MANNITOL injection, solution
Mannitol by
Drug Labeling and Warnings
Mannitol by is a Prescription medication manufactured, distributed, or labeled by General Injectables & Vaccines, Inc. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
DESCRIPTION
Mannitol intravenous (Mannitol Injection, USP) is a sterile, nonpyrogenic solution of mannitol in water for injection available in a concentration of 25% in a fliptop vial for administration by intravenous infusion only.
The content and characteristics are as follows:
The solution contains no bacteriostat, antimicrobial agent or added buffer (except for pH adjustment) and is intended only as a single-dose injection. When smaller doses are required the unused portion should be discarded.
Mannitol Injection, USP is a parenteral obligatory osmotic diuretic.
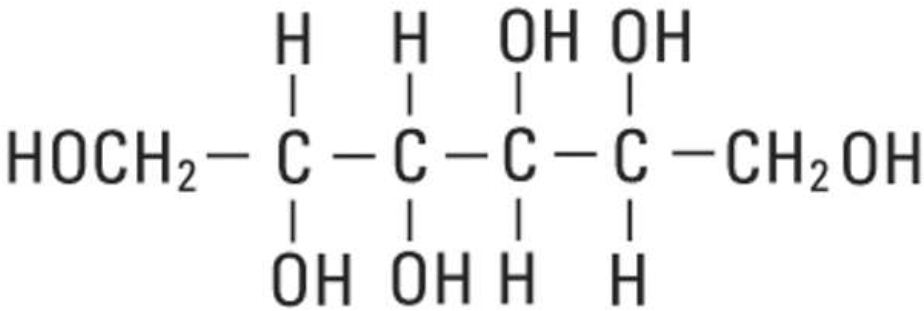
Mannitol, USP is chemically designated D-mannitol (C6H14O6), a white crystalline powder or free-flowing granules freely soluble in water. It has the following structural formula:
-
CLINICAL PHARMACOLOGY
When administered intravenously mannitol is confined to the extracellular space, only slightly metabolized and rapidly excreted by the kidney. Approximately 80% of a 100 g dose appears in the urine in 3 hours. The drug is freely filtered by the glomeruli with less than 10% tubular reabsorption; it is not secreted by tubular cells. Mannitol induces diuresis by elevating the osmolarity of the glomerular filtrate and thereby hindering tubular reabsorption of water. Excretion of sodium and chloride is also enhanced.
-
INDICATIONS AND USAGE
Mannitol intravenous (Mannitol Injection, USP) is indicated for the following purposes in adults and pediatric patients.
Therapeutic Use
- Reduction of intracranial pressure and brain mass.
- Reduction of high intraocular pressure when the pressure cannot be lowered by other means.
Diagnostic Use
Measurement of glomerular filtration rate.
-
CONTRAINDICATIONS
- Well established anuria due to severe renal disease.
- Severe pulmonary congestion or frank pulmonary edema.
- Active intracranial bleeding except during craniotomy.
- Severe dehydration.
- Progressive heart failure or pulmonary congestion after institution of mannitol therapy.
- Do not administer to patients with a known hypersensitivity to mannitol.
-
WARNINGS
- Renal complications, including irreversible renal failure have been reported in patients receiving mannitol. Reversible, oliguric acute kidney injury (AKI) has occurred in patients with normal pretreatment renal function who received mannitol. Patients with pre-existing renal disease, patients with conditions that put them at risk for renal failure, or those receiving potentially nephrotoxic drugs or other diuretics, are at increased risk for renal failure. Avoid concomitant administration of nephrotoxic drugs (e.g., aminoglycosides) or other diuretics with mannitol (see PRECAUTIONS). If urine output declines during mannitol infusion, the patient's clinical status should be closely reviewed and mannitol infusion suspended if necessary.
- The obligatory diuretic response following rapid infusion of 25% mannitol may further aggravate pre-existing hemoconcentration. Excessive loss of water and electrolytes may lead to serious imbalances. Serum sodium and potassium should be carefully monitored during mannitol administration.
- Accumulation of mannitol may result in overexpansion of the extracellular fluid which may intensify existing or latent congestive heart failure.
- Excessive loss of water and electrolytes may lead to serious imbalances. With continued administration of mannitol, loss of water in excess of electrolytes can cause hypernatremia. Electrolyte measurements, including sodium and potassium are therefore of vital importance in monitoring the infusion of mannitol.
- Osmotic nephrosis, a reversible vacuolization of the tubules of no known clinical significance, may proceed to severe irreversible nephrosis, so that the renal function must be closely monitored during mannitol infusion.
- Mannitol injection may increase cerebral blood flow and the risk of postoperative bleeding in neurosurgical patients.
- For intravenous use only. Do not administer intramuscularly or subcutaneously. Never add mannitol in whole blood for transfusion.
- Mannitol may increase the cerebral blood flow and worsen intracranial hypertension in children who develop a generalized cerebral hyperemia during the first 24 to 48 hours post injury.
-
PRECAUTIONS
- The cardiovascular status of the patient should be carefully evaluated before rapidly administering mannitol since sudden expansion of the extracellular fluid may lead to fulminating congestive heart failure.
- Shift of sodium-free intracellular fluid into the extracellular compartment following mannitol infusion may lower serum sodium concentration and aggravate pre-existing hyponatremia.
- By sustaining diuresis, mannitol administration may obscure and intensify inadequate hydration or hypovolemia.
- Avoid concomitant administration of nephrotoxic drugs (e.g., aminoglycosides) or other diuretics with mannitol.
- Electrolyte-free mannitol solutions should not be given conjointly with blood. If it is essential that blood be given simultaneously, at least 20 mEq of sodium chloride should be added to each liter of mannitol solution to avoid pseudoagglutination.
- When exposed to low temperatures, solutions of mannitol may crystallize. If crystals are observed, the container should be warmed to redissolve, then cooled to body temperature before administering (see NOTE under HOW SUPPLIED). When infusing 25% mannitol, the administration set should include a filter. Do not infuse mannitol solution if crystals are present.
- Do not administer unless solution is clear and container is undamaged. Discard unused portion. Do not administer 25% mannitol if the fliptop vial seal is not intact.
Carcinogenesis, Mutagenesis, Impairment of Fertility
Studies with Mannitol Injection (USP) have not been performed to evaluate carcinogenic potential, mutagenic potential or effects on fertility.
Pregnancy
Animal reproduction studies have not been conducted with mannitol injection. It is also not known whether mannitol injection can cause fetal harm when given to a pregnant woman or can affect reproduction. Mannitol injection should be given to a pregnant woman only if clearly needed.
Nursing Mothers
It is not known whether this drug is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when mannitol is administered to a nursing woman.
-
ADVERSE REACTIONS
Adverse reactions more commonly reported during or after the infusion of mannitol include: Pulmonary congestion, fluid and electrolyte imbalance, acidosis, electrolyte loss, dryness of mouth, thirst, marked diuresis, urinary retention, edema, headache, blurred vision, convulsions, nausea, vomiting, rhinitis, arm pain, skin necrosis, thrombophlebitis, chills, dizziness, urticaria, dehydration, hypotension, tachycardia, fever and angina-like chest pains.
Reactions which may occur because of the solution or the technique of administration include febrile response, infection at the site of injection, venous thrombosis or phlebitis extending from the site of injection, extravasation and hypervolemia.
If an adverse reaction does occur, discontinue the infusion, evaluate the patient, institute appropriate therapeutic countermeasures and save the remainder of the fluid for examination if deemed necessary.
-
OVERDOSAGE
Too rapid infusion of large amounts of mannitol will cause a shift of intracellular water into the extracellular compartment resulting in cellular dehydration and overexpansion of the intravascular space with hyponatremia, congestive heart failure and pulmonary edema. Repeated doses should not be given to patients with persistent oliguria as this can produce a hyperosmolar state and precipitate congestive heart failure and pulmonary edema due to volume overload. Dosage must be carefully monitored and adjusted in accordance with the clinical situation to avoid the consequences of overdosage (see CONTRAINDICATIONS, WARNINGS, PRECAUTIONS and DOSAGE AND ADMINISTRATION).
-
DOSAGE AND ADMINISTRATION
Reduction of Intracranial Pressure and Brain Mass: In adults a dose of 0.25 to 2 g/kg body weight as a 15% to 25% solution administered over a period of 30 to 60 minutes; pediatric patients 1 to 2 g/kg body weight or 30 to 60 g/m2 body surface area over a period of 30 to 60 minutes. In small or debilitated patients, a dose of 500 mg/kg may be sufficient. Careful evaluation must be made of the circulatory and renal reserve prior to and during administration of mannitol at the higher doses and rapid infusion rates. Careful attention must be paid to fluid and electrolyte balance, body weight, and total input and output before and after infusion of mannitol. Evidence of reduced cerebral spinal fluid pressure must be observed within 15 minutes after starting infusion.
Reduction of Intraocular Pressure: In adults a dose of 0.25 to 2 g/kg body weight as a 15% to 25% solution administered over a period of 30 to 60 minutes; pediatric patients 1 to 2 g/kg body weight or 30 to 60 g/m2 body surface area over a period of 30 to 60 minutes. In small or debilitated patients, a dose of 500 mg/kg may be sufficient. When used preoperatively, the dose should be given one to one and one-half hours before surgery to achieve maximal reduction of intraocular pressure before operation.
Measurement of Glomerular Filtration Rate (GFR): 100 mL of a 20% solution (20 g) should be diluted with 180 mL of sodium chloride injection (normal saline) or 200 mL of a 10% solution (20 g) should be diluted with 80 mL of sodium chloride injection (normal saline). The resulting 280 mL of 7.2% solution is infused at a rate of 20 mL per minute. The urine is collected by catheter for a specific period of time and analyzed for mannitol excreted in mg per minute. A blood sample is drawn at the start and at the end of the time period and the concentration of mannitol determined in mg/mL of plasma. GFR is the number of mL of plasma that must have been filtered to account for the amount excreted per minute in the urine. Normal clearance rates are approximately 125 mL/minute for men; 116 mL/minute for women.
Drug Interactions
Additives may be incompatible. Consult with pharmacist, if available.
Do not place 25% Mannitol Injection, USP in polyvinylchloride bags; a white flocculent precipitate may form from contact with PVC surfaces. Parenteral drug products should be inspected visually for particulate matter and discoloration; whenever container and solution permit (see PRECAUTIONS).
- INSTRUCTIONS FOR USE
-
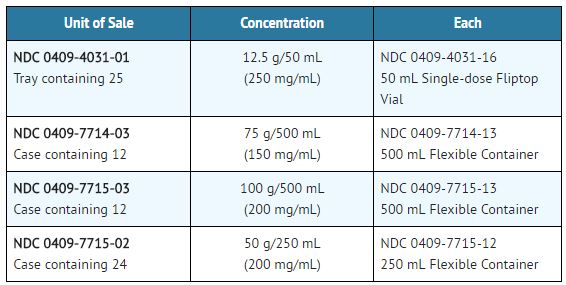
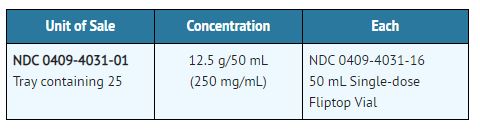
HOW SUPPLIED
Mannitol Intravenous (Mannitol Injection, USP) is supplied in single-dose containers as follows:
NOTE: Crystals may form in mannitol solutions especially if the solutions are chilled. To dissolve the crystals, warm the bottle in hot water at 80°C and periodically shake vigorously. 25% Mannitol Injection, USP may be autoclaved at 121°C for 20 minutes at 15 psi. Remove cover from fliptop vial and cleanse stopper with antiseptic before use. Cool to body temperature or less before administering. When infusing 25% mannitol concentrations, the administration set should include a filter.
Protect from freezing. Store at 20 to 25°C (68 to 77°F). [See USP Controlled Room Temperature.]
- SAMPLE PACKAGE LABEL
-
INGREDIENTS AND APPEARANCE
MANNITOL
mannitol injection, solutionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 52584-031(NDC:0409-4031) Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength Mannitol (UNII: 3OWL53L36A) (Mannitol - UNII:3OWL53L36A) Mannitol 12.5 g in 50 mL Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 52584-031-01 1 in 1 BAG 11/19/2019 1 50 mL in 1 VIAL, SINGLE-DOSE; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA016269 11/19/2019 Labeler - General Injectables & Vaccines, Inc (108250663)
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.