DULOXETINE capsule, delayed release pellets
Duloxetine by
Drug Labeling and Warnings
Duloxetine by is a Prescription medication manufactured, distributed, or labeled by Actavis Pharma, Inc.. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use DULOXETINE DELAYED-RELEASE CAPSULES safely and effectively. See full prescribing information for DULOXETINE DELAYED-RELEASE CAPSULES.
DULOXETINE delayed-release capsules, for oral use
Initial U.S. Approval: 2004RECENT MAJOR CHANGES
Warnings and Precautions (5.5) 10/2019
INDICATIONS AND USAGE
DOSAGE AND ADMINISTRATION
- Take duloxetine delayed-release capsules once daily, with or without food. Swallow duloxetine delayed-release capsules whole; do not crush or chew, do not open capsule. Take a missed dose as soon as it is remembered. Do not take two doses of duloxetine delayed-release capsules at the same time. (2)
Indication
Starting
DoseTarget
DoseMaximum
DoseMDD (2.1)
40 mg/day to
60 mg/day
Acute Treatment:
40 mg/day
(20 mg twice daily) to 60 mg/day (once daily or as 30 mgtwice daily); Maintenance Treatment:
60 mg/day120 mg/day
GAD (2.2)
Adults
60 mg/day
60 mg/day
(once daily)120 mg/day
DPNP (2.3)
60 mg/day
60 mg/day
(once daily)60 mg/day
FM (2.4)
30 mg/day
60 mg/day
(once daily)60 mg/day
Chronic Musculoskeletal Pain (2.5)
30 mg/day
60 mg/day
(once daily)60 mg/day
- Some patients may benefit from starting at 30 mg once daily (2)
- There is no evidence that doses greater than 60 mg/day confers additional benefit, while some adverse reactions were observed to be dose-dependent (2)
- Discontinuing duloxetine delayed-release capsules: Gradually reduce dosage to avoid discontinuation symptoms (2.7, 5.7)
- Hepatic Impairment: Avoid use in patients with chronic liver disease or cirrhosis (5.14)
- Renal Impairment: Avoid use in patients with severe renal impairment, GFR less than 30 mL/min (5.14)
DOSAGE FORMS AND STRENGTHS
20 mg, 30 mg, and 60 mg delayed-release capsules (3)
CONTRAINDICATIONS
- Serotonin Syndrome and MAOIs: Do not use MAOIs intended to treat psychiatric disorders with duloxetine delayed-release capsules or within 5 days of stopping treatment with duloxetine delayed-release capsules. Do not use duloxetine delayed-release capsules within 14 days of stopping an MAOI intended to treat psychiatric disorders. In addition, do not start duloxetine delayed-release capsules in a patient who is being treated with linezolid or intravenous methylene blue (4)
WARNINGS AND PRECAUTIONS
- Hepatotoxicity: Hepatic failure, sometimes fatal, has been reported in patients treated with duloxetine delayed-release capsules. Duloxetine delayed-release capsules should be discontinued in patients who develop jaundice or other evidence of clinically significant liver dysfunction and should not be resumed unless another cause can be established. Duloxetine delayed-release capsules should not be prescribed to patients with substantial alcohol use or evidence of chronic liver disease (5.2)
- Orthostatic Hypotension, Falls and Syncope: Cases have been reported with duloxetine delayed-release capsules therapy (5.3)
- Serotonin Syndrome: Increased risk when co-administered with other serotonergic agents (e.g., SSRIs, SNRIs, triptans), but also when taken alone. If it occurs, discontinue duloxetine delayed-release capsules and initiate supportive treatment (5.4)
- Increased Risk of Bleeding: Duloxetine delayed-release capsules may increase the risk of bleeding events. Concomitant use of NSAIDs, aspirin, other antiplatelet drugs, warfarin, and anticoagulants may increase this risk (5.5, 7.4, 8.1)
- Severe Skin Reactions: Severe skin reactions, including erythema multiforme and Stevens-Johnson Syndrome (SJS), can occur with duloxetine delayed-release capsules. Duloxetine delayed-release capsules should be discontinued at the first appearance of blisters, peeling rash, mucosal erosions, or any other sign of hypersensitivity if no other etiology can be identified. (5.6)
- Discontinuation: Taper dose when possible and monitor for discontinuation symptoms (5.7)
- Activation of mania or hypomania has occurred (5.8)
- Angle-Closure Glaucoma: Angle-closure glaucoma has occurred in patients with untreated anatomically narrow angles treated with antidepressants. (5.9)
- Seizures: Prescribe with care in patients with a history of seizure disorder (5.10)
- Blood Pressure: Monitor blood pressure prior to initiating treatment and periodically throughout treatment (5.11)
- Inhibitors of CYP1A2 or Thioridazine: Should not administer with duloxetine delayed-release capsules (5.12)
- Hyponatremia: Can occur in association with SIADH. Cases of hyponatremia have been reported (5.13)
- Glucose Control in Diabetes: In diabetic peripheral neuropathic pain patients, small increases in fasting blood glucose, and HbA1c have been observed (5.14)
- Conditions that Slow Gastric Emptying: Use cautiously in these patients (5.14)
ADVERSE REACTIONS
Most common adverse reactions (greater than or equal to 5% and at least twice the incidence of placebo patients): nausea, dry mouth, somnolence, constipation, decreased appetite, and hyperhidrosis (6.3).
To report SUSPECTED ADVERSE REACTIONS, contact Actavis at 1-800-432-8534 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
USE IN SPECIFIC POPULATIONS
- Pregnancy: Third trimester use may increase risk for symptoms of poor adaptation (respiratory distress, temperature instability, feeding difficulty, hypotonia, tremor, irritability) in the neonate (8.1)
Pediatric use information for patients ages 7 to 17 years is approved for Eli Lilly and Company, Inc.'s CYMBALTA® (duloxetine) delayed-release capsules. However, due to Eli Lilly and Company, Inc.'s marketing exclusivity rights, this drug product is not labeled with that pediatric information.
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide.
Revised: 11/2019
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
WARNING: SUICIDAL THOUGHTS AND BEHAVIORS
RECENT MAJOR CHANGES
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Dosage for Treatment of Major Depressive Disorder
2.2 Dosage for Treatment of Generalized Anxiety Disorder
2.3 Dosage for Treatment of Diabetic Peripheral Neuropathic Pain
2.4 Dosage for Treatment of Fibromyalgia
2.5 Dosage for Treatment of Chronic Musculoskeletal Pain
2.6 Dosing in Special Populations
2.7 Discontinuing Duloxetine Delayed-Release Capsules
2.8 Switching a Patient to or from a Monoamine Oxidase Inhibitor (MAOI) Intended to Treat Psychiatric Disorders
2.9 Use of Duloxetine Delayed-Release Capsules with Other MAOIs such as Linezolid or Methylene Blue
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Suicidal Thoughts and Behaviors in Children, Adolescents, and Young Adults
5.2 Hepatotoxicity
5.3 Orthostatic Hypotension, Falls and Syncope
5.4 Serotonin Syndrome
5.5 Increased Risk of Bleeding
5.6 Severe Skin Reactions
5.7 Discontinuation of Treatment with Duloxetine Delayed-Release Capsules
5.8 Activation of Mania/Hypomania
5.9 Angle-Closure Glaucoma
5.10 Seizures
5.11 Effect on Blood Pressure
5.12 Clinically Important Drug Interactions
5.13 Hyponatremia
5.14 Use in Patients with Concomitant Illness
5.15 Urinary Hesitation and Retention
6 ADVERSE REACTIONS
6.1 Clinical Studies Experience
6.2 Postmarketing Experience
7 DRUG INTERACTIONS
7.1 Inhibitors of CYP1A2
7.2 Inhibitors of CYP2D6
7.3 Dual Inhibition of CYP1A2 and CYP2D6
7.4 Drugs that Interfere with Hemostasis (e.g., NSAIDs, Aspirin, and Warfarin)
7.5 Lorazepam
7.6 Temazepam
7.7 Drugs that Affect Gastric Acidity
7.8 Drugs Metabolized by CYP1A2
7.9 Drugs Metabolized by CYP2D6
7.10 Drugs Metabolized by CYP2C9
7.11 Drugs Metabolized by CYP3A
7.12 Drugs Metabolized by CYP2C19
7.13 Monoamine Oxidase Inhibitors (MAOIs)
7.14 Serotonergic Drugs
7.15 Alcohol
7.16 CNS Drugs
7.17 Drugs Highly Bound to Plasma Protein
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.4 Pediatric Use
8.5 Geriatric Use
8.6 Gender
8.7 Smoking Status
8.8 Race
8.9 Hepatic Impairment
8.10 Severe Renal Impairment
9 DRUG ABUSE AND DEPENDENCE
9.2 Abuse
9.3 Dependence
10 OVERDOSAGE
10.1 Signs and Symptoms
10.2 Management of Overdose
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis and Mutagenesis and Impairment of Fertility
14 CLINICAL STUDIES
14.1 Major Depressive Disorder
14.2 Generalized Anxiety Disorder
14.3 Diabetic Peripheral Neuropathic Pain
14.4 Fibromyalgia
14.5 Chronic Musculoskeletal Pain
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 How Supplied
16.2 Storage and Handling
17 PATIENT COUNSELING INFORMATION
- * Sections or subsections omitted from the full prescribing information are not listed.
-
BOXED WARNING
(What is this?)
WARNING: SUICIDAL THOUGHTS AND BEHAVIORS
Antidepressants increased the risk of suicidal thoughts and behavior in children, adolescents, and young adults in short-term studies. These studies did not show an increase in the risk of suicidal thoughts and behavior with antidepressant use in patients over age 24; there was a reduction in risk with antidepressant use in patients aged 65 and older [see Warnings and Precautions (5.1)].
In patients of all ages who are started on antidepressant therapy, monitor closely for worsening, and for emergence of suicidal thoughts and behaviors. Advise families and caregivers of the need for close observation and communication with the prescriber [see Warnings and Precautions (5.1)].
-
1 INDICATIONS AND USAGE
Duloxetine delayed-release capsules are indicated for the treatment of:
- Major Depressive Disorder [see Clinical Studies (14.1)]
- Generalized Anxiety Disorder [see Clinical Studies (14.2)]
- Diabetic Peripheral Neuropathy [see Clinical Studies (14.3)]
- Fibromyalgia [see Clinical Studies (14.4)]
- Chronic Musculoskeletal Pain [see Clinical Studies (14.5)]
-
2 DOSAGE AND ADMINISTRATION
Swallow duloxetine delayed-release capsules whole. Do not chew or crush. Do not open the capsule and sprinkle its contents on food or mix with liquids. All of these might affect the enteric coating. Duloxetine delayed-release capsules can be given without regard to meals. If a dose of duloxetine delayed-release capsules is missed, take the missed dose as soon as it is remembered. If it is almost time for the next dose, skip the missed dose and take the next dose at the regular time. Do not take two doses of duloxetine delayed-release capsules at the same time.
2.1 Dosage for Treatment of Major Depressive Disorder
Administer duloxetine delayed-release capsules at a total dose of 40 mg/day (given as 20 mg twice daily) to 60 mg/day (given either once daily or as 30 mg twice daily). For some patients, it may be desirable to start at 30 mg once daily for 1 week, to allow patients to adjust to the medication before increasing to 60 mg once daily. While a 120 mg/day dose was shown to be effective, there is no evidence that doses greater than 60 mg/day confer any additional benefits. The safety of doses above 120 mg/day has not been adequately evaluated. Periodically reassess to determine the need for maintenance treatment and the appropriate dose for such treatment [see Clinical Studies (14.1)].
2.2 Dosage for Treatment of Generalized Anxiety Disorder
Adults - For most patients, initiate duloxetine delayed-release capsules 60 mg once daily. For some patients, it may be desirable to start at 30 mg once daily for 1 week, to allow patients to adjust to the medication before increasing to 60 mg once daily. While a 120 mg once daily dose was shown to be effective, there is no evidence that doses greater than 60 mg/day confer additional benefit. Nevertheless, if a decision is made to increase the dose beyond 60 mg once daily, increase dose in increments of 30 mg once daily. The safety of doses above 120 mg once daily has not been adequately evaluated. Periodically reassess to determine the continued need for maintenance treatment and the appropriate dose for such treatment [see Clinical Studies (14.2)].
Pediatric use information for patients ages 7 to 17 years is approved for Eli Lilly and Company, Inc.'s CYMBALTA® (duloxetine) delayed-release capsules. However, due to Eli Lilly and Company, Inc.'s marketing exclusivity rights, this drug product is not labeled with that pediatric information.
2.3 Dosage for Treatment of Diabetic Peripheral Neuropathic Pain
Administer duloxetine delayed-release capsules 60 mg once daily. There is no evidence that doses higher than 60 mg confer additional significant benefit and the higher dose is clearly less well tolerated [see Clinical Studies (14.3)]. For patients for whom tolerability is a concern, a lower starting dose may be considered.
Since diabetes is frequently complicated by renal disease, consider a lower starting dose and gradual increase in dose for patients with renal impairment [see Dosage and Administration (2.6), Use in Specific Populations (8.10), and Clinical Pharmacology (12.3)].
2.4 Dosage for Treatment of Fibromyalgia
Administer duloxetine delayed-release capsules 60 mg once daily. Begin treatment at 30 mg once daily for 1 week, to allow patients to adjust to the medication before increasing to 60 mg once daily. Some patients may respond to the starting dose. There is no evidence that doses greater than 60 mg/day confer additional benefit, even in patients who do not respond to a 60 mg dose, and higher doses are associated with a higher rate of adverse reactions [see Clinical Studies (14.4)].
2.5 Dosage for Treatment of Chronic Musculoskeletal Pain
Administer duloxetine delayed-release capsules 60 mg once daily. Begin treatment at 30 mg for one week, to allow patients to adjust to the medication before increasing to 60 mg once daily. There is no evidence that higher doses confer additional benefit, even in patients who do not respond to a 60 mg dose, and higher doses are associated with a higher rate of adverse reactions [see Clinical Studies (14.5)].
2.6 Dosing in Special Populations
Hepatic Impairment - Avoid use in patients with chronic liver disease or cirrhosis [see Warnings and Precautions (5.14) and Use in Specific Populations (8.9)].
Severe Renal Impairment - Avoid use in patients with severe renal impairment, GFR less than 30 mL/min [see Warnings and Precautions (5.14) and Use in Specific Populations (8.10)].
2.7 Discontinuing Duloxetine Delayed-Release Capsules
Adverse reactions after discontinuation of duloxetine delayed-release capsules, after abrupt or tapered discontinuation, include: dizziness, headache, nausea, diarrhea, paresthesia, irritability, vomiting, insomnia, anxiety, hyperhidrosis, and fatigue. A gradual reduction in dosage rather than abrupt cessation is recommended whenever possible [see Warnings and Precautions (5.7)].
2.8 Switching a Patient to or from a Monoamine Oxidase Inhibitor (MAOI) Intended to Treat Psychiatric Disorders
At least 14 days should elapse between discontinuation of an MAOI intended to treat psychiatric disorders and initiation of therapy with duloxetine delayed-release capsules. Conversely, at least 5 days should be allowed after stopping duloxetine delayed-release capsules before starting an MAOI intended to treat psychiatric disorders [see Contraindications (4)].
2.9 Use of Duloxetine Delayed-Release Capsules with Other MAOIs such as Linezolid or Methylene Blue
Do not start duloxetine delayed-release capsules in a patient who is being treated with linezolid or intravenous methylene blue because there is an increased risk of serotonin syndrome. In a patient who requires more urgent treatment of a psychiatric condition, other interventions, including hospitalization, should be considered [see Contraindications (4)].
In some cases, a patient already receiving duloxetine delayed-release capsules therapy may require urgent treatment with linezolid or intravenous methylene blue. If acceptable alternatives to linezolid or intravenous methylene blue treatment are not available and the potential benefits of linezolid or intravenous methylene blue treatment are judged to outweigh the risks of serotonin syndrome in a particular patient, duloxetine delayed-release capsules should be stopped promptly, and linezolid or intravenous methylene blue can be administered. The patient should be monitored for symptoms of serotonin syndrome for 5 days or until 24 hours after the last dose of linezolid or intravenous methylene blue, whichever comes first. Therapy with duloxetine delayed-release capsules may be resumed 24 hours after the last dose of linezolid or intravenous methylene blue [see Warnings and Precautions (5.4)].
The risk of administering methylene blue by non-intravenous routes (such as oral tablets or by local injection) or in intravenous doses much lower than 1 mg/kg with duloxetine delayed-release capsules is unclear. The clinician should, nevertheless, be aware of the possibility of emergent symptoms of serotonin syndrome with such use [see Warnings and Precautions (5.4)].
- 3 DOSAGE FORMS AND STRENGTHS
-
4 CONTRAINDICATIONS
Monoamine Oxidase Inhibitors (MAOIs) - The use of MAOIs intended to treat psychiatric disorders with duloxetine delayed-release capsules or within 5 days of stopping treatment with duloxetine delayed-release capsules are contraindicated because of an increased risk of serotonin syndrome. The use of duloxetine delayed-release capsules within 14 days of stopping an MAOI intended to treat psychiatric disorders is also contraindicated [see Dosage and Administration (2.8) and Warnings and Precautions (5.4)].
Starting duloxetine delayed-release capsules in a patient who is being treated with MAOIs such as linezolid or intravenous methylene blue is also contraindicated because of an increased risk of serotonin syndrome [see Dosage and Administration (2.9) and Warnings and Precautions (5.4)].
-
5 WARNINGS AND PRECAUTIONS
5.1 Suicidal Thoughts and Behaviors in Children, Adolescents, and Young Adults
Patients with major depressive disorder (MDD), both adult and pediatric, may experience worsening of their depression and/or the emergence of suicidal ideation and behavior (suicidality) or unusual changes in behavior, whether or not they are taking antidepressant medications, and this risk may persist until significant remission occurs. Suicide is a known risk of depression and certain other psychiatric disorders, and these disorders themselves are the strongest predictors of suicide. There has been a long-standing concern, however, that antidepressants may have a role in inducing worsening of depression and the emergence of suicidality in certain patients during the early phases of treatment.
Pooled analyses of short-term placebo-controlled trials of antidepressant drugs (SSRIs and others) showed that these drugs increase the risk of suicidal thinking and behavior (suicidality) in children, adolescents, and young adults (ages 18 to 24) with major depressive disorder (MDD) and other psychiatric disorders. Short-term studies did not show an increase in the risk of suicidality with antidepressants compared to placebo in adults beyond age 24; there was a reduction with antidepressants compared to placebo in adults aged 65 and older.
The pooled analyses of placebo-controlled trials in children and adolescents with MDD, obsessive compulsive disorder (OCD), or other psychiatric disorders included a total of 24 short-term trials of 9 antidepressant drugs in over 4400 patients. The pooled analyses of placebo-controlled trials in adults with MDD or other psychiatric disorders included a total of 295 short-term trials (median duration of 2 months) of 11 antidepressant drugs in over 77,000 patients. There was considerable variation in risk of suicidality among drugs, but a tendency toward an increase in the younger patients for almost all drugs studied. There were differences in absolute risk of suicidality across the different indications, with the highest incidence in MDD. The risk of differences (drug vs placebo), however, were relatively stable within age strata and across indications. These risk differences (drug-placebo difference in the number of cases of suicidality per 1000 patients treated) are provided in Table 1.
Table 1 Age Range
Drug-Placebo Difference in Number of Cases of Suicidality per 1000 Patients Treated
Increases Compared to Placebo
<18
14 additional cases
18 to 24
5 additional cases
Decreases Compared to Placebo
25 to 64
1 fewer case
≥65
6 fewer cases
No suicides occurred in any of the pediatric trials. There were suicides in the adult trials, but the number was not sufficient to reach any conclusion about drug effect on suicide.
It is unknown whether the suicidality risk extends to longer-term use, i.e., beyond several months. However, there is substantial evidence from placebo-controlled maintenance trials in adults with depression that the use of antidepressants can delay the recurrence of depression.
All patients being treated with antidepressants for any indication should be monitored appropriately and observed closely for clinical worsening, suicidality, and unusual changes in behavior, especially during the initial few months of a course of drug therapy, or at times of dose changes, either increases or decreases.
The following symptoms, anxiety, agitation, panic attacks, insomnia, irritability, hostility, aggressiveness, impulsivity, akathisia (psychomotor restlessness), hypomania, and mania, have been reported in adult and pediatric patients being treated with antidepressants for major depressive disorder as well as for other indications, both psychiatric and nonpsychiatric. Although a causal link between the emergence of such symptoms and either the worsening of depression and/or the emergence of suicidal impulses has not been established, there is concern that such symptoms may represent precursors to emerging suicidality.
Consideration should be given to changing the therapeutic regimen, including possibly discontinuing the medication, in patients whose depression is persistently worse, or who are experiencing emergent suicidality or symptoms that might be precursors to worsening depression or suicidality, especially if these symptoms are severe, abrupt in onset, or were not part of the patient’s presenting symptoms.
If the decision has been made to discontinue treatment, medication should be tapered, as rapidly as is feasible, but with recognition that discontinuation can be associated with certain symptoms [see Dosage and Administration (2.7) and Warnings and Precautions (5.7) for descriptions of the risks of discontinuation of duloxetine delayed-release capsules].
Families and caregivers of patients being treated with antidepressants for major depressive disorder or other indications, both psychiatric and nonpsychiatric, should be alerted about the need to monitor patients for the emergence of agitation, irritability, unusual changes in behavior, and the other symptoms described above, as well as the emergence of suicidality, and to report such symptoms immediately to health care providers. Such monitoring should include daily observation by families and caregivers. Prescriptions for duloxetine delayed-release capsulesshould be written for the smallest quantity of capsules consistent with good patient management, in order to reduce the risk of overdose.
Screening Patients for Bipolar Disorder - A major depressive episode may be the initial presentation of bipolar disorder. It is generally believed (though not established in controlled trials) that treating such an episode with an antidepressant alone may increase the likelihood of precipitation of a mixed/manic episode in patients at risk for bipolar disorder. Whether any of the symptoms described above represent such a conversion is unknown. However, prior to initiating treatment with an antidepressant, patients with depressive symptoms should be adequately screened to determine if they are at risk for bipolar disorder; such screening should include a detailed psychiatric history, including a family history of suicide, bipolar disorder, and depression. It should be noted that duloxetine delayed-release capsules are not approved for use in treating bipolar depression.
5.2 Hepatotoxicity
There have been reports of hepatic failure, sometimes fatal, in patients treated with duloxetine delayed-release capsules. These cases have presented as hepatitis with abdominal pain, hepatomegaly, and elevation of transaminase levels to more than twenty times the upper limit of normal with or without jaundice, reflecting a mixed or hepatocellular pattern of liver injury. Duloxetine delayed-release capsules should be discontinued in patients who develop jaundice or other evidence of clinically significant liver dysfunction and should not be resumed unless another cause can be established.
Cases of cholestatic jaundice with minimal elevation of transaminase levels have also been reported. Other postmarketing reports indicate that elevated transaminases, bilirubin, and alkaline phosphatase have occurred in patients with chronic liver disease or cirrhosis.
Duloxetine delayed-release capsules increased the risk of elevation of serum transaminase levels in development program clinical trials. Liver transaminase elevations resulted in the discontinuation of 0.3% (92/34,756) of duloxetine delayed-release capsule-treated patients. In most patients, the median time to detection of the transaminase elevation was about two months. In adult placebo-controlled trials in any indication, for patients with normal and abnormal baseline ALT values, elevation of ALT greater than 3 times the upper limit of normal occurred in 1.25% (144/11,496) of duloxetine delayed-release capsule-treated patients compared to 0.45% (39/8716) of placebo-treated patients. In adult placebo-controlled studies using a fixed dose design, there was evidence of a dose response relationship for ALT and AST elevation of greater than 3 times the upper limit of normal and greater than 5 times the upper limit of normal, respectively.
Because it is possible that duloxetine delayed-release capsules and alcohol may interact to cause liver injury or that duloxetine delayed-release capsules may aggravate pre-existing liver disease, duloxetine delayed-release capsules should not be prescribed to patients with substantial alcohol use or evidence of chronic liver disease.
5.3 Orthostatic Hypotension, Falls and Syncope
Orthostatic hypotension, falls and syncope have been reported with therapeutic doses of duloxetine delayed-release capsules. Syncope and orthostatic hypotension tend to occur within the first week of therapy but can occur at any time during duloxetine delayed-release capsules treatment, particularly after dose increases. The risk of falling appears to be related to the degree of orthostatic decrease in blood pressure as well as other factors that may increase the underlying risk of falls.
In an analysis of patients from all placebo-controlled trials, patients treated with duloxetine delayed-release capsules reported a higher rate of falls compared to patients treated with placebo. Risk appears to be related to the presence of orthostatic decrease in blood pressure. The risk of blood pressure decreases may be greater in patients taking concomitant medications that induce orthostatic hypotension (such as antihypertensives) or are potent CYP1A2 inhibitors [seeWarnings and Precautions (5.12) and Drug Interactions (7.1)] and in patients taking duloxetine delayed-release capsules at doses above 60 mg daily. Consideration should be given to dose reduction or discontinuation of duloxetine delayed-release capsules in patients who experience symptomatic orthostatic hypotension, falls and/or syncope during duloxetine delayed-release capsules therapy.
Risk of falling also appeared to be proportional to a patient’s underlying risk for falls and appeared to increase steadily with age. As elderly patients tend to have a higher underlying risk for falls due to a higher prevalence of risk factors such as use of multiple medications, medical comorbidities and gait disturbances, the impact of increasing age by itself is unclear. Falls with serious consequences including bone fractures and hospitalizations have been reported [see Adverse Reactions (6.10) and Patient Counseling Information (17)].
5.4 Serotonin Syndrome
The development of a potentially life-threatening serotonin syndrome has been reported with SNRIs and SSRIs, including duloxetine delayed-release capsules, alone but particularly with concomitant use of other serotonergic drugs (including triptans, tricyclic antidepressants, fentanyl, lithium, tramadol, tryptophan, buspirone, amphetamines, and St. John’s Wort) and with drugs that impair metabolism of serotonin (in particular, MAOIs, both those intended to treat psychiatric disorders and also others, such as linezolid and intravenous methylene blue).
Serotonin syndrome symptoms may include mental status changes (e.g., agitation, hallucinations, delirium, and coma), autonomic instability (e.g., tachycardia, labile blood pressure, dizziness, diaphoresis, flushing, hyperthermia), neuromuscular symptoms (e.g., tremor, rigidity, myoclonus, hyperreflexia, incoordination), seizures, and/or gastrointestinal symptoms (e.g., nausea, vomiting, diarrhea). Patients should be monitored for the emergence of serotonin syndrome.
The concomitant use of duloxetine delayed-release capsules with MAOIs intended to treat psychiatric disorders is contraindicated. Duloxetine delayed-release capsules should also not be started in a patient who is being treated with MAOIs such as linezolid or intravenous methylene blue. All reports with methylene blue that provided information on the route of administration involved intravenous administration in the dose range of
1 mg/kg to 8 mg/kg. No reports involved the administration of methylene blue by other routes (such as oral tablets or local tissue injection) or at lower doses. There may be circumstances when it is necessary to initiate treatment with an MAOI such as linezolid or intravenous methylene blue in a patient taking duloxetine delayed-release capsules. Duloxetine delayed-release capsules should be discontinued before initiating treatment with the MAOI [see Dosage and Administration (2.8, 2.9), and Contraindications (4)].If concomitant use of duloxetine delayed-release capsules with other serotonergic drugs including triptans, tricyclic antidepressants, fentanyl, lithium, tramadol, buspirone, tryptophan, amphetamines, and St. John’s Wort is clinically warranted, patients should be made aware of a potential increased risk for serotonin syndrome, particularly during treatment initiation and dose increases. Treatment with duloxetine delayed-release capsules and any concomitant serotonergic agents, should be discontinued immediately if the above events occur and supportive symptomatic treatment should be initiated.
5.5 Increased Risk of Bleeding
Drugs that interfere with serotonin reuptake inhibition, including duloxetine delayed-release capsules, may increase the risk of bleeding events. Case reports and epidemiological studies (case-control and cohort design) have demonstrated an association between use of drugs that interfere with serotonin reuptake and the occurrence of gastrointestinal bleeding. A post-marketing study showed a higher incidence of postpartum hemorrhage in mothers taking duloxetine. Other bleeding events related to SSRI and SNRI use have ranged from ecchymoses, hematomas, epistaxis, and petechiae to life-threatening hemorrhages. Concomitant use of aspirin, nonsteroidal anti-inflammatory drugs (NSAIDs), warfarin, and other anti-coagulants may add to this risk.
Inform patients about the risk of bleeding associated with the concomitant use of duloxetine delayed-release capsules and NSAIDs, aspirin, or other drugs that affect coagulation [see Drug Interactions (7.4)].
5.6 Severe Skin Reactions
Severe skin reactions, including erythema multiforme and Stevens-Johnson Syndrome (SJS), can occur with duloxetine delayed-release capsules. The reporting rate of SJS associated with duloxetine delayed-release capsules use exceeds the general population background incidence rate for this serious skin reaction (1 to 2 cases per million person years). The reporting rate is generally accepted to be an underestimate due to underreporting.
Duloxetine delayed-release capsules should be discontinued at the first appearance of blisters, peeling rash, mucosal erosions, or any other sign of hypersensitivity if no other etiology can be identified.
5.7 Discontinuation of Treatment with Duloxetine Delayed-Release Capsules
Discontinuation symptoms have been systematically evaluated in patients taking duloxetine delayed-release capsules. Following abrupt or tapered discontinuation in adult placebo-controlled clinical trials, the following symptoms occurred at 1% or greater and at a significantly higher rate in duloxetine delayed-release capsule-treated patients compared to those discontinuing from placebo: dizziness, headache, nausea, diarrhea, paresthesia, irritability, vomiting, insomnia, anxiety, hyperhidrosis, and fatigue.
During marketing of other SSRIs and SNRIs (serotonin and norepinephrine reuptake inhibitors), there have been spontaneous reports of adverse events occurring upon discontinuation of these drugs, particularly when abrupt, including the following: dysphoric mood, irritability, agitation, dizziness, sensory disturbances (e.g., paresthesias such as electric shock sensations), anxiety, confusion, headache, lethargy, emotional lability, insomnia, hypomania, tinnitus, and seizures. Although these events are generally self-limiting, some have been reported to be severe.
Patients should be monitored for these symptoms when discontinuing treatment with duloxetine delayed-release capsules. A gradual reduction in the dose rather than abrupt cessation is recommended whenever possible. If intolerable symptoms occur following a decrease in the dose or upon discontinuation of treatment, then resuming the previously prescribed dose may be considered. Subsequently, the physician may continue decreasing the dose but at a more gradual rate [see Dosage and Administration (2.7)].
5.8 Activation of Mania/Hypomania
In adult placebo-controlled trials in patients with major depressive disorder, activation of mania or hypomania was reported in 0.1% (4/3779) of duloxetine delayed-release capsule-treated patients and 0.04% (1/2536) of placebo-treated patients. No activation of mania or hypomania was reported in DPNP, GAD, fibromyalgia, or chronic musculoskeletal pain placebo-controlled trials. Activation of mania or hypomania has been reported in a small proportion of patients with mood disorders who were treated with other marketed drugs effective in the treatment of major depressive disorder. As with these other agents, duloxetine delayed-release capsules should be used cautiously in patients with a history of mania.
5.9 Angle-Closure Glaucoma
The pupillary dilation that occurs following use of many antidepressant drugs including duloxetine delayed-release capsules may trigger an angle closure attack in a patient with anatomically narrow angles who does not have a patent iridectomy.
5.10 Seizures
Duloxetine delayed-release capsules have not been systematically evaluated in patients with a seizure disorder, and such patients were excluded from clinical studies. In adult placebo-controlled clinical trials, seizures/convulsions occurred in 0.02% (3/12,722) of patients treated with duloxetine delayed-release capsules and 0.01% (1/9513) of patients treated with placebo. Duloxetine delayed-release capsules should be prescribed with care in patients with a history of a seizure disorder.
5.11 Effect on Blood Pressure
In adult placebo-controlled clinical trials across indications from baseline to endpoint, duloxetine delayed-release capsules treatment was associated with mean increases of 0.5 mm Hg in systolic blood pressure and 0.8 mm Hg in diastolic blood pressure compared to mean decreases of 0.6 mm Hg systolic and 0.3 mm Hg diastolic in placebo-treated patients. There was no significant difference in the frequency of sustained (3 consecutive visits) elevated blood pressure. In a clinical pharmacology study designed to evaluate the effects of duloxetine delayed-release capsules on various parameters, including blood pressure at supratherapeutic doses with an accelerated dose titration, there was evidence of increases in supine blood pressure at doses up to 200 mg twice daily. At the highest 200 mg twice daily dose, the increase in mean pulse rate was 5.0 to 6.8 beats and increases in mean blood pressure were 4.7 to 6.8 mm Hg (systolic) and 4.5 to 7 mm Hg (diastolic) up to 12 hours after dosing.
Blood pressure should be measured prior to initiating treatment and periodically measured throughout treatment [see Adverse Reactions (6.7)].
5.12 Clinically Important Drug Interactions
Both CYP1A2 and CYP2D6 are responsible for duloxetine delayed-release metabolism.
Potential for Other Drugs to Affect Duloxetine Delayed-Release Capsules
CYP1A2 Inhibitors - Co-administration of duloxetine delayed-release capsules with potent CYP1A2 inhibitors should be avoided [see Drug Interactions (7.1)].
CYP2D6 Inhibitors - Because CYP2D6 is involved in duloxetine delayed-release capsules metabolism, concomitant use of duloxetine delayed-release capsules with potent inhibitors of CYP2D6 would be expected to, and does, result in higher concentrations (on average of 60%) of duloxetine delayed-release capsules [see Drug Interactions (7.2)].
Potential for Duloxetine Delayed-Release Capsules to Affect Other Drugs
Drugs Metabolized by CYP2D6 - Co-administration of duloxetine delayed-release capsules with drugs that are extensively metabolized by CYP2D6 and that have a narrow therapeutic index, including certain antidepressants (tricyclic antidepressants [TCAs], such as nortriptyline, amitriptyline, and imipramine), phenothiazines and Type 1C antiarrhythmics (e.g., propafenone, flecainide), should be approached with caution. Plasma TCA concentrations may need to be monitored and the dose of the TCA may need to be reduced if a TCA is co-administered with duloxetine delayed-release capsules. Because of the risk of serious ventricular arrhythmias and sudden death potentially associated with elevated plasma levels of thioridazine, duloxetine delayed-release capsules and thioridazine should not be co-administered [see Drug Interactions (7.9)].
Other Clinically Important Drug Interactions
Alcohol - Use of duloxetine delayed-release capsules concomitantly with heavy alcohol intake may be associated with severe liver injury. For this reason, duloxetine delayed-release capsules should not be prescribed for patients with substantial alcohol use [see Warnings and Precautions (5.2) and Drug Interactions (7.15)].
CNS Acting Drugs - Given the primary CNS effects of duloxetine delayed-release capsules, it should be used with caution when it is taken in combination with or substituted for other centrally acting drugs, including those with a similar mechanism of action [see Warnings and Precautions (5.12) and Drug Interactions (7.16)].
5.13 Hyponatremia
Hyponatremia may occur as a result of treatment with SSRIs and SNRIs, including duloxetine delayed-release capsules. In many cases, this hyponatremia appears to be the result of the syndrome of inappropriate antidiuretic hormone secretion (SIADH). Cases with serum sodium lower than 110 mmol/L have been reported and appeared to be reversible when duloxetine delayed-release capsules were discontinued. Elderly patients may be at greater risk of developing hyponatremia with SSRIs and SNRIs. Also, patients taking diuretics or who are otherwise volume depleted may be at greater risk [see Use in Specific Populations (8.5)]. Discontinuation of duloxetine delayed-release capsules should be considered in patients with symptomatic hyponatremia and appropriate medical intervention should be instituted.
Signs and symptoms of hyponatremia include headache, difficulty concentrating, memory impairment, confusion, weakness, and unsteadiness, which may lead to falls. More severe and/or acute cases have been associated with hallucination, syncope, seizure, coma, respiratory arrest, and death.
5.14 Use in Patients with Concomitant Illness
Clinical experience with duloxetine delayed-release capsules in patients with concomitant systemic illnesses is limited. There is no information on the effect that alterations in gastric motility may have on the stability of duloxetine delayed-release capsules enteric coating. In extremely acidic conditions, duloxetine delayed-release capsules, unprotected by the enteric coating, may undergo hydrolysis to form naphthol. Caution is advised in using duloxetine delayed-release capsules in patients with conditions that may slow gastric emptying (e.g., some diabetics).
Duloxetine delayed-release capsules have not been systematically evaluated in patients with a recent history of myocardial infarction or unstable coronary artery disease. Patients with these diagnoses were generally excluded from clinical studies during the product’s premarketing testing.
Hepatic Impairment - Avoid use in patients with chronic liver disease or cirrhosis [see Dosage and Administration (2.6), Warnings and Precautions (5.2), and Use in Specific Populations (8.9)].
Severe Renal Impairment - Avoid use in patients with severe renal impairment, GFR less than 30 mL/min. Increased plasma concentration of duloxetine delayed-release capsules, and especially of its metabolites, occur in patients with end-stage renal disease (requiring dialysis) [see Dosage and Administration (2.6) and Use in Specific Populations (8.10)].
Glycemic Control in Patients with Diabetes - As observed in DPNP trials, duloxetine delayed-release capsules treatment worsens glycemic control in some patients with diabetes. In three clinical trials of duloxetine delayed-release capsules for the management of neuropathic pain associated with diabetic peripheral neuropathy, the mean duration of diabetes was approximately 12 years, the mean baseline fasting blood glucose was 176 mg/dL, and the mean baseline hemoglobin A1c (HbA1c) was 7.8%. In the 12-week acute treatment phase of these studies, duloxetine delayed-release capsules were associated with a small increase in mean fasting blood glucose as compared to placebo. In the extension phase of these studies, which lasted up to 52 weeks, mean fasting blood glucose increased by 12 mg/dL in the duloxetine delayed-release capsule group and decreased by 11.5 mg/dL in the routine care group. HbA1c increased by 0.5% in the duloxetine delayed-release capsule group and by 0.2% in the routine care groups.
5.15 Urinary Hesitation and Retention
Duloxetine delayed-release capsules are in a class of drugs known to affect urethral resistance. If symptoms of urinary hesitation develop during treatment with duloxetine delayed-release capsules, consideration should be given to the possibility that they might be drug-related.
In postmarketing experience, cases of urinary retention have been observed. In some instances of urinary retention associated with duloxetine delayed-release capsule use, hospitalization and/or catheterization has been needed.
-
6 ADVERSE REACTIONS
The following serious adverse reactions are described below and elsewhere in the labeling:
- Suicidal Thoughts and Behaviors in Children, Adolescents and Young Adults [see Boxed Warning and Warnings and Precautions (5.1)]
- Hepatotoxicity [see Warnings and Precautions (5.2)]
- Orthostatic Hypotension, Falls and Syncope [see Warnings and Precautions (5.3)]
- Serotonin Syndrome [see Warnings and Precautions (5.4)]
- Abnormal Bleeding [see Warnings and Precautions (5.5)]
- Severe Skin Reactions [see Warnings and Precautions (5.6)]
- Discontinuation of Treatment with Duloxetine Delayed-Release Capsules [see Warnings and Precautions (5.7)]
- Activation of Mania/Hypomania [see Warnings and Precautions (5.8)]
- Angle-Closure Glaucoma [see Warnings and Precautions (5.9)]
- Seizures [see Warnings and Precautions (5.10)]
- Effect on Blood Pressure [see Warnings and Precautions (5.11)]
- Clinically Important Drug Interactions [see Warnings and Precautions (5.12)]
- Hyponatremia [see Warnings and Precautions (5.13)]
- Urinary Hesitation and Retention [see Warnings and Precautions (5.15)]
6.1 Clinical Studies Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The stated frequencies of adverse reactions represent the proportion of individuals who experienced, at least once, a treatment-emergent adverse reaction of the type listed. A reaction was considered treatment-emergent if it occurred for the first time or worsened while receiving therapy following baseline evaluation. Reactions reported during the studies were not necessarily caused by the therapy, and the frequencies do not reflect investigator impression (assessment) of causality.
Adults - The data described below reflect exposure to duloxetine delayed-release capsules in placebo-controlled trials for MDD (N=3779), GAD (N=1018), OA (N=503), CLBP (N=600), DPNP (N=906), and FM (N=1294). The population studied was 17 to 89 years of age; 65.7%, 60.8%, 60.6%, 42.9%, and 94.4% female; and 81.8%, 72.6%, 85.3%, 74.0%, and 85.7% Caucasian for MDD, GAD, OA and CLBP, DPNP, and FM, respectively. Most patients received doses of a total of 60 to 120 mg per day [see Clinical Studies (14)].
Information describing two additional clinical studies in which efficacy was not demonstrated in patients ages 7 to 17 years is approved for Eli Lilly and Company, Inc.’s CYMBALTA® (duloxetine) delayed-release capsules. Other pediatric use information for patients ages 7 to 17 years is approved for Eli Lilly and Company, Inc.'s CYMBALTA® (duloxetine) delayed-release capsules. However, due to Eli Lilly and Company, Inc.'s marketing exclusivity rights, this drug product is not labeled with that pediatric information.
Adverse Reactions Reported as Reasons for Discontinuation of Treatment in Adult Placebo-Controlled Trials
Major Depressive Disorder - Approximately 8.4% (319/3779) of the patients who received duloxetine delayed-release capsules in placebo-controlled trials for MDD discontinued treatment due to an adverse reaction, compared with 4.6% (117/2536) of the patients receiving placebo. Nausea (duloxetine delayed-release capsules 1.1%, placebo 0.4%) was the only common adverse reaction reported as a reason for discontinuation and considered to be drug-related (i.e., discontinuation occurring in at least 1% of the duloxetine delayed-release capsule-treated patients and at a rate of at least twice that of placebo).
Generalized Anxiety Disorder - Approximately 13.7% (139/1018) of the patients who received duloxetine delayed-release capsules in placebo-controlled trials for GAD discontinued treatment due to an adverse reaction, compared with 5.0% (38/767) for placebo. Common adverse reactions reported as a reason for discontinuation and considered to be drug-related (as defined above) included nausea (duloxetine delayed-release capsules 3.3%, placebo 0.4%), and dizziness (duloxetine delayed-release capsules 1.3%, placebo 0.4%).
Diabetic Peripheral Neuropathic Pain - Approximately 12.9% (117/906) of the patients who received duloxetine delayed-release capsules in placebo-controlled trials for DPNP discontinued treatment due to an adverse reaction, compared with 5.1% (23/448) for placebo. Common adverse reactions reported as a reason for discontinuation and considered to be drug-related (as defined above) included nausea (duloxetine delayed-release capsules 3.5%, placebo 0.7%), dizziness (duloxetine delayed-release capsules 1.2%, placebo 0.4%), and somnolence (duloxetine delayed-release capsules 1.1%, placebo 0.0%).
Fibromyalgia - Approximately 17.5% (227/1294) of the patients who received duloxetine delayed-release capsules in 3 to 6 month placebo-controlled trials for FM discontinued treatment due to an adverse reaction, compared with 10.1% (96/955) for placebo. Common adverse reactions reported as a reason for discontinuation and considered to be drug-related (as defined above) included nausea (duloxetine delayed-release capsules 2.0%, placebo 0.5%), headache (duloxetine delayed-release capsules 1.2%, placebo 0.3%), somnolence (duloxetine delayed-release capsules 1.1%, placebo 0.0%), and fatigue (duloxetine delayed-release capsules 1.1%, placebo 0.1%).
Chronic Pain due to Osteoarthritis - Approximately 15.7% (79/503) of the patients who received duloxetine delayed-release capsules in 13-week, placebo-controlled trials for chronic pain due to OA discontinued treatment due to an adverse reaction, compared with 7.3% (37/508) for placebo. Common adverse reactions reported as a reason for discontinuation and considered to be drug-related (as defined above) included nausea (duloxetine delayed-release capsules 2.2%, placebo 1.0%).
Chronic Low Back Pain - Approximately 16.5% (99/600) of the patients who received duloxetine delayed-release capsules in 13-week, placebo-controlled trials for CLBP discontinued treatment due to an adverse reaction, compared with 6.3% (28/441) for placebo. Common adverse reactions reported as a reason for discontinuation and considered to be drug-related (as defined above) included nausea (duloxetine delayed-release capsules 3.0%, placebo 0.7%), and somnolence (duloxetine delayed-release capsules 1.0%, placebo 0.0%).
Most Common Adult Adverse Reactions
Pooled Trials for all Approved Indications - The most commonly observed adverse reactions in duloxetine delayed-release capsule-treated patients (incidence of at least 5% and at least twice the incidence in placebo patients) were nausea, dry mouth, somnolence, constipation, decreased appetite, and hyperhidrosis.
Diabetic Peripheral Neuropathic Pain - The most commonly observed adverse reactions in duloxetine delayed-release capsule-treated patients (as defined above) were nausea, somnolence, decreased appetite, constipation, hyperhidrosis, and dry mouth.
Fibromyalgia - The most commonly observed adverse reactions in duloxetine delayed-release capsule-treated patients (as defined above) were nausea, dry mouth, constipation, somnolence, decreased appetite, hyperhidrosis, and agitation.
Chronic Pain due to Osteoarthritis - The most commonly observed adverse reactions in duloxetine delayed-release capsule-treated patients (as defined above) were nausea, fatigue, constipation, dry mouth, insomnia, somnolence, and dizziness.
Chronic Low Back Pain - The most commonly observed adverse reactions in duloxetine delayed-release capsule-treated patients (as defined above) were nausea, dry mouth, insomnia, somnolence, constipation, dizziness, and fatigue.
Adverse Reactions Occurring at an Incidence of 5% or More Among Duloxetine Delayed-Release Capsule-Treated Patients in Adult Placebo-Controlled Trials
Table 2 gives the incidence of treatment-emergent adverse reactions in placebo-controlled trials for approved indications that occurred in 5% or more of patients treated with duloxetine delayed-release capsules and with an incidence greater than placebo.
Table 2: Treatment-Emergent Adverse Reactions: Incidence of 5% or More and Greater than Placebo in Placebo-Controlled Trials of Approved Indicationsa Percentage of Patients Reporting Reaction
Adverse Reaction
Duloxetine Delayed-Release Capsules
Placebo
(N=8100)
(N=5655)
Nauseac
23
8
Headache
14
12
Dry mouth
13
5
Somnolencee
10
3
Fatigueb,c
9
5
Insomniad
9
5
Constipationc
9
4
Dizzinessc
9
5
Diarrhea
9
6
Decreased appetitec
7
2
Hyperhidrosisc
6
1
Abdominal painf
5
4
aThe inclusion of an event in the table is determined based on the percentages before rounding; however, the percentages displayed in the table are rounded to the nearest integer.
bAlso includes asthenia.
cEvents for which there was a significant dose-dependent relationship in fixed-dose studies, excluding three MDD studies which did not have a placebo lead-in period or dose titration.
dAlso includes initial insomnia, middle insomnia, and early morning awakening.
eAlso includes hypersomnia and sedation.
fAlso includes abdominal discomfort, abdominal pain lower, abdominal pain upper, abdominal tenderness, and gastrointestinal pain.
Adverse Reactions Occurring at an Incidence of 2% or More Among Duloxetine Delayed-Release Capsule-Treated Patients in Adult Placebo-Controlled Trials
Pooled MDD and GAD Trials - Table 3 gives the incidence of treatment-emergent adverse reactions in MDD and GAD placebo-controlled trials for approved indications that occurred in 2% or more of patients treated with duloxetine delayed-release capsules and with an incidence greater than placebo.
Table 3: Treatment-Emergent Adverse Reactions: Incidence of 2% or More and Greater than Placebo in MDD and GAD Placebo-Controlled Trialsa Percentage of Patients Reporting Reaction
System Organ Class / Adverse Reaction
Duloxetine Delayed-Release Capsules
Placebo
(N=4797)
(N=3303)
Cardiac Disorders
Palpitations
2
1
Eye Disorders
Vision blurred
3
1
Gastrointestinal Disorders
Nauseac
23
8
Dry mouth
14
6
Constipationc
9
4
Diarrhea
9
6
Abdominal paind
5
4
Vomiting
4
2
General Disorders and Administration Site Conditions
Fatiguee
9
5
Metabolism and Nutrition Disorders
Decreased appetitec
6
2
Nervous System Disorders
Headache
14
14
Dizzinessc
9
5
Somnolencef
9
3
Tremor
3
1
Psychiatric Disorders
Insomniag
9
5
Agitationh
4
2
Anxiety
3
2
Reproductive System and Breast Disorders
Erectile dysfunction
4
1
Ejaculation delayedc
2
1
Libido decreasedi
3
1
Orgasm abnormalj
2
<1
Respiratory, Thoracic, and Mediastinal Disorders
Yawning
2
<1
Skin and Subcutaneous Tissue Disorders
Hyperhidrosis
6
2
aThe inclusion of an event in the table is determined based on the percentages before rounding; however, the percentages displayed in the table are rounded to the nearest integer.
cEvents for which there was a significant dose-dependent relationship in fixed-dose studies, excluding three MDD studies which did not have a placebo lead-in period or dose titration.
dAlso includes abdominal pain upper, abdominal pain lower, abdominal tenderness, abdominal discomfort, and gastrointestinal pain
eAlso includes asthenia
fAlso includes hypersomnia and sedation
gAlso includes initial insomnia, middle insomnia, and early morning awakening
hAlso includes feeling jittery, nervousness, restlessness, tension and psychomotor hyperactivity
iAlso includes loss of libido
jAlso includes anorgasmia
DPNP, FM, OA, and CLBP - Table 4 gives the incidence of treatment-emergent adverse events that occurred in 2% or more of patients treated with duloxetine delayed-release capsules (determined prior to rounding) in the premarketing acute phase of DPNP, FM, OA, and CLBP placebo-controlled trials and with an incidence greater than placebo.
Table 4: Treatment-Emergent Adverse Reactions: Incidence of 2% or More and Greater than Placebo in DPNP, FM, OA, and CLBP Placebo-Controlled Trialsa Percentage of Patients Reporting Reaction
System Organ Class / Adverse Reaction
Duloxetine Delayed-Release Capsules
Placebo
(N=3303)
(N=2352)
Gastrointestinal Disorders
Nausea
23
7
Dry Mouthb
11
3
Constipationb
10
3
Diarrhea
9
5
Abdominal Painc
5
4
Vomiting
3
2
Dyspepsia
2
1
General Disorders and Administration Site
Conditions
Fatigued
11
5
Infections and Infestations
Nasopharyngitis
4
4
Upper Respiratory Tract Infection
3
3
Influenza
2
2
Metabolism and Nutrition Disorders
Decreased Appetiteb
8
1
Musculoskeletal and Connective Tissue
Musculoskeletal Paine
3
3
Muscle Spasms
2
2
Nervous System Disorders
Headache
13
8
Somnolenceb,f
11
3
Dizziness
9
5
Paraesthesiag
2
2
Tremorb
2
<1
Psychiatric Disorders
Insomniab,h
10
5
Agitationi
3
1
Reproductive System and Breast Disorders
Erectile Dysfunctionb
4
<1
Ejaculation Disorderj
2
<1
Respiratory, Thoracic, and Mediastinal Disorders
Cough
2
2
Skin and Subcutaneous Tissue Disorders
Hyperhidrosis
6
1
Vascular Disorders
Flushingk
3
1
Blood pressure increasedl
2
1
aThe inclusion of an event in the table is determined based on the percentages before rounding; however, the percentages displayed in the table are rounded to the nearest integer.
bIncidence of 120 mg/day is significantly greater than the incidence for 60 mg/day.
cAlso includes abdominal discomfort, abdominal pain lower, abdominal pain upper, abdominal tenderness and gastrointestinal pain
dAlso includes asthenia
eAlso includes myalgia and neck pain
fAlso includes hypersomnia and sedation
gAlso includes hypoaesthesia, hypoaesthesia facial, genital hypoaesthesia and paraesthesia oral
hAlso includes initial insomnia, middle insomnia, and early morning awakening.
iAlso includes feeling jittery, nervousness, restlessness, tension and psychomotor hyperactivity
jAlso includes ejaculation failure
kAlso includes hot flush
lAlso includes blood pressure diastolic increased, blood pressure systolic increased, diastolic hypertension, essential hypertension, hypertension, hypertensive crisis, labile hypertension, orthostatic hypertension, secondary hypertension, and systolic hypertension
Effects on Male and Female Sexual Function in Adults
Changes in sexual desire, sexual performance and sexual satisfaction often occur as manifestations of psychiatric disorders or diabetes, but they may also be a consequence of pharmacologic treatment. Because adverse sexual reactions are presumed to be voluntarily underreported, the Arizona Sexual Experience Scale (ASEX), a validated measure designed to identify sexual side effects, was used prospectively in 4 MDD placebo-controlled trials. In these trials, as shown in Table 5 below, patients treated with duloxetine delayed-release capsules experienced significantly more sexual dysfunction, as measured by the total score on the ASEX, than did patients treated with placebo. Gender analysis showed that this difference occurred only in males. Males treated with duloxetine delayed-release capsules experienced more difficulty with ability to reach orgasm (ASEX Item 4) than males treated with placebo. Females did not experience more sexual dysfunction on duloxetine delayed-release capsules than on placebo as measured by ASEX total score. Negative numbers signify an improvement from a baseline level of dysfunction, which is commonly seen in depressed patients. Physicians should routinely inquire about possible sexual side effects.
Table 5: Mean Change in ASEX Scores by Gender in MDD Placebo-Controlled Trials Male Patientsa
Female Patientsa
Duloxetine Delayed-Release Capsules
PlaceboDuloxetine Delayed-Release Capsules
Placebo(n=175)
(n=83)
(n=241)
(n=126)
ASEX Total (Items 1 to 5)
0.56b
-1.07
-1.15
-1.07
Item 1 - Sex drive
-0.07
-0.12
-0.32
-0.24
Item 2 - Arousal
0.01
-0.26
-0.21
-0.18
Item 3 - Ability to achieve erection
0.03
-0.25
-0.17
-0.18
(men); Lubrication (women)
Item 4 - Ease of reaching orgasm
0.40c
-0.24
-0.09
-0.13
Item 5 - Orgasm satisfaction
0.09
-0.13
-0.11
-0.17
an=Number of patients with non-missing change score for ASEX total
bp=0.013 versus placebo
cp<0.001 versus placebo
Vital Sign Changes in Adults
In placebo-controlled clinical trials across approved indications for change from baseline to endpoint, duloxetine delayed-release capsules treatment was associated with mean increases of 0.23 mm Hg in systolic blood pressure and 0.73 mm Hg in diastolic blood pressure compared to mean decreases of 1.09 mm Hg systolic and 0.55 mm Hg diastolic in placebo-treated patients. There was no significant difference in the frequency of sustained (3 consecutive visits) elevated blood pressure [see Warnings and Precautions (5.3, 5.11)].
Duloxetine delayed-release capsules treatment, for up to 26 weeks in placebo-controlled trials across approved indications, typically caused a small increase in heart rate for change from baseline to endpoint compared to placebo of up to 1.37 beats per minute (increase of 1.20 beats per minute in duloxetine delayed-release capsule-treated patients, decrease of 0.17 beats per minute in placebo-treated patients).
Laboratory Changes in Adults
Duloxetine delayed-release capsules treatment in placebo-controlled clinical trials across approved indications, was associated with small mean increases from baseline to endpoint in ALT, AST, CPK, and alkaline phosphatase; infrequent, modest, transient, abnormal values were observed for these analytes in duloxetine delayed-release capsule-treated patients when compared with placebo-treated patients [see Warnings and Precautions (5.2)]. High bicarbonate, cholesterol, and abnormal (high or low) potassium, were observed more frequently in duloxetine delayed-release capsule-treated patients compared to placebo.
Electrocardiogram Changes in Adults
The effect of duloxetine delayed-release capsules 160 mg and 200 mg administered twice daily to steady state was evaluated in a randomized, double-blinded, two-way crossover study in 117 healthy female subjects. No QT interval prolongation was detected. Duloxetine delayed-release capsules appear to be associated with concentration-dependent but not clinically meaningful QT shortening.
Other Adverse Reactions Observed During the Premarketing and Postmarketing Clinical Trial Evaluation of Duloxetine Delayed-Release Capsules in Adults
Following is a list of treatment-emergent adverse reactions reported by patients treated with duloxetine delayed-release capsules in clinical trials. In clinical trials of all indications, 34,756 patients were treated with duloxetine delayed-release capsules. Of these, 26.9% (9337) took duloxetine delayed-release capsules for at least 6 months, and 12.4% (4317) for at least one year. The following listing is not intended to include reactions (1) already listed in previous tables or elsewhere in labeling, (2) for which a drug cause was remote, (3) which were so general as to be uninformative, (4) which were not considered to have significant clinical implications, or (5) which occurred at a rate equal to or less than placebo.
Reactions are categorized by body system according to the following definitions: frequent adverse reactions are those occurring in at least 1/100 patients; infrequent adverse reactions are those occurring in 1/100 to 1/1000 patients; rare reactions are those occurring in fewer than 1/1000 patients.
Cardiac Disorders - Frequent: palpitations; Infrequent: myocardial infarction, tachycardia, and Takotsubo cardiomyopathy.
Ear and Labyrinth Disorders - Frequent: vertigo; Infrequent: ear pain and tinnitus.
Endocrine Disorders - Infrequent: hypothyroidism.
Eye Disorders - Frequent: vision blurred; Infrequent: diplopia, dry eye, and visual impairment.
Gastrointestinal Disorders - Frequent: flatulence; Infrequent: dysphagia, eructation, gastritis, gastrointestinal hemorrhage, halitosis, and stomatitis; Rare: gastric ulcer.
General Disorders and Administration Site Conditions - Frequent: chills/rigors; Infrequent: falls, feeling abnormal, feeling hot and/or cold, malaise, and thirst; Rare: gait disturbance.
Infections and Infestations - Infrequent: gastroenteritis and laryngitis.
Investigations - Frequent: weight increased, weight decreased; Infrequent: blood cholesterol increased.
Metabolism and Nutrition Disorders - Infrequent: dehydration and hyperlipidemia; Rare: dyslipidemia.
Musculoskeletal and Connective Tissue Disorders - Frequent: musculoskeletal pain; Infrequent: muscle tightness and muscle twitching.
Nervous System Disorders - Frequent: dysgeusia, lethargy, and paraesthesia/hypoesthesia; Infrequent:
disturbance in attention, dyskinesia, myoclonus, and poor quality sleep; Rare: dysarthria.
Psychiatric Disorders - Frequent: abnormal dreams and sleep disorder; Infrequent: apathy, bruxism, disorientation/confusional state, irritability, mood swings, and suicide attempt; Rare: completed suicide.
Renal and Urinary Disorders - Frequent: urinary frequency; Infrequent: dysuria, micturition urgency, nocturia, polyuria, and urine odor abnormal.
Reproductive System and Breast Disorders - Frequent: anorgasmia/orgasm abnormal; Infrequent: menopausal symptoms, sexual dysfunction, and testicular pain; Rare: menstrual disorder.
Respiratory, Thoracic and Mediastinal Disorders - Frequent: yawning, oropharyngeal pain; Infrequent: throat tightness.
Skin and Subcutaneous Tissue Disorders - Frequent: pruritus; Infrequent: cold sweat, dermatitis contact, erythema, increased tendency to bruise, night sweats, and photosensitivity reaction; Rare: ecchymosis.
Vascular Disorders - Frequent: hot flush; Infrequent: flushing, orthostatic hypotension, and peripheral coldness.
Adverse Reactions Observed in Children and Adolescent Placebo-Controlled Clinical Trials
The adverse drug reaction profile observed in pediatric clinical trials (children and adolescents) was consistent with the adverse drug reaction profile observed in adult clinical trials. The specific adverse drug reactions observed in adult patients can be expected to be observed in pediatric patients (children and adolescents) [see Adverse Reactions (6.5)].
The most common (greater than or equal to 5% and twice placebo) adverse reactions observed in pediatric clinical trials include: nausea, diarrhea, decreased weight, and dizziness.
Table 6 provides the incidence of treatment-emergent adverse reactions in pediatric placebo-controlled trials that occurred in greater than 2% of patients treated with duloxetine delayed-release capsules and with an incidence greater than placebo.
Table 6: Treatment-Emergent Adverse Reactions: Incidence of 2% or More and Greater than Placebo in three 10-week Pediatric Placebo-Controlled Trialsa Percentage of Pediatric Patients Reporting Reaction
System Organ Class/Adverse Reaction
Duloxetine Delayed-Release Capsules
Placebo
(N=476)
(N=362)
Gastrointestinal Disorders
Nausea
18
8
Abdominal Painb
13
10
Vomiting
9
4
Diarrhea
6
3
Dry Mouth
2
1
General Disorders and Administration Site Conditions
Fatiguec
7
5
Investigations
Decreased Weightd
14
6
Metabolism and Nutrition Disorders
Decreased Appetite
10
5
Nervous System Disorders
Headache
18
13
Somnolencee
11
6
Dizziness
8
4
Psychiatric Disorders
Insomniaf
7
4
Respiratory, Thoracic, and Mediastinal Disorders
Oropharyngeal Pain
4
2
Cough
3
1
aThe inclusion of an event in the table is determined based on the percentages before rounding; however, the percentages displayed in the table are rounded to the nearest integer.
bAlso includes abdominal pain upper, abdominal pain lower, abdominal tenderness, abdominal discomfort, and gastrointestinal pain.
cAlso includes asthenia.
dFrequency based on weight measurement meeting potentially clinically significant threshold of greater than or equal to 3.5% weight loss (N=467 duloxetine delayed-release capsules; N=354 Placebo).
eAlso includes hypersomnia and sedation.
fAlso includes initial insomnia, insomnia, middle insomnia, and terminal insomnia.
Other adverse reactions that occurred at an incidence of less than 2% but were reported by more duloxetine delayed-release capsule-treated patients than placebo treated patients and are associated duloxetine delayed-release capsules treatment: abnormal dreams (including nightmare), anxiety, flushing (including hot flush), hyperhidrosis, palpitations, pulse increased, and tremor.
Discontinuation-emergent symptoms have been reported when stopping duloxetine delayed-release capsules. The most commonly reported symptoms following discontinuation of duloxetine delayed-release capsules in pediatric clinical trials have included headache, dizziness, insomnia, and abdominal pain [see Warnings and Precautions (5.7) and Adverse Reactions (6.2)].
Growth (Height and Weight) - Decreased appetite and weight loss have been observed in association with the use of SSRIs and SNRIs. In studies up to 9 months, duloxetine delayed-release capsule-treated pediatric patients experienced an increase in height of 1.7 cm on average (2.2 cm increase in children [7 to 11 years of age] and 1.3 cm increase in adolescents [12 to 17 years of age]). While height increase was observed during these studies, a mean decrease of 1% in height percentile was observed (decrease of 2% in children [7 to 11 years of age] and increase of 0.3% in adolescents [12 to 17 years of age]). Weight and height should be monitored regularly in children and adolescents treated with duloxetine delayed-release capsules.
Information describing two additional clinical studies in which efficacy was not demonstrated in patients ages 7 to 17 years is approved for Eli Lilly and Company, Inc.’s CYMBALTA® (duloxetine) delayed-release capsules. Other pediatric use information for patients ages 7 to 17 years is approved for Eli Lilly and Company, Inc.'s CYMBALTA® (duloxetine) delayed-release capsules. However, due to Eli Lilly and Company, Inc.'s marketing exclusivity rights, this drug product is not labeled with that pediatric information.
6.2 Postmarketing Experience
The following adverse reactions have been identified during post approval use of duloxetine delayed-release capsules. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Adverse reactions reported since market introduction that were temporally related to duloxetine delayed-release capsules therapy and not mentioned elsewhere in labeling include: acute pancreatitis, anaphylactic reaction, aggression and anger (particularly early in treatment or after treatment discontinuation), angioneurotic edema, angle-closure glaucoma, colitis (microscopic or unspecified), cutaneous vasculitis (sometimes associated with systemic involvement), extrapyramidal disorder, galactorrhea, gynecological bleeding, hallucinations, hyperglycemia, hyperprolactinemia, hypersensitivity, hypertensive crisis, muscle spasm, rash, restless legs syndrome, seizures upon treatment discontinuation, supraventricular arrhythmia, tinnitus (upon treatment discontinuation), trismus, and urticaria.
-
7 DRUG INTERACTIONS
Both CYP1A2 and CYP2D6 are responsible for duloxetine metabolism.
7.1 Inhibitors of CYP1A2
When duloxetine 60 mg was co-administered with fluvoxamine 100 mg, a potent CYP1A2 inhibitor, to male subjects (n=14) duloxetine AUC was increased approximately 6-fold, the Cmax was increased about 2.5-fold, and duloxetine t1/2 was increased approximately 3-fold. Other drugs that inhibit CYP1A2 metabolism include cimetidine and quinolone antimicrobials such as ciprofloxacin and enoxacin [see Warnings and Precautions (5.12)].
7.2 Inhibitors of CYP2D6
Concomitant use of duloxetine (40 mg once daily) with paroxetine (20 mg once daily) increased the concentration of duloxetine AUC by about 60%, and greater degrees of inhibition are expected with higher doses of paroxetine. Similar effects would be expected with other potent CYP2D6 inhibitors (e.g., fluoxetine, quinidine) [see Warnings and Precautions (5.12)].
7.3 Dual Inhibition of CYP1A2 and CYP2D6
Concomitant administration of duloxetine 40 mg twice daily with fluvoxamine 100 mg, a potent CYP1A2 inhibitor, to CYP2D6 poor metabolizer subjects (n=14) resulted in a 6-fold increase in duloxetine AUC and Cmax.
7.4 Drugs that Interfere with Hemostasis (e.g., NSAIDs, Aspirin, and Warfarin)
Serotonin release by platelets plays an important role in hemostasis. Epidemiological studies of the case-control and cohort design that have demonstrated an association between use of psychotropic drugs that interfere with serotonin reuptake and the occurrence of upper gastrointestinal bleeding have also shown that concurrent use of an NSAID or aspirin may potentiate this risk of bleeding. Altered anticoagulant effects, including increased bleeding, have been reported when SSRIs or SNRIs are co-administered with warfarin. Concomitant administration of warfarin (2 to 9 mg once daily) under steady state conditions with duloxetine 60 or 120 mg once daily for up to 14 days in healthy subjects (n=15) did not significantly change INR from baseline (mean INR changes ranged from 0.05 to +0.07). The total warfarin (protein bound plus free drug) pharmacokinetics (AUCτ,ss, Cmax,ss or tmax,ss) for both R- and S-warfarin were not altered by duloxetine. Because of the potential effect of duloxetine on platelets, patients receiving warfarin therapy should be carefully monitored when duloxetine is initiated or discontinued [see Warnings and Precautions (5.5)].
7.5 Lorazepam
Under steady-state conditions for duloxetine (60 mg Q 12 hours) and lorazepam (2 mg Q 12 hours), the pharmacokinetics of duloxetine were not affected by co-administration.
7.6 Temazepam
Under steady-state conditions for duloxetine (20 mg qhs) and temazepam (30 mg qhs), the pharmacokinetics of duloxetine were not affected by co-administration.
7.7 Drugs that Affect Gastric Acidity
Duloxetine delayed-release capsules have an enteric coating that resists dissolution until reaching a segment of the gastrointestinal tract where the pH exceeds 5.5. In extremely acidic conditions, duloxetine delayed-release capsules, unprotected by the enteric coating, may undergo hydrolysis to form naphthol. Caution is advised in using duloxetine delayed-release capsules in patients with conditions that may slow gastric emptying (e.g., some diabetics). Drugs that raise the gastrointestinal pH may lead to an earlier release of duloxetine. However, co-administration of duloxetine delayed-release capsules with aluminum- and magnesium-containing antacids (51 mEq) or duloxetine delayed-release capsules with famotidine, had no significant effect on the rate or extent of duloxetine absorption after administration of a 40 mg oral dose. It is unknown whether the concomitant administration of proton pump inhibitors affects duloxetine absorption [see Warnings and Precautions (5.14)].
7.8 Drugs Metabolized by CYP1A2
In vitro drug interaction studies demonstrate that duloxetine does not induce CYP1A2 activity. Therefore, an increase in the metabolism of CYP1A2 substrates (e.g., theophylline, caffeine) resulting from induction is not anticipated, although clinical studies of induction have not been performed. Duloxetine is an inhibitor of the CYP1A2 isoform in in vitro studies, and in two clinical studies the average (90% confidence interval) increase in theophylline AUC was 7% (1% to 15%) and 20% (13% to 27%) when co-administered with duloxetine (60 mg twice daily).
7.9 Drugs Metabolized by CYP2D6
Duloxetine is a moderate inhibitor of CYP2D6. When duloxetine was administered (at a dose of 60 mg twice daily) in conjunction with a single 50 mg dose of desipramine, a CYP2D6 substrate, the AUC of desipramine increased 3-fold [see Warnings and Precautions (5.12)].
7.10 Drugs Metabolized by CYP2C9
Results of in vitro studies demonstrate that duloxetine does not inhibit activity. In a clinical study, the pharmacokinetics of S-warfarin, a CYP2C9 substrate, were not significantly affected by duloxetine [see Drug Interactions (7.4)].
7.11 Drugs Metabolized by CYP3A
Results of in vitro studies demonstrate that duloxetine does not inhibit or induce CYP3A activity. Therefore, an increase or decrease in the metabolism of CYP3A substrates (e.g., oral contraceptives and other steroidal agents) resulting from induction or inhibition is not anticipated, although clinical studies have not been performed.
7.12 Drugs Metabolized by CYP2C19
Results of in vitro studies demonstrate that duloxetine does not inhibit CYP2C19 activity at therapeutic concentrations. Inhibition of the metabolism of CYP2C19 substrates is therefore not anticipated, although clinical studies have not been performed.
7.13 Monoamine Oxidase Inhibitors (MAOIs)
[See Dosage and Administration (2.8, 2.9), Contraindications (4), and Warnings and Precautions (5.4)].
7.14 Serotonergic Drugs
[See Dosage and Administration (2.8, 2.9), Contraindications (4), and Warnings and Precautions (5.4)].
7.15 Alcohol
When duloxetine delayed-release capsules and ethanol were administered several hours apart so that peak concentrations of each would coincide, duloxetine delayed-release capsules did not increase the impairment of mental and motor skills caused by alcohol.
In the duloxetine delayed-release capsules clinical trials database, three duloxetine delayed-release capsule-treated patients had liver injury as manifested by ALT and total bilirubin elevations, with evidence of obstruction. Substantial intercurrent ethanol use was present in each of these cases, and this may have contributed to the abnormalities seen [see Warnings and Precautions (5.2, 5.12)].
7.17 Drugs Highly Bound to Plasma Protein
Because duloxetine is highly bound to plasma protein, administration of duloxetine delayed-release capsules to a patient taking another drug that is highly protein bound may cause increased free concentrations of the other drug, potentially resulting in adverse reactions. However, co-administration of duloxetine (60 mg or 120 mg) with warfarin (2 mg to 9 mg), a highly protein-bound drug, did not result in significant changes in INR and in the pharmacokinetics of either total S-or total R-warfarin (protein bound plus free drug) [see Drug Interactions (7.4)].
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
Data from a postmarketing retrospective cohort study indicate that use of duloxetine in the month before delivery may be associated with an increased risk of postpartum hemorrhage. Data from published literature and from a postmarketing retrospective cohort study have not identified a clear drug-associated risk of major birth defects or other adverse developmental outcomes (see Data). There are risks associated with untreated depression and fibromyalgia in pregnancy, and with exposure to SNRIs and SSRIs, including duloxetine delayed-release capsules, during pregnancy (see Clinical Considerations).In rats and rabbits treated with duloxetine during the period of organogenesis, fetal weights were decreased but there was no evidence of developmental effects at doses up to 3 and 6 times, respectively, the maximum recommended human dose (MRHD) of 120 mg/day given to adolescents on a mg/m2 basis. When duloxetine was administered orally to pregnant rats throughout gestation and lactation, pup weights at birth and pup survival to 1 day postpartum were decreased at a dose 2 times the MRHD given to adolescents on a mg/m2 basis. At this dose, pup behaviors consistent with increased reactivity, such as increased startle response to noise and decreased habituation of locomotor activity were observed. Post-weaning growth was not adversely affected.
The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2 to 4% and 15 to 20%, respectively.
Clinical Considerations
Disease-associated Maternal and/or Embryo/Fetal RiskWomen who discontinue antidepressants during pregnancy are more likely to experience a relapse of major depression than women who continue antidepressants. This finding is from a prospective, longitudinal study that followed 201 pregnant women with a history of major depressive disorder who were euthymic and taking antidepressants at the beginning of pregnancy. Consider the risk of untreated depression when discontinuing or changing treatment with antidepressant medication during pregnancy and postpartum.
Pregnant women with fibromyalgia are at increased risk for adverse maternal and infant outcomes including preterm premature rupture of membranes, preterm birth, small for gestational age, intrauterine growth restriction, placental disruption, and venous thrombosis. It is not known if these adverse maternal and fetal outcomes are a direct result of fibromyalgia or other comorbid factors.
Maternal Adverse Reactions
Use of duloxetine in the month before delivery may be associated with an increased risk of postpartum hemorrhage [see Warnings and Precautions (5.5)].
Fetal/Neonatal Adverse Reaction
Neonates exposed to duloxetine and other SNRIs or SSRIs late in the third trimester have developed complications requiring prolonged hospitalization, respiratory support, and tube feeding. Such complications can arise immediately upon delivery. Reported clinical findings have included respiratory distress, cyanosis, apnea, seizures, temperature instability, feeding difficulty, vomiting, hypoglycemia, hypotonia, hypertonia, hyperreflexia, tremor, jitteriness, irritability, and constant crying. These findings are consistent with either a direct toxic effect of the SNRIs or SSRIs, or possibly, a drug discontinuation syndrome. It should be noted that, in some cases, the clinical picture is consistent with serotonin syndrome [see Warnings and Precautions (5.4)].
Data
Human DataData from a postmarketing retrospective claims-based cohort study found an increased risk for postpartum hemorrhage among 955 pregnant women exposed to duloxetine in the last month of pregnancy compared to 4,128,460 unexposed pregnant women (adjusted relative risk: 1.53; 95% CI: 1.08 to 2.18). The same study did not find a clinically meaningful increase in the risk for major birth defects in the comparison of 2532 women exposed to duloxetine in the first trimester of pregnancy to 1,284,827 unexposed women after adjusting for several confounders. Methodologic limitations include possible residual confounding, misclassification of exposure and outcomes, lack of direct measures of disease severity, and lack of information about alcohol use, nutrition, and over-the-counter medication exposures.
Animal Data
In animal reproduction studies, duloxetine has been shown to have adverse effects on embryo/fetal and postnatal development.
When duloxetine was administered orally to pregnant rats and rabbits during the period of organogenesis, there was no evidence of malformations or developmental variations at doses up to 45 mg/kg/day [3 and 6 times, respectively, the MRHD of 120 mg/day given to adolescents on a mg/m2 basis]. However, fetal weights were decreased at this dose, with a no-effect dose of 10 mg/kg/day (approximately equal to the MRHD in rats and 2 times the MRHD in rabbits).
When duloxetine was administered orally to pregnant rats throughout gestation and lactation, the survival of pups to 1 day postpartum and pup body weights at birth and during the lactation period were decreased at a dose of 30 mg/kg/day (2 times the MRHD given to adolescents on a mg/m2 basis); the no-effect dose was 10 mg/kg/day. Furthermore, behaviors consistent with increased reactivity, such as increased startle response to noise and decreased habituation of locomotor activity, were observed in pups following maternal exposure to 30 mg/kg/day. Post-weaning growth and reproductive performance of the progeny were not affected adversely by maternal duloxetine treatment.
8.2 Lactation
Risk Summary
Data from published literature report the presence of duloxetine in human milk (see Data). There are reports of sedation, poor feeding, and poor weight gain in infants exposed to duloxetine through breast milk (see Clinical Considerations). There are no data on the effect of duloxetine on milk production.
The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for duloxetine delayed-release capsules and any potential adverse effects on the breastfed child from duloxetine delayed-release capsules or from the underlying maternal condition.
Clinical Considerations
Infants exposed to duloxetine delayed-release capsules should be monitored for sedation, poor feeding and poor weight gain.
Data
Disposition of duloxetine delayed-release capsules was studied in 6 lactating women who were at least 12 weeks postpartum and had elected to wean their infants. The women were given 40 mg of duloxetine delayed-release capsules twice daily for 3.5 days. The peak concentration measured in breast milk occurred at a median of 3 hours after the dose. The amount of duloxetine hydrochloride in breast milk was approximately 7 mcg/day while on that dose; the estimated daily infant dose was approximately 2 mcg/kg/day, which is less than 1% of the maternal dose. The presence of duloxetine hydrochloride metabolites in breast milk was not examined.
8.4 Pediatric Use
The safety and effectiveness in pediatric patients less than 7 years of age have not been established.
Safety and effectiveness of duloxetine delayed-release capsules have not been established in pediatric patients less than 18 years of age with MDD.
Decreased appetite and weight loss have been observed in association with the use of SSRIs and SNRIs. Perform regular monitoring of weight and growth in children and adolescents treated with an SNRI such as duloxetine delayed-release capsules [see Adverse Reactions (6.11)].
Information describing two additional clinical studies in which efficacy was not demonstrated in patients ages 7 to 17 years is approved for Eli Lilly and Company, Inc.’s CYMBALTA® (duloxetine) delayed-release capsules. Other pediatric use information for patients ages 7 to 17 years is approved for Eli Lilly and Company, Inc.'s CYMBALTA® (duloxetine) delayed-release capsules. However, due to Eli Lilly and Company, Inc.’s marketing exclusivity rights, this drug product is not labeled with that pediatric information.
Animal Data - Duloxetine administration to young rats from post-natal day 21 (weaning) through post-natal day 90 (adult) resulted in decreased body weights that persisted into adulthood, but recovered when drug treatment was discontinued; slightly delayed (~1.5 days) sexual maturation in females, without any effect on fertility; and a delay in learning a complex task in adulthood, which was not observed after drug treatment was discontinued. These effects were observed at the high dose of 45 mg/kg/day (2 times the MRHD, for a child); the no-effect-level was 20 mg/kg/day (≈1 times the MRHD, for a child).
8.5 Geriatric Use
Of the 2,418 patients in premarketing clinical studies of duloxetine delayed-release capsules for MDD, 5.9% (143) were 65 years of age or over. Of the 1041 patients in CLBP premarketing studies, 21.2% (221) were 65 years of age or over. Of the 487 patients in OA premarketing studies, 40.5% (197) were 65 years of age or over. Of the 1,074 patients in the DPNP premarketing studies, 33% (357) were 65 years of age or over. Of the 1,761 patients in FM premarketing studies, 7.9% (140) were 65 years of age or over. In the MDD, DPNP, FM, OA, CLBP and other studies, no overall differences in safety or effectiveness were generally observed between these subjects and younger subjects, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out. SSRIs and SNRIs, including duloxetine delayed-release capsules have been associated with cases of clinically significant hyponatremia in elderly patients, who may be at greater risk for this adverse event [see Warnings and Precautions (5.13)].
In an analysis of data from all placebo-controlled-trials, patients treated with duloxetine delayed-release capsules reported a higher rate of falls compared to patients treated with placebo. The increased risk appears to be proportional to a patient’s underlying risk for falls. Underlying risk appears to increase steadily with age. As elderly patients tend to have a higher prevalence of risk factors for falls such as medications, medical comorbidities and gait disturbances, the impact of increasing age by itself on falls during treatment with duloxetine delayed-release capsules is unclear. Falls with serious consequences including bone fractures and hospitalizations have been reported [see Warnings and Precautions (5.3) and Adverse Reactions (6.10)].
8.6 Gender
Duloxetine’s half-life is similar in men and women. Dosage adjustment based on gender is not necessary.
8.7 Smoking Status
Duloxetine bioavailability (AUC) appears to be reduced by about one-third in smokers. Dosage modifications are not recommended for smokers.
8.9 Hepatic Impairment
Patients with clinically evident hepatic impairment have decreased duloxetine metabolism and elimination. After a single 20 mg dose of duloxetine delayed-release capsules, 6 cirrhotic patients with moderate liver impairment (Child-Pugh Class B) had a mean plasma duloxetine clearance about 15% that of age- and gender-matched healthy subjects, with a 5-fold increase in mean exposure (AUC). Although Cmax was similar to normals in the cirrhotic patients, the half-life was about 3 times longer [see Dosage and Administration (2.6) and Warnings and Precautions (5.14)].
8.10 Severe Renal Impairment
Limited data are available on the effects of duloxetine in patients with end-stage renal disease (ESRD). After a single 60 mg dose of duloxetine, Cmax and AUC values were approximately 100% greater in patients with end-stage renal disease receiving chronic intermittent hemodialysis than in subjects with normal renal function. The elimination half-life, however, was similar in both groups. The AUCs of the major circulating metabolites, 4-hydroxy duloxetine glucuronide and 5-hydroxy, 6-methoxy duloxetine sulfate, largely excreted in urine, were approximately 7- to 9-fold higher and would be expected to increase further with multiple dosing. Population PK analyses suggest that mild to moderate degrees of renal impairment (estimated CrCl 30 to 80 mL/min) have no significant effect on duloxetine apparent clearance [see Dosage and Administration (2.6) and Warnings and Precautions (5.14)].
-
9 DRUG ABUSE AND DEPENDENCE
9.2 Abuse
In animal studies, duloxetine did not demonstrate barbiturate-like (depressant) abuse potential.
While duloxetine delayed-release capsules have not been systematically studied in humans for their potential for abuse, there was no indication of drug-seeking behavior in the clinical trials. However, it is not possible to predict on the basis of premarketing experience the extent to which a CNS active drug will be misused, diverted, and/or abused once marketed. Consequently, physicians should carefully evaluate patients for a history of drug abuse and follow such patients closely, observing them for signs of misuse or abuse of duloxetine delayed-release capsules (e.g., development of tolerance, incrementation of dose, drug-seeking behavior).
-
10 OVERDOSAGE
10.1 Signs and Symptoms
In postmarketing experience, fatal outcomes have been reported for acute overdoses, primarily with mixed overdoses, but also with duloxetine only, at doses as low as 1,000 mg. Signs and symptoms of overdose (duloxetine alone or with mixed drugs) included somnolence, coma, serotonin syndrome, seizures, syncope, tachycardia, hypotension, hypertension, and vomiting.
10.2 Management of Overdose
There is no specific antidote to duloxetine delayed-release capsules, but if serotonin syndrome ensues, specific treatment (such as with cyproheptadine and/or temperature control) may be considered. In case of acute overdose, treatment should consist of those general measures employed in the management of overdose with any drug.
An adequate airway, oxygenation, and ventilation should be assured, and cardiac rhythm and vital signs should be monitored. Induction of emesis is not recommended. Gastric lavage with a large-bore orogastric tube with appropriate airway protection, if needed, may be indicated if performed soon after ingestion or in symptomatic patients.
Activated charcoal may be useful in limiting absorption of duloxetine from the gastrointestinal tract. Administration of activated charcoal has been shown to decrease AUC and Cmax by an average of one-third, although some subjects had a limited effect of activated charcoal. Due to the large volume of distribution of this drug, forced diuresis, dialysis, hemoperfusion, and exchange transfusion are unlikely to be beneficial.
In managing overdose, the possibility of multiple drug involvement should be considered. A specific caution involves patients who are taking or have recently taken duloxetine delayed-release capsules and might ingest excessive quantities of a TCA. In such a case, decreased clearance of the parent tricyclic and/or its active metabolite may increase the possibility of clinically significant sequelae and extend the time needed for close medical observation [see Warnings and Precautions (5.4) and Drug Interactions (7)]. The physician should consider contacting a poison control center (1-800-222-1222 or www.poison.org) for additional information on the treatment of any overdose. Telephone numbers for certified poison control centers are listed in the Physicians’ Desk Reference (PDR).
-
11 DESCRIPTION
Duloxetine Delayed-Release Capsules, USP are a selective serotonin and norepinephrine reuptake inhibitor (SNRI) for oral administration. Its chemical designation is (+)-(S)-N-methyl-γ-(1-naphthyloxy)-2-thiophenepropylamine hydrochloride. The structural formula is:
C18H19NOSHCl M.W. 333.88
Duloxetine hydrochloride, USP is a white to slightly brownish white solid, which is slightly soluble in water.
Each capsule contains enteric-coated pellets of 22.4, 33.7, or 67.3 mg of duloxetine hydrochloride, USP equivalent to 20, 30, or 60 mg of duloxetine, respectively. These enteric-coated pellets are designed to prevent degradation of the drug in the acidic environment of the stomach. Inactive ingredients include ammonium hydroxide, black iron oxide, gelatin, hydroxypropyl cellulose, hydroxypropyl methylcellulose phthalate, hypromellose, potassium hydroxide, propylene glycol, shellac, sugar spheres (which contain sucrose and corn starch), talc, titanium dioxide, and triethyl citrate. The 20 mg and 30 mg capsules also contain FD&C Blue #1 Aluminum Lake.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Although the exact mechanisms of the antidepressant, central pain inhibitory and anxiolytic actions of duloxetine in humans are unknown, these actions are believed to be related to its potentiation of serotonergic and noradrenergic activity in the CNS.
12.2 Pharmacodynamics
Preclinical studies have shown that duloxetine is a potent inhibitor of neuronal serotonin and norepinephrine reuptake and a less potent inhibitor of dopamine reuptake. Duloxetine has no significant affinity for dopaminergic, adrenergic, cholinergic, histaminergic, opioid, glutamate, and GABA receptors in vitro. Duloxetine does not inhibit monoamine oxidase (MAO).
Duloxetine delayed-release capsules are in a class of drugs known to affect urethral resistance. If symptoms of urinary hesitation develop during treatment with duloxetine delayed-release capsules, consideration should be given to the possibility that they might be drug-related.
12.3 Pharmacokinetics
Duloxetine has an elimination half-life of about 12 hours (range 8 to 17 hours) and its pharmacokinetics are dose proportional over the therapeutic range. Steady-state plasma concentrations are typically achieved after 3 days of dosing. Elimination of duloxetine is mainly through hepatic metabolism involving two P450 isozymes, CYP1A2 and CYP2D6.
Absorption and Distribution - Orally administered duloxetine hydrochloride is well absorbed. There is a median 2 hour lag until absorption begins (Tlag), with maximal plasma concentrations (Cmax) of duloxetine occurring 6 hours post dose. Food does not affect the Cmax of duloxetine, but delays the time to reach peak concentration from 6 to 10 hours and it marginally decreases the extent of absorption (AUC) by about 10%. There is a 3 hour delay in absorption and a one-third increase in apparent clearance of duloxetine after an evening dose as compared to a morning dose.
The apparent volume of distribution averages about 1640 L. Duloxetine is highly bound (greater than 90%) to proteins in human plasma, binding primarily to albumin and α1-acid glycoprotein. The interaction between duloxetine and other highly protein bound drugs has not been fully evaluated. Plasma protein binding of duloxetine is not affected by renal or hepatic impairment.
Metabolism and Elimination - Biotransformation and disposition of duloxetine in humans have been determined following oral administration of 14C-labeled duloxetine. Duloxetine comprises about 3% of the total radiolabeled material in the plasma, indicating that it undergoes extensive metabolism to numerous metabolites. The major biotransformation pathways for duloxetine involve oxidation of the naphthyl ring followed by conjugation and further oxidation. Both CYP1A2 and CYP2D6 catalyze the oxidation of the naphthyl ring in vitro. Metabolites found in plasma include 4-hydroxy duloxetine glucuronide and 5-hydroxy, 6-methoxy duloxetine sulfate. Many additional metabolites have been identified in urine, some representing only minor pathways of elimination. Only trace (less than 1% of the dose) amounts of unchanged duloxetine are present in the urine. Most (about 70%) of the duloxetine dose appears in the urine as metabolites of duloxetine; about 20% is excreted in the feces. Duloxetine undergoes extensive metabolism, but the major circulating metabolites have not been shown to contribute significantly to the pharmacologic activity of duloxetine.
Pediatric use information for patients ages 7 to 17 years is approved for Eli Lilly and Company, Inc.'s CYMBALTA® (duloxetine) delayed-release capsules. However, due to Eli Lilly and Company, Inc.'s marketing exclusivity rights, this drug product is not labeled with that pediatric information.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis and Mutagenesis and Impairment of Fertility
Carcinogenesis - Duloxetine was administered in the diet to mice and rats for 2 years.
In female mice receiving duloxetine at 140 mg/kg/day (6 times the maximum recommended human dose (MRHD) of 120 mg/day on a mg/m2 basis), there was an increased incidence of hepatocellular adenomas and carcinomas. The no-effect dose was 50 mg/kg/day (2 times the MRHD). Tumor incidence was not increased in male mice receiving duloxetine at doses up to 100 mg/kg/day (4 times the MRHD).
In rats, dietary doses of duloxetine up to 27 mg/kg/day in females (2 times the MRHD) and up to 36 mg/kg/day in males (3 times the MRHD) did not increase the incidence of tumors.
Mutagenesis - Duloxetine was not mutagenic in the in vitro bacterial reverse mutation assay (Ames test) and was not clastogenic in an in vivo chromosomal aberration test in mouse bone marrow cells. Additionally, duloxetine was not genotoxic in an in vitro mammalian forward gene mutation assay in mouse lymphoma cells or in an in vitro unscheduled DNA synthesis (UDS) assay in primary rat hepatocytes, and did not induce sister chromatid exchange in Chinese hamster bone marrow in vivo.
Impairment of Fertility - Duloxetine administered orally to either male or female rats prior to and throughout mating at doses up to 45 mg/kg/day (4 times the MRHD) did not alter mating or fertility.
Pediatric use information for patients ages 7 to 17 years is approved for Eli Lilly and Company, Inc.'s CYMBALTA® (duloxetine) delayed-release capsules. However, due to Eli Lilly and Company, Inc.'s marketing exclusivity rights, this drug product is not labeled with that pediatric information.
-
14 CLINICAL STUDIES
The efficacy of duloxetine delayed-release capsules has been established in the following adequate and well-controlled trials:
- Major Depressive Disorder (MDD): 4 short-term and 1 maintenance trial in adults [see Clinical Studies (14.1)].
- Generalized Anxiety Disorder (GAD): 3 short-term trials in adults, 1 maintenance trial in adults [see Clinical Studies (14.2)].
- Diabetic Peripheral Neuropathic Pain (DPNP): Two 12-week trials in adults [see Clinical Studies (14.3)].
- Fibromyalgia (FM): Two trials in adults (one of 3 months duration and one of 6 months duration) [see Clinical Studies (14.4)].
- Chronic Musculoskeletal Pain: Two 12- to 13-week trials in adult patients with chronic low back pain (CLBP) and one 13-week trial in adult patients with chronic pain due to osteoarthritis [see Clinical Studies (14.5)].
Pediatric use information for patients ages 7 to 17 years is approved for Eli Lilly and Company, Inc.'s CYMBALTA® (duloxetine) delayed-release capsules. However, due to Eli Lilly and Company, Inc.'s marketing exclusivity rights, this drug product is not labeled with that pediatric information.
14.1 Major Depressive Disorder
The efficacy of duloxetine delayed-release capsules as a treatment for depression was established in 4 randomized, double-blind, placebo-controlled, fixed-dose studies in adult outpatients (18 to 83 years) meeting DSM-IV criteria for major depression. In 2 studies, patients were randomized to duloxetine delayed-release capsules 60 mg once daily (N=123 and N=128, respectively) or placebo (N=122 and N=139, respectively) for 9 weeks; in the third study, patients were randomized to duloxetine delayed-release capsules 20 mg or 40 mg twice daily (N=86 and N=91, respectively) or placebo (N=89) for 8 weeks; in the fourth study, patients were randomized to duloxetine delayed-release capsules 40 mg or 60 mg twice daily (N=95 and N=93, respectively) or placebo (N=93) for 8 weeks. There is no evidence that doses greater than 60 mg/day confer additional benefits.
In all 4 studies, duloxetine delayed-release capsules demonstrated superiority over placebo as measured by improvement in the 17-item Hamilton Depression Rating Scale (HAMD-17) total score (Studies 1 to 4 in Table 7).
In all of these clinical studies, analyses of the relationship between treatment outcome and age, gender, and race did not suggest any differential responsiveness on the basis of these patient characteristics.
Table 7: Summary of the Primary Efficacy Results for Studies in Major Depressive Disorder Primary Efficacy Measure: HAMD-17
Study
Treatment Group
Mean Baseline
LS Mean Change
Placebo-subtracted
Number
Score (SD)
from Baseline (SE)
Differencea(95% CI)
Study 1
Duloxetine Delayed-Release Capsules (60 mg/day)b
21.5 (4.10)
-10.9 (0.70)
-4.9 (-6.8, -2.9)
Placebo
21.1 (3.71)
-6.1 (0.69)
--
Study 2
Duloxetine Delayed-Release Capsules (60 mg/day)b
20.3 (3.32)
-10.5 (0.71)
-2.2 (-4.0, -0.3)
Placebo
20.5 (3.42)
-8.3 (0.67)
--
Study 3
Duloxetine Delayed-Release Capsules (20 mg BID)b
18.6 (5.85)
-7.4 (0.80)
-2.4 (-4.7, -0.2)
Duloxetine Delayed-Release Capsules (40 mg BID)b
18.1 (4.52)
-8.6 (0.81)
-3.6 (-5.9, -1.4)
Placebo
17.2 (5.11)
-5.0 (0.81)
--
Study 4
Duloxetine Delayed-Release Capsules (40 mg BID)b
19.9 (3.54)
-11.0 (0.49)
-2.2 (-3.6, -0.9)
Duloxetine Delayed-Release Capsules (60 mg BID)b
20.2 (3.41)
-12.1 (0.49)
-3.3 (-4.7, -1.9)
Placebo
19.9 (3.58)
-8.8 (0.50)
--
SD: standard deviation; SE: standard error; LS Mean: least-squares mean; CI: confidence interval, not adjusted for multiplicity in trials where multiple dose groups were included.
aDifference (drug minus placebo) in least-squares mean change from baseline.
bDoses statistically significantly superior to placebo.
In another study, 533 patients meeting DSM-IV criteria for MDD received duloxetine delayed-release capsules 60 mg once daily during an initial 12-week open-label treatment phase. Two hundred and seventy-eight patients who responded to open label treatment (defined as meeting the following criteria at weeks 10 and 12: a HAMD-17 total score less than or equal to 9, Clinical Global Impressions of Severity (CGI-S) less than or equal to 2, and not meeting the DSM-IV criteria for MDD) were randomly assigned to continuation of duloxetine delayed-release capsules at the same dose (N=136) or to placebo (N=142) for 6 months. Patients on duloxetine delayed-release capsules experienced a statistically significantly longer time to relapse of depression than did patients on placebo (Study 5 in Figure 1). Relapse was defined as an increase in the CGI-S score of greater than or equal to 2 points compared with that obtained at week 12, as well as meeting the DSM-IV criteria for MDD at 2 consecutive visits at least 2 weeks apart, where the 2-week temporal criterion had to be satisfied at only the second visit. The effectiveness of duloxetine delayed-release capsules in hospitalized patients with major depressive disorder has not been studied.
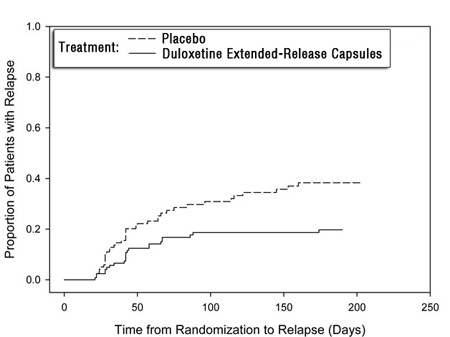
Figure 1: Kaplan-Meier Estimation of Cumulative Proportion of Patients with Relapse (MDD Study 5)
14.2 Generalized Anxiety Disorder
The efficacy of duloxetine delayed-release capsules in the treatment of generalized anxiety disorder (GAD) was established in 1 fixed-dose randomized, double-blind, placebo-controlled trial and 2 flexible-dose randomized, double-blind, placebo-controlled trials in adult outpatients between 18 and 83 years of age meeting the DSM-IV criteria for GAD.
In 1 flexible-dose study and in the fixed-dose study, the starting dose was 60 mg once daily where down titration to 30 mg once daily was allowed for tolerability reasons before increasing it to 60 mg once daily. Fifteen percent of patients were down titrated. One flexible-dose study had a starting dose of 30 mg once daily for 1 week before increasing it to 60 mg once daily.
The 2 flexible-dose studies involved dose titration with duloxetine delayed-release capsule doses ranging from 60 mg once daily to 120 mg once daily (N=168 and N=162) compared to placebo (N=159 and N=161) over a 10-week treatment period. The mean dose for completers at endpoint in the flexible-dose studies was 104.75 mg/day. The fixed-dose study evaluated duloxetine delayed-release capsule doses of 60 mg once daily (N=168) and 120 mg once daily (N=170) compared to placebo (N=175) over a 9-week treatment period. While a 120 mg/day dose was shown to be effective, there is no evidence that doses greater than 60 mg/day confer additional benefit.
In all 3 studies, duloxetine delayed-release capsules demonstrated superiority over placebo as measured by greater improvement in the Hamilton Anxiety Scale (HAM-A) total score (Studies 1 to 3 in Table 8) and by the Sheehan Disability Scale (SDS) global functional impairment score. The SDS is a composite measurement of the extent emotional symptoms disrupt patient functioning in 3 life domains: work/school, social life/leisure activities, and family life/home responsibilities.
In another study, 887 patients meeting DSM-IV-TR criteria for GAD received duloxetine delayed-release capsules 60 mg to 120 mg once daily during an initial 26-week open-label treatment phase. Four hundred and twenty-nine patients who responded to open-label treatment (defined as meeting the following criteria at weeks 24 and 26: a decrease from baseline HAM-A total score by at least 50% to a score no higher than 11, and a Clinical Global Impressions of Improvement [CGI-Improvement] score of 1 or 2) were randomly assigned to continuation of duloxetine delayed-release capsules at the same dose (N=216) or to placebo (N=213) and were observed for relapse. Of the patients randomized, 73% had been in a responder status for at least 10 weeks.
Relapse was defined as an increase in CGI-Severity score at least 2 points to a score greater than or equal to 4 and a MINI (Mini-International Neuropsychiatric Interview) diagnosis of GAD (excluding duration), or discontinuation due to lack of efficacy. Patients taking duloxetine delayed-release capsules experienced a statistically significantly longer time to relapse of GAD than did patients taking placebo (Study 4 in Figure 2).
Subgroup analyses did not indicate that there were any differences in treatment outcomes as a function of age or gender.
Table 8: Summary of the Primary Efficacy Results for Studies in General Anxiety Disorder Study
Primary Efficacy Measure
Number
Mean Baseline
LS Mean Change from
Placebo-subtracted
Treatment Group
Score (SD)
Baseline (SE)
Differencea (95% CI)
Study 1
Duloxetine Delayed-Release Capsules (60 mg/day)b
25.1 (7.18)
-12.8 (0.68)
-4.4 (-6.2, -2.5)
(HAM-A)
Duloxetine Delayed-Release Capsules (120 mg/day)b
25.1 (7.24)
-12.5 (0.67)
-4.1 (-5.9, -2.3)
Placebo
25.8 (7.66)
-8.4 (0.67)
--
Study 2
Duloxetine Delayed-Release Capsules (60 to 120 mg/day)b
22.5 (7.44)
-8.1 (0.70)
-2.2 (-4.2, -0.3)
(HAM-A)
Placebo
23.5 (7.91)
-5.9 (0.70)
--
Study 3
Duloxetine Delayed-Release Capsules (60 to 120 mg/day)b
25.8 (5.66)
-11.8 (0.69)
-2.6 (-4.5, -0.7)
(HAM-A)
Placebo
25.0 (5.82)
-9.2 (0.67)
--
SD: standard deviation; SE: standard error; LS Mean: least-squares mean; CI: confidence interval, not adjusted for multiplicity in trials where multiple dose groups were included.
a Difference (drug minus placebo) in least squares mean change from baseline.
b Dose statistically significantly superior to placebo.
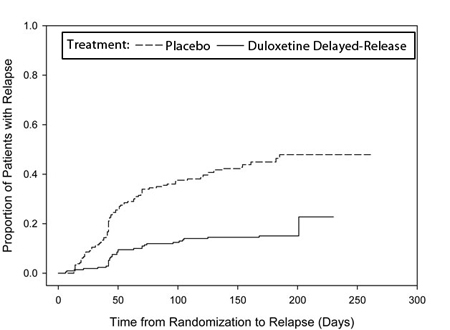
Figure 2: Kaplan-Meier Estimation of Cumulative Proportion of Patients with Relapse (GAD Study 4)
Pediatric use information for patients ages 7 to 17 years is approved for Eli Lilly and Company, Inc.'s CYMBALTA® (duloxetine) delayed-release capsules. However, due to Eli Lilly and Company, Inc.'s marketing exclusivity rights, this drug product is not labeled with that pediatric information.
14.3 Diabetic Peripheral Neuropathic Pain
The efficacy of duloxetine delayed-release capsules for the management of neuropathic pain associated with diabetic peripheral neuropathy was established in 2 randomized, 12-week, double-blind, placebo-controlled, fixed-dose studies in adult patients having diabetic peripheral neuropathic pain for at least 6 months. Study DPNP-1 and Study DPNP-2 enrolled a total of 791 patients of whom 592 (75%) completed the studies. Patients enrolled had Type I or II diabetes mellitus with a diagnosis of painful distal symmetrical sensorimotor polyneuropathy for at least 6 months. The patients had a baseline pain score of greater than or equal to 4 on an 11-point scale ranging from 0 (no pain) to 10 (worst possible pain). Patients were permitted up to 4 g of acetaminophen per day as needed for pain, in addition to duloxetine delayed-release capsules. Patients recorded their pain daily in a diary.
Both studies compared duloxetine delayed-release capsules 60 mg once daily or 60 mg twice daily with placebo. DPNP-1 additionally compared duloxetine delayed-release capsules 20 mg with placebo. A total of 457 patients (342 duloxetine delayed-release capsules, 115 placebo) were enrolled in DPNP-1 and a total of 334 patients (226 duloxetine delayed-release capsules, 108 placebo) were enrolled in DPNP-2. Treatment with duloxetine delayed-release capsules 60 mg one or two times a day statistically significantly improved the endpoint mean pain scores from baseline and increased the proportion of patients with at least a 50% reduction in pain scores from baseline. For various degrees of improvement in pain from baseline to study endpoint, Figures 3 and 4 show the fraction of patients achieving that degree of improvement. The figures are cumulative, so that patients whose change from baseline is, for example, 50%, are also included at every level of improvement below 50%. Patients who did not complete the study were assigned 0% improvement. Some patients experienced a decrease in pain as early as week 1, which persisted throughout the study.
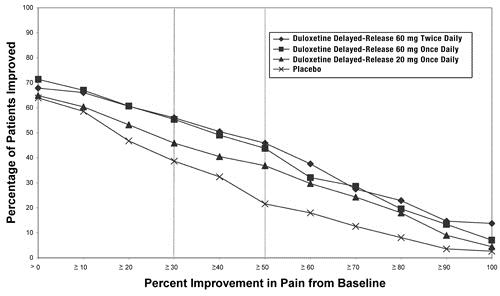
Figure 3: Percentage of Patients Achieving Various Levels of Pain Relief as Measured by 24-Hour Average Pain Severity - DPNP-1
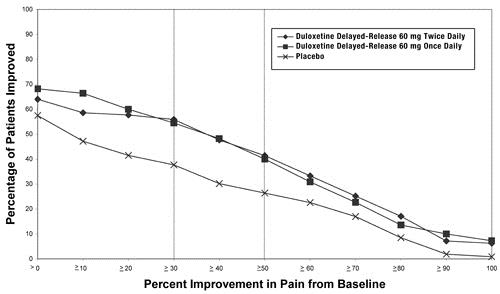
Figure 4: Percentage of Patients Achieving Various Levels of Pain Relief as Measured by 24-Hour Average Pain Severity - DPNP-2
14.4 Fibromyalgia
The efficacy of duloxetine delayed-release capsules for the management of fibromyalgia was established in two randomized, double-blind, placebo-controlled, fixed-dose studies in adult patients meeting the American College of Rheumatology criteria for fibromyalgia (a history of widespread pain for 3 months, and pain present at 11 or more of the 18 specific tender point sites). Study FM-1 was three months in duration and enrolled female patients only. Study FM-2 was six months in duration and enrolled male and female patients. Approximately 25% of participants had a comorbid diagnosis of major depressive disorder (MDD). FM-1 and FM-2 enrolled a total of 874 patients of whom 541 (62%) completed the studies. The patients had a baseline pain score of 6.5 on an 11-point scale ranging from 0 (no pain) to 10 (worse possible pain).
Both studies compared duloxetine delayed-release capsules 60 mg once daily or 120 mg daily (given in divided doses in FM-1 and as a single daily dose in FM-2) with placebo. FM-2 additionally compared duloxetine delayed-release capsules 20 mg with placebo during the initial three months of a six-month study. A total of 354 patients (234 duloxetine delayed-release capsules, 120 placebo) were enrolled in FM-1 and a total of 520 patients (376 duloxetine delayed-release capsules, 144 placebo) were enrolled in FM-2 (5% male, 95% female). Treatment with duloxetine delayed-release capsules 60 mg or 120 mg daily statistically significantly improved the endpoint mean pain scores from baseline and increased the proportion of patients with at least a 50% reduction in pain score from baseline. Pain reduction was observed in patients both with and without comorbid MDD. However, the degree of pain reduction may be greater in patients with comorbid MDD. For various degrees of improvement in pain from baseline to study endpoint, Figures 5 and 6 show the fraction of patients achieving that degree of improvement. The figures are cumulative so that patients whose change from baseline is, for example, 50%, are also included at every level of improvement below 50%. Patients who did not complete the study were assigned 0% improvement. Some patients experienced a decrease in pain as early as week 1, which persisted throughout the study. Improvement was also demonstrated on measures of function (Fibromyalgia Impact Questionnaires) and patient global impression of change (PGI). Neither study demonstrated a benefit of 120 mg compared to 60 mg, and a higher dose was associated with more adverse reactions and premature discontinuations of treatment.
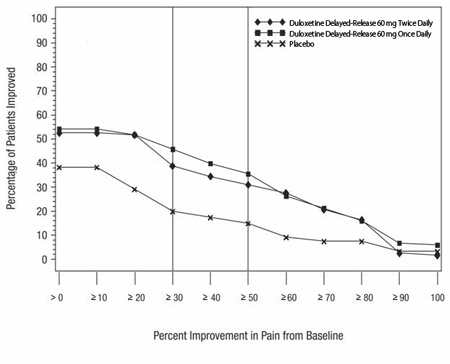
Figure 5: Percentage of Patients Achieving Various Levels of Pain Relief as Measured by 24-Hour Average Pain Severity - FM-1
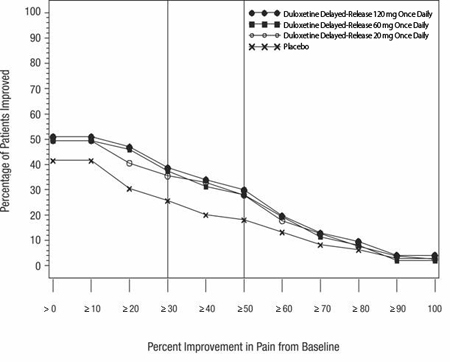
Figure 6: Percentage of Patients Achieving Various Levels of Pain Relief as Measured by 24-Hour Average Pain Severity - FM-2
Additionally, the benefit of up-titration in non-responders to duloxetine delayed-release capsules at 60 mg/day was evaluated in a separate study. Patients were initially treated with duloxetine delayed-release capsules 60 mg once daily for eight weeks in open-label fashion.
Subsequently, completers of this phase were randomized to double-blind treatment with duloxetine delayed-release capsules at either 60 mg once daily or 120 mg once daily. Those patients who were considered non-responders, where response was defined as at least a 30% reduction in pain score from baseline at the end of the 8-week treatment, were no more likely to meet response criteria at the end of 60 weeks of treatment if blindly titrated to duloxetine delayed-release capsules 120 mg as compared to those who were blindly continued on duloxetine delayed-release capsules 60 mg.
14.5 Chronic Musculoskeletal Pain
Duloxetine delayed-release capsules are indicated for the management of chronic musculoskeletal pain. This has been established in studies in patients with chronic low back pain and chronic pain due to osteoarthritis.
Studies in Chronic Low Back Pain
The efficacy of duloxetine delayed-release capsules in chronic low back pain (CLBP) was assessed in two double-blind, placebo-controlled, randomized clinical trials of 13-weeks duration (Study CLBP-1 and Study CLBP-2), and one of 12-weeks duration (CLBP-3). CLBP-1 and CLBP-3 demonstrated efficacy of duloxetine delayed-release capsules in the treatment of chronic low back pain. Patients in all studies had no signs of radiculopathy or spinal stenosis.
Study CLBP-1: Two hundred thirty-six adult patients (N=115 on duloxetine delayed-release capsules, N=121 on placebo) enrolled and 182 (77%) completed 13-week treatment phase. After 7 weeks of treatment, duloxetine delayed-release capsules patients with less than 30% reduction in average daily pain and who were able to tolerate duloxetine delayed-release capsules 60 mg once daily had their dose of duloxetine delayed-release capsules, in a double-blinded fashion, increased to 120 mg once daily for the remainder of the study. Patients had a mean baseline pain rating of 6 on a numerical rating scale ranging from 0 (no pain) to 10 (worst possible pain). After 13 weeks of treatment, patients taking duloxetine delayed-release capsules 60 mg to 120 mg daily had a significantly greater pain reduction compared to placebo. Randomization was stratified by the patients’ baseline NSAIDs-use status. Subgroup analyses did not indicate that there were differences in treatment outcomes as a function of NSAIDs use.
Study CLBP-2: Four hundred and four patients were randomized to receive fixed doses of duloxetine delayed-release capsules daily or a matching placebo (N=59 on duloxetine delayed-release capsules 20 mg, N=116 on duloxetine delayed-release capsules 60 mg, N=112 on duloxetine delayed-release capsules 120 mg, N=117 on placebo) and 267 (66%) completed the entire 13-week study. After 13 weeks of treatment, none of the three duloxetine delayed-release capsule doses showed a statistically significant difference in pain reduction compared to placebo.
Study CLBP-3: Four hundred and one patients were randomized to receive fixed doses of duloxetine delayed-release capsules 60 mg daily or placebo (N=198 on duloxetine delayed-release capsules, N=203 on placebo), and 303 (76%) completed the study. Patients had a mean baseline pain rating of 6 on a numerical rating scale ranging from 0 (no pain) to 10 (worst possible pain). After 12 weeks of treatment, patients taking duloxetine delayed-release capsules 60 mg daily had significantly greater pain reduction compared to placebo.
For various degrees of improvement in pain from baseline to study endpoint, Figures 7 and 8 show the fraction of patients in CLBP-1 and CLBP-3 achieving that degree of improvement. The figures are cumulative, so that patients whose change from baseline is, for example, 50%, are also included at every level of improvement below 50%. Patients who did not complete the study were assigned the value of 0% improvement.
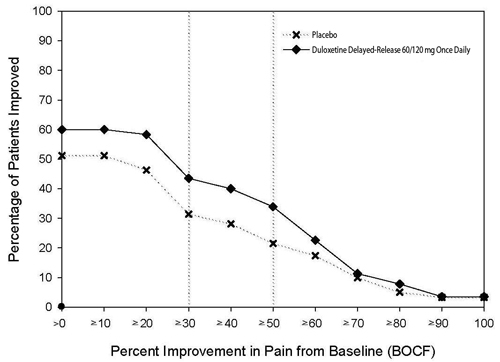
Figure 7: Percentage of Patients Achieving Various Levels of Pain Relief as Measured by 24-Hour Average Pain Severity – CLBP-1
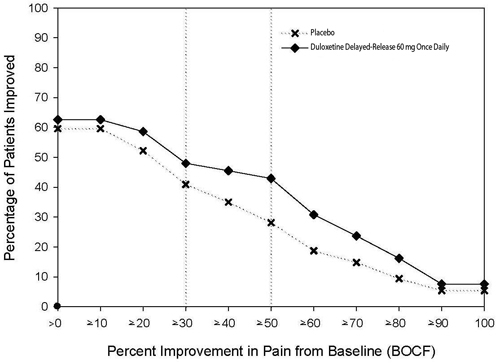
Figure 8: Percentage of Patients Achieving Various Levels of Pain Relief as Measured by 24-Hour Average Pain Severity – CLBP-3
Studies in Chronic Pain Due to Osteoarthritis
The efficacy of duloxetine delayed-release capsules in chronic pain due to osteoarthritis was assessed in 2 double-blind, placebo-controlled, randomized clinical trials of 13-weeks duration (Study OA-1 and Study OA-2). All patients in both studies fulfilled the ACR clinical and radiographic criteria for classification of idiopathic osteoarthritis of the knee. Randomization was stratified by the patients’ baseline NSAIDs-use status. Patients assigned to duloxetine delayed-release capsules started treatment in both studies at a dose of 30 mg once daily for one week. After the first week, the dose of duloxetine delayed-release capsules was increased to 60 mg once daily. After 7 weeks of treatment with duloxetine delayed-release capsules 60 mg once daily, in OA-1 patients with sub-optimal response to treatment (less than 30% pain reduction) and tolerated duloxetine delayed-release capsules 60 mg once daily had their dose increased to 120 mg. However, in OA-2, all patients, regardless of their response to treatment after 7 weeks, were re-randomized to either continue receiving duloxetine delayed-release capsules 60 mg once daily or have their dose increased to 120 mg once daily for the remainder of the study. Patients in the placebo treatment groups in both studies received a matching placebo for the entire duration of studies. For both studies, efficacy analyses were conducted using 13-week data from the combined duloxetine delayed-release capsules 60 mg and 120 mg once daily treatment groups compared to the placebo group.
Study OA-1: Two hundred fifty-six patients (N=128 on duloxetine delayed-release capsules, N=128 on placebo) enrolled and 204 (80%) completed the study. Patients had a mean baseline pain rating of 6 on a numerical rating scale ranging from 0 (no pain) to 10 (worst possible pain). After 13 weeks of treatment, patients taking duloxetine delayed-release capsules had significantly greater pain reduction. Subgroup analyses did not indicate that there were differences in treatment outcomes as a function of NSAIDs use.
Study OA-2: Two hundred thirty-one patients (N=111 on duloxetine delayed-release capsules, N=120 on placebo) enrolled and 173 (75%) completed the study. Patients had a mean baseline pain of 6 on a numerical rating scale ranging from 0 (no pain) to 10 (worst possible pain). After 13 weeks of treatment, patients taking duloxetine delayed-release capsules did not show a significantly greater pain reduction.
In Study OA-1, for various degrees of improvement in pain from baseline to study endpoint, Figure 7 shows the fraction of patients achieving that degree of improvement. The figure is cumulative, so that patients whose change from baseline is, for example, 50%, are also included at every level of improvement below 50%. Patients who did not complete the study were assigned the value of 0% improvement.
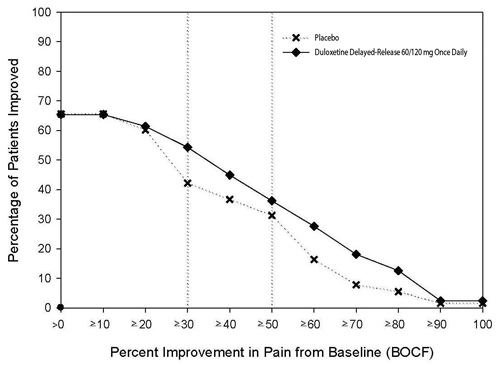
Figure 9: Percentage of Patients Achieving Various Levels of Pain Relief as Measured by 24-Hour Average Pain Severity – OA-1
-
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 How Supplied
Duloxetine hydrochloride, USP is available as delayed-release capsules in the following strengths:
20 mg – Each capsule with blue opaque cap and body, printed with
 and 2890 on both cap and body in black ink contains 22.4 mg of duloxetine hydrochloride, USP equivalent to 20 mg of duloxetine. Capsules are supplied in bottles of 60 (NDC: 0228-2890-06).
and 2890 on both cap and body in black ink contains 22.4 mg of duloxetine hydrochloride, USP equivalent to 20 mg of duloxetine. Capsules are supplied in bottles of 60 (NDC: 0228-2890-06).30 mg – Each capsule with gray opaque body and blue opaque cap, printed with
 and 2891 on both cap and body in black ink contains 33.7 mg of duloxetine hydrochloride, USP equivalent to 30 mg of duloxetine. Capsules are supplied in bottles of 30 (NDC: 0228-2891-03) and bottles of 500 (0228-2891-50).
and 2891 on both cap and body in black ink contains 33.7 mg of duloxetine hydrochloride, USP equivalent to 30 mg of duloxetine. Capsules are supplied in bottles of 30 (NDC: 0228-2891-03) and bottles of 500 (0228-2891-50).60 mg – Each capsule with gray opaque body and white opaque cap, printed with
 and 2892 on both cap and body in black ink contains 67.3 mg of duloxetine hydrochloride, USP equivalent to 60 mg of duloxetine. Capsules are supplied in bottles of 30 (NDC: 0228-2892-03) and bottles of 1000 (0228-2892-96).
and 2892 on both cap and body in black ink contains 67.3 mg of duloxetine hydrochloride, USP equivalent to 60 mg of duloxetine. Capsules are supplied in bottles of 30 (NDC: 0228-2892-03) and bottles of 1000 (0228-2892-96). -
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Medication Guide).
- Suicidal Thoughts and Behaviors ― Advise patients, their families, and their caregivers to look for the emergence of suicidal ideation and behavior, especially during treatment and when the dose is adjusted up or down and instruct them to report such symptoms to their healthcare provider [see Boxed Warning, and Warnings and Precautions (5.1)].
- Duloxetine delayed-release capsules should be swallowed whole and should not be chewed or crushed, nor should the capsule be opened and its contents be sprinkled on food or mixed with liquids. All of these might affect the enteric coating.
- Hepatotoxicity ― Inform patients that severe liver problems, sometimes fatal, have been reported in patients treated with duloxetine delayed-release capsules. Instruct patients to talk to their healthcare provider if they develop itching, right upper belly pain, dark urine, or yellow skin/eyes while taking duloxetine delayed-release capsules, which may be signs of liver problems. Instruct patients to talk to their healthcare provider about their alcohol consumption. Use of duloxetine delayed-release capsules with heavy alcohol intake may be associated with severe liver injury [see Warnings and Precautions (5.2)].
- Alcohol ― Although duloxetine delayed-release capsules do not increase the impairment of mental and motor skills caused by alcohol, use of duloxetine delayed-release capsules concomitantly with heavy alcohol intake may be associated with severe liver injury. For this reason, duloxetine delayed-release capsules should not be prescribed for patients with substantial alcohol use [see Warnings and Precautions (5.2) and Drug Interactions (7.15)].
- Orthostatic Hypotension, Falls and Syncope ― Advise patients of the risk of orthostatic hypotension, falls and syncope, especially during the period of initial use and subsequent dose escalation, and in association with the use of concomitant drugs that might potentiate the orthostatic effect of duloxetine delayed-release capsules [see Warnings and Precautions (5.3)].
-
Serotonin Syndrome ― Caution patients about the risk of serotonin syndrome with the concomitant use of duloxetine delayed-release capsules and other serotonergic agents including triptans, tricyclic antidepressants, fentanyl, lithium, tramadol, buspirone, tryptophan, amphetamines, and St. John’s Wort [see Contraindications (4), Warnings and Precautions (5.4), and Drug Interactions (7.14)].
Advise patients of the signs and symptoms associated with serotonin syndrome that may include mental status changes (e.g., agitation, hallucinations, delirium, and coma), autonomic instability (e.g., tachycardia, labile blood pressure, dizziness, diaphoresis, flushing, hyperthermia), neuromuscular changes (e.g., tremor, rigidity, myoclonus, hyperreflexia, incoordination), seizures, and/or gastrointestinal symptoms (e.g., nausea, vomiting, diarrhea). Caution patients to seek medical care immediately if they experience these symptoms. - Abnormal Bleeding ― Caution patients about the concomitant use of duloxetine delayed-release capsules and NSAIDs, aspirin, warfarin, or other drugs that affect coagulation since combined use of psychotropic drugs that interfere with serotonin reuptake and these agents has been associated with an increased risk of bleeding [see Warnings and Precautions (5.5) and Use in Specific Populations (8.1)].
- Severe Skin Reactions ― Caution patients that duloxetine delayed-release capsules may cause serious skin reactions. This may need to be treated in a hospital and may be life-threatening. Counsel patients to call their doctor right away or get emergency help if they have skin blisters, peeling rash, sores in their mouth, hives, or any other allergic reactions [see Warnings and Precautions (5.6)].
- Discontinuation of Treatment ― Instruct patients that discontinuation of duloxetine delayed-release capsules may be associated with symptoms such as dizziness, headache, nausea, diarrhea, paresthesia, irritability, vomiting, insomnia, anxiety, hyperhidrosis, and fatigue, and should be advised not to alter their dosing regimen, or stop taking duloxetine delayed-release capsules without consulting their physician [see Warnings and Precautions (5.7)].
- Activation of Mania or Hypomania ― Adequately screen patients with depressive symptoms for risk of bipolar disorder (e.g. family history of suicide, bipolar disorder, and depression) prior to initiating treatment with duloxetine delayed-release capsules. Advise patients to report any signs or symptoms of a manic reaction such as greatly increased energy, severe trouble sleeping, racing thoughts, reckless behavior, talking more or faster than usual, unusually grand ideas, and excessive happiness or irritability [see Warnings and Precautions (5.8)].
- Angle-Closure Glaucoma ― Advise patients that taking duloxetine delayed-release capsules can cause mild pupillary dilation, which in susceptible individuals, can lead to an episode of angle-closure glaucoma. Pre-existing glaucoma is almost always open-angle glaucoma because angle-closure glaucoma, when diagnosed, can be treated definitively with iridectomy. Open-angle glaucoma is not a risk factor for angle-closure glaucoma. Patients may wish to be examined to determine whether they are susceptible to angle-closure, and have a prophylactic procedure (e.g., iridectomy), if they are susceptible. [See Warnings and Precautions (5.9)].
- Seizures ― Advise patients to inform their physician if they have a history of seizure disorder [see Warnings and Precautions (5.10)].
- Effects on Blood Pressure - Caution patients that duloxetine delayed-release capsules may cause an increase in blood pressure [see Warnings and Precautions (5.11)].
- Concomitant Medications ― Advise patients to inform their physicians if they are taking, or plan to take, any prescription or over-the-counter medications, since there is a potential for interactions [see Dosage and Administration (2.8, 2.9), Contraindications (4), Warnings and Precautions (5.4, 5.12), and Drug Interactions (7)].
- Hyponatremia ― Advise patients that hyponatremia has been reported as a result of treatment with SNRIs and SSRIs, including duloxetine delayed-release capsules. Advise patients of the signs and symptoms of hyponatremia [see Warnings and Precautions (5.13)].
- Concomitant Illnesses ― Advise patients to inform their physicians about all of their medical conditions [see Warnings and Precautions (5.14)].
- Duloxetine delayed-release capsules are in a class of medicines that may affect urination. Instruct patients to consult with their healthcare provider if they develop any problems with urine flow [see Warnings and Precautions (5.15)].
- Pregnancy
- Advise pregnant women to notify their healthcare provider if they become pregnant or intend to become pregnant during treatment with duloxetine delayed-release capsules.
- Advise patients that duloxetine delayed-release capsules use during the month before delivery may lead to an increased risk for postpartum hemorrhage and may increase the risk of neonatal complications requiring prolonged hospitalization, respiratory support, and tube feeding.
- Advise pregnant women that there is a risk of relapse with discontinuation of antidepressants.
- Advise patients that there is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to duloxetine during pregnancy [see Use in Specific Populations (8.1)].
- Lactation ― Advise breastfeeding women using duloxetine delayed-release capsules to monitor infants for sedation, poor feeding and poor weight gain and to seek medical care if they notice these signs [see Use in Specific Populations (8.2)].
- Pediatric Use ―
Pediatric use information for patients ages 7 to 17 years with GAD is approved for Eli Lilly and Company, Inc.'s Cymbalta® (duloxetine) delayed-release capsules. However, due to Eli Lilly and Company, Inc.'s marketing exclusivity rights, this drug product is not labeled with that pediatric information. The safety and effectiveness of CYMBALTA have not been established in pediatric patients less than 18 years of age with other indications.
The safety and effectiveness of duloxetine delayed-release capsules have not been established in pediatric patients less than 18 years of age with other indications. [See Use in SpecificPopulations (8.4)].
- Interference with Psychomotor Performance ― Any psychoactive drug may impair judgment, thinking, or motor skills. Although in controlled studies duloxetine delayed-release capsules have not been shown to impair psychomotor performance, cognitive function, or memory, it may be associated with sedation and dizziness. Therefore, caution patients about operating hazardous machinery including automobiles, until they are reasonably certain that duloxetine delayed-release capsules therapy does not affect their ability to engage in such activities.
Manufactured by:
Actavis Elizabeth LLC
Elizabeth, NJ 07207 USADistributed by:
Actavis Pharma, Inc.
Parsippany, NJ 07054 USARev. A 10/2019
-
MEDICATION GUIDE
Duloxetine (doo lox' e teen)
Delayed-Release CapsulesRead this Medication Guide before you start taking duloxetine delayed-release capsules and each time you get a refill. There may be new information. This information does not take the place of talking to your healthcare provider about your medical condition or treatment.
Talk to your healthcare provider about:
- all risks and benefits of treatment with antidepressant medicines
- all treatment choices for depression or other serious mental illness
What is the most important information I should know about antidepressant medicines, depression, other serious mental illnesses, and suicidal thoughts or actions?
1. Duloxetine delayed-release capsules and other antidepressant medicines may increase suicidal thoughts or actions in some children, teenagers, or young adults within the first few months of treatment or when the dose is changed.
2. Depression and other serious mental illnesses are the most important causes of suicidal thoughts or actions. Some people may have a particularly high risk of having suicidal thoughts or actions. These include people who have (or have a family history of) bipolar illness (also called manic-depressive illness).
3. How can I watch for and try to prevent suicidal thoughts and actions?
- Pay close attention to any changes in mood, behavior, actions, thoughts, or feelings, especially sudden changes. This is very important when an antidepressant medicine is started or when the dose is changed.
- Call your healthcare provider right away to report new or sudden changes in mood, behavior, thoughts, or feelings.
- Keep all follow-up visits with your healthcare provider as scheduled. Call your healthcare provider between visits as needed, especially if you have concerns about symptoms.
Call your healthcare provider right away if you have any of the following symptoms or feelings, especially if they are new, worse, or worry you. In an emergency, call 911.
- attempts to commit suicide
- acting on dangerous impulses
- acting aggressive, being angry, or violent
- thoughts about suicide or dying
- new or worse depression
- new or worse anxiety
- panic attacks
- feeling very agitated or restless
- new or worse irritability
- trouble sleeping
- an extreme increase in activity or talking (mania)
- other unusual changes in behavior or mood
What else do I need to know about antidepressant medicines?
- Never stop an antidepressant medicine without first talking to a healthcare provider.
Stopping an antidepressant medicine suddenly can cause other symptoms.
- Antidepressants are medicines used to treat depression and other illnesses. It is important to discuss all the risks of treating depression and also the risks of not treating it. Patients should discuss all treatment choices with your healthcare provider, not just the use of antidepressants.
- Antidepressant medicines have other side effects. Talk to your healthcare provider about the side effects of the medicine prescribed for you or your family member.
- Antidepressant medicines can interact with other medicines. Know all of the medicines that you or your family member takes. Keep a list of all medicines to show your healthcare provider. Do not start new medicines without first checking with your healthcare provider.
What are duloxetine delayed-release capsules?
Duloxetine delayed-release capsules are a prescription medicine used to treat a certain type of depression called Major Depressive Disorder (MDD). Duloxetine delayed-release capsules belong to a class of medicines known as SNRIs (or serotonin-norepinephrine reuptake inhibitors).
Duloxetine delayed-release capsules are also used to treat or manage:
- Generalized Anxiety Disorder (GAD)
- Diabetic Peripheral Neuropathic Pain (DPNP)
- Fibromyalgia (FM)
- Chronic Musculoskeletal Pain
Who should not take duloxetine delayed-release capsules?
Do Not take duloxetine delayed-release capsules if you:
- take a Monoamine Oxidase Inhibitor (MAOI). Ask your healthcare provider or pharmacist if you are not sure if you take an MAOI, including the antibiotic linezolid or intravenous methylene blue.
- Do not take an MAOI within 5 days of stopping duloxetine delayed-release capsules unless directed to do so by your healthcare provider.
- Do not start duloxetine delayed-release capsules if you stopped taking an MAOI in the last 14 days unless directed to do so by your healthcare provider.
People who take duloxetine delayed-release capsules close in time to an MAOI may have a serious problem called Serotonin Syndrome (see “What are the possible side effects of duloxetine delayed-release capsules?”).
What should I tell my healthcare provider before taking duloxetine delayed-release capsules?
Before starting duloxetine delayed-release capsules, tell your healthcare provider if you:
- have heart problems or high blood pressure
- have diabetes (duloxetine delayed-release capsules treatment makes it harder for some people with diabetes to control their blood sugar)
- have liver problems
- have kidney problems
- have glaucoma
- have or had seizures or convulsions
- have bipolar disorder or mania
- have low sodium levels in your blood
- have delayed stomach emptying
- have or had bleeding problems
- are pregnant or plan to become pregnant. Duloxetine delayed-release capsules may harm your unborn baby. Talk to your healthcare provider about the risk to your unborn baby if you take duloxetine delayed-release capsules during pregnancy.
- Tell your healthcare provider right away if you become pregnant or think you are pregnant during treatment with duloxetine delayed-release capsules.
- are breastfeeding or plan to breastfeed. Duloxetine hydrochloride passes into your breast milk and may harm your baby. Talk to your healthcare provider about the best way to feed your baby while taking duloxetine delayed-release capsules.
Tell your healthcare provider about all the medicines that you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. Duloxetine delayed-release capsules and some medicines may interact with each other, may not work as well, or may cause serious side effects.
Especially tell your healthcare provider if you take:
- triptans used to treat migraine headache
- medicines used to treat mood, anxiety, psychotic or thought disorders, including tricyclics, lithium, buspirone, SSRIs, SNRIs or MAOIs
- tramadol and fentanyl
- amphetamines
- cimetidine
- the antibiotics ciprofloxacin, enoxacin
- medicine to treat irregular heart rate (like propafenone, flecainide, quinidine)
- theophylline
- the blood thinner warfarin (Coumadin, Jantoven)
- non-steroidal anti-inflammatory drug (NSAID)(like ibuprofen, naproxen or aspirin).
- over-the-counter supplements such as tryptophan or St. John’s Wort
- thioridazine (Mellaril). Mellaril together with duloxetine delayed-release capsules can cause serious heart rhythm problems or sudden death.
Ask your healthcare provider for a list of these medicines if you are not sure. Do not take duloxetine delayed-release capsules with any other medicine that contain duloxetine.
How should I take duloxetine delayed-release capsules?
- Take duloxetine delayed-release capsules exactly as your healthcare provider tells you to take it. Your healthcare provider may need to change the dose of duloxetine delayed-release capsules until it is the right dose for you.
- Swallow duloxetine delayed-release capsules whole. Do not chew or crush duloxetine delayed-release capsules.
- Do not open the capsule and sprinkle on food or mix with liquids. Opening the capsule may affect how well duloxetine delayed-release capsules work.
- Duloxetine delayed-release capsules may be taken with or without food.
- If you miss a dose of duloxetine delayed-release capsules, take the missed dose as soon as you remember. If it is almost time for the next dose, skip the missed dose and take your next dose at the regular time. Do not take two doses of duloxetine delayed-release capsules at the same time.
- If you take too many duloxetine delayed-release capsules, call your healthcare provider or poison control center at 1-800-222-1222 right away, or get emergency treatment.
- When switching from another antidepressant to duloxetine delayed-release capsules your healthcare provider may want to lower the dose of the initial antidepressant first to potentially avoid side effects.
What should I avoid while taking duloxetine delayed-release capsules?
- Duloxetine delayed-release capsules can cause sleepiness or may affect your ability to make decisions, think clearly, or react quickly. You should not drive, operate heavy machinery, or do other dangerous activities until you know how duloxetine delayed-release capsules affect you.
- Use of duloxetine delayed-release capsules concomitantly with heavy alcohol intake may be associated with severe liver injury. Avoid heavy alcohol use while taking duloxetine delayed-release capsules.
What are the possible side effects of duloxetine delayed-release capsules?
Duloxetine delayed-release capsules may cause serious side effects, including: See “What is the most important information I should know about duloxetine delayed-release capsules?”
Common possible side effects in people who take duloxetine delayed-release capsules include:
1. liver damage. Symptoms may include:
- itching
- right upper abdominal pain
- dark urine
- yellow skin or eyes
- enlarged liver
- increased liver enzymes
2. changes in blood pressure and falls. Monitor your blood pressure before starting and throughout treatment.
Duloxetine delayed-release capsules may:
- increase your blood pressure.
- decrease your blood pressure when standing and cause dizziness or fainting, mostly when first starting duloxetine delayed-release capsules or when increasing the dose.
- increase risk of falls, especially in elderly.
3. Serotonin Syndrome: This condition can be life-threatening and symptoms may include:
- agitation, hallucinations, coma or other changes in mental status
- coordination problems or muscle twitching (overactive reflexes)
- racing heartbeat, high or low blood pressure
- sweating or fever
- nausea, vomiting, or diarrhea
- muscle rigidity
- dizziness
- flushing
- tremor
- seizures
4. abnormal bleeding: Duloxetine delayed-release capsules and other antidepressant medicines may increase your risk of bleeding or bruising, especially if you take the blood thinner warfarin (Coumadin, Jantoven), a non-steroidal anti-inflammatory drug (NSAIDs, like ibuprofen or naproxen), or aspirin.
5. severe skin reactions: Duloxetine delayed-release capsules may cause serious skin reactions that may require stopping its use. This may need to be treated in a hospital and may be life-threatening. Call your healthcare provider right away or get emergency help if you have skin blisters, peeling rash, sores in the mouth, hives or any other allergic reactions.
6. discontinuation symptoms: Do not stop duloxetine delayed-release capsules without first talking to your healthcare provider. Stopping duloxetine delayed-release capsules too quickly or changing from another antidepressant too quickly may result in serious symptoms including:
- anxiety
- irritability
- feeling tired or problems sleeping
- headache
- sweating
- dizziness
- electric shock-like sensations
- vomiting or nausea
- diarrhea
7. manic episodes:
- greatly increased energy
- severe trouble sleeping
- racing thoughts
- reckless behavior
- unusually grand ideas
- excessive happiness or irritability
- talking more or faster than usual
8. visual problems:
- eye pain
- changes in vision
- swelling or redness in or around the eye
Only some people are at risk for these problems. You may want to undergo an eye examination to see if you are at risk and receive preventative treatment if you are.
9. seizures or convulsions
10. low salt (sodium) levels in the blood. Elderly people may be at greater risk for this.
- Symptoms may include:
- headache
- weakness or feeling unsteady
- confusion, problems concentrating or thinking or memory problems
11. problems with urination. Symptoms may include:
- decreased urine flow
- unable to pass any urine
The most common side effects of duloxetine delayed-release capsules include:
- nausea
- dry mouth
- sleepiness
- fatigue
- constipation
- loss of appetite
- increased sweating
- dizziness
Common possible side effects in children and adolescents who take duloxetine delayed-release capsules include:
- nausea
- decreased weight
- dizziness
Side effects in adults may also occur in children and adolescents who take duloxetine delayed-release capsules. Children and adolescents should have height and weight monitored during treatment.
Tell your healthcare provider if you have any side effect that bothers you or that does not go away.
These are not all the possible side effects of duloxetine delayed-release capsules. For more information, ask your healthcare provider or pharmacist.
Call your doctor for medical advice about side effects. You may report side effects to 1-800-FDA-1088.
How should I store duloxetine delayed-release capsules?
Store duloxetine delayed-release capsules at room temperature between 68°F to 77°F (20°C to 25°C).
Keep duloxetine delayed-release capsules and all medicines out of the reach of children.
General information about the safe and effective use of duloxetine delayed-release capsules.
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use duloxetine delayed-release capsules for a condition for which it was not prescribed. Do not give duloxetine delayed-release capsules to other people, even if they have the same symptoms that you have. It may harm them.
This Medication Guide summarizes the most important information about duloxetine delayed-release capsules. If you would like more information, talk with your healthcare provider. You may ask your healthcare provider or pharmacist for information about duloxetine delayed-release capsules that is written for healthcare professionals.
For more information about duloxetine delayed-release capsules call Actavis at 1-800-432-8534.
What are the ingredients in duloxetine delayed-release capsules?
Active ingredient: duloxetine hydrochloride
Inactive ingredients: ammonium hydroxide, black iron oxide, gelatin, hydroxypropyl cellulose, hydroxypropyl methylcellulose phthalate, hypromellose, potassium hydroxide, propylene glycol, shellac, sugar spheres (which contain sucrose and corn starch), talc, titanium dioxide, and triethyl citrate. The 20 mg and 30 mg capsules also contain FD&C Blue #1 Aluminum Lake.
This Medication Guide has been approved by the U.S. Food and Drug Administration.
Brands listed are trademarks of their respective owners.
Manufactured by:
Actavis Elizabeth LLC
Elizabeth, NJ 07207 USADistributed by:
Actavis Pharma, Inc.
Parsippany, NJ 07054 USARev. A 10/2019
-
PACKAGE LABEL.PRINCIPAL DISPLAY PANEL
NDC: 0228-2890-06
20 mg
Duloxetine
Delayed-Release
Capsules, USP
PHARMACIST: Dispense the Medication Guide provided separately to each patient.
60 Capsules
Rx Only
Actavis
-
PACKAGE LABEL.PRINCIPAL DISPLAY PANEL
NDC: 0228-2891-03
30 mg
Duloxetine
Delayed-Release
Capsules, USP
PHARMACIST: Dispense the Medication Guide provided separately to each patient.
30 Capsules
Rx Only
Actavis
-
PACKAGE LABEL.PRINCIPAL DISPLAY PANEL
NDC: 0228-2892-03
60 mg
Duloxetine
Delayed-Release
Capsules, USP
PHARMACIST: Dispense the Medication Guide provided separately to each patient.
30 Capsules
Rx Only
Actavis
-
INGREDIENTS AND APPEARANCE
DULOXETINE
duloxetine capsule, delayed release pelletsProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 0228-2890 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength DULOXETINE HYDROCHLORIDE (UNII: 9044SC542W) (DULOXETINE - UNII:O5TNM5N07U) DULOXETINE 20 mg Inactive Ingredients Ingredient Name Strength AMMONIA (UNII: 5138Q19F1X) FERROSOFERRIC OXIDE (UNII: XM0M87F357) GELATIN, UNSPECIFIED (UNII: 2G86QN327L) HYDROXYPROPYL CELLULOSE, UNSPECIFIED (UNII: 9XZ8H6N6OH) HYPROMELLOSE PHTHALATE (31% PHTHALATE, 40 CST) (UNII: G4U024CQK6) HYPROMELLOSE 2910 (15 MPA.S) (UNII: 36SFW2JZ0W) POTASSIUM HYDROXIDE (UNII: WZH3C48M4T) PROPYLENE GLYCOL (UNII: 6DC9Q167V3) SHELLAC (UNII: 46N107B71O) SUCROSE (UNII: C151H8M554) STARCH, CORN (UNII: O8232NY3SJ) TALC (UNII: 7SEV7J4R1U) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) TRIETHYL CITRATE (UNII: 8Z96QXD6UM) FD&C BLUE NO. 1 (UNII: H3R47K3TBD) Product Characteristics Color BLUE Score no score Shape CAPSULE Size 16mm Flavor Imprint Code 2890;2890 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 0228-2890-06 60 in 1 BOTTLE; Type 0: Not a Combination Product 12/17/2013 
Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA090776 12/17/2013 DULOXETINE
duloxetine capsule, delayed release pelletsProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 0228-2891 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength DULOXETINE HYDROCHLORIDE (UNII: 9044SC542W) (DULOXETINE - UNII:O5TNM5N07U) DULOXETINE 30 mg Inactive Ingredients Ingredient Name Strength AMMONIA (UNII: 5138Q19F1X) FERROSOFERRIC OXIDE (UNII: XM0M87F357) GELATIN, UNSPECIFIED (UNII: 2G86QN327L) HYDROXYPROPYL CELLULOSE, UNSPECIFIED (UNII: 9XZ8H6N6OH) HYPROMELLOSE PHTHALATE (31% PHTHALATE, 40 CST) (UNII: G4U024CQK6) HYPROMELLOSE 2910 (15 MPA.S) (UNII: 36SFW2JZ0W) POTASSIUM HYDROXIDE (UNII: WZH3C48M4T) PROPYLENE GLYCOL (UNII: 6DC9Q167V3) SHELLAC (UNII: 46N107B71O) SUCROSE (UNII: C151H8M554) STARCH, CORN (UNII: O8232NY3SJ) TALC (UNII: 7SEV7J4R1U) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) TRIETHYL CITRATE (UNII: 8Z96QXD6UM) FD&C BLUE NO. 1 (UNII: H3R47K3TBD) Product Characteristics Color GRAY, BLUE Score no score Shape CAPSULE Size 18mm Flavor Imprint Code 2891;2891 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 0228-2891-03 30 in 1 BOTTLE; Type 0: Not a Combination Product 12/17/2013 2 NDC: 0228-2891-50 500 in 1 BOTTLE; Type 0: Not a Combination Product 09/05/2014 
Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA090776 12/17/2013 DULOXETINE
duloxetine capsule, delayed release pelletsProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 0228-2892 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength DULOXETINE HYDROCHLORIDE (UNII: 9044SC542W) (DULOXETINE - UNII:O5TNM5N07U) DULOXETINE 60 mg Inactive Ingredients Ingredient Name Strength AMMONIA (UNII: 5138Q19F1X) FERROSOFERRIC OXIDE (UNII: XM0M87F357) GELATIN, UNSPECIFIED (UNII: 2G86QN327L) HYDROXYPROPYL CELLULOSE, UNSPECIFIED (UNII: 9XZ8H6N6OH) HYPROMELLOSE PHTHALATE (31% PHTHALATE, 40 CST) (UNII: G4U024CQK6) HYPROMELLOSE 2910 (15 MPA.S) (UNII: 36SFW2JZ0W) POTASSIUM HYDROXIDE (UNII: WZH3C48M4T) PROPYLENE GLYCOL (UNII: 6DC9Q167V3) SHELLAC (UNII: 46N107B71O) SUCROSE (UNII: C151H8M554) STARCH, CORN (UNII: O8232NY3SJ) TALC (UNII: 7SEV7J4R1U) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) TRIETHYL CITRATE (UNII: 8Z96QXD6UM) Product Characteristics Color GRAY, WHITE Score no score Shape CAPSULE Size 20mm Flavor Imprint Code 2892;2892 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 0228-2892-03 30 in 1 BOTTLE; Type 0: Not a Combination Product 12/17/2013 2 NDC: 0228-2892-96 1000 in 1 BOTTLE; Type 0: Not a Combination Product 09/05/2014 
Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA090776 12/17/2013 Labeler - Actavis Pharma, Inc. (119723554)
 2890”
2890”  2891”
2891”  2892”
2892” © 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.