JANUMET- sitagliptin and metformin hydrochloride tablet, film coated
JANUMET by
Drug Labeling and Warnings
JANUMET by is a Prescription medication manufactured, distributed, or labeled by Merck Sharp & Dohme Corp.. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use JANUMET safely and effectively. See full prescribing information for JANUMET.
JANUMET® (sitagliptin and metformin hydrochloride) tablets, for oral use
Initial U.S. Approval: 2007WARNING: LACTIC ACIDOSIS
See full prescribing information for complete boxed warning.
- Postmarketing cases of metformin-associated lactic acidosis have resulted in death, hypothermia, hypotension, and resistant bradyarrhythmias. Symptoms included malaise, myalgias, respiratory distress, somnolence, and abdominal pain. Laboratory abnormalities included elevated blood lactate levels, anion gap acidosis, increased lactate/pyruvate ratio, and metformin plasma levels generally >5 mcg/mL. (5.1)
- Risk factors include renal impairment, concomitant use of certain drugs, age ≥65 years old, radiological studies with contrast, surgery and other procedures, hypoxic states, excessive alcohol intake, and hepatic impairment. Steps to reduce the risk of and manage metformin-associated lactic acidosis in these high risk groups are provided in the Full Prescribing Information. (5.1)
- If lactic acidosis is suspected, discontinue JANUMET and institute general supportive measures in a hospital setting. Prompt hemodialysis is recommended. (5.1)
INDICATIONS AND USAGE
JANUMET is a combination of sitagliptin, a dipeptidyl peptidase-4 (DPP-4) inhibitor, and metformin hydrochloride (HCl), a biguanide, indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus. (1)
Limitations of Use:DOSAGE AND ADMINISTRATION
- Individualize the starting dose of JANUMET based on the patient's current regimen. (2.1)
- Adjust the dosing based on effectiveness and tolerability while not exceeding the maximum recommended daily dose of 100 mg sitagliptin and 2000 mg metformin. (2.1)
- Give twice daily with meals, with gradual dose escalation, to reduce the gastrointestinal effects due to metformin. (2.1)
- Prior to initiation, assess renal function with estimated glomerular filtration rate (eGFR) (2.2)
- Do not use in patients with eGFR below 30 mL/min/1.73 m2.
- JANUMET is not recommended in patients with eGFR between 30 and less than 45 mL/min/1.73 m2.
- JANUMET may need to be discontinued at time of, or prior to, iodinated contrast imaging procedures. (2.3)
DOSAGE FORMS AND STRENGTHS
Tablets: 50 mg sitagliptin/500 mg metformin HCl and 50 mg sitagliptin/1000 mg metformin HCl (3)
CONTRAINDICATIONS
WARNINGS AND PRECAUTIONS
- Lactic acidosis: See boxed warning. (5.1)
- There have been postmarketing reports of acute pancreatitis, including fatal and non-fatal hemorrhagic or necrotizing pancreatitis. If pancreatitis is suspected, promptly discontinue JANUMET. (5.2)
- Heart failure has been observed with two other members of the DPP-4 inhibitor class. Consider risks and benefits of JANUMET in patients who have known risk factors for heart failure. Monitor patients for signs and symptoms. (5.3)
- There have been postmarketing reports of acute renal failure, sometimes requiring dialysis. Before initiating JANUMET and at least annually thereafter, assess renal function. (5.4)
- Vitamin B12 deficiency: Metformin may lower vitamin B12 levels. Measure hematologic parameters annually. (5.5)
- When used with an insulin secretagogue (e.g., sulfonylurea) or with insulin, a lower dose of the insulin secretagogue or insulin may be required to reduce the risk of hypoglycemia. (5.7)
- There have been postmarketing reports of serious allergic and hypersensitivity reactions in patients treated with sitagliptin (one of the components of JANUMET), such as anaphylaxis, angioedema, and exfoliative skin conditions including Stevens-Johnson syndrome. In such cases, promptly stop JANUMET, assess for other potential causes, institute appropriate monitoring and treatment, and initiate alternative treatment for diabetes. (5.9)
- Severe and disabling arthralgia has been reported in patients taking DPP-4 inhibitors. Consider as a possible cause for severe joint pain and discontinue drug if appropriate. (5.10)
- There have been postmarketing reports of bullous pemphigoid requiring hospitalization in patients taking DPP-4 inhibitors. Tell patients to report development of blisters or erosions. If bullous pemphigoid is suspected, discontinue JANUMET. (5.11)
- There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with JANUMET. (5.12)
ADVERSE REACTIONS
- The most common adverse reactions reported in ≥5% of patients simultaneously started on sitagliptin and metformin and more commonly than in patients treated with placebo were diarrhea, upper respiratory tract infection, and headache. (6.1)
- Adverse reactions reported in ≥5% of patients treated with sitagliptin in combination with sulfonylurea and metformin and more commonly than in patients treated with placebo in combination with sulfonylurea and metformin were hypoglycemia and headache. (6.1)
- Hypoglycemia was the only adverse reaction reported in ≥5% of patients treated with sitagliptin in combination with insulin and metformin and more commonly than in patients treated with placebo in combination with insulin and metformin. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., at 1-877-888-4231 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.DRUG INTERACTIONS
- Carbonic anhydrase inhibitors may increase risk of lactic acidosis. Consider more frequent monitoring. (7.1)
- Drugs that reduce metformin clearance (such as ranolazine, vandetanib, dolutegravir, and cimetidine) may increase the accumulation of metformin. Consider the benefits and risks of concomitant use. (7.2)
- Alcohol can potentiate the effect of metformin on lactate metabolism. Warn patients against excessive alcohol intake. (7.3)
USE IN SPECIFIC POPULATIONS
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide.
Revised: 8/2019
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
WARNING: LACTIC ACIDOSIS
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dosing
2.2 Recommendations for Use in Renal Impairment
2.3 Discontinuation for Iodinated Contrast Imaging Procedures
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Lactic Acidosis
5.2 Pancreatitis
5.3 Heart Failure
5.4 Assessment of Renal Function
5.5 Vitamin B12 Deficiency
5.6 Change in Clinical Status of Patients with Previously Controlled Type 2 Diabetes
5.7 Use with Medications Known to Cause Hypoglycemia
5.8 Loss of Control of Blood Glucose
5.9 Hypersensitivity Reactions
5.10 Severe and Disabling Arthralgia
5.11 Bullous Pemphigoid
5.12 Macrovascular Outcomes
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
6.2 Postmarketing Experience
7 DRUG INTERACTIONS
7.1 Carbonic Anhydrase Inhibitors
7.2 Drugs that Reduce Metformin Clearance
7.3 Alcohol
7.4 Insulin Secretagogues or Insulin
7.5 Use of Metformin with Other Drugs
7.6 Digoxin
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.3 Females and Males of Reproductive Potential
8.4 Pediatric Use
8.5 Geriatric Use
8.6 Renal Impairment
8.7 Hepatic Impairment
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- * Sections or subsections omitted from the full prescribing information are not listed.
-
BOXED WARNING
(What is this?)
WARNING: LACTIC ACIDOSIS
Postmarketing cases of metformin-associated lactic acidosis have resulted in death, hypothermia, hypotension, and resistant bradyarrhythmias. The onset of metformin-associated lactic acidosis is often subtle, accompanied only by nonspecific symptoms such as malaise, myalgias, respiratory distress, somnolence, and abdominal pain. Metformin-associated lactic acidosis was characterized by elevated blood lactate levels (>5 mmol/Liter), anion gap acidosis (without evidence of ketonuria or ketonemia), an increased lactate/pyruvate ratio, and metformin plasma levels generally >5 mcg/mL [see Warnings and Precautions (5.1)].
Risk factors for metformin-associated lactic acidosis include renal impairment, concomitant use of certain drugs (e.g., carbonic anhydrase inhibitors such as topiramate), age 65 years old or greater, having a radiological study with contrast, surgery and other procedures, hypoxic states (e.g., acute congestive heart failure), excessive alcohol intake, and hepatic impairment.
Steps to reduce the risk of and manage metformin-associated lactic acidosis in these high risk groups are provided in the full prescribing information [see Dosage and Administration (2.2), Contraindications (4), Warnings and Precautions (5.1), Drug Interactions (7), and Use in Specific Populations (8.6, 8.7)].
If metformin-associated lactic acidosis is suspected, immediately discontinue JANUMET and institute general supportive measures in a hospital setting. Prompt hemodialysis is recommended [see Warnings and Precautions (5.1)].
-
1 INDICATIONS AND USAGE
JANUMET is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus.
Limitations of Use
JANUMET should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis.
JANUMET has not been studied in patients with a history of pancreatitis. It is unknown whether patients with a history of pancreatitis are at increased risk for the development of pancreatitis while using JANUMET. [See Warnings and Precautions (5.2).]
-
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dosing
The dosage of JANUMET should be individualized on the basis of the patient's current regimen, effectiveness, and tolerability while not exceeding the maximum recommended daily dose of 100 mg sitagliptin and 2000 mg metformin hydrochloride (HCl). Initial combination therapy or maintenance of combination therapy should be individualized and left to the discretion of the health care provider.
JANUMET should generally be given twice daily with meals, with gradual dose escalation, to reduce the gastrointestinal (GI) side effects due to metformin. JANUMET must not be split or divided before swallowing.
The starting dose of JANUMET should be based on the patient's current regimen. JANUMET should be given twice daily with meals. The following doses are available:
50 mg sitagliptin/500 mg metformin HCl
50 mg sitagliptin/1000 mg metformin HCl.
The recommended starting dose in patients not currently treated with metformin is 50 mg sitagliptin/500 mg metformin HCl twice daily, with gradual dose escalation recommended to reduce gastrointestinal side effects associated with metformin.
The starting dose in patients already treated with metformin should provide sitagliptin dosed as 50 mg twice daily (100 mg total daily dose) and the dose of metformin already being taken. For patients taking metformin 850 mg twice daily, the recommended starting dose of JANUMET is 50 mg sitagliptin/1000 mg metformin HCl twice daily.
No studies have been performed specifically examining the safety and efficacy of JANUMET in patients previously treated with other oral antihyperglycemic agents and switched to JANUMET. Any change in therapy of type 2 diabetes should be undertaken with care and appropriate monitoring as changes in glycemic control can occur.
2.2 Recommendations for Use in Renal Impairment
Assess renal function prior to initiation of JANUMET and periodically thereafter.
JANUMET is contraindicated in patients with an estimated glomerular filtration rate (eGFR) below 30 mL/min/1.73 m2 [see Contraindications (4) and Warnings and Precautions (5.1)].
JANUMET is not recommended in patients with an eGFR between 30 and less than 45 mL/min/1.73 m2 because these patients require a lower dosage of sitagliptin than what is available in the fixed combination JANUMET product.
2.3 Discontinuation for Iodinated Contrast Imaging Procedures
Discontinue JANUMET at the time of, or prior to, an iodinated contrast imaging procedure in patients with an eGFR between 30 and 60 mL/min/1.73 m2; in patients with a history of liver disease, alcoholism, or heart failure; or in patients who will be administered intra-arterial iodinated contrast. Re-evaluate eGFR 48 hours after the imaging procedure; restart JANUMET if renal function is stable [see Warnings and Precautions (5.1)].
- 3 DOSAGE FORMS AND STRENGTHS
-
4 CONTRAINDICATIONS
JANUMET is contraindicated in patients with:
- Severe renal impairment (eGFR below 30 mL/min/1.73 m2) [see Warnings and Precautions (5.1)].
- Acute or chronic metabolic acidosis, including diabetic ketoacidosis. Diabetic ketoacidosis should be treated with insulin.
- History of a serious hypersensitivity reaction to JANUMET, sitagliptin, or metformin, such as anaphylaxis or angioedema. [See Warnings and Precautions (5.9); Adverse Reactions (6.2).]
-
5 WARNINGS AND PRECAUTIONS
5.1 Lactic Acidosis
There have been postmarketing cases of metformin-associated lactic acidosis, including fatal cases. These cases had a subtle onset and were accompanied by nonspecific symptoms such as malaise, myalgias, abdominal pain, respiratory distress, or increased somnolence; however, hypothermia, hypotension and resistant bradyarrhythmias have occurred with severe acidosis. Metformin-associated lactic acidosis was characterized by elevated blood lactate concentrations (>5 mmol/Liter), anion gap acidosis (without evidence of ketonuria or ketonemia), and an increased lactate/pyruvate ratio; metformin plasma levels were generally >5 mcg/mL. Metformin decreases liver uptake of lactate increasing lactate blood levels which may increase the risk of lactic acidosis, especially in patients at risk.
If metformin-associated lactic acidosis is suspected, general supportive measures should be instituted promptly in a hospital setting, along with immediate discontinuation of JANUMET. In JANUMET-treated patients with a diagnosis or strong suspicion of lactic acidosis, prompt hemodialysis is recommended to correct the acidosis and remove accumulated metformin (metformin HCl is dialyzable, with a clearance of up to 170 mL/min under good hemodynamic conditions). Hemodialysis has often resulted in reversal of symptoms and recovery.
Educate patients and their families about the symptoms of lactic acidosis and if these symptoms occur instruct them to discontinue JANUMET and report these symptoms to their health care provider.
For each of the known and possible risk factors for metformin-associated lactic acidosis, recommendations to reduce the risk of and manage metformin-associated lactic acidosis are provided below:
Renal Impairment
The postmarketing metformin-associated lactic acidosis cases primarily occurred in patients with significant renal impairment. The risk of metformin accumulation and metformin-associated lactic acidosis increases with the severity of renal impairment because metformin is substantially excreted by the kidney. Clinical recommendations based upon the patient's renal function include [see Dosage and Administration (2.2), Clinical Pharmacology (12.3)]:
- Before initiating JANUMET, obtain an estimated glomerular filtration rate (eGFR).
- JANUMET is contraindicated in patients with an eGFR below 30 mL/min/1.73 m2 [see Contraindications (4)].
- JANUMET is not recommended in patients with an eGFR between 30 and less than 45 mL/min/1.73 m2 because these patients require a lower dosage of sitagliptin than what is available in the fixed combination JANUMET product.
- Obtain an eGFR at least annually in all patients taking JANUMET. In patients at increased risk for the development of renal impairment (e.g., the elderly), renal function should be assessed more frequently.
Drug Interactions
The concomitant use of JANUMET with specific drugs may increase the risk of metformin-associated lactic acidosis: those that impair renal function, result in significant hemodynamic change, interfere with acid-base balance or increase metformin accumulation [see Drug Interactions (7)]. Therefore, consider more frequent monitoring of patients.
Age 65 or Greater
The risk of metformin-associated lactic acidosis increases with the patient's age because elderly patients have a greater likelihood of having hepatic, renal, or cardiac impairment than younger patients. Assess renal function more frequently in elderly patients [see Use in Specific Populations (8.5)].
Radiological Studies with Contrast
Administration of intravascular iodinated contrast agents in metformin-treated patients has led to an acute decrease in renal function and the occurrence of lactic acidosis. Stop JANUMET at the time of, or prior to, an iodinated contrast imaging procedure in patients with an eGFR between 30 and 60 mL/min/1.73 m2; in patients with a history of hepatic impairment, alcoholism, or heart failure; or in patients who will be administered intra-arterial iodinated contrast. Re-evaluate eGFR 48 hours after the imaging procedure, and restart JANUMET if renal function is stable.
Surgery and Other Procedures
Withholding of food and fluids during surgical or other procedures may increase the risk for volume depletion, hypotension and renal impairment. JANUMET should be temporarily discontinued while patients have restricted food and fluid intake.
Hypoxic States
Several of the postmarketing cases of metformin-associated lactic acidosis occurred in the setting of acute congestive heart failure (particularly when accompanied by hypoperfusion and hypoxemia). Cardiovascular collapse (shock), acute myocardial infarction, sepsis, and other conditions associated with hypoxemia have been associated with lactic acidosis and may also cause prerenal azotemia. When such events occur, discontinue JANUMET.
Excessive Alcohol Intake
Alcohol potentiates the effect of metformin on lactate metabolism and this may increase the risk of metformin-associated lactic acidosis. Warn patients against excessive alcohol intake while receiving JANUMET.
Hepatic Impairment
Patients with hepatic impairment have developed with cases of metformin-associated lactic acidosis. This may be due to impaired lactate clearance resulting in higher lactate blood levels. Therefore, avoid use of JANUMET in patients with clinical or laboratory evidence of hepatic disease.
5.2 Pancreatitis
There have been postmarketing reports of acute pancreatitis, including fatal and non-fatal hemorrhagic or necrotizing pancreatitis, in patients taking JANUMET. After initiation of JANUMET, patients should be observed carefully for signs and symptoms of pancreatitis. If pancreatitis is suspected, JANUMET should promptly be discontinued and appropriate management should be initiated. It is unknown whether patients with a history of pancreatitis are at increased risk for the development of pancreatitis while using JANUMET.
5.3 Heart Failure
An association between dipeptidyl peptidase-4 (DPP-4) inhibitor treatment and heart failure has been observed in cardiovascular outcomes trials for two other members of the DPP-4 inhibitor class. These trials evaluated patients with type 2 diabetes mellitus and atherosclerotic cardiovascular disease.
Consider the risks and benefits of JANUMET prior to initiating treatment in patients at risk for heart failure, such as those with a prior history of heart failure and a history of renal impairment, and observe these patients for signs and symptoms of heart failure during therapy. Advise patients of the characteristic symptoms of heart failure and to immediately report such symptoms. If heart failure develops, evaluate and manage according to current standards of care and consider discontinuation of JANUMET.
5.4 Assessment of Renal Function
Metformin and sitagliptin are known to be substantially excreted by the kidney.
Metformin HCl
JANUMET is contraindicated in patients with severe renal impairment [see Contraindications (4) and Warnings and Precautions (5.1)].
Sitagliptin
There have been postmarketing reports of worsening renal function, including acute renal failure, sometimes requiring dialysis. Before initiation of therapy with JANUMET and at least annually thereafter, renal function should be assessed. In patients in whom development of renal dysfunction is anticipated, particularly in elderly patients, renal function should be assessed more frequently and JANUMET discontinued if evidence of renal impairment is present.
5.5 Vitamin B12 Deficiency
In controlled clinical trials of metformin of 29 weeks duration, a decrease to subnormal levels of previously normal serum vitamin B12 levels was observed in approximately 7% of patients. Such decrease, possibly due to interference with B12 absorption from the B12-intrinsic factor complex, may be associated with anemia but appears to be rapidly reversible with discontinuation of metformin or vitamin B12 supplementation. Certain individuals (those with inadequate vitamin B12 or calcium intake or absorption) appear to be predisposed to developing subnormal vitamin B12 levels. Measure hematologic parameters on an annual basis and vitamin B12 measurements at 2- to 3-year intervals in patients on JANUMET and manage any abnormalities [see Adverse Reactions (6.1)].
5.6 Change in Clinical Status of Patients with Previously Controlled Type 2 Diabetes
A patient with type 2 diabetes previously well controlled on JANUMET who develops laboratory abnormalities or clinical illness (especially vague and poorly defined illness) should be evaluated promptly for evidence of ketoacidosis or lactic acidosis. Evaluation should include serum electrolytes and ketones, blood glucose and, if indicated, blood pH, lactate, pyruvate, and metformin levels. If acidosis of either form occurs, JANUMET must be stopped immediately and other appropriate corrective measures initiated.
5.7 Use with Medications Known to Cause Hypoglycemia
Sitagliptin
When sitagliptin was used in combination with a sulfonylurea or with insulin, medications known to cause hypoglycemia, the incidence of hypoglycemia was increased over that of placebo used in combination with a sulfonylurea or with insulin [see Adverse Reactions (6)]. Therefore, patients also receiving an insulin secretagogue (e.g., sulfonylurea) or insulin may require a lower dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemia [see Drug Interactions (7.4)].
Metformin HCl
Hypoglycemia does not occur in patients receiving metformin alone under usual circumstances of use, but could occur when caloric intake is deficient, when strenuous exercise is not compensated by caloric supplementation, or during concomitant use with other glucose-lowering agents (such as sulfonylureas and insulin) or ethanol. Elderly, debilitated, or malnourished patients, and those with adrenal or pituitary insufficiency or alcohol intoxication are particularly susceptible to hypoglycemic effects. Hypoglycemia may be difficult to recognize in the elderly, and in people who are taking β-adrenergic blocking drugs.
5.8 Loss of Control of Blood Glucose
When a patient stabilized on any diabetic regimen is exposed to stress such as fever, trauma, infection, or surgery, a temporary loss of glycemic control may occur. At such times, it may be necessary to withhold JANUMET and temporarily administer insulin. JANUMET may be reinstituted after the acute episode is resolved.
5.9 Hypersensitivity Reactions
There have been postmarketing reports of serious hypersensitivity reactions in patients treated with sitagliptin, one of the components of JANUMET. These reactions include anaphylaxis, angioedema, and exfoliative skin conditions including Stevens-Johnson syndrome. Onset of these reactions occurred within the first 3 months after initiation of treatment with sitagliptin, with some reports occurring after the first dose. If a hypersensitivity reaction is suspected, discontinue JANUMET, assess for other potential causes for the event, and institute alternative treatment for diabetes. [See Adverse Reactions (6.2).]
Angioedema has also been reported with other DPP-4 inhibitors. Use caution in a patient with a history of angioedema with another DPP-4 inhibitor because it is unknown whether such patients will be predisposed to angioedema with JANUMET.
5.10 Severe and Disabling Arthralgia
There have been postmarketing reports of severe and disabling arthralgia in patients taking DPP-4 inhibitors. The time to onset of symptoms following initiation of drug therapy varied from one day to years. Patients experienced relief of symptoms upon discontinuation of the medication. A subset of patients experienced a recurrence of symptoms when restarting the same drug or a different DPP-4 inhibitor. Consider DPP-4 inhibitors as a possible cause for severe joint pain and discontinue drug if appropriate.
5.11 Bullous Pemphigoid
Postmarketing cases of bullous pemphigoid requiring hospitalization have been reported with DPP-4 inhibitor use. In reported cases, patients typically recovered with topical or systemic immunosuppressive treatment and discontinuation of the DPP-4 inhibitor. Tell patients to report development of blisters or erosions while receiving JANUMET. If bullous pemphigoid is suspected, JANUMET should be discontinued and referral to a dermatologist should be considered for diagnosis and appropriate treatment.
-
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Sitagliptin and Metformin Coadministration in Patients with Type 2 Diabetes Inadequately Controlled on Diet and Exercise
Table 1 summarizes the most common (≥5% of patients) adverse reactions reported (regardless of investigator assessment of causality) in a 24-week placebo-controlled factorial study in which sitagliptin and metformin were coadministered to patients with type 2 diabetes inadequately controlled on diet and exercise.
Table 1: Sitagliptin and Metformin Coadministered to Patients with Type 2 Diabetes Inadequately Controlled on Diet and Exercise: Adverse Reactions Reported (Regardless of Investigator Assessment of Causality) in ≥5% of Patients Receiving Combination Therapy (and Greater than in Patients Receiving Placebo)* Number of Patients (%) Placebo Sitagliptin 100 mg once daily Metformin 500 mg/ Metformin 1000 mg twice daily† Sitagliptin 50 mg twice daily + Metformin 500 mg/ Metformin 1000 mg twice daily† N = 176 N = 179 N = 364† N = 372† - * Intent-to-treat population.
- † Data pooled for the patients given the lower and higher doses of metformin.
Diarrhea 7 (4.0) 5 (2.8) 28 (7.7) 28 (7.5) Upper Respiratory Tract Infection 9 (5.1) 8 (4.5) 19 (5.2) 23 (6.2) Headache 5 (2.8) 2 (1.1) 14 (3.8) 22 (5.9) Sitagliptin Add-on Therapy in Patients with Type 2 Diabetes Inadequately Controlled on Metformin Alone
In a 24-week placebo-controlled trial of sitagliptin 100 mg administered once daily added to a twice daily metformin regimen, there were no adverse reactions reported regardless of investigator assessment of causality in ≥5% of patients and more commonly than in patients given placebo. Discontinuation of therapy due to clinical adverse reactions was similar to the placebo treatment group (sitagliptin and metformin, 1.9%; placebo and metformin, 2.5%).
Gastrointestinal Adverse Reactions
The incidences of pre-selected gastrointestinal adverse experiences in patients treated with sitagliptin and metformin were similar to those reported for patients treated with metformin alone. See Table 2.
Table 2: Pre-selected Gastrointestinal Adverse Reactions (Regardless of Investigator Assessment of Causality) Reported in Patients with Type 2 Diabetes Receiving Sitagliptin and Metformin Number of Patients (%) Study of Sitagliptin and Metformin in Patients Inadequately Controlled on Diet and Exercise Study of Sitagliptin Add-on in Patients Inadequately Controlled on Metformin Alone
Placebo
Sitagliptin 100 mg once daily
Metformin 500 mg/ Metformin 1000 mg twice daily*Sitagliptin 50 mg twice daily + Metformin 500 mg/ Metformin 1000 mg twice daily* Placebo and Metformin ≥1500 mg daily Sitagliptin 100 mg once daily and Metformin ≥1500 mg daily N = 176 N = 179 N = 364 N = 372 N = 237 N = 464 - * Data pooled for the patients given the lower and higher doses of metformin.
- † Abdominal discomfort was included in the analysis of abdominal pain in the study of initial therapy.
Diarrhea 7 (4.0) 5 (2.8) 28 (7.7) 28 (7.5) 6 (2.5) 11 (2.4) Nausea 2 (1.1) 2 (1.1) 20 (5.5) 18 (4.8) 2 (0.8) 6 (1.3) Vomiting 1 (0.6) 0 (0.0) 2 (0.5) 8 (2.2) 2 (0.8) 5 (1.1) Abdominal Pain† 4 (2.3) 6 (3.4) 14 (3.8) 11 (3.0) 9 (3.8) 10 (2.2) Sitagliptin in Combination with Metformin and Glimepiride
In a 24-week placebo-controlled study of sitagliptin 100 mg as add-on therapy in patients with type 2 diabetes inadequately controlled on metformin and glimepiride (sitagliptin, N=116; placebo, N=113), the adverse reactions reported regardless of investigator assessment of causality in ≥5% of patients treated with sitagliptin and more commonly than in patients treated with placebo were: hypoglycemia (Table 3) and headache (6.9%, 2.7%).
Sitagliptin in Combination with Metformin and Rosiglitazone
In a placebo-controlled study of sitagliptin 100 mg as add-on therapy in patients with type 2 diabetes inadequately controlled on metformin and rosiglitazone (sitagliptin, N=181; placebo, N=97), the adverse reactions reported regardless of investigator assessment of causality through Week 18 in ≥5% of patients treated with sitagliptin and more commonly than in patients treated with placebo were: upper respiratory tract infection (sitagliptin, 5.5%; placebo, 5.2%) and nasopharyngitis (6.1%, 4.1%). Through Week 54, the adverse reactions reported regardless of investigator assessment of causality in ≥5% of patients treated with sitagliptin and more commonly than in patients treated with placebo were: upper respiratory tract infection (sitagliptin, 15.5%; placebo, 6.2%), nasopharyngitis (11.0%, 9.3%), peripheral edema (8.3%, 5.2%), and headache (5.5%, 4.1%).
Sitagliptin in Combination with Metformin and Insulin
In a 24-week placebo-controlled study of sitagliptin 100 mg as add-on therapy in patients with type 2 diabetes inadequately controlled on metformin and insulin (sitagliptin, N=229; placebo, N=233), the only adverse reaction reported regardless of investigator assessment of causality in ≥5% of patients treated with sitagliptin and more commonly than in patients treated with placebo was hypoglycemia (Table 3).
Hypoglycemia
In the above studies (N=5), adverse reactions of hypoglycemia were based on all reports of symptomatic hypoglycemia; a concurrent glucose measurement was not required although most (77%) reports of hypoglycemia were accompanied by a blood glucose measurement ≤70 mg/dL. When the combination of sitagliptin and metformin was coadministered with a sulfonylurea or with insulin, the percentage of patients reporting at least one adverse reaction of hypoglycemia was higher than that observed with placebo and metformin coadministered with a sulfonylurea or with insulin (Table 3).
Table 3: Incidence and Rate of Hypoglycemia* (Regardless of Investigator Assessment of Causality) in Placebo-Controlled Clinical Studies of Sitagliptin in Combination with Metformin Coadministered with Glimepiride or Insulin - * Adverse reactions of hypoglycemia were based on all reports of symptomatic hypoglycemia; a concurrent glucose measurement was not required: Intent-to-treat population.
- † Based on total number of events (i.e., a single patient may have had multiple events).
- ‡ Severe events of hypoglycemia were defined as those events requiring medical assistance or exhibiting depressed level/loss of consciousness or seizure.
Add-On to Glimepiride + Metformin (24 weeks) Sitagliptin 100 mg + Metformin + Glimepiride Placebo + Metformin + Glimepiride N = 116 N = 113 Overall (%) 19 (16.4) 1 (0.9) Rate (episodes/patient-year)† 0.82 0.02 Severe (%)‡ 0 (0.0) 0 (0.0) Add-On to Insulin + Metformin (24 weeks) Sitagliptin 100 mg + Metformin + Insulin Placebo + Metformin + Insulin N = 229 N = 233 Overall (%) 35 (15.3) 19 (8.2) Rate (episodes/patient-year)† 0.98 0.61 Severe (%)‡ 1 (0.4) 1 (0.4) The overall incidence of reported adverse reactions of hypoglycemia in patients with type 2 diabetes inadequately controlled on diet and exercise was 0.6% in patients given placebo, 0.6% in patients given sitagliptin alone, 0.8% in patients given metformin alone, and 1.6% in patients given sitagliptin in combination with metformin. In patients with type 2 diabetes inadequately controlled on metformin alone, the overall incidence of adverse reactions of hypoglycemia was 1.3% in patients given add-on sitagliptin and 2.1% in patients given add-on placebo.
In the study of sitagliptin and add-on combination therapy with metformin and rosiglitazone, the overall incidence of hypoglycemia was 2.2% in patients given add-on sitagliptin and 0.0% in patients given add-on placebo through Week 18. Through Week 54, the overall incidence of hypoglycemia was 3.9% in patients given add-on sitagliptin and 1.0% in patients given add-on placebo.
In an additional, 30-week placebo-controlled, study of patients with type 2 diabetes inadequately controlled with metformin comparing the maintenance of sitagliptin 100 mg versus withdrawal of sitagliptin when initiating basal insulin therapy, the event rate and incidence of documented symptomatic hypoglycemia (blood glucose measurement ≤70 mg/dL) did not differ between the sitagliptin and placebo groups.
Vital Signs and Electrocardiograms
With the combination of sitagliptin and metformin, no clinically meaningful changes in vital signs or in ECG (including in QTc interval) were observed.
Pancreatitis
In a pooled analysis of 19 double-blind clinical trials that included data from 10,246 patients randomized to receive sitagliptin 100 mg/day (N=5429) or corresponding (active or placebo) control (N=4817), the incidence of acute pancreatitis was 0.1 per 100 patient-years in each group (4 patients with an event in 4708 patient-years for sitagliptin and 4 patients with an event in 3942 patient-years for control). [See Warnings and Precautions (5.2).]
Sitagliptin
The most common adverse experience in sitagliptin monotherapy reported regardless of investigator assessment of causality in ≥5% of patients and more commonly than in patients given placebo was nasopharyngitis.
Metformin HCl
The most common (>5%) established adverse reactions due to initiation of metformin therapy are diarrhea, nausea/vomiting, flatulence, abdominal discomfort, indigestion, asthenia, and headache.
Laboratory Tests
Sitagliptin
The incidence of laboratory adverse reactions was similar in patients treated with sitagliptin and metformin (7.6%) compared to patients treated with placebo and metformin (8.7%). In most but not all studies, a small increase in white blood cell count (approximately 200 cells/microL difference in WBC vs placebo; mean baseline WBC approximately 6600 cells/microL) was observed due to a small increase in neutrophils. This change in laboratory parameters is not considered to be clinically relevant.
Metformin HCl
In controlled clinical trials of metformin of 29 weeks duration, a decrease to subnormal levels of previously normal serum vitamin B12 levels, without clinical manifestations, was observed in approximately 7% of patients. Such decrease, possibly due to interference with B12 absorption from the B12-intrinsic factor complex, is, however, very rarely associated with anemia and appears to be rapidly reversible with discontinuation of metformin or vitamin B12 supplementation. [See Warnings and Precautions (5.5).]
6.2 Postmarketing Experience
Additional adverse reactions have been identified during postapproval use of JANUMET, sitagliptin, or metformin. Because these reactions are reported voluntarily from a population of uncertain size, it is generally not possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Hypersensitivity reactions including anaphylaxis, angioedema, rash, urticaria, cutaneous vasculitis, and exfoliative skin conditions including Stevens-Johnson syndrome [see Warnings and Precautions (5.9)]; upper respiratory tract infection; hepatic enzyme elevations; acute pancreatitis, including fatal and non-fatal hemorrhagic and necrotizing pancreatitis [see Indications and Usage (1); Warnings and Precautions (5.2)]; worsening renal function, including acute renal failure (sometimes requiring dialysis) [see Warnings and Precautions (5.4)]; severe and disabling arthralgia [see Warnings and Precautions (5.10)]; bullous pemphigoid [see Warnings and Precautions (5.11)]; constipation; vomiting; headache; myalgia; pain in extremity; back pain; pruritus; mouth ulceration; stomatitis; cholestatic, hepatocellular, and mixed hepatocellular liver injury; rhabdomyolysis.
-
7 DRUG INTERACTIONS
7.1 Carbonic Anhydrase Inhibitors
Topiramate or other carbonic anhydrase inhibitors (e.g., zonisamide, acetazolamide or dichlorphenamide) frequently cause a decrease in serum bicarbonate and induce non-anion gap, hyperchloremic metabolic acidosis. Concomitant use of these drugs with JANUMET may increase the risk of lactic acidosis. Consider more frequent monitoring of these patients.
7.2 Drugs that Reduce Metformin Clearance
Concomitant use of drugs that interfere with common renal tubular transport systems involved in the renal elimination of metformin (e.g., organic cationic transporter-2 [OCT2] / multidrug and toxin extrusion [MATE] inhibitors such as ranolazine, vandetanib, dolutegravir, and cimetidine) could increase systemic exposure to metformin and may increase the risk for lactic acidosis [see Clinical Pharmacology (12.3)]. Consider the benefits and risks of concomitant use.
7.3 Alcohol
Alcohol is known to potentiate the effect of metformin on lactate metabolism. Warn patients against excessive alcohol intake while receiving JANUMET.
7.4 Insulin Secretagogues or Insulin
Coadministration of JANUMET with an insulin secretagogue (e.g., sulfonylurea) or insulin may require lower doses of the insulin secretagogue or insulin to reduce the risk of hypoglycemia. [See Warnings and Precautions (5.7).]
7.5 Use of Metformin with Other Drugs
Certain drugs tend to produce hyperglycemia and may lead to loss of glycemic control. These drugs include the thiazides and other diuretics, corticosteroids, phenothiazines, thyroid products, estrogens, oral contraceptives, phenytoin, nicotinic acid, sympathomimetics, calcium channel blocking drugs, and isoniazid. When such drugs are administered to a patient receiving JANUMET the patient should be closely observed to maintain adequate glycemic control.
7.6 Digoxin
There was a slight increase in the area under the curve (AUC, 11%) and mean peak drug concentration (Cmax, 18%) of digoxin with the coadministration of 100 mg sitagliptin for 10 days. Patients receiving digoxin should be monitored appropriately. No dosage adjustment of digoxin or JANUMET is recommended.
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Exposure Registry
There is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to JANUMET during pregnancy. Health care providers are encouraged to report any prenatal exposure to JANUMET by calling the Pregnancy Registry at 1-800-986-8999.
Risk Summary
The limited available data with JANUMET in pregnant women are not sufficient to inform a drug-associated risk for major birth defects and miscarriage. Published studies with metformin use during pregnancy have not reported a clear association with metformin and major birth defect or miscarriage risk [see Data]. There are risks to the mother and fetus associated with poorly controlled diabetes in pregnancy [see Clinical Considerations]. No adverse developmental effects were observed when sitagliptin was administered to pregnant rats and rabbits during organogenesis at oral doses up to 30-times and 20-times, respectively, the 100 mg clinical dose, based on AUC. No adverse developmental effects were observed when metformin was administered to pregnant Sprague Dawley rats and rabbits during organogenesis at doses up to 2- and 6-times, respectively, a 2000 mg clinical dose, based on body surface area [see Data].
The estimated background risk of major birth defects is 6-10% in women with pre-gestational diabetes with a Hemoglobin A1c >7% and has been reported to be as high as 20-25% in women with a Hemoglobin A1c >10%. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2-4% and 15-20% respectively.
Disease-Associated Maternal and/or Embryo/Fetal Risk
Poorly controlled diabetes in pregnancy increases the maternal risk for diabetic ketoacidosis, pre-eclampsia, spontaneous abortions, preterm delivery, and delivery complications. Poorly controlled diabetes increases the fetal risk for major birth defects, still birth, and macrosomia related morbidity.
Human Data
Published data from post-marketing studies do not report a clear association with metformin and major birth defects, miscarriage, or adverse maternal or fetal outcomes when metformin is used during pregnancy. However, these studies cannot definitely establish the absence of any risk because of methodological limitations, including small sample size and inconsistent comparator groups.
Animal Data
Sitagliptin and Metformin
No animal reproduction studies were conducted with the coadministration of sitagliptin and metformin.
Sitagliptin
In embryo-fetal development studies, sitagliptin administered to pregnant rats and rabbits during organogenesis (gestation day 6 to 20) did not adversely affect developmental outcomes at oral doses up to 250 mg/kg (30-times the 100 mg clinical dose) and 125 mg/kg (20-times the 100 mg clinical dose), respectively, based on AUC. Higher doses in rats associated with maternal toxicity increased the incidence of rib malformations in offspring at 1000 mg/kg, or approximately 100-times the clinical dose, based on AUC. Placental transfer of sitagliptin was observed in pregnant rats and rabbits.
Sitagliptin administered to female rats from gestation day 6 to lactation day 21 caused no functional or behavioral toxicity in offspring of rats at doses up to 1000 mg/kg.
Metformin HCl
Metformin HCl did not cause adverse developmental effects when administered to pregnant Sprague Dawley rats and rabbits up to 600 mg/kg/day during the period of organogenesis. This represents an exposure of about 2- and 6-times a 2000 mg clinical dose based on body surface area (mg/m2) for rats and rabbits, respectively.
8.2 Lactation
Risk Summary
JANUMET
There is no information regarding the presence of JANUMET in human milk, the effects on the breastfed infant, or the effects on milk production. Limited published studies report that metformin is present in human milk [see Data]. There are no reports of adverse effects on breastfed infants exposed to metformin. There is no information on the effects of metformin on milk production. Sitagliptin is present in rat milk and therefore possibly present in human milk [see Data]. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for JANUMET and any potential adverse effects on the breastfed infant from JANUMET or from the underlying maternal condition.
Metformin HCl
Published clinical lactation studies report that metformin is present in human milk, which resulted in infant doses approximately 0.11% to 1% of the maternal weight-adjusted dosage and a milk/plasma ratio ranging between 0.13 and 1. However, the studies were not designed to definitely establish the risk of use of metformin during lactation because of small sample size and limited adverse event data collected in infants.
8.3 Females and Males of Reproductive Potential
Discuss the potential for unintended pregnancy with premenopausal women as therapy with metformin may result in ovulation in some anovulatory women.
8.4 Pediatric Use
Safety and effectiveness of JANUMET in pediatric patients under 18 years have not been established.
8.5 Geriatric Use
JANUMET
Because sitagliptin and metformin are substantially excreted by the kidney, and because aging can be associated with reduced renal function, renal function should be assessed more frequently in elderly patients. [See Warnings and Precautions (5.1, 5.4); Clinical Pharmacology (12.3).]
Sitagliptin
Of the total number of subjects (N=3884) in Phase II and III clinical studies of sitagliptin, 725 patients were 65 years and over, while 61 patients were 75 years and over. No overall differences in safety or effectiveness were observed between subjects 65 years and over and younger subjects. While this and other reported clinical experience have not identified differences in responses between the elderly and younger patients, greater sensitivity of some older individuals cannot be ruled out.
Metformin HCl
Controlled clinical studies of metformin did not include sufficient numbers of elderly patients to determine whether they respond differently from younger patients, although other reported clinical experience has not identified differences in responses between the elderly and young patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy and the higher risk of lactic acidosis. Assess renal function more frequently in elderly patients. [See Contraindications (4); Warnings and Precautions (5.1); Clinical Pharmacology (12.3).]
8.6 Renal Impairment
JANUMET
JANUMET is not recommended in patients with an eGFR between 30 and less than 45 mL/min/1.73 m2 because these patients require a lower dosage of sitagliptin than what is available in the fixed dose combination JANUMET product. JANUMET is contraindicated in severe renal impairment, patients with an eGFR below 30 mL/min/1.73 m2. [See Dosage and Administration (2.2), Contraindications (4), Warnings and Precautions (5.1) and Clinical Pharmacology (12.3).]
8.7 Hepatic Impairment
Use of metformin in patients with hepatic impairment has been associated with some cases of lactic acidosis. JANUMET is not recommended in patients with hepatic impairment. [See Warnings and Precautions (5.1).]
-
10 OVERDOSAGE
In the event of overdose with JANUMET, contact the Poison Control Center.
In the event of an overdose, it is reasonable to employ supportive measures, e.g., remove unabsorbed material from the gastrointestinal tract, employ clinical monitoring (including obtaining an electrocardiogram), and institute supportive therapy as indicated by the patient's clinical status.
Sitagliptin is modestly dialyzable. In clinical studies, approximately 13.5% of the dose was removed over a 3- to 4-hour hemodialysis session. Prolonged hemodialysis may be considered if clinically appropriate. It is not known if sitagliptin is dialyzable by peritoneal dialysis.
Overdose of metformin HCl has occurred, including ingestion of amounts greater than 50 grams. Hypoglycemia was reported in approximately 10% of cases, but no causal association with metformin HCl has been established. Lactic acidosis has been reported in approximately 32% of metformin overdose cases [see Warnings and Precautions (5.1)]. Metformin is dialyzable with a clearance of up to 170 mL/min under good hemodynamic conditions. Therefore, hemodialysis may be useful for removal of accumulated drug from patients in whom metformin overdosage is suspected.
-
11 DESCRIPTION
JANUMET (sitagliptin and metformin HCl) tablets contain two oral antihyperglycemic drugs: sitagliptin and metformin HCl.
Sitagliptin
Sitagliptin is an orally-active inhibitor of the dipeptidyl peptidase-4 (DPP-4) enzyme. Sitagliptin is present in JANUMET tablets in the form of sitagliptin phosphate monohydrate. Sitagliptin phosphate monohydrate is described chemically as 7-[(3R)-3-amino-1-oxo-4-(2,4,5-trifluorophenyl)butyl]-5,6,7,8-tetrahydro-3-(trifluoromethyl)-1,2,4-triazolo[4,3-a]pyrazine phosphate (1:1) monohydrate with an empirical formula of C16H15F6N5O∙H3PO4∙H2O and a molecular weight of 523.32. The structural formula is:
Sitagliptin phosphate monohydrate is a white to off-white, crystalline, non-hygroscopic powder. It is soluble in water and N,N-dimethyl formamide; slightly soluble in methanol; very slightly soluble in ethanol, acetone, and acetonitrile; and insoluble in isopropanol and isopropyl acetate.
Metformin HCl
Metformin HCl (N,N-dimethylimidodicarbonimidic diamide hydrochloride) is not chemically or pharmacologically related to any other classes of oral antihyperglycemic agents. Metformin HCl is a white to off-white crystalline compound with a molecular formula of C4H11N5∙HCl and a molecular weight of 165.63. Metformin HCl is freely soluble in water and is practically insoluble in acetone, ether, and chloroform. The pKa of metformin is 12.4. The pH of a 1% aqueous solution of metformin HCl is 6.68. The structural formula is as shown:
JANUMET
JANUMET is available as film-coated tablets containing:
- 64.25 mg sitagliptin monohydrate equivalent to 50 mg of sitagliptin and 389.93 mg of metformin equivalent to 500 mg metformin HCl (JANUMET 50/500).
- 64.25 mg sitagliptin monohydrate equivalent to 50 mg of sitagliptin and 779.86 mg of metformin equivalent to 1000 mg metformin HCl (JANUMET 50/1000).
Each film-coated tablet of JANUMET contains the following inactive ingredients: microcrystalline cellulose, polyvinylpyrrolidone, sodium lauryl sulfate, and sodium stearyl fumarate. In addition, the film coating contains the following inactive ingredients: polyvinyl alcohol, polyethylene glycol, talc, titanium dioxide, red iron oxide, and black iron oxide.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
JANUMET
JANUMET combines two antihyperglycemic agents with complementary mechanisms of action to improve glycemic control in patients with type 2 diabetes mellitus: sitagliptin, a dipeptidyl peptidase-4 (DPP-4) inhibitor, and metformin HCl, a member of the biguanide class.
Sitagliptin
Sitagliptin is a DPP-4 inhibitor, which is believed to exert its actions in patients with type 2 diabetes by slowing the inactivation of incretin hormones. Concentrations of the active intact hormones are increased by sitagliptin, thereby increasing and prolonging the action of these hormones. Incretin hormones, including glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP), are released by the intestine throughout the day, and levels are increased in response to a meal. These hormones are rapidly inactivated by the enzyme DPP-4. The incretins are part of an endogenous system involved in the physiologic regulation of glucose homeostasis. When blood glucose concentrations are normal or elevated, GLP-1 and GIP increase insulin synthesis and release from pancreatic beta cells by intracellular signaling pathways involving cyclic AMP. GLP-1 also lowers glucagon secretion from pancreatic alpha cells, leading to reduced hepatic glucose production. By increasing and prolonging active incretin levels, sitagliptin increases insulin release and decreases glucagon levels in the circulation in a glucose-dependent manner. Sitagliptin demonstrates selectivity for DPP-4 and does not inhibit DPP-8 or DPP-9 activity in vitro at concentrations approximating those from therapeutic doses.
Metformin HCl
Metformin is an antihyperglycemic agent which improves glucose tolerance in patients with type 2 diabetes mellitus, lowering both basal and postprandial plasma glucose. Metformin decreases hepatic glucose production, decreases intestinal absorption of glucose, and improves insulin sensitivity by increasing peripheral glucose uptake and utilization. With metformin therapy, insulin secretion remains unchanged while fasting insulin levels and day-long plasma insulin response may decrease.
12.2 Pharmacodynamics
Sitagliptin
In patients with type 2 diabetes mellitus, administration of sitagliptin led to inhibition of DPP-4 enzyme activity for a 24-hour period. After an oral glucose load or a meal, this DPP-4 inhibition resulted in a 2- to 3-fold increase in circulating levels of active GLP-1 and GIP, decreased glucagon concentrations, and increased responsiveness of insulin release to glucose, resulting in higher C-peptide and insulin concentrations. The rise in insulin with the decrease in glucagon was associated with lower fasting glucose concentrations and reduced glucose excursion following an oral glucose load or a meal.
In studies with healthy subjects, sitagliptin did not lower blood glucose or cause hypoglycemia.
Sitagliptin and Metformin HCl Coadministration
In a two-day study in healthy subjects, sitagliptin alone increased active GLP-1 concentrations, whereas metformin alone increased active and total GLP-1 concentrations to similar extents. Coadministration of sitagliptin and metformin had an additive effect on active GLP-1 concentrations. Sitagliptin, but not metformin, increased active GIP concentrations. It is unclear what these findings mean for changes in glycemic control in patients with type 2 diabetes mellitus.
Cardiac Electrophysiology
In a randomized, placebo-controlled crossover study, 79 healthy subjects were administered a single oral dose of sitagliptin 100 mg, sitagliptin 800 mg (8 times the recommended dose), and placebo. At the recommended dose of 100 mg, there was no effect on the QTc interval obtained at the peak plasma concentration, or at any other time during the study. Following the 800-mg dose, the maximum increase in the placebo-corrected mean change in QTc from baseline at 3 hours postdose was 8.0 msec. This increase is not considered to be clinically significant. At the 800-mg dose, peak sitagliptin plasma concentrations were approximately 11 times higher than the peak concentrations following a 100-mg dose.
In patients with type 2 diabetes mellitus administered sitagliptin 100 mg (N=81) or sitagliptin 200 mg (N=63) daily, there were no meaningful changes in QTc interval based on ECG data obtained at the time of expected peak plasma concentration.
12.3 Pharmacokinetics
Sitagliptin
The pharmacokinetics of sitagliptin have been extensively characterized in healthy subjects and patients with type 2 diabetes mellitus. Following a single oral 100-mg dose to healthy volunteers, mean plasma AUC of sitagliptin was 8.52 µM∙hr, Cmax was 950 nM, and apparent terminal half-life (t1/2) was 12.4 hours. Plasma AUC of sitagliptin increased in a dose-proportional manner and increased approximately 14% following 100 mg doses at steady-state compared to the first dose. The intra-subject and inter-subject coefficients of variation for sitagliptin AUC were small (5.8% and 15.1%). The pharmacokinetics of sitagliptin was generally similar in healthy subjects and in patients with type 2 diabetes mellitus.
Absorption
Sitagliptin
After oral administration of a 100 mg dose to healthy subjects, sitagliptin was rapidly absorbed with peak plasma concentrations (median Tmax) occurring 1 to 4 hours postdose. The absolute bioavailability of sitagliptin is approximately 87%.
Metformin HCl
The absolute bioavailability of a metformin HCl 500-mg tablet given under fasting conditions is approximately 50-60%. Studies using single oral doses of metformin HCl tablets 500 mg to 1,500 mg, and 850 mg to 2,550 mg (approximately 1.3 times the maximum recommended daily dosage), indicate that there is a lack of dose proportionality with increasing doses, which is due to decreased absorption rather than an alteration in elimination.
Effect of Food
Food decreases the extent of and slightly delays the absorption of metformin, as shown by approximately a 40% lower mean peak plasma concentration (Cmax), a 25% lower area under the plasma concentration versus time curve (AUC), and a 35-minute prolongation of time to peak plasma concentration (Tmax) following administration of a single 850-mg tablet of metformin with food, compared to the same tablet strength administered fasting. The clinical relevance of these decreases is unknown.
Distribution
Sitagliptin
The mean volume of distribution at steady state following a single 100-mg intravenous dose of sitagliptin to healthy subjects is approximately 198 liters. The fraction of sitagliptin reversibly bound to plasma proteins is low (38%).
Metformin HCl
The apparent volume of distribution (V/F) of metformin following single oral doses of metformin HCl tablets 850 mg averaged 654 ± 358 L. Metformin is negligibly bound to plasma proteins, in contrast to sulfonylureas, which are more than 90% protein bound. Metformin partitions into erythrocytes, most likely as a function of time. At usual clinical doses and dosing schedules of metformin HCl tablets, steady-state plasma concentrations of metformin are reached within 24-48 hours and are generally <1 mcg/mL.
Elimination
Sitagliptin
Approximately 79% of sitagliptin is excreted unchanged in the urine with metabolism being a minor pathway of elimination. The apparent terminal t1/2 following a 100 mg oral dose of sitagliptin was approximately 12.4 hours and renal clearance was approximately 350 mL/min.
Metformin HCl
Following oral administration, approximately 90% of the absorbed drug is eliminated via the renal route within the first 24 hours, with a plasma elimination half-life of approximately 6.2 hours. In blood, the elimination half-life is approximately 17.6 hours, suggesting that the erythrocyte mass may be a compartment of distribution.
Metabolism
Sitagliptin
Following a [14C]sitagliptin oral dose, approximately 16% of the radioactivity was excreted as metabolites of sitagliptin. Six metabolites were detected at trace levels and are not expected to contribute to the plasma DPP-4 inhibitory activity of sitagliptin. In vitro studies indicated that the primary enzyme responsible for the limited metabolism of sitagliptin was CYP3A4, with contribution from CYP2C8.
Excretion
Sitagliptin
Following administration of an oral [14C]sitagliptin dose to healthy subjects, approximately 100% of the administered radioactivity was eliminated in feces (13%) or urine (87%) within one week of dosing.
Elimination of sitagliptin occurs primarily via renal excretion and involves active tubular secretion. Sitagliptin is a substrate for human organic anion transporter-3 (hOAT-3), which may be involved in the renal elimination of sitagliptin. The clinical relevance of hOAT-3 in sitagliptin transport has not been established. Sitagliptin is also a substrate of p-glycoprotein (P-gp), which may also be involved in mediating the renal elimination of sitagliptin. However, cyclosporine, a P-gp inhibitor, did not reduce the renal clearance of sitagliptin.
Specific Populations
Patients with Renal Impairment
JANUMET
Studies characterizing the pharmacokinetics of sitagliptin and metformin after administration of JANUMET in renally impaired patients have not been performed [see Dosage and Administration (2.2)].
Sitagliptin
An approximately 2-fold increase in the plasma AUC of sitagliptin was observed in patients with moderate renal impairment with eGFR of 30 to less than 45 mL/min/1.73 m2, and an approximately 4-fold increase was observed in patients with severe renal impairment including patients with end-stage renal disease (ESRD) on hemodialysis, as compared to normal healthy control subjects. [See Dosage and Administration (2.2).]
Metformin HCl
In patients with decreased renal function, the plasma and blood half-life of metformin is prolonged and the renal clearance is decreased [see Contraindications (4); Warnings and Precautions (5.1)].
Patients with Hepatic Impairment
JANUMET
Studies characterizing the pharmacokinetics of sitagliptin and metformin after administration of JANUMET in patients with hepatic impairment have not been performed.
Sitagliptin
In patients with moderate hepatic impairment (Child-Pugh score 7 to 9), mean AUC and Cmax of sitagliptin increased approximately 21% and 13%, respectively, compared to healthy matched controls following administration of a single 100-mg dose of sitagliptin. These differences are not considered to be clinically meaningful. There is no clinical experience in patients with severe hepatic impairment (Child-Pugh score >9) [see Use in Specific Populations (8.7)].
Effects of Age, Body Mass Index (BMI), Gender, and Race
Sitagliptin
Based on a population pharmacokinetic analysis or a composite analysis of available pharmacokinetic data, BMI, gender, and race do not have a clinically meaningful effect on the pharmacokinetics of sitagliptin. When the effects of age on renal function are taken into account, age alone did not have a clinically meaningful impact on the pharmacokinetics of sitagliptin based on a population pharmacokinetic analysis. Elderly subjects (65 to 80 years) had approximately 19% higher plasma concentrations of sitagliptin compared to younger subjects.
Metformin HCl
Limited data from controlled pharmacokinetic studies of metformin in healthy elderly subjects suggest that total plasma clearance of metformin is decreased, the half-life is prolonged, and Cmax is increased, compared to healthy young subjects. From these data, it appears that the change in metformin pharmacokinetics with aging is primarily accounted for by a change in renal function.
Metformin pharmacokinetic parameters did not differ significantly between normal subjects and patients with type 2 diabetes mellitus when analyzed according to gender. Similarly, in controlled clinical studies in patients with type 2 diabetes mellitus, the antihyperglycemic effect of metformin was comparable in males and females.
No studies of metformin pharmacokinetic parameters according to race have been performed. In controlled clinical studies of metformin in patients with type 2 diabetes mellitus, the antihyperglycemic effect was comparable in Whites (n=249), Blacks (n=51), and Hispanics (n=24).
Drug Interaction Studies
JANUMET
Coadministration of multiple doses of sitagliptin (50 mg) and metformin (1000 mg) given twice daily did not meaningfully alter the pharmacokinetics of either sitagliptin or metformin in patients with type 2 diabetes.
Pharmacokinetic drug interaction studies with JANUMET have not been performed; however, such studies have been conducted with the individual components of JANUMET (sitagliptin and metformin HCl).
Sitagliptin
In Vitro Assessment of Drug Interactions
Sitagliptin is not an inhibitor of CYP isozymes CYP3A4, 2C8, 2C9, 2D6, 1A2, 2C19 or 2B6, and is not an inducer of CYP3A4. Sitagliptin is a P-gp substrate but does not inhibit P-gp mediated transport of digoxin. Based on these results, sitagliptin is considered unlikely to cause interactions with other drugs that utilize these pathways.
Sitagliptin is not extensively bound to plasma proteins. Therefore, the propensity of sitagliptin to be involved in clinically meaningful drug-drug interactions mediated by plasma protein binding displacement is very low.
In Vivo Assessment of Drug Interactions
Effects of Sitagliptin on Other Drugs
In clinical studies, sitagliptin did not meaningfully alter the pharmacokinetics of metformin, glyburide, simvastatin, rosiglitazone, digoxin, warfarin, or an oral contraception (ethinyl estradiol and norethindrone) (Table 4), providing in vivo evidence of a low propensity for causing drug interactions with substrates of CYP3A4, CYP2C8, CYP2C9, P-gp, and organic cationic transporter (OCT).
Table 4: Effect of Sitagliptin on Systemic Exposure of Coadministered Drugs Coadministered Drug Dose of Coadministered Drug* Dose of Sitagliptin* Geometric Mean Ratio
(ratio with/without sitagliptin)
No Effect = 1.00AUC† Cmax - * All doses administered as single dose unless otherwise specified.
- † AUC is reported as AUC0-∞ unless otherwise specified.
- ‡ Multiple dose.
- § AUC0-24hr.
- ¶ AUC0-last.
- # AUC0-12hr.
Digoxin 0.25 mg‡ once daily for 10 days 100 mg‡ once daily for 10 days Digoxin 1.11§ 1.18 Glyburide 1.25 mg 200 mg‡ once daily for 6 days Glyburide 1.09 1.01 Simvastatin 20 mg 200 mg‡ once daily for 5 days Simvastatin 0.85¶ 0.80 Simvastatin Acid 1.12¶ 1.06 Rosiglitazone 4 mg 200 mg‡ once daily for 5 days Rosiglitazone 0.98 0.99 Warfarin 30 mg single dose on day 5 200 mg‡ once daily for 11 days S(-) Warfarin 0.95 0.89 R(+) Warfarin 0.99 0.89 Ethinyl estradiol and norethindrone 21 days once daily of 35 µg ethinyl estradiol with norethindrone 0.5 mg × 7 days, 0.75 mg × 7 days, 1.0 mg × 7 days 200 mg‡ once daily for 21 days Ethinyl estradiol 0.99 0.97 Norethindrone 1.03 0.98 Metformin 1000 mg‡ twice daily for 14 days 50 mg‡ twice daily for 7 days Metformin 1.02# 0.97 Effects of Other Drugs on Sitagliptin
Clinical data described below suggest that sitagliptin is not susceptible to clinically meaningful interactions by coadministered medications (Table 5).
Table 5: Effect of Coadministered Drugs on Systemic Exposure of Sitagliptin Coadministered Drug Dose of Coadministered Drug* Dose of Sitagliptin* Geometric Mean Ratio
(ratio with/without coadministered drug)
No Effect = 1.00AUC† Cmax - * All doses administered as single dose unless otherwise specified.
- † AUC is reported as AUC0-∞ unless otherwise specified.
- ‡ Multiple dose.
- § AUC0-12hr.
Cyclosporine 600 mg once daily 100 mg once daily Sitagliptin 1.29 1.68 Metformin 1000 mg‡ twice daily for 14 days 50 mg‡ twice daily for 7 days Sitagliptin 1.02§ 1.05 Metformin HCl
Table 6: Effect of Metformin on Systemic Exposure of Coadministered Drugs Coadministered Drug Dose of Coadministered Drug* Dose of Metformin* Geometric Mean Ratio
(ratio with/without metformin)
No Effect = 1.00AUC† Cmax - * All doses administered as single dose unless otherwise specified.
- † AUC is reported as AUC0-∞ unless otherwise specified.
- ‡ AUC0-24hr.
- § GLUMETZA (metformin HCl extended-release tablets) 500 mg.
- ¶ Ratio of arithmetic means, p value of difference <0.05.
- # Ratio of arithmetic means.
Cimetidine 400 mg 850 mg Cimetidine 0.95‡ 1.01 Glyburide 5 mg 500 mg§ Glyburide 0.78¶ 0.63¶ Furosemide 40 mg 850 mg Furosemide 0.87¶ 0.69¶ Nifedipine 10 mg 850 mg Nifedipine 1.10‡ 1.08 Propranolol 40 mg 850 mg Propranolol 1.01‡ 0.94 Ibuprofen 400 mg 850 mg Ibuprofen 0.97# 1.01# Table 7: Effect of Coadministered Drugs on Systemic Exposure of Metformin Coadministered Drug Dose of Coadministered Drug* Dose of Metformin* Geometric Mean Ratio
(ratio with/without coadministered drug)
No Effect = 1.00AUC† Cmax - * All doses administered as single dose unless otherwise specified.
- † AUC is reported as AUC0-∞ unless otherwise specified.
- ‡ GLUMETZA (metformin HCl extended-release tablets) 500 mg.
- § Ratio of arithmetic means.
- ¶ Steady state 100 mg Topiramate every 12 hr + metformin 500 mg every 12 hr AUC = AUC0-12hr.
Glyburide 5 mg 500 mg‡ Metformin‡ 0.98§ 0.99§ Furosemide 40 mg 850 mg Metformin 1.09§ 1.22§ Nifedipine 10 mg 850 mg Metformin 1.16 1.21 Propranolol 40 mg 850 mg Metformin 0.90 0.94 Ibuprofen 400 mg 850 mg Metformin 1.05§ 1.07§ Drugs that are eliminated by renal tubular secretion may increase the accumulation of metformin. [See Warnings and Precautions (5.1) and Drug Interactions (7.2).] Cimetidine 400 mg 850 mg Metformin 1.40 1.61 Carbonic anhydrase inhibitors may cause metabolic acidosis. [See Warnings and Precautions (5.1) and Drug Interactions (7.1).] Topiramate 100 mg¶ 500 mg¶ Metformin 1.25¶ 1.17 -
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
JANUMET
No animal studies have been conducted with the combined products in JANUMET to evaluate carcinogenesis, mutagenesis or impairment of fertility. The following data are based on the findings in studies with sitagliptin and metformin individually.
Sitagliptin
A two-year carcinogenicity study was conducted in male and female rats given oral doses of sitagliptin of 50, 150, and 500 mg/kg/day. There was an increased incidence of combined liver adenoma/carcinoma in males and females and of liver carcinoma in females at 500 mg/kg. This dose results in exposures approximately 60 times the human exposure at the maximum recommended daily adult human dose (MRHD) of 100 mg/day based on AUC comparisons. Liver tumors were not observed at 150 mg/kg, approximately 20 times the human exposure at the MRHD. A two-year carcinogenicity study was conducted in male and female mice given oral doses of sitagliptin of 50, 125, 250, and 500 mg/kg/day. There was no increase in the incidence of tumors in any organ up to 500 mg/kg, approximately 70 times human exposure at the MRHD. Sitagliptin was not mutagenic or clastogenic with or without metabolic activation in the Ames bacterial mutagenicity assay, a Chinese hamster ovary (CHO) chromosome aberration assay, an in vitro cytogenetics assay in CHO, an in vitro rat hepatocyte DNA alkaline elution assay, and an in vivo micronucleus assay.
In rat fertility studies with oral gavage doses of 125, 250, and 1000 mg/kg, males were treated for 4 weeks prior to mating, during mating, up to scheduled termination (approximately 8 weeks total), and females were treated 2 weeks prior to mating through gestation day 7. No adverse effect on fertility was observed at 125 mg/kg (approximately 12 times human exposure at the MRHD of 100 mg/day based on AUC comparisons). At higher doses, nondose-related increased resorptions in females were observed (approximately 25 and 100 times human exposure at the MRHD based on AUC comparison).
Metformin HCl
Long-term carcinogenicity studies have been performed in rats (dosing duration of 104 weeks) and mice (dosing duration of 91 weeks) at doses up to and including 900 mg/kg/day and 1500 mg/kg/day, respectively. These doses are both approximately four times the maximum recommended human daily dose of 2000 mg based on body surface area comparisons. No evidence of carcinogenicity with metformin was found in either male or female mice. Similarly, there was no tumorigenic potential observed with metformin in male rats. There was, however, an increased incidence of benign stromal uterine polyps in female rats treated with 900 mg/kg/day.
There was no evidence of a mutagenic potential of metformin in the following in vitro tests: Ames test (S. typhimurium), gene mutation test (mouse lymphoma cells), or chromosomal aberrations test (human lymphocytes). Results in the in vivo mouse micronucleus test were also negative. Fertility of male or female rats was unaffected by metformin when administered at doses as high as 600 mg/kg/day, which is approximately three times the maximum recommended human daily dose based on body surface area comparisons.
-
14 CLINICAL STUDIES
The coadministration of sitagliptin and metformin has been studied in patients with type 2 diabetes inadequately controlled on diet and exercise and in combination with other antihyperglycemic agents.
None of the clinical efficacy studies described below was conducted with JANUMET; however, bioequivalence of JANUMET with coadministered sitagliptin and metformin HCl tablets was demonstrated.
Sitagliptin and Metformin Coadministration in Patients with Type 2 Diabetes Inadequately Controlled on Diet and Exercise
A total of 1091 patients with type 2 diabetes and inadequate glycemic control on diet and exercise participated in a 24-week, randomized, double-blind, placebo-controlled factorial study designed to assess the efficacy of sitagliptin and metformin coadministration. Patients on an antihyperglycemic agent (N=541) underwent a diet, exercise, and drug washout period of up to 12 weeks duration. After the washout period, patients with inadequate glycemic control (A1C 7.5% to 11%) were randomized after completing a 2-week single-blind placebo run-in period. Patients not on antihyperglycemic agents at study entry (N=550) with inadequate glycemic control (A1C 7.5% to 11%) immediately entered the 2-week single-blind placebo run-in period and then were randomized. Approximately equal numbers of patients were randomized to receive placebo, 100 mg of sitagliptin once daily, 500 mg or 1000 mg of metformin twice daily, or 50 mg of sitagliptin twice daily in combination with 500 mg or 1000 mg of metformin twice daily. Patients who failed to meet specific glycemic goals during the study were treated with glyburide (glibenclamide) rescue.
Sitagliptin and metformin coadministration provided significant improvements in A1C, FPG, and 2-hour PPG compared to placebo, to metformin alone, and to sitagliptin alone (Table 8, Figure 1). Mean reductions from baseline in A1C were generally greater for patients with higher baseline A1C values. For patients not on an antihyperglycemic agent at study entry, mean reductions from baseline in A1C were: sitagliptin 100 mg once daily, -1.1%; metformin 500 mg bid, -1.1%; metformin 1000 mg bid, -1.2%; sitagliptin 50 mg bid with metformin 500 mg bid, -1.6%; sitagliptin 50 mg bid with metformin 1000 mg bid, -1.9%; and for patients receiving placebo, -0.2%. Lipid effects were generally neutral. The decrease in body weight in the groups given sitagliptin in combination with metformin was similar to that in the groups given metformin alone or placebo.
Table 8: Glycemic Parameters at Final Visit (24-Week Study) for Sitagliptin and Metformin, Alone and in Combination in Patients with Type 2 Diabetes Inadequately Controlled on Diet and Exercise*
Placebo
Sitagliptin 100 mg once daily
Metformin
500 mg twice daily
Metformin
1000 mg twice dailySitagliptin
50 mg twice daily +
Metformin
500 mg twice dailySitagliptin
50 mg twice daily +
Metformin
1000 mg twice daily- * Intent-to-treat population using last observation on study prior to glyburide (glibenclamide) rescue therapy.
- † Least squares means adjusted for prior antihyperglycemic therapy status and baseline value.
- ‡ p<0.001 compared to placebo.
A1C (%) N = 165 N = 175 N = 178 N = 177 N = 183 N = 178 Baseline (mean) 8.7 8.9 8.9 8.7 8.8 8.8 Change from baseline (adjusted mean†) 0.2 -0.7 -0.8 -1.1 -1.4 -1.9 Difference from placebo (adjusted mean†) (95% CI) -0.8‡
(-1.1, -0.6)-1.0‡
(-1.2, -0.8)-1.3‡
(-1.5, -1.1)-1.6‡
(-1.8, -1.3)-2.1‡
(-2.3, -1.8)Patients (%) achieving A1C <7% 15 (9%) 35 (20%) 41 (23%) 68 (38%) 79 (43%) 118 (66%) % Patients receiving rescue medication 32 21 17 12 8 2 FPG (mg/dL) N = 169 N = 178 N = 179 N = 179 N = 183 N = 180 Baseline (mean) 196 201 205 197 204 197 Change from baseline (adjusted mean†) 6 -17 -27 -29 -47 -64 Difference from placebo (adjusted mean†) (95% CI) -23‡
(-33, -14)-33‡
(-43, -24)-35‡
(-45, -26)-53‡
(-62, -43)-70‡
(-79, -60)2-hour PPG (mg/dL) N = 129 N = 136 N = 141 N = 138 N = 147 N = 152 Baseline (mean) 277 285 293 283 292 287 Change from baseline (adjusted mean†) 0 -52 -53 -78 -93 -117 Difference from placebo (adjusted mean†) (95% CI) -52‡
(-67, -37)-54‡
(-69, -39)-78‡
(-93, -63)-93‡
(-107, -78)-117‡
(-131, -102)Figure 1: Mean Change from Baseline for A1C (%) over 24 Weeks with Sitagliptin and Metformin, Alone and in Combination in Patients with Type 2 Diabetes Inadequately Controlled with Diet and Exercise* - * All Patients Treated Population: least squares means adjusted for prior antihyperglycemic therapy and baseline value.
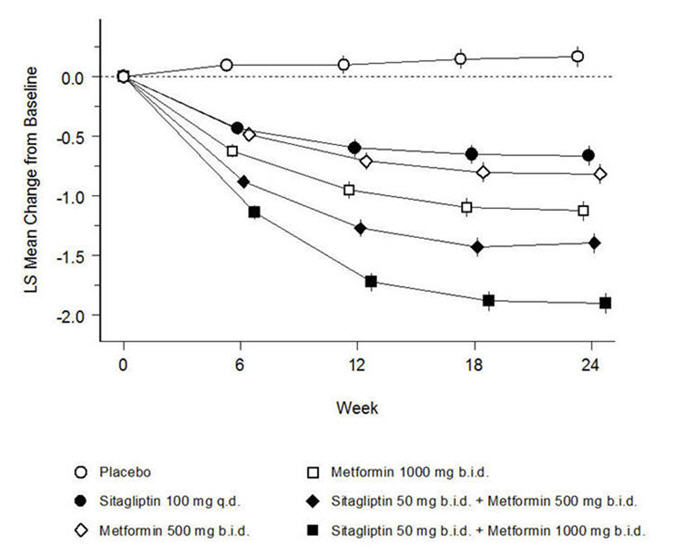
Initial combination therapy or maintenance of combination therapy should be individualized and are left to the discretion of the health care provider.
Sitagliptin Add-on Therapy in Patients with Type 2 Diabetes Inadequately Controlled on Metformin Alone
A total of 701 patients with type 2 diabetes participated in a 24-week, randomized, double-blind, placebo-controlled study designed to assess the efficacy of sitagliptin in combination with metformin. Patients already on metformin (N=431) at a dose of at least 1500 mg per day were randomized after completing a 2-week, single-blind placebo run-in period. Patients on metformin and another antihyperglycemic agent (N=229) and patients not on any antihyperglycemic agents (off therapy for at least 8 weeks, N=41) were randomized after a run-in period of approximately 10 weeks on metformin (at a dose of at least 1500 mg per day) in monotherapy. Patients were randomized to the addition of either 100 mg of sitagliptin or placebo, administered once daily. Patients who failed to meet specific glycemic goals during the studies were treated with pioglitazone rescue.
In combination with metformin, sitagliptin provided significant improvements in A1C, FPG, and 2-hour PPG compared to placebo with metformin (Table 9). Rescue glycemic therapy was used in 5% of patients treated with sitagliptin 100 mg and 14% of patients treated with placebo. A similar decrease in body weight was observed for both treatment groups.
Table 9: Glycemic Parameters at Final Visit (24-Week Study) of Sitagliptin as Add-on Combination Therapy with Metformin* Sitagliptin 100 mg once daily + Metformin Placebo + Metformin - * Intent-to-treat population using last observation on study prior to pioglitazone rescue therapy.
- † Least squares means adjusted for prior antihyperglycemic therapy and baseline value.
- ‡ p<0.001 compared to placebo + metformin.
A1C (%) N = 453 N = 224 Baseline (mean) 8.0 8.0 Change from baseline (adjusted mean†) -0.7 -0.0 Difference from placebo + metformin (adjusted mean†) (95% CI) -0.7‡
(-0.8, -0.5)Patients (%) achieving A1C <7% 213 (47%) 41 (18%) FPG (mg/dL) N = 454 N = 226 Baseline (mean) 170 174 Change from baseline (adjusted mean†) -17 9 Difference from placebo + metformin (adjusted mean†) (95% CI) -25‡
(-31, -20)2-hour PPG (mg/dL) N = 387 N = 182 Baseline (mean) 275 272 Change from baseline (adjusted mean†) -62 -11 Difference from placebo + metformin (adjusted mean†) (95% CI) -51‡
(-61, -41)Sitagliptin Add-on Therapy in Patients with Type 2 Diabetes Inadequately Controlled on the Combination of Metformin and Glimepiride
A total of 441 patients with type 2 diabetes participated in a 24-week, randomized, double-blind, placebo-controlled study designed to assess the efficacy of sitagliptin in combination with glimepiride, with or without metformin. Patients entered a run-in treatment period on glimepiride (≥4 mg per day) alone or glimepiride in combination with metformin (≥1500 mg per day). After a dose-titration and dose-stable run-in period of up to 16 weeks and a 2-week placebo run-in period, patients with inadequate glycemic control (A1C 7.5% to 10.5%) were randomized to the addition of either 100 mg of sitagliptin or placebo, administered once daily. Patients who failed to meet specific glycemic goals during the studies were treated with pioglitazone rescue.
Patients receiving sitagliptin with metformin and glimepiride had significant improvements in A1C and FPG compared to patients receiving placebo with metformin and glimepiride (Table 10), with mean reductions from baseline relative to placebo in A1C of -0.9% and in FPG of -21 mg/dL. Rescue therapy was used in 8% of patients treated with add-on sitagliptin 100 mg and 29% of patients treated with add-on placebo. The patients treated with add-on sitagliptin had a mean increase in body weight of 1.1 kg vs. add-on placebo (+0.4 kg vs. -0.7 kg). In addition, add-on sitagliptin resulted in an increased rate of hypoglycemia compared to add-on placebo. [See Warnings and Precautions (5.7); Adverse Reactions (6.1).]
Table 10: Glycemic Parameters at Final Visit (24-Week Study) for Sitagliptin in Combination with Metformin and Glimepiride* Sitagliptin 100 mg + Metformin and Glimepiride Placebo + Metformin and Glimepiride - * Intent-to-treat population using last observation on study prior to pioglitazone rescue therapy.
- † Least squares means adjusted for prior antihyperglycemic therapy status and baseline value.
- ‡ p<0.001 compared to placebo.
A1C (%) N = 115 N = 105 Baseline (mean) 8.3 8.3 Change from baseline (adjusted mean†) -0.6 0.3 Difference from placebo (adjusted mean†) (95% CI) -0.9‡
(-1.1, -0.7)Patients (%) achieving A1C <7% 26 (23%) 1 (1%) FPG (mg/dL) N = 115 N = 109 Baseline (mean) 179 179 Change from baseline (adjusted mean†) -8 13 Difference from placebo (adjusted mean†) (95% CI) -21‡
(-32, -10)Sitagliptin Add-on Therapy in Patients with Type 2 Diabetes Inadequately Controlled on the Combination of Metformin and Rosiglitazone
A total of 278 patients with type 2 diabetes participated in a 54-week, randomized, double-blind, placebo-controlled study designed to assess the efficacy of sitagliptin in combination with metformin and rosiglitazone. Patients on dual therapy with metformin ≥1500 mg/day and rosiglitazone ≥4 mg/day or with metformin ≥1500 mg/day and pioglitazone ≥30 mg/day (switched to rosiglitazone ≥4 mg/day) entered a dose-stable run-in period of 6 weeks. Patients on other dual therapy were switched to metformin ≥1500 mg/day and rosiglitazone ≥4 mg/day in a dose titration/stabilization run-in period of up to 20 weeks in duration. After the run-in period, patients with inadequate glycemic control (A1C 7.5% to 11%) were randomized 2:1 to the addition of either 100 mg of sitagliptin or placebo, administered once daily. Patients who failed to meet specific glycemic goals during the studies were treated with glipizide (or other sulfonylurea) rescue. The primary time point for evaluation of glycemic parameters was Week 18.
In combination with metformin and rosiglitazone, sitagliptin provided significant improvements in A1C, FPG, and 2-hour PPG compared to placebo with metformin and rosiglitazone (Table 11) at Week 18. At Week 54, mean reduction in A1C was -1.0% for patients treated with sitagliptin and -0.3% for patients treated with placebo in an analysis based on the intent-to-treat population. Rescue therapy was used in 18% of patients treated with sitagliptin 100 mg and 40% of patients treated with placebo. There was no significant difference between sitagliptin and placebo in body weight change.
Table 11: Glycemic Parameters at Week 18 for Sitagliptin in Add-on Combination Therapy with Metformin and Rosiglitazone* Week 18 Sitagliptin 100 mg + Metformin + Rosiglitazone Placebo + Metformin + Rosiglitazone - * Intent-to-treat population using last observation on study prior to glipizide (or other sulfonylurea) rescue therapy.
- † Least squares means adjusted for prior antihyperglycemic therapy status and baseline value.
- ‡ p<0.001 compared to placebo + metformin + rosiglitazone.
A1C (%) N = 176 N = 93 Baseline (mean) 8.8 8.7 Change from baseline (adjusted mean†) -1.0 -0.4 Difference from placebo + rosiglitazone + metformin (adjusted mean†) (95% CI) -0.7‡
(-0.9,-0.4)Patients (%) achieving A1C <7% 39 (22%) 9 (10%) FPG (mg/dL) N = 179 N = 94 Baseline (mean) 181 182 Change from baseline (adjusted mean†) -30 -11 Difference from placebo + rosiglitazone + metformin (adjusted mean†) (95% CI) -18‡
(-26, -10)2-hour PPG (mg/dL) N = 152 N = 80 Baseline (mean) 256 248 Change from baseline (adjusted mean†) -59 -21 Difference from placebo + rosiglitazone + metformin (adjusted mean†) (95% CI) -39‡
(-51, -26)Sitagliptin Add-on Therapy in Patients with Type 2 Diabetes Inadequately Controlled on the Combination of Metformin and Insulin
A total of 641 patients with type 2 diabetes participated in a 24-week, randomized, double-blind, placebo-controlled study designed to assess the efficacy of sitagliptin as add-on to insulin therapy. Approximately 75% of patients were also taking metformin. Patients entered a 2-week, single-blind run-in treatment period on pre-mixed, long-acting, or intermediate-acting insulin, with or without metformin (≥1500 mg per day). Patients using short-acting insulins were excluded unless the short-acting insulin was administered as part of a pre-mixed insulin. After the run-in period, patients with inadequate glycemic control (A1C 7.5% to 11%) were randomized to the addition of either 100 mg of sitagliptin (N=229) or placebo (N=233), administered once daily. Patients were on a stable dose of insulin prior to enrollment with no changes in insulin dose permitted during the run-in period. Patients who failed to meet specific glycemic goals during the double-blind treatment period were to have uptitration of the background insulin dose as rescue therapy.
Among patients also receiving metformin, the median daily insulin (pre-mixed, intermediate or long acting) dose at baseline was 40 units in the sitagliptin-treated patients and 42 units in the placebo-treated patients. The median change from baseline in daily dose of insulin was zero for both groups at the end of the study. Patients receiving sitagliptin with metformin and insulin had significant improvements in A1C, FPG and 2-hour PPG compared to patients receiving placebo with metformin and insulin (Table 12). The adjusted mean change from baseline in body weight was -0.3 kg in patients receiving sitagliptin with metformin and insulin and -0.2 kg in patients receiving placebo with metformin and insulin. There was an increased rate of hypoglycemia in patients treated with sitagliptin. [See Warnings and Precautions (5.7); Adverse Reactions (6.1).]
Table 12: Glycemic Parameters at Final Visit (24-Week Study) for Sitagliptin as Add-on Combination Therapy with Metformin and Insulin* Sitagliptin 100 mg + Metformin + Insulin Placebo + Metformin + Insulin - * Intent-to-treat population using last observation on study prior to rescue therapy.
- † Least squares means adjusted for insulin use at the screening visit, type of insulin used at the screening visit (pre-mixed vs. non pre-mixed [intermediate- or long-acting]), and baseline value.
- ‡ Treatment by insulin stratum interaction was not significant (p >0.10).
- § p<0.001 compared to placebo.
A1C (%) N = 223 N = 229 Baseline (mean) 8.7 8.6 Change from baseline (adjusted mean†,‡) -0.7 -0.1 Difference from placebo (adjusted mean†) (95% CI) -0.5§ (-0.7, -0.4) Patients (%) achieving A1C <7% 32 (14%) 12 (5%) FPG (mg/dL) N = 225 N = 229 Baseline (mean) 173 176 Change from baseline (adjusted mean†) -22 -4 Difference from placebo (adjusted mean†) (95% CI) -18§ (-28, -8.4) 2-hour PPG (mg/dL) N = 182 N = 189 Baseline (mean) 281 281 Change from baseline (adjusted mean†) -39 1 Difference from placebo (adjusted mean†) (95% CI) -40§ (-53, -28) Maintenance of Sitagliptin During Initiation and Titration of Insulin Glargine
A total of 746 patients with type 2 diabetes (mean baseline HbA1C 8.8%, disease duration 10.8 years) participated in a 30-week, randomized, double-blind, placebo-controlled study to assess the efficacy and safety of continuing sitagliptin during the initiation and uptitration of insulin glargine. Patients who were on a stable dose of metformin (≥1500 mg/day) in combination with a DPP-4 inhibitor and/or sulfonylurea but with inadequate glycemic control (A1C 7.5% to 11%) were enrolled in the study. Those on metformin and sitagliptin (100 mg/day) directly entered the double-blind treatment period; those on another DPP-4 inhibitor and/or on a sulfonylurea entered a 4-8 week run-in period in which they were maintained on metformin and switched to sitagliptin (100 mg); other DPP-4 inhibitors and sulfonylureas were discontinued. At randomization patients were randomized either to continue sitagliptin or to discontinue sitagliptin and switch to a matching placebo. On the day of randomization, insulin glargine was initiated at a dose of 10 units subcutaneously in the evening. Patients were instructed to uptitrate their insulin dose in the evening based on fasting blood glucose measurements to achieve a target of 72-100 mg/dL.
At 30 weeks, the mean reduction in A1C was greater in the sitagliptin group than in the placebo group (Table 13). At the end of the trial, 27.3% of patients in the sitagliptin group and 27.3% in the placebo group had a fasting plasma glucose (FPG) in the target range; there was no significant difference in insulin dose between arms.
Table 13: Change from Baseline in A1C and FPG at Week 30 in the Maintenance of Sitagliptin During Initiation and Titration of Insulin Glargine Study Sitagliptin 100 mg +Metformin + Insulin Glargine Placebo +Metformin + Insulin Glargine - * N is the number of randomized and treated patients.
- † Analysis of Covariance including all post-baseline data regardless of rescue or treatment discontinuation. Model estimates calculated using multiple imputation to model washout of the treatment effect using placebo data for all subjects having missing Week 30 data.
- ‡ p<0.001 compared to placebo.
A1C (%) N = 373* N = 370* Baseline (mean) 8.8 8.8 Week 30 (mean) 6.9 7.3 Change from baseline (adjusted mean)† -1.9 -1.4 Difference from placebo (adjusted mean) (95% CI)† -0.4 (-0.6, -0.3)‡ Patients (%) with A1C <7% 202 (54.2%) 131 (35.4%) FPG (mg/dL) N = 373* N = 370* Baseline (mean) 199 201 Week 30 (mean) 118 123 Change from baseline (adjusted mean)† -81 -76 Sitagliptin Add-on Therapy vs. Glipizide Add-on Therapy in Patients with Type 2 Diabetes Inadequately Controlled on Metformin
The efficacy of sitagliptin was evaluated in a 52-week, double-blind, glipizide-controlled noninferiority trial in patients with type 2 diabetes. Patients not on treatment or on other antihyperglycemic agents entered a run-in treatment period of up to 12 weeks duration with metformin monotherapy (dose of ≥1500 mg per day) which included washout of medications other than metformin, if applicable. After the run-in period, those with inadequate glycemic control (A1C 6.5% to 10%) were randomized 1:1 to the addition of sitagliptin 100 mg once daily or glipizide for 52 weeks. Patients receiving glipizide were given an initial dosage of 5 mg/day and then electively titrated over the next 18 weeks to a maximum dosage of 20 mg/day as needed to optimize glycemic control. Thereafter, the glipizide dose was to be kept constant, except for down-titration to prevent hypoglycemia. The mean dose of glipizide after the titration period was 10 mg.
After 52 weeks, sitagliptin and glipizide had similar mean reductions from baseline in A1C in the intent-to-treat analysis (Table 14). These results were consistent with the per protocol analysis (Figure 2). A conclusion in favor of the non-inferiority of sitagliptin to glipizide may be limited to patients with baseline A1C comparable to those included in the study (over 70% of patients had baseline A1C less than 8% and over 90% had A1C less than 9%).
Table 14: Glycemic Parameters in a 52-Week Study Comparing Sitagliptin to Glipizide as Add-On Therapy in Patients Inadequately Controlled on Metformin (Intent-to-Treat Population)* Sitagliptin 100 mg + Metformin Glipizide + Metformin - * The intent-to-treat analysis used the patients' last observation in the study prior to discontinuation.
- † Least squares means adjusted for prior antihyperglycemic therapy status and baseline A1C value.
A1C (%) N = 576 N = 559 Baseline (mean) 7.7 7.6 Change from baseline (adjusted mean†) -0.5 -0.6 FPG (mg/dL) N = 583 N = 568 Baseline (mean) 166 164 Change from baseline (adjusted mean†) -8 -8 Figure 2: Mean Change from Baseline for A1C (%) Over 52 Weeks in a Study Comparing Sitagliptin to Glipizide as Add-On Therapy in Patients Inadequately Controlled on Metformin (Per Protocol Population) * - * The per protocol population (mean baseline A1C of 7.5%) included patients without major protocol violations who had observations at baseline and at Week 52.
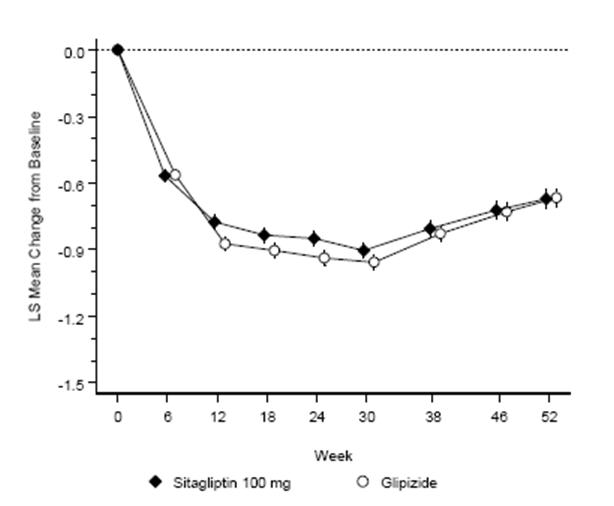
The incidence of hypoglycemia in the sitagliptin group (4.9%) was significantly (p<0.001) lower than that in the glipizide group (32.0%). Patients treated with sitagliptin exhibited a significant mean decrease from baseline in body weight compared to a significant weight gain in patients administered glipizide (-1.5 kg vs. +1.1 kg).
-
16 HOW SUPPLIED/STORAGE AND HANDLING
Tablets: JANUMET, 50 mg/500 mg, are light pink, capsule-shaped, film-coated tablets with "575" debossed on one side. They are supplied as follows:
NDC 0006-0575-61 unit-of-use bottles of 60
NDC 0006-0575-62 unit-of-use bottles of 180
NDC 0006-0575-82 bulk bottles of 1000.
Tablets: JANUMET, 50 mg/1000 mg, are red, capsule-shaped, film-coated tablets with "577" debossed on one side. They are supplied as follows:
NDC 0006-0577-61 unit-of-use bottles of 60
NDC 0006-0577-62 unit-of-use bottles of 180
NDC 0006-0577-82 bulk bottles of 1000.
-
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Medication Guide).
Lactic Acidosis
Inform patients of the risks of lactic acidosis due to the metformin component, its symptoms, and conditions that predispose to its development, as noted in Warnings and Precautions (5.1). Advise patients to discontinue JANUMET immediately and to promptly notify their health practitioner if unexplained hyperventilation, myalgia, malaise, unusual somnolence, dizziness, slow or irregular heart beat, sensation of feeling cold (especially in the extremities) or other nonspecific symptoms occur. Gastrointestinal symptoms are common during initiation of metformin treatment and may occur during initiation of JANUMET therapy; however, inform patients to consult their physician if they develop unexplained symptoms. Although gastrointestinal symptoms that occur after stabilization are unlikely to be drug related, such an occurrence of symptoms should be evaluated to determine if it may be due to lactic acidosis or other serious disease. Instruct patients to inform their doctor that they are taking JANUMET prior to any surgical or radiological procedure, as temporary discontinuation of JANUMET may be required until renal function has been confirmed to have returned to its prior level [see Warnings and Precautions (5.1)].
Counsel patients against excessive alcohol intake, either acute or chronic, while receiving JANUMET.
Inform patients about the importance of regular testing of renal function and hematological parameters when receiving treatment with JANUMET.
Pancreatitis
Inform patients that acute pancreatitis has been reported during postmarketing use of JANUMET. Inform patients that persistent severe abdominal pain, sometimes radiating to the back, which may or may not be accompanied by vomiting, is the hallmark symptom of acute pancreatitis. Instruct patients to promptly discontinue JANUMET and contact their physician if persistent severe abdominal pain occurs [see Warnings and Precautions (5.2)].
Heart Failure
Inform patients of the signs and symptoms of heart failure. Before initiating JANUMET, ask patients about a history of heart failure or other risk factors for heart failure including moderate to severe renal impairment. Instruct patients to contact their health care provider as soon as possible if they experience symptoms of heart failure, including increasing shortness of breath, rapid increase in weight or swelling of the feet [see Warnings and Precautions (5.3)].
Hypoglycemia
Inform patients that the incidence of hypoglycemia is increased when JANUMET is added to an insulin secretagogue (e.g., sulfonylurea) or insulin therapy and that a lower dose of the insulin secretagogue or insulin may be required to reduce the risk of hypoglycemia.
Hypersensitivity Reactions
Inform patients that allergic reactions have been reported during postmarketing use of sitagliptin, one of the components of JANUMET. If symptoms of allergic reactions (including rash, hives, and swelling of the face, lips, tongue, and throat that may cause difficulty in breathing or swallowing) occur, patients must stop taking JANUMET and seek medical advice promptly.
Severe and Disabling Arthralgia
Inform patients that severe and disabling joint pain may occur with this class of drugs. The time to onset of symptoms can range from one day to years. Instruct patients to seek medical advice if severe joint pain occurs [see Warnings and Precautions (5.10)].
Bullous Pemphigoid
Inform patients that bullous pemphigoid may occur with this class of drugs. Instruct patients to seek medical advice if blisters or erosions occur [see Warnings and Precautions (5.11)].
-
SPL UNCLASSIFIED SECTION
Dist. by: Merck Sharp & Dohme Corp., a subsidiary of
MERCK & CO., INC., Whitehouse Station, NJ 08889, USAFor patent information: www.merck.com/product/patent/home.html
The trademarks depicted herein are owned by their respective companies.
Copyright © 2007-2019 Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc.
All rights reserved.uspi-mk0431a-t-1908r019
-
MEDICATION GUIDE
Medication Guide
JANUMET® (JAN-you-met)
(sitagliptin and metformin hydrochloride)
TabletsThis Medication Guide has been approved by the U.S. Food and Drug Administration. Revised: 08/2017 Read this Medication Guide carefully before you start taking JANUMET and each time you get a refill. There may be new information. This information does not take the place of talking with your doctor about your medical condition or your treatment. If you have any questions about JANUMET, ask your doctor or pharmacist. What is the most important information I should know about JANUMET?
Serious side effects can happen in people taking JANUMET, including:
- 1. Lactic Acidosis. Metformin, one of the medicines in JANUMET, can cause a rare but serious condition called lactic acidosis (a buildup of an acid in the blood) that can cause death. Lactic acidosis is a medical emergency and must be treated in the hospital.
Call your doctor right away if you have any of the following symptoms, which could be signs of lactic acidosis:
- you feel cold in your hands or feet
- you feel dizzy or lightheaded
- you have a slow or irregular heartbeat
- you feel very weak or tired
- you have unusual (not normal) muscle pain
- you have trouble breathing
- you feel sleepy or drowsy
- you have stomach pains, nausea or vomiting
Most people who have had lactic acidosis with metformin have other things that, combined with the metformin, led to the lactic acidosis. Tell your doctor if you have any of the following, because you have a higher chance for getting lactic acidosis with JANUMET if you:
- have severe kidney problems or your kidneys are affected by certain x-ray tests that use injectable dye
- have liver problems
- drink alcohol very often, or drink a lot of alcohol in short-term "binge" drinking
- get dehydrated (lose a large amount of body fluids). This can happen if you are sick with a fever, vomiting, or diarrhea. Dehydration can also happen when you sweat a lot with activity or exercise and do not drink enough fluids
- have surgery
- have a heart attack, severe infection, or stroke
The best way to keep from having a problem with lactic acidosis from metformin is to tell your doctor if you have any of the problems in the list above. Your doctor may decide to stop your JANUMET for a while if you have any of these things.
JANUMET can have other serious side effects. See "What are the possible side effects of JANUMET?"
- 2.
Pancreatitis (inflammation of the pancreas) which may be severe and lead to death.
Certain medical problems make you more likely to get pancreatitis.
Before you start taking JANUMET:
Tell your doctor if you have ever had
-
- pancreatitis
- stones in your gallbladder (gallstones)
- a history of alcoholism
- high blood triglyceride levels
Stop taking JANUMET and call your doctor right away if you have pain in your stomach area (abdomen) that is severe and will not go away. The pain may be felt going from your abdomen through to your back. The pain may happen with or without vomiting. These may be symptoms of pancreatitis.
- 3. Heart failure. Heart failure means that your heart does not pump blood well enough.
Before you start taking JANUMET, tell your doctor if you have ever had heart failure or have problems with your kidneys.
Contact your doctor right away if you have any of the following symptoms:- increasing shortness of breath or trouble breathing, especially when you lie down
- swelling or fluid retention, especially in the feet, ankles or legs
- an unusually fast increase in weight
- unusual tiredness
- JANUMET is a prescription medicine that contains 2 prescription diabetes medicines, sitagliptin (JANUVIA®) and metformin. JANUMET can be used along with diet and exercise to lower blood sugar in adults with type 2 diabetes.
- JANUMET is not for people with type 1 diabetes.
- JANUMET is not for people with diabetic ketoacidosis (increased ketones in your blood or urine).
- If you have had pancreatitis (inflammation of the pancreas) in the past, it is not known if you have a higher chance of getting pancreatitis while you take JANUMET.
- It is not known if JANUMET is safe and effective when used in children under 18 years of age.
Do not take JANUMET if:
- you have severe kidney problems.
- you are allergic to any of the ingredients in JANUMET. See the end of this Medication Guide for a complete list of ingredients in JANUMET.
Symptoms of a serious allergic reaction to JANUMET may include rash, raised red patches on your skin (hives) or swelling of the face, lips, tongue, and throat that may cause difficulty in breathing or swallowing.
- you have diabetic ketoacidosis. See "What is JANUMET?".
What should I tell my doctor before taking JANUMET?
Before you take JANUMET, tell your doctor if you:
- have or have had inflammation of your pancreas (pancreatitis).
- have severe kidney problems.
- have liver problems.
- have heart problems, including congestive heart failure.
- drink alcohol very often, or drink a lot of alcohol in short-term "binge" drinking.
- are going to get an injection of dye or contrast agents for an x-ray procedure; JANUMET may need to be stopped for a short time. Talk to your doctor about when you should stop JANUMET and when you should start JANUMET again. See "What is the most important information I should know about JANUMET?".
- have any other medical conditions.
- are pregnant or plan to become pregnant. It is not known if JANUMET will harm your unborn baby. If you are pregnant, talk with your doctor about the best way to control your blood sugar while you are pregnant.
Pregnancy Registry: If you take JANUMET at any time during your pregnancy, talk with your doctor about how you can join the JANUMET pregnancy registry. The purpose of this registry is to collect information about the health of you and your baby. You can enroll in this registry by calling 1-800-986-8999. - are breast-feeding or plan to breast-feed. It is not known if JANUMET will pass into your breast milk. Talk with your doctor about the best way to feed your baby if you are taking JANUMET.
Tell your doctor about all the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. JANUMET may affect how well other drugs work and some drugs can affect how well JANUMET works.
Know the medicines you take. Keep a list of your medicines and show it to your doctor and pharmacist when you get a new medicine.
How should I take JANUMET?
- Take JANUMET exactly as your doctor tells you. Your doctor will tell you how many JANUMET tablets to take and when you should take them.
- Your doctor may change your dose of JANUMET if needed.
- Your doctor may tell you to take JANUMET along with certain other diabetes medicines. Low blood sugar (hypoglycemia) can happen more often when JANUMET is taken with certain other diabetes medicines. See "What are the possible side effects of JANUMET?".
- Take JANUMET with meals to help to lower your chance of having an upset stomach.
- Do not break or cut JANUMET tablets before swallowing. If you cannot swallow JANUMET tablets whole, tell your doctor.
- Continue to take JANUMET as long as your doctor tells you.
- If you take too much JANUMET, call your doctor or local Poison Control Center right away.
- If you miss a dose, take it as soon as you remember. If you do not remember until it is time for your next dose, skip the missed dose and go back to your regular schedule. Do not take 2 doses of JANUMET at the same time.
- You may need to stop taking JANUMET for a short time. Call your doctor for instructions if you:
- are dehydrated (have lost too much body fluid). Dehydration can occur if you are sick with severe vomiting, diarrhea or fever, or if you drink a lot less fluid than normal.
- plan to have surgery.
- are going to get an injection of dye or contrast agent for an x-ray procedure. See "What is the most important information I should know about JANUMET?" and "What should I tell my doctor before taking JANUMET?".
- When your body is under some types of stress, such as fever, trauma (such as a car accident), infection or surgery, the amount of diabetes medicine that you need may change. Tell your doctor right away if you have any of these problems and follow your doctor's instructions.
- Check your blood sugar as your doctor tells you to.
- Stay on your prescribed diet and exercise program while taking JANUMET.
- Talk to your doctor about how to prevent, recognize and manage low blood sugar (hypoglycemia), high blood sugar (hyperglycemia), and problems you have because of your diabetes.
- Your doctor will check your diabetes with regular blood tests, including your blood sugar levels and your hemoglobin A1C.
- Your doctor will do blood tests to check how well your kidneys are working before and during your treatment with JANUMET.
What are the possible side effects of JANUMET?
Serious side effects have happened in people taking JANUMET or the individual medicines in JANUMET.
- See "What is the most important information I should know about JANUMET?".
- Low blood sugar (hypoglycemia). If you take JANUMET with another medicine that can cause low blood sugar, such as a sulfonylurea or insulin, your risk of getting low blood sugar is higher. The dose of your sulfonylurea medicine or insulin may need to be lowered while you use JANUMET. Signs and symptoms of low blood sugar may include:
- headache
- drowsiness
- irritability
- hunger
- dizziness
- confusion
- sweating
- feeling jittery
- weakness
- fast heart beat
- Serious allergic reactions. If you have any symptoms of a serious allergic reaction, stop taking JANUMET and call your doctor right away. See "Who should not take JANUMET?". Your doctor may give you a medicine for your allergic reaction and prescribe a different medicine for your diabetes.
- Kidney problems, sometimes requiring dialysis.
- Joint pain. Some people who take medicines called DPP-4 inhibitors, one of the medicines in JANUMET, may develop joint pain that can be severe. Call your doctor if you have severe joint pain.
- Skin reaction. Some people who take medicines called DPP-4 inhibitors, one of the medicines in JANUMET, may develop a skin reaction called bullous pemphigoid that can require treatment in a hospital. Tell your doctor right away if you develop blisters or the breakdown of the outer layer of your skin (erosion). Your doctor may tell you to stop taking JANUMET.
The most common side effects of JANUMET include:
- stuffy or runny nose and sore throat
- gas, upset stomach, indigestion
- headache
- upper respiratory infection
- weakness
- diarrhea
- low blood sugar (hypoglycemia) when used in combination with certain medications, such as a sulfonylurea or insulin.
- nausea and vomiting
Taking JANUMET with meals can help lessen the common stomach side effects of metformin that usually happen at the beginning of treatment. If you have unusual or sudden stomach problems, talk with your doctor. Stomach problems that start later during treatment may be a sign of something more serious.
JANUMET may have other side effects, including swelling of the hands or legs. Swelling of the hands and legs can happen if you take JANUMET in combination with rosiglitazone (Avandia®). Rosiglitazone is another type of diabetes medicine.
These are not all the possible side effects of JANUMET. For more information, ask your doctor or pharmacist.
Tell your doctor if you have any side effect that bothers you, is unusual, or does not go away.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
How should I store JANUMET?
Store JANUMET at 68°F to 77°F (20°C to 25°C).
Keep JANUMET and all medicines out of the reach of children.
General information about the use of JANUMET.
Medicines are sometimes prescribed for purposes other than those listed in Medication Guides. Do not use JANUMET for a condition for which it was not prescribed. Do not give JANUMET to other people, even if they have the same symptoms you have. It may harm them.
This Medication Guide summarizes the most important information about JANUMET. If you would like to know more information, talk with your doctor. You can ask your doctor or pharmacist for additional information about JANUMET that is written for health care professionals. For more information go to www.janumet.com or call 1-800-622-4477.
What are the ingredients in JANUMET?
Active ingredients: sitagliptin and metformin
Inactive ingredients: microcrystalline cellulose, polyvinylpyrrolidone, sodium lauryl sulfate, and sodium stearyl fumarate. The tablet film coating contains the following inactive ingredients: polyvinyl alcohol, polyethylene glycol, talc, titanium dioxide, red iron oxide, and black iron oxide.
What is type 2 diabetes?
Type 2 diabetes is a condition in which your body does not make enough insulin, and the insulin that your body produces does not work as well as it should. Your body can also make too much sugar. When this happens, sugar (glucose) builds up in the blood. This can lead to serious medical problems.
High blood sugar can be lowered by diet and exercise, and by certain medicines when necessary.
Dist. by: Merck Sharp & Dohme Corp., a subsidiary of
MERCK & CO., INC., Whitehouse Station, NJ 08889, USAFor patent information: www.merck.com/product/patent/home.html. The trademarks depicted herein are owned by their respective companies. Copyright © 2010-2017 Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc. All rights reserved. usmg-mk0431a-t-1708r012
-
PRINCIPAL DISPLAY PANEL - 50 mg/500 mg Tablet Bottle Label
NDC: 0006-0575-61
Janumet®
(sitagliptin and
metformin HCl) tablets50 mg/500 mg
Dispense the accompanying Medication
Guide to each patient.Each tablet contains 64.25 mg sitagliptin phosphate
(equivalent to 50 mg sitagliptin) and 500 mg
metformin hydrochloride.Rx only
60 Tablets
-
PRINCIPAL DISPLAY PANEL - 50 mg/1,000 mg Tablet Bottle Label
NDC: 0006-0577-61
Janumet®
(sitagliptin and
metformin HCl) tablets50 mg/1,000 mg
Dispense the accompanying Medication Guide
to each patient.Each tablet contains 64.25 mg sitagliptin phosphate
(equivalent to 50 mg sitagliptin) and 1,000 mg
metformin hydrochloride.Rx only
60 Tablets
-
INGREDIENTS AND APPEARANCE
JANUMET
sitagliptin and metformin hydrochloride tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 0006-0575 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength SITAGLIPTIN PHOSPHATE (UNII: TS63EW8X6F) (SITAGLIPTIN - UNII:QFP0P1DV7Z) SITAGLIPTIN 50 mg METFORMIN HYDROCHLORIDE (UNII: 786Z46389E) (METFORMIN - UNII:9100L32L2N) METFORMIN HYDROCHLORIDE 500 mg Inactive Ingredients Ingredient Name Strength FERROSOFERRIC OXIDE (UNII: XM0M87F357) MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) POLYETHYLENE GLYCOL, UNSPECIFIED (UNII: 3WJQ0SDW1A) POLYVINYL ALCOHOL, UNSPECIFIED (UNII: 532B59J990) POVIDONE K30 (UNII: U725QWY32X) FERRIC OXIDE RED (UNII: 1K09F3G675) SODIUM LAURYL SULFATE (UNII: 368GB5141J) SODIUM STEARYL FUMARATE (UNII: 7CV7WJK4UI) TALC (UNII: 7SEV7J4R1U) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) Product Characteristics Color PINK (light pink) Score no score Shape OVAL (capsule-shaped) Size 17mm Flavor Imprint Code 575 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 0006-0575-82 1000 in 1 BOTTLE; Type 0: Not a Combination Product 03/30/2007 2 NDC: 0006-0575-61 60 in 1 BOTTLE; Type 0: Not a Combination Product 03/30/2007 3 NDC: 0006-0575-62 180 in 1 BOTTLE; Type 0: Not a Combination Product 03/30/2007 4 NDC: 0006-0575-52 5 in 1 CARTON 03/30/2007 08/20/2011 4 NDC: 0006-0575-01 10 in 1 BLISTER PACK; Type 0: Not a Combination Product 5 NDC: 0006-0575-56 4 in 1 CARTON 03/30/2007 5 2 in 1 POUCH 5 7 in 1 BLISTER PACK; Type 0: Not a Combination Product 6 NDC: 0006-0575-03 2 in 1 CARTON 03/30/2007 6 NDC: 0006-0575-02 14 in 1 BOTTLE; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA022044 03/30/2007 JANUMET
sitagliptin and metformin hydrochloride tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 0006-0577 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength SITAGLIPTIN PHOSPHATE (UNII: TS63EW8X6F) (SITAGLIPTIN - UNII:QFP0P1DV7Z) SITAGLIPTIN 50 mg METFORMIN HYDROCHLORIDE (UNII: 786Z46389E) (METFORMIN - UNII:9100L32L2N) METFORMIN HYDROCHLORIDE 1000 mg Inactive Ingredients Ingredient Name Strength FERROSOFERRIC OXIDE (UNII: XM0M87F357) MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) POLYETHYLENE GLYCOL, UNSPECIFIED (UNII: 3WJQ0SDW1A) POLYVINYL ALCOHOL, UNSPECIFIED (UNII: 532B59J990) POVIDONE K30 (UNII: U725QWY32X) FERRIC OXIDE RED (UNII: 1K09F3G675) SODIUM LAURYL SULFATE (UNII: 368GB5141J) SODIUM STEARYL FUMARATE (UNII: 7CV7WJK4UI) TALC (UNII: 7SEV7J4R1U) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) Product Characteristics Color RED (red) Score no score Shape OVAL (capsule-shaped) Size 21mm Flavor Imprint Code 577 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 0006-0577-61 60 in 1 BOTTLE; Type 0: Not a Combination Product 03/30/2007 2 NDC: 0006-0577-62 180 in 1 BOTTLE; Type 0: Not a Combination Product 03/30/2007 3 NDC: 0006-0577-82 1000 in 1 BOTTLE; Type 0: Not a Combination Product 03/30/2007 4 NDC: 0006-0577-52 5 in 1 CARTON 03/30/2007 10/05/2011 4 NDC: 0006-0577-01 10 in 1 BLISTER PACK; Type 0: Not a Combination Product 5 NDC: 0006-0577-56 4 in 1 CARTON 03/30/2007 5 2 in 1 POUCH 5 7 in 1 BLISTER PACK; Type 0: Not a Combination Product 6 NDC: 0006-0577-03 2 in 1 CARTON 03/30/2007 6 NDC: 0006-0577-02 14 in 1 BOTTLE; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA022044 03/30/2007 Labeler - Merck Sharp & Dohme Corp. (001317601)
Trademark Results [JANUMET]
Mark Image Registration | Serial | Company Trademark Application Date |
|---|---|
 JANUMET 78934999 3363805 Live/Registered |
MERCK SHARP & DOHME CORP. 2006-07-21 |
 JANUMET 78773912 3374065 Live/Registered |
MERCK SHARP & DOHME CORP. 2005-12-15 |
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.