DILTIAZEM HYDROCHLORIDE injection, solution DILTIAZEM HYDROCHLORIDE injection, powder, lyophilized, for solution
Diltiazem Hydrochloride by
Drug Labeling and Warnings
Diltiazem Hydrochloride by is a Prescription medication manufactured, distributed, or labeled by Hospira, Inc.. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
- SPL UNCLASSIFIED SECTION
-
DESCRIPTION
Diltiazem hydrochloride is a calcium ion cellular influx inhibitor (slow channel blocker or calcium channel antagonist). Chemically, diltiazem hydrochloride is 1,5-benzothiazepin-4(5H)-one, 3-(acetyloxy)-5-[2-(dimethylamino)ethyl]-2, 3-dihydro-2-(4-methoxyphenyl)-, monohydrochloride,(+)-cis-. The chemical structure is:
Diltiazem hydrochloride is a white to off-white crystalline powder with a bitter taste. It is soluble in water, methanol, and chloroform. It has a molecular weight of 450.98.
Diltiazem hydrochloride injection is a clear, colorless, sterile, nonpyrogenic solution. It has a pH range of 3.7 to 4.1.
Diltiazem hydrochloride injection is for direct intravenous bolus injection and continuous intravenous infusion.
25-mg, 5-mL vial-each sterile vial contains 25 mg diltiazem hydrochloride, 3.75 mg citric acid USP, 3.25 mg sodium citrate dihydrate USP, 250 mg sorbitol NF and water for injection USP up to 5 mL. Sodium hydroxide or hydrochloric acid is used for pH adjustment.
50-mg, 10-mL vial-each sterile vial contains 50 mg diltiazem hydrochloride, 7.5 mg citric acid USP, 6.5 mg sodium citrate dihydrate USP, 500 mg sorbitol NF and water for injection USP up to 10 mL. Sodium hydroxide or hydrochloric acid is used for pH adjustment.
Diltiazem hydrochloride for injection is an off-white lyophilized powder and, after reconstitution in an infusion bag, produces a clear, colorless, sterile, nonpyrogenic solution.
Diltiazem hydrochloride for injection for continuous intravenous infusion is available in ADD-Vantage Vials. The vial contains lyophilized powder comprised of diltiazem hydrochloride 100 mg and mannitol USP 75 mg for reconstitution in the ADD-Vantage Flexible Diluent Container containing 5% dextrose injection or 0.9% sodium chloride injection.
-
CLINICAL PHARMACOLOGY
Mechanisms of Action
Diltiazem inhibits the influx of calcium (Ca2+) ions during membrane depolarization of cardiac and vascular smooth muscle. The therapeutic benefits of diltiazem in supraventricular tachycardias are related to its ability to slow AV nodal conduction time and prolong AV nodal refractoriness. Diltiazem exhibits frequency (use) dependent effects on AV nodal conduction such that it may selectively reduce the heart rate during tachycardias involving the AV node with little or no effect on normal AV nodal conduction at normal heart rates.
Diltiazem slows the ventricular rate in patients with a rapid ventricular response during atrial fibrillation or atrial flutter. Diltiazem converts paroxysmal supraventricular tachycardia (PSVT) to normal sinus rhythm by interrupting the reentry circuit in AV nodal reentrant tachycardias and reciprocating tachycardias, e.g., Wolff-Parkinson-White syndrome (WPW).
Diltiazem prolongs the sinus cycle length. It has no effect on the sinus node recovery time or on the sinoatrial conduction time in patients without SA nodal dysfunction. Diltiazem has no significant electrophysiologic effects on tissues in the heart that are fast sodium channel dependent, e.g., His-Purkinje tissue, atrial and ventricular muscle, and extranodal accessory pathways.
Like other calcium channel antagonists, because of its effect on vascular smooth muscle, diltiazem decreases total peripheral resistance resulting in a decrease in both systolic and diastolic blood pressure.
Hemodynamics
In patients with cardiovascular disease, diltiazem hydrochloride injection administered intravenously in single bolus doses, followed in some cases by a continuous infusion, reduced blood pressure, systemic vascular resistance, the rate-pressure product, and coronary vascular resistance and increased coronary blood flow. In a limited number of studies of patients with compromised myocardium (severe congestive heart failure, acute myocardial infarction, hypertrophic cardiomyopathy), administration of intravenous diltiazem produced no significant effect on contractility, left ventricular end diastolic pressure, or pulmonary capillary wedge pressure. The mean ejection fraction and cardiac output/index remained unchanged or increased. Maximal hemodynamic effects usually occurred within 2 to 5 minutes of an injection. However, in rare instances, worsening of congestive heart failure has been reported in patients with preexisting impaired ventricular function.
Pharmacodynamics
The prolongation of PR interval correlated significantly with plasma diltiazem concentration in normal volunteers using the Sigmoidal Emax model. Changes in heart rate, systolic blood pressure, and diastolic blood pressure did not correlate with diltiazem plasma concentrations in normal volunteers. Reduction in mean arterial pressure correlated linearly with diltiazem plasma concentration in a group of hypertensive patients.
In patients with atrial fibrillation and atrial flutter, a significant correlation was observed between the percent reduction in HR and plasma diltiazem concentration using the Sigmoidal Emax model. Based on this relationship, the mean plasma diltiazem concentration required to produce a 20% decrease in heart rate was determined to be 80 ng/mL. Mean plasma diltiazem concentrations of 130 ng/mL and 300 ng/mL were determined to produce reductions in heart rate of 30% and 40%.
Pharmacokinetics and Metabolism
Following a single intravenous injection in healthy male volunteers, diltiazem hydrochloride appears to obey linear pharmacokinetics over a dose range of 10.5 to 21 mg. The plasma elimination half-life is approximately 3.4 hours. The apparent volume of distribution of diltiazem hydrochloride is approximately 305 L. Diltiazem hydrochloride is extensively metabolized in the liver with a systemic clearance of approximately 65 L/h.
After constant rate intravenous infusion to healthy male volunteers, diltiazem exhibits nonlinear pharmacokinetics over an infusion range of 4.8 to 13.2 mg/h for 24 hours. Over this infusion range, as the dose is increased, systemic clearance decreases from 64 to 48 L/h while the plasma elimination half-life increases from 4.1 to 4.9 hours. The apparent volume of distribution remains unchanged (360 to 391 L). In patients with atrial fibrillation or atrial flutter, diltiazem systemic clearance has been found to be decreased compared to healthy volunteers. In patients administered bolus doses ranging from 2.5 mg to 38.5 mg, systemic clearance averaged 36 L/h. In patients administered continuous infusions at 10 mg/h or 15 mg/h for 24 hours, diltiazem systemic clearance averaged 42 L/h and 31 L/h, respectively.
Based on the results of pharmacokinetic studies in healthy volunteers administered different oral diltiazem hydrochloride formulations, constant rate intravenous infusions of diltiazem hydrochloride at 3, 5, 7, and 11 mg/h are predicted to produce steady-state plasma diltiazem concentrations equivalent to 120-, 180-, 240-, and 360-mg total daily oral doses of diltiazem hydrochloride tablets or diltiazem hydrochloride extended-release capsules.
After oral administration, diltiazem undergoes extensive metabolism in man by deacetylation, N-demethylation, and O-demethylation via cytochrome P-450 (oxidative metabolism) in addition to conjugation. Metabolites N-monodesmethyldiltiazem, desacetyldiltiazem, desacetyl-N-monodesmethyldiltiazem, desacetyl-O-desmethyldiltiazem, and desacetyl-N, O-desmethyldiltiazem have been identified in human urine. Following oral administration, 2% to 4% of the unchanged diltiazem appears in the urine. Drugs which induce or inhibit hepatic microsomal enzymes may alter diltiazem disposition.
Following single intravenous injection of diltiazem hydrochloride, however, plasma concentrations of N-monodesmethyldiltiazem and desacetyldiltiazem, two principal metabolites found in plasma after oral administration, are typically not detected. These metabolites are observed, however, following 24 hour constant rate intravenous infusion. Total radioactivity measurement following short IV administration in healthy volunteers suggests the presence of other unidentified metabolites which attain higher concentrations than those of diltiazem and are more slowly eliminated; half-life of total radioactivity is about 20 hours compared to 2 to 5 hours for diltiazem.
Diltiazem hydrochloride is 70% to 80% bound to plasma proteins. In vitro studies suggest alpha1–acid glycoprotein binds approximately 40% of the drug at clinically significant concentrations. Albumin appears to bind approximately 30% of the drug, while other constituents bind the remaining bound fraction. Competitive in vitro ligand binding studies have shown that diltiazem binding is not altered by therapeutic concentrations of digoxin, phenytoin, hydrochlorothiazide, indomethacin, phenylbutazone, propranolol, salicylic acid, tolbutamide, or warfarin.
Renal insufficiency, or even end-stage renal disease, does not appear to influence diltiazem disposition following oral administration. Liver cirrhosis was shown to reduce diltiazem's apparent oral clearance and prolong its half-life.
-
INDICATIONS AND USAGE
Diltiazem Hydrochloride Injection or Diltiazem Hydrochloride for Injection are indicated for the following:
Atrial Fibrillation or Atrial Flutter
Temporary control of rapid ventricular rate in atrial fibrillation or atrial flutter. It should not be used in patients with atrial fibrillation or atrial flutter associated with an accessory bypass tract such as in Wolff-Parkinson-White (WPW) syndrome or short PR syndrome.
In addition, Diltiazem Hydrochloride Injection is indicated for:
Paroxysmal Supraventricular Tachycardia
Rapid conversion of paroxysmal supraventricular tachycardias (PSVT) to sinus rhythm. This includes AV nodal reentrant tachycardias and reciprocating tachycardias associated with an extranodal accessory pathway such as the WPW syndrome or short PR syndrome. Unless otherwise contraindicated, appropriate vagal maneuvers should be attempted prior to administration of diltiazem hydrochloride injection.
The use of diltiazem hydrochloride injection or diltiazem hydrochloride for injection should be undertaken with caution when the patient is compromised hemodynamically or is taking other drugs that decrease any or all of the following: peripheral resistance, myocardial filling, myocardial contractility, or electrical impulse propagation in the myocardium.
For either indication and particularly when employing continuous intravenous infusion, the setting should include continuous monitoring of the ECG and frequent measurement of blood pressure. A defibrillator and emergency equipment should be readily available.
In domestic controlled trials in patients with atrial fibrillation or atrial flutter, bolus administration of diltiazem hydrochloride injection was effective in reducing heart rate by at least 20% in 95% of patients. Diltiazem hydrochloride injection rarely converts atrial fibrillation or atrial flutter to normal sinus rhythm. Following administration of one or two intravenous bolus doses of diltiazem hydrochloride injection, response usually occurs within 3 minutes and maximal heart rate reduction generally occurs in 2 to 7 minutes. Heart rate reduction may last from 1 to 3 hours. If hypotension occurs, it is generally short-lived, but may last from 1 to 3 hours.
A 24-hour continuous infusion of diltiazem hydrochloride injection in the treatment of atrial fibrillation or atrial flutter maintained at least a 20% heart rate reduction during the infusion in 83% of patients. Upon discontinuation of infusion, heart rate reduction may last from 0.5 hours to more than 10 hours (median duration 7 hours). Hypotension, if it occurs, may be similarly persistent.
In the controlled clinical trials, 3.2% of patients required some form of intervention (typically, use of intravenous fluids or the Trendelenburg position) for blood pressure support following diltiazem hydrochloride injection.
In domestic controlled trials, bolus administration of diltiazem hydrochloride injection was effective in converting PSVT to normal sinus rhythm in 88% of patients within 3 minutes of the first or second bolus dose.
Symptoms associated with the arrhythmia were improved in conjunction with decreased heart rate or conversion to normal sinus rhythm following administration of diltiazem hydrochloride injection.
-
CONTRAINDICATIONS
Injectable forms of diltiazem are contraindicated in:
- Patients with sick sinus syndrome except in the presence of a functioning ventricular pacemaker.
- Patients with second- or third-degree AV block except in the presence of a functioning ventricular pacemaker.
- Patients with severe hypotension or cardiogenic shock.
- Patients who have demonstrated hypersensitivity to the drug.
- Intravenous diltiazem and intravenous beta-blockers should not be administered together or in close proximity (within a few hours).
- Patients with atrial fibrillation or atrial flutter associated with an accessory bypass tract such as in WPW syndrome or short PR syndrome.
As with other agents which slow AV nodal conduction and do not prolong the refractoriness of the accessory pathway (e.g., verapamil, digoxin), in rare instances patients in atrial fibrillation or atrial flutter associated with an accessory bypass tract may experience a potentially life-threatening increase in heart rate accompanied by hypotension when treated with injectable forms of diltiazem. As such, the initial use of injectable forms of diltiazem should be, if possible, in a setting where monitoring and resuscitation capabilities, including DC cardioversion/defibrillation, are present (see OVERDOSAGE). Once familiarity of the patient's response is established, use in an office setting may be acceptable. - Patients with ventricular tachycardia. Administration of other calcium channel blockers to patients with wide complex tachycardia (QRS ≥ 0.12 seconds) has resulted in hemodynamic deterioration and ventricular fibrillation. It is important that an accurate pretreatment diagnosis distinguish wide complex QRS tachycardia of supraventricular origin from that of ventricular origin prior to administration of injectable forms of diltiazem.
-
WARNINGS
- Cardiac Conduction. Diltiazem prolongs AV nodal conduction and refractoriness that may rarely result in second- or third-degree AV block in sinus rhythm. Concomitant use of diltiazem with agents known to affect cardiac conduction may result in additive effects (see Drug Interactions). If high-degree AV block occurs in sinus rhythm, intravenous diltiazem should be discontinued and appropriate supportive measures instituted (see OVERDOSAGE).
- Congestive Heart Failure. Although diltiazem has a negative inotropic effect in isolated animal tissue preparations, hemodynamic studies in humans with normal ventricular function and in patients with a compromised myocardium, such as severe CHF, acute MI, and hypertrophic cardiomyopathy, have not shown a reduction in cardiac index nor consistent negative effects on contractility (dp/dt). Administration of oral diltiazem in patients with acute myocardial infarction and pulmonary congestion documented by x-ray on admission is contraindicated. Experience with the use of diltiazem hydrochloride injection in patients with impaired ventricular function is limited. Caution should be exercised when using the drug in such patients.
- Hypotension. Decreases in blood pressure associated with diltiazem hydrochloride injection therapy may occasionally result in symptomatic hypotension (3.2%). The use of intravenous diltiazem for control of ventricular response in patients with supraventricular arrhythmias should be undertaken with caution when the patient is compromised hemodynamically. In addition, caution should be used in patients taking other drugs that decrease peripheral resistance, intravascular volume, myocardial contractility or conduction.
- Acute Hepatic Injury. In rare instances, significant elevations in enzymes such as alkaline phosphatase, LDH, SGOT, SGPT, and other phenomena consistent with acute hepatic injury have been noted following oral diltiazem. Therefore, the potential for acute hepatic injury exists following administration of intravenous diltiazem.
- Ventricular Premature Beats (VPBs). VPBs may be present on conversion of PSVT to sinus rhythm with diltiazem hydrochloride injection. These VPBs are transient, are typically considered to be benign, and appear to have no clinical significance. Similar ventricular complexes have been noted during cardioversion, other pharmacologic therapy, and during spontaneous conversion of PSVT to sinus rhythm.
-
PRECAUTIONS
General
Diltiazem hydrochloride is extensively metabolized by the liver and excreted by the kidneys and in bile. The drug should be used with caution in patients with impaired renal or hepatic function (see WARNINGS). High intravenous dosages (4.5 mg/kg tid) administered to dogs resulted in significant bradycardia and alterations in AV conduction. In subacute and chronic dog and rat studies designed to produce toxicity, high oral doses of diltiazem were associated with hepatic damage. In special subacute hepatic studies, oral doses of 125 mg/kg and higher in rats were associated with histological changes in the liver, which were reversible when the drug was discontinued. In dogs, oral doses of 20 mg/kg were also associated with hepatic changes; however, these changes were reversible with continued dosing.
Dermatologic events progressing to erythema multiforme and/or exfoliative dermatitis have been infrequently reported following oral diltiazem. Therefore, the potential for these dermatologic reactions exists following exposure to intravenous diltiazem. Should a dermatologic reaction persist, the drug should be discontinued.
Drug Interactions
As with all drugs, care should be exercised when treating patients with multiple medications. Diltiazem is both a substrate and an inhibitor of the cytochrome P-450 3A4 enzyme system. Other drugs that are specific substrates, inhibitors, or inducers of this enzyme system may have a significant impact on the efficacy and side effect profile of diltiazem. Patients taking other drugs that are substrates of CYP450 3A4, especially patients with renal and/or hepatic impairment, may require dosage adjustment when starting or stopping concomitantly administered diltiazem in order to maintain optimum therapeutic blood levels.
Anesthetics
The depression of cardiac contractility, conductivity, and automaticity as well as the vascular dilation associated with anesthetics may be potentiated by calcium channel blockers. When used concomitantly, anesthetics and calcium blockers should be titrated carefully.
Benzodiazepines
Studies showed that diltiazem increased the AUC of midazolam and triazolam by 3- to 4-fold and Cmax by 2-fold, compared to placebo. The elimination half-life of midazolam and triazolam also increased (1.5- to 2.5-fold) during coadministration with diltiazem. These pharmacokinetic effects seen during diltiazem coadministration can result in increased clinical effects (e.g., prolonged sedation) of both midazolam and triazolam.
Beta-blockers
Intravenous diltiazem has been administered to patients on chronic oral beta-blocker therapy. The combination of the two drugs was generally well tolerated without serious adverse effects. If intravenous diltiazem is administered to patients receiving chronic oral beta-blocker therapy, the possibility for bradycardia, AV block, and/or depression of contractility should be considered (see CONTRAINDICATIONS). Oral administration of diltiazem with propranolol in five normal volunteers resulted in increased propranolol levels in all subjects and bioavailability of propranolol was increased approximately 50%. In vitro, propranolol appears to be displaced from its binding sites by diltiazem.
Buspirone
In nine healthy subjects, diltiazem significantly increased the mean buspirone AUC 5.5-fold and Cmax 4.1-fold compared to placebo. The T1/2 and Tmax of buspirone were not significantly affected by diltiazem. Enhanced effects and increased toxicity of buspirone may be possible during concomitant administration with diltiazem. Subsequent dose adjustments may be necessary during coadministration, and should be based on clinical assessment.
Carbamazepine
Concomitant administration of oral diltiazem with carbamazepine has been reported to result in elevated plasma levels of carbamazepine (by 40 to 72%), resulting in toxicity in some cases. Patients receiving these drugs concurrently should be monitored for a potential drug interaction.
Cimetidine
A study in six healthy volunteers has shown a significant increase in peak diltiazem plasma levels (58%) and area-under-the-curve (53%) after a 1-week course of cimetidine at 1200 mg per day and a single dose of diltiazem 60 mg. Ranitidine produced smaller, nonsignificant increases. The effect may be mediated by cimetidine's known inhibition of hepatic cytochrome P-450, the enzyme system responsible for the first-pass metabolism of diltiazem. Patients currently receiving diltiazem therapy should be carefully monitored for a change in pharmacological effect when initiating and discontinuing therapy with cimetidine. An adjustment in the diltiazem dose may be warranted.
Clonidine
Sinus bradycardia resulting in hospitalization and pacemaker insertion has been reported in association with the use of clonidine concurrently with diltiazem. Monitor heart rate in patients receiving concomitant diltiazem and clonidine.
Cyclosporine
A pharmacokinetic interaction between diltiazem and cyclosporine has been observed during studies involving renal and cardiac transplant patients. In renal and cardiac transplant recipients, a reduction of cyclosporine dose ranging from 15% to 48% was necessary to maintain cyclosporine trough concentrations similar to those seen prior to the addition of diltiazem. If these agents are to be administered concurrently, cyclosporine concentrations should be monitored, especially when diltiazem therapy is initiated, adjusted or discontinued.
The effect of cyclosporine on diltiazem plasma concentrations has not been evaluated.
Digitalis
Intravenous diltiazem has been administered to patients receiving either intravenous or oral digitalis therapy. The combination of the two drugs was well tolerated without serious adverse effects. However, since both drugs affect AV nodal conduction, patients should be monitored for excessive slowing of the heart rate and/or AV block.
Ivabradine
Concurrent use of diltiazem increases exposure to ivabradine and may exacerbate bradycardia and conduction disturbances. Avoid concomitant use of ivabradine and diltiazem.
Quinidine
Diltiazem significantly increases the AUC(0→∞) of quinidine by 51%, T1/2 by 36% and decreases its CLoral by 33%. Monitoring for quinidine adverse effects may be warranted and the dose adjusted accordingly.
Rifampin
Coadministration of rifampin with diltiazem lowered the diltiazem plasma concentrations to undetectable levels. Coadministration of diltiazem with rifampin or any known CYP3A4 inducer should be avoided when possible, and alternative therapy considered.
Statins
Diltiazem is an inhibitor of CYP3A4 and has been shown to increase significantly the AUC of some statins. The risk of myopathy and rhabdomyolysis with statins metabolized by CYP3A4 may be increased with concomitant use of diltiazem. When possible, use a non-CYP3A4-metabolized statin together with diltiazem; otherwise, dose adjustments for both diltiazem and the statin should be considered along with close monitoring for signs and symptoms of any statin related adverse events.
In a healthy volunteer cross-over study (N = 10), coadministration of a single 20 mg dose of simvastatin at the end of a 14-day regimen with 120 mg BID diltiazem SR resulted in a 5-fold increase in mean simvastatin AUC versus simvastatin alone. Subjects with increased average steady-state exposures of diltiazem showed a greater-fold increase in simvastatin exposure. Computer-based simulations showed that at a daily dose of 480 mg of diltiazem, an 8- to 9-fold mean increase in simvastatin AUC can be expected. If coadministration of simvastatin with diltiazem is required, limit the daily doses of simvastatin to 10 mg and diltiazem to 240 mg.
In a ten-subject randomized, open label, 4-way cross-over study, coadministration of diltiazem (120 mg bid, diltiazem SR for 2 weeks) with a single 20 mg dose of lovastatin resulted in a 3- to 4-fold increase in mean lovastatin AUC and Cmax versus lovastatin alone. In the same study, there was no significant change in 20 mg single-dose pravastatin AUC and Cmax during diltiazem coadministration. Diltiazem plasma levels were not significantly affected by lovastatin or pravastatin.
Carcinogenesis, Mutagenesis, Impairment of Fertility
A 24-month study in rats at oral dosage levels of up to 100 mg/kg/day and a 21-month study in mice at oral dosage levels of up to 30 mg/kg/day showed no evidence of carcinogenicity. There was also no mutagenic response in vitro or in vivo in mammalian cell assays or in vitro in bacteria. No evidence of impaired fertility was observed in a study performed in male and female rats at oral dosages of up to 100 mg/kg/day.
Pregnancy
Reproduction studies have been conducted in mice, rats, and rabbits.
Administration of oral doses ranging from five to ten times greater (on a mg/kg basis) than the daily recommended oral antianginal therapeutic dose has resulted in embryo and fetal lethality. These doses, in some studies, have been reported to cause skeletal abnormalities. In the perinatal/postnatal studies there was some reduction in early individual pup weights and survival rates. There was an increased incidence of stillbirths at doses of 20 times the human oral antianginal dose or greater.
There are no well-controlled studies in pregnant women; therefore, use diltiazem hydrochloride in pregnant women only if the potential benefit justifies the potential risk to the fetus.
Nursing Mothers
Diltiazem is excreted in human milk. One report with oral diltiazem suggests that concentrations in breast milk may approximate serum levels. If use of diltiazem hydrochloride is deemed essential, an alternative method of infant feeding should be instituted.
Geriatric Use
Clinical studies of diltiazem did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
Atrial fibrillation or atrial flutter
In clinical studies with diltiazem hydrochloride injection for AF/Fl, 135 of 257 patients were over 65 years of age. No overall differences in safety or effectiveness were observed between these patients and younger patients, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
In subgroup analysis of double-blind and open-label trials following first-dose response, 116 patients over 65 years of age had a response rate of 84%. One hundred two (102) patients <65 had a response rate of 78%. In subgroup analysis following a two-dose procedure in double-blind and open-label studies, 104 patients over 65 years of age and 95 patients <65 both had a 95% response rate.
Paroxysmal supraventricular tachycardia
Clinical studies of diltiazem hydrochloride injection for PSVT did not include sufficient numbers of patients aged 65 and over to determine whether they respond differently from younger patients. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
Diltiazem hydrochloride is extensively metabolized by the liver and excreted by the kidneys and in bile. The risk of toxic reactions to this drug may be greater in patients with impaired renal or hepatic function. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function. As with all drugs, care should be exercised when treating patients with multiple medications (see PRECAUTIONS, General, and Drug Interactions.)
-
ADVERSE REACTIONS
The following adverse reaction rates are based on the use of diltiazem hydrochloride injection in over 400 domestic clinical trial patients with atrial fibrillation/flutter or PSVT under double-blind or open-label conditions. Worldwide experience in over 1,300 patients was similar.
Adverse events reported in controlled and uncontrolled clinical trials were generally mild and transient. Hypotension was the most commonly reported adverse event during clinical trials. Asymptomatic hypotension occurred in 4.3% of patients. Symptomatic hypotension occurred in 3.2% of patients. When treatment for hypotension was required, it generally consisted of administration of saline or placing the patient in the Trendelenburg position. Other events reported in at least 1% of the diltiazem-treated patients were injection site reactions (e.g., itching, burning) - 3.9%, vasodilation (flushing) - 1.7%, and arrhythmia (junctional rhythm or isorhythmic dissociation) - 1%.
In addition, the following events were reported infrequently (less than 1%):
Cardiovascular: Asystole, atrial flutter, AV block first degree, AV block second degree, bradycardia, chest pain, congestive heart failure, sinus pause, sinus node dysfunction, syncope, ventricular arrhythmia, ventricular fibrillation, ventricular tachycardia
Dermatologic: Pruritus, sweating
Gastrointestinal: Constipation, elevated SGOT or alkaline phosphatase, nausea, vomiting
Nervous System: Dizziness, paresthesia
Other: Amblyopia, asthenia, dry mouth, dyspnea, edema, headache, hyperuricemia
Although not observed in clinical trials with diltiazem hydrochloride injection, the following events associated with oral diltiazem may occur:
Cardiovascular: AV block (third degree), bundle branch block, ECG abnormality, palpitations, syncope, tachycardia, ventricular extrasystoles
Dermatologic: Alopecia, erythema multiforme (including Stevens-Johnson syndrome, toxic epidermal necrolysis), exfoliative dermatitis, leukocytoclastic vasculitis, petechiae, photosensitivity, purpura, rash, urticaria
Gastrointestinal: Anorexia, diarrhea, dysgeusia, dyspepsia, mild elevations of SGPT and LDH, thirst, weight increase
Nervous System: Abnormal dreams, amnesia, depression, extrapyramidal symptoms, gait abnormality, hallucinations, insomnia, nervousness, personality change, somnolence, tremor
Other: Acute generalized exanthematous pustulosis, allergic reactions, angioedema (including facial or periorbital edema), CPK elevation, epistaxis, eye irritation, gingival hyperplasia, hemolytic anemia, hyperglycemia, impotence, increased bleeding time, leukopenia, muscle cramps, myopathy, nasal congestion, nocturia, osteoarticular pain, photosensitivity (including lichenoid keratosis and hyperpigmentation at sun-exposed skin areas), polyuria, retinopathy, sexual difficulties, thrombocytopenia, tinnitus.
Events such as myocardial infarction have been observed which are not readily distinguishable from the natural history of the disease for the patient.
-
OVERDOSAGE
Overdosage experience is limited. In the event of overdosage or an exaggerated response, appropriate supportive measures should be employed. The following measures may be considered:
Bradycardia: Administer atropine (0.6 to 1 mg). If there is no response to vagal blockade administer isoproterenol cautiously.
High-degree AV Block: Treat as for bradycardia above. Fixed high-degree AV block should be treated with cardiac pacing.
Cardiac Failure: Administer inotropic agents (isoproterenol, dopamine, or dobutamine) and diuretics.
Hypotension: Vasopressors (e.g., dopamine or norepinephrine).
The effectiveness of intravenous calcium administration to reverse the pharmacological effects of diltiazem overdose has been inconsistent. In a few reported cases, overdose with calcium channel blockers associated with hypotension and bradycardia that was initially refractory to atropine became more responsive to atropine after the patients received intravenous calcium. In some cases intravenous calcium has been administered (1 g calcium chloride or 3 g calcium gluconate) over 5 minutes, and repeated every 10 to 20 minutes as necessary. Calcium gluconate has also been administered as a continuous infusion at a rate of 2 g per hour for 10 hours. Infusions of calcium for 24 hours or more may be required. Patients should be monitored for signs of hypercalcemia.
Actual treatment and dosage should depend on the severity of the clinical situation and the judgment and experience of the treating physician.
Diltiazem does not appear to be removed by peritoneal or hemodialysis. Limited data suggest that plasmapheresis or charcoal hemoperfusion may hasten diltiazem elimination following overdose.
The intravenous LD50's in mice and rats were 60 and 38 mg/kg, respectively. The toxic dose in man is not known.
-
DOSAGE AND ADMINISTRATION
Direct Intravenous Single Injections (Bolus)
The initial dose of diltiazem hydrochloride injection should be 0.25 mg/kg actual body weight as a bolus administered over 2 minutes (20 mg is a reasonable dose for the average patient). If response is inadequate, a second dose may be administered after 15 minutes. The second bolus dose of diltiazem hydrochloride injection should be 0.35 mg/kg actual body weight administered over 2 minutes (25 mg is a reasonable dose for the average patient). Subsequent intravenous bolus doses should be individualized for each patient. Patients with low body weights should be dosed on a mg/kg basis. Some patients may respond to an initial dose of 0.15 mg/kg, although duration of action may be shorter. Experience with this dose is limited.
Continuous Intravenous Infusion
For continued reduction of the heart rate (up to 24 hours) in patients with atrial fibrillation or atrial flutter, an intravenous infusion of diltiazem hydrochloride injection or diltiazem hydrochloride for injection may be administered. (For reconstitution of diltiazem hydrochloride for injection, see instructions contained within packaging.) Immediately following bolus administration of 20 mg (0.25 mg/kg) or 25 mg (0.35 mg/kg) diltiazem hydrochloride injection and reduction of heart rate, begin an intravenous infusion of diltiazem hydrochloride injection or diltiazem hydrochloride for injection. The recommended initial infusion rate of diltiazem hydrochloride injection or diltiazem hydrochloride for injection is 10 mg/h. Some patients may maintain response to an initial rate of 5 mg/h. The infusion rate may be increased in 5 mg/h increments up to 15 mg/h as needed, if further reduction in heart rate is required. The infusion may be maintained for up to 24 hours.
Diltiazem shows dose-dependent, non-linear pharmacokinetics. Duration of infusion longer than 24 hours and infusion rates greater than 15 mg/h have not been studied. Therefore, infusion duration exceeding 24 hours and infusion rates exceeding 15 mg/h are not recommended.
Dilution
To prepare diltiazem hydrochloride injection for continuous intravenous infusion, aseptically transfer the appropriate quantity (see chart) of diltiazem hydrochloride to the desired volume of either Normal Saline, D5W, or D5W/0.45% NaCl. Mix thoroughly. Keep diluted diltiazem hydrochloride injection refrigerated until use. Use within 24 hours.
To prepare diltiazem hydrochloride for injection for continuous intravenous infusion, assemble the ADD-Vantage vial as directed for use with either 0.9% Sodium Chloride or Dextrose (5%) injection. Mix thoroughly. Keep diluted diltiazem hydrochloride for injection at controlled room temperature 15° to 30°C (59° to 86°F) [See USP] or refrigerated 2° to 8°C (36° to 46°F) until use. Use within 24 hours.
Diltiazem Hydrochloride Injection Diluent Volume Quantity of Diltiazem hydrochloride injection Final Concentration Administration Dose* Infusion Rate - * 5 mg/h may be appropriate for some patients
100 mL 125 mg (25 mL)
Final Volume 125 mL1 mg/mL 10 mg/h
15 mg/h10 mL/h
15 mL/h250 mL 250 mg (50 mL)
Final Volume 300 mL0.83 mg/mL 10 mg/h
15 mg/h12 mL/h
18 mL/h500 mL 250 mg (50 mL)
Final Volume 550 mL0.45 mg/mL 10 mg/h
15 mg/h22 mL/h
33 mL/h -
INSTRUCTIONS FOR USE
To Use Vial in ADD-Vantage® Flexible Diluent Container
To Open:
Peel overwrap at corner and remove solution container. Some opacity of the plastic due to moisture absorption during the sterilization process may be observed. This is normal and does not affect the solution quality or safety. The opacity will diminish gradually.
To Assemble Vial and Flexible Diluent Container:
(Use Aseptic Technique)
- Remove the protective covers from the top of the vial and the vial port on the diluent container as follows:
- To remove the breakaway vial cap, swing the pull ring over the top of the vial and pull down far enough to start the opening (SEE FIGURE 1.), then pull straight up to remove the cap. (SEE FIGURE 2.) NOTE: Do not access vial with syringe.
- To remove the vial port cover, grasp the tab on the pull ring, pull up to break the tie membrane, then pull back to remove the cover. (SEE FIGURE 3.)
- Screw the vial into the vial port until it will go no further. THE VIAL MUST BE SCREWED IN TIGHTLY TO ASSURE A SEAL. This occurs approximately 1/2 turn (180°) after the first audible click. (SEE FIGURE 4.) The clicking sound does not assure a seal; the vial must be turned as far as it will go.
NOTE: Once vial is seated, do not attempt to remove. (SEE FIGURE 4.) - Recheck the vial to assure that it is tight by trying to turn it further in the direction of assembly.
- Label appropriately.
To Reconstitute the Drug:
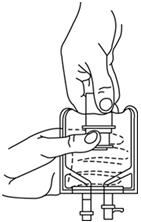
- Squeeze the bottom of the diluent container gently to inflate the portion of the container surrounding the end of the drug vial.
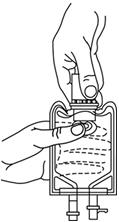
- With the other hand, push the drug vial down into the container telescoping the walls of the container. Grasp the inner cap of the vial through the walls of the container. (SEE FIGURE 5.)
- Pull the inner cap from the drug vial. (SEE FIGURE 6.) Verify that the rubber stopper has been pulled out, allowing the drug and diluent to mix.
- Mix container contents thoroughly and use within the specified time.
Preparation for Administration:
(Use Aseptic Technique)
- Confirm the activation and admixture of vial contents.
- Check for leaks by squeezing container firmly. If leaks are found, discard unit as sterility may be impaired.
- Close flow control clamp of administration set.
- Remove cover from outlet port at bottom of container.
- Insert piercing pin of administration set into port with a twisting motion until the pin is firmly seated. NOTE: See full directions on administration set carton.
- Lift the free end of the hanger loop on the bottom of the vial, breaking the two tie strings. Bend the loop outward to lock it in the upright position, then suspend container from hanger.
- Squeeze and release drip chamber to establish proper fluid level in chamber.
- Open flow control clamp and clear air from set. Close clamp.
- Attach set to venipuncture device. If device is not indwelling, prime and make venipuncture.
- Regulate rate of administration with flow control clamp.
WARNING: Do not use flexible containers in series connections.
Compatibility: Diltiazem hydrochloride injection and diltiazem hydrochloride for injection were tested for compatibility with three commonly used intravenous fluids at a maximal concentration of 1 mg diltiazem hydrochloride per milliliter. Diltiazem hydrochloride injection and diltiazem hydrochloride for injection were found to be physically compatible and chemically stable in the following parenteral solutions for at least 24 hours when stored in glass (diltiazem hydrochloride injection only) or polyvinylchloride (PVC) bags at controlled room temperature 20° to 25°C (68° to 77°F) [see USP] or under refrigeration 2° to 8°C (36° to 46°F).
- dextrose (5%) injection USP
- sodium chloride (0.9%) injection USP
- dextrose (5%) and sodium chloride (0.45%) injection USP
Physical Incompatibilities:
Because of potential physical incompatibilities, it is recommended that diltiazem hydrochloride injection or diltiazem hydrochloride for injection not be mixed with any other drugs in the same container. If possible, it is recommended that diltiazem hydrochloride injection or diltiazem hydrochloride for injection not be co-infused in the same intravenous line. Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration whenever solution and container permit.
Diltiazem hydrochloride injection. Physical incompatibilities (precipitate formation or cloudiness) were observed when diltiazem hydrochloride injection was infused in the same intravenous line with the following drugs: acetazolamide, acyclovir, aminophylline, ampicillin, ampicillin sodium/sulbactam sodium, cefamandole, cefoperazone, diazepam, furosemide, hydrocortisone sodium succinate, insulin, (regular: 100 units/mL), methylprednisolone sodium succinate, mezlocillin, nafcillin, phenytoin, rifampin, and sodium bicarbonate.
Diltiazem hydrochloride for injection. Physical incompatibilities (precipitate formation or cloudiness) were observed when diltiazem hydrochloride for injection at a concentration of 1 mg/mL diluted in normal saline was infused in the same intravenous line with the following drugs: acetazolamide, acyclovir, cefoperazone sodium, diazepam, furosemide, phenytoin and rifampin.
NOTE: Diltiazem hydrochloride for injection at a concentration of 1 mg/mL diluted in normal saline was infused in the same intravenous line and was found to be compatible with the following drugs: aminophylline, ampicillin sodium, ampicillin sodium/sulbactam sodium, cefamandole, hydrocortisone sodium succinate, regular insulin (100 units/mL), methylprednisolone sodium succinate, mezlocillin sodium, nafcillin sodium and sodium bicarbonate.
Transition to Further Antiarrhythmic Therapy.
Transition to other antiarrhythmic agents following administration of diltiazem hydrochloride injection is generally safe. However, reference should be made to the respective agent manufacturer's package insert for information relative to dosage and administration.
In controlled clinical trials, therapy with antiarrhythmic agents to maintain reduced heart rate in atrial fibrillation or atrial flutter or for prophylaxis of PSVT was generally started within 3 hours after bolus administration of diltiazem hydrochloride injection. These antiarrhythmic agents were intravenous or oral digoxin, Class 1 antiarrhythmics (e.g., quinidine, procainamide), calcium channel blockers, and oral beta-blockers.
Experience in the use of antiarrhythmic agents following maintenance infusion of diltiazem hydrochloride injection is limited. Patients should be dosed on an individual basis and reference should be made to the respective manufacturer's package insert for information relative to dosage and administration.
- Remove the protective covers from the top of the vial and the vial port on the diluent container as follows:
-
HOW SUPPLIED
Diltiazem Hydrochloride Injection is supplied in single-dose Fliptop vials as follows:
Unit of Sale Concentration Each NDC: 0409-1171-01
Carton containing 10 Single-Dose Fliptop Vials25 mg/5 mL
(5 mg/mL)NDC: 0409-1171-11
5 mL Single-Dose Fliptop VialNDC: 0409-1171-02
Carton containing 10 Single-Dose Fliptop Vials50 mg/10 mL
(5 mg/mL)NDC: 0409-1171-12
10 mL Single-Dose Fliptop VialDILTIAZEM HYDROCHLORIDE INJECTION IS TO BE STORED UNDER REFRIGERATION 2 TO 8°C (36 TO 46°F). DO NOT FREEZE. MAY BE STORED AT ROOM TEMPERATURE FOR UP TO 1 MONTH. DESTROY AFTER 1 MONTH AT ROOM TEMPERATURE. SINGLE-DOSE VIALS. DISCARD UNUSED PORTION.
Diltiazem Hydrochloride for Injection for continuous infusion is supplied in single-dose ADD-Vantage vials as follows:
Unit of Sale Size Each NDC: 0409-4350-03
Tray containing 10 ADD-Vantage Vials100 mg NDC: 0409-4350-13
100 mg/ADD-Vantage Vial - SPL UNCLASSIFIED SECTION
- PRINCIPAL DISPLAY PANEL - 5 mL Vial Label
- PRINCIPAL DISPLAY PANEL - 5 mL Vial Carton
- PRINCIPAL DISPLAY PANEL - 10 mL Vial Label
- PRINCIPAL DISPLAY PANEL - 10 mL Vial Carton
- PRINCIPAL DISPLAY PANEL - 100 mg Vial Label
-
PRINCIPAL DISPLAY PANEL - 100 mg Vial Tray
10 Single-dose ADD-Vantage™ Vials
Sterile Powder
Rx only
NDC: 0409-4350-03
Contains 10 of NDC: 0409-4350-13Diltiazem HCl for Injection
For Continuous Intravenous Infusion
Not For Bolus
Usual Dosage: See insert.Equivalent to 100 mg Diltiazem HCl
Hospira
-
INGREDIENTS AND APPEARANCE
DILTIAZEM HYDROCHLORIDE
diltiazem hydrochloride injection, solutionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 0409-1171 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength DILTIAZEM HYDROCHLORIDE (UNII: OLH94387TE) (DILTIAZEM - UNII:EE92BBP03H) DILTIAZEM HYDROCHLORIDE 5 mg in 1 mL Inactive Ingredients Ingredient Name Strength CITRIC ACID MONOHYDRATE (UNII: 2968PHW8QP) 0.75 mg in 1 mL TRISODIUM CITRATE DIHYDRATE (UNII: B22547B95K) 0.65 mg in 1 mL SORBITOL (UNII: 506T60A25R) 50 mg in 1 mL WATER (UNII: 059QF0KO0R) SODIUM HYDROXIDE (UNII: 55X04QC32I) HYDROCHLORIC ACID (UNII: QTT17582CB) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 0409-1171-01 10 in 1 CARTON 09/13/2006 1 NDC: 0409-1171-11 5 mL in 1 VIAL, SINGLE-DOSE; Type 0: Not a Combination Product 2 NDC: 0409-1171-02 10 in 1 CARTON 05/05/2006 2 NDC: 0409-1171-12 10 mL in 1 VIAL, SINGLE-DOSE; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA074941 05/05/2006 DILTIAZEM HYDROCHLORIDE
diltiazem hydrochloride injection, powder, lyophilized, for solutionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 0409-4350 Route of Administration INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength DILTIAZEM HYDROCHLORIDE (UNII: OLH94387TE) (DILTIAZEM - UNII:EE92BBP03H) DILTIAZEM HYDROCHLORIDE 100 mg Inactive Ingredients Ingredient Name Strength MANNITOL (UNII: 3OWL53L36A) 75 mg Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 0409-4350-03 10 in 1 TRAY 04/30/2005 1 NDC: 0409-4350-13 1 in 1 VIAL, PATENT DELIVERY SYSTEM; Type 2: Prefilled Drug Delivery Device/System (syringe, patch, etc.) Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA075853 04/30/2005 Labeler - Hospira, Inc. (141588017) Establishment Name Address ID/FEI Business Operations Hospira, Inc. 030606222 ANALYSIS(0409-1171, 0409-4350) , LABEL(0409-1171, 0409-4350) , MANUFACTURE(0409-1171, 0409-4350) , PACK(0409-1171, 0409-4350)





© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.