HYPERHEP B S/D (hepatitis b immune globulin- human injection
HYPERHEP B by
Drug Labeling and Warnings
HYPERHEP B by is a Other medication manufactured, distributed, or labeled by GRIFOLS USA, LLC, Grifols Therapeutics LLC. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
DESCRIPTION
Hepatitis B Immune Globulin (Human) — HyperHEP B® S/D treated with solvent/detergent is a colorless to pale yellow or pink sterile solution of hepatitis B hyperimmune immune globulin for intramuscular administration; it is preservative-free and latex-free. HyperHEP B S/D is prepared by cold ethanol fractionation from the plasma of donors with high titers of antibody to the hepatitis B surface antigen (anti-HBs). The immune globulin is isolated from solubilized Cohn Fraction II. The Fraction II solution is adjusted to a final concentration of 0.3% tri-n-butyl phosphate (TNBP) and 0.2% sodium cholate. After the addition of solvent (TNBP) and detergent (sodium cholate), the solution is heated to 30°C and maintained at that temperature for not less than 6 hours. After the viral inactivation step, the reactants are removed by precipitation, filtration and finally ultrafiltration and diafiltration. HyperHEP B S/D is formulated as a 15–18% protein solution at a pH of 6.4–7.2 in 0.21–0.32 M glycine. HyperHEP B S/D is then incubated in the final container for 21–28 days at 20–27°C. Each vial or syringe contains anti-HBs antibody equivalent to or exceeding the potency of anti-HBs in a U.S. reference hepatitis B immune globulin (Center for Biologics Evaluation and Research, FDA). The U.S. reference has been tested against the World Health Organization standard Hepatitis B Immune Globulin and found to be equal to 220 international units (IU) per mL.
The removal and inactivation of spiked model enveloped and non-enveloped viruses during the manufacturing process for HyperHEP B S/D has been validated in laboratory studies. Human Immunodeficiency Virus, Type 1 (HIV-1), was chosen as the relevant virus for blood products; Bovine Viral Diarrhea Virus (BVDV) was chosen to model Hepatitis C virus; Pseudorabies virus (PRV) was chosen to model Human Herpes viruses and other large enveloped DNA viruses; and Reo virus type 3 (Reo) was chosen to model non-enveloped viruses and for its resistance to physical and chemical inactivation. Significant removal of model enveloped and non-enveloped viruses is achieved at two steps in the Cohn fractionation process leading to the collection of Cohn Fraction II: the precipitation and removal of Fraction III in the processing of Fraction II + IIIW suspension to Effluent III and the filtration step in the processing of Effluent III to Filtrate III.
Significant inactivation of enveloped viruses is achieved at the time of treatment of solubilized Cohn Fraction II with TNBP/sodium cholate.
Additionally, the manufacturing process was investigated for its capacity to decrease the infectivity of an experimental agent of transmissible spongiform encephalopathy (TSE), considered as a model for the vCJD and CJD agents. [22–25]
Studies of the HyperHEP B S/D manufacturing process demonstrate that TSE clearance is achieved during the Pooled Plasma to Effluent III Fractionation Process (6.7 log10). These studies provide reasonable assurance that low levels of CJD/vCJD agent infectivity, if present in the starting material, would be removed.
-
CLINICAL PHARMACOLOGY
Hepatitis B Immune Globulin (Human) provides passive immunization for individuals exposed to the hepatitis B virus (HBV) as evidenced by a reduction in the attack rate of hepatitis B following its use. [1-6] The administration of the usual recommended dose of this immune globulin generally results in a detectable level of circulating anti-HBs which persists for approximately 2 months or longer. The highest antibody (IgG) serum levels were seen in the following distribution of subjects studied: [7]
DAY % OF SUBJECTS 3 38.9% 7 41.7% 14 11.1% 21 8.3% Mean values for half-life were between 17.5 and 25 days, with the shortest being 5.9 days and the longest 35 days. [7]
Cases of type B hepatitis are rarely seen following exposure to HBV in persons with preexisting anti-HBs. No confirmed instance of transmission of hepatitis B has been associated with this product.
In a clinical study in eight healthy human adults receiving another hyperimmune immune globulin product treated with solvent/detergent, Rabies Immune Globulin (Human), HyperRAB® S/D, prepared by the same manufacturing process, detectable passive antibody titers were observed in the serum of all subjects by 24 hours post injection and persisted through the 21 day study period. These results suggest that passive immunization with immune globulin products is not affected by the solvent/detergent treatment.
-
INDICATIONS AND USAGE
Recommendations on post-exposure prophylaxis are based on available efficacy data and on the likelihood of future HBV exposure for the person requiring treatment. In all exposures, a regimen combining Hepatitis B Immune Globulin (Human) with hepatitis B vaccine will provide both short- and long-term protection, will be less costly than the two-dose Hepatitis B Immune Globulin (Human) treatment alone, and is the treatment of choice. [8] HyperHEP B S/D is indicated for post-exposure prophylaxis in the following situations:
Acute Exposure to Blood Containing HBsAg
After either parenteral exposure, e.g., by accidental “needlestick” or direct mucous membrane contact (accidental splash), or oral ingestion (pipetting accident) involving HBsAg-positive materials such as blood, plasma or serum. For inadvertent percutaneous exposure, a regimen of two doses of Hepatitis B Immune Globulin (Human), one given after exposure and one a month later, is about 75% effective in preventing hepatitis B in this setting.
Perinatal Exposure of Infants Born to HBsAg-positive Mothers
Infants born to HBsAg-positive mothers are at risk of being infected with hepatitis B virus and becoming chronic carriers. [5,8-10] This risk is especially great if the mother is HBeAg-positive. [11-13] For an infant with perinatal exposure to an HBsAg-positive and HBeAg-positive mother, a regimen combining one dose of Hepatitis B Immune Globulin (Human) at birth with the hepatitis B vaccine series started soon after birth is 85%–95% effective in preventing development of the HBV carrier state. [8,14] Regimens involving either multiple doses of Hepatitis B Immune Globulin (Human) alone or the vaccine series alone have 70%–90% efficacy, while a single dose of Hepatitis B Immune Globulin (Human) alone has only 50% efficacy. [8,15]
Sexual Exposure to an HBsAg-positive Person
Sex partners of HBsAg-positive persons are at increased risk of acquiring HBV infection. For sexual exposure to a person with acute hepatitis B, a single dose of Hepatitis B Immune Globulin (Human) is 75% effective if administered within 2 weeks of last sexual exposure. [8]
Household Exposure to Persons with Acute HBV Infection
Since infants have close contact with primary care-givers and they have a higher risk of becoming HBV carriers after acute HBV infection, prophylaxis of an infant less than 12 months of age with Hepatitis B Immune Globulin (Human) and hepatitis B vaccine is indicated if the mother or primary caregiver has acute HBV infection. [8]
Administration of Hepatitis B Immune Globulin (Human) either preceding or concomitant with the commencement of active immunization with Hepatitis B Vaccine provides for more rapid achievement of protective levels of hepatitis B antibody, than when the vaccine alone is administered. [16] Rapid achievement of protective levels of antibody to hepatitis B virus may be desirable in certain clinical situations, as in cases of accidental inoculations with contaminated medical instruments. [16] Administration of Hepatitis B Immune Globulin (Human) either 1 month preceding or at the time of commencement of a program of active vaccination with Hepatitis B Vaccine has been shown not to interfere with the active immune response to the vaccine. [16]
- CONTRAINDICATIONS
-
WARNINGS
HyperHEP B S/D is made from human plasma. Products made from human plasma may contain infectious agents, such as viruses, and, theoretically, the Creutzfeldt-Jakob Disease (CJD) agent that can cause disease. The risk that such products will transmit an infectious agent has been reduced by screening plasma donors for prior exposure to certain viruses, by testing for the presence of certain current virus infections, and by inactivating and/or removing certain viruses. Despite these measures, such products can still potentially transmit disease. There is also the possibility that unknown infectious agents may be present in such products. Individuals who receive infusions of blood or plasma products may develop signs and/or symptoms of some viral infections, particularly hepatitis C. ALL infections thought by a physician possibly to have been transmitted by this product should be reported by the physician or other healthcare provider to Grifols Therapeutics LLC [1-800-520-2807].
The physician should discuss the risks and benefits of this product with the patient, before prescribing or administering it to the patient.
HyperHEP B S/D should be given with caution to patients with a history of prior systemic allergic reactions following the administration of human immune globulin preparations. Epinephrine should be available.
In patients who have severe thrombocytopenia or any coagulation disorder that would contraindicate intramuscular injections, Hepatitis B Immune Globulin (Human) should be given only if the expected benefits outweigh the risks.
-
PRECAUTIONS
General
HyperHEP B S/D should not be administered intravenously because of the potential for serious reactions. Injections should be made intramuscularly, and care should be taken to draw back on the plunger of the syringe before injection in order to be certain that the needle is not in a blood vessel.
Intramuscular injections are preferably administered in the deltoid muscle of the upper arm or lateral thigh muscle. The gluteal region should not be used as an injection site because of the risk of injury to the sciatic nerve. [17] An individual decision as to which muscle is injected must be made for each patient based on the volume of material to be administered.
Drug Interactions
Although administration of Hepatitis B Immune Globulin (Human) did not interfere with measles vaccination, [18] it is not known whether Hepatitis B Immune Globulin (Human) may interfere with other live virus vaccines. Therefore, use of such vaccines should be deferred until approximately 3 months after Hepatitis B Immune Globulin (Human) administration. Hepatitis B Vaccine may be administered at the same time, but at a different injection site, without interfering with the immune response. [16] No interactions with other products are known.
-
ADVERSE REACTIONS
Local pain and tenderness at the injection site, urticaria and angioedema may occur; anaphylactic reactions, although rare, have been reported following the injection of human immune globulin preparations. [19]
- OVERDOSAGE
-
DOSAGE AND ADMINISTRATION
Acute Exposure to Blood Containing HBsAg [15]
Table 1 summarizes prophylaxis for percutaneous (needlestick or bite), ocular, or mucous-membrane exposure to blood according to the source of exposure and vaccination status of the exposed person. For greatest effectiveness, passive prophylaxis with Hepatitis B Immune Globulin (Human) should be given as soon as possible after exposure (its value beyond 7 days of exposure is unclear). If Hepatitis B Immune Globulin (Human) is indicated (see Table 1), an injection of 0.06 mL/kg of body weight should be administered intramuscularly (see PRECAUTIONS) as soon as possible after exposure and within 24 hours, if possible. Consult Hepatitis B Vaccine package insert for dosage information regarding that product.
Table 1. (adapted from [20]) Recommendations for Hepatitis B Prophylaxis Following Percutaneous or Permucosal Exposure - * Hepatitis B Immune Globulin (Human), dose 0.06 mL / kg IM.
- † HB Vaccine dose 20 μg IM for adults; 10 μg IM for infants or children under 10 years of age. First dose within 1 week; second and third doses, 1 and 6 months later.
- ‡ Less than 10 sample ratio units (SRU) by radioimmunoassay (RIA), negative by enzyme immunoassay (EIA).
Exposed Person Source Unvaccinated Vaccinated HBsAg-Positive 1. Hepatitis B Immune Globulin (Human) x1 immediately* 1. Test exposed person for anti-HBs. 2. Initiate HB Vaccine Series† 2. If inadequate antibody,‡ Hepatitis B Immune Globulin (Human) (x1) immediately plus HB Vaccine booster dose, or 2 doses of HBIG,* one as soon as possible after exposure and the second 1 month later. Known Source
(High Risk)1. Initiate HB Vaccine Series 1. Test Source for HBsAg only if exposed is vaccine nonresponder; if source is HBsAg-positive, give Hepatitis B Immune Globulin (Human) x1 immediately plus HB Vaccine booster dose, or 2 doses of HBIG,* one as soon as possible after exposure and the second 1 month later. 2. Test source for HBsAg. If positive, Hepatitis B Immune Globulin (Human) x1 Low Risk
HBsAg-PositiveInitiate HB Vaccine series Nothing required. Unknown
SourceInitiate HB Vaccine series within 7 days of exposure Nothing required. For persons who refuse Hepatitis B Vaccine, a second dose of Hepatitis B Immune Globulin (Human) should be given 1 month after the first dose.
Prophylaxis of Infants Born to HBsAg and HBeAg Positive Mothers
Efficacy of prophylactic Hepatitis B Immune Globulin (Human) in infants at risk depends on administering Hepatitis B Immune Globulin (Human) on the day of birth. It is therefore vital that HBsAg-positive mothers be identified before delivery.
Hepatitis B Immune Globulin (Human) (0.5 mL) should be administered intramuscularly (IM) to the newborn infant after physiologic stabilization of the infant and preferably within 12 hours of birth. Hepatitis B Immune Globulin (Human) efficacy decreases markedly if treatment is delayed beyond 48 hours. Hepatitis B Vaccine should be administered IM in three doses of 0.5 mL of vaccine (10 μg) each. The first dose should be given within 7 days of birth and may be given concurrently with Hepatitis B Immune Globulin (Human) but at a separate site. The second and third doses of vaccine should be given 1 month and 6 months, respectively, after the first. If administration of the first dose of Hepatitis B Vaccine is delayed for as long as 3 months, then a 0.5 mL dose of Hepatitis B Immune Globulin (Human) should be repeated at 3 months. If Hepatitis B Vaccine is refused, the 0.5 mL dose of Hepatitis B Immune Globulin (Human) should be repeated at 3 and 6 months. Hepatitis B Immune Globulin (Human) administered at birth should not interfere with oral polio and diphtheria-tetanus-pertussis vaccines administered at 2 months of age. [15]
Sexual Exposure to an HBsAg-positive Person
All susceptible persons whose sex partners have acute hepatitis B infection should receive a single dose of HBIG (0.06 mL/kg) and should begin the hepatitis B vaccine series if prophylaxis can be started within 14 days of the last sexual contact or if sexual contact with the infected person will continue (see Table 2 below). Administering the vaccine with HBIG may improve the efficacy of postexposure treatment. The vaccine has the added advantage of conferring long-lasting protection. [8]
Table 2. (adapted from [21]) Recommendations for Postexposure Prophylaxis for Sexual Exposure to Hepatitis B - * HBIG = Hepatitis B Immune Globulin (Human)
- † IM = intramuscularly
- ‡ The first dose can be administered the same time as the HBIG dose but at a different site; subsequent doses should be administered as recommended for specific vaccine.
HBIG* Vaccine Dose Recommended timing Dose Recommended timing 0.06 mL/kg IM† Single dose within 14 days of last sexual contact 1.0 mL IM† First dose at time of HBIG* treatment‡ Household Exposure to Persons with Acute HBV Infection
Prophylactic treatment with a 0.5 mL dose of Hepatitis B Immune Globulin (Human) and hepatitis B vaccine is indicated for infants <12 months of age who have been exposed to a primary care-giver who has acute hepatitis B. Prophylaxis for other household contacts of persons with acute HBV infection is not indicated unless they have had identifiable blood exposure to the index patient, such as by sharing toothbrushes or razors. Such exposures should be treated like sexual exposures. If the index patient becomes an HBV carrier, all household contacts should receive hepatitis B vaccine. [8]
Hepatitis B Immune Globulin (Human) may be administered at the same time (but at a different site), or up to 1 month preceding Hepatitis B Vaccination without impairing the active immune response from Hepatitis B Vaccination.[16]
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit.
Administer intramuscularly. Do not inject intravenously.
Hepatitis B Immune Globulin (Human) — HyperHEP B® S/D is supplied in a syringe with an attached UltraSafe® Needle Guard for your protection and convenience, as well as in vials. Please follow instructions below for proper use of syringe and UltraSafe® Needle Guard.
Directions for Syringe Usage
-
Remove the prefilled syringe from the package. Lift syringe by barrel,
not by plunger. -
Twist the plunger rod clockwise until the threads are seated.
-
With the rubber needle shield secured on the syringe tip, push the plunger rod forward a few millimeters to break any friction seal between the rubber stopper and the glass syringe barrel.
-
Remove the needle shield and expel air bubbles. [Do not remove the rubber needle shield to prepare the product for administration until immediately prior to the anticipated injection time.]
-
Proceed with hypodermic needle puncture.
-
Aspirate prior to injection to confirm that the needle is not in a vein or artery.
- Inject the medication.
-
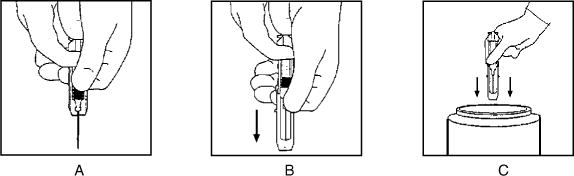
Keeping your hands behind the needle, grasp the guard with free hand and slide forward toward needle until it is completely covered and guard clicks into place. If audible click is not heard, guard may not be completely activated. (See Diagrams A and B)
-
Place entire prefilled glass syringe with guard activated into an approved sharps container for proper disposal. (See Diagram C)
A number of factors could reduce the efficacy of this product or even result in an ill effect following its use. These include improper storage and handling of the product after it leaves our hands, diagnosis, dosage, method of administration and biological differences in individual patients. Because of these factors, it is important that this product be stored properly and that the directions be followed carefully during use.
-
HOW SUPPLIED
HyperHEP B S/D is supplied in a 0.5 mL neonatal single dose syringe with attached needle, a 1 mL single dose syringe with attached needle and a 1 mL and a 5 mL single dose vial. HyperHEP B S/D is preservative-free and latex-free.
NDC Number Size 13533-636-03 0.5 mL syringe 13533-636-02 1 mL syringe 13533-636-01 1 mL vial 13533-636-05 5 mL vial - STORAGE
- CAUTION
-
REFERENCES
- Grady GF, Lee VA: Hepatitis B immune globulin — prevention of hepatitis from accidental exposure among medical personnel. N Engl J Med 293(21):1067–70, 1975.
- Seeff LB, Zimmerman HJ, Wright EC, et al: Efficacy of hepatitis B immune serum globulin after accidental exposure. Lancet 2(7942):939-41, 1975.
- Krugman S, Giles JP: Viral hepatitis, type B (MS-2-strain). Further observations on natural history and prevention. N Engl J Med 288(15):755-60, 1973.
- Current trends: Health status of Indochinese refugees: malaria and hepatitis B. MMWR 28(39):463-4; 469-70, 1979.
- Jhaveri R, Rosenfeld W, Salazar JD, et al: High titer multiple dose therapy with HBIG in newborn infants of HBsAg positive mothers. J Pediatr 97(2):305–8, 1980.
- Hoofnagle JH, Seeff LB, Bales ZB, et al: Passive-active immunity from hepatitis B immune globulin. Ann Intern Med 91(6):813-8, 1979.
- Scheiermann N, Kuwert EK: Uptake and elimination of hepatitis B immunoglobulins after intramuscular application in man. Dev Biol Stand 54:347-55, 1983.
- Recommendations of the Immunization Practices Advisory Committee (ACIP): Hepatitis B Virus: A Comprehensive Strategy for Eliminating Transmission in the United States Through Universal Childhood Vaccination. Appendix A: Postexposure Prophylaxis for Hepatitis B. MMWR 40(RR-13):21-25, 1991.
- Stevens CE, Beasley RP, Tsui J, et al: Vertical transmission of hepatitis B antigen in Taiwan. N Engl J Med 292(15):771-4, 1975.
- Shiraki K, Yoshihara N, Kawana T, et al: Hepatitis B surface antigen and chronic hepatitis in infants born to asymptomatic carrier mothers. Am J Dis Child 131(6):644-7, 1977.
- Recommendation of the Immunization Practices Advisory Committee (ACIP): Immune globulins for protection against viral hepatitis. MMWR 30(34):423-8; 433-5, 1981.
- Okada K, Kamiyama I, Inomata M, et al: e antigen and anti-e in the serum of asymptomatic carrier mothers as indicators of positive and negative transmission of hepatitis B virus to their infants. N Engl J Med 294(14):746-9, 1976.
- Beasley RP, Trepo C, Stevens CE, et al: The e antigen and vertical transmission of hepatitis B surface antigen. Am J Epidemiol 105(2):94-8, 1977.
- Beasley RP, Hwang LY, Lee GCY, et al: Prevention of perinatally transmitted hepatitis B virus infections with hepatitis B immune globulin and hepatitis B vaccine. Lancet 2(8359): 1099-102, 1983.
- Recommendation of the Immunization Practices Advisory Committee (ACIP): Recommendations for protection against viral hepatitis. MMWR 34(22):313–35, 1985.
- Szmuness W, Stevens CE, Olesko WR, et al: Passive-active immunisation against hepatitis B: immunogenicity studies in adult Americans. Lancet 1:575–77, 1981.
- Recommendations of the Advisory Committee on Immunization Practices (ACIP) and the AmericanAcademy of Family Physicians (AAFP): General recommendations on immunization. MMWR 2002:51 (RR02), 1-36.
- Beasley RP, Hwang LY: Measles vaccination not interfered with by hepatitis B immune globulin. Lancet 1:161, 1982.
- Ellis EF, Henney CS: Adverse reactions following administration of human gamma globulin. J Allerg 43(1):45-54, 1969.
- Recommendations of the Immunization Practices Advisory Committee (ACIP): Update on Adult Immunization. Table 9. Recommendations for postexposure prophylaxis for percutaneous or permucosal exposure to hepatitis B, United States. MMWR 40(RR-12):70, 1991.
- Recommendations of the Immunization Practices Advisory Committee (ACIP): Update on Adult Immunization. Table 10. Recommendations for postexposure prophylaxis for perinatal and sexual exposure to hepatitis B, United States. MMWR 40(RR-12):71, 1991.
- Stenland CJ, Lee DC, Brown P, et al. Partitioning of human and sheep forms of the pathogenic prion protein during the purification of therapeutic proteins from human plasma. Transfusion 2002. 42(11):1497-500.
- Lee DC, Stenland CJ, Miller JL, et al. A direct relationship between the partitioning of the pathogenic prion protein and transmissible spongiform encephalopathy infectivity during the purification of plasma proteins. Transfusion 2001. 41(4):449-55.
- Lee DC, Stenland CJ, Hartwell RC, et al. Monitoring plasma processing steps with a sensitive Western blot assay for the detection of the prion protein. J Virol Methods 2000. 84(1):77-89.
- Cai K, Miller JL, Stenland CJ, et al. Solvent-dependent precipitation of prion protein. Biochim Biophys Acta 2002. 1597(1):28-35.
Grifols Therapeutics LLC
Research Triangle Park, NC 27709 USA
U.S. License No. 18713051849
(Rev. 6/2018) -
PACKAGE LABEL
Hepatitis B Immune Globulin (Human)
HyperHEP B® S/D
Solvent/Detergent Treated
Preservative-free, latex-free
5 mL
Sterile Solution
NDC 13533-636-05
GRIFOLS
The patient and physician should discuss the risks and benefits of this product.
One Single Dose Vial
FOR INTRAMUSCULAR INJECTION ONLY. DO NOT GIVE INTRAVENOUSLY.
For complete dosage and administration information, read enclosed package insert.
Store at 2–8°C (36–46°F).
Do not freeze.
If the shrink band is absent or shows any sign of tampering, do not use the product and notify Grifols Therapeutics LLC immediately.
Not returnable for credit or exchange.
Rx only
CAUTION: U.S. federal law prohibits dispensing without prescription.
Hepatitis B Immune Globulin (Human) is a sterile solution of immunoglobulin containing 15%–18% protein stabilized with 0.21–0.32 M glycine. The pH is adjusted with sodium carbonate.
The potency is equivalent to or exceeds that of the U.S. Food and Drug Administration Reference Hepatitis B Immune Globulin. The U.S. reference has been tested against the World Health Organization standard Hepatitis B Immune Globulin and found to be equal to 220 international units (IU) per mL.
Grifols Therapeutics LLC
Research Triangle Park,
NC 27709 USA
U.S. License No. 1871
LOT XXXXXXXXXX
EXP DDMMMYYYY
SN XXXXXXXXXXXXXXXX
GTIN 00313533636050
3051844
Lot/Exp.
NDC 13533-636-50
Hepatitis B Immune
Globulin (Human)
HyperHEP B® S/D 5 mL
Solvent/Detergent Treated
The patient and physician should discuss the risks and benefits of this product.
Dosage & Administration: See insert.
Grifols Therapeutics LLC
RTP, NC 27709 USA
U.S. License No. 1871
-
INGREDIENTS AND APPEARANCE
HYPERHEP B S/D
hepatitis b immune globulin (human) injectionProduct Information Product Type PLASMA DERIVATIVE Item Code (Source) NDC: 13533-636 Route of Administration INTRAMUSCULAR Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength Human Hepatitis B Virus Immune Globulin (UNII: XII270YC6M) (Human Hepatitis B Virus Immune Globulin - UNII:XII270YC6M) Human Hepatitis B Virus Immune Globulin 220 [iU] in 1 mL Inactive Ingredients Ingredient Name Strength Glycine (UNII: TE7660XO1C) Water (UNII: 059QF0KO0R) Product Characteristics Color YELLOW (YELLOW (Clear liquid, colorless to pale yellow or pink)) Score Shape Size Flavor Imprint Code Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 13533-636-01 1 in 1 CARTON 1 NDC: 13533-636-10 1 mL in 1 VIAL, GLASS; Type 0: Not a Combination Product 2 NDC: 13533-636-02 1 in 1 CARTON 2 NDC: 13533-636-20 1 mL in 1 SYRINGE, GLASS; Type 3: Prefilled Biologic Delivery Device/System (syringe, patch, etc.) 3 NDC: 13533-636-03 1 in 1 CARTON 3 NDC: 13533-636-30 0.5 mL in 1 SYRINGE, GLASS; Type 3: Prefilled Biologic Delivery Device/System (syringe, patch, etc.) 4 NDC: 13533-636-05 1 in 1 CARTON 4 NDC: 13533-636-50 5 mL in 1 VIAL, GLASS; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA101146 10/09/1996 Labeler - GRIFOLS USA, LLC (048987452) Establishment Name Address ID/FEI Business Operations Grifols Therapeutics LLC 611019113 manufacture(13533-636)
Trademark Results [HYPERHEP B]
Mark Image Registration | Serial | Company Trademark Application Date |
|---|---|
 HYPERHEP B 78622916 3197566 Live/Registered |
GRIFOLS THERAPEUTICS LLC 2005-05-04 |
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.