SULFACETAMIDE SODIUM AND PREDNISOLONE SODIUM PHOSPHATE solution/ drops
Sulfacetamide Sodium and Prednisolone Sodium Phosphate by
Drug Labeling and Warnings
Sulfacetamide Sodium and Prednisolone Sodium Phosphate by is a Prescription medication manufactured, distributed, or labeled by NuCare Pharmaceuticals,Inc.. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
- SPL UNCLASSIFIED SECTION
-
DESCRIPTION
Sulfacetamide Sodium and Prednisolone Sodium Phosphate Ophthalmic Solution is a sterile topical ophthalmic solution combining an anti-infective and an adrenocortical steroid.
Each mL contains: ACTIVES: Sulfacetamide Sodium 100 mg, Prednisolone Sodium Phosphate 2.5 mg (equivalent to Prednisolone Phosphate 2.3 mg); INACTIVES: Poloxamer 407, Boric Acid, Edetate Disodium, Purified Water. Hydrochloric Acid and/or Sodium Hydroxide may be added to adjust pH (6.5-7.5). PRESERVATIVE ADDED: Thimerosal 0.01%.
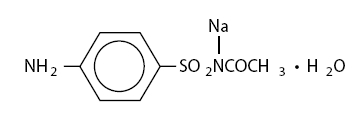
The chemical name for sulfacetamide sodium is N-sulfanilylacetamide monosodium salt monohydrate.
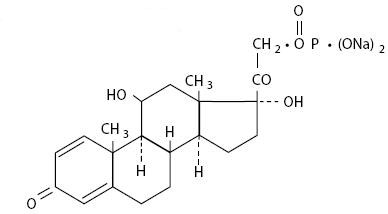
The chemical name for prednisolone sodium phosphate is 11β, 17, 21-trihydroxypregna-1, 4-diene-3,20-dione, 21-(disodium phosphate).
They have the following structural formulas:
Sulfacetamide Sodium
C 8H 9N 2NaO 3SH 2O Mol. Wt. 254.24
Prednisolone Sodium Phosphate
C 21H 27Na 2O 8P Mol. Wt. 484.39
-
CLINICAL PHARMACOLOGY
Corticosteroids suppress the inflammatory response to a variety of agents and they probably delay or slow healing. Since corticosteroids may inhibit the body's defense mechanism against infection, a concomitant antimicrobial drug may be used when this inhibition is considered to be clinically significant in a particular case.
When a decision to administer both a corticosteroid and an antimicrobial is made, the administration of such drugs in combination has the advantage of greater patient compliance and convenience, with the added assurance that the appropriate dosage of both drugs is administered, plus assured compatibility of ingredients when both types of drugs are in the same formulation and, particularly, that the correct amount of drug is delivered and retained.
The relative potency of a corticosteroid depends on the molecular structure, concentration, and release from the vehicle.
Microbiology
Sulfacetamide sodium exerts a bacteriostatic effect against susceptible bacteria by restricting the synthesis of folic acid required for growth through competition with p-aminobenzoic acid.
Some strains of bacteria may be resistant to sulfacetamide or resistant strains may emerge in vivo.
The anti-infective component in Sulfacetamide Sodium and Prednisolone Sodium Phosphate Ophthalmic Solution is included to provide action against specific organisms susceptible to it. Sulfacetamide sodium is active in vitro against susceptible strains of the following microorganisms: Escherichia coli, Staphylococcus aureus, Streptococcus (viridans group) , Haemophilus influenzae, Klebsiella species and Enterobacter species. The product does not provide adequate coverage against: Neisseria species, Pseudomonas species, Serratia marcescens (see INDICATIONS AND USAGE).
-
INDICATIONS AND USAGE
Sulfacetamide Sodium and Prednisolone Sodium Phosphate Ophthalmic Solution is indicated for corticosteroid-responsive inflammatory ocular conditions for which a corticosteroid is indicated and where superficial bacterial ocular infection or a risk of bacterial ocular infection exists.
Ocular corticosteroids are indicated in inflammatory conditions of the palpebral and bulbar conjunctiva, cornea, and anterior segment of the globe where the inherent risk of corticosteroid use in certain infective conjunctivitides is accepted to obtain diminution in edema and inflammation. They are also indicated in chronic anterior uveitis and corneal injury from chemical, radiation, or thermal burns or penetration of foreign bodies.
The use of a combination drug with an anti-infective component is indicated where the risk of superficial ocular infection is high or where there is an expectation that potentially dangerous numbers of bacteria will be present in the eye.
The particular anti-infective drug in this product is active against the following common bacterial eye pathogens: Escherichia coli, Staphylococcus aureus, Streptococcus pneumoniae, Streptococcus (viridans group), Haemophilus influenzae, Klebsiella species, and Enterobacter species.
This product does not provide adequate coverage against: Neisseria species, Serratia marcescens.
A significant percentage of staphylococcal isolates are completely resistant to sulfa drugs.
-
CONTRAINDICATIONS
Sulfacetamide Sodium and Prednisolone Sodium Phosphate Ophthalmic Solution is contraindicated in most viral diseases of the cornea and conjunctiva including epithelial herpes simplex keratitis (dendritic keratitis), vaccinia, and varicella, and also in mycobacterial infection of the eye and fungal diseases of ocular structures. This product is also contraindicated in individuals with known or suspected hypersensitivity to any of the ingredients of this preparation, to other sulfonamides, or to other corticosteroids. (Hypersensitivity to the antimicrobial components occurs at a higher rate than for other components).
-
WARNINGS
NOT FOR INJECTION INTO THE EYE.
Prolonged use of corticosteroids may result in ocular hypertension/glaucoma with damage to the optic nerve, defects in visual acuity and fields of vision, and in posterior subcapsular cataract formation.
Acute anterior uveitis may occur in susceptible individuals, primarily Blacks.
Prolonged use of Sulfacetamide Sodium and Prednisolone Sodium Phosphate Ophthalmic Solution may suppress the host response and thus increase the hazard of secondary ocular infections. In those diseases causing thinning of the cornea or sclera, perforations have been known to occur with the use of topical corticosteroids. In acute purulent conditions of the eye, corticosteroids may mask infection or enhance existing infection.
If this product is used for 10 days or longer, intraocular pressure should be routinely monitored even though it may be difficult in children and uncooperative patients. Corticosteroids should be used with caution in the presence of glaucoma. Intraocular pressure should be checked frequently.
The use of corticosteroids after cataract surgery may delay healing and increase the incidence of filtering blebs.
The use of ocular corticosteroids may prolong the course and may exacerbate the severity of many viral infections of the eye (including herpes simplex). Employment of corticosteroid medication in the treatment of herpes simplex requires great caution.
A significant percentage of staphylococcal isolates are completely resistant to sulfonamides.
Topical corticosteroids are not effective in mustard gas keratitis and Sjögren's keratoconjunctivitis.
Fatalities have occurred, although rarely, due to severe reactions to sulfonamides including Stevens-Johnson syndrome, toxic epidermal necrolysis, fulminant hepatic necrosis, agranulocytosis, aplastic anemia, and other blood dyscrasias. Sensitizations may recur when a sulfonamide is readministered irrespective of the route of administration. If signs of hypersensitivity or other serious reactions occur, discontinue use of this preparation. Cross-sensitivity among corticosteroids have been demonstrated (see ADVERSE REACTIONS).
Do not administer this product to patients who are sensitive/allergic to thimerosal or any other mercury containing ingredient.
-
PRECAUTIONS
General
The initial prescription and renewal of the medication order beyond 20 mL of Sulfacetamide Sodium and Prednisolone Sodium Phosphate Ophthalmic Solution should be made by a physician only after examination of the patient with the aid of magnification such as slit-lamp biomicroscopy and, where appropriate, fluorescein staining. If signs and symptoms fail to improve after two days, the patient should return to the office for further evaluation.
The possibility of fungal infections of the cornea should be considered after prolonged corticosteroid dosing. Fungal cultures should be taken when appropriate.
The p-aminobenzoic acid present in purulent exudates competes with sulfonamides and can reduce their effectiveness.
Sulfonamide solutions darken on prolonged standing and exposure to heat and light. Do not use if solution has darkened. Yellowing does not affect activity.
Information For Patients
If inflammation or pain persists longer than 48 hours or becomes aggravated, the patient should be advised to discontinue use of the medication and consult a physician.
This product is sterile when packaged. To prevent contamination, care should be taken to avoid touching dropper tip to eyelids or to any other surface. The use of this dispenser by more than one person may spread infection. Keep bottle tightly closed when not in use. Protect from light. Sulfonamide solutions darken on prolonged standing and exposure to heat and light. Do not use if solution has darkened. Yellowing does not affect activity. Keep out of the reach of children.
Laboratory Tests
Eyelid cultures and tests to determine the susceptibility of organisms to sulfacetamide may be indicated if signs and symptoms persist or recur in spite of the recommended course of treatment with Sulfacetamide Sodium and Prednisolone Sodium Phosphate Ophthalmic Solution.
Drug Interactions
Sulfacetamide Sodium and Prednisolone Sodium Phosphate Ophthalmic Solution is incompatible with silver preparations. Local anesthetics related to p-aminobenzoic acid may antagonize the action of the sulfonamides.
Carcinogenesis, Mutagenesis, and Impairment of Fertility
Prednisolone has been reported to be noncarcinogenic. Long-term animal studies for carcinogenic potential have not been performed with prednisolone or sulfacetamide.
One author detected chromosomal nondisjunction in the yeast Saccharomyces cerevisiae following application of sulfacetamide sodium. The significance of this finding to the topical ophthalmic use of sulfacetamide sodium in the human is unknown.
Mutagenic studies with prednisolone have been negative. Studies on reproduction and fertility have not been performed with sulfacetamide. A long-term chronic toxicity study in dogs showed that high oral doses of prednisolone prevented estrus. A decrease in fertility was seen in male and female rats that were mated following oral dosing with another glucocorticosteroid.
Pregnancy
Teratogenic Effects
Prednisolone has been shown to be teratogenic in rabbits, hamsters, and mice. In mice, prednisolone has been shown to be teratogenic when given in doses 1 to 10 times the human ocular dose. Dexamethasone, hydrocortisone and prednisolone were ocularly applied to both eyes of pregnant mice five times per day on days 10 through 13 of gestation. A significant increase in the incidence of cleft palate was observed in the fetuses of the treated mice. There are no adequate, well-controlled studies in pregnant women dosed with corticosteroids.
Kernicterus may be precipitated in infants by sulfonamides given systemically during the third trimester of pregnancy. It is not known whether sulfacetamide sodium can cause fetal harm when administered to a pregnant woman or whether it can affect reproductive capacity.
Sulfacetamide Sodium and Prednisolone Sodium Phosphate Ophthalmic Solution should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
Nursing Mothers
It is not known whether topical administration of corticosteroids could result in sufficient systemic absorption to produce detectable quantities in human milk. Systemically administered corticosteroids appear in human milk and could suppress growth, interfere with endogenous corticosteroid production, or cause other untoward effects. Systemically administered sulfonamides are capable of producing kernicterus in infants of lactating women. Because of the potential for serious adverse reactions in nursing infants from sulfacetamide sodium and prednisolone sodium phosphate ophthalmic solution, a decision should be made whether to discontinue nursing or to discontinue the medication.
-
ADVERSE REACTIONS
Adverse reactions have occurred with corticosteroid/anti-infective combination drugs which can be attributed to the corticosteroid component, the anti-infective component, or the combination. Exact incidence figures are not available since no denominator of treated patients is available.
Reactions occurring most often from the presence of the anti-infective ingredient are allergic sensitizations. Fatalities have occurred, although rarely, due to severe reactions to sulfonamides including Stevens-Johnson syndrome, toxic epidermal necrolysis, fulminant hepatic necrosis, agranulocytosis, aplastic anemia, and other blood dyscrasias (see WARNINGS).
Sulfacetamide sodium may cause local irritation.
The reactions due to the corticosteroid component in decreasing order of frequency are: elevation of intraocular pressure (IOP) with possible development of glaucoma, and infrequent optic nerve damage; posterior subcapsular cataract formation; and delayed wound healing.
Although systemic effects are extremely uncommon, there have been rare occurrences of systemic hypercorticoidism after use of topical corticosteroids.
Corticosteroid-containing preparations can also cause acute anterior uveitis or perforation of the globe. Mydriasis, loss of accommodation and ptosis have occasionally been reported following local use of corticosteroids.
Secondary Infection
The development of secondary infection has occurred after use of combinations containing corticosteroids and antimicrobials. Fungal and viral infections of the cornea are particularly prone to develop coincidentally with long-term applications of corticosteroid. The possibility of fungal invasion must be considered in any persistent corneal ulceration where corticosteroid treatment has been used.
Secondary bacterial ocular infection following suppression of host responses also occurs.
To report SUSPECTED ADVERSE REACTIONS, contact Bausch + Lomb, a division of Valeant Pharmaceuticals North America LLC, at 1-800-321-4576 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
-
DOSAGE AND ADMINISTRATION
Instill two drops of Sulfacetamide Sodium and Prednisolone Sodium Phosphate Ophthalmic Solution topically in the eye(s) every four hours. Not more than 20 mL should be prescribed initially. If signs and symptoms fail to improve after two days, patients should be re-evaluated (see PRECAUTIONS).
Care should be taken not to discontinue therapy prematurely. In chronic conditions, withdrawal of treatment should be carried out by gradually decreasing the frequency of application.
FOR OPHTHALMIC USE ONLY
-
HOW SUPPLIED
Sulfacetamide Sodium and Prednisolone Sodium Phosphate Ophthalmic Solution 10%/0.23% (prednisolone phosphate) is supplied in a plastic bottle with a white cap and controlled drop tip in the following sizes:
5 mL bottle – NDC68071-1650-5
DO NOT USE IF IMPRINTED NECKBAND IS NOT INTACT.
Storage:
Store between 15°–25°C (59°–77°F). KEEP FROM FREEZING. PROTECT FROM LIGHT. KEEP TIGHTLY CLOSED. Sulfonamide solutions darken on prolonged standing and exposure to heat and light. Do not use if solution has darkened. Yellowing does not affect activity.
KEEP OUT OF REACH OF CHILDREN.
Revised: July 2016
Bausch + Lomb, a division of Valeant Pharmaceuticals North America LLC
Bridgewater, NJ 08807 USA
©Bausch & Lomb Incorporated9118004 (Folded)
9118104 (Flat) - PACKAGE/LABEL PRINCIPAL DISPLAY PANEL
-
INGREDIENTS AND APPEARANCE
SULFACETAMIDE SODIUM AND PREDNISOLONE SODIUM PHOSPHATE
sulfacetamide sodium and prednisolone sodium phosphate solution/ dropsProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 68071-1650(NDC:24208-317) Route of Administration OPHTHALMIC Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength SULFACETAMIDE SODIUM (UNII: 4NRT660KJQ) (SULFACETAMIDE - UNII:4965G3J0F5) SULFACETAMIDE SODIUM 100 mg in 1 mL PREDNISOLONE SODIUM PHOSPHATE (UNII: IV021NXA9J) (PREDNISOLONE - UNII:9PHQ9Y1OLM) PREDNISOLONE 21-PHOSPHATE 2.3 mg in 1 mL Inactive Ingredients Ingredient Name Strength POLOXAMER 407 (UNII: TUF2IVW3M2) BORIC ACID (UNII: R57ZHV85D4) EDETATE DISODIUM (UNII: 7FLD91C86K) WATER (UNII: 059QF0KO0R) HYDROCHLORIC ACID (UNII: QTT17582CB) SODIUM HYDROXIDE (UNII: 55X04QC32I) THIMEROSAL (UNII: 2225PI3MOV) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 68071-1650-5 5 mL in 1 BOX; Type 0: Not a Combination Product 03/05/2019 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA074449 12/29/1995 Labeler - NuCare Pharmaceuticals,Inc. (010632300) Establishment Name Address ID/FEI Business Operations NuCare Pharmaceuticals,Inc. 010632300 relabel(68071-1650)
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.