Zinc Chloride by Somerset Therapeutics, LLC / Somerset Therapeutics Private Limited ZINC CHLORIDE injection
Zinc Chloride by
Drug Labeling and Warnings
Zinc Chloride by is a Prescription medication manufactured, distributed, or labeled by Somerset Therapeutics, LLC, Somerset Therapeutics Private Limited. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
DESCRIPTION
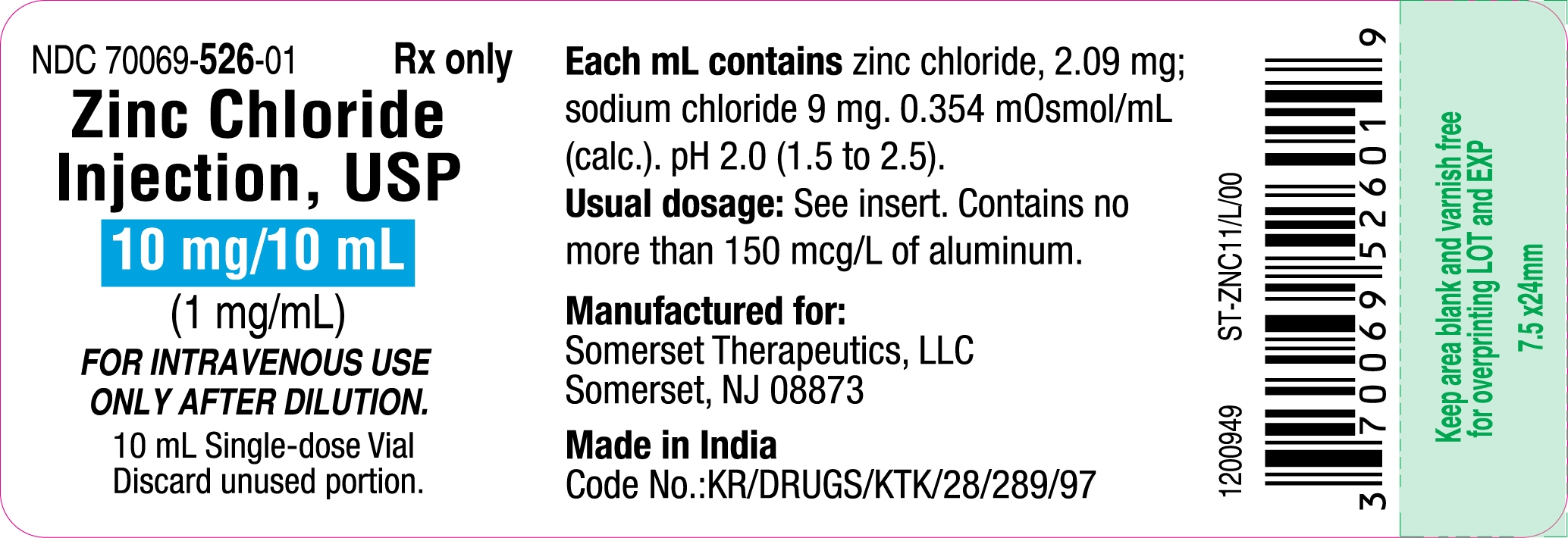
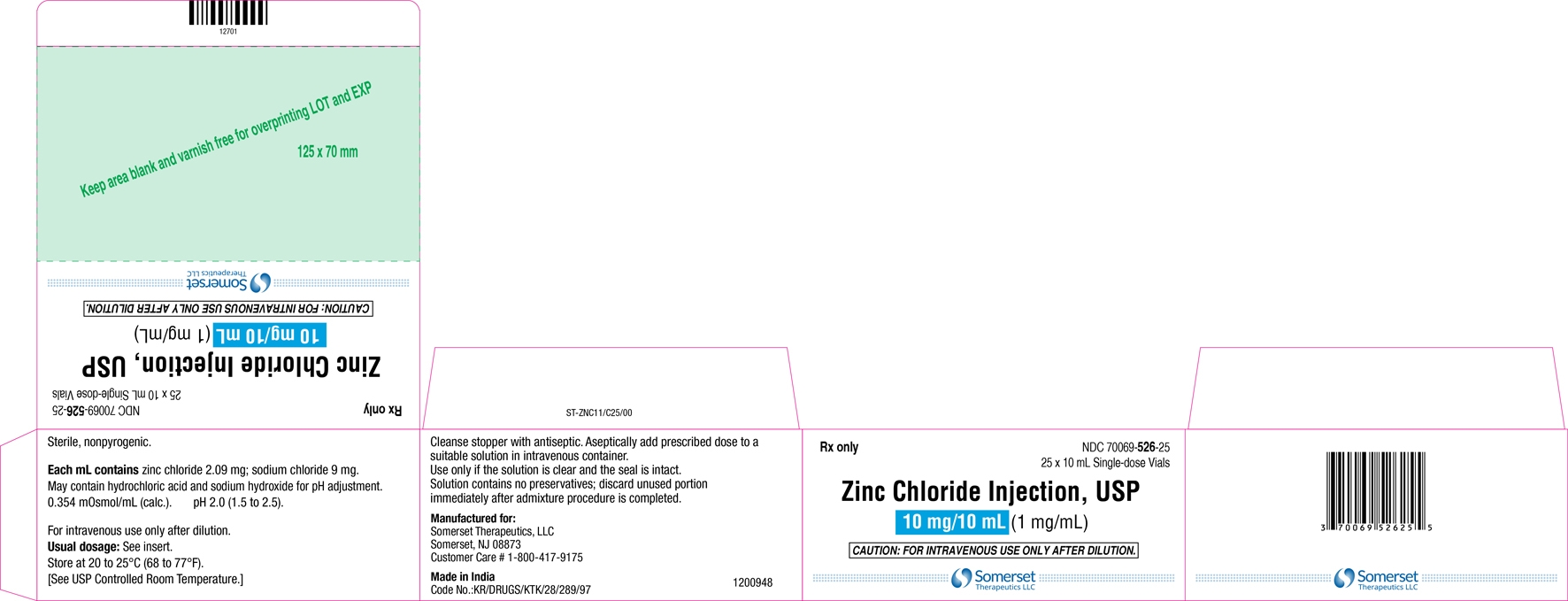
Zinc chloride injection, USP is a sterile, nonpyrogenic solution intended for use as an additive to intravenous solutions for total parenteral nutrition. Each mL of solution contains 2.09 mg zinc chloride and 9 mg sodium chloride. The solution contains no bacteriostat, antimicrobial agent or added buffer. The pH is 2.0 (1.5 to 2.5); product may contain hydrochloric acid and sodium hydroxide for pH adjustment. The osmolarity is 0.354 mOsmoL/mL (calc.).
Zinc Chloride, USP is chemically designated ZnCl2, a white crystalline compound freely soluble in water.
Sodium Chloride, USP is chemically designated NaCl, a white crystalline compound freely soluble in water.
The semi-rigid vial is fabricated from a specially formulated polyolefin. It is a copolymer of ethylene and propylene. The safety of the plastic has been confirmed by tests in animals according to USP biological standards for plastic containers. The small amount of water vapor that can pass through the plastic container wall will not significantly alter the drug concentration.
-
CLINICAL PHARMACOLOGY
Zinc is an essential nutritional requirement and serves as a cofactor for more than 70 different enzymes including carbonic anhydrase, alkaline phosphatase, lactic dehydrogenase, and both RNA and DNA polymerase. Zinc facilitates wound healing, helps maintain normal growth rates, normal skin hydration, and the senses of taste and smell.
Zinc resides in muscle, bone, skin, kidney, liver, pancreas, retina, prostate and particularly in the red and white blood cells. Zinc binds to plasma albumin, α2-macroglobulin, and some plasma amino acids including histidine, cysteine, threonine, glycine, and asparagine. Ingested zinc is excreted mainly in the stool (approximately 90%), and to a lesser extent in the urine and in perspiration.
Providing zinc helps prevent development of deficiency symptoms such as: Parakeratosis, hypogeusia, anorexia, dysosmia, geophagia, hypogonadism, growth retardation and hepatosplenomegaly.
The initial manifestations of hypozincemia in total parenteral nutrition are diarrhea, apathy and depression. At plasma levels below 20 mcg zinc/100 mL dermatitis followed by alopecia has been reported for total parenteral nutrition patients. Normal zinc plasma levels are 100 ± 12 mcg/100 mL.
- INDICATIONS AND USAGE
- CONTRAINDICATIONS
-
WARNINGS
Direct intramuscular or intravenous injection of zinc chloride injection is contraindicated as the acidic pH of the solution (2) may cause considerable tissue irritation.
Severe kidney disease may make it necessary to reduce or omit chromium and zinc doses because these elements are primarily eliminated in the urine.
Copper Deficiency
Several post-marketing cases have reported that zinc products taken over extended periods of time (i.e., months to years) may result in copper deficiency. The cases reported the following complications of copper deficiency: anemia, granulocytopenia, leukopenia, neutropenia, pancytopenia, thrombocytopenia, and myeloneuropathy.
If a patient develops signs and/or symptoms of copper deficiency during treatment with zinc chloride, interrupt zinc treatment and check zinc and copper levels. Consider supplemental copper administration to treat copper deficiency and monitor zinc levels.
Aluminum Toxicity
This product contains aluminum that may be toxic. Aluminum may reach toxic levels with prolonged parenteral administration if kidney function is impaired. Premature neonates are particularly at risk because their kidneys are immature, and they require large amounts of calcium and phosphate solutions, which contain aluminum.
Research indicates that patients with impaired kidney function, including premature neonates, who receive parenteral levels of aluminum at greater than 4 to 5 mcg/kg/day accumulate aluminum at levels associated with central nervous system and bone toxicity. Tissue loading may occur at even lower rates of administration.
-
PRECAUTIONS
Use only if the solution is clear and the seal is intact.
Zinc chloride injection should only be used in conjunction with a pharmacy directed admixture program using aseptic technique in a laminar flow environment; it should be used promptly and in a single operation without any repeated penetrations. Solution contains no preservatives; discard unused portion immediately after admixture procedure is completed.
Zinc should not be given undiluted by direct injection into a peripheral vein because of the likelihood of infusion phlebitis and the potential for increased excretory loss of zinc from a bolus injection.
Administration of zinc in the absence of copper may cause a decrease in serum copper levels.
Laboratory Tests
Periodic determinations of serum copper as well as zinc are suggested as a guideline for subsequent zinc administration.
Carcinogenesis, Mutagenesis, and Impairment of Fertility
Long-term animal studies to evaluate the carcinogenic potential of Zinc chloride injection have not been performed, nor have studies been done to assess mutagenesis or impairment of fertility.
Nursing Mothers
It is not known whether this drug is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when zinc chloride injection is administered to a nursing woman.
Pediatric Use
See DOSAGE and ADMINISTRATION section.
Pregnancy
Animal reproduction studies have not been conducted with zinc chloride. It is also not known whether zinc chloride can cause fetal harm when administered to a pregnant woman or can affect reproduction capacity. Zinc chloride should be given to a pregnant woman only if clearly needed.
Geriatric Use
An evaluation of current literature revealed no clinical experience identifying differences in response between elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
- ADVERSE REACTIONS
-
OVERDOSAGE
Single intravenous doses of 1 to 2 mg zinc/kg body weight have been given to adult leukemic patients without toxic manifestations. However, acute toxicity was reported in an adult when 10 mg zinc was infused over a period of one hour on each of four consecutive days. Profuse sweating, decreased level of consciousness, blurred vision, tachycardia (140/min), and marked hypothermia (94.2° F) on the fourth day were accompanied by a serum zinc concentration of 207 mcg/dl. Symptoms abated within three hours.
Hyperamylasemia may be a sign of impending zinc overdosage; patients receiving an inadvertent overdose (25 mg zinc/liter of total parenteral nutrition solution, equivalent to 50 to 70 mg zinc/day) developed hyperamylasemia (557 to 1850 Klein units; normal: 130 to 310).
Death resulted from an overdosage in which 1683 mg zinc was delivered intravenously over the course of 60 hours to a 72-year-old patient.
Symptoms of zinc toxicity included hypotension (80/40 mm Hg), pulmonary edema, diarrhea, vomiting, jaundice, and oliguria, with a serum zinc level of 4184 mcg/dl.
Calcium supplements may confer a protective effect against zinc toxicity.
-
DOSAGE AND ADMINISTRATION
Zinc chloride injection contains 1 mg zinc/mL and is administered intravenously only after dilution. The additive should be diluted prior to administration in a volume of fluid not less than 100 mL. For the metabolically stable adult receiving total parenteral nutrition, the suggested intravenous dosage is 2.5 to 4 mg zinc/day (2.5 to 4 mL/day). An additional 2 mg zinc/day (2 mL/day) is suggested for acute catabolic states. For the stable adult with fluid loss from the small bowel, an additional 12.2 mg zinc/liter of small bowel fluid lost (12.2 mL/liter of small bowel fluid lost), or an additional 17.1 mg zinc/kg of stool or ileostomy output (17.1 mL/kg of stool or ileostomy output) is recommended. Frequent monitoring of zinc blood levels is suggested for patients receiving more than the usual maintenance dosage level of zinc.
For full term infants and children up to 5 years of age, 100 mcg zinc/kg/day (0.1 mL/kg/day) is recommended. For premature infants (birth weight less than 1500 g) up to 3 kg in body weight, 300 mcg zinc/kg/day (0.3 mL/kg/day) is suggested.
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit. (See PRECAUTIONS.).
-
HOW SUPPLIED
Zinc chloride injection, USP is supplied in 10 mL single-dose Plastic Vials.
Unit of Sale
Concentration
Each
NDC: 70069-526-25
25 in a carton
10 mg/10 mL
(1 mg/mL)
NDC: 70069-526-01
10 mg single-dose vial
Store at 20 to 25°C (68 to 77°F). [See USP Controlled Room Temperature.]
- SPL UNCLASSIFIED SECTION
- PACKAGE LABEL.PRINCIPAL DISPLAY PANEL
-
INGREDIENTS AND APPEARANCE
ZINC CHLORIDE
zinc chloride injectionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 70069-526 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength ZINC CHLORIDE (UNII: 86Q357L16B) (ZINC CATION - UNII:13S1S8SF37) ZINC CATION 1 mg in 1 mL Inactive Ingredients Ingredient Name Strength SODIUM CHLORIDE (UNII: 451W47IQ8X) SODIUM HYDROXIDE (UNII: 55X04QC32I) HYDROCHLORIC ACID (UNII: QTT17582CB) WATER (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 70069-526-25 25 in 1 CARTON 10/16/2024 1 NDC: 70069-526-01 10 mL in 1 VIAL, PLASTIC; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA216152 10/16/2024 Labeler - Somerset Therapeutics, LLC (079947873) Registrant - Somerset Therapeutics, LLC (079947873) Establishment Name Address ID/FEI Business Operations Somerset Therapeutics Private Limited 677236695 ANALYSIS(70069-526) , LABEL(70069-526) , PACK(70069-526) , MANUFACTURE(70069-526)
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.