SILVER SULFADIAZINE cream
Silver Sulfadiazine by
Drug Labeling and Warnings
Silver Sulfadiazine by is a Prescription medication manufactured, distributed, or labeled by DIRECT RX. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
DESCRIPTION SECTION
SSD™ (1% Silver Sulfadiazine Cream) and SSD AF™ (1% Silver Sulfadiazine Cream), 1% are topical antibacterial preparations which have as their active antimicrobial ingredient silver sulfadiazine. The active moiety is contained within an opaque, white, water miscible cream base.
Each 1000 grams of SSD/SSD AF Cream contains 10 grams of silver sulfadiazine.
Inactive Ingrediants: cetyl alcohol (SSD Cream only), isopropyl myristate, polyoxyl 40 stearate, propylene glycol, purified water, stearyl alcohol, sodium hydroxide, sorbitan monooleate, white petrolatum; with 0.3% methyl paraben, as a preservative.
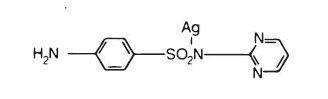
Silver sulfadiazine has an emprical formula of C10H9AgN4O2S, molecular weight of 357.14 and structural formula as shown:
-
CLINICAL PHARMACOLOGY SECTION
Silver sulfadiazine has broad antimicrobial activity. It is bactericidal for many gram-negative and gram-positive bacteria as well as being effective against yeast. Results from in vitro testing are listed below. Sufficient data have been obtained to demonstrate that silver sulfadiazine will inhibit bacteria that are resistant to other antimicrobial agents and that the compound is superior to sulfadiazine. Studies utilizing radioactive micronized silver sulfadiazine, electron microscopy, and biochemical techniques have revealed that the mechanism of action of silver sulfadiazine on bacteria differs from silver nitrate and sodium sulfadiazine. Silver sulfadiazine acts only on the cell wall to produce its bactericidal effect.
Results of In Vitro Testing With Silver Sulfadiazine Cream, 1% Concentration of Silver Sulfadiazine
Number of Sensitive Strains / Total Number of Strains TestedGenus and Species 50 micrograms/mL 100 micrograms/mL
Pseudomonas Aeruginosa 130/130 130/130
Xanthomonas (Pseudomonas)
Maltophilia 7/7 7/7
Enterobacter Species 48/50 50/50
Enterobacter cloacae 24/24 24/24
Klebsiella Species 53/54 54/54
Escherichia Coli 63/63 63/63
Serratia Species 27/28 28/28
Proteus Mirabilis 53/53 53/53
Morganella Morganii 10/10 10/10
Providencia Rettgeri 2/2 2/2
Proteus Vulgaris 2/2 2/2
Providencia Species 1/1 1/1
Citrobacter Species 10/10 10/10
Acinetobacter Calcoaceticus 10/11 11/11
Stahylococcus Aureus 100/101 101/101
Staphylococcus Epidermidis 51/51 51/51
B-Hemolytic Streptococcus 4/4 4/4
Enterococcus Species 52/53 53/53
Corynebacterium Diphtheriae 2/2 2/2
Clostridium Perfringens 0/2 2/2
Clostridium Perfringens 0/2 2/2
Candida Albicans 43/50 50/50
Silver sulfadiazine is not a carbonic anhydrase inhibitor and may be useful in situations where such agents are contraindicated.
- INDICATIONS & USAGE SECTION
-
CONTRAINDICATIONS SECTION
Silver Sulfadiazine Cream is contraindicated in patients who are hypersensitive to silver sulfadiazine or any of the other ingredients in the preparation.
Because sulfonamide therapy is known to increase the possibility of kernicterus, Silver Sulfadiazine Cream should not be used on pregnant women approaching or at term, on premature infants, or on newborn infants during the first 2 months of life.
-
WARNINGS SECTION
There is a potential cross-sensitivity between silver sulfadiazine and other sulfonamides. If allergic reactions attributable to treatment with silver sulfadiazine occur, continuation of therapy must be weighed against the potential hazards of the particular allergic reaction.
Fungal proliferation in and below the eschar may occur. However, the incidence of clinically reported fungal superinfection is low.
The use of Silver Sulfadiazine Cream in some cases of glucose-6-phosphate dehydrogenase-deficient individuals may be hazardous, as hemolysis may occur.
-
PRECAUTIONS SECTION
-
If hepatic and renal functions become impaired and elimination of the drug decreases accumulation may occur and discontinuation of Silver Sulfadiazine Cream should be weighed against the therapeutic benefit being achieved.
In considering the use of topical proteolytic enzymes in conjunction with Silver Sulfadiazine Cream, the possibility should be noted that silver may inactivate such enzymes.
Laboratory Tests: In the treatment of burn wounds involving extensive areas of the body, the serum sulfa concentrations may approach adult therapeutic levels (8 to 12mg %). Therefore, in these patients it would be advisable to monitor serum sulfa concentrations. Renal function should be carefully monitored and the urine should be checked for sulfa crystals.
Absorption of the propylene glycol vehicle has been reported to affect serum osmolality, which may affect the interpretation of laboratory tests.
-
-
CARCINOGENESIS & MUTAGENESIS & IMPAIRMENT OF FERTILITY SECTION
Long-term dermal toxicity studies of 24 months duration in rats and 18 months in mice with concentrations of silver sulfadiazine three to ten times the concentration in Silver Sulfadiazine Cream revealed no evidence of carcinogenicity.
Pregnancy: Pregnancy Category B. A reproductive study has been performed in rabbits at doses up to three to ten times the concentration of silver sulfadiazine in Silver Sulfadiazine Cream and has revealed no evidence of harm to the fetus due to silver sulfadiazine. There are, however, no adequate and well-controlled studies in pregnant women. Because animal reproduction studies are not always predictive of human response, this drug should be used during pregnancy only if clearly justified, especially in pregnant women approaching or at term. (See CONTRAINDICATIONS)
Nursing Mother: It is not known whether Silver Sulfadiazine Cream is excreted in human milk. However, sulfonamides are known to be excreted in human milk and all sulfonamides derivatives are known to increase the possibility of kernicterus. Because of the potential for serious adverse reactions in nursing infants from sulfonamides, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
Pediatric Use: Safety and effectiveness in children have not been established. (See CONTRAINDICATIONS)
-
ADVERSE REACTIONS SECTION
Several cases of transient leucopenia have been reported in patients receiving silver sulfadiazine therapy. Leucopenia associated with silver sulfadiazine administration is primarily characterized by decreased neutrophil count. Maximal white blood cell depression occurs within two to four days of initiation of therapy. Rebound to normal leukocyte levels follows onset within two to three days. Recovery is not influenced by continuation of silver sulfadiazine therapy. The incidence of leucopenia in various reports averages about 20%. A higher incidence has been seen in patients treated concurrently with cimetidine.
Other infrequently occurring events include skin necrosis, erythema multiforme, skin discoloration, burning sensation, rashes, and interstitial nephritis. Reduction in bacterial growth after application of topical antibacterial agents has been reported to permit spontaneous healing of deep partial thickness burns by preventing conversion of the partial thickness to full thickness by sepsis. However, reduction in bacterial colonization has caused delayed separation, in some cases necessitating escharotomy in order to prevent contracture.
Absorption of silver sulfadiazine varies depending upon the percent of body surface area and the extent of the tissue damage. Although few have been reported, it is possible that any adverse reaction associated with sulfonamides may occur. Some of the reactions which have been associated with sulfonamides are as follows: blood dyscrasias, agranulocytosis, aplastic anemia, thrombocytopenia, leucopenia, hemolytic anemia, dermatologic reactions, allergic reactions, Stevens-Johnson syndrome, exfoliative dermatitis, gastrointestinal reactions, hepatitis, hepatocellular necrosis, CNS reactions, and toxic nephrosis.
-
DOSAGE & ADMINISTRATION SECTION
Prompt institution of appropriate regimens for care of the burned patient is of prime importance and includes the control of shock and pain. The burn wounds are then cleansed and debrided; Silver Sulfadiazine Cream is then applied under sterile conditions. The burn areas should be covered with Silver Sulfadiazine Cream at all times. The cream should be applied once to twice daily to a thickness of approximately one sixteenth of an inch. Whenever necessary, the cream should be reapplied to any areas from which it has been removed due to patient activity. Administration may be accomplished in minimal time because dressings are not required. However, if individual patient requirements make dressings necessary, they may be used. Reapply immediately after hydrotherapy. Treatment with Silver Sulfadiazine Cream should be continued until satisfactory healing has occurred or until the burn site is ready for grafting. The drug should not be withdrawn from the therapeutic regimen while there remains the possibility of infection except if a significant adverse reaction occurs.
-
HOW SUPPLIED SECTION
-
SSD™ (1% Silver Sulfadiazine) Cream: white to off-white cream.
50 gram jar NDC: 43598-210-55
400 gram jar NDC: 43598-210-40
25 gram tube NDC: 43598-210-25
50 gram tube NDC: 43598-210-50
85 gram tube NDC: 43598-210-85
SSD AF™ (1% Silver Sulfadiazine) Cream: white to off-white cream.
50 gram jar NDC: 43598-211-55
400 gram jar NDC: 43598-211-40
Store at controlled room temperature 15° - 30°C (59° - 86°F)
SSD is a trademark of Dr. Reddy's Laboratories, Inc.
Manufactured by:
Dr. Reddy's Laboratories Louisiana LLC
Shreveport, LA 71106 USARevised, June 2013
-
- PACKAGE LABEL.PRINCIPAL DISPLAY PANEL
-
INGREDIENTS AND APPEARANCE
SILVER SULFADIAZINE
silver sulfadiazine creamProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 61919-237(NDC:43598-210) Route of Administration TOPICAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength SILVER SULFADIAZINE (UNII: W46JY43EJR) (SILVER CATION - UNII:57N7B0K90A) SILVER SULFADIAZINE 10 g in 1000 g Inactive Ingredients Ingredient Name Strength WATER (UNII: 059QF0KO0R) CETYL ALCOHOL (UNII: 936JST6JCN) STEARYL ALCOHOL (UNII: 2KR89I4H1Y) PETROLATUM (UNII: 4T6H12BN9U) POLYOXYL 40 STEARATE (UNII: 13A4J4NH9I) PROPYLENE GLYCOL (UNII: 6DC9Q167V3) ISOPROPYL MYRISTATE (UNII: 0RE8K4LNJS) SORBITAN MONOOLEATE (UNII: 06XEA2VD56) METHYLPARABEN (UNII: A2I8C7HI9T) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 61919-237-25 25 g in 1 TUBE; Type 0: Not a Combination Product 01/01/2015 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA018578 01/01/2014 Labeler - DIRECT RX (079254320) Establishment Name Address ID/FEI Business Operations DIRECT RX 079254320 relabel(61919-237) , repack(61919-237)
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.