SARCLISA- isatuximab injection, solution, concentrate
Sarclisa by
Drug Labeling and Warnings
Sarclisa by is a Prescription medication manufactured, distributed, or labeled by sanof-aventis U.S. LLC, Sanofi-Aventis Deutschland GmbH, Genzyme Corporation, Sanofi Chimie, Quality Assistance, S.A.. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use SARCLISA safely and effectively. See full prescribing information for SARCLISA.
SARCLISA® (isatuximab-irfc) injection, for intravenous use
Initial U.S. Approval: 2020INDICATIONS AND USAGE
SARCLISA is a CD38-directed cytolytic antibody indicated, in combination with pomalidomide and dexamethasone, for the treatment of adult patients with multiple myeloma who have received at least two prior therapies including lenalidomide and a proteasome inhibitor. (1)
DOSAGE AND ADMINISTRATION
- Premedicate with dexamethasone, acetaminophen, H2 antagonists, and diphenhydramine. (2.2)
- The recommended dose of SARCLISA is 10 mg/kg as an intravenous infusion every week for 4 weeks followed by every 2 weeks in combination with pomalidomide and dexamethasone until disease progression or unacceptable toxicity. (2.1)
- See Full Prescribing Information for instructions on preparation and administration. (2.4, 2.5)
DOSAGE FORMS AND STRENGTHS
CONTRAINDICATIONS
Patients with severe hypersensitivity to isatuximab-irfc or to any of its excipients (4)
WARNINGS AND PRECAUTIONS
- Infusion-Related Reactions: Interrupt SARCLISA and manage medically. Permanently discontinue for grade ≥3 reactions. (5.1)
- Neutropenia: Monitor complete blood cell counts periodically during treatment. Monitor patients with neutropenia for signs of infection. SARCLISA dose delays and the use of colony-stimulating factor may be required to allow improvement of neutrophil count. (5.2)
- Second Primary Malignancies (SPM): Monitor patients for the development of second primary malignancies, as per IMWG guidelines. (5.3)
- Laboratory Test Interference:
- Interference with Serological Testing (Indirect Antiglobulin Test): Type and screen patients prior to starting treatment. Inform blood banks that a patient has received SARCLISA. (5.4, 7.1)
- Interference with Serum Protein Electrophoresis and Immunofixation Tests: SARCLISA may interfere with the assays used to monitor M-protein, which may impact the determination of complete response. (5.4, 7.1)
- Embryo-Fetal Toxicity: Can cause fetal harm. (5.5)
ADVERSE REACTIONS
The most common adverse reactions (in ≥20% of patients) were neutropenia, infusion-related reactions, pneumonia, upper respiratory tract infection, and diarrhea. (6.1)
The most common hematology laboratory abnormalities (in ≥80% of patients) were anemia, neutropenia, lymphopenia, and thrombocytopenia.
To report SUSPECTED ADVERSE REACTIONS, contact sanofi-aventis U.S. LLC at 1-800-633-1610 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.
Revised: 3/2020
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dosage
2.2 Recommended Premedications
2.3 Dose Modifications
2.4 Preparation
2.5 Administration
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Infusion-Related Reactions
5.2 Neutropenia
5.3 Second Primary Malignancies
5.4 Laboratory Test Interference
5.5 Embryo-Fetal Toxicity
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
6.2 Immunogenicity
7 DRUG INTERACTIONS
7.1 Laboratory Test Interference
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.3 Females and Males of Reproductive Potential
8.4 Pediatric Use
8.5 Geriatric Use
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
14.1 Multiple Myeloma
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 How Supplied
16.2 Storage
16.3 Handling and Disposal
17 PATIENT COUNSELING INFORMATION
- * Sections or subsections omitted from the full prescribing information are not listed.
- 1 INDICATIONS AND USAGE
-
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dosage
- Administer pre-infusion medications [see Dosage and Administration (2.2)].
- SARCLISA should be administered by a healthcare professional, with immediate access to emergency equipment and appropriate medical support to manage infusion-related reactions if they occur [see Warnings and Precautions (5.1)].
The recommended dose of SARCLISA is 10 mg/kg actual body weight administered as an intravenous infusion in combination with pomalidomide and dexamethasone, according to the schedule in Table 1 [see Clinical Studies (14)].
Table 1: SARCLISA Dosing Schedule in Combination with Pomalidomide and Dexamethasone Cycle Dosing schedule Cycle 1 Days 1, 8, 15, and 22 (weekly) Cycle 2 and beyond Days 1, 15 (every 2 weeks) Each treatment cycle consists of a 28-day period. Treatment is repeated until disease progression or unacceptable toxicity.
SARCLISA is used in combination with pomalidomide and dexamethasone.
2.2 Recommended Premedications
Administer the following premedications prior to SARCLISA infusion to reduce the risk and severity of infusion-related reactions [see Warnings and Precautions (5.1)]:
- Dexamethasone 40 mg orally or intravenously (or 20 mg orally or intravenously for patients ≥75 years of age).
- Acetaminophen 650 mg to 1000 mg orally (or equivalent).
- H2 antagonists.
- Diphenhydramine 25 mg to 50 mg orally or intravenously (or equivalent). The intravenous route is preferred for at least the first 4 infusions.
The above recommended dose of dexamethasone (orally or intravenously) corresponds to the total dose to be administered only once before infusion as part of the premedication and of the backbone treatment, before SARCLISA and pomalidomide administration.
Administer the recommended premedication agents 15 to 60 minutes prior to starting a SARCLISA infusion.
2.3 Dose Modifications
No dose reduction of SARCLISA is recommended. Dose delay may be required to allow recovery of blood counts in the event of hematological toxicity [see Warnings and Precautions (5.2, 5.4)]. For information concerning drugs given in combination with SARCLISA, see manufacturer's prescribing information.
For other medicinal products that are administered with SARCLISA, refer to the respective current prescribing information.
2.4 Preparation
Prepare the solution for infusion using aseptic technique as follows:
Calculate the dose (mg) of required SARCLISA based on actual patient weight (measured prior to each cycle to have the administered dose adjusted accordingly) [see Dosage and Administration (2.1)]. More than one SARCLISA vial may be necessary to obtain the required dose for the patient.
- Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit.
- Remove the volume of diluent from the 250 mL Sodium Chloride Injection, USP, or 5% Dextrose Injection, USP diluent bag that is equal to the required volume of SARCLISA injection.
- Withdraw the necessary volume of SARCLISA injection and dilute by adding to the infusion bag of 0.9% Sodium Chloride Injection, USP or 5% Dextrose Injection, USP to achieve the appropriate SARCLISA concentration for infusion.
- The infusion bag must be made of polyolefins (PO), polyethylene (PE), polypropylene (PP), polyvinyl chloride (PVC) with di-(2-ethylhexyl) phthalate (DEHP) or ethyl vinyl acetate (EVA).
- Gently homogenize the diluted solution by inverting the bag. Do not shake.
2.5 Administration
- Administer the infusion solution by intravenous infusion using an intravenous tubing infusion set (in PE, PVC with or without DEHP, polybutadiene [PBD], or polyurethane [PU]) with a 0.22 micron in-line filter (polyethersulfone [PES], polysulfone, or nylon).
- The infusion solution should be administered for a period of time that will depend on the infusion rate (see Table 2). Use prepared SARCLISA infusion solution within 48 hours when stored refrigerated at 2°C–8°C, followed by 8 hours (including the infusion time) at room temperature.
- Do not administer SARCLISA infusion solution concomitantly in the same intravenous line with other agents.
Infusion Rates
Following dilution, administer the SARCLISA infusion solution intravenously at the infusion rates presented in Table 2. Incremental escalation of the infusion rate should be considered only in the absence of infusion-related reactions [see Warnings and Precautions (5.1) and Adverse Reactions (6.1)].
Table 2: Infusion Rates of SARCLISA Administration Dilution Volume Initial Rate Absence of Infusion-Related Reaction Rate Increment Maximum Rate First infusion 250 mL 25 mL/hour For 60 minutes 25 mL/hour every 30 minutes 150 mL/hour Second infusion 250 mL 50 mL/hour For 30 minutes 50 mL/hour for 30 minutes then increase by 100 mL/hour every 30 minutes 200 mL/hour Subsequent infusions 250 mL 200 mL/hour – – 200 mL/hour - 3 DOSAGE FORMS AND STRENGTHS
-
4 CONTRAINDICATIONS
SARCLISA is contraindicated in patients with severe hypersensitivity to isatuximab-irfc or to any of its excipients [see Warnings and Precautions (5.1)].
-
5 WARNINGS AND PRECAUTIONS
5.1 Infusion-Related Reactions
Infusion-related reactions have been observed in 39% of patients treated with SARCLISA [see Adverse Reactions (6.1)]. All infusion-related reactions started during the first SARCLISA infusion and resolved on the same day in 98% of the cases. The most common symptoms of an infusion-related reaction included dyspnea, cough, chills, and nausea. The most common severe signs and symptoms included hypertension and dyspnea [see Adverse Reactions (6.1)].
To decrease the risk and severity of infusion-related reactions, premedicate patients prior to SARCLISA infusion with acetaminophen, H2 antagonists, diphenhydramine, or equivalent; dexamethasone [see Dosage and Administration (2.2)]. Monitor vital signs frequently during the entire SARCLISA infusion. For patients with grade 1 or 2 reactions, interrupt SARCLISA infusion and provide appropriate medical support. If symptoms improve, restart SARCLISA infusion at half of the initial infusion rate, with supportive care as needed, and closely monitor patients. If symptoms do not recur after 30 minutes, the infusion rate may be increased to the initial rate, and then increased incrementally, as shown in Table 2 [see Dosage and Administration (2.5)]. In case symptoms do not improve or recur after interruption, permanently discontinue SARCLISA and institute appropriate management. Permanently discontinue SARCLISA therapy if a grade 3 or higher infusion-related reaction occurs and institute appropriate medical management.
5.2 Neutropenia
SARCLISA may cause neutropenia. Neutropenia (reported as laboratory abnormality) occurred in 96% of patients and grade 3-4 neutropenia occurred in 85% of patients treated with SARCLISA, pomalidomide, and dexamethasone (Isa-Pd). Febrile neutropenia occurred in 12% of patients and neutropenic infections, defined as infection with concurrent grade ≥3 neutropenia, occurred in 25% of patients treated with Isa-Pd. The most frequent neutropenic infections included those of upper respiratory tract (10%), lower respiratory tract (9%), and urinary tract (3%) [see Adverse Reactions (6.1)].
Monitor complete blood cell counts periodically during treatment. Consider the use of antibiotics and antiviral prophylaxis during treatment. Monitor patients with neutropenia for signs of infection. In case of grade 4 neutropenia delay SARCLISA dose until neutrophil count recovery to at least 1.0 × 109/L, and provide supportive care with growth factors, according to institutional guidelines. No dose reductions of SARCLISA are recommended.
5.3 Second Primary Malignancies
Second primary malignancies were reported in 3.9% of patients in the SARCLISA, pomalidomide and dexamethasone (Isa-Pd) arm and in 0.7% of patients in the pomalidomide and dexamethasone (Pd) arm, and consisted of skin squamous cell carcinoma (2.6% of patients in the Isa-Pd arm and in 0.7% of patients in the Pd arm), breast angiosarcoma (0.7% of patients in the Isa-Pd arm) and myelodysplastic syndrome (0.7% of patients in the Isa-Pd arm). With the exception of the patient with myelodysplastic syndrome, patients were able to continue SARCLISA treatment. Monitor patients for the development of second primary malignancies, as per International Myeloma Working Group (IMWG) guidelines.
5.4 Laboratory Test Interference
Interference with Serological Testing (Indirect Antiglobulin Test)
SARCLISA binds to CD38 on red blood cells (RBCs) and may result in a false positive indirect antiglobulin test (indirect Coombs test). In ICARIA-multiple myeloma (MM), the indirect antiglobulin test was positive during SARCLISA treatment in 67.7% of the tested patients. In patients with a positive indirect antiglobulin test, blood transfusions were administered without evidence of hemolysis. ABO/RhD typing was not affected by SARCLISA treatment. Before the first SARCLISA infusion, conduct blood type and screen tests on SARCLISA-treated patients. Consider phenotyping prior to starting SARCLISA treatment. If treatment with SARCLISA has already started, inform the blood bank that the patient is receiving SARCLISA and SARCLISA interference with blood compatibility testing can be resolved using dithiothreitol-treated RBCs. If an emergency transfusion is required, non–cross-matched ABO/RhD-compatible RBCs can be given as per local blood bank practices [see Drug Interactions (7.1)].
Interference with Serum Protein Electrophoresis and Immunofixation Tests
SARCLISA is an IgG kappa monoclonal antibody that can be incidentally detected on both serum protein electrophoresis and immunofixation assays used for the clinical monitoring of endogenous M-protein. This interference can impact the accuracy of the determination of complete response in some patients with IgG kappa myeloma protein [see Drug Interactions (7.1)].
5.5 Embryo-Fetal Toxicity
Based on the mechanism of action, SARCLISA can cause fetal harm when administered to a pregnant woman. SARCLISA may cause fetal immune cell depletion and decreased bone density. Advise pregnant women of the potential risk to a fetus. Advise females with reproductive potential to use an effective method of contraception during treatment with SARCLISA and for at least 5 months after the last dose [see Use in Specific Populations (8.1, 8.3)]. The combination of SARCLISA with pomalidomide is contraindicated in pregnant women because pomalidomide may cause birth defects and death of the unborn child. Refer to the pomalidomide prescribing information on use during pregnancy.
-
6 ADVERSE REACTIONS
The following clinically significant adverse reactions from SARCLISA are also described in other sections of the labeling:
- Infusion-Related Reactions [see Warnings and Precautions (5.1)]
- Neutropenia [see Warnings and Precautions (5.2)]
- Second Primary Malignancies [see Warnings and Precautions (5.3)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Multiple Myeloma
The safety of SARCLISA was evaluated in ICARIA-MM, a randomized, open-label clinical trial in patients with previously treated multiple myeloma. Patients were eligible for inclusion if they had ECOG status of 0–2, platelets ≥75,000 cells/mm3, absolute neutrophil count ≥1 × 109/L, creatinine clearance ≥30 mL/min (MDRD formula), and AST and/or ALT ≤3 × ULN. Patients received SARCLISA 10 mg/kg intravenously, weekly in the first cycle and every two weeks thereafter, in combination with pomalidomide and low dose dexamethasone (Isa-Pd) (n=152) or pomalidomide and low dose dexamethasone (Pd) (n=149) [see Clinical Studies (14)]. Among patients receiving Isa-Pd, 66% were exposed to SARCLISA for 6 months or longer and 24% were exposed for greater than 12 months or longer.
The median age of patients who received Isa-Pd was 68 years (range 36–83); 58% male, 76% white, and 14% Asian.
Serious adverse reactions occurred in 62% of patients receiving Isa-Pd. Serious adverse reactions in >5% of patients who received Isa-Pd included pneumonia (26%), upper respiratory tract infections (7%), and febrile neutropenia (7%). Fatal adverse reactions occurred in 11% of patients (those that occurred in more than 1% of patients were pneumonia and other infections [3%]).
Permanent discontinuation due to an adverse reaction (grades 1-4) occurred in 7% of patients who received Isa-Pd. The most frequent adverse reactions requiring permanent discontinuation in patients who received Isa-Pd were infections (2.6%). In addition, SARCLISA alone was discontinued in 3% of patients due to infusion-related reactions.
Dosage interruptions due to an adverse reaction occurred in 31% of patients who received SARCLISA. The most frequent adverse reaction requiring dosage interruption was infusion-related reaction (28%).
The most common adverse reactions (≥20%) were neutropenia, infusion-related reactions, pneumonia, upper respiratory tract infection, and diarrhea.
Table 3 summarizes the adverse reactions in ICARIA-MM.
Table 3: Adverse Reactions (≥10%) in Patients Receiving SARCLISA, Pomalidomide, and Dexamethasone with a Difference Between Arms of ≥5% Compared to Control Arm in ICARIA-MM Trial Adverse Reactions SARCLISA + Pomalidomide + Dexamethasone (Isa-Pd) Pomalidomide + Dexamethasone (Pd) (N=152) (N=149) All grades
(%)Grade 3
(%)Grade 4
(%)All grades
(%)Grade 3
(%)Grade 4
(%)CTCAE version 4.03 - * Pneumonia includes atypical pneumonia, bronchopulmonary aspergillosis, pneumonia, pneumonia haemophilus, pneumonia influenzal, pneumonia pneumococcal, pneumonia streptococcal, pneumonia viral, candida pneumonia, pneumonia bacterial, haemophilus infection, lung infection, pneumonia fungal, and pneumocystis jirovecii pneumonia.
- † Upper respiratory tract infection includes bronchiolitis, bronchitis, bronchitis viral, chronic sinusitis, fungal pharyngitis, influenza-like illness, laryngitis, nasopharyngitis, parainfluenzae virus infection, pharyngitis, respiratory tract infection, respiratory tract infection viral, rhinitis, sinusitis, tracheitis, upper respiratory tract infection, and upper respiratory tract infection bacterial.
- ‡ Dyspnea includes dyspnea, dyspnea exertional, and dyspnea at rest.
Infusion-related reaction 38 1.3 1.3 0 0 0 Infections Pneumonia* 31 22 3.3 23 16 2.7 Upper respiratory tract infection† 57 9 0 42 3.4 0 Blood and lymphatic system disorders Febrile neutropenia 12 11 1.3 2 1.3 0.7 Respiratory, thoracic and mediastinal disorders Dyspnea‡ 17 5.0 0 12 1.3 0 Gastrointestinal disorders Diarrhea 26 2 – 19 0.7 – Nausea 15 0 – 9 0 – Vomiting 12 1.3 – 3.4 0 – Table 4 summarizes the hematology laboratory abnormalities in ICARIA-MM.
Table 4: Treatment Emergent Hematology Laboratory Abnormalities in Patients Receiving Isa-Pd Treatment versus Pd Treatment – ICARIA-MM Laboratory Parameter n (%) SARCLISA + Pomalidomide + Dexamethasone (Isa-Pd) Pomalidomide + Dexamethasone (Pd) (N=152) (N=149) All Grades Grade 3 Grade 4 All Grades Grade 3 Grade 4 Anemia 151 (99) 48 (32) 0 145 (97) 41 (28) 0 Neutropenia 146 (96) 37 (24) 92 (61) 137 (92) 57 (38) 46 (31) Lymphopenia 140 (92) 64 (42) 19 (13) 137 (92) 52 (35) 12 (8) Thrombocytopenia 127 (84) 22 (14) 25 (16) 118 (79) 14 (9) 22 (15) Description of Selected Adverse Reactions
Infusion-related reactions
In ICARIA-MM, infusion-related reactions (defined as adverse reactions associated with the SARCLISA infusions, with an onset typically within 24 hours from the start of the infusion) were reported in 58 patients (38%) treated with SARCLISA. All patients who experienced infusion-related reactions, experienced them during the 1st infusion of SARCLISA, with 3 patients (2%) also having infusion-related reactions at their 2nd infusion, and 2 patients (1.3%) at their 4th infusion. Grade 1 infusion-related reactions were reported in 3.9%, Grade 2 in 32%, Grade 3 in 1.3%, and Grade 4 in 1.3% of the patients. Signs and symptoms of Grade 3 or higher infusion-related reactions included dyspnea, hypertension, and bronchospasm. The incidence of infusion interruptions because of infusion-related reactions was 29.6%. The median time to infusion interruption was 55 minutes.
In a separate study (TCD 14079 Part B) with SARCLISA 10 mg/kg administered from a 250 mL fixed-volume infusion in combination with Pd, infusion-related reactions (all Grade 2) were reported in 40% of patients, at the first administration, the day of the infusion. Overall, the infusion-related reactions of SARCLISA 10 mg/kg administered as a 250 mL fixed-volume infusion were similar to that of SARCLISA as administered in ICARIA-MM.
Infections
In ICARIA-MM, the incidence of Grade 3 or higher infections was 43% in Isa-Pd group. Pneumonia was the most commonly reported severe infection with Grade 3 reported in 22% of patients in Isa-Pd group compared to 16% in Pd group, and Grade 4 in 3.3% of patients in Isa-Pd group compared to 2.7% in Pd group. Discontinuations from treatment due to infection were reported in 2.6% of patients in Isa-Pd group compared to 5.4% in Pd group. Fatal infections were reported in 3.3% of patients in Isa-Pd group and in 4% in Pd group.
6.2 Immunogenicity
As with all therapeutic proteins, there is a potential for immunogenicity. The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assay may be influenced by several factors, including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of antibodies in the studies described below with the incidence of antibodies in other studies or to other isatuximab-irfc products may be misleading.
In ICARIA-MM, no patients tested positive for antidrug antibodies (ADA). Therefore, the neutralizing ADA status was not determined. Overall, across 6 clinical studies in multiple myeloma (MM) with SARCLISA single agent and combination therapies including ICARIA-MM (N=564), the incidence of treatment emergent ADAs was 2.3%. No clinically significant differences in the pharmacokinetics, safety, or efficacy of isatuximab-irfc were observed in patients with ADAs.
-
7 DRUG INTERACTIONS
7.1 Laboratory Test Interference
Interference with Serological Testing
SARCLISA, an anti-CD38 antibody, may interfere with blood bank serologic tests with false positive reactions in indirect antiglobulin tests (indirect Coombs tests), antibody detection (screening) tests, antibody identification panels, and antihuman globulin crossmatches in patients treated with SARCLISA [see Warnings and Precautions (5.4)].
Interference with Serum Protein Electrophoresis and Immunofixation Tests
SARCLISA may be incidentally detected by serum protein electrophoresis and immunofixation assays used for the monitoring of M-protein and may interfere with accurate response classification based on International Myeloma Working Group (IMWG) criteria [see Warnings and Precautions (5.4)].
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
SARCLISA can cause fetal harm when administered to a pregnant woman. The assessment of isatuximab-irfc-associated risks is based on the mechanism of action and data from target antigen CD38 knockout animal models (see Data). There are no available data on SARCLISA use in pregnant women to evaluate for a drug-associated risk of major birth defects, miscarriage or adverse maternal or fetal outcomes. Animal reproduction toxicity studies have not been conducted with isatuximab-irfc. The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, miscarriage, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
The combination of SARCLISA and pomalidomide is contraindicated in pregnant women because pomalidomide may cause birth defects and death of the unborn child. Refer to the pomalidomide prescribing information on use during pregnancy. Pomalidomide is only available through a REMS program.
Clinical Considerations
Fetal/neonatal reactions
Immunoglobulin G1 monoclonal antibodies are known to cross the placenta. Based on its mechanism of action, SARCLISA may cause depletion of fetal CD38-positive immune cells and decreased bone density. Defer administration of live vaccines to neonates and infants exposed to SARCLISA in utero until a hematology evaluation is completed.
Data
Animal data
Mice that were genetically modified to eliminate all CD38 expression (CD38 knockout mice) had reduced bone density which recovered 5 months after birth. Data from studies using CD38 knockout animal models also suggest the involvement of CD38 in regulating humoral immune responses (mice), feto-maternal immune tolerance (mice), and early embryonic development (frogs).
8.2 Lactation
Risk Summary
There are no available data on the presence of isatuximab-irfc in human milk, milk production, or the effects on the breastfed child. Maternal immunoglobulin G is known to be present in human milk. The effects of local gastrointestinal exposure and limited systemic exposure in the breastfed infant to SARCLISA are unknown. Because of the potential for serious adverse reactions in the breastfed child from isatuximab-irfc administered in combination with pomalidomide and dexamethasone, advise lactating women not to breastfeed during treatment with SARCLISA. Refer to pomalidomide prescribing information for additional information.
8.3 Females and Males of Reproductive Potential
Pregnancy Testing
With the combination of SARCLISA with pomalidomide, refer to the pomalidomide labeling for pregnancy testing requirements prior to initiating treatment in females of reproductive potential.
Contraception
Females
SARCLISA can cause fetal harm when administered to a pregnant woman [see Use in Specific Populations (8.1)]. Advise female patients of reproductive potential to use effective contraception during treatment and for at least 5 months after the last dose of SARCLISA. Additionally, refer to the pomalidomide labeling for contraception requirements prior to initiating treatment in females of reproductive potential.
8.5 Geriatric Use
Of the total number of subjects in clinical studies of SARCLISA, 53% (306 patients) were 65 and over, while 14% (82 patients) were 75 and over. No overall differences in safety or effectiveness were observed between subjects 65 and over and younger subjects, and other reported clinical experience has not identified differences in responses between the adults 65 years and over and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
- 10 OVERDOSAGE
-
11 DESCRIPTION
Isatuximab-irfc, a CD38-directed cytolytic antibody, is a chimeric immunoglobulin G1 (IgG1) monoclonal antibody (mAb). Isatuximab-irfc is produced from a mammalian cell line (Chinese hamster ovary, CHO) using a fed-batch production process. Isatuximab-irfc is composed of two identical immunoglobulin kappa light chains and two identical immunoglobulin gamma heavy chains and has an overall molecular weight of approximately 148 kDa.
SARCLISA (isatuximab-irfc) injection is a sterile, preservative-free, clear to slightly opalescent, colorless to slightly yellow solution, essentially free of visible particles in a single-dose vial for intravenous use. Each vial contains either 100 mg/5 mL or 500 mg/25 mL of isatuximab-irfc at a concentration of 20 mg/mL with a pH of 6.0. Each mL of solution contains 20 mg isatuximab-irfc, histidine (1.46 mg), histidine hydrochloride monohydrate (2.22 mg), polysorbate 80 (0.2 mg), sucrose (100 mg), and water for injection.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Isatuximab-irfc is an IgG1-derived monoclonal antibody that binds to CD38 expressed on the surface of hematopoietic and tumor cells, including multiple myeloma cells. Isatuximab-irfc induces apoptosis of tumor cells and activation of immune effector mechanisms including antibody-dependent cell-mediated cytotoxicity (ADCC), antibody-dependent cellular phagocytosis (ADCP), and complement dependent cytotoxicity (CDC). Isatuximab-irfc inhibits the ADP-ribosyl cyclase activity of CD38. Isatuximab-irfc can activate natural killer (NK) cells in the absence of CD38-positive target tumor cells and suppresses CD38-positive T-regulatory cells.
The combination of isatuximab-irfc and pomalidomide enhanced ADCC activity and direct tumor cell killing compared to that of isatuximab-irfc alone in vitro, and enhanced antitumor activity compared to the activity of isatuximab-irfc or pomalidomide alone in a human multiple myeloma xenograft model.
12.2 Pharmacodynamics
In multiple myeloma patients treated with SARCLISA combined with pomalidomide and dexamethasone, a decrease in absolute counts of total NK cells (including inflammatory CD16+ low CD56+ bright and cytotoxic CD16+ bright CD56+ dim NK cells) and CD19+ B cells was observed in peripheral blood.
Cardiac Electrophysiology
Up to 2 times the approved recommended dose, SARCLISA does not prolong the QT interval to any clinically relevant extent.
A relationship between isatuximab-irfc exposure and overall response rate and progression-free survival was observed.
No apparent relationship was observed between an increase of isatuximab-irfc exposure and adverse reactions.
12.3 Pharmacokinetics
Following the administration of isatuximab-irfc at the recommended dose and schedule, the steady state isatuximab-irfc mean (CV %) predicted maximum plasma concentration (Cmax) was 351 µg/mL (36.0%) and area under the plasma concentration-time curve (AUC) was 72,600 µg∙h/mL (51.7%). The median time to reach steady state of isatuximab-irfc was 8 weeks with a 3.1-fold accumulation.
Isatuximab-irfc AUC increases in a greater than dose proportional manner over a dosage range from 1 mg/kg to 20 mg/kg (0.1 to 2 times the approved recommended dosage) every 2 weeks. Isatuximab-irfc AUC increases proportionally over a dosage range from 5 mg/kg to 20 mg/kg (0.5 to 2 times the approved recommended dosage) every week for 4 weeks followed by every 2 weeks.
Distribution
The mean (CV %) predicted total volume of distribution of isatuximab-irfc is of 8.13 L (26.2%).
Elimination
Isatuximab-irfc total clearance decreased with increasing dose and with multiple doses. At steady state, the near elimination (≥99%) of isatuximab-irfc from plasma after the last dose is predicted to occur in approximately 2 months. The elimination of isatuximab-irfc was similar when given as a single agent or as combination therapy.
Specific Populations
Isatuximab-irfc exposure (AUC) at steady state decreases with increasing body weight. The following factors have no clinically meaningful effect on the exposure of isatuximab-irfc: age (36 to 85 years, 70 patients were >75 years old), sex, race (Caucasian, Black, Asian), renal impairment (eGFR <90 mL/min/1.73 m2), and mild hepatic impairment (total bilirubin 1 to 1.5 times upper limit of normal [ULN] or aspartate amino transferase [AST] > ULN). The effect of moderate (total bilirubin >1.5 times to 3 times ULN and any AST) and severe (total bilirubin >3 times ULN and any AST) hepatic impairment on isatuximab-irfc pharmacokinetics is unknown.
No dose adjustments are recommended in these specific patient populations.
- 13 NONCLINICAL TOXICOLOGY
-
14 CLINICAL STUDIES
14.1 Multiple Myeloma
ICARIA-MM
The efficacy and safety of SARCLISA in combination with pomalidomide and low-dose dexamethasone (Isa-Pd) were evaluated in ICARIA-MM (NCT02990338), a multicenter, multinational, randomized, open-label, 2-arm, phase 3 study in patients with relapsed and refractory multiple myeloma. Patients had received at least two prior therapies including lenalidomide and a proteasome inhibitor.
A total of 307 patients were randomized in a 1:1 ratio to receive either SARCLISA in combination with pomalidomide and low-dose dexamethasone (Isa-Pd, 154 patients) or pomalidomide and low-dose dexamethasone (Pd, 153 patients). Treatment was administered in both groups in 28-day cycles until disease progression or unacceptable toxicity. SARCLISA 10 mg/kg was administered as an intravenous infusion weekly in the first cycle and every two weeks thereafter. Pomalidomide 4 mg was taken orally once daily from day 1 to day 21 of each 28-day cycle. Low-dose dexamethasone (orally or intravenously) 40 mg (20 mg for patients ≥75 years of age) was given on days 1, 8, 15, and 22 for each 28-day cycle.
Overall, demographic and disease characteristics at baseline were similar between the two treatment groups. The median patient age was 67 years (range 36–86), 20% of patients were ≥75 years; 10% of patients entered the study with a history of COPD or asthma. The proportion of patients with renal impairment (creatinine clearance <60 mL/min/1.73 m2) was 34%. The International Staging System (ISS) stage at study entry was I in 37%, II in 36% and III in 25% of patients. Overall, 20% of patients had high-risk chromosomal abnormalities at study entry; del(17p), t(4;14) and t(14;16) were present in 12%, 8% and 2% of patients, respectively.
The median number of prior lines of therapy was 3 (range 2–11). All patients received a prior proteasome inhibitor, all patients received prior lenalidomide, and 56% of patients received prior stem cell transplantation; the majority of patients (93%) were refractory to lenalidomide, 76% to a proteasome inhibitor, and 73% to both an immunomodulator and a proteasome inhibitor.
The median duration of treatment was 41 weeks for Isa-Pd group compared to 24 weeks for Pd group.
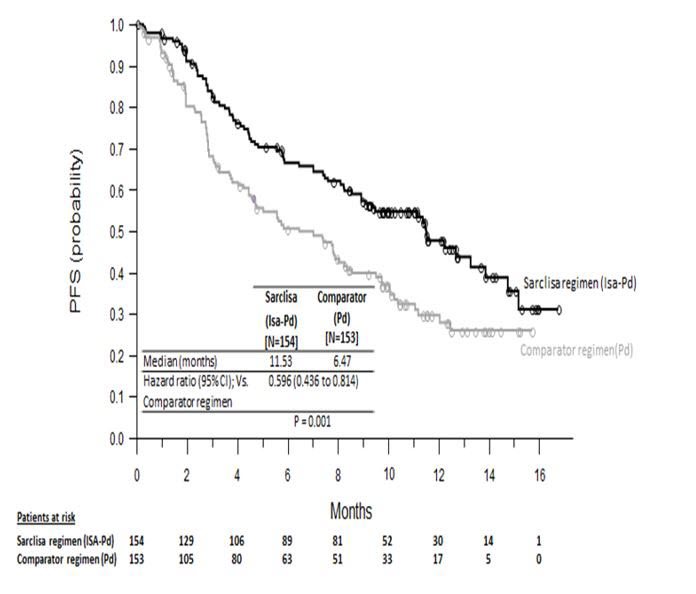
The efficacy of SARCLISA was based upon progression-free survival (PFS). PFS results were assessed by an Independent Response Committee based on central laboratory data for M-protein and central radiologic imaging review using the International Myeloma Working Group (IMWG) criteria. The improvement in PFS represented a 40% reduction in the risk of disease progression or death in patients treated with Isa-Pd.
Efficacy results are presented in Table 5 and Kaplan-Meier curve for PFS is provided in Figure 1.
Table 5: Efficacy of SARCLISA in Combination with Pomalidomide and Low-Dose Dexamethasone versus Pomalidomide and Dexamethasone in the Treatment of Multiple Myeloma (ICARIA-MM) Endpoint SARCLISA + Pomalidomide + Dexamethasone Pomalidomide + Dexamethasone N=154 N=153 - * Stratified on age (<75 years versus ≥75 years) and number of previous lines of therapy (2 or 3 vs >3) according to IRT.
- † sCR, CR, VGPR and PR were evaluated by the IRC using the IMWG response criteria.
- ‡ Estimated using Clopper-Pearson method.
Progression-Free Survival Median (months) 11.53 6.47 [95% CI] [8.94–13.9] [4.47–8.28] Hazard ratio* [95% CI] 0.596 [0.44–0.81] p-value* (stratified log-rank test) 0.0010 Overall Response Rate† Responders (sCR+CR+VGPR+PR) n (%) 93 (60.4) 54 (35.3) [95% CI]‡ [52.2%–68.2%] [27.8%–43.4%] p-value (stratified Cochran-Mantel-Haenszel)* <0.0001 Stringent Complete Response (sCR) + Complete Response (CR) n (%) 7 (4.5) 3 (2) Very Good Partial Response (VGPR) n (%) 42 (27.3) 10 (6.5) Partial Response (PR) n (%) 44 (28.6) 41 (26.8) The median time to first response in responders was 35 days in Isa-Pd group versus 58 days in Pd group. The median duration of response was 13.3 months (95% CI: 10.6-NR) in the Isa-Pd group versus 11.1 months (95% CI: 8.5-NR) in the Pd group. Median overall survival was not reached for either treatment group. At a median follow-up time of 11.6 months, 43 (27.9%) patients on Isa-Pd and 56 (36.6%) patients on Pd had died. The OS results at interim analysis did not reach statistical significance.
Figure 1: Kaplan-Meier Curves of PFS – ITT Population – ICARIA-MM (assessment by the IRC)
-
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 How Supplied
SARCLISA (isatuximab-irfc) injection is a clear to slightly opalescent, colorless to slightly yellow solution, essentially free of visible particulates, supplied as follows:
- One 100 mg/5 mL single-dose vial in a carton: NDC: 0024-0654-01
- One 500 mg/25 mL single-dose vial in a carton: NDC: 0024-0656-01
-
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient Information).
Infusion-Related Reaction
Instruct patients to immediately report any occurrence of symptoms occurring within 24 hours of start of infusion to their healthcare provider [see Warnings and Precautions (5.1)].
Neutropenia
Inform patients about the risk of neutropenia and infection during SARCLISA treatment and the importance of reporting immediately any fever or symptoms of infection to their healthcare provider [see Warnings and Precautions (5.2) and Adverse Reactions (6.1)].
Second Primary Malignancies
Inform patients of the risk of developing second primary malignancies during treatment with SARCLISA in combination with pomalidomide and low-dose dexamethasone [see Warnings and Precautions (5.3)].
Interference with Laboratory Tests
Advise patients to inform healthcare providers and transfusion center personnel that they are treated with SARCLISA in case a red blood cell transfusion is planned [see Warnings and Precautions (5.4) and Drug Interactions (7.1)].
Embryo-Fetal Toxicity
Advise women of the potential hazard to a fetus and to avoid becoming pregnant during treatment and for at least 5 months after the last dose of SARCLISA [see Use in Specific Populations (8.1, 8.3)].
Advise patients that pomalidomide has the potential to cause fetal harm and has specific requirements regarding contraception, pregnancy testing, blood and sperm donation, and transmission in sperm. Advise patients to report suspected or known pregnancies. Pomalidomide is only available through a REMS program [see Use in Specific Populations (8.1, 8.3)].
- SPL UNCLASSIFIED SECTION
-
PATIENT PACKAGE INSERT
This Patient Information has been approved by the U.S. Food and Drug Administration. Issued: March 2020 Patient Information
SARCLISA® (sar-cli-sa)
(isatuximab-irfc)
injectionSARCLISA is used in combination with other medicines called pomalidomide and dexamethasone. You should also read the Medication Guide that comes with pomalidomide. You can ask your healthcare provider or pharmacist for information about dexamethasone. What is SARCLISA?
SARCLISA is a prescription medicine used in combination with pomalidomide and dexamethasone to treat adults who have received at least 2 prior therapies, including lenalidomide and a proteasome inhibitor, to treat multiple myeloma.
It is not known if SARCLISA is safe and effective in children.Do not receive SARCLISA if you have a history of a severe allergic reaction to isatuximab-irfc or any of the ingredients in SARCLISA. See the end of this leaflet for complete list of ingredients in SARCLISA. Before receiving SARCLISA, tell your healthcare provider about all of your medical conditions, including if you: - are pregnant or plan to become pregnant. SARCLISA may harm your unborn baby. You should not receive SARCLISA during pregnancy.
- Females who are able to become pregnant should use an effective method of birth control during treatment and for 5 months after your last dose of SARCLISA. Talk to your healthcare provider about birth control methods that you can use during this time.
- are breastfeeding or plan to breastfeed. It is not known if SARCLISA passes into your breast milk. You should not breastfeed during treatment with SARCLISA.
How will I receive SARCLISA? - SARCLISA will be given to you by your healthcare provider by intravenous (IV) infusion into your vein.
- SARCLISA is given in treatment cycles of 28 days (4 weeks), together with the medicines pomalidomide and dexamethasone.
- In cycle 1, SARCLISA is usually given weekly.
- Starting in cycle 2, SARCLISA is usually given every 2 weeks.
- If you miss any appointments, call your healthcare provider as soon as possible to reschedule your appointment.
- Your healthcare provider will give you medicines before each dose of SARCLISA, to help reduce the risk of infusion reactions (make them less frequent and severe).
What are the possible side effects of SARCLISA?
SARCLISA may cause serious side effects including:-
Infusion reactions. Infusion reactions are common with SARCLISA and can sometimes be severe.
- Your healthcare provider will prescribe medicines before each infusion of SARCLISA to help decrease your risk for infusion reactions or to help make any infusion reaction less severe. You will be monitored for infusion reactions during each dose of SARCLISA.
- Your healthcare provider may slow down or stop your infusion, or completely stop treatment with SARCLISA if you have an infusion reaction.
- feeling short of breath
- cough
- chills
- nausea
-
Decreased white blood cell counts. Decreased white blood cell counts are common with SARCLISA and certain white blood cells can be severely decreased. You may have an increased risk of getting certain infections, such as upper and lower respiratory infections.
Your healthcare provider will check your blood cell counts during treatment with SARCLISA. Your healthcare provider may prescribe an antibiotic or antiviral medicine to help prevent infection, or a medicine to help increase your white blood cell counts during treatment with SARCLISA.
Tell your healthcare provider right away if you develop any fever or symptoms of infection during treatment with SARCLISA. - Risk of new cancers. New cancers have happened in people during treatment with SARCLISA. Your healthcare provider will monitor you for new cancers during treatment with SARCLISA.
- Change in blood tests. SARCLISA can affect the results of blood tests to match your blood type. Your healthcare provider will do blood tests to match your blood type before you start treatment with SARCLISA. Tell all of your healthcare providers that you are being treated with SARCLISA before receiving blood transfusions.
- lung infection (pneumonia)
- decreased red blood cell counts (anemia)
- upper respiratory tract infection
- decreased platelet counts (thrombocytopenia)
- diarrhea
These are not all the possible side effects of SARCLISA. For more information, ask your healthcare provider or pharmacist.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
General information about the safe and effective use of SARCLISA.
Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. You can ask your pharmacist or healthcare provider for information about SARCLISA that is written for health professionals.What are the ingredients in SARCLISA?
Active ingredient: isatuximab-irfc
Inactive ingredients: histidine, histidine hydrochloride monohydrate, polysorbate 80, sucrose, and water for injection.Manufactured by: sanofi-aventis U.S. LLC, Bridgewater, NJ 08807, A SANOFI COMPANY, U.S. License No. 1752
SARCLISA is a registered trademark of Sanofi ©2020 sanofi-aventis U.S. LLC
For more information, go to www.sanofi-aventis.us or call 1-800-633-1610. - are pregnant or plan to become pregnant. SARCLISA may harm your unborn baby. You should not receive SARCLISA during pregnancy.
-
PRINCIPAL DISPLAY PANEL - 100 mg/5 mL Vial Carton
NDC: 0024-0654-01
Rx onlySARCLISA®
(isatuximab-irfc)
Injection100 mg/5 mL (20 mg/mL)
For Intravenous Infusion After Dilution
One single-dose vial
Discard unused portionSANOFI

-
PRINCIPAL DISPLAY PANEL - 500 mg/25 mL Vial Carton
NDC: 0024-0656-01
Rx onlySARCLISA®
(isatuximab-irfc)
Injection500 mg/25 mL (20 mg/mL)
For Intravenous Infusion After Dilution
One single-dose vial
Discard unused portionSANOFI
-
INGREDIENTS AND APPEARANCE
SARCLISA
isatuximab injection, solution, concentrateProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 0024-0654 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength isatuximab (UNII: R30772KCU0) (isatuximab - UNII:R30772KCU0) isatuximab 100 mg in 5 mL Inactive Ingredients Ingredient Name Strength sucrose (UNII: C151H8M554) 500 mg in 5 mL HISTIDINE MONOHYDROCHLORIDE MONOHYDRATE (UNII: X573657P6P) 11.1 mg in 5 mL HISTIDINE (UNII: 4QD397987E) 7.3 mg in 5 mL polysorbate 80 (UNII: 6OZP39ZG8H) 1 mg in 5 mL water (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 0024-0654-01 1 in 1 CARTON 03/02/2020 1 5 mL in 1 VIAL, SINGLE-DOSE; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA761113 03/02/2020 SARCLISA
isatuximab injection, solution, concentrateProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 0024-0656 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength isatuximab (UNII: R30772KCU0) (isatuximab - UNII:R30772KCU0) isatuximab 500 mg in 25 mL Inactive Ingredients Ingredient Name Strength sucrose (UNII: C151H8M554) 2500 mg in 25 mL HISTIDINE MONOHYDROCHLORIDE MONOHYDRATE (UNII: X573657P6P) 55.5 mg in 25 mL histidine (UNII: 4QD397987E) 36.5 mg in 25 mL polysorbate 80 (UNII: 6OZP39ZG8H) 5 mg in 25 mL water (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 0024-0656-01 1 in 1 CARTON 03/02/2020 1 25 mL in 1 VIAL, SINGLE-DOSE; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA761113 03/02/2020 Labeler - sanof-aventis U.S. LLC (824676584) Establishment Name Address ID/FEI Business Operations Sanofi-Aventis Deutschland GmbH 313218430 MANUFACTURE(0024-0654, 0024-0656) , ANALYSIS(0024-0654, 0024-0656) , LABEL(0024-0654, 0024-0656) , PACK(0024-0654, 0024-0656) Establishment Name Address ID/FEI Business Operations Genzyme Corporation 050424395 LABEL(0024-0654, 0024-0656) , PACK(0024-0654, 0024-0656) Establishment Name Address ID/FEI Business Operations Sanofi Chimie 291592785 API MANUFACTURE(0024-0654, 0024-0656) , ANALYSIS(0024-0654, 0024-0656) Establishment Name Address ID/FEI Business Operations Quality Assistance, S.A. 283676641 ANALYSIS(0024-0654, 0024-0656)
Trademark Results [Sarclisa]
Mark Image Registration | Serial | Company Trademark Application Date |
|---|---|
 SARCLISA 88289456 5889106 Live/Registered |
Sanofi 2019-02-05 |
 SARCLISA 87573433 5479433 Live/Registered |
Sanofi 2017-08-17 |
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.