teratogenic effect in fetuses. Doses were 25, 50 and 200 mg/kg in rats and 25, 50 and 100 mg/kg in rabbits which are approximately 0.3, 0.6 and 2-times (rats) and 0.6, 1 and 2-times (rabbits) the MRHD, for schizophrenia of 800 mg/day based on mg/m2 body surface area. However, there was evidence of embryo-fetal toxicity, including delays in skeletal ossification at approximately 1 and 2 times the MRHD of 800 mg/day in both rats and rabbits and an increased incidence of carpal/tarsal flexure (minor soft tissue anomaly) in rabbit fetuses at approximately 2 times the MRHD. In addition, fetal weights were decreased in both species. Maternal toxicity (observed as decreased body weights and/or death) occurred at 2 times the MRHD in rats and at approximately 1-2 times the MRHD (all doses tested) in rabbits.
In a peri/postnatal reproductive study in rats, no drug-related effects were observed when pregnant dams were treated with quetiapine at doses 0.01, 0.1, and 0.2 times the MRHD of 800 mg/day based on mg/m2 body surface area. However, in a preliminary peri/postnatal study, there were increases in fetal and pup death, and decreases in mean litter weight at 3 times the MRHD.
8.2 Lactation
Risk Summary
Limited data from published literature report the presence of quetiapine in human breast milk at relative infant dose of <1% of the maternal weight-adjusted dosage. There are no consistent adverse events that have been reported in infants exposed to quetiapine through breast milk. There is no information on the effects of quetiapine on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for quetiapine and any potential adverse effects on the breastfed child from quetiapine or from the mother’s underlying condition.
8.3 Females and Males of Reproductive Potential
Infertility
Females
Based on the pharmacologic action of quetiapine (D2 antagonism), treatment with quetiapine may result in an increase in serum prolactin levels, which may lead to a reversible reduction in fertility in females of reproductive potential [see Warnings and Precautions (5.15)].
8.4 Pediatric Use
Safety and effectiveness of quetiapine fumarate extended-release tablets is supported by studies of quetiapine fumarate tablets for schizophrenia in adolescent patients 13-17 years of age and in bipolar mania in children and adolescent patients 10-17 years of age [see Clinical Studies (14.1 and 14.2)].
In general, the adverse reactions observed in children and adolescents during the clinical trials with quetiapine fumarate tablets were similar to those in the adult population with few exceptions. Increases in systolic and diastolic blood pressure occurred in children and adolescents and did not occur in adults. Orthostatic hypotension occurred more frequently in adults (4-7%) compared to children and adolescents (<1%) [see Warnings and Precautions (5.7) and Adverse Reactions (6.1)].
Bipolar Depression
The effectiveness of quetiapine fumarate extended-release tablets for the treatment of bipolar depression in patients under the age of 18 years has not been established. One 8-week trial was conducted to evaluate the safety and efficacy of quetiapine fumarate extended-release tablets in the treatment of bipolar depression in pediatric patients 10-17 years of age. The primary objective of the study was to evaluate whether quetiapine fumarate extended-release tablets at a dose of 150 to 300 mg/day demonstrated superior efficacy (as measured by change in CDRS-R total score from baseline to end of 8 weeks) compared to placebo in children and adolescents 10-17 years of age with bipolar depression. A total of 193 patients with bipolar depression were randomized to placebo or quetiapine fumarate extended-release tablets. The primary results of this study did not show a difference between quetiapine fumarate extended-release tablets and placebo in decreasing depression symptoms in children and adolescents with bipolar disorder. In this study, patients treated with quetiapine fumarate extended-release tablets exhibited metabolic changes, weight gain, increases in blood pressure and increases in heart rate [see Warnings and Precautions (5.5, 5.9) and Adverse Reactions (6.1)].
Some differences in the pharmacokinetics of quetiapine were noted between children/adolescents (10-17 years of age) and adults. When adjusted for weight, the AUC and Cmax of quetiapine were 41% and 39% lower, respectively, in children and adolescents compared to adults. The pharmacokinetics of the active metabolite, norquetiapine, were similar between children/adolescents and adults after adjusting for weight [see Clinical Pharmacology (12.3)].
Schizophrenia
The efficacy and safety of quetiapine fumarate extended-release tablets in the treatment of schizophrenia in adolescents aged 13-17 years is supported by one 6-week, double-blind, placebo-controlled trial with quetiapine fumarate tablets [see Indications and Usage (1.1), Dosage and Administration (2.2), Adverse Reactions (6.1), and Clinical Studies (14.1)].
Safety and effectiveness of quetiapine fumarate extended-release tablets in pediatric patients less than 13 years of age with schizophrenia have not been established.
The safety and effectiveness of quetiapine fumarate extended-release tablets in the maintenance treatment of schizophrenia has not been established in patients less than 18 years of age.
Bipolar Mania
The efficacy and safety of quetiapine fumarate extended-release tablets in the treatment of bipolar mania in children and adolescents ages 10-17 years is supported by one 3-week, double-blind, placebo-controlled trial with quetiapine fumarate tablets [see Indications and Usage (1.2), Dosage and Administration (2.2), Adverse Reactions (6.1), and Clinical Studies (14.2)].
Safety and effectiveness of quetiapine fumarate extended-release tablets in pediatric patients less than 10 years of age with bipolar mania have not been established.
The safety and effectiveness of quetiapine fumarate extended-release tablets in the maintenance treatment of bipolar disorder has not been established in patients less than 18 years of age.
8.5 Geriatric Use
Sixty-eight patients in clinical studies with quetiapine fumarate extended-release tablets were 65 years of age or over. In general, there was no indication of any different tolerability of quetiapine fumarate extended-release tablets in the elderly compared to younger adults. Nevertheless, the presence of factors that might decrease pharmacokinetic clearance, increase the pharmacodynamic response to quetiapine fumarate extended-release tablets, or cause poorer tolerance or orthostasis, should lead to consideration of a lower starting dose, slower titration, and careful monitoring during the initial dosing period in the elderly. The mean plasma clearance of quetiapine was reduced by 30% to 50% in elderly patients when compared to younger patients [see Dosage and Administration (2.3) and Clinical Pharmacology (12.3)].
8.6 Renal Impairment
Clinical experience with quetiapine fumarate extended-release tablets in patients with renal impairment is limited [see Clinical Pharmacology (12.3)].
8.7 Hepatic Impairment
Since quetiapine is extensively metabolized by the liver, higher plasma levels are expected in patients with hepatic impairment. In this population, a low starting dose of 50 mg/day is recommended and the dose may be increased in increments of 50 mg/day [see Dosage and Administration (2.4) and Clinical Pharmacology (12.3)].
9 DRUG ABUSE AND DEPENDENCE
9.1 Controlled Substance
Quetiapine fumarate extended-release tablets are not a controlled substance.
9.2 Abuse
Quetiapine fumarate extended-release tablets have not been systematically studied in animals or humans for its potential for abuse, tolerance, or physical dependence. While the clinical trials did not reveal any tendency for any drug-seeking behavior, these observations were not systematic and it is not possible to predict on the basis of this limited experience the extent to which a CNS-active drug will be misused, diverted, and/or abused once marketed. Consequently, patients should be evaluated carefully for a history of drug abuse, and such patients should be observed closely for signs of misuse or abuse of quetiapine fumarate extended-release tablets (e.g., development of tolerance, increases in dose, drug-seeking behavior).
10 OVERDOSAGE
10.1 Human Experience
In clinical trials, survival has been reported in acute overdoses of up to 30 grams of quetiapine. Most patients who overdosed experienced no adverse reactions or recovered fully from the reported events. Death has been reported in a clinical trial following an overdose of 13.6 grams of quetiapine alone. In general, reported signs and symptoms were those resulting from an exaggeration of the drug’s known pharmacological effects, i.e., drowsiness, sedation, tachycardia, hypotension, and anticholinergic toxicity including coma and delirium. Patients with pre-existing severe cardiovascular disease may be at an increased risk of the effects of overdose [see Warnings and Precautions (5.12)]. One case, involving an estimated overdose of 9600 mg, was associated with hypokalemia and first degree heart block. In post-marketing experience, there were cases reported of QT prolongation with overdose.
10.2 Management of Overdosage
Establish and maintain an airway and ensure adequate oxygenation and ventilation. Cardiovascular monitoring should commence immediately and should include continuous electrocardiographic monitoring to detect possible arrhythmias.
Appropriate supportive measures are the mainstay of management. For the most up-to-date information on the management of quetiapine fumarate extended-release tablets overdosage, contact a certified Regional Poison Control Center (1-800-222-1222).
11 DESCRIPTION
Quetiapine fumarate extended-release tablets are an atypical antipsychotic belonging to a chemical class, the dibenzothiazepine derivatives. The chemical designation is 2-[2-(4-dibenzo [b,f ] [1,4] thiazepin-11-yl-1-piperazinyl)ethoxy]-ethanol fumarate (2:1) (salt). It is present in tablets as the fumarate salt. All doses and tablet strengths are expressed as milligrams of base, not as fumarate salt. Its molecular formula is C42H50N6O4S2C4H4O4 and it has a molecular weight of 883.11 (fumarate salt). The structural formula is:
Quetiapine fumarate is a white to off-white crystalline powder which is moderately soluble in water.
Quetiapine fumarate extended-release tablets are supplied for oral administration as 50 mg (peach), 150 mg (white), 200 mg (yellow), 300 mg (pale yellow), and 400 mg (white). All tablets are capsule shaped and film coated.
Inactive ingredients for quetiapine fumarate extended-release tablets are lactose monohydrate, microcrystalline cellulose, sodium citrate, hypromellose, and magnesium stearate. The film coating for all quetiapine fumarate extended-release tablets contain hypromellose, polyethylene glycol 400 and titanium dioxide. In addition, yellow iron oxide (50, 200 and 300 mg tablets) and red iron oxide (50 mg tablets) are included in the film coating of specific strengths.
Each 50 mg tablet contains 58 mg of quetiapine fumarate equivalent to 50 mg quetiapine. Each 150 mg tablet contains 173 mg of quetiapine fumarate equivalent to 150 mg quetiapine. Each 200 mg tablet contains 230 mg of quetiapine fumarate equivalent to 200 mg quetiapine. Each 300 mg tablet contains 345 mg of quetiapine fumarate equivalent to 300 mg quetiapine. Each 400 mg tablet contains 461 mg of quetiapine fumarate equivalent to 400 mg quetiapine.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
The mechanism of action of quetiapine in the listed indications is unclear. However, the efficacy of quetiapine in these indications could be mediated through a combination of dopamine type 2 (D2) and serotonin type 2A (5HT2A) antagonism. The active metabolite, N-desalkyl quetiapine (norquetiapine), has similar activity at D2, but greater activity at 5HT2A receptors, than the parent drug (quetiapine).
12.2 Pharmacodynamics
Quetiapine and its metabolite norquetiapine have affinity for multiple neurotransmitter receptors with norquetiapine binding with higher affinity than quetiapine in general. The Ki values for quetiapine and norquetiapine at the dopamine D1 are 428/99.8 nM, at D2 626/489nM, at serotonin 5HT1A 1040/191 nM at 5HT2A 38/2.9 nM, at histamine H1 4.4/1.1 nM, at muscarinic M1 1086/38.3 nM, and at adrenergic α1b 14.6/46.4 nM and, at α2 receptors 617/1290 nM, respectively. Quetiapine and norquetiapine lack appreciable affinity to the benzodiazepine receptors.
Effect on QT Interval
In clinical trials quetiapine was not associated with a persistent increase in QT intervals. However, the QT effect was not systematically evaluated in a thorough QT study. In post marketing experience, there were cases reported of QT prolongation in patients who overdosed on quetiapine [see Overdosage (10.1)], in patients with concomitant illness, and in patients taking medicines known to cause electrolyte imbalance or increase QT interval.
12.3 Pharmacokinetics
Adults
Following multiple dosing of quetiapine up to a total daily dose of 800 mg, administered in divided doses, the plasma concentration of quetiapine and norquetiapine, the major active metabolite of quetiapine, were proportional to the total daily dose. Accumulation is predictable upon multiple dosing. Steady-state mean Cmax and AUC of norquetiapine are about 21-27% and 46-56%, respectively, of that observed for quetiapine. Elimination of quetiapine is mainly via hepatic metabolism. The mean-terminal half-life is approximately 7 hours for quetiapine and approximately 12 hours for norquetiapine within the clinical dose range. Steady-state concentrations are expected to be achieved within two days of dosing. Quetiapine fumarate extended-release tablets is unlikely to interfere with the metabolism of drugs metabolized by cytochrome P450 enzymes.
Children and Adolescents
At steady state, the pharmacokinetics of the parent compound, in children and adolescents (10-17 years of age), were similar to adults. However, when adjusted for dose and weight, AUC and Cmax of the parent compound were 41% and 39% lower, respectively, in children and adolescents than in adults. For the active metabolite, norquetiapine, AUC and Cmax were 45% and 31% higher, respectively, in children and adolescents than in adults. When adjusted for dose and weight, the pharmacokinetics of the metabolite, norquetiapine, was similar between children and adolescents and adults [see Use in Specific Populations (8.4)].
Absorption
Quetiapine fumarate reaches peak plasma concentrations approximately 6 hours following administration. Quetiapine fumarate extended-release tablets dosed once daily at steady state has comparable bioavailability to an equivalent total daily dose of quetiapine fumarate administered in divided doses, twice daily. A high-fat meal (approximately 800 to 1000 calories) was found to produce statistically significant increases in the quetiapine fumarate extended-release tablets Cmax and AUC of 44% to 52% and 20% to 22%, respectively, for the 50 mg and 300 mg tablets. In comparison, a light meal (approximately 300 calories) had no significant effect on the Cmax or AUC of quetiapine. It is recommended that quetiapine fumarate extended-release tablets be taken without food or with a light meal [see Dosage and Administration (2.1)].
Distribution
Quetiapine is widely distributed throughout the body with an apparent volume of distribution of 10±4 L/kg. It is 83% bound to plasma proteins at therapeutic concentrations. In vitro, quetiapine did not affect the binding of warfarin or diazepam to human serum albumin. In turn, neither warfarin nor diazepam altered the binding of quetiapine.
Metabolism and Elimination
Following a single oral dose of 14C-quetiapine, less than 1% of the administered dose was excreted as unchanged drug, indicating that quetiapine is highly metabolized. Approximately 73% and 20% of the dose was recovered in the urine and feces, respectively. The average dose fraction of free quetiapine and its major active metabolite is <5% excreted in the urine.
Quetiapine is extensively metabolized by the liver. The major metabolic pathways are sulfoxidation to the sulfoxide metabolite and oxidation to the parent acid metabolite; both metabolites are pharmacologically inactive. In vitro studies using human liver microsomes revealed that the cytochrome P450 3A4 isoenzyme is involved in the metabolism of quetiapine to its major, but inactive, sulfoxide metabolite and in the metabolism of its active metabolite norquetiapine.
Age
Oral clearance of quetiapine was reduced by 40% in elderly patients (≥65 years, n=9) compared to young patients (n=12), and dosing adjustment may be necessary [see Dosage and Administration (2.3)].
Gender
There is no gender effect on the pharmacokinetics of quetiapine.
Race
There is no race effect on the pharmacokinetics of quetiapine.
Smoking
Smoking has no effect on the oral clearance of quetiapine.
Renal Insufficiency
Patients with severe renal impairment (CLcr=10-30 mL/min/1.73m2, n=8) had a 25% lower mean oral clearance than normal subjects (CLcr>80 mL/min/1.73m2, n=8), but plasma quetiapine concentrations in the subjects with renal insufficiency were within the range of concentrations seen in normal subjects receiving the same dose. Dosage adjustment is therefore not needed in these patients [see Use in Specific Populations (8.6)].
Hepatic Insufficiency
Hepatically impaired patients (n=8) had a 30% lower mean oral clearance of quetiapine than normal subjects. In 2 of the 8 hepatically impaired patients, AUC and Cmax were 3 times higher than those observed typically in healthy subjects. Since quetiapine is extensively metabolized by the liver, higher plasma levels are expected in the hepatically impaired population, and dosage adjustment may be needed [see Dosage and Administration (2.4) and Use in Specific Populations (8.7)].
Drug-Drug Interaction Studies
The in vivo assessments of effect of other drugs on the pharmacokinetics of quetiapine are summarized in Table 24 [see Dosage and Administration (2.5, 2.6) and Drug Interactions (7.1)].
|
Coadministered Drug |
Dose Schedules |
Effect on Quetiapine Pharmacokinetics |
|
|
Coadministered Drug |
Quetiapine |
||
|
Phenytoin |
100 mg three times daily |
250 mg three times daily |
5-fold Increase in oral clearance |
|
Divalproex |
500 mg twice daily |
150 mg twice daily |
17% increase mean max plasma concentration at steady state. No effect on absorption or mean oral clearance |
|
Thioridazine |
200 mg twice daily |
300 mg twice daily |
65% increase in oral clearance |
|
Cimetidine |
400 mg three times daily for 4 days |
150 mg three times daily |
20% decrease in mean oral clearance |
|
Ketoconazole (potent CYP 3A4 inhibitor) |
200 mg once daily for 4 days |
25 mg single dose |
84% decrease in oral clearance resulting in a 6.2-fold increase in AUC of quetiapine |
|
Fluoxetine |
60 mg once daily |
300 mg twice daily |
No change in steady state PK |
|
Imipramine |
75 mg twice daily |
300 mg twice daily |
No change in steady state PK |
|
Haloperidol |
7.5 mg twice daily |
300 mg twice daily |
No change in steady state PK |
|
Risperidone |
3 mg twice daily |
300 mg twice daily |
No change in steady state PK |
In vitro enzyme inhibition data suggest that quetiapine and 9 of its metabolites would have little inhibitory effect on in vivo metabolism mediated by cytochromes CYP 1A2, 2C9, 2C19, 2D6, and 3A4. Quetiapine at doses of 750 mg/day did not affect the single dose pharmacokinetics of antipyrine, lithium or lorazepam (Table 25) [see Drug Interactions (7.2)].
|
Coadministered Drug |
Dose Schedules |
Effect on Other Drugs Pharmacokinetics |
|
|
Coadministered Drug |
Quetiapine |
||
|
Lorazepam |
2 mg, single dose |
250 mg three times daily |
Oral clearance of lorazepam reduced by 20% |
|
Divalproex |
500 mg twice daily |
150 mg twice daily |
Cmax and AUC of free valproic acid at steady-state was decreased by 10-12% |
|
Lithium |
Up to 2400 mg/day given in twice daily doses |
250 mg three times daily |
No effect on steady-state pharmacokinetics of lithium |
|
Antipyrine |
1 g, single dose |
250 mg three times daily |
No effect on clearance of antipyrine or urinary recovery of its metabolites |
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
Carcinogenicity studies were conducted in C57BL mice and Wistar rats. Quetiapine was administered in the diet to mice at doses of 20, 75, 250, and 750 mg/kg and to rats by gavage at doses of 25, 75, and 250 mg/kg for two years. These doses are equivalent to 0.1, 0.5, 1.5, and 4.5 times the MRHD of 800 mg/day based on mg/m2 body surface area (mice) or 0.3, 1, and 3 times the MRHD based on mg/m2 body surface area (rats). There were statistically significant increases in thyroid gland follicular adenomas in male mice at doses 1.5 and 4.5 times the MRHD based on mg/m2 body surface area and in male rats at a dose of 3 times the MRHD on mg/m2 body surface area. Mammary gland adenocarcinomas were statistically significantly increased in female rats at all doses tested (0.3, 1, and 3 times the MRHD based on mg/m2 body surface area).
Thyroid follicular cell adenomas may have resulted from chronic stimulation of the thyroid gland by thyroid stimulating hormone (TSH) resulting from enhanced metabolism and clearance of thyroxine by rodent liver. Changes in TSH, thyroxine, and thyroxine clearance consistent with this mechanism were observed in subchronic toxicity studies in rat and mouse and in a 1-year toxicity study in rat; however, the results of these studies were not definitive. The relevance of the increases in thyroid follicular cell adenomas to human risk, through whatever mechanism, is unknown.
Antipsychotic drugs have been shown to chronically elevate prolactin levels in rodents. Serum measurements in a 1-year toxicity study showed that quetiapine increased median serum prolactin levels a maximum of 32- and 13-fold in male and female rats, respectively. Increases in mammary neoplasms have been found in rodents after chronic administration of other antipsychotic drugs and are considered to be prolactin-mediated. The relevance of this increased incidence of prolactin-mediated mammary gland tumors in rats to human risk is unknown [see Warnings and Precautions (5.15)].
Mutagenesis
Quetiapine was not mutagenic or clastogenic in standard genotoxicity tests. The mutagenic potential of quetiapine was tested in the in vitro Ames bacterial gene mutation assay and in the in vitro mammalian gene mutation assay in Chinese Hamster Ovary cells. The clastogenic potential of quetiapine was tested in the in vitro chromosomal aberration assay in cultured human lymphocytes and in the in vivo bone marrow micronucleus assay in rats up to 500 mg/kg which is 6 times the maximum recommended human dose on mg/m2 body surface area.
Impairment of Fertility
Quetiapine decreased mating and fertility in male Sprague-Dawley rats at oral doses of 50 and 150 mg/kg or approximately 1 and 3 times the MRHD of 800 mg/day based on mg/m2 body surface area. Drug-related effects included increases in interval to mate and in the number of matings required for successful impregnation. These effects continued to be observed at 3 times the MRHD even after a two-week period without treatment. The no-effect dose for impaired mating and fertility in male rats was 25 mg/kg, or 0.3 times the MRHD dose based on mg/m2 body surface area. Quetiapine adversely affected mating and fertility in female Sprague-Dawley rats at an oral dose approximately 1 times the MRHD of 800 mg/day based on mg/m2 body surface area. Drug-related effects included decreases in matings and in matings resulting in pregnancy, and an increase in the interval to mate. An increase in irregular estrus cycles was observed at doses of 10 and 50 mg/kg, or approximately 0.1 and 1 times the MRHD of 800 mg/day based on mg/m2 body surface area. The no-effect dose in female rats was 1 mg/kg, or 0.01 times the MRHD of 800 mg/day based on mg/m2 body surface area.
13.2 Animal Toxicology and/or Pharmacology
Quetiapine caused a dose-related increase in pigment deposition in thyroid gland in rat toxicity studies which were 4 weeks in duration or longer and in a mouse 2-year carcinogenicity study. Doses were 10, 25, 50, 75, 150 and 250 mg/kg in rat studies which are approximately 0.1, 0.3, 0.6, 1, 2 and 3-times the MRHD of 800 mg/day based on mg/m2 body surface area, respectively. Doses in the mouse carcinogenicity study were 20, 75, 250 and 750 mg/kg which are approximately 0.1, 0.5, 1.5, and 4.5 times the MRHD of 800 mg/day based on mg/m2 body surface area. Pigment deposition was shown to be irreversible in rats. The identity of the pigment could not be determined, but was found to be co-localized with quetiapine in thyroid gland follicular epithelial cells. The functional effects and the relevance of this finding to human risk are unknown.
In dogs receiving quetiapine for 6 or 12 months, but not for 1-month, focal triangular cataracts occurred at the junction of posterior sutures in the outer cortex of the lens at a dose of 100 mg/kg, or 4 times the MRHD of 800 mg/day based on mg/m2 body surface area. This finding may be due to inhibition of cholesterol biosynthesis by quetiapine. Quetiapine caused a dose-related reduction in plasma cholesterol levels in repeat-dose dog and monkey studies; however, there was no correlation between plasma cholesterol and the presence of cataracts in individual dogs. The appearance of delta-8-cholestanol in plasma is consistent with inhibition of a late stage in cholesterol biosynthesis in these species. There also was a 25% reduction in cholesterol content of the outer cortex of the lens observed in a special study in quetiapine treated female dogs. Drug-related cataracts have not been seen in any other species; however, in a 1-year study in monkeys, a striated appearance of the anterior lens surface was detected in 2/7 females at a dose of 225 mg/kg or 5.5 times the MRHD of 800 mg/day based on mg/m2 body surface area.
14 CLINICAL STUDIES
14.1 Schizophrenia
Short-term Trials-Adults
The efficacy of quetiapine fumarate extended-release tablets in the treatment of schizophrenia was demonstrated in 1 short-term, 6-week, fixed-dose, placebo-controlled trial of inpatients and outpatients with schizophrenia (n=573) who met DSM-IV criteria for schizophrenia. Quetiapine fumarate extended-release tablets (once daily) was administered as 300 mg on Day 1, and the dose was increased to either 400 mg or 600 mg by Day 2, or 800 mg by Day 3. The primary endpoint was the change from baseline of the Positive and Negative Syndrome Scale (PANSS) total score at the end of treatment (Day 42). Quetiapine fumarate extended-release tablets doses of 400 mg, 600 mg and 800 mg once daily were superior to placebo in the PANSS total score at Day 42 (study 1 in Table 26).
Short-term Trials -Adolescents (ages 13-17)
The efficacy of quetiapine fumarate extended-release tablets in the treatment of schizophrenia in adolescents (13-17 years of age) was supported by a 6-week, double-blind, placebo-controlled trial. Patients who met DSM-IV diagnostic criteria for schizophrenia were randomized into one of three treatment groups: quetiapine fumarate tablets 400 mg/day (n=73), quetiapine fumarate tablets 800 mg/day (n=74), or placebo (n=75). Study medication was initiated at 50 mg/day and on day 2 increased to 100 mg/per day (divided and given two or three times per day). Subsequently, the dose was titrated to the target dose of 400 mg/day or 800 mg/day using increments of 100 mg/day, divided and given two or three times daily. The primary efficacy variable was the mean change from baseline in total Positive and Negative Syndrome Scale (PANSS). Quetiapine fumarate tablets at 400 mg/day and 800 mg/day was superior to placebo in the reduction of PANSS total score (study 2 in Table 26).
|
|
||||
|
Study Number |
Treatment Group |
Primary Efficacy Endpoint: PANSS Total |
||
|
Mean Baseline Score (SD) |
LS Mean Change from Baseline (SE) |
Placebo-subtracted Difference* (95% CI) |
||
|
Study 1 |
Quetiapine fumarate extended-release tablets (400 mg/day)† |
95.8 (13.9) |
-24.8 (2.5) |
-6.1 (-11.5, -0.6) |
|
Quetiapine fumarate extended-release tablets (600 mg/day)† |
96.8 (14.1) |
-30.9 (2.5) |
-12.1 (-17.6, -6.7) |
|
|
Quetiapine fumarate extended-release tablets (800 mg/day)† |
97.3 (14.7) |
-31.3 (2.5) |
-12.5 (-17.9, -7.1) |
|
|
96.5 (16.0) |
-26.6 (2.4) |
-7.8 (-13.1, -2.4) |
||
|
Placebo |
96.2 (13.3) |
-18.8 (2.5) |
-- |
|
|
Study 2 (adolescents) |
Quetiapine fumarate tablets (400 mg/day)† |
96.2 (17.7) |
-27.3 (2.6) |
-8.2 (-16.1, -0.3) |
|
Quetiapine fumarate tablets (800 mg/day)† |
96.9 (15.3) |
-28.4 (1.8) |
-9.3 (-16.2, -2.4) |
|
|
Placebo |
96.2 (17.7) |
-19.2 (3.0) | ||
|
SD: standard deviation; SE: standard error; LS Mean: least-squares mean; CI: unadjusted confidence interval. |
||||
Maintenance Trials
In a longer-term trial (study 3), clinically stable adult outpatients (n=171) meeting DSM-IV criteria for schizophrenia who remained stable following 16 weeks of open-label treatment with flexible doses of quetiapine fumarate extended-release tablets (400 mg/day-800 mg/day) were randomized to placebo or to continue on their current quetiapine fumarate extended-release tablets (400 mg/day-800 mg/day) for observation for possible relapse during the double-blind continuation (maintenance) phase. Stabilization during the open-label phase was defined as receiving a stable dose of quetiapine fumarate extended-release tablets and having a CGI-S≤4 and a PANSS score ≤60 from beginning to end of this open-label phase (with no increase of ≥10 points in PANSS total score). Relapse during the double-blind phase was defined in terms of a ≥30% increase in the PANSS Total score, or CGI-Improvement score of ≥6, or hospitalization due to worsening of schizophrenia, or need for any other antipsychotic medication. Patients on quetiapine fumarate extended-release tablets experienced a statistically significant longer time to relapse than did patients on placebo (Figure 1).
Figure 1: Kaplan-Meier Curves of Time to Schizophrenic Relapse (study 3)
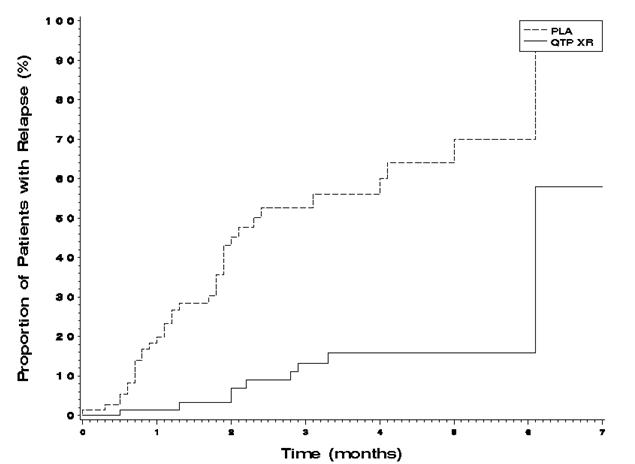
PLA Placebo. QTP Quetiapine. XR Extended-release.
Note: Results are from the interim analysis.
14.2 Bipolar Disorder
Bipolar I Disorder, manic or mixed episodes
Adults
The efficacy of quetiapine fumarate extended-release tablets in the acute treatment of manic episodes was established in one 3-week, placebo-controlled trial (Study 1 in Table 27) in patients who met DSM-IV criteria for bipolar I disorder with manic or mixed episodes with or without psychotic features (N=316). Patients were hospitalized for a minimum of 4 days at randomization. Patients randomized to quetiapine fumarate extended-release tablets received 300 mg on Day 1 and 600 mg on Day 2. Afterwards, the dose could be adjusted between 400 mg and 800 mg per day.
The primary rating instrument used for assessing manic symptoms in these trials was the Young Mania Rating Scale (YMRS), an 11-item clinician-rated scale traditionally used to assess the degree of manic symptoms in a range from 0 (no manic features) to 60 (maximum score). Quetiapine fumarate extended-release tablets was superior to placebo in the reduction of the YMRS total score at week 3.
The efficacy of quetiapine fumarate tablets in the treatment of acute manic episodes was also established in 3 placebo-controlled trials in patients who met DSM-IV criteria for bipolar I disorder with manic episodes. These trials included patients with or without psychotic features and excluded patients with rapid cycling and mixed episodes. Of these trials, 2 were monotherapy (12 weeks) and 1 was adjunct therapy (3 weeks) to either lithium or divalproex. Key outcomes in these trials were change from baseline in the YMRS score at 3 and 12 weeks for monotherapy and at 3 weeks for adjunct therapy. Adjunct therapy is defined as the simultaneous initiation or subsequent administration of quetiapine fumarate tablets with lithium or divalproex.
The results of the trials follow:
Monotherapy
In two 12-week trials (n=300, n=299) comparing quetiapine fumarate tablets to placebo, quetiapine fumarate tablets was superior to placebo in the reduction of the YMRS total score at weeks 3 and 12. The majority of patients in these trials taking quetiapine fumarate tablets were dosed in a range between 400 mg/day and 800 mg/ day (Studies 2 and 3 in Table 27).
Adjunct Therapy
In a 3-week placebo-controlled trial, 170 patients with bipolar mania (YMRS ≥20) were randomized to receive quetiapine fumarate tablets or placebo as adjunct treatment to lithium or divalproex. Patients may or may not have received an adequate treatment course of lithium or divalproex prior to randomization. Quetiapine fumarate tablets was superior to placebo when added to lithium or divalproex alone in the reduction of YMRS total score. The majority of patients in this trial taking quetiapine fumarate tablets were dosed in a range between 400 mg/day and 800 mg/day (study 4 in Table 27).
Children and Adolescents (ages 10-17)
The efficacy of quetiapine fumarate extended-release tablets in the acute treatment of manic episodes associated with bipolar I disorder in children and adolescents (10-17 years of age) was extrapolated from a 3-week, double-blind, placebo-controlled, multicenter trial. Patients who met DSM-IV diagnostic criteria for a manic episode were randomized into one of three treatment groups: quetiapine fumarate tablets 400 mg/day (n=95), quetiapine fumarate tablets 600 mg/day (n=98), or placebo (n=91). Study medication was initiated at 50 mg/day and on day 2 increased to 100 mg/day (divided doses given two or three times daily). Subsequently, the dose was titrated to a target dose of 400 mg/day or 600 mg/day using increments of 100 mg/day, given in divided doses two or three times daily. The primary efficacy variable was the mean change from baseline in total YMRS score. Quetiapine fumarate tablets 400 mg/day and 600 mg/day were superior to placebo in the reduction of YMRS total score (study 5 in Table 27).
|
|
||||
|
Study Number |
Treatment Group |
Primary Efficacy Measure: YMRS Total |
||
|
Mean Baseline Score (SD)* |
LS Mean Change from Baseline (SE) |
Placebo-subtracted Difference† (95% CI) |
||
|
Study 1 |
Quetiapine fumarate extended-release tablets (400-800 mg/day)‡ |
28.8 (5.4) |
-14.3 (0.9) |
-3.8 (-5.7, -2.0) |
|
Placebo |
28.4 (5.1) |
-10.5 (0.9) |
-- |
|
|
Study 2 |
Quetiapine fumarate tablets (200-800 mg/day)‡ |
34.0 (6.1) |
-12.3 (1.3) |
-4.0 (-7.0, -1.0) |
|
32.3 (6.0) |
-15.7 (1.3) |
-7.4 (-10.4, -4.4) |
||
|
Placebo |
33.1 (6.6) |
-8.3 (1.3) |
-- |
|
|
Study 3 |
Quetiapine fumarate tablets (200-800 mg/day)‡ |
32.7 (6.5) |
-14.6 (1.5) |
-7.9 (-10.9, -5.0) |
|
33.3 (7.1) |
-15.2 (1.6) |
-8.5 (-11.5, -5.5) |
||
|
Placebo + mood stabilizer |
34.0 (6.9) |
-6.7 (1.6) |
-- |
|
|
Study 4 |
Quetiapine fumarate tablets (200-800 mg/day)‡ + mood stabilizer |
31.5 (5.8) |
-13.8 (1.6) |
-3.8 (-7.1, -0.6) |
|
Placebo + mood stabilizer |
31.1 (5.5) |
-10 (1.5) |
-- |
|
|
Study 5 (children and adolescents) |
Quetiapine fumarate tablets (400 mg/day)‡ |
29.4 (5.9) |
-14.3 (0.96) |
-5.2 (-8.1, -2.3) |
|
Quetiapine fumarate tablets (600 mg/day)‡ |
29.6 (6.4) |
-15.6 (0.97) |
-6.6 (-9.5, -3.7) |
|
|
Placebo |
30.7 (5.9) |
-9.0 (1.1) |
-- |
|
|
Mood stabilizer: lithium or divalproex; SD: standard deviation; SE: standard error; LS Mean: least-squares mean; CI: unadjusted confidence interval. |
||||
Bipolar Disorder, Depressive Episodes
Adults
The efficacy of quetiapine fumarate extended-release tablets for the acute treatment of depressive episodes associated with bipolar disorder in patients who met DSM-IV criteria for bipolar disorder was established in one 8-week, randomized, double-blind, placebo-controlled study (N=280 outpatients). This study included patients with bipolar I and II disorder, and those with and without a rapid cycling course. Patients randomized to quetiapine fumarate extended-release tablets were administered 50 mg on Day 1, 100 mg on Day 2, 200 mg on Day 3, and 300 mg on Day 4 and after.
The primary rating instrument used to assess depressive symptoms was the Montgomery-Asberg Depression Rating Scale (MADRS), a 10-item clinician-rated scale with scores ranging from 0 (no depressive features) to 60 (maximum score). The primary endpoint was the change from baseline in MADRS score at week 8. Quetiapine fumarate extended-release tablets was superior to placebo in reduction of MADRS score at week 8 (study 6 in Table 28).
The efficacy of quetiapine fumarate tablets for the treatment of depressive episodes associated with bipolar disorder was established in 2 identical 8-week, randomized, double-blind, placebo-controlled studies (N=1045). These studies included patients with either bipolar I or II disorder and those with or without a rapid cycling course. Patients randomized to quetiapine fumarate tablets were administered fixed doses of either 300 mg or 600 mg once daily.
The primary rating instrument used to assess depressive symptoms in these studies was the MADRS. The primary endpoint in both studies was the change from baseline in MADRS score at week 8. In both studies, quetiapine fumarate tablets was superior to placebo in reduction of MADRS score at week 8 (Studies 7 and 8 in Table 28). In these studies, no additional benefit was seen with the 600 mg dose. For the 300 mg dose group, statistically significant improvements over placebo were seen in overall quality of life and satisfaction related to various areas of functioning, as measured using the Q-LES-Q(SF).
|
|
||||
|
Study Number |
Treatment Group |
Primary Efficacy Measure: MADRS Total |
||
|
Mean Baseline Score (SD) |
LS Mean Change from Baseline (SE) |
Placebo-subtracted Difference* (95% CI) |
||
|
Study 6 |
Quetiapine fumarate extended-release tablets (300 mg/day)† |
29.8 (5.2) |
-17.4 (1.2) |
-5.5 (-7.9, -3.2) |
|
Placebo |
30.1 (5.5) |
-11.9 (1.2) |
-- |
|
|
Study 7 |
Quetiapine fumarate tablets (300 mg/day)† |
30.3 (5.0) |
-16.4 (0.9) |
-6.1 (-8.3, -3.9) |
|
Quetiapine fumarate tablets (600 mg/day)† |
30.3 (5.3) |
-16.7 (0.9) |
-6.5 (-8.7, -4.3) |
|
|
Placebo |
30.6 (5.3) |
-10.3 (0.9) |
-- |
|
|
Study 8 |
Quetiapine fumarate tablets (300 mg/day)† |
31.1 (5.7) |
-16.9 (1.0) |
-5.0 (-7.3, -2.7) |
|
Quetiapine fumarate tablets (600 mg/day)† |
29.9 (5.6) |
-16.0 (1.0) |
-4.1 (-6.4, -1.8) |
|
|
Placebo |
29.6 (5.4) |
-11.9 (1.0) |
-- |
|
|
SD: standard deviation; SE: standard error; LS Mean: least-squares mean; CI: unadjusted confidence interval. |
||||
Maintenance Treatment as an Adjunct to Lithium or Divalproex
The efficacy of quetiapine fumarate tablets in the maintenance treatment of bipolar I disorder was established in 2 placebo-controlled trials in patients (n=1326) who met DSM-IV criteria for bipolar I disorder (studies 9 and 10). The trials included patients whose most recent episode was manic, depressed, or mixed, with or without psychotic features. In the open-label phase, patients were required to be stable on quetiapine fumarate tablets plus lithium or divalproex for at least 12 weeks in order to be randomized. On average, patients were stabilized for 15 weeks. In the randomization phase, patients continued treatment with lithium or divalproex and were randomized to receive either quetiapine fumarate tablets (administered twice-daily totaling 400 mg/day to 800 mg/day) or placebo. Approximately 50% of the patients had discontinued from the quetiapine fumarate tablets group by day 280 and 50% of the placebo group had discontinued by day 117 of double-blind treatment. The primary endpoint in these studies was time to recurrence of a mood event (manic, mixed, or depressed episode). A mood event was defined as medication initiation or hospitalization for a mood episode; YMRS score ≥20 or MADRS score ≥20 at 2 consecutive assessments; or study discontinuation due to a mood event.
In both studies, quetiapine fumarate tablets was superior to placebo in increasing the time to recurrence of any mood event (Figure 2 and Figure 3). The treatment effect was present for increasing time to recurrence of both manic and depressed episodes. The effect of quetiapine fumarate tablets was independent of any specific subgroup (assigned mood stabilizer, sex, age, race, most recent bipolar episode, or rapid cycling course).
Figure 2: Kaplan-Meier Curves of Time to Recurrence of a Mood Event (Study 9)
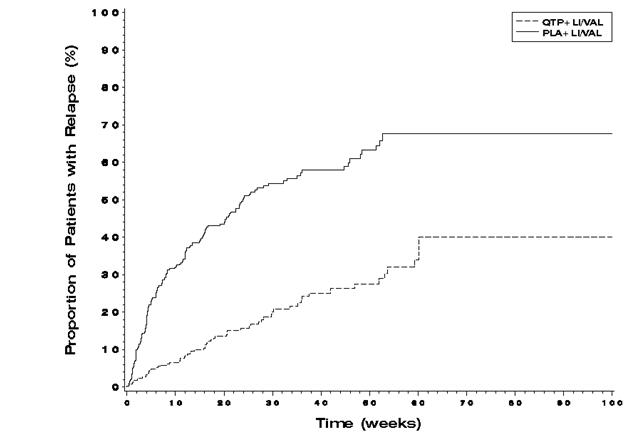
Figure 3: Kaplan-Meier Curves of Time to Recurrence of a Mood Event (Study 10)
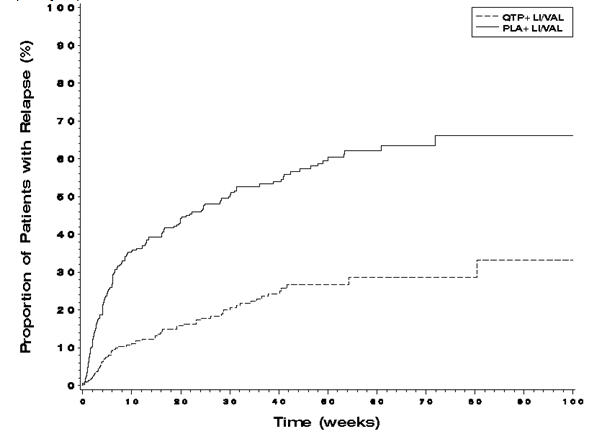
14.3 Major Depressive Disorder, Adjunctive Therapy to Antidepressants
The efficacy of quetiapine fumarate extended-release tablets as adjunctive therapy to antidepressants in the treatment of MDD was demonstrated in two 6-week placebo-controlled, fixed-dose trials (n=936). Quetiapine fumarate extended-release tablets 150 mg/day or 300 mg/day was given as adjunctive therapy to existing antidepressant therapy in patients who had previously shown an inadequate response to at least one antidepressant. Quetiapine fumarate extended-release tablets were administered as 50 mg/day on Days 1 and 2, and increased to 150 mg/day on Day 3 for both dose groups. On Day 5, the dose was increased to 300 mg/day in the 300 mg/day fixed-dose group. Inadequate response was defined as having continued depressive symptoms for the current episode [Hamilton Depression Rating Scale (HAM-D) total score of ≥20] despite using an antidepressant for 6 weeks at or above the minimally effective labelled dose. The mean HAM-D total score at entry was 24, and 17% of patients scored 28 or greater. Patients were on various antidepressants prior to study entry including SSRI’s (paroxetine, fluoxetine, sertraline, escitalopram, or citalopram), SNRI’s, (duloxetine and venlafaxine,) TCA (amitriptyline), and other (bupropion).
The primary endpoint in these trials was change from baseline to week 6 in the Montgomery-Asberg Depression Rating Scale (MADRS.), quetiapine fumarate extended-release tablets 300 mg once daily as adjunctive treatment to other antidepressant therapy was superior to antidepressant alone in reduction of MADRS total score in both trials. Quetiapine fumarate extended-release tablets 150 mg once daily as adjunctive treatment was superior to antidepressant therapy alone in reduction of MADRS total score in one trial (studies 1 and 2 in Table 29).
|
|
||||
|
Study Number |
Treatment Group |
Primary Efficacy Measure: MADRS Total |
||
|
Mean Baseline Score (SD) |
LS Mean Change from Baseline (SE) |
Placebo-subtracted Difference* (95% CI) |
||
|
Study 1 |
Quetiapine fumarate extended-release tablets (150 mg/day) + AD |
27.2 (5.2) |
-13.6 (0.8) |
-1.9 (-3.9, 0.1) |
|
Quetiapine fumarate extended-release tablets (300 mg/day)† + AD |
27.6 (5.0) |
-14.7 (0.8) |
-3.0 (-5.0, -1.0) |
|
|
Placebo + AD |
27.6 (5.5) |
-11.7 (0.8) |
-- |
|
|
Study 2 |
Quetiapine fumarate extended-release tablets (150 mg/day) + AD |
28.6 (5.4) |
-15.3 (0.7) |
-3.1 (-4.9, -1.2) |
|
Quetiapine fumarate extended-release tablets (300 mg/day) + AD |
28.4 (5.5) |
-14.9 (0.7) |
-2.7 (-4.6, -0.8) |
|
|
Placebo |
28.2 (5.6) |
-12.2 (0.7) |
-- |
|
|
AD: Antidepressant; SD: standard deviation; SE: standard error; LS Mean: least-squares mean; CI: unadjusted confidence interval. |
||||
16 HOW SUPPLIED/STORAGE AND HANDLING
- 50 mg Tablets (NDC: 49884-805-02) peach, film-coated, capsule-shaped, biconvex, intagliated tablet with “XR 50” on one side and plain on the other are supplied in bottles of 60 tablets.
- 150 mg Tablets (NDC: 49884-806-02) white, film-coated, capsule-shaped, biconvex, intagliated tablet with “XR 150” on one side and plain on the other are supplied in bottles of 60 tablets.
- 200 mg Tablets (NDC: 49884-807-02) yellow, film-coated, capsule-shaped, biconvex, intagliated tablet with “XR 200” on one side and plain on the other are supplied in bottles of 60 tablets.
- 300 mg Tablets (NDC: 49884-808-02) pale yellow, film-coated, capsule-shaped, biconvex, intagliated tablet with “XR 300” on one side and plain on the other are supplied in bottles of 60 tablets.
Store quetiapine fumarate extended-release tablets at 25ºC (77ºF); excursions permitted to 15 to 30ºC (59 to 86ºF) [See USP Controlled Room Temperature].
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Medication Guide)
Patients should be advised of the following issues and asked to alert their prescriber if these occur while taking quetiapine fumarate extended-release tablets.
Increased Mortality in Elderly Patients with Dementia-Related Psychosis
Patients and caregivers should be advised that elderly patients with dementia-related psychoses treated with atypical antipsychotic drugs are at increased risk of death compared with placebo. Quetiapine fumarate extended-release tablets are not approved for elderly patients with dementia-related psychosis [see Warnings and Precautions (5.1)].
Suicidal Thoughts and Behaviors
Patients, their families, and their caregivers should be encouraged to be alert to the emergence of anxiety, agitation, panic attacks, insomnia, irritability, hostility, aggressiveness, impulsivity, akathisia (psychomotor restlessness), hypomania, mania, other unusual changes in behavior, worsening of depression, and suicidal ideation, especially early during antidepressant treatment and when the dose is adjusted up or down. Families and caregivers of patients should be advised to look for the emergence of such symptoms on a day-to-day basis, since changes may be abrupt. Such symptoms should be reported to the patient's prescriber or health professional, especially if they are severe, abrupt in onset, or were not part of the patient's presenting symptoms. Symptoms such as these may be associated with an increased risk for suicidal thinking and behavior and indicate a need for very close monitoring and possibly changes in the medication [see Warnings and Precautions (5.2)].
Neuroleptic Malignant Syndrome (NMS)
Patients should be advised to report to their physician any signs or symptoms that may be related to NMS. These may include muscle stiffness and high fever [see Warnings and Precautions (5.4)].
Hyperglycemia and Diabetes Mellitus
Patients should be aware of the symptoms of hyperglycemia (high blood sugar) and diabetes mellitus. Patients who are diagnosed with diabetes, those with risk factors for diabetes, or those that develop these symptoms during treatment should have their blood glucose monitored at the beginning of and periodically during treatment [see Warnings and Precautions (5.5)].
Hyperlipidemia
Patients should be advised that elevations in total cholesterol, LDL-cholesterol and triglycerides and decreases in HDL-cholesterol may occur. Patients should have their lipid profile monitored at the beginning of and periodically during treatment [see Warnings and Precautions (5.5)].
Weight Gain
Patients should be advised that they may experience weight gain. Patients should have their weight monitored regularly [see Warnings and Precautions (5.5)].
Orthostatic Hypotension
Patients should be advised of the risk of orthostatic hypotension (symptoms include feeling dizzy or lightheaded upon standing, which may lead to falls) especially during the period of initial dose titration, and also at times of re-initiating treatment or increases in dose [see Warnings and Precautions (5.7)].
Increased Blood Pressure in Children and Adolescents
Children and adolescent patients should have their blood pressure measured at the beginning of, and periodically during, treatment [see Warnings and Precautions (5.9)].
Leukopenia/Neutropenia
Patients with a pre-existing low WBC or a history of drug induced leukopenia/neutropenia should be advised that they should have their CBC monitored while taking quetiapine fumarate extended-release tablets. Patients should be advised to talk to their doctor as soon as possible if they have a fever, flu-like symptoms, sore throat, or any other infection as this could be a result of a very low WBC, which may require quetiapine fumarate extended-release tablets to be stopped and/or treatment to be given [see Warnings and Precautions (5.10)].
Interference with Cognitive and Motor Performance
Patients should be advised of the risk of somnolence or sedation (which may lead to falls), especially during the period of initial dose titration. Patients should be cautioned about performing any activity requiring mental alertness, such as operating a motor vehicle (including automobiles) or operating machinery, until they are reasonably certain quetiapine therapy does not affect them adversely [see Warnings and Precautions (5.16)].
Heat Exposure and Dehydration
Patients should be advised regarding appropriate care in avoiding overheating and dehydration [see Warnings and Precautions (5.17)].
Concomitant Medication
As with other medications, patients should be advised to notify their physicians if they are taking, or plan to take, any prescription or over-the-counter drugs [see Drug Interactions (7.1)].
Pregnancy
Advise pregnant women to notify their healthcare provider if they become pregnant or intend to become pregnant during treatment with quetiapine fumarate extended-release tablets Advise patients that quetiapine fumarate extended-release tablets may cause extrapyramidal and/or withdrawal symptoms (agitation, hypertonia, hypotonia, tremor, somnolence, respiratory distress, and feeding disorder) in a neonate. Advise patients that there is a pregnancy registry that monitors pregnancy outcomes in women exposed to quetiapine fumarate extended-release tablets during pregnancy [see Use in Specific Populations (8.1)].
Infertility
Advise females of reproductive potential that quetiapine may impair fertility due to an increase in serum prolactin levels. The effects on fertility are reversible [see Use in Specific Populations (8.3)].
Need for Comprehensive Treatment Program
Quetiapine fumarate extended-release tablets are indicated as an integral part of a total treatment program for adolescents with schizophrenia and pediatric bipolar disorder that may include other measures (psychological, educational, and social). Effectiveness and safety of quetiapine fumarate extended-release tablets have not been established in pediatric patients less than 13 years of age for schizophrenia or less than 10 years of age for bipolar mania. Appropriate educational placement is essential and psychosocial intervention is often helpful. The decision to prescribe atypical antipsychotic medication will depend upon the physician’s assessment of the chronicity and severity of the patient’s symptoms [see Indications and Usage (1.4)].
Distributed by:
Par Pharmaceutical
Chestnut Ridge, NY 10977 U.S.A.
|
MEDICATION GUIDE
Quetiapine Fumarate (kweh-TIE-ah-peen)
Extended-Release Tablets
|
|
Read this Medication Guide before you start taking quetiapine fumarate extended-release tablets and each time you get a refill. There may be new information. This Medication Guide does not take the place of talking to your healthcare provider about your medical condition or treatment.
What is the most important information I should know about quetiapine fumarate extended-release tablets? Quetiapine fumarate extended-release tablets may cause serious side effects, including:
|
|
Talk to your or your family member’s, healthcare provider about:
|
|
Call a healthcare provider right away if you or your family member has any of the following symptoms, especially if they are new, worse, or worry you:
|
|
What else do I need to know about antidepressant medicines?
|
|
What is quetiapine fumarate extended-release tablets? Quetiapine fumarate extended-release tablets are a prescription medicine used to treat:
It is not known if quetiapine fumarate extended-release tablets are safe and effective in children under 10 years of age.
|
|
Who should not take quetiapine fumarate extended-release tablets?
Do not take quetiapine fumarate extended-release tablets if you are allergic to quetiapine fumarate or any of the ingredients in quetiapine fumarate extended-release tablets. See the end of this Medication Guide for a complete list of ingredients in quetiapine fumarate extended-release tablets.
|
|
What should I tell my healthcare provider before taking quetiapine fumarate extended-release tablets? Before you take quetiapine fumarate extended-release tablets, tell your healthcare provider if you have or have had:
Tell the healthcare provider about all the medicines that you take or recently have taken including prescription medicines, over-the-counter medicines, herbal supplements and vitamins. Quetiapine fumarate extended-release tablets and other medicines may affect each other causing serious side effects. Quetiapine fumarate extended-release tablets may affect the way other medicines work, and other medicines may affect how quetiapine fumarate extended-release tablets work.
Tell your healthcare provider if you are having a urine drug screen because quetiapine fumarate extended-release tablets may affect your test results. Tell those giving the test that you are taking quetiapine fumarate extended-release tablets.
|
|
How should I take quetiapine fumarate extended-release tablets?
What should I avoid while taking quetiapine fumarate extended-release tablets?
|
|
What are possible side effects of quetiapine fumarate extended-release tablets?
Quetiapine fumarate extended-release tablets can cause serious side effects, including: See “What is the most important information I should know about quetiapine fumarate extended-release tablets?”
|
|
Increases in blood sugar can happen in some people who take quetiapine fumarate extended-release tablets. Extremely high blood sugar can lead to coma or death. If you have diabetes or risk factors for diabetes (such as being overweight or a family history of diabetes) your healthcare provider should check your blood sugar before you start quetiapine fumarate extended-release tablets and during therapy. Call your healthcare provider if you have any of these symptoms of high blood sugar (hyperglycemia) while taking quetiapine fumarate extended-release tablets:
|
The most common side effects of quetiapine fumarate extended-release tablets include:
Children and Adolescents:
These are not all the possible side effects of quetiapine fumarate extended-release tablets. For more information, ask your healthcare provider or pharmacist. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
|
|
How should I store quetiapine fumarate extended-release tablets?
General information about the safe and effective use of quetiapine fumarate extended-release tablets. Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use quetiapine fumarate extended-release tablets for a condition for which it was not prescribed. Do not give quetiapine fumarate extended-release tablets to other people, even if they have the same symptoms you have. It may harm them. This Medication Guide summarizes the most important information about quetiapine fumarate extended-release tablets. If you would like more information, talk with your healthcare provider. You can ask your pharmacist or healthcare provider for information about quetiapine fumarate extended-release tablets that is written for health professionals.
What are the ingredients in quetiapine fumarate extended-release tablets?
Active ingredient: quetiapine fumarate
Inactive ingredients: lactose monohydrate, microcrystalline cellulose, sodium citrate, hypromellose, and magnesium stearate. The film coating for all quetiapine fumarate extended-release tablets contain hypromellose, polyethylene glycol 400 and titanium dioxide. In addition, yellow iron oxide (50, 200 and 300 mg tablets) and red iron oxide (50 mg tablets) are included in the film coating of specific strengths.
This Medication Guide has been approved by the U.S. Food and Drug Administration.
Distributed by: Par Pharmaceutical Chestnut Ridge, NY 10977 U.S.A. Revised: October 2019 |
| QUETIAPINE FUMARATE
EXTENDED RELEASE
quetiapine fumarate tablet, extended release |
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
| QUETIAPINE FUMARATE
EXTENDED RELEASE
quetiapine fumarate tablet, extended release |
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
| QUETIAPINE FUMARATE
EXTENDED RELEASE
quetiapine fumarate tablet, extended release |
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
| QUETIAPINE FUMARATE
EXTENDED RELEASE
quetiapine fumarate tablet, extended release |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| Labeler - Par Pharmaceutical Inc. (092733690) |
| Registrant - AstraZeneca PLC (230790719) |