L-METHYL-MC- levomefolate calcium, riboflavin, pyridoxine hydrochloride, and cyanocobalamin tablet, coated
L-Methyl-MC by
Drug Labeling and Warnings
L-Methyl-MC by is a Other medication manufactured, distributed, or labeled by Virtus Pharmaceuticals. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
- SPL UNCLASSIFIED SECTION
-
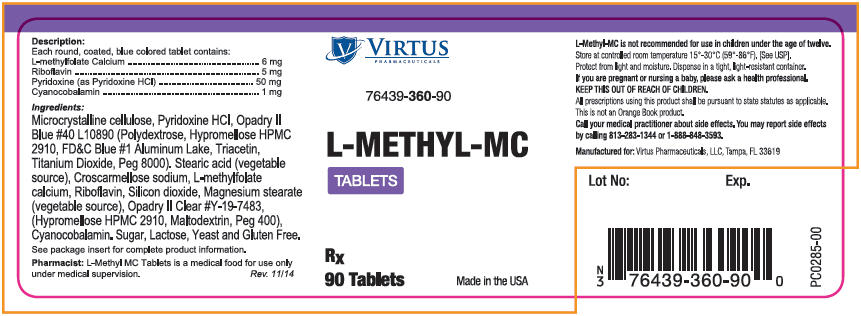
Description
Each round coated blue colored tablet contains:
Dietary Ingredients: L-methylfolate Calcium 6 mg Riboflavin 5 mg Pyridoxine (as Pyridoxine HCl) 50 mg Cyanocobalamin 1 mg Ingredients
Microcrystalline Cellulose, Pyridoxine HCl,Opadry II Blue #40L10890 (Polydextrose, Hypromellose HPMC 2910, FD&C Blue #1 Aluminum Lake, Triacetin, Titanium Dioxide, Peg 8000). Stearic Acid (Vegetable Source), Croscarmellose Sodium, L-methylfolate Calcium, Riboflavin, Silicon Dioxide, Magnesium Stearate (Vegetable Source), Opadry II Clear #Y-19-7483, (Hypromellose HPMC 2910, Maltodextrin, Peg 400), Cyanocobalamin.
L-Methyl-MC Tablets do not contain sugar, lactose, yeast or gluten.
- Indication and Usage
-
Precautions
Folates, when administered as a single agent in doses above 0.1mg daily, may obscure pernicious anemia in that hematologic remission can occur while neurological manifestations remain progressive. The 1 mg of cyanocobalamin contained in L-Methyl-MC Tablets has been shown to provide an adequate amount of cyanocobalamin to address this precaution4. A safe upper limit of 100 mg per day has been established for the unsupervised medical use of pyridoxine. Consider all sources of pyridoxine supplementation when prescribing L-Methyl-MC Tablets.
-
Adverse Reactions
While allergic sensitization has been reported following both oral and parenteral administration of folic acid, allergic sensitization has not been reported with the use of L-Methylfolate Calcium. Paresthesia, somnolence, nausea and headaches have been reported with pyridoxine. Mild transient diarrhea, polycythemia vera, itching, transitory exanthema and the feeling of swelling of the entire body has been associated with cyanocobalamin. Transient headaches have been reported infrequently with the use of L-Methyl-MC Tablets. If headaches should occur with the use of L-Methyl-MC Tablets consult with your medical practitioner.
- Contraindications
-
Drug Interactions
L-Methyl-MC Tablets added to other drugs
High dose folic acid may result in decreased serum levels for pyrimethamine and first-generation anticonvulsants (carbamazepine, fosphenytoin, phenytoin, phenobarbital, primidone, valproic acid, valproate). This may possibly reduce first generation anticonvulsants effectiveness and/or increasing the frequency of seizures in susceptible patients. While the concurrent use of folic acid and first generation anticonvulsants or pyrimethamine may result in decreased efficacy of anticonvulsants, no such decreased effectiveness has been reported with the use of L-methylfolate. Nevertheless, caution should be used when prescribing L-METHYL-MC TABLETS among patients who are receiving treatment with first generation anticonvulsants or pyrimethamine. Pyridoxine should not be given to patients receiving the drug levodopa, because the action of levodopa is antagonized by pyridoxine. However, pyridoxine may be used concurrently in patients receiving a preparation containing both carbidopa and levodopa. Capecitabine (Xeloda®) toxicity may increase with the addition of leucovorin (5-formyltetrahydrofolate) (folate).
Drugs added to L-METHYL-MC TABLETS
Antibiotics may alter the intestinal microflora and may decrease the absorption of cyanocobalamin. Cholestyramine, colchicines or colestipol may decrease the enterohepatic reabsorption of cyanocobalamin. Metformin, para-aminosalicylic acid and potassium chloride may decrease the absorption of cyanocobalamin. Nitrous oxide can produce a functional cyanocobalamin deficiency. Several drugs are associated with lowering serum folate levels or reducing the amount of active folate available. First generation anticonvulsants (carbamazepine, fosphenytoin, phenytoin, phenobarbital, primidone, valproic acid, valproate) and lamotrigine (a second-generation anticonvulsant) may decrease folate plasma levels. Information on other second-generation anticonvulsants impact on folate levels is limited and cannot be ruled out. Methotrexate, alcohol (in excess), sulfasalazine, cholestyramine, colchicine, colestipol, L-dopa, methylprednisone, NSAIDs (high dose), pancreatic enzymes (pancrelipase, pancratin), pentamidine, pyrimethamine, smoking, triamterene, and trimethoprim may decrease folate plasma levels. Warfarin can produce significant impairment in folate status after a 6 month therapy.
- Patient Information
- Dosage and Administration
-
How Supplied
Available as a round coated blue colored tablet. Debossed with "V360" on one side and blank on the other. Commercial product is supplied in bottles of 90 tablets (76439-360-901). Use under medical/physician supervision.
- 1 Virtus Pharmaceuticals, LLC does not represent this product code to be a National Drug Code (NDC) number. Instead, Virtus Pharmaceuticals, LLC has assigned a product code formatted according to standard industry practice to meet the formatting requirements of pharmacy and health insurance computer systems.
- Patents
-
References
1 Lehmann M, Regland B, Blennow K, and Gottfries CG: Vitamin B12-B6-Folate Treatment Improves Blood-Brain Barrier Function in Patients with Hyperhomocysteinaemia and Mild Cognitive Impairment. Dementia and Geriatric Cognitive Disorders 2003;16:145-150.
2 Nilsson K, Gustafson L, and Hultberg B: Improvement of cognitive functions after cobalamin/folate supplementation in elderly patients with dementia and elevated plasma homocysteine. International Journal of Geriatric Psychiatry 2001;16:609-614.
3 Seshadri S, Beiser A, Selhub J, Jacques PF, Rosenberg IH, D'Agostino RB, Wilson PWF, and Wolf PA: Plasma Homocysteine As A Risk Factor For Dementia And Alzheimer's Disease. New England Journal of Medicine 2002:Vol346, No. 7:476-483.
4 Lederle FA: Oral cobalamin for pernicious anaemia: medicine's best kept secret. JAMA 1991;265:94-95.
- SPL UNCLASSIFIED SECTION
- PRINCIPAL DISPLAY PANEL - 90 Tablet Bottle Label
-
INGREDIENTS AND APPEARANCE
L-METHYL-MC
levomefolate calcium, riboflavin, pyridoxine hydrochloride, and cyanocobalamin tablet, coatedProduct Information Product Type MEDICAL FOOD Item Code (Source) NHRIC:76439-360 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength Levomefolate Calcium (UNII: A9R10K3F2F) (Levomefolic Acid - UNII:8S95DH25XC) Levomefolate Calcium 6 mg Riboflavin (UNII: TLM2976OFR) (Riboflavin - UNII:TLM2976OFR) Riboflavin 5 mg Pyridoxine Hydrochloride (UNII: 68Y4CF58BV) (Pyridoxine - UNII:KV2JZ1BI6Z) Pyridoxine Hydrochloride 50 mg Cyanocobalamin (UNII: P6YC3EG204) (Cyanocobalamin - UNII:P6YC3EG204) Cyanocobalamin 1 mg Inactive Ingredients Ingredient Name Strength Cellulose, Microcrystalline (UNII: OP1R32D61U) Polydextrose (UNII: VH2XOU12IE) FD&C Blue No. 1 (UNII: H3R47K3TBD) Aluminum Oxide (UNII: LMI26O6933) Triacetin (UNII: XHX3C3X673) Titanium Dioxide (UNII: 15FIX9V2JP) Polyethylene Glycol 8000 (UNII: Q662QK8M3B) Stearic Acid (UNII: 4ELV7Z65AP) Croscarmellose Sodium (UNII: M28OL1HH48) Silicon Dioxide (UNII: ETJ7Z6XBU4) Magnesium Stearate (UNII: 70097M6I30) Maltodextrin (UNII: 7CVR7L4A2D) Polyethylene Glycol 400 (UNII: B697894SGQ) Product Characteristics Color BLUE Score no score Shape ROUND Size 10mm Flavor Imprint Code V360 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NHRIC:76439-360-90 90 in 1 BOTTLE Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date MEDICAL FOOD 02/09/2015 Labeler - Virtus Pharmaceuticals (969483143)
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.