VETMEDIN SOLUTION- pimobendan solution
Vetmedin Solution by
Drug Labeling and Warnings
Vetmedin Solution by is a Animal medication manufactured, distributed, or labeled by Boehringer Ingelheim Animal Health USA Inc.. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
- SPL UNCLASSIFIED SECTION
- Caution:
-
Description:
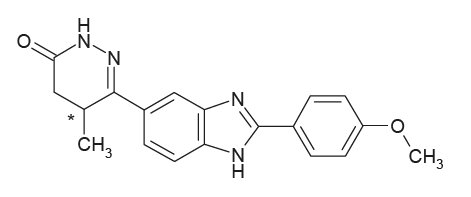
VETMEDIN® Solution (pimobendan oral solution) is a clear to yellow to slightly green to slightly brown aqueous solution containing 1.5 mg/mL pimobendan. Pimobendan, a benzimidazole-pyridazinone derivative, is a non-sympathomimetic, non-glycoside inotropic drug with vasodilatative properties. The chemical name of pimobendan is 4,5-dihydro-6-[2-(4-methoxyphenyl)-1H-benzimidazole-5-yl]-5-methyl-,(±)-3(2H)-pyridazinone.
The structural formula of pimobendan is:
-
Indications:
VETMEDIN Solution (pimobendan oral solution) is indicated for the delay of onset of congestive heart failure in dogs with Stage B2 preclinical myxomatous mitral valve disease. Stage B2 preclinical myxomatous mitral valve disease (MMVD) refers to dogs with asymptomatic MMVD that have a moderate or loud mitral murmur due to mitral regurgitation and cardiomegaly.
VETMEDIN Solution (pimobendan oral solution) is indicated for the management of the signs of mild, moderate, or severe congestive heart failure (CHF) in dogs due to clinical MMVD or dilated cardiomyopathy (DCM). VETMEDIN Solution is indicated for use with concurrent therapy for congestive heart failure (e.g., furosemide, etc.) as appropriate on a case-by-case basis.
-
Dosage and Administration:
VETMEDIN Solution should be administered orally at a total daily dose of 0.23 mg/lb (0.5 mg/kg) body weight. The total daily dose should be divided into 2 equal portions administered approximately 12 hours apart (i.e., morning and evening).
The syringe is calibrated to deliver the appropriate morning or evening dose when drawn to the dog’s nearest weight in pounds.
VETMEDIN Solution should be administered directly into the mouth. Do not mix into food.
VETMEDIN Solution includes an amber glass bottle sealed with a white cap (A), an orange cap with integrated plastic plug (B), and an orange dosing syringe (C).
Do not shake the bottle before or during use to avoid foaming.
VETMEDIN Solution should be administered using the orange dosing syringe provided in the package. At the time of first use, the white cap should be removed and discarded. Once the orange cap has been screwed onto the bottle and the integrated plastic plug is in place, the dosing syringe fits onto plug. The dosing syringe has 1 pound incremental marks. Each dose should be rounded to the nearest 1 pound increment (e.g., a dose for a dog 5.5 lb or greater should be rounded up to 6 lb).
An in-use video demonstration can be found using the URL https://go.boehringer.com/q7lKE or the QR code below.
Close the bottle tightly using the orange cap. After administration, clean the outside of the syringe by wiping with a clean, dry cloth or tissue after each use. If the syringe clogs, rinse without removing the plunger by using water and wiping the outside of the syringe dry with a clean cloth or tissue.
-
Contraindications:
Do not administer VETMEDIN Solution in cases of hypertrophic cardiomyopathy, aortic stenosis, or any other clinical condition where an augmentation of cardiac output is inappropriate for functional or anatomical reasons.
Do not administer VETMEDIN Solution to dogs with Stage A or B1 preclinical MMVD due to the risk of cardiac pathology associated with exaggerated hemodynamic responses to VETMEDIN Solution.
-
Warnings:
User Safety Warnings: Not for use in humans. Keep this and all medications out of reach of children. Consult a physician in case of accidental ingestion by humans.
Wash hands after use. This product may cause eye irritation. Avoid contact with eyes. In case of contact, flush affected eye(s) immediately and thoroughly with water. If wearing contact lenses, flush the eyes first with water and then remove the lens(es) and continue to flush thoroughly with water. If eye irritation continues, seek medical advice and provide this product information to the physician.
Exposure to product may induce a local or systemic allergic reaction in sensitized individuals.
Animal Safety Warnings: Only for use in dogs with Stage B2 preclinical MMVD or clinical evidence of CHF. At 3 and 5 times the recommended dosage, administered over a 6-month period of time, pimobendan caused an exaggerated hemodynamic response in the normal dog heart, which was associated with cardiac pathology (See Target Animal Safety).
Keep VETMEDIN Solution in a secure location out of reach of dogs, cats, and other animals to prevent accidental ingestion or overdose.
-
Precautions:
The safety of VETMEDIN Solution has not been established in dogs with asymptomatic heart disease caused by etiologies other than MMVD or in CHF caused by etiologies other than MMVD or DCM. The safety of VETMEDIN Solution has not been evaluated in dogs younger than 6 months of age, dogs with congenital heart defects, dogs with diabetes mellitus or other serious metabolic diseases, dogs used for breeding, or pregnant or lactating bitches.
For Stage B2 preclinical MMVD, use only in dogs that have a moderate or loud mitral murmur due to mitral regurgitation and cardiomegaly. A diagnosis of MMVD should be made by means of a comprehensive physical and cardiac examination which should include radiography and echocardiography. Stage B2 cardiomegaly1 is diagnosed based on meeting all three of the following criteria:
- Radiographic vertebral heart score (VHS) >10.5, and
- Echocardiographic left atrium/aorta ratio (LA/Ao ratio) ≥1.6, and
- Echocardiographic left ventricular internal diastolic diameter normalized to body weight (LVIDDN) ≥1.7.
Echocardiographic examination is recommended in all cases to diagnose MMVD and confirm cardiomegaly. If therapy is initiated prior to the development of cardiomegaly, treated dogs are at risk for cardiac pathology associated with exaggerated hemodynamic responses to VETMEDIN Solution.
If only radiographic examination is possible, cardiomegaly may be diagnosed in cases where the VHS ≥11.5 and the vertebral left atrial size (VLAS) ≥3.01,2. If radiographic cardiomegaly does not meet both of these criteria, an echocardiogram should be performed prior to the initiation of therapy with VETMEDIN Solution.
VETMEDIN Solution has not been evaluated in Stage B2 preclinical MMVD dogs receiving concomitant heart medications.
Dogs in Stage B2 preclinical MMVD may eventually progress to clinical stages of MMVD (Stages C and D). A plan to recheck dogs at regular intervals is recommended as temporal changes in radiographic findings and clinical variables may be useful in diagnosing progression to CHF. In addition, it is recommended that dog owners be educated to recognize clinical signs associated with CHF (e.g., coughing or tachypnea) so they may promptly present the dog for an examination.
-
Adverse Reactions:
The safety and effectiveness of VETMEDIN Solution was established by demonstrating bioequivalence with VETMEDIN Chewable Tablets. (See Clinical Pharmacology).
Pre-Approval Experience in Stage B2 Preclinical MMVD: Clinical findings/adverse reactions were recorded in two multi-site field studies of dogs diagnosed with Stage B2 preclinical MMVD.
Study 1: In the first study, 363 dogs with Stage B2 preclinical MMVD received at least one dose of VETMEDIN (n=182) or the vehicle control chewable tablets (n=181). Dogs were followed until the development of left-sided CHF, cardiac-related death or euthanasia, or until the end of the study (up to 3 years). Adverse reactions were seen in both treatment groups with many findings associated with MMVD and comorbidities consistent with the age of the enrolled dogs.
Cough was the most frequently reported adverse reaction in this study. This clinical finding is commonly reported in cases of MMVD, and the incidence was similar between treatment groups. Gastrointestinal upset (vomiting and diarrhea) was the most frequently reported non-cardiac adverse reaction associated with VETMEDIN.
Mortality rate, regardless of reason, prior to CHF was similar between the VETMEDIN and the control groups.
Table 1: Cardiac Related Adverse Reactionsa (Study 1)
Adverse Reaction
VETMEDIN Group (n=182)
Vehicle Control (n=181)
Cough
39 (21.4%)
42 (23.2%)
Lethargy
16 (8.8%)
13 (7.2%)
Inappetence
14 (7.7%)
13 (7.2%)
Tachypnea/panting
13 (7.1%)
12 (6.6%)
Arrhythmia
7 (3.9%)
3 (1.7%)
Collapseb
4 (2.2%)
2 (1.1%)
Dyspnea
4 (2.2%)
3 (1.7%)
Syncopeb
0 (0.0%)
5 (2.8%)
Table 2: Non-cardiac Adverse Reactions (Study 1)
Adverse Reaction
VETMEDIN Group (n=182)
Vehicle Control (n=181)
Musculoskeletal pain
24 (13.2%)
12 (6.6%)
Diarrhea
21 (11.5%)
16 (8.8%)
Vomiting
18 (9.9%)
24 (13.3%)
Seizureb
7 (3.8%)
2 (1.1%)
Pruritus
7 (3.9%)
3 (1.7%)
Lameness
7 (3.9%)
3 (1.7%)
Urinary tract infection
7 (3.9%)
2 (1.1%)
Restlessness
4 (2.2%)
0 (0%)
a These adverse reactions are commonly associated with cardiac disease, although some cases may have non-cardiac causes.
b Most cases of collapse, syncope, and seizure were reported by the owner. These clinical signs can be difficult to differentiate.
Study 2: In the second study, 161 dogs with Stage B2 preclinical MMVD were treated with at least one dose of VETMEDIN. All enrolled dogs were treated with VETMEDIN. The dogs were followed for up to 1 year (365 days), or until the development of left-sided CHF, malignant arrhythmias, syncope, advanced coughing, increased resting respiration rate (RRR), or death.
Adverse reactions identified in this study were similar to the first study with many findings associated with MMVD and age-related comorbidities. Cough was the most frequently reported cardiac related adverse reaction and gastrointestinal upset (vomiting and diarrhea) was the most frequently reported non-cardiac adverse reaction associated with VETMEDIN.
Chordae tendineae rupture occurred in 3 dogs receiving VETMEDIN in Study 2, resulting in the euthanasia of one dog. In Study 1, chordae tendineae rupture was observed in 3 control dogs and in 0 VETMEDIN-treated dogs.
In Study 2, 14 VETMEDIN-treated dogs died or were euthanized by Day 365; 8 for cardiac related reasons and 6 for reasons unrelated to MMVD or treatment with VETMEDIN.
Table 3: Cardiac Related Adverse Reactionsa (Study 2)
Adverse Reaction
VETMEDIN (n=161)
Cough
48 (29.8%)
Inappetence
30 (18.6%)
Lethargy
25 (15.5%)
Tachypnea/panting
17 (10.6%)
Arrhythmia
13 (8.1%)
Dyspnea
6 (3.7%)
Syncopeb
5 (3.1%)
Collapseb
2 (1.2%)
Table 4: Non-cardiac Adverse Reactions (Study 2)
Adverse Reaction
VETMEDIN (n=161)
Vomiting
59 (36.6%)
Diarrhea
53 (32.9%)
Musculoskeletal pain
12 (7.5%)
Lameness
10 (6.2%)
Dermal mass
9 (5.6%)
Polydipsia
9 (5.6%)
Pruritus
7 (4.3%)
Polyuria
6 (3.7%)
Urinary tract infection
6 (3.7%)
Restlessness
4 (2.5%)
Seizureb
3 (1.9%)
a These adverse reactions are commonly associated with cardiac disease, although some cases may have non-cardiac causes.
b Most cases of collapse, syncope, and seizure were reported by the owner. These clinical signs can be difficult to differentiate.
Pre-Approval Experience in Clinical MMVD or DCM: In a separate study, clinical findings/adverse reactions were recorded in a 56-day field study of dogs with CHF due to MMVD (256 dogs) or DCM (99 dogs). Dogs were treated with either VETMEDIN (175 dogs) or the active control enalapril maleate (180 dogs). Dogs in both treatment groups received additional background cardiac therapy (See Effectiveness for details and the difference in digoxin administration between treatment groups).
The VETMEDIN group had the following incidence (percent of dogs with at least one occurrence) of common adverse reactions/new clinical findings (not present in a dog prior to beginning study treatments). Incidence was similar in the active control group. The incidence of renal failure was higher in the active control group (4%) compared to the VETMEDIN group (1%).
Table 5: Adverse Reactions (Clinical MMVD or DCM)
Adverse Reaction
VETMEDIN (n=175)
Poor appetite
67 (38%)
Lethargy
58 (33%)
Diarrhea
53 (30%)
Dyspnea
51 (29%)
Azotemia
25 (14%)
Weakness/ataxia
23 (13%)
Pleural effusion
18 (10%)
Syncope
16 (9%)
Cough
12 (7%)
Sudden death
11 (6%)
Ascites
11 (6%)
Heart Murmur
5 (3%)
Adverse reactions/new clinical findings were seen in both treatment groups and were potentially related to CHF, the therapy of CHF, or both. The following adverse reactions/new clinical findings are listed according to body system and are not in order of prevalence:
CHF death, sudden death, chordae tendineae rupture, left atrial tear, arrhythmias overall, tachycardia, syncope, weak pulses, irregular pulses, increased pulmonary edema, dyspnea, increased respiratory rate, coughing, gagging, pleural effusion, ascites, hepatic congestion, decreased appetite, vomiting, diarrhea, melena, weight loss, lethargy, depression, weakness, collapse, shaking, trembling, ataxia, seizures, restlessness, agitation, pruritus, increased water consumption, increased urination, urinary accidents, azotemia, dehydration, abnormal serum electrolyte, protein, and glucose values, mild increases in serum hepatic enzyme levels, and mildly decreased platelet counts.
See Table 6 for mortality due to CHF (including euthanasia, natural death, and sudden death) and for the development of new arrhythmias (not present in a dog prior to beginning study treatments) by treatment group and type of heart disease (MMVD or DCM) in the 56-day field study.
Table 6: CHF Death and New Arrhythmias in the 56-Day Field Study
VETMEDIN Group
Active Control Group
Dogs that died due to CHF
14.3%
n = 175
14.4%
n = 180
9 of 126 dogs with MMVD
16 of 130 dogs with MMVD
16 of 49 dogs with DCM
10 of 50 dogs with DCM
Dogs that developed new arrhythmiasa
39.4%
n = 175
45.0%
n = 180
45 of 126 dogs with MMVD
59 of 130 dogs with MMVD
24 of 49 dogs with DCM
22 of 50 dogs with DCM
a New arrhythmias included supraventricular premature beats and tachycardia, atrial fibrillation, atrioventricular block, sinus bradycardia, ventricular premature beats and tachycardia, and bundle branch block.
Following the 56-day masked field study, 137 dogs in the VETMEDIN group were allowed to continue on VETMEDIN in an open-label extended-use study without restrictions on concurrent therapy. The adverse reactions/new clinical findings in the extended-use study were consistent with those reported in the 56-day study, with the following exception: One dog in the extended-use study developed acute cholestatic liver failure after 140 days on VETMEDIN and furosemide.
Post-Approval Experience (2023):
The following adverse events are based on post-approval adverse drug experience reporting for VETMEDIN. Not all adverse events are reported to FDA/CVM. It is not always possible to reliably estimate the adverse event frequency or establish a causal relationship to product exposure using these data.
The following adverse events reported in dogs, are listed in decreasing order of reporting frequency:
Diarrhea, lethargy, anorexia, emesis, cough, tachycardia, ataxia, dyspnea, convulsion, elevated liver enzymes (ALT, ALP), increased BUN and/or creatinine, tremors, hyperactivity, pruritus, syncope, allergic reactions (including allergic edema/facial edema, erythema, and hives), hypotension, hypertension, coagulation abnormalities (including thrombocytopenia, hemorrhage and petechia), and hyperglycemia (with or without diabetes mellitus).
Death has been reported in some cases.
-
Contact Information:
To report suspected adverse reactions, to obtain a Safety Data Sheet (SDS), or for technical assistance, contact Boehringer Ingelheim Animal Health USA Inc. at 1-888-637-4251. For additional information about adverse drug experience reporting for animal drugs, contact the FDA at 1-888-FDA-VETS or at www.fda.gov/reportanimalae.
-
Clinical Pharmacology:
Pimobendan is oxidatively demethylated to a pharmacologically active metabolite which is then conjugated with sulfate or glucuronic acid and excreted mainly via feces. The mean extent of protein binding of pimobendan and the active metabolite in dog plasma is >90%. Following a single oral administration of 0.25 mg/kg VETMEDIN tablets the maximal mean (± 1 SD) plasma concentrations (Cmax) of pimobendan and the active metabolite were 3.09 (0.76) ng/mL and 3.66 (1.21) ng/mL, respectively. Individual dog Cmax values for pimobendan and the active metabolite were observed 1 to 4 hours post-dose (mean: 2 and 3 hours, respectively). The total body clearance of pimobendan was approximately 90 mL/min/kg, and the terminal elimination half-lives of pimobendan and the active metabolite were approximately 0.5 hours and 2 hours, respectively.
Plasma levels of pimobendan and active metabolite were below quantifiable levels by 4 and 8 hours after oral administration, respectively. The steady-state volume of distribution of pimobendan is 2.6 L/kg indicating that the drug is readily distributed into tissues. Food decreased the bioavailability of an aqueous solution of pimobendan, but the effect of food on the absorption of pimobendan from VETMEDIN tablets is unknown.
In normal dogs instrumented with left ventricular (LV) pressure transducers, pimobendan increased LV dP/dtmax (a measure of contractility of the heart) in a dose dependent manner between 0.1 and 0.5 mg/kg orally. The effect was still present 8 hours after dosing. There was a delay between peak blood levels of pimobendan and active metabolite and the maximum physiologic response (peak LV dP/dtmax). Blood levels of pimobendan and active metabolite began to drop before maximum contractility was seen. Repeated oral administration of pimobendan did not result in evidence of tachyphylaxis (decreased positive inotropic effect) or drug accumulation (increased positive inotropic effect). Laboratory studies indicate that the positive inotropic effect of pimobendan may be attenuated by the concurrent use of a β-adrenergic blocker or a calcium channel blocker.
-
Effectiveness:
The effectiveness of VETMEDIN Solution was established by demonstrating bioequivalence with VETMEDIN Chewable Tablets. (See Clinical Pharmacology).
Stage B2 Preclinical MMVD: Effectiveness of VETMEDIN for the delay of onset of CHF in dogs diagnosed with Stage B2 preclinical MMVD is based on results from two multi-site field studies.
Study 1: The first study was a multicenter, vehicle-controlled field study. This study demonstrated a significant delay in the onset of CHF in dogs with cardiomegaly and heart murmur secondary to Stage B2 MMVD when treated with VETMEDIN at the targeted total daily dose of 0.23 mg/lb (0.5 mg/kg) divided into two administrations approximately 12 hours apart.
A total of 363 dogs across various breeds were randomized to treatment. The resulting population evaluated for effectiveness consisted of 343 dogs receiving either VETMEDIN (n=173) or vehicle control chewable tablets (n=170).
Dogs ranged between 6 and 17 years of age and weighed between 9 and 33 lbs (4.1 to 15.1 kg) at enrollment. Dogs were confirmed to have evidence of Stage B2 preclinical MMVD prior to enrollment, including a systolic heart murmur grade of ≥3/6 and radiographic and echocardiographic evidence of cardiomegaly, including a VHS >10.5, LA/Ao ratio ≥1.6, and LVIDDN ≥1.7.
Dogs were ineligible if they were found to have current or previous evidence of cardiogenic pulmonary edema, clinically significant tachyarrhythmias, cardiac disease other than MMVD, significant systemic disease, evidence of pulmonary hypertension (RA:RV gradient >65 mmHg), or were pregnant or lactating.
The primary endpoint evaluated was a composite of the development of left-sided CHF, cardiac-related death or euthanasia. Left-sided CHF was confirmed by radiographic evidence of cardiogenic pulmonary edema. If a dog died in the absence of evidence of a non-cardiac cause of death, prior to radiographic confirmation of pulmonary edema, it was also considered to have reached the primary endpoint. The study was designed to follow individual dogs for up to 3 years or until disease progressed to a primary endpoint.
At study termination, 42.2% of the dogs in the VETMEDIN group had reached the primary endpoint, compared to 53.5% in the vehicle control group. The median time to the primary endpoint was 1127 days in the VETMEDIN group compared to 732 days in the vehicle control group. Thus, administration of VETMEDIN to dogs with Stage B2 preclinical MMVD resulted in the prolongation of the primary endpoints by 395 days (13.2 months) compared to dogs receiving vehicle control product.
The time to onset of verified CHF was evaluated as a separated component of the primary endpoint. The median time to onset of CHF was 1231 days in the VETMEDIN group versus 806 days in the control group. Thus, administration of VETMEDIN to dogs with Stage B2 preclinical MMVD resulted in the prolongation of the time to onset of verified CHF by 425 days (14.2 months), compared to dogs receiving vehicle control product.
Study 2: The second study was a historically controlled, multi-site field study. As in the first study, dogs were treated with VETMEDIN at the targeted total daily dose of 0.23 mg/lb (0.5 mg/kg) divided into two administrations approximately 12 hours apart. While Study 1 enrolled all dogs with Stage B2 MMVD (LA/Ao ratio ≥1.6), Study 2 enrolled a subset of dogs with Stage B2 MMVD and more advanced cardiomegaly (LA/Ao ratio ≥1.8). The historical control for Study 2 was derived from the vehicle control group from Study 1 (described above) and included dogs with an LA/Ao ratio ≥1.8.
A total of 161 dogs across various breeds were treated with at least one dose of VETMEDIN. The number of dogs included in the population for effectiveness was 125 dogs. Dogs ranged between 6 and 16 years of age and weighed between 9 and 33 lbs (4.1 to 15.0 kg) at enrollment. Dogs were confirmed to have evidence of Stage B2 preclinical MMVD prior to enrollment, including a systolic heart murmur grade of ≥3/6 and evidence of cardiomegaly, including a VHS >10.5, and echocardiographic evidence of LA/Ao ratio ≥1.8.
Dogs were ineligible if they were found to have current or previous evidence of cardiogenic pulmonary edema, clinically significant tachyarrhythmias, current or previous evidence of coughing that interferes with the clinical assessment of progressing clinical signs, current or previous evidence of syncope, cardiac disease other than MMVD, significant systemic disease, evidence of clinically relevant pulmonary hypertension (RA:RV gradient >65 mmHg), or were pregnant or lactating.
The primary endpoint was individual treatment success or failure for each animal. A dog was considered a treatment success if it had no radiographic evidence of CHF at or before Day 365 AND did not develop malignant arrhythmias, syncope, significant coughing, and/or increased resting respiratory rate, requiring concomitant therapy at or before Day 365. A dog was considered a treatment failure if at or before Day 365 it developed clinical signs of CHF with radiographic evidence documented and confirmed by an independent verification committee; or it was euthanized or died in the absence of evidence of a non-cardiac cause of death; or it developed malignant arrhythmias, syncope, significantly increased RRR and/or advanced coughing that required concomitant therapy in absence of radiographic CHF.
Left-sided CHF was confirmed by radiographic evidence of cardiogenic pulmonary edema with left-sided cardiomegaly. In addition to the radiographic confirmation of CHF, dogs had to exhibit contemporaneous clinical signs consistent with left-sided CHF, such as increased respiratory rate and effort, cough, orthopnea, and elevated heart rate without sinus arrhythmia. The study was designed to follow individual dogs for up to 365 days or until disease progressed to a primary endpoint.
By Day 365, 79.2% of dogs on study were treatment successes, with a 2-sided 95% confidence interval (0.7026, 0.8594), which met the study success criteria of the lower bound of the 95% confidence interval greater than or equal to 54% and the estimated success rate for the IVP greater than or equal to 65%.
Clinical MMVD or DCM: Effectiveness of VETMEDIN for the management of the signs of mild, moderate, or severe CHF in dogs due to clinical MMVD or DCM is based on a separate study – a double-masked, multi-site, 56-day field study, in which 355 dogs with modified New York Heart Association‡ (NYHA) Class II, III, or IV CHF due to MMVD or DCM were randomly assigned to either the active control (enalapril maleate) or the VETMEDIN (pimobendan) treatment group. Of the 355 dogs, 52% were male and 48% were female; 72% were diagnosed with MMVD and 28% were diagnosed with DCM; 34% had Class II, 47% had Class III, and 19% had Class IV CHF. Dogs ranged in age and weight from 1 to 17 years and 3.3 to 191 lbs, respectively.
The most common breeds were mixed breed, Doberman Pinscher, Cocker Spaniel, Miniature/Toy Poodle, Maltese, Chihuahua, Miniature Schnauzer, Dachshund, and Cavalier King Charles Spaniel. The 180 dogs (130 MMVD, 50 DCM) in the active control group received enalapril maleate (0.5 mg/kg once or twice daily), and all but 2 received furosemide. Per protocol, all dogs with DCM in the active control group received digoxin. The 175 dogs (126 MMVD, 49 DCM) in the VETMEDIN group received pimobendan (0.5 mg/kg/day divided into 2 portions that were not necessarily equal, and the portions were administered approximately 12 hours apart), and all but 4 received furosemide. Digoxin was optional for treating supraventricular tachyarrhythmia in either treatment group, as was the addition of a β-adrenergic blocker if digoxin was ineffective in controlling heart rate. After initial treatment at the clinic on Day 1, dog owners were to administer the assigned product and concurrent medications for up to 56±4 days.
The determination of effectiveness (treatment success) for each case was based on improvement in at least 2 of the 3 following primary variables: modified NYHA classification, pulmonary edema score by a masked veterinary radiologist, and the investigator’s overall clinical effectiveness score (based on physical examination, radiography, electrocardiography, and clinical pathology). Attitude, pleural effusion, coughing, activity level, furosemide dosage change, cardiac size, body weight, survival, and owner observations were secondary evaluations contributing information supportive to product effectiveness and safety.
Based on protocol compliance and individual case integrity, 265 cases (134 VETMEDIN, 131 active control) were evaluated for treatment success on Day 29. See Table 7 for effectiveness results.
Table 7: Effectiveness Results for the 56-Day Field Study
VETMEDIN Group
Active Control Group
Treatment Success on
Day 29
80.7%
n = 134
76.3%
n = 131
88 of 101 dogs with MMVD
77 of 100 dogs with MMVD
20 of 33 dogs with DCM
23 of 31 dogs with DCM
Treatment Success on
Day 56
71.1%
n = 113
67.2%
n = 110
66 of 85 dogs with MMVD
56 of 85 dogs with MMVD
13 of 28 dogs with DCM
17 of 25 dogs with DCM
No increase in furosemide dose between Day 1 and Day 29
78.3%
n = 130
68.6%
n = 126
At the end of the 56-day study, dogs in the VETMEDIN group were enrolled in an unmasked field study to monitor safety under extended use, without restrictions on concurrent medications.
VETMEDIN was used safely in dogs concurrently receiving furosemide, digoxin, enalapril, atenolol, spironolactone, nitroglycerin, hydralazine, diltiazem, antiparasitic products (including heartworm disease prevention), antibiotics (metronidazole, cephalexin, amoxicillin-clavulanate, fluoroquinolones), topical ophthalmic and otic products, famotidine, theophylline, levothyroxine sodium, diphenhydramine, hydrocodone, metoclopramide, and butorphanol, and in dogs on sodium-restricted diets.
‡ The modified NYHA classification was historically used to stage dogs with heart disease.
A dog with modified NYHA Class II heart failure has fatigue, shortness of breath, coughing, etc. apparent when ordinary exercise is exceeded.
A dog with modified NYHA Class III heart failure is comfortable at rest, but exercise capacity is minimal.
A dog with modified NYHA Class IV heart failure has no capacity for exercise and disabling clinical signs are present even at rest.
-
Target Animal Safety:
The safety of VETMEDIN Solution was established by demonstrating bioequivalence with VETMEDIN Chewable Tablets. (See Clinical Pharmacology).
In a laboratory study, VETMEDIN Chewable Tablets were administered to 6 healthy Beagles per treatment group at 0 (vehicle control), 1, 3, and 5 times the recommended dosage for 6 months. See Table 8 for cardiac pathology results. The cardiac pathology/histopathology noted in the 3X and 5X dose groups is typical of positive inotropic and vasodilator drug toxicity in normal dog hearts, and is associated with exaggerated hemodynamic responses to these drugs. None of the dogs developed signs of heart failure and there was no mortality.
Table 8: Incidence of Cardiac Pathology/Histopathology in the Six-month Safety Study
Severe left ventricular hypertrophy with
multifocal subendocardial ischemic lesions
One 3X and two 5X dogsa
Moderate to marked myxomatous thickening of the mitral valves
Three 5X dogs
Myxomatous thickening of the chordae
tendineae
One 3X and two 5X dogs
Endocardial thickening of the left ventricular outflow tract
One 1X, two 3X, and two 5X dogs
Left atrial endocardial thickening (jet lesions) in 2 of the dogs that developed murmurs of mitral valve insufficiency
One 3X and one 5X dog
Granulomatous inflammatory lesion
in the right atrial myocardium
One 3X dog
a Most of the gross and histopathologic findings occurred in these three dogs
Murmurs of mitral valve insufficiency were detected in one 3X (Day 65) and two 5X dogs
(Days 135 and 163). These murmurs (grades II-III of VI) were not associated with clinical signs.
Indirect blood pressure was unaffected by VETMEDIN at the label dose (1X). Mean diastolic blood pressure was decreased in the 3X group (74 mmHg) compared to the control group (82 mmHg). Mean systolic blood pressure was decreased in the 5X group (117 mmHg) compared to the control group (124 mmHg). None of the dogs had clinical signs of hypotension.
On 24-hour Holter monitoring, mean heart rate was increased in the 5X group (101 beats/min) compared to the control group (94 beats/min). Not counting escape beats, the 3X and 5X groups had slightly higher numbers of isolated ventricular ectopic complexes (VEs). The maximum number of non-escape VEs recorded either at baseline or in a control group dog was 4 VEs/24 hours. At either Week 4 or Week 20, three 3X group dogs had maximums of 33, 13, and 10 VEs/24 hours, and two 5X group dogs had maximums of 22 and 9 VEs/24 hours. One 1X group dog with no VEs at baseline had 6 VEs/24 hours at Week 4 and again at Week 20. Second-degree atrioventricular heart block was recorded in one 3X group dog at Weeks 4 and 20, and in one dog from each of the 1X and 5X groups at Week 20. None of the dogs had clinical signs associated with these electrocardiogram changes.
Treatment was associated with small differences in mean platelet counts (decreased in the 3X and 1X groups), potassium (increased in the 5X group), glucose (decreased in the 1X and 3X groups), and maximum blood glucose in glucose curves (increased in the 5X group).
All individual values for these variables were within the normal range. Three 1X and one 5X group dogs had mild elevations of alkaline phosphatase (less than two times normal).
Loose stools and vomiting were infrequent and self-limiting.
- Storage Information:
-
How Supplied:
VETMEDIN Solution (pimobendan oral solution): Available as 1.5 mg/mL, 50 mL fill volume, is supplied in a 60 mL amber glass bottle sealed with a white cap, an orange in-use cap with integrated plastic plug, and an orange dosing syringe.
NDC: 0010-4131-01
Approved by FDA under NADA # 141-575
-
References:
1 Keene, B., et al. (2019) ACVIM consensus guidelines for the diagnosis and treatment of myxomatous mitral valve disease in dogs. J Vet Intern Med. 33(3):1127-1540.
2 Malcolm, E.L. et. al. (2018) Diagnostic value of vertebral left atrial size as determined from thoracic radiographs for assessment of left atrial size in dogs with myxomatous mitral valve disease. J AM VetMed Assoc. 253(8):1038-1045.
- Marketed by:
- Principal Display Panel – 50 mL Display Carton
-
INGREDIENTS AND APPEARANCE
VETMEDIN SOLUTION
pimobendan solutionProduct Information Product Type PRESCRIPTION ANIMAL DRUG Item Code (Source) NDC: 0010-4131 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength PIMOBENDAN (UNII: 34AP3BBP9T) (PIMOBENDAN - UNII:34AP3BBP9T) PIMOBENDAN 1.5 mg in 1 mL Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 0010-4131-01 1 in 1 CARTON 1 50 mL in 1 BOTTLE, GLASS Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NADA NADA141575 11/11/2024 Labeler - Boehringer Ingelheim Animal Health USA Inc. (007134091)


© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.