QUINAPRIL HYDROCHLORIDE/HYDROCHLOROTHIAZIDE tablet, film coated
Quinapril Hydrochloride/Hydrochlorothiazide by
Drug Labeling and Warnings
Quinapril Hydrochloride/Hydrochlorothiazide by is a Prescription medication manufactured, distributed, or labeled by Lake Erie Medical DBA Quality Care Products LLC. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
BOXED WARNING
(What is this?)
WARNING: FETAL TOXICITY
- When pregnancy is detected, discontinue quinapril hydrochloride/hydrochlorothiazide as soon as possible.
- Drugs that act directly on the renin-angiotensin system can cause injury and death to the developing fetus. See WARNINGS: Fetal Toxicity.
-
DESCRIPTION
Quinapril hydrochloride/hydrochlorothiazide is a fixed-combination tablet that combines an angiotensin-converting enzyme (ACE) inhibitor, quinapril hydrochloride, and a thiazide diuretic, hydrochlorothiazide.
Quinapril hydrochloride is chemically described as [3S-[2[R*(R*)], 3R*]]-2-[2-[[1-(ethoxycarbonyl)-3-phenylpropyl]amino]-1-oxopropyl]-1,2,3,4-tetrahydro-3-isoquinolinecarboxylic acid, monohydrochloride. Its molecular formula is C25H30N2O5. HCl and its structural formula is: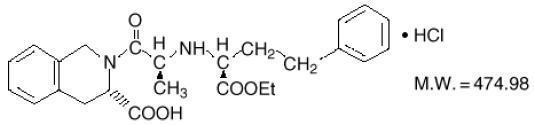
Quinapril hydrochloride USP is a white to off-white amorphous powder that is freely soluble in aqueous solvents.
Hydrochlorothiazide is chemically described as: 6-Chloro-3,4-dihydro-2H-1,2,4-benzothiadiazine-7-sulfonamide 1,1-dioxide. Its molecular formula is C7H8CIN3O4S2 and its structural formula is: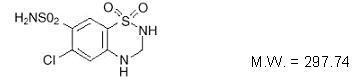
Hydrochlorothiazide USP is a white to off-white, crystalline powder which is slightly soluble in water but freely soluble in sodium hydroxide solution.
Quinapril hydrochloride/hydrochlorothiazide is available for oral use as fixed combination tablets in three strengths of quinapril with hydrochlorothiazide: 10 mg with 12.5 mg (quinapril hydrochloride/hydrochlorothiazide 10/12.5), 20 mg with 12.5 mg (quinapril hydrochloride/hydrochlorothiazide 20/12.5), and 20 mg with 25 mg (quinapril hydrochloride/hydrochlorothiazide20/25). The strength of the quinapril hydrochloride component is in terms of quinapril. Inactive ingredients: lactose monohydrate, magnesium carbonate, crospovidone, povidone, magnesium stearate, hypromellose, hydroxypropyl cellulose, polyethylene glycol 400, titanium dioxide, iron oxide red and iron oxide yellow. -
CLINICAL PHARMACOLOGY
Mechanism of Action
The principal metabolite of quinapril, quinaprilat, is an inhibitor of ACE activity in human subjects and animals. ACE is peptidyl dipeptidase that catalyzes the conversion of angiotensin I to the vasoconstrictor, angiotensin II. The effect of quinapril in hypertension appears to result primarily from the inhibition of circulating and tissue ACE activity, thereby reducing angiotensin II formation. Quinapril inhibits the elevation in blood pressure caused by intravenously administered angiotensin I, but has no effect on the pressor response to angiotensin II, norepinephrine, or epinephrine. Angiotensin II also stimulates the secretion of aldosterone from the adrenal cortex, thereby facilitating renal sodium and fluid reabsorption. Reduced aldosterone secretion by quinapril may result in a small increase in serum potassium. In controlled hypertension trials, treatment with quinapril alone resulted in mean increases in potassium of 0.07 mmol/L (see PRECAUTIONS). Removal of angiotensin II negative feedback on renin secretion leads to increased plasma renin activity (PRA).
While the principal mechanism of antihypertensive effect is thought to be through the renin-angiotensin-aldosterone system, quinapril exerts antihypertensive actions even in patients with low renin hypertension. Quinapril was an effective antihypertensive in all races studied, although it was somewhat less effective in blacks (usually a predominantly low renin group) than in non-blacks. ACE is identical to kininase II, an enzyme that degrades bradykinin, a potent peptide vasodilator; whether increased levels of bradykinin play a role in the therapeutic effect of quinapril remains to be elucidated.
Hydrochlorothiazide is a thiazide diuretic. Thiazides affect the renal tubular mechanisms of electrolyte reabsorption, directly increasing excretion of sodium and chloride in approximately equivalent amounts. Indirectly, the diuretic action of hydrochlorothiazide reduces plasma volume, with consequent increases in plasma renin activity, increases in aldosterone secretion, increases in urinary potassium loss, and decreases in serum potassium. The renin-aldolsterone link is mediated by angiotensin, so coadministration of an ACE inhibitor tends to reverse the potassium loss associated with these diuretics.
The mechanism of the antihypertensive effect of thiazides is unknown.
Pharmacokinetics and Metabolism
The rate and extent of absorption of quinapril and hydrochlorothiazide from quinapril hydrochloride/hydrochlorothiazide tablets are not different, respectively, from the rate and extent of absorption of quinapril and hydrochlorothiazide from immediate-release monotherapy formulations, either administered concurrently or separately. Following oral administration of quinapril monotherapy tablets, peak plasma quinapril concentrations are observed within 1 hour. Based on recovery of quinapril and its metabolites in urine, the extent of absorption is at least 60%. The absorption of hydrochlorothiazide is somewhat slower (1 to 2.5 hours) and more complete (50% to 80%).
The rate of quinapril absorption was reduced by 14% when quinapril hydrochloride/hydrochlorothiazide tablets were administered with a high-fat meal as compared to fasting, while the extent of absorption was not affected. The rate of hydrochlorothiazide absorption was reduced by 12% when quinapril hydrochloride/hydrochlorothiazide tablets were administered with a high-fat meal, while the extent of absorption was not significantly affected. Therefore, quinapril hydrochloride/hydrochlorothiazide may be administered without regard to food.
Following absorption, quinapril is deesterified to its major active metabolite, quinaprilat (about 38% of oral dose), and to other minor inactive metabolites. Following multiple oral dosing of quinapril, there is an effective accumulation half-life of quinaprilat of approximately 3 hours, and peak plasma quinaprilat concentrations are observed approximately 2 hours postdose. Approximately 97% of either quinapril or quinaprilat circulating in plasma is bound to proteins. Hydrochlorothiazide is not metabolized. Its apparent volume of distribution is 3.6 to 7.8 L/kg, consistent with measured plasma protein binding of 67.9%. The drug also accumulates in red blood cells, so that whole blood levels are 1.6 to 1.8 times those measured in plasma.
Some placental passage occurred when quinapril was administered to pregnant rats. Studies in rats indicate that quinapril and its metabolites do not cross the blood-brain barrier. Hydrochlorothiazide crosses the placenta freely but not the blood-brain barrier.
Quinaprilat is eliminated primarily by renal excretion, up to 96% of an IV dose, and has an elimination half-life in plasma of approximately 2 hours and a prolonged terminal phase with a half-life of 25 hours. Hydrochlorothiazide is excreted unchanged by the kidney. When plasma levels have been followed for at least 24 hours, the plasma half-life has been observed to vary between 4 to 15 hours. At least 61% of the oral dose is eliminated unchanged within 24 hours.
In patients with renal insufficiency, the elimination half-life of quinaprilat increases as creatinine clearance decreases. There is a linear correlation between plasma quinaprilat clearance and creatinine clearance. In patients with end-stage renal disease, chronic hemodialysis or continuous ambulatory peritoneal dialysis have little effect on the elimination of quinapril and quinaprilat. Elimination of quinaprilat is reduced in elderly patients (≥65 years) and in those with heart failure; this reduction is attributable to decrease in renal function (see DOSAGE AND ADMINISTRATION). Quinaprilat concentrations are reduced in patients with alcoholic cirrhosis due to impaired deesterification of quinapril. In a study of patients with impaired renal function (mean creatinine clearance of 19 mL/min), the half-life of hydrochlorothiazide elimination was lengthened to 21 hours.
The pharmacokinetics of quinapril and quinaprilat are linear over a single-dose range of 5 to 80 mg doses and 40 to 160 mg in multiple daily doses.
Pharmacodynamics and Clinical Effects
Single doses of 20 mg of quinapril provide over 80% inhibition of plasma ACE for 24 hours. Inhibition of the pressor response to angiotensin I is shorter-lived, with a 20 mg dose giving 75% inhibition for about 4 hours, 50% inhibition for about 8 hours, and 20% inhibition at 24 hours. With chronic dosing, however, there is substantial inhibition of angiotensin II levels at 24 hours by doses of 20 to 80 mg.
Administration of 10 to 80 mg of quinapril to patients with mild to severe hypertension results in a reduction of sitting and standing blood pressure to about the same extent with minimal effect on heart rate. Symptomatic postural hypotension is infrequent, although it can occur in patients who are salt- and/or volume-depleted (see WARNINGS).
Antihypertensive activity commences within 1 hour with peak effects usually achieved by 2 to 4 hours after dosing. During chronic therapy, most of the blood pressure lowering effect of a given dose is obtained in 1 to 2 weeks. In multiple-dose studies, 10 to 80 mg per day in single or divided doses lowered systolic and diastolic blood pressure throughout the dosing interval, with a trough effect of about 5 to 11/3 to 7 mm Hg. The trough effect represents about 50% of the peak effect.
While the dose-response relationship is relatively flat, doses of 40 to 80 mg were somewhat more effective at trough than 10 to 20 mg, and twice-daily dosing tended to give a somewhat lower trough blood pressure than once-daily dosing with the same total dose. The antihypertensive effect of quinapril continues during long-term therapy, with no evidence of loss of effectiveness.
Hemodynamic assessments in patients with hypertension indicate that blood pressure reduction produced by quinapril is accompanied by a reduction in total peripheral resistance and renal vascular resistance with little or no change in heart rate, cardiac index, renal blood flow, glomerular filtration rate, or filtration fraction.
Therapeutic effects of quinapril appear to be the same for elderly (≥65 years of age) and younger adult patients given the same daily dosages, with no increase in adverse events in elderly patients. In patients with hypertension, quinapril 10 to 40 mg was similar in effectiveness to captopril, enalapril, propranolol, and thiazide diuretics.
After oral administration of hydrochlorothiazide, diuresis begins within 2 hours, peaks in about 4 hours, and lasts about 6 to 12 hours. Use of quinapril with a thiazide diuretic gives blood pressure lowering effect greater than that seen with either agent alone. In clinical trials of quinapril/hydrochlorothiazide using quinapril doses of 2.5 to 40 mg and hydrochlorothiazide doses of 6.25 to 25 mg, the antihypertensive effects were sustained for at least 24 hours, and increased with increasing dose of either component. Although quinapril monotherapy is somewhat less effective in blacks than in non-blacks, the efficacy of combination therapy appears to be independent of race. By blocking the renin-angiotensin-aldosterone axis, administration of quinapril tends to reduce the potassium loss associated with the diuretic. In clinical trials of quinapril hydrochloride/hydrochlorothiazide, the average change in serum potassium was near zero when 2.5 to 40 mg of quinapril was combined with hydrochlorothiazide 6.25 mg, and the average subject who received 10 to 20/12.5 to 25 mg experienced a milder reduction in serum potassium than that experienced by the average subject receiving the same dose of hydrochlorothiazide monotherapy. -
INDICATIONS AND USAGE
Quinapril hydrochloride/hydrochlorothiazide tablets are indicated for the treatment of hypertension. This fixed combination is not indicated for the initial therapy of hypertension (see DOSAGE AND ADMINISTRATION).
In using quinapril hydrochloride/hydrochlorothiazide, consideration should be given to the fact that another angiotensin-converting enzyme inhibitor, captopril, has caused agranulocytosis, particularly in patients with renal impairment or collagen-vascular disease. Available data are insufficient to show that quinapril does not have a similar risk (see WARNINGS: Neutropenia/Agranulocytosis).
Angioedema in Black Patients
Black patients receiving ACE inhibitor monotherapy have been reported to have a higher incidence of angioedema compared to non-blacks. It should also be noted that in controlled clinical trials, ACE inhibitors have an effect on blood pressure that is less in black patients than in non-blacks. -
CONTRAINDICATIONS
Quinapril hydrochloride/hydrochlorothiazidetablets are contraindicated in patients who are hypersensitive to quinapril or hydrochlorothiazide and in patients with a history of angioedema related to previous treatment with an ACE inhibitor.
Because of the hydrochlorothiazide components, this product is contraindicated in patients with anuria or hypersensitivity to other sulfonamide-derived drugs.
Do not co-administer aliskiren with quinapril hydrochloride/hydrochlorothiazide tablets in patients with diabetes. -
WARNINGS
Anaphylactoid and Possibly Related Reactions
Presumably because angiotensin converting inhibitors affect the metabolism of eicosanoids and polypeptides, including endogenous bradykinin, patients receiving ACE inhibitors (including quinapril) may be subject to a variety of adverse reactions, some of them serious.
Head and Neck Angioedema
Angioedema of the face, extremities, lips, tongue, glottis, and larynx has been reported in patients treated with ACE inhibitors and has been seen in 0.1% of patients receiving quinapril. In two similarly sized US postmarketing quinapril trials that, combined, enrolled over 3,000 black patients and over 19,000 non-blacks, angioedema was reported in 0.3% and 0.55% of blacks (in Study 1 and 2, respectively) and 0.39% and 0.17% of non-blacks. Angioedema associated with laryngeal edema can be fatal. If laryngeal stridor or angioedema of the face, tongue, or glottis occurs, treatment with quinapril hydrochloride/hydrochlorothiazide should be discontinued immediately, the patient treated in accordance with accepted medical care, and carefully observed until the swelling disappears. In instances where swelling is confined to the face and lips, the condition generally resolves without treatment; antihistamines may be useful in relieving symptoms. Where there is involvement of the tongue, glottis, or larynx likely to cause airway obstruction, emergency therapy including, but not limited to, subcutaneous epinephrine solution 1:1000 (0.3 to 0.5 mL) should be promptly administered (see PRECAUTIONS and ADVERSE REACTIONS).
Intestinal Angioedema
Intestinal angioedema has been reported in patients treated with ACE inhibitors. These patients presented with abdominal pain (with or without nausea or vomiting); in some cases there was no prior history of facial angioedema and C-1 esterase levels were normal. The angioedema was diagnosed by procedures including abdominal CT scan or ultrasound, or at surgery, and symptoms resolved after stopping the ACE inhibitor. Intestinal angioedema should be included in the differential diagnosis of patients on ACE inhibitors presenting with abdominal pain.
Patients With a History of Angioedema
Patients with a history of angioedema unrelated to ACE inhibitor therapy may be at increased risk of angioedema while receiving an ACE inhibitor (see also CONTRAINDICATIONS).
Anaphylactoid Reactions During Desensitization
Two patients undergoing desensitizing treatment with Hymenoptera venom while receiving ACE inhibitors sustained life-threatening anaphylactoid reactions. In the same patients, these reactions were avoided when ACE inhibitors were temporarily withheld, but they reappeared upon inadvertent challenge.
Anaphylactoid Reactions During Membrane Exposure
Anaphylactoid reactions have been reported in patients dialyzed with high-flux membranes and treated concomitantly with an ACE inhibitor. Anaphylactoid reactions have also been reported in patients undergoing low-density lipoprotein apheresis with dextran sulfate absorption.
Hepatic Failure
Rarely, ACE inhibitors have been associated with a syndrome that starts with cholestatic jaundice and progresses to fulminant hepatic necrosis and (sometimes) death. The mechanism of this syndrome is not understood. Patients receiving ACE inhibitors who develop jaundice or marked elevations of hepatic enzymes should discontinue the ACE inhibitor and receive appropriate medical follow-up.
Hypotension
Quinapril hydrochloride/hydrochlorothiazide can cause symptomatic hypotension, probably not more frequently than either monotherapy. It was reported in 1.2% of 1,571 patients receiving quinapril hydrochloride/hydrochlorothiazide during clinical trials. Like other ACE inhibitors, quinapril has been only rarely associated with hypotension in uncomplicated hypertensive patients.
Symptomatic hypotension sometimes associated with oliguria and/or progressive azotemia, and rarely acute renal failure and/or death, include patients with the following conditions or characteristics: heart failure, hyponatremia, high dose diuretic therapy, recent intensive diuresis or increase in diuretic dose, renal dialysis or severe volume and/or salt depletion of any etiology. Volume and/or salt depletion should be corrected before initiating therapy with quinapril hydrochloride/hydrochlorothiazide.
Quinapril hydrochloride/hydrochlorothiazide should be used cautiously in patients receiving concomitant therapy with other antihypertensives. The thiazide component of quinapril hydrochloride/hydrochlorothiazide may potentiate the action of other antihypertensive drugs, especially ganglionic or peripheral adrenergic-blocking drugs. The antihypertensive effects of the thiazide component may also be enhanced in the postsympathectomy patients.
In patients at risk of excessive hypotension, therapy with quinapril hydrochloride/hydrochlorothiazide should be started under close medical supervision. Such patients should be followed closely for the first 2 weeks of treatment and whenever the dosage of quinapril or diuretic is increased. Similar considerations may apply to patients with ischemic heart or cerebrovascular disease in whom an excessive fall in blood pressure could result in myocardial infarction or cerebrovascular accident.
If excessive hypotension occurs, the patient should be placed in a supine position and, if necessary, treated with intravenous infusion of normal saline. Quinapril hydrochloride/hydrochlorothiazide treatment usually can be continued following restoration of blood pressure and volume. If symptomatic hypotension develops, a dose reduction or discontinuation of quinapril hydrochloride/hydrochlorothiazide may be necessary.
Impaired Renal Function
Quinapril hydrochloride/hydrochlorothiazide should be used with caution in patients with severe renal disease. Thiazides may precipitate azotemia in such patients, and the effects of repeated dosing may be cumulative.
When the renin-angiotensin-aldosterone system is inhibited by quinapril, changes in renal function may be anticipated in susceptible individuals. In patients with severe congestive heart failure, whose renal function may depend on the activity of the renin-angiotensin-aldosterone system, treatment with angiotensin-converting enzyme inhibitors (including quinapril) may be associated with oliguria and/or progressive azotemia and (rarely) with acute renal failure and/or death.
In clinical studies in hypertensive patients with unilateral renal artery stenosis, treatment with ACE inhibitors was associated with increases in blood urea nitrogen and serum creatinine; these increases were reversible upon discontinuation of ACE inhibitor, concomitant diuretic, or both. When such patients are treated with quinapril hydrochloride/hydrochlorothiazide, renal function should be monitored during the first few weeks of therapy.
Some quinapril-treated hypertensive patients with no apparent preexisting renal vascular diseases have developed increases in blood urea nitrogen and serum creatinine, usually minor and transient, especially when quinapril has been given concomitantly with a diuretic. This is more likely to occur in patients with pre-existing renal impairment. Dosage reduction of quinapril hydrochloride/hydrochlorothiazide may be required. Evaluation of the hypertensive patients should also include assessment of the renal function (see DOSAGE AND ADMINISTRATION).Neutropenia/Agranulocytosis
Another ACE inhibitor, captopril, has been shown to cause agranulocytosis and bone marrow depression rarely in patients with uncomplicated hypertension, but more frequently in patients with renal impairment, especially if they also have a collagen vascular disease, such as systemic lupus erythematosus or scleroderma. Agranulocytosis did occur during quinapril treatment in one patient with a history of neutropenia during previous captopril therapy. Available data from clinical trials of quinapril are insufficient to show that, in patients without prior reactions to other ACE inhibitors, quinapril does not cause agranulocytosis at similar rates. As with other ACE inhibitors, periodic monitoring of white blood cell counts in patients with collagen vascular disease and/or renal disease should be considered.
Fetal Toxicity
Pregnancy Category D
Use of drugs that act on the renin-angiotensin system during the second and third trimesters of pregnancy reduces fetal renal function and increases fetal and neonatal morbidity and death. Resulting oligohydramnios can be associated with fetal lung hypoplasia and skeletal deformations. Potential neonatal adverse effects include skull hypoplasia, anuria, hypotension, renal failure, and death. When pregnancy is detected, discontinue quinapril hydrochloride/hydrochlorothiazide as soon as possible. These adverse outcomes are usually associated with use of these drugs in the second and third trimester of pregnancy. Most epidemiologic studies examining fetal abnormalities after exposure to antihypertensive use in the first trimester have not distinguished drugs affecting the renin-angiotensin system from other antihypertensive agents. Appropriate management of maternal hypertension during pregnancy is important to optimize outcomes for both mother and fetus.
In the unusual case that there is no appropriate alternative to therapy with drugs affecting the renin-angiotensin system for a particular patient, apprise the mother of the potential risk to the fetus. Perform serial ultrasound examinations to assess the intra-amniotic environment. If oligohydramnios is observed, discontinue quinapril hydrochloride/hydrochlorothiazide, unless it is considered life-saving for the mother. Fetal testing may be appropriate, based on the week of pregnancy. Patients and physicians should be aware, however, that oligohydramnios may not appear until after the fetus has sustained irreversible injury. Closely observe infants with histories of in utero exposure to quinapril hydrochloride/hydrochlorothiazide for hypotension, oliguria, and hyperkalemia (see PRECAUTIONS, Pediatric Use).
Intrauterine exposure to thiazide diuretics is associated with fetal or neonatal jaundice, thrombocytopenia, and possibly other adverse reactions that occurred in adults.
No teratogenic effects of quinapril were seen in studies of pregnant rats and rabbits. On a mg/kg basis, the doses used were up to 180 times (in rats) and one time (in rabbits) the maximum recommended human dose. No teratogenic effects of quinapril hydrochloride/hydrochlorothiazide were seen in studies of pregnant rats and rabbits. On a mg/kg (quinapril/hydrochlorothiazide) basis, the doses used were up to 188/94 times (in rats) and 0.6/0.3 times (in rabbits) the maximum recommended human dose.
Impaired Hepatic Function
Quinapril hydrochloride/hydrochlorothiazide should be used with caution in patients with impaired hepatic function or progressive liver disease, since minor alterations of fluid and electrolyte balance may precipitate hepatic coma. Also, since the metabolism of quinapril to quinaprilat is normally dependent upon hepatic esterases, patients with impaired liver function could develop markedly elevated plasma levels of quinapril. No normal pharmacokinetic studies have been carried out in hypertensive patients with impaired liver function.
Systemic Lupus Erythematosus
Thiazide diuretics have been reported to cause exacerbation or activation of systemic lupus erythematosus.
Acute Myopia and Secondary Angle-Closure Glaucoma
Hydrochlorothiazide, a sulfonamide, can cause an idiosyncratic reaction, resulting in acute transient myopia and acute angle-closure glaucoma. Symptoms include acute onset of decreased visual acuity or ocular pain and typically occur within hours to weeks of drug initiation. Untreated acute angle-closure glaucoma can lead to permanent vision loss. The primary treatment is to discontinue hydrochlorothiazide as rapidly as possible. Prompt medical or surgical treatments may need to be considered if the intraocular pressure remains uncontrolled. Risk factors for developing acute angle-closure glaucoma may include a history of sulfonamide or penicillin allergy. -
PRECAUTIONS
General
Derangements of Serum Electrolytes
In clinical trials, hyperkalemia (serum potassium ≥5.8 mmol/L) occurred in approximately 2% of patients receiving quinapril. In most cases, elevated serum potassium levels were isolated values which resolved despite continued therapy. Less than 0.1% of patients discontinued therapy due to hyperkalemia. Risk factors for the development of hyperkalemia include renal insufficiency, diabetes mellitus, and the concomitant use of potassium-sparing diuretics, potassium supplements, and/or potassium-containing salt substitutes.
Treatment with thiazide diuretics has been associated with hypokalemia, hyponatremia, and hypochloremic alkalosis. These disturbances have sometimes been manifest as one or more of dryness of mouth, thirst, weakness, lethargy, drowsiness, restlessness, muscle pains or cramps, muscular fatigue, hypotension, oliguria, tachycardia, nausea, and vomiting. Hypokalemia can also sensitize or exaggerate the response of the heart to the toxic effects of digitalis. The risk of hypokalemia is greatest in patients with cirrhosis of the liver, in patients experiencing a brisk diuresis, in patients who are receiving inadequate oral intake of electrolytes, and in patients receiving concomitant therapy with corticosteroids or ACTH.
The opposite effects of quinapril and hydrochlorothiazide on serum potassium will approximately balance each other in many patients, so that no net effect upon serum potassium will be seen. In other patients, one or the other effect may be dominant. Initial and periodic determinations of serum electrolytes to detect possible electrolyte imbalance should be performed at appropriate intervals.
Chloride deficits secondary to thiazide therapy are generally mild and require specific treatment only under extraordinary circumstances (e.g., in liver disease or renal disease). Dilutional hyponatremia may occur in edematous patients in hot weather; appropriate therapy is water restriction rather than administration of salt, except in rare instances when the hyponatremia is life threatening. In actual salt depletion, appropriate replacement is the therapy of choice.
Calcium excretion is decreased by thiazides. In a few patients on prolonged thiazide therapy, pathological changes in the parathyroid gland have been observed, with hypercalcemia and hypophosphatemia. More serious complications of hyperparathyroidism (renal lithiasis, bone resorption, and peptic ulceration) have not been seen.
Thiazides increase the urinary excretion of magnesium, and hypomagnesemia may result.
Other Metabolic Disturbances
Thiazide diuretics tend to reduce glucose tolerance and to raise serum levels of cholesterol, triglycerides, and uric acid. These effects are usually minor, but frank gout or overt diabetes may be precipitated in susceptible patients.
Cough
Presumably due to the inhibition of the degradation of endogenous bradykinin, persistent nonproductive cough has been reported with all ACE inhibitors, resolving after discontinuation of therapy. ACE inhibitor-induced cough should be considered in the differential diagnosis of cough.
Surgery/Anesthesia
In patients undergoing surgery or during anesthesia with agents that produce hypotension, quinapril will block the angiotensin II formation that could otherwise occur secondary to compensatory renin release. Hypotension that occurs as a result of this mechanism can be corrected by volume expansion.Information for Patients
Angioedema
Angioedema, including laryngeal edema, can occur with treatment with ACE inhibitors, especially following the first dose. Patients receiving quinapril hydrochloride/hydrochlorothiazide should be told to report immediately any signs or symptoms suggesting angioedema (swelling of face, eyes, lips, or tongue, or difficulty in breathing) and to take no more drug until after consulting with the prescribing physician.
Pregnancy
Female patients of childbearing age should be told about the consequences of exposure to quinapril hydrochloride/hydrochlorothiazide during pregnancy. Discuss treatment options with women planning to become pregnant. Patients should be asked to report pregnancies to their physicians as soon as possible.
Symptomatic Hypotension
A patient receiving quinapril hydrochloride/hydrochlorothiazide should be cautioned that lightheadedness can occur, especially during the first days of therapy, and that it should be reported to the prescribing physician. The patient should be told that if syncope occurs, quinapril hydrochloride/hydrochlorothiazide should be discontinued until the physician has been consulted.
All patients should be cautioned that inadequate fluid intake, excessive perspiration, diarrhea, or vomiting can lead to an excessive fall in blood pressure because of reduction in fluid volume, with the same consequences of lightheadedness and possible syncope.
Patients planning to undergo major surgery and/ or general or spinal anesthesia should be told to inform their physicians that they are taking an ACE inhibitor.
Hyperkalemia
A patient receiving quinapril hydrochloride/hydrochlorothiazide should be told not to use potassium supplements or salt substitutes containing potassium without consulting the prescribing physician.
Neutropenia
Patients should be told to promptly report any indication of infection (e.g., sore throat, fever) which could be a sign of neutropenia.
NOTE: As with many other drugs, certain advice to patients being treated with quinapril is warranted. This information is intended to aid in the safe and effective use of this medication. It is not a disclosure of all possible adverse or intended effects.Laboratory Tests
The hydrochlorothiazide component of quinapril hydrochloride/hydrochlorothiazide may decrease serum PBI levels without signs of thyroid disturbance.
Therapy with quinapril hydrochloride/hydrochlorothiazide should be interrupted for a few days before carrying out tests of parathyroid function.Drug Interactions
Potassium Supplements and Potassium-Sparing Diuretics
As noted above (“Derangements of Serum Electrolytes”), the net effect of quinapril hydrochloride/hydrochlorothiazide may be to elevate a patient’s serum potassium, to reduce it, or to leave it unchanged. Potassium-sparing diuretics (spironolactone, amiloride, triamterene, and others) or potassium supplements can increase the risk of hyperkalemia. If concomitant use of such agents is indicated, they should be given with caution, and the patient’s serum potassium should be monitored frequently.
Lithium
Increased serum lithium levels and symptoms of lithium toxicity have been reported in patients receiving ACE inhibitors during therapy with lithium. Because renal clearance of lithium is reduced by thiazides, the risk of lithium toxicity is presumably raised further when, as in therapy with quinapril hydrochloride/hydrochlorothiazide, a thiazide diuretic is coadministered with the ACE inhibitor. Quinapril hydrochloride/hydrochlorothiazide and lithium should be coadministered with caution, and frequent monitoring of serum lithium levels is recommended.
Tetracycline and Other Drugs That Interact with Magnesium
Simultaneous administration of tetracycline with quinapril reduced the absorption of tetracycline by approximately 28% to 37%, possibly due to the high magnesium content in quinapril tablets. This interaction should be considered if coprescribing quinapril and tetracycline or other drugs that interact with magnesium.
Gold
Nitritoid reactions (symptoms include facial flushing, nausea, vomiting, and hypotension) have been reported rarely in patients on therapy with injectable gold (sodium aurothiomalate) and concomitant ACE inhibitor therapy.
Other Agents
Drug interaction studies of quinapril and other agents showed:
- Multiple dose therapy with propranolol or cimetidine has no effect on the pharmacokinetics of single doses of quinapril.
- The anticoagulant effect of a single dose of warfarin (measured by prothrombin time) was not significantly changed by quinapril coadministration twice daily.
- Quinapril treatment did not affect the pharmacokinetics of digoxin.
- No pharmacokinetic interaction was observed when single doses of quinapril and hydrochlorothiazide were administered concomitantly.
When administered concurrently, the following drugs may interact with thiazide diuretics.- Alcohol, Barbiturates, or Narcotics—potentiation of orthostatic hypotension may occur.
- Antidiabetic Drugs (oral hypoglycemic agents and insulin)—dosage adjustments of the antidiabetic drug may be required.
- Cholestyramine and Colestipol Resin—absorption of hydrochlorothiazide is impaired in the presence of anionic exchange resins. Single doses of either cholestyramine or colestipol resins bind the hydrochlorothiazide and reduce its absorption from the gastrointestinal tract by up to 85% and 43%, respectively.
- Corticosteroids, ACTH—intensified electrolyte depletion, particularly hypokalemia.
- Pressor Amines (e.g., norepinephrine)—possible decreased response to pressor amines, but not sufficient to preclude their therapeutic use.
- Skeletal Muscle Relaxants, Nondepolarizing (e.g., tubocurarine)—possible increased responsiveness to the muscle relaxant.
- Non-Steroidal Anti-Inflammatory Agents including Selective Cyclooxygenase-2 Inhibitors (COX-2 Inhibitors)—in patients who are elderly, volume-depleted (including those on diuretic therapy), or with compromised renal function, coadministration of NSAIDs, including selective COX-2 inhibitors, with ACE inhibitors, including quinapril, may result in deterioration of renal function, including possible acute renal failure. These effects are usually reversible. Monitor renal function periodically in patients receiving quinapril and NSAID therapy.
The antihypertensive effect of ACE inhibitors, including quinapril may be attenuated by NSAIDs.
Dual Blockade of the Renin-Angiotensin System (RAS)
Dual blockade of the RAS with angiotensin receptor blockers, ACE inhibitors, or aliskiren is associated with increased risks of hypotension, hyperkalemia, and changes in renal function (including acute renal failure) compared to monotherapy. Closely monitor blood pressure, renal function and electrolytes in patients on quinapril hydrochloride/hydrochlorothiazide and other agents that affect the RAS.
Do not co-administer aliskiren with quinapril hydrochloride/hydrochlorothiazide in patients with diabetes. Avoid use of aliskiren with quinapril hydrochloride/hydrochlorothiazide in patients with renal impairment (GFR <60 mL/min).Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity, mutagenicity, and fertility studies have not been conducted in animals with quinapril hydrochloride/hydrochlorothiazide.
Quinapril hydrochloride was not carcinogenic in mice or rats when given in doses up to 75 or 100 mg/kg/day (50 or 60 times the maximum human daily dose, respectively, on a mg/kg basis and 3.8 or 10 times the maximum human daily dose on a mg/m2 basis) for 104 weeks. Female rats given the highest dose level had an increased incidence of mesenteric lymph node hemangiomas and skin/subcutaneous lipomas. Neither quinapril nor quinaprilat were mutagenic in the Ames bacterial assay with or without metabolic activation. Quinapril was also negative in the following genetic toxicology studies: in vitro mammalian cell point mutation, sister chromatid exchange in cultured mammalian cells, micronucleus test with mice, in vitro chromosome aberration with V79 cultured lung cells, and in an in vivo cytogenetic study with rat bone marrow. There were no adverse effects on fertility or reproduction in rats at doses up to 100 mg/kg/day (60 and 10 times the maximum daily human dose when based on mg/kg and mg/m2, respectively).
Under the auspices of the National Toxicology Program, rats and mice received hydrochlorothiazide in their feed for 2 years, at doses up to 600 mg/kg/day in mice and up to 100 mg/kg/day in rats. These studies uncovered no evidence of a carcinogenic potential of hydrochlorothiazide in rats or female mice, but there was “equivocal” evidence of hepatocarcinogenicity in male mice. Hydrochlorothiazide was not genotoxic in in vitro assays using strains TA 98, TA 100, TA 1535, TA 1537, and TA 1538 of Salmonella typhimurium (the Ames test); in the Chinese hamster ovary (CHO) test for chromosomal aberrations; or in vivo assays using mouse germinal cell chromosomes, Chinese hamster bone marrow chromosomes, and the Drosophila sex-linked recessive lethal trait gene. Positive test results were obtained in the in vitro CHO sister chromatid exchange (clastogenicity) test and in the mouse lymphoma cell (mutagenicity) assays, using concentrations of hydrochlorothiazide of 43 to 1300 mcg/mL. Positive test results were also obtained in the Aspergillus nidulans nondisjunction assay, using an unspecified concentration of hydrochlorothiazide.
Hydrochlorothiazide had no adverse effects on the fertility of mice and rats of either sex in studies wherein these species were exposed, via their diets, to doses of up to 100 and 4 mg/kg/day, respectively, prior to mating and throughout gestation.Nursing Mothers
Because quinapril and hydrochlorothiazide are secreted in human milk, caution should be exercised when quinapril hydrochloride/hydrochlorothiazide is administered to a nursing woman.
Because of the potential for serious adverse reactions in nursing infants from hydrochlorothiazide and the unknown effects of quinapril in infants, a decision should be made whether to discontinue nursing or to discontinue quinapril hydrochloride/ hydrochlorothiazide, taking into account the importance of the drug to the mother.Geriatric Use
Clinical studies of quinapril hydrochloride/hydrochlorothiazide did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
Pediatric Use
Neonates with a history of in utero exposure to quinapril hydrochloride/hydrochlorothiazide
If oliguria or hypotension occurs, direct attention toward support of blood pressure and renal perfusion. Exchange transfusions or dialysis may be required as a means of reversing hypotension and/or substituting for disordered renal function. Removal of quinapril, which crosses the placenta, from the neonatal circulation is not significantly accelerated by these means.
Safety and effectiveness of quinapril hydrochloride/hydrochlorothiazidein children have not been established. -
ADVERSE REACTIONS
Quinapril hydrochloride/hydrochlorothiazidehas been evaluated for safety in 1571 patients in controlled and uncontrolled studies. Of these, 498 were given quinapril plus hydrochlorothiazide for at least 1 year, with 153 patients extending combination therapy for over 2 years. In clinical trials with quinapril hydrochloride/hydrochlorothiazide, no adverse experience specific to the combination has been observed. Adverse experiences that have occurred have been limited to those that have been previously reported with quinapril or hydrochlorothiazide.
Adverse experiences were usually mild and transient, and there was no relationship between side effects and age, sex, race, or duration of therapy. Discontinuation of therapy because of adverse effects was required in 2.1% in patients in controlled studies. The most common reasons for discontinuation of therapy with quinapril hydrochloride/hydrochlorothiazidewere cough (1%; see PRECAUTIONS) and headache (0.7%).
Adverse experiences probably or possibly related to therapy or of unknown relationship to therapy occurring in 1% or more of the 943 patients treated with quinapril plus hydrochlorothiazide in controlled trials are shown below.
Percent of Patients in Controlled Trials Quinapril/HCTZ
N = 943Placebo
N = 100Headache 6.7 30 Dizziness 4.8 4 Coughing 3.2 2 Fatigue 2.9 3 Myalgia 2.4 5 Viral Infection 1.9 4 Rhinitis 2 3 Nausea and/or Vomiting 1.8 6 Abdominal Pain 1.7 4 Back Pain 1.5 2 Diarrhea 1.4 1 Upper Respiratory Infection 1.3 4 Insomnia 1.2 2 Somnolence 1.2 0 Bronchitis 1.2 1 Dyspepsia 1.2 2 Asthenia 1.1 1 Pharyngitis 1.1 2 Vasodilatation 1 1 Vertigo 1 2 Chest Pain 1 2
Clinical adverse experiences probably, possibly, or definitely related or of uncertain relationship to therapy occurring in ≥0.5% to <1% (except as noted) of the patients treated with quinapril/HCTZ in controlled and uncontrolled trials (N=1571) and less frequent, clinically significant events seen in clinical trials or postmarketing experience (the rarer events are in italics) include (listed by body system):BODY AS A WHOLE: Asthenia, Malaise CARDIOVASCULAR: Palpitation, Tachycardia, Heart Failure, Hyperkalemia, Myocardial Infarction, Cerebrovascular Accident, Hypertensive Crisis, Angina Pectoris, Orthostatic Hypotension, Cardiac Rhythm Disturbance GASTROINTESTINAL: Mouth or Throat Dry, Gastrointestinal Hemorrhage, Pancreatitis, Abnormal Liver Function Tests NERVOUS/PSYCHIATRIC: Nervousness, Vertigo, Paresthesia RESPIRATORY: Sinusitis, Dyspnea INTEGUMENTARY: Pruritus, Sweating Increased, Erythema Multiforme, Exfoliative Dermatitis, Photosensitivity Reaction, Alopecia, Pemphigus UROGENITAL SYSTEM: OTHER: Acute Renal Failure, Impotence
Agranulocytosis, Thrombocytopenia, ArthralgiaAngioedema: Angioedema has been reported in 0.1% of patients receiving quinapril (0.1%) (see WARNINGS).
Postmarketing Experience
The following serious nonfatal adverse events, regardless of their relationship to quinapril and HCTZ combination tablets, have been reported during extensive postmarketing experience:
BODY AS A WHOLE: Shock, accidental injury, neoplasm, cellulitis, ascites, generalized edema, hernia and anaphylactoid reaction.
CARDIOVASCULAR SYSTEM: Bradycardia, cor pulmonale, vasculitis, and deep thrombosis.
DIGESTIVE SYSTEM: Gastrointestinal carcinoma, cholestatic jaundice, hepatitis, esophagitis, vomiting, and diarrhea.
HEMIC SYSTEM: Anemia.
METABOLIC AND NUTRITIONAL DISORDERS: Weight loss.
MUSCULOSKELETAL SYSTEM: Myopathy, myositis, and arthritis.
NERVOUS SYSTEM: Paralysis, hemiplegia, speech disorder, abnormal gait, meningism, and amnesia.
RESPIRATORY SYSTEM: Pneumonia, asthma, respiratory infiltration, and lung disorder.
SKIN AND APPENDAGES: Urticaria, macropapular rash, and petechiases.
SPECIAL SENSES: Abnormal vision.
UROGENITAL SYSTEM: Kidney function abnormal, albuminuria, pyuria, hematuria, and nephrosis.
Quinapril monotherapy has been evaluated for safety in 4960 patients. In clinical trials adverse events which occurred with quinapril were also seen with quinapril hydrochloride/hydrochlorothiazide. In addition, the following were reported for quinapril at an incidence >0.5%: depression, back pain, constipation, syncope, and amblyopia.
Hydrochlorothiazide has been extensively prescribed for many years, but there has not been enough systematic collection of data to support an estimate of the frequency of the observed adverse reactions. Within organ-system groups, the reported reactions are listed here in decreasing order of severity, without regard to frequency.BODY AS A WHOLE: Weakness. CARDIOVASCULAR: Orthostatic hypotension (may be potentiated by alcohol, barbiturates, or narcotics). DIGESTIVE: Pancreatitis, jaundice (intrahepatic cholestatic), sialadenitis, vomiting, diarrhea, cramping, nausea, gastric irritation, constipation, and anorexia. NEUROLOGIC: Vertigo, lightheadedness, transient blurred vision, headache, paresthesia, xanthopsia, weakness, and restlessness. MUSCULOSKELETAL: Muscle spasm. HEMATOLOGIC: Aplastic anemia, agranulocytosis, leukopenia, thrombocytopenia, and hemolytic anemia. RENAL: Renal failure, renal dysfunction, interstitial nephritis (see WARNINGS). METABOLIC: Hyperglycemia, glycosuria, and hyperuricemia. HYPERSENSITIVITY: Necrotizing angiitis, Stevens-Johnson syndrome, respiratory distress (including pneumonitis and pulmonary edema), purpura, urticaria, rash, and photosensitivity.
Clinical Laboratory Test Findings
Serum Electrolytes: See PRECAUTIONS.
Creatinine, Blood Urea Nitrogen
Increases (>1.25 times the upper limit of normal) in serum creatinine and blood urea nitrogen were observed in 3% and 4%, respectively, of patients treated with quinapril hydrochloride/hydrochlorothiazide. Most increases were minor and reversible, which can occur in patients with essential hypertension but most frequently in patients with renal artery stenosis (see PRECAUTIONS).
PBI and Tests of Parathyroid Function: See PRECAUTIONS.
Hematology: See WARNINGS.
Other (causal relationships unknown)
Other clinically important changes in standard laboratory tests were rarely associated with quinapril hydrochloride/hydrochlorothiazide administration. Elevations in uric acid, glucose, magnesium, cholesterol, triglyceride, and calcium (see PRECAUTIONS) have been reported. -
OVERDOSAGE
No specific information is available on the treatment of overdosage with quinapril hydrochloride/hydrochlorothiazide or quinapril monotherapy; treatment should be symptomatic and supportive. Therapy with quinapril hydrochloride/hydrochlorothiazide should be discontinued, and the patient should be observed. Dehydration, electrolyte imbalance, and hypotension should be treated by established procedures.
The oral median lethal dose of quinapril/hydrochlorothiazide in combination ranges from 1063/664 to 4640/2896 mg/kg in mice and rats. Doses of 1440 to 4280 mg/kg of quinapril cause significant lethality in mice and rats. In single-dose studies of hydrochlorothiazide, most rats survived doses up to 2.75 g/kg.
Data from human overdoses of ACE inhibitors are scanty; the most likely manifestation of human quinapril overdosage is hypotension. In human hydrochlorothiazide overdose, the most common signs and symptoms observed have been those of dehydration and electrolyte depletion (hypokalemia, hypochloremia, hyponatremia). If digitalis has also been administered, hypokalemia may accentuate cardiac arrhythmias.
Laboratory determinations of serum levels of quinapril and its metabolites are not widely available, and such determinations have, in any event, no established role in the management of quinapril overdose.
No data are available to suggest physiological maneuvers (e.g., maneuvers to change the pH of the urine) that might accelerate elimination of quinapril and its metabolites. Hemodialysis and peritoneal dialysis have little effect on the elimination of quinapril and quinaprilat.
Angiotensin II could presumably serve as a specific antagonist-antidote in the setting of quinapril overdose, but angiotensin II is essentially unavailable outside of scattered research facilities. Because the hypotensive effect of quinapril is achieved through vasodilation and effective hypovolemia, it is reasonable to treat quinapril overdose by infusion of normal saline solution. -
DOSAGE AND ADMINISTRATION
As individual monotherapy, quinapril is an effective treatment of hypertension in once-daily doses of 10 to 80 mg and hydrochlorothiazide is effective in doses of 12.5 to 50 mg. In clinical trials of quinapril/hydrochlorothiazide combination therapy using quinapril doses of 2.5 to 40 mg and hydrochlorothiazide doses of 6.25 to 25 mg, the antihypertensive effects increased with increasing dose of either component.
The side effects (see WARNINGS) of quinapril are generally rare and apparently independent of dose; those of hydrochlorothiazide are a mixture of dose-dependent phenomena (primarily hypokalemia) and dose-independent phenomena (e.g., pancreatitis), the former much more common than the latter. Therapy with any combination of quinapril and hydrochlorothiazide will be associated with both sets of dose-independent side effects, but regimens that combine low doses of hydrochlorothiazide with quinapril produce minimal effects on serum potassium. In clinical trials of quinapril/hydrochlorothiazide, the average change in serum potassium was near zero in subjects who received HCTZ 6.25 mg in the combination, and the average subject who received 10 to 40/12.5 to 25 mg experienced a milder reduction in serum potassium than that experienced by the average subject receiving the same dose of hydrochlorothiazide monotherapy.
To minimize dose-independent side effects, it is usually appropriate to begin combination therapy only after a patient has failed to achieve the desired effect with monotherapy.
Therapy Guided by Clinical Effect
Patients whose blood pressures are not adequately controlled with quinapril monotherapy may instead be given quinapril/hydrochlorothiazide 10/12.5 or 20/12.5. Further increases of either or both components could depend on clinical response. The hydrochlorothiazide dose should generally not be increased until 2 to 3 weeks have elapsed. Patients whose blood pressures are adequately controlled with 25 mg of daily hydrochlorothiazide, but who experience significant potassium loss with this regimen, may achieve blood pressure control with less electrolyte disturbance if they are switched to quinapril/hydrochlorothiazide 10/12.5 or 20/12.5.
Replacement Therapy
For convenience, patients who are adequately treated with 20 mg of quinapril and 25 mg of hydrochlorothiazide and experience no significant electrolyte disturbances may instead wish to receive quinapril/hydrochlorothiazide 20/25.
Use in Renal Impairment
Regimens of therapy with quinapril hydrochloride/hydrochlorothiazide tablets need not take account of renal function as long as the patient’s creatinine clearance is >30 mL/min/ 1.73 m2 (serum creatinine roughly ≤3 mg/dL or 265 µmol/L). In patients with more severe renal impairment, loop diuretics are preferred to thiazides. Therefore, quinapril hydrochloride/hydrochlorothiazide tablets are not recommended for use in these patients. -
HOW SUPPLIED
Quinapril Hydrochloride/Hydrochlorothiazide 10 mg/12.5 mg* Tablets are Pink colored, scored, oval shaped, biconvex, film-coated tablets debossed with ‘D’ on scored side and ‘18’ on other side.
*Quinapril hydrochloride equivalent to 10 mg of quinapril.
Quinapril Hydrochloride/Hydrochlorothiazide 20 mg/12.5 mg* Tablets are Pink colored, scored, round shaped, biconvex, film-coated tablets debossed with ‘D’ on scored side and ‘19’ on other side.
NDC: 35356-998-30 Bottles of 30NDC: 35356-998-60 Bottles of 60
NDC: 35356-998-90 Bottles of 90
*Quinapril hydrochloride equivalent to 20 mg of quinapril.
Quinapril Hydrochloride/Hydrochlorothiazide 20 mg/25 mg* Tablets are Pink colored, round shaped, biconvex, film-coated tablets debossed with ‘D’ on one side and ‘20’ on other side.
*Quinapril hydrochloride equivalent to 20 mg of quinapril.
Store at 20° to 25°C (68° to 77°F); excursions permitted to 15° to 30°C (59° to 86°F) [see USP Controlled Room Temperature]. Protect from light.
Manufactured for:
Aurobindo Pharma USA, Inc.
2400 Route 130 North
Dayton, NJ 08810
Manufactured by:
Aurobindo Pharma Limited
Hyderabad–500 072, India
Revised: 10/2012 - Image of Label
-
INGREDIENTS AND APPEARANCE
QUINAPRIL HYDROCHLORIDE/HYDROCHLOROTHIAZIDE
quinapril hydrochloride/hydrochlorothiazide tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 35356-998(NDC:65862-162) Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength QUINAPRIL HYDROCHLORIDE (UNII: 33067B3N2M) (QUINAPRILAT - UNII:34SSX5LDE5) QUINAPRIL 20 mg HYDROCHLOROTHIAZIDE (UNII: 0J48LPH2TH) (HYDROCHLOROTHIAZIDE - UNII:0J48LPH2TH) HYDROCHLOROTHIAZIDE 12.5 mg Inactive Ingredients Ingredient Name Strength LACTOSE MONOHYDRATE (UNII: EWQ57Q8I5X) MAGNESIUM CARBONATE (UNII: 0E53J927NA) CROSPOVIDONE (UNII: 2S7830E561) POVIDONE K30 (UNII: U725QWY32X) MAGNESIUM STEARATE (UNII: 70097M6I30) HYPROMELLOSE 2910 (3 MPA.S) (UNII: 0VUT3PMY82) HYPROMELLOSE 2910 (50 MPA.S) (UNII: 1IVH67816N) HYDROXYPROPYL CELLULOSE (UNII: RFW2ET671P) POLYETHYLENE GLYCOL 400 (UNII: B697894SGQ) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) FERRIC OXIDE RED (UNII: 1K09F3G675) FERRIC OXIDE YELLOW (UNII: EX438O2MRT) Product Characteristics Color PINK Score 2 pieces Shape ROUND (Biconvex) Size 9mm Flavor Imprint Code D;19 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 35356-998-30 30 in 1 BOTTLE; Type 0: Not a Combination Product 08/24/2007 2 NDC: 35356-998-60 60 in 1 BOTTLE; Type 0: Not a Combination Product 08/24/2007 3 NDC: 35356-998-90 90 in 1 BOTTLE; Type 0: Not a Combination Product 08/24/2007 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA078450 08/24/2007 Labeler - Lake Erie Medical DBA Quality Care Products LLC (831276758) Establishment Name Address ID/FEI Business Operations Lake Erie Medical DBA Quality Care Products LLC 831276758 repack(35356-998)
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.