EVKEEZA- evinacumab injection, solution, concentrate
Evkeeza by
Drug Labeling and Warnings
Evkeeza by is a Prescription medication manufactured, distributed, or labeled by Regeneron Pharmaceuticals, Inc., Regn Ireland DAC. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use EVKEEZA safely and effectively. See full prescribing information for EVKEEZA.
EVKEEZA® (evinacumab-dgnb) injection, for intravenous use
Initial U.S. Approval: 2021RECENT MAJOR CHANGES
INDICATIONS AND USAGE
EVKEEZA is an angiopoietin-like 3 (ANGPTL3) inhibitor indicated as an adjunct to diet and exercise and other low-density lipoprotein-cholesterol (LDL-C) lowering therapies to reduce LDL-C in adults and pediatric patients, aged 1 year and older, with homozygous familial hypercholesterolemia (HoFH). (1)
DOSAGE AND ADMINISTRATION
- The recommended dosage of EVKEEZA is 15 mg/kg administered by intravenous (IV) infusion once monthly (every 4 weeks). (2.1)
- See the Full Prescribing Information for preparation instructions for the intravenous infusion. (2.2)
- Administer the diluted solution via IV infusion over 60 minutes through an IV line containing a sterile, in-line or add-on, 0.2-micron to 5-micron filter. (2.3)
- Do not mix other medications with EVKEEZA or administer other medications concomitantly via the same infusion line. (2.3)
- The rate of infusion may be slowed, interrupted or discontinued if the patient develops any signs of adverse reactions, including infusion or hypersensitivity reactions. (2.3)
DOSAGE FORMS AND STRENGTHS
- Injection: 345 mg/2.3 mL (150 mg/mL) and 1,200 mg/8 mL (150 mg/mL) solution in single-dose vials. (3)
CONTRAINDICATIONS
- History of serious hypersensitivity reactions to evinacumab-dgnb or to any of the excipients in EVKEEZA. (4)
WARNINGS AND PRECAUTIONS
- Serious Hypersensitivity Reactions: Have occurred with EVKEEZA in clinical trials. If a serious hypersensitivity reaction occurs, discontinue EVKEEZA, treat according to standard-of-care and monitor until signs and symptoms resolve. (5.1)
- Embryo-Fetal Toxicity: EVKEEZA may cause fetal harm based on animal studies. Advise patients who may become pregnant of the risk to a fetus. Consider obtaining a pregnancy test prior to initiating treatment with EVKEEZA. Advise patients who may become pregnant to use contraception during treatment and for at least 5 months following the last dosage. (5.2, 8.1, 8.3)
ADVERSE REACTIONS
Common adverse reactions (≥5%) were nasopharyngitis, influenza-like illness, dizziness, rhinorrhea, nausea, and fatigue. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Regeneron at 1-833-385-3392 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.
Revised: 9/2025
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dosage
2.2 Preparation Instructions for Intravenous Infusion
2.3 Administration Instructions for Intravenous Infusion
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Serious Hypersensitivity Reactions
5.2 Embryo-Fetal Toxicity
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.3 Females and Males of Reproductive Potential
8.4 Pediatric Use
8.5 Geriatric Use
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
12.6 Immunogenicity
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- * Sections or subsections omitted from the full prescribing information are not listed.
- 1 INDICATIONS AND USAGE
-
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dosage
- The recommended dosage of EVKEEZA is 15 mg/kg administered by intravenous (IV) infusion over 60 minutes once monthly (every 4 weeks).
- If a dosage of EVKEEZA is missed, administer as soon as possible. Thereafter, EVKEEZA should be scheduled monthly from the date of the last dosage.
- Assess LDL-C when clinically appropriate. The LDL-lowering effect of EVKEEZA may be measured as early as 2 weeks after initiation.
2.2 Preparation Instructions for Intravenous Infusion
- Calculate the dosage (mg), total volume (mL) of EVKEEZA required, and the number of vials required based on the patient's current body weight.
- Visually inspect the solution for cloudiness, discoloration, and particulate matter prior to administration. EVKEEZA is a clear to slightly opalescent, colorless to pale-yellow solution. Do not administer if the solution is cloudy, discolored, or contains particulate matter.
- EVKEEZA is supplied as single-dose vials and does not contain a preservative. Prepare the diluted infusion using aseptic technique.
- Do not shake the vial. Withdraw the required volume from the vial(s) of EVKEEZA and transfer into an IV infusion bag of 0.9% Sodium Chloride Injection or 5% Dextrose Injection. Discard any unused portion left in the vials. Mix the diluted solution by gentle inversion; do not shake. Maximum diluent volume by patient weight is summarized in Table 1.
-
Table 1: Maximum Diluent Volume by Patient Weight
Patient Weight Maximum Diluent Volume 3 kg to less than 26 kg 5 mL/kg 26 kg to less than 45 kg 150 mL 45 kg and greater 250 mL - The final concentration of the diluted solution should be between 0.5 mg/mL and 20 mg/mL depending on the patient's current body weight.
- Administer the diluted solution immediately after preparation and discard any unused portion left in the vial.
- If not administered immediately, store the diluted solution refrigerated at 2 °C to 8 °C (36 °F to 46 °F) for no more than 24 hours from the time of preparation OR at room temperature up to 25 °C (77 °F) for no more than 6 hours from the time of preparation to the end of the infusion. Do not freeze the diluted solution.
2.3 Administration Instructions for Intravenous Infusion
- If refrigerated, allow the diluted solution to come to room temperature prior to administration.
- Administer EVKEEZA diluted solution via IV infusion through an IV line containing a sterile, in-line or add-on, 0.2-micron to 5-micron filter over 60 minutes.
- Do not mix other medications with EVKEEZA or administer other medications concomitantly via the same infusion line.
- The rate of infusion may be slowed, interrupted or discontinued if the patient develops any signs of adverse reactions, including infusion or hypersensitivity reactions [see Warnings and Precautions (5.1) and Adverse Reactions (6.1)].
- EVKEEZA can be administered without regard to the timing of lipoprotein apheresis.
- 3 DOSAGE FORMS AND STRENGTHS
-
4 CONTRAINDICATIONS
EVKEEZA is contraindicated in patients with a history of serious hypersensitivity reaction to evinacumab-dgnb or to any of the excipients in EVKEEZA. Serious hypersensitivity reactions, including anaphylaxis, have occurred [see Warnings and Precautions (5.1)].
-
5 WARNINGS AND PRECAUTIONS
5.1 Serious Hypersensitivity Reactions
Serious hypersensitivity reactions, including anaphylaxis, have occurred with EVKEEZA [see Adverse Reactions (6.1)]. If signs or symptoms of serious hypersensitivity reactions occur, discontinue EVKEEZA infusion, treat according to the standard-of-care, and monitor until signs and symptoms resolve. EVKEEZA is contraindicated in patients with a history of serious hypersensitivity reaction to evinacumab-dgnb.
5.2 Embryo-Fetal Toxicity
Based on the findings in animal reproduction studies, EVKEEZA may cause fetal harm when administered to pregnant patients. Administration of evinacumab-dgnb to rabbits during organogenesis caused increases in fetal malformations at doses below the human exposure. Advise patients who may become pregnant of the risk to a fetus. Consider obtaining a pregnancy test prior to initiating treatment with EVKEEZA. Advise patients who may become pregnant to use effective contraception during treatment with EVKEEZA and for at least 5 months following the last dosage of EVKEEZA [see Use in Specific Populations (8.1, 8.3)].
-
6 ADVERSE REACTIONS
The following clinically significant adverse reactions are described elsewhere in the labeling:
- Serious Hypersensitivity Reactions [see Warnings and Precautions (5.1)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Adverse Reactions in Adult and Pediatric Patients (aged 12 to 17 years) with HoFH
Safety data are based on pooled results from two randomized, double-blind, placebo-controlled trials that included 81 patients treated with EVKEEZA. The mean age of EVKEEZA-treated patients was 48 years (range: 15 to 75 years); 52% were females; 5% were Hispanic; 82% were White, 7% Asian, 3% Black or African American, and 9% other races. Forty-four (54%) EVKEEZA-treated patients had HoFH. Patients received EVKEEZA as add-on therapy to other lipid-lowering therapies, including maximally tolerated statin, ezetimibe, proprotein convertase subtilisin kexin type 9 (PCSK9) inhibitors, lomitapide, and apheresis.
Adverse reactions led to discontinuation of treatment in 1 (2%) patient who received placebo, and 2 (2%) patients treated with EVKEEZA, including 1 case of anaphylaxis. The most common adverse reactions (reported in greater than 3% of EVKEEZA-treated patients and more frequently than in placebo) are shown in Table 2.
Table 2: Adverse Reactions Occurring in >3% of Adult and Pediatric Patients Aged 12 to 17 Years Treated with EVKEEZA and Greater than Placebo in 24-Week, Pooled, Placebo-Controlled Trials Adverse Reactions Placebo
(N = 54)
%EVKEEZA
(N = 81)
%Nasopharyngitis 13 16 Influenza like illness 6 7 Dizziness 0 6 Rhinorrhea 0 5 Nausea 2 5 Pain in extremity 0 4 Asthenia 0 4 Other adverse reactions occurring in less than 3% of patients treated with EVKEEZA and greater than placebo included constipation, upper respiratory tract infection, nasal congestion, and abdominal pain.
Transient, mild to moderate decreases in diastolic blood pressure and increases in heart rate occurred in clinical trials of EVKEEZA infusion but did not require intervention and resolved post-infusion.
Serious Hypersensitivity Reactions
Anaphylaxis was reported in 0% patients who received placebo and 1 (1%) patient treated with EVKEEZA.
Infusion Reactions
Infusion reactions were reported in 2 (4%) patients who received placebo and 6 (7%) patients treated with EVKEEZA. The following infusion reactions occurred in EVKEEZA-treated patients: infusion site pruritus, pyrexia, muscular weakness, nausea, and nasal congestion.
Adverse Reactions in Pediatric Patients (aged 5 to 11 years) with HoFH
Safety data are based on pooled results from a three-part, open-label trial in 20 pediatric patients with HoFH (aged 5 to 11 years) with a median treatment duration of 50 weeks. Part A was a trial of 6 patients who received a single intravenous dose of EVKEEZA 15 mg/kg to determine the dosage for the rest of the trial. Part B was a single-arm, 24-week trial of EVKEEZA 15 mg/kg given intravenously every 4 weeks in 14 unique patients [see Clinical Studies (14)]. Part C was a 48-week extension trial of EVKEEZA 15 mg/kg given intravenously every 4 weeks that consisted of 20 patients who entered directly from Parts A or B. The mean age was 9 years (range: 5 to 11 years); 60% females; 70% White, 10% Asian, 5% Black or African American, 5% American Indian or Alaska Native, and 10% other races. The safety profile of EVKEEZA observed in these patients was consistent with the safety profile observed in adults and pediatric patients aged 12 years and older, with the additional adverse reaction of fatigue. Fatigue was reported in 3 (15%) patients.
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
Based on data from animal reproduction studies, EVKEEZA may cause fetal harm when administered to pregnant patients. Available human data are insufficient to evaluate for a drug-associated risk of major birth defects, miscarriage or adverse maternal or fetal outcomes. Evinacumab-dgnb is a human IgG4 monoclonal antibody [see Description (11)], and human IgG is known to cross the placental barrier; therefore, evinacumab-dgnb has the potential to be transmitted from the mother to the developing fetus.
Subcutaneous administration of evinacumab-dgnb to pregnant rabbits during the period of organogenesis resulted in fetal malformations (domed head, hydrocephalus, and flexed limbs) at doses below the maximum recommended human dose (MRHD). No adverse embryofetal effects were observed with subcutaneous administration of evinacumab-dgnb to pregnant rats during the period of organogenesis at doses below the MRHD. Measurable evinacumab-dgnb serum concentrations were observed in fetal rabbit and rat sera at birth, indicating that evinacumab-dgnb, like other IgG antibodies, crosses the placental barrier (see Data). Advise pregnant women of the potential risk to a fetus.
The estimated background risk of major birth defects and miscarriage for the indicated population are unknown. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2-4% and 15-20%, respectively.
If a patient becomes pregnant while receiving EVKEEZA, healthcare providers should report EVKEEZA exposure by calling 1-833-385-3392.
Animal Data
In an embryo-fetal development study in pregnant rabbits, evinacumab-dgnb was administered subcutaneously at doses of 1, 5, 10 and 30 mg/kg every 3 days (Q3D) during the period of organogenesis from gestation day 7 to day 19. Evinacumab-dgnb was teratogenic in rabbits, causing domed head, dilation of the lateral and third ventricles of the brain, and flexed fore/hind paws at maternal evinacumab-dgnb exposures below human exposure at the MRHD of 15 mg/kg every 4 weeks, based on AUC. Other fetal malformations, consisting of irregular and abnormal ossification in the skull, palate, and metacarpal, and enlarged anterior and/or posterior fontanelles occurred and were consistent with significant maternal toxicity (including early deaths due to abortion and premature delivery at all doses, reduction in maternal body weight gains, and reduced maternal food consumption). Increased incidences of post-implantation losses, resorptions (total, early, and late), and decreased fetal body weight were also consistent with maternal toxicity. Evinacumab-dgnb was present in the sera of fetuses born from mothers at 10 and 30 mg/kg/Q3D at levels higher than in maternal serum.
In an embryo-fetal development study in pregnant rats, evinacumab-dgnb was administered subcutaneously at doses of 5, 10, 30 and 100 mg/kg/Q3D during the period of organogenesis from gestation day 6 to day 18. Maternal exposures to evinacumab-dgnb were below the human exposure measured at the MRHD. Evinacumab-dgnb resulted in unexplained maternal deaths at 100 mg/kg/Q3D. Evinacumab-dgnb crossed the placenta and was present at ratios (CFetal/CMaternal) ranging from 0.42 to 0.65. No adverse effects on embryofetal development were observed at any dose.
In a combined fertility, embryofetal, and pre- and postnatal development study, female rats were administered evinacumab-dgnb via subcutaneous injection at doses of 30 and 100 mg/kg/Q3D beginning 2 weeks prior to mating and continuing to gestation day 21 or lactation day 21. Mean maternal systemic exposures were below the human exposure at the MRHD throughout the study. No maternal or developmental toxicity was observed.
8.2 Lactation
Risk Summary
There are no data on the presence of evinacumab-dgnb in human milk or animal milk, the effects on the breastfed infant, or the effects on milk production. Maternal IgG is known to be present in human milk. The effects of local gastrointestinal exposure and limited systemic exposure in the breastfed infant to evinacumab-dgnb are unknown. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for EVKEEZA and any potential adverse effects on the breastfed infant from EVKEEZA or from the underlying maternal condition.
8.3 Females and Males of Reproductive Potential
Pregnancy Testing
Consider pregnancy testing in patients who may become pregnant prior to starting treatment with EVKEEZA [see Warnings and Precautions (5.2) and Use in Specific Populations (8.1)].
Contraception
Females
Based on animal studies, EVKEEZA may cause fetal harm when administered to pregnant patients [see Use in Specific Populations (8.1)]. Patients who may become pregnant should use effective contraception during treatment with EVKEEZA and for at least 5 months following the last dosage of EVKEEZA.
8.4 Pediatric Use
The safety and effectiveness of EVKEEZA as an adjunct to other LDL-C-lowering therapies for the treatment of HoFH have been established in pediatric patients aged 1 year and older. Use of EVKEEZA for this indication is supported by evidence from adequate and well-controlled trials in adults with additional pharmacokinetic, efficacy, and safety data in pediatric patients aged 1 year and older [see Adverse Reactions (6.1), Clinical Pharmacology (12.3) and Clinical Studies (14)]. The safety profile of EVKEEZA in pediatric patients aged 1 to 11 years was similar to the safety profile in adults and pediatric patients aged 12 years and older, with the additional adverse reaction of fatigue in patients aged 5 to 11 years [see Adverse Reactions (6.1)].
The safety and effectiveness of EVKEEZA have not been established in pediatric patients younger than 1 year of age.
-
11 DESCRIPTION
Evinacumab-dgnb is an angiopoietin-like protein 3 (ANGPTL3) inhibitor monoclonal antibody (IgG4 isotype) produced by recombinant DNA technology in Chinese hamster ovary (CHO) cell suspension culture. Evinacumab-dgnb has an approximate molecular weight of 146 kDa.
EVKEEZA (evinacumab-dgnb) injection is a sterile, preservative-free solution for intravenous use. The solution is clear to slightly opalescent, colorless to pale-yellow, and free from visible particles.
Each vial contains 345 mg/2.3 mL or 1,200 mg/8 mL. Each mL contains 150 mg of evinacumab-dgnb, and L-arginine hydrochloride (14.8 mg), L-histidine (0.74 mg), L-histidine monohydrochloride monohydrate (1.1 mg), L-proline (30 mg), polysorbate 80 (1 mg) and Water for Injection, USP. The pH is 6.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Evinacumab-dgnb is a recombinant human monoclonal antibody that binds to and inhibits ANGPTL3. ANGPTL3 is a member of the angiopoietin-like protein family that is expressed primarily in the liver and plays a role in the regulation of lipid metabolism by inhibiting lipoprotein lipase (LPL) and endothelial lipase (EL). Evinacumab-dgnb inhibition of ANGPTL3 leads to reduction in LDL-C, high-density lipoprotein cholesterol (HDL-C), and triglycerides (TG). Evinacumab-dgnb reduces LDL-C independent of the presence of LDL receptor (LDLR) by promoting very low-density lipoprotein (VLDL) processing and clearance upstream of LDL formation. Evinacumab-dgnb blockade of ANGPTL3 lowers TG and HDL-C by rescuing LPL and EL activities, respectively.
12.2 Pharmacodynamics
Administration of evinacumab-dgnb in patients with HoFH resulted in reductions in LDL-C, total cholesterol (TC), HDL-C, apolipoprotein B and TG [see Clinical Studies (14)].
12.3 Pharmacokinetics
The pharmacokinetic parameters described in this section are presented following administration of evinacumab-dgnb 15 mg/kg intravenously every 4 weeks, unless otherwise specified.
Steady-state is reached after 4 doses, and the accumulation ratio is 2. According to population pharmacokinetic modeling, the mean (standard deviation) steady-state trough concentration is 266 (120) mg/L in adult patients, whereas the mean (standard deviation) Cmax at the end of infusion is 718 (183) mg/L in adult patients. Due to non-linear clearance, a 4.3-fold increase in area under the concentration-time curve at steady-state (AUCtau.ss) for a 3-fold increase in evinacumab-dgnb dose up to 15 mg/kg IV every 4 weeks was predicted in patients with HoFH.
Distribution
The steady-state volume of distribution estimated via population pharmacokinetic analysis was approximately 4.7 L in adult patients.
Elimination
Evinacumab-dgnb elimination is mediated via parallel linear and non-linear pathways. At higher concentrations, evinacumab-dgnb elimination is primarily through a non-saturable proteolytic pathway, whereas at lower concentrations, the non-linear, saturable ANGPTL3 target-mediated elimination predominates. The elimination half-life is a function of serum evinacumab-dgnb concentrations and is not a constant.
Based on a population pharmacokinetic analysis, the median time for serum evinacumab-dgnb concentrations to decrease below the lower limit of quantitation (78 ng/mL) is approximately 20 weeks after the last steady-state dose of 15 mg/kg IV every 4 weeks.
Metabolism
The exact pathway through which evinacumab-dgnb is metabolized has not been characterized. As a human monoclonal IgG4 antibody, evinacumab-dgnb is expected to be degraded into small peptides and amino acids via catabolic pathways in the same manner as endogenous IgG.
Excretion
Evinacumab-dgnb, a monoclonal antibody, is not likely to undergo renal excretion.
Specific Populations
A population PK analysis conducted on data from 183 healthy subjects and 139 patients with HoFH suggests that the following factors have no clinically significant effect on the exposure of evinacumab-dgnb: age (5 to 75 years), gender, body weight (20 to 152 kg), and race (White, Asian, Black or African American, American Indian or Alaska Native, and other races).
Pediatric Patients
Fourteen (14) patients aged 12 to less than 18 years with HoFH received evinacumab-dgnb at 15 mg/kg IV every 4 weeks. Steady-state trough and end-of-infusion concentrations were within the range observed in adult patients.
Twenty (20) patients aged 5 to less than 12 years with HoFH received evinacumab-dgnb at 15 mg/kg IV every 4 weeks. According to population pharmacokinetic modeling, the mean (standard deviation) steady-state trough concentration is 160 (57.6) mg/L in pediatric patients, whereas the mean (standard deviation) Cmax at the end of infusion is 419 (99.4) mg/L in pediatric patients. Steady-state trough and end-of-infusion concentrations were lower but within the range observed in adult patients.
The predicted mean (standard deviation) steady-state trough and maximum concentrations were 135 (62) and 500(182) mg/L for patients aged 1 year to less than 2 years. The predicted mean (standard deviation) steady-state trough and maximum concentrations were 141(61) and 513(179) mg/L for patients aged 2 to less than 5 years.
Patients with Renal Impairment
Observed trough serum evinacumab-dgnb concentrations at steady-state were comparable between patients with mild or moderate renal impairment and patients with normal renal function. No data are available in patients with severe renal impairment.
Patients with Hepatic Impairment
No data are available in patients with hepatic impairment.
Drug Interaction Studies
Drug interaction studies have not been conducted with evinacumab-dgnb. In a clinical trial, the concentrations of statins (atorvastatin, rosuvastatin, simvastatin) were not meaningfully altered in patients taking statins prior to and post administration of evinacumab-dgnb. Concentrations of evinacumab-dgnb were comparable in patients with HoFH taking or not taking background lipid-lowering therapy.
12.6 Immunogenicity
The observed incidence of anti-drug antibodies is highly dependent on the sensitivity and specificity of the assay. Differences in assay methods preclude meaningful comparisons of the incidence of anti-drug antibodies in the trials described below with the incidence of anti-drug antibodies in other trials, including those of EVKEEZA or of other evinacumab-dgnb products. During the 24-week treatment period in the trials in:
- Adult and pediatric patients aged 12 years and older with HoFH (Trials 1 and 2) [see Clinical Studies (14)], the incidence of anti-evinacumab-dgnb antibody formation was 0% (0 of 56) in EVKEEZA-treated patients.
- Pediatric patients aged 5 to 11 years with HoFH (Trial 3) [see Clinical Studies (14)], the incidence of anti-evinacumab-dgnb antibody formation was 5% (1 of 20) in EVKEEZA-treated patients. In the one patient that developed anti-evinacumab-dgnb antibodies, there were no effects on efficacy or evinacumab-dgnb concentrations.
- Because of the low occurrence of anti-evinacumab-dgnb antibodies, the effect of these antibodies on the pharmacokinetics, pharmacodynamics, safety, and/or effectiveness of evinacumab products is unknown.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis and Mutagenesis
Carcinogenicity studies have not been conducted with evinacumab-dgnb. The mutagenic potential of evinacumab-dgnb has not been evaluated; however, monoclonal antibodies are not expected to alter DNA or chromosomes.
Impairment of Fertility
There were no adverse effects on surrogate markers of fertility (estrous cyclicity, testicular volume, ejaculate volume, sperm motility, total sperm count per ejaculate, and histology of reproductive organs) in a 6-month chronic toxicology study in sexually-mature male and female monkeys subcutaneously administered 10, 30, or 100 mg/kg/week (0.2, 1, and 3-fold MRHD based on AUC, respectively) and intravenously administered 100 mg/kg/week (4-fold MRHD, based on AUC).
In a combined fertility and early embryonic and pre-and postnatal development study in female rats administered evinacumab-dgnb via subcutaneous injection at dosages 30 and 100 mg/kg/Q3D beginning 2 weeks prior to mating, no adverse effect on female fertility were observed at any dosage. Exposures to evinacumab-dgnb represented less than the human exposure at the MRHD, based on AUC. No effects on male fertility were observed with evinacumab-dgnb administration to male rabbits for 40 days prior to mating with treatment-naïve females. Evinacumab-dgnb was administered to male rabbits intravenously at 100 and 300 mg/kg/Q5D, representing exposures 2- and 5-times, respectively, the human exposure at the MRHD, based on AUC.
-
14 CLINICAL STUDIES
Adult and Pediatric Patients Aged 12 Years and Older with HoFH
Trial ELIPSE-HoFH (NCT03399786; Trial 1) was a multicenter, double-blind, randomized, placebo-controlled trial that evaluated the efficacy of EVKEEZA compared to placebo in 65 patients with HoFH (63 adult patients and 2 pediatric patients). During the 24-week, double-blind treatment period, patients were randomized to receive EVKEEZA 15 mg/kg given intravenously every 4 weeks (n=43) or placebo given intravenously every 4 weeks (n=22). After the double-blind treatment period, 64 of 65 patients entered a 24-week open-label extension period in which all patients received EVKEEZA 15 mg/kg given intravenously every 4 weeks.
Patients were on a background of other lipid-lowering therapies, including maximally tolerated statins, ezetimibe, PCSK9 inhibitor antibodies, lomitapide, and lipoprotein apheresis. Enrollment was stratified by apheresis status and geographical region. The diagnosis of HoFH was determined by genetic testing or by the presence of the following clinical criteria: history of an untreated total cholesterol (TC) >500 mg/dL and either xanthoma before 10 years of age or evidence of TC >250 mg/dL in both parents.
Baseline Disease and Demographic Characteristics
In this trial, 40% (26 of 65) patients had limited LDL receptor (LDLR) function, defined by either <15% receptor function by in vitro assays or by genetic variants likely to result in minimal to no LDLR function by mutation analysis.
The mean LDL-C at baseline was 255 mg/dL (in patients with limited LDLR function, the mean LDL-C at baseline was 307 mg/dL). At baseline, 94% of patients were on statins, 75% on ezetimibe, 77% on a PCSK9 inhibitor antibody, 22% on lomitapide, and 34% were receiving lipoprotein apheresis. The mean age at baseline was 42 years (range 12 to 75) with 12% ≥65 years old; 54% females; 3% Hispanic; 74% White, 15% Asian, 3% Black or African American, and 8% other races or race was not reported.
Endpoint Results
The primary efficacy endpoint was percent change in LDL-C from baseline to Week 24. At Week 24, the least squares (LS) mean treatment difference between the EVKEEZA and placebo groups in mean percent change in LDL-C from baseline was −49% (95% confidence interval: −65% to −33%; p <0.0001). After 24 weeks of open-label EVKEEZA treatment (Week 24 to Week 48), the observed LDL-C reduction from baseline was similar in patients who crossed over from placebo to EVKEEZA and was maintained in patients who remained on EVKEEZA for 48 weeks. For efficacy results see Table 3.
At Week 24, the observed reduction in LDL-C with EVKEEZA was similar across predefined subgroups, including age, sex, limited LDLR activity, concomitant treatment with lipoprotein apheresis, and concomitant background lipid-lowering medications (statins, ezetimibe, PCSK9 inhibitor antibodies, and lomitapide).
Table 3: Lipid Parameters in Patients (63 Adults and 2 Pediatric Patients) with HoFH on Other Lipid-Lowering Therapies in Trial ELIPSE-HoFH (Trial 1) LDL-C ApoB Non-HDL-C TC TG* HDL-C* One subject in the placebo group discontinued the trial before Week 24. The treatment difference and 95% confidence interval (CI) were estimated using a mixed model repeated measures analysis.
Abbreviations: HoFH=homozygous familial hypercholesterolemia, ITT=intent-to-treat, LS mean=least squares mean, N=number of randomized patients, CI=confidence interval- * Neither TG nor HDL-C were pre-specified in the hypothesis testing
- † Mean percent change, based on safety population (EVKEEZA, n=44; placebo, n=21); HDL-C is presented for completeness but was not an efficacy endpoint that was statistically analyzed.
Baseline (mean), mg/dL
(N=65)255 171 278 322 124 44 LS Mean: EVKEEZA
(N = 43)−47% −41% −50% −47% −55% −30%† LS Mean: Placebo
(N = 22)+2% −5% +2% +1% −5% +1%† LS Mean Difference from Placebo
(95% CI)−49%
(−65 to −33)−37%
(−49 to −25)−52%
(−65 to −39)−48%
(−59 to −38)−50%
(−66 to −35)-† The LS mean LDL-C percent changes over time are presented in Figure 1.
Abbreviations: LS mean=least squares mean, HoFH=homozygous familial hypercholesterolemia, DBTP=double-blind treatment period, SE=standard error Figure 1: Calculated LDL-C LS Mean Percent Change from Baseline Over Time Through Week 24 in Patients (63 Adults and 2 Pediatric Patients) with HoFH in Trial ELIPSE-HoFH (Trial 1) 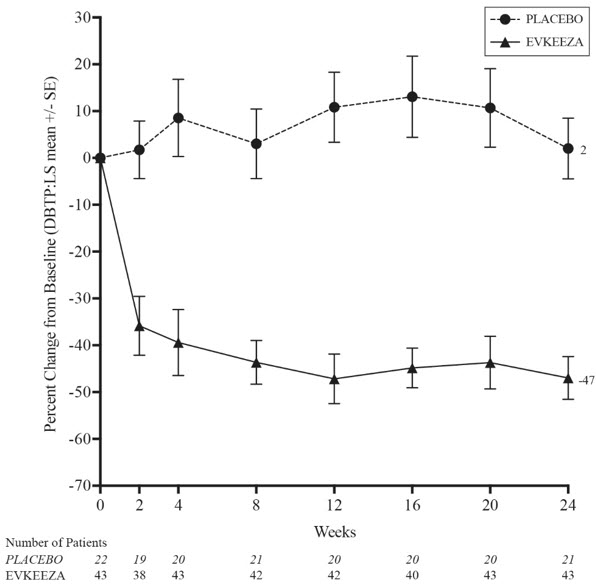
Pediatric Patients (aged 12 to 17 years) with HoFH
In an open-label trial (Trial 2), 13 pediatric patients with HoFH (aged 12 to 17 years) received 15 mg/kg of EVKEEZA given intravenously every 4 weeks as an adjunct to other lipid-lowering therapies (e.g., statins, ezetimibe, PCSK9 inhibitor antibodies and lipoprotein apheresis) for a median treatment duration of 33 weeks. The mean percent change from baseline in LDL-C at Week 24 was −52% in the 9 patients who completed treatment and had a lipid assessment at Week 24. Overall, the effect of EVKEEZA on lipid parameters in pediatric patients aged 12 to 17 years with HoFH was generally similar to that seen in adults with HoFH.
Pediatric Patients (aged 5 to 11 years) with HoFH
Trial R1500-CL-17100 (NCT04233918; Trial 3) was a multicenter, three-part, single-arm, open-label trial in pediatric patients aged 5 to 11 years with HoFH [see Adverse Reactions (6.1)]. Part B of this trial evaluated the efficacy of EVKEEZA 15 mg/kg given intravenously every 4 weeks as an adjunct to other lipid-lowering therapies (e.g., statins, ezetimibe, lomitapide, and lipoprotein apheresis) for 24 weeks in 14 patients with HoFH.
Baseline Disease and Demographic Characteristics
In Part B, the mean LDL-C at baseline was 264 mg/dL.
At baseline, 86% of patients were on statins, 93% on ezetimibe, 14% on lomitapide, and 50% were receiving lipoprotein apheresis.
The mean age at baseline was 9 years (range 5 to 11); 57% females; 0% Hispanic; 57% White, 14% Asian, 7% Black or African American, 7% American Indian or Alaska Native, and 14% other races. Mean body weight was 40 kg. Body mass index (BMI) was 20 kg/m2.
Endpoint Results
The primary efficacy endpoint was percent change in calculated LDL-C from baseline to Week 24. At Week 24, the mean percent change in calculated LDL-C from baseline was −48% (95% confidence interval: −69% to −28%). For efficacy results see Table 4. HDL-C and TG reductions observed in this trial were similar to changes seen in Trial 1, see Table 3.
At Week 24, the reduction in LDL-C with EVKEEZA was similar across baseline characteristics, including age, sex, limited LDLR activity, concomitant treatment with lipoprotein apheresis, and concomitant background lipid-lowering medications (statins, ezetimibe, and lomitapide).
Table 4: Lipid Parameters in EVKEEZA-Treated Pediatric Patients (aged 5 to 11 years) with HoFH Who Received Concomitant Lipid-Lowering Therapies (Trial 3) LDL-C ApoB Non-HDL-C TC Abbreviations: HoFH=homozygous familial hypercholesterolemia, N=number of randomized patients, CI=confidence interval Baseline (mean)
(N=14)264 mg/dL 168 mg/dL 282 mg/dL 316 mg/dL Percent Change from Baseline at Week 24
(95% CI)-48
(-69 to -28)-41
(-59 to -24)-49
(-68 to -30)-49
(-65 to -33)Pediatric Patients (aged 1 to less than 5 years) with HoFH
Clinical data were collected through an expanded access program that required each patient's treating physician to provide adequate documentation to demonstrate that the patient met the eligibility criteria for the program and to provide effectiveness information, including LDL-C values. The efficacy of EVKEEZA was evaluated in 6 patients aged 1 to less than 5 years with HoFH. Four females and two males were enrolled in the program. At baseline, 83% of patients were on statins, 83% on ezetimibe, 17% on PCSK9 inhibitors, and 17% were receiving plasmapheresis. The mean LDL-C at baseline was 499 mg/dL (range 238 to 872 mg/dL), the mean age was 3.2 years (range 1.1 to 4.4 years), and the mean weight was 14.5 kg (range 8 to 17 kg). Patients received 15 mg/kg EVKEEZA every 4 weeks for up to 98 weeks. Administration of EVKEEZA resulted in a reduction of LDL-C [mean (standard deviation) change at Week 40 of -60% (16.8)].
-
16 HOW SUPPLIED/STORAGE AND HANDLING
EVKEEZA (evinacumab-dgnb) injection is a clear to slightly opalescent, colorless to pale yellow solution. It is supplied as one single-dose vial per carton.
- 345 mg/2.3 mL (150 mg/mL) NDC: 61755-013-01
- 1,200 mg/8 mL (150 mg/mL) NDC: 61755-010-01
Storage
Store in a refrigerator at 2 °C to 8 °C (36 °F to 46 °F). Store the vial in the original carton to protect from light. Do not freeze. Do not shake.
EVKEEZA does not contain a preservative. If not used immediately, store the diluted solution refrigerated at 2 °C to 8 °C (36 °F to 46 °F) for no more than 24 hours from the time of preparation OR at room temperature up to 25 °C (77 °F) for no more than 6 hours from the time of infusion preparation to the end of the infusion [see Dosage and Administration (2.2)].
-
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient Information).
Hypersensitivity Reactions
Inform patients that hypersensitivity reactions have occurred with EVKEEZA. Advise patients to contact their healthcare provider immediately if they experience signs or symptoms of a hypersensitivity reaction [see Warnings and Precautions (5.1)].
Embryofetal Toxicity
Advise pregnant patients and patients that may become pregnant of the potential risk to a fetus and to inform their healthcare provider of a known or suspected pregnancy. Advise patients who may become pregnant to use effective contraception during treatment with EVKEEZA and for 5 months after the final dosage. Encourage patients who become pregnant to report their pregnancy to 1-833-385-3392 [see Warnings and Precautions (5.2) and Use in Specific Populations (8.1, 8.3)].
- SPL UNCLASSIFIED SECTION
-
PATIENT PACKAGE INSERT
Patient Information
EVKEEZA® (ev-kee'-zah)
(evinacumab-dgnb)
injection, for intravenous useThis Patient Information has been approved by the U.S. Food and Drug Administration. Revised: September 2025 What is EVKEEZA?
EVKEEZA is an injectable prescription medicine used along with diet and exercise and other low-density lipoprotein cholesterol (LDL-C) lowering medicines to lower LDL-C in adults and children 1 year of age and older with a type of high cholesterol called homozygous familial hypercholesterolemia (HoFH).It is not known if EVKEEZA is safe and effective in children under 1 year of age. Who should not use EVKEEZA?
Do not use EVKEEZA if you are allergic to evinacumab-dgnb or to any of the ingredients in EVKEEZA. See the end of this leaflet for a complete list of ingredients in EVKEEZA.Before receiving EVKEEZA, tell your healthcare provider about all of your medical conditions, including if you: - are pregnant or plan to become pregnant. EVKEEZA may harm your unborn baby. Tell your healthcare provider if you become pregnant while using EVKEEZA. People who are able to become pregnant:
- Your healthcare provider may do a pregnancy test before you start treatment with EVKEEZA.
- You should use an effective method of birth control during treatment and for at least 5 months after the last dose of EVKEEZA. Talk with your healthcare provider about birth control methods that you can use during this time.
- are breastfeeding or plan to breastfeed. It is not known if EVKEEZA passes into your breast milk. You and your healthcare provider should decide if you will receive EVKEEZA or breastfeed.
How will I receive EVKEEZA? - Your healthcare provider will give you EVKEEZA into your veins through an intravenous (IV) line over 60 minutes.
- EVKEEZA should be given every month (4 weeks).
- If you miss any infusion appointments, call your healthcare provider as soon as possible to reschedule.
- Your healthcare provider may slow down your infusion rate, temporarily stop, or permanently stop treatment with EVKEEZA if you have certain side effects. See "What are the possible side effects of EVKEEZA?"
- Your healthcare provider may prescribe other cholesterol-lowering medicines, to use with EVKEEZA. Use the other prescribed medicines exactly as your healthcare provider tells you to.
What are the possible side effects of EVKEEZA?
EVKEEZA can cause serious side effects, including:- Allergic reactions (hypersensitivity), including a severe reaction known as anaphylaxis. Tell your healthcare provider right away if you get any of the following symptoms:
- swelling – mainly of the lips, tongue or throat which makes it difficult to swallow or breathe
- breathing problems or wheezing
- feeling dizzy or fainting
- rash, hives
- itching
The most common side effects of EVKEEZA include: - symptoms of the common cold
- flu like symptoms
- dizziness
- runny nose
- nausea
- feeling tired or weak
Tell your healthcare provider if you have any side effect that bothers you or that does not go away.
These are not all of the possible side effects of EVKEEZA.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.General information about the safe and effective use of EVKEEZA.
Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. If you would like more information about EVKEEZA, talk with your healthcare provider. You can ask your healthcare provider for information about EVKEEZA that is written for health professionals.What are the ingredients in EVKEEZA?
Active ingredient: evinacumab-dgnb
Inactive ingredients: L-arginine hydrochloride, L-histidine, L-histidine monohydrochloride monohydrate, L-proline, polysorbate 80, and Water for Injection, USP.Manufactured by:
Regeneron Pharmaceuticals, Inc. 777 Old Saw Mill River Road Tarrytown, NY 10591-6707 U.S. License No. 1760
©2025 Regeneron Pharmaceuticals, Inc. All rights reserved.
For more information about EVKEEZA, go to www.EVKEEZA.com or call 1-833-EVKEEZA (833-385-3392) - are pregnant or plan to become pregnant. EVKEEZA may harm your unborn baby. Tell your healthcare provider if you become pregnant while using EVKEEZA. People who are able to become pregnant:
-
PRINCIPAL DISPLAY PANEL - 345 mg/2.3 mL Vial Carton
NDC: 61755-013-01
Rx onlyEvkeeza®
(evinacumab-dgnb)
Injection345 mg/2.3 mL (150 mg/mL)
For Intravenous Infusion after Dilution
Single-Dose Vial – Discard Unused Portion
Must dilute before use.
Do not use vial if seal is broken or missing.
Do not use after expiration.
Store in the original carton to
protect from light.
-
PRINCIPAL DISPLAY PANEL - 1200 mg/8 mL Vial Carton
NDC: 61755-010-01
Rx onlyEvkeeza®
(evinacumab-dgnb)
Injection1200 mg/8 mL (150 mg/mL)
For Intravenous Infusion after Dilution
Single-Dose Vial – Discard Unused Portion
Must dilute before use.
Do not use vial if seal is broken or missing.
Do not use after expiration.
Store in the original carton to protect
from light.
-
INGREDIENTS AND APPEARANCE
EVKEEZA
evinacumab injection, solution, concentrateProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 61755-013 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength evinacumab (UNII: T8B2ORP1DW) (evinacumab - UNII:T8B2ORP1DW) evinacumab 150 mg in 1 mL Inactive Ingredients Ingredient Name Strength Histidine (UNII: 4QD397987E) 0.74 mg in 1 mL Histidine monohydrochloride monohydrate (UNII: X573657P6P) 1.1 mg in 1 mL Proline (UNII: 9DLQ4CIU6V) 30 mg in 1 mL Polysorbate 80 (UNII: 6OZP39ZG8H) 1 mg in 1 mL Arginine hydrochloride (UNII: F7LTH1E20Y) 14.75 mg in 1 mL Water (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 61755-013-01 1 in 1 CARTON 02/11/2021 1 2.3 mL in 1 VIAL, SINGLE-USE; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA761181 02/11/2021 EVKEEZA
evinacumab injection, solution, concentrateProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 61755-010 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength evinacumab (UNII: T8B2ORP1DW) (evinacumab - UNII:T8B2ORP1DW) evinacumab 150 mg in 1 mL Inactive Ingredients Ingredient Name Strength Histidine (UNII: 4QD397987E) 0.74 mg in 1 mL Histidine monohydrochloride monohydrate (UNII: X573657P6P) 1.1 mg in 1 mL Proline (UNII: 9DLQ4CIU6V) 30 mg in 1 mL Polysorbate 80 (UNII: 6OZP39ZG8H) 1 mg in 1 mL Arginine hydrochloride (UNII: F7LTH1E20Y) 14.75 mg in 1 mL Water (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 61755-010-01 1 in 1 CARTON 02/11/2021 1 8 mL in 1 VIAL, SINGLE-USE; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA761181 02/11/2021 Labeler - Regeneron Pharmaceuticals, Inc. (194873139) Establishment Name Address ID/FEI Business Operations Regn Ireland DAC 986063166 ANALYSIS(61755-013, 61755-010)
Trademark Results [Evkeeza]
Mark Image Registration | Serial | Company Trademark Application Date |
|---|---|
 EVKEEZA 88589908 not registered Live/Pending |
Regeneron Pharmaceuticals, Inc. 2019-08-23 |
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.