VYKOURA- leucovorin calcium injection
VYKOURA by
Drug Labeling and Warnings
VYKOURA by is a Prescription medication manufactured, distributed, or labeled by Avyxa Pharma, LLC, Avyxa Holdings, LLC.. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use VYKOURA safely and effectively. See full prescribing information for VYKOURA.
VYKOURATM (leucovorin calcium) injection, for intravenous or intramuscular use
Initial U.S. Approval: 1952INDICATIONS AND USAGE
VYKOURA is a folate analog indicated for:
- Rescue after high-dose methotrexate therapy in adult and pediatric patients. (1.1)
- Reducing the toxicity of
- methotrexate in adult and pediatric patients with impaired methotrexate elimination or
- folic acid antagonists or dihydrofolate reductase (DHFR) inhibitors following an overdose in adult and pediatric patients. (1.2)
- Treatment of megaloblastic anemias due to folic acid deficiency in adult and pediatric patients when oral therapy is not feasible. (1.3)
- Treatment of patients with metastatic colorectal cancer in combination with 5-fluorouracil. (1.4)
Limitations of Use:
VYKOURA is not indicated for the treatment of pernicious anemia and megaloblastic anemia secondary to lack of vitamin B12, because of the risk of progression of neurologic manifestations despite hematologic remission. (1.3)
DOSAGE AND ADMINISTRATION
VYKOURA is indicated for intravenous or intramuscular administration. Do not administer intrathecally. (2.1)
Rescue After High-Dose Methotrexate Therapy:
- Rescue recommendations are based on methotrexate dose of 12 to 15 grams/m2administered by intravenous infusion over 4 hours. Initiate rescue at a dose of 15 mg (approximately 10 mg/m2) every 6 hours beginning 24 hours after the beginning of methotrexate infusion. (2.2)
- Continue until the methotrexate level is below 0.05 micromolar (5 x 10-8M). Adjust dose, if necessary, based on methotrexate elimination. (2.2)
Reducing the Toxicity of Methotrexate in Patients with Impaired Methotrexate Elimination or Following an Overdosage of Folic Acid Antagonists or DHFR Inhibitors:
- Start as soon as possible after methotrexate overdosage or within 24 hours of delayed methotrexate elimination. (2.3)
- Administer VYKOURA 10 mg/m2intravenously or intramuscularly every 6 hours until methotrexate level is less than 0.01 micromolar (1 x 10-8M). (2.3)
Metastatic Colorectal Cancer in Combination with Fluorouracil:
- 20 mg/m2to 500 mg/m2based on specific combination regimen.
- Administer VYKOURA before fluorouracil. (2.4)
- Do not mix VYKOURA with other drugs or administer other drugs through the same intravenous line. (2.4).
Megaloblastic Anemia Due to Folic Acid Deficiency:
- Up to 1 mg/day administered intravenously until adequate hematologic response is achieved.
DOSAGE FORMS AND STRENGTHS
Injection: 50 mg/5 mL, 350 mg/35 mL, and 500 mg/50 mL (10 mg/mL) in a single-dose vial. (3)
CONTRAINDICATIONS
VYKOURA is contraindicated in patients who have had a severe hypersensitivity reaction to leucovorin (folinic acid), levoleucovorin, or folic acid. (4)
WARNINGS AND PRECAUTIONS
- Hypersensitivity: Hypersensitivity reactions, including anaphylactic reactions and urticaria can occur. Withhold or permanently discontinue VYKOURA based on the severity of hypersensitivity. (5.1)
- Hypercalcemia: Due to calcium content, inject no more than 16 mL (160 mg) of VYKOURA intravenously per minute. (5.2)
- Risk of Administration Errors: Do not administer VYKOURA intrathecally. (5.3)
ADVERSE REACTIONS
- The most common adverse reactions (≥20%) in patients receiving high-dose methotrexate therapy with leucovorin rescue are stomatitis and vomiting. (6.1)
- The most common adverse reactions (>50%) in patients receiving leucovorin in combination with fluorouracil for metastatic colorectal cancer are stomatitis, diarrhea, and nausea. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Avyxa Pharma, LLC at 1-888-520-0954 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
See 17 for PATIENT COUNSELING INFORMATION.
Revised: 2/2026
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Important Administration Information
2.2 Recommended Dosage for Rescue After High-Dose Methotrexate Therapy
2.3 Recommended Dosage to Reduce Toxicity of Folic Acid Antagonists or Dihydrofolate Reductase (DHFR) Inhibitors or for Impaired Methotrexate Elimination
2.4 Recommended Dosage in Combination with Fluorouracil for Advanced Colorectal Cancer
2.5 Recommended Dosage for Megaloblastic Anemia Due to Folic Acid Deficiency
2.6 Preparation and Administration
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Hypersensitivity
5.2 Hypercalcemia
5.3 Risk of Administration Errors
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
7 DRUG INTERACTIONS
7.1 Effects of Other Drugs on VYKOURA
7.2 Effects of VYKOURA on Other Drugs
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.4 Pediatric Use
8.5 Geriatric Use
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- * Sections or subsections omitted from the full prescribing information are not listed.
-
1 INDICATIONS AND USAGE
1.1 Rescue after high-dose methotrexate (MTX) therapy in adult and pediatric patients.
1.2 Reducing the toxicity of:
- Methotrexate in adult and pediatric patients with impaired methotrexate elimination or
- Folic acid antagonists or dihydrofolate reductase (DHFR) inhibitors following an overdose in adult and pediatric patients.
1.3 Treatment of megaloblastic anemias due to folic acid deficiency in adult and pediatric patients when oral therapy is not feasible.
1.4 Treatment of patients with metastatic colorectal cancer in combination with fluorouracil.
Limitations of Use
VYKOURA is not indicated for pernicious anemia and megaloblastic anemia secondary to the lack of vitamin B12, because of the risk of progression of neurologic manifestations despite hematologic remission.
-
2 DOSAGE AND ADMINISTRATION
2.1 Important Administration Information
- VYKOURA is indicated for intravenous (IV) and intramuscular (IM) administration. Do not administer intrathecally. VYKOURA may be harmful or fatal if given intrathecally.
- Do NOT mix VYKOURA with other drugs or administer other drugs through the same intravenous line. A precipitate may form if VYKOURA is mixed with fluorouracil.
- Due to the calcium content of VYKOURA, do NOT exceed the maximum infusion rate of 160 mg/minute to avoid hypercalcemia. [SeeWarnings and Precautions (5.2)]
2.2 Recommended Dosage for Rescue After High-Dose Methotrexate Therapy
- The recommended dosage for VYKOURA is based on serum methotrexate levels obtained 24 hours following the methotrexate infusion (refer to the methotrexate prescribing information). Table 1 describes the VYKOURA regimen in patients who receive a dose of 12-15 grams/m2of methotrexate. Consult institutional guidelines for additional dosing information as appropriate.
- Begin VYKOURA twenty-four hours after starting the methotrexate infusion. As the time interval between methotrexate administration and VYKOURA increases, the effectiveness of VYKOURA to diminish methotrexate toxicity may decrease.
- VYKOURA may be administered intravenously or intramuscularly [see Dosage and Administration (2.6)].
- Monitor serum creatinine and methotrexate levels at least once daily. Administer intravenous fluids (3 Liters per day) and alkalinize the urine to a pH of 7 or greater until the methotrexate level is below 0.05 micromolar (5 x 10-8M).
Table 1 Recommended Dosage for VYKOURA After High-Dose Methotrexate Based on Serum Methotrexate and Serum Creatinine Levels * These patients are likely to develop reversible renal failure. In addition to appropriate VYKOURA therapy, continue hydration and urinary alkalinization and monitor fluid and electrolyte status, until the serum methotrexate level has fallen to below 0.05 micromolar and the renal failure has resolved.
Clinical Situation
Laboratory Findings
Recommended Dosage
Normal Methotrexate Elimination
Serum methotrexate level approximately 10 micromolar at 24 hours after administration, 1 micromolar at 48 hours, and less than 0.2 micromolar at 72 hours.
15 mg intravenously or intramuscularly every 6 hours for 60 hours for a total of 10 doses.
Begin VYKOURA 24 hours after the start of methotrexate infusion.
Delayed Late
Methotrexate
Elimination
Serum methotrexate level remaining above 0.2 micromolar at 72 hours, and more than 0.05 micromolar at 96 hours after administration.
Continue 15 mg intravenously or intramuscularly every 6 hours, until methotrexate level is less than 0.05 micromolar.
Delayed Early
Methotrexate
Elimination and/or
Evidence of Acute
Renal Injury*
Serum methotrexate level of 50 micromolar or more at 24 hours, or 5 micromolar or more at 48 hours after administration,
OR
100% or greater increase in serum creatinine level at 24 hours after methotrexate administration (e.g., an increase from 0.5 mg/dL to a level of 1 mg/dL or more).
150 mg intravenously or intramuscularly every 3 hours, until methotrexate level is less than 1 micromolar; then 15 mg intravenously or intramuscularly every 3 hours until methotrexate level is less than 0.05 micromolar.
Extend VYKOURA rescue for an additional 24 hours (total of 14 doses over 84 hours) in subsequent courses of methotrexate in patients with:
- Impaired methotrexate elimination including third-space fluid accumulation and inadequate hydration
- Renal impairment
2.3 Recommended Dosage to Reduce Toxicity of Folic Acid Antagonists or Dihydrofolate Reductase (DHFR) Inhibitors or for Impaired Methotrexate Elimination
Start VYKOURA as soon as possible after an inadvertent overdosage of methotrexate or within 24 hours of methotrexate administration when methotrexate elimination is impaired. As the time interval between methotrexate administration and VYKOURA increases, the effectiveness of VYKOURA to diminish methotrexate toxicity may decrease.
Administer VYKOURA 10 mg/m2 intravenously or intramuscularly every 6 hours until the serum methotrexate level is less than 0.01 micromolar (1 x 10-8 M).
Monitor serum creatinine and methotrexate levels at least every 24 hours. Increase the dosage of VYKOURA to 100 mg/m2 intravenously every 3 hours if
- serum creatinine at 24-hours increases 50% or more compared to baseline
- the methotrexate level at 24-hours is greater than 5 micromolar (5 x 10-6M)
- the methotrexate level at 48-hours is greater than 0.9 micromolar (9 x 10-7M)
Continue VYKOURA at the same dosage until the methotrexate level is less than 0.01 micromolar (1 x 10-8 M).
Continue intravenous fluids (3 L per day) and sodium bicarbonate. Adjust the sodium bicarbonate dose to maintain urine pH at 7.0 or greater.
2.4 Recommended Dosage in Combination with Fluorouracil for Advanced Colorectal Cancer
Administer VYKOURA intravenously prior to fluorouracil.
Dosage of VYKOURA in combination with fluorouracil varies by regimen and ranges from 20 mg/m2 to 500 mg/m2. Consult institutional guidelines for recommended dosing, dosing frequency, and duration of therapy.
Refer to the Prescribing Information for fluorouracil and other drugs used in combination with VYKOURA for additional information on management of adverse reactions.
2.5 Recommended Dosage for Megaloblastic Anemia Due to Folic Acid Deficiency
Up to 1 mg daily administered intravenously until adequate hematologic response is achieved. There is no evidence that doses greater than 1 mg/day have greater efficacy than those of 1 mg; additionally, loss of folate in urine becomes roughly logarithmic as the amount administered exceeds 1 mg.
2.6 Preparation and Administration
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit.
For Intravenous Injection
Preparation
- Select the appropriate number of vial(s) based on the prescribed dose.
- Withdraw the calculated dose into a sterile syringe and administer immediately.
- Discard partially used or empty vials as VYKOURA does not contain any preservatives.
- Administer VYKOURA slowly. Do not exceed an intravenous administration rate of 160 mg per minute (16 mL per minute) to avoid hypercalcemia[see Warnings and Precautions (5.2)].
Preparation
- Select the appropriate number of vial(s) based on the prescribed dose.
- Withdraw the calculated dose into a sterile syringe and administer immediately.
- Discard partially used or empty vials as VYKOURA does not contain any preservatives.
- Administer the prescribed dose of VYKOURA by intramuscular injection using standard aseptic technique.
- 3 DOSAGE FORMS AND STRENGTHS
-
4 CONTRAINDICATIONS
VYKOURA is contraindicated in patients who have had a severe hypersensitivity reaction to leucovorin (folinic acid), levoleucovorin, or folic acid [see Warnings and Precautions (5.1)]. Reactions have included anaphylactic reactions.
-
5 WARNINGS AND PRECAUTIONS
5.1 Hypersensitivity
Hypersensitivity reactions, including anaphylactic reactions and urticaria, have been reported following the administration of leucovorin. VYKOURA is contraindicated in patients who have had a severe hypersensitivity reaction to leucovorin, levoleucovorin, or folic acid [see Contraindications (4)]. Withhold or permanently discontinue VYKOURA based on the severity of hypersensitivity.
5.2 Hypercalcemia
Because of the calcium content of the VYKOURA, do not administer more than 160 mg of VYKOURA intravenously per minute [see Dosing and Administration (2.6)].
-
6 ADVERSE REACTIONS
The following clinically significant adverse reactions are described elsewhere in the labeling:
- Hypersensitivity [see Warnings and Precautions (5.1)]
- Hypercalcemia [see Warnings and Precautions (5.2)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
Table 2 summarizes significant adverse events occurring in 316 patients treated with the leucovorin/5-fluorouracil combinations compared against 70 patients treated with 5-fluorouracil alone for advanced colorectal carcinoma. These data are taken from the Mayo/NCCTG large multicenter prospective trial evaluating the efficacy and safety of the combination regimen.
Table 2: Percentage of Patients Treated with Leucovorin and Fluorouracil for Advanced Colorectal Carcinoma Reporting Adverse Experiences or Hospitalized for Toxicity High LV = Leucovorin 200 mg/m2, Low LV = Leucovorin 20 mg/m2
Any = percentage of patients reporting toxicity of any severity
Grade 3+ = percentage of patients reporting toxicity of Grade 3 or higher
(High LV)/5-FU
(N = 155)
(Low LV)/5-FU
(N = 161)
5-FU Alone
(N = 70)
Any
(%)
Grade 3+
(%)
Any
(%)
Grade 3+
(%)
Any
(%)
Grade 3+
(%)
Leukopenia
69
14
83
23
93
48
Thrombocytopenia
8
2
8
1
18
3
Infection
8
1
3
1
7
2
Nausea
74
10
80
9
60
6
Vomiting
46
8
44
9
40
7
Diarrhea
66
18
67
14
43
11
Stomatitis
75
27
84
29
59
16
Constipation
3
0
4
0
1
-
Lethargy/Malaise/Fatigue
13
3
12
2
6
3
Alopecia
42
5
43
6
37
7
Dermatitis
21
2
25
1
13
-
Anorexia
14
1
22
4
14
-
Hospitalization for Toxicity
5%
15%
7%
-
7 DRUG INTERACTIONS
7.1 Effects of Other Drugs on VYKOURA
Administer VYKOURA at least 2 hours before or 2 hours after the glucarpidase dose when administering concomitantly.
Glucarpidase can decrease leucovorin concentrations, which may decrease the effect of leucovorin rescue.
7.2 Effects of VYKOURA on Other Drugs
Increase monitoring for seizure activity in patients taking certain concomitant antiepileptic drugs.
Folic acid in high doses may reduce the effectiveness of certain antiepileptic drugs (e.g., phenobarbital, phenytoin, and primidone) and thereby increase the frequency of seizures. It is not known whether folinic acid, including VYKOURA, has the same effects; however, both folic and folinic acids, including VYKOURA share some common metabolic pathways.
Trimethoprim-Sulfamethoxazole
Avoid concomitant use of VYKOURA with trimethoprim-sulfamethoxazole. The effectiveness of trimethoprim-sulfamethoxazole can be decreased if used concomitantly with VYKOURA which was associated with increased rates of treatment failure and mortality in patients with HIV infection who receive trimethoprim-sulfamethoxazole for the acute treatment of Pneumocystis jirovecii pneumonia.
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Available data on the use of leucovorin during pregnancy have not identified a drug-associated risk of major birth defects, miscarriage, or adverse maternal or fetal outcomes.
Adequate animal reproduction studies have not been conducted with leucovorin.
Agents administered in combination with VYKOURA may cause fetal harm. Refer to the Prescribing Information for agents administered in combination with VYKOURA for additional information, as appropriate.
In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
8.2 Lactation
There are no available data on the presence of leucovorin in either human or animal milk, the effect on the breastfed infant, or on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for VYKOURA and any potential adverse effects on the breastfed infant from VYKOURA or from the underlying maternal condition.
Refer to the Prescribing Information for agents administered in combination with VYKOURA for breastfeeding recommendations, as appropriate.
8.4 Pediatric Use
VYKOURA is indicated to reduce the toxicity of MTX in pediatric patients with impaired MTX elimination, and folic acid antagonists or dihydrofolate reductase (DHFR) inhibitors following an overdose.
8.5 Geriatric Use
Clinical studies of leucovorin calcium did not show differences in safety or effectiveness between subjects over 65 and younger subjects. Other clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older patients cannot be ruled out. This drug is known to be excreted by the kidney and the risk of toxic reactions to the drug may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection in this patient population.
-
11 DESCRIPTION
Leucovorin is a folate analog, also known as folinic acid, Citrovorum factor, or 5-formyl-5,6,7,8-tetrahydrofolic acid calcium salt. This compound has the chemical designation of Calcium N-(p-((((6RS)-2-amino-5-formyl 5,6,7,8-tetrahydro-4-hydroxy-6-pteridinyl)methyl)amino)benzoyl)-L-glutamate (1:1). The structural formula of leucovorin calcium is:
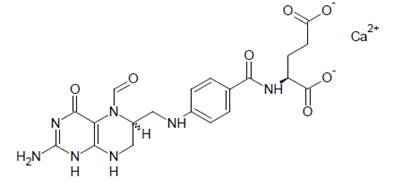
Leucovorin calcium is a white to light yellow crystalline powder with the molecular formula C20H21N7O7Ca and a molecular weight of 511.50 (calculated on the anhydrous basis).
VYKOURA (leucovorin calcium), for intravenous and intramuscular use, is supplied as a sterile, preservative-free, clear, colorless to yellow solution available in 50 mg/5 mL, 350 mg/35 mL and 500 mg/50 mL single-dose vials containing 10 mg/mL of leucovorin. Each mL contains 10.803 mg leucovorin calcium (equivalent to 10 mg leucovorin), 50 mg betadex sulfobutyl ether sodium, 4 mg sodium chloride, 7 mg tromethamine, and sodium hydroxide and/or hydrochloric acid for pH adjustment (pH 6.5 to 8.5).
There is 0.004 mEq of calcium per mg of leucovorin.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
High-Dose Methotrexate Therapy
Leucovorin is a mixture of the diastereoisomers of the 5-formyl derivative of tetrahydrofolic acid (THF). The biologically active compound of the mixture is the (-)-l isomer, known as Citrovorum factor or (-)-folinic acid. Leucovorin does not require reduction by the enzyme dihydrofolate reductase in order to participate in reactions utilizing folates as a source of "one-carbon" moieties. l-Leucovorin (l-5 formyltetrahydrofolate) is rapidly metabolized (via 5, 10-methenyltetrahydrofolate then 5, 10-methylenetetrahydrofolate) to l-5-methyltetrahydrofolate. L-5-methyltetrahydrofolate can in turn be metabolized via other pathways back to 5,10 methylenetetrahydrofolate, which is converted to 5-methyltetrahydrofolate by an irreversible, enzyme catalyzed reduction using the cofactors FADH2 and NADPH. Administration of leucovorin can counteract the therapeutic and toxic effects of folic acid antagonists such as methotrexate, which act by inhibiting dihydrofolate reductase.
Combination with Fluorouracil in Colorectal Cancer
Leucovorin can enhance the therapeutic and toxic effects of fluoropyrimidines used in cancer therapy, such as 5-fluorouracil. Concurrent administration of leucovorin does not appear to alter the plasma pharmacokinetics of 5-fluorouracil. 5-Fluorouracil is metabolized to fluorodeoxyuridylic acid, which binds to and inhibits the enzyme thymidylate synthase (an enzyme important in DNA repair and replication). Leucovorin is readily converted to another reduced folate, 5,10-methylenetetrahydrofolate, which acts to stabilize the binding of fluorodeoxyuridylic acid to thymidylate synthase and thereby enhances the inhibition of this enzyme.
12.2 Pharmacodynamics
Leucovorin exposure-response relationships and time course of pharmacodynamic response is not fully characterized.
12.3 Pharmacokinetics
Leucovorin pharmacokinetics were observed after a single intramuscular dose of 10 mg/m2 in healthy subjects and are presented as mean (CV%) unless otherwise specified. Leucovorin baseline-corrected maximum plasma concentration (Cmax) is 1,832 ng/mL (14%) and the total systemic exposure (AUC) is 23,043 ng*hr/mL (15%).
Absorption
Leucovorin median (min, max) time to maximum plasma concentration (Tmax) is 1.7 hours (0.7, 4.5).
Elimination
Leucovorin estimated terminal half-life is approximately 9.5 hours (CV 17%).
Metabolism
Leucovorin is rapidly metabolized (via 5, 10-methenyltetrahydrofolate then 5, 10-methylenetetrahydrofolate) to l,5-methyltetrahydrofolate. l,5-Methyltetrahydrofolate can be metabolized via other pathways back to 5,10-methylenetetrahydrofolate, which is converted to 5-methyltetrahydrofolate by an irreversible, enzyme catalyzed reduction using the cofactors FADH2 and NADPH.
- 13 NONCLINICAL TOXICOLOGY
-
16 HOW SUPPLIED/STORAGE AND HANDLING
VYKOURA (leucovorin calcium) injection is a clear, colorless to yellow color solution supplied in single-dose vial. Each carton contains one single-dose vial delivering 10 mg/mL leucovorin in the following strengths:
Strength
NDC Number
50 mg/5 mL (10 mg/mL)
83831-147-05
350 mg/35 mL (10 mg/mL)
83831-148-35
500 mg/50 mL (10 mg/mL)
83831-149-50
This container closure is not made with natural rubber latex.
Storage and Handling
Store in refrigerator at 2°C to 8°C (36°F to 46°F) in original carton to protect from light.
-
17 PATIENT COUNSELING INFORMATION
Advise patients of the following risks of VYKOURA:
Hypersensitivity Reactions
Inform patients that hypersensitivity reactions can occur with VYKOURA including anaphylactic reactions and urticaria. Inform patients about the signs and symptoms of hypersensitivity reactions and to contact their healthcare provider immediately if these occur during or after the administration of VYKOURA [see Warnings and Precautions (5.1)].
Hypercalcemia
Advise patients that hypercalcemia may occur with the use of VYKOURA and to report nausea, vomiting, headache and decreased alertness during or after the administration of VYKOURA. [see Warnings and Precautions (5.2)].
Drug Interactions
Advise patients to inform their health care providers of all concomitant drugs, including prescription drugs, nonprescription drugs, vitamins, and herbal products [see Drug Interactions (7)].
Manufactured for:
Avyxa Pharma, LLC
New Jersey 07054, USA
Made in Switzerland

-
PACKAGE LABEL.PRINCIPAL DISPLAY PANEL
VYKOURA (leucovorin) Injection, 50 mg/5 mL -Container Label

VYKOURA (leucovorin) Injection, 50 mg/5 mL -Carton Label
VYKOURA (leucovorin) Injection, 350 mg/35 mL -Container Label
VYKOURA (leucovorin) Injection, 350 mg/35 mL -Carton Label
VYKOURA (leucovorin) Injection, 500 mg/50 mL -Conatiner Label
VYKOURA (leucovorin) Injection, 500 mg/50 mL -Carton Label
-
INGREDIENTS AND APPEARANCE
VYKOURA
leucovorin calcium injectionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 83831-147 Route of Administration INTRAMUSCULAR, INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength LEUCOVORIN CALCIUM (UNII: RPR1R4C0P4) (LEUCOVORIN - UNII:Q573I9DVLP) LEUCOVORIN 50 mg in 5 mL Inactive Ingredients Ingredient Name Strength SODIUM CHLORIDE (UNII: 451W47IQ8X) TROMETHAMINE (UNII: 023C2WHX2V) BETADEX SULFOBUTYL ETHER SODIUM (UNII: 2PP9364507) SODIUM HYDROXIDE (UNII: 55X04QC32I) HYDROCHLORIC ACID (UNII: QTT17582CB) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 83831-147-05 1 in 1 CARTON 03/16/2026 1 5 mL in 1 VIAL, SINGLE-USE; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA220406 03/16/2026 VYKOURA
leucovorin calcium injectionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 83831-148 Route of Administration INTRAMUSCULAR, INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength LEUCOVORIN CALCIUM (UNII: RPR1R4C0P4) (LEUCOVORIN - UNII:Q573I9DVLP) LEUCOVORIN 350 mg in 35 mL Inactive Ingredients Ingredient Name Strength SODIUM CHLORIDE (UNII: 451W47IQ8X) TROMETHAMINE (UNII: 023C2WHX2V) BETADEX SULFOBUTYL ETHER SODIUM (UNII: 2PP9364507) SODIUM HYDROXIDE (UNII: 55X04QC32I) HYDROCHLORIC ACID (UNII: QTT17582CB) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 83831-148-35 1 in 1 CARTON 03/16/2026 1 35 mL in 1 VIAL, SINGLE-USE; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA220406 03/16/2026 VYKOURA
leucovorin calcium injectionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 83831-149 Route of Administration INTRAMUSCULAR, INTRAVENOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength LEUCOVORIN CALCIUM (UNII: RPR1R4C0P4) (LEUCOVORIN - UNII:Q573I9DVLP) LEUCOVORIN 500 mg in 50 mL Inactive Ingredients Ingredient Name Strength SODIUM CHLORIDE (UNII: 451W47IQ8X) TROMETHAMINE (UNII: 023C2WHX2V) BETADEX SULFOBUTYL ETHER SODIUM (UNII: 2PP9364507) SODIUM HYDROXIDE (UNII: 55X04QC32I) HYDROCHLORIC ACID (UNII: QTT17582CB) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 83831-149-50 1 in 1 CARTON 03/16/2026 1 50 mL in 1 VIAL, SINGLE-USE; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA220406 03/16/2026 Labeler - Avyxa Pharma, LLC (128918748) Registrant - Avyxa Holdings, LLC. (119187191)
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.