clindamycin phosphate- Clindamycin Phosphate solution
Drug Labeling and Warnings
Drug Details [pdf]
- N/A - Section Title Not Found In Database
- SPL UNCLASSIFIED SECTION
-
DESCRIPTION
Clindamycin Phosphate Topical Solution USP, 1% contains clindamycin phosphate, at a concentration equivalent to 10 mg clindamycin per milliliter. Each Clindamycin Phosphate Topical Solution pledget applicator contains approximately 1 mL of topical solution.
The solution contains isopropyl alcohol 50% v/v, propylene glycol, and purified water. Clindamycin phosphate is a water soluble ester of the semi-synthetic antibiotic produced by a 7(S)-chloro-substitution of the 7(R)-hydroxyl group of the parent antibiotic lincomycin.
The structural formula is represented below:
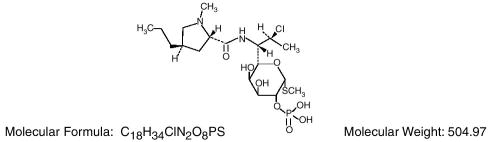
The chemical name for clindamycin phosphate is: Methyl 7-chloro-6,7,8-trideoxy-6-(1-methyl-trans-4-propyl-L-2-pyrrolidinecarboxamido)-1-thio-L-threo-α-D-galacto-octopyranoside 2-(dihydrogen phosphate). pH between 4.0 and 7.0.
-
CLINICAL PHARMACOLOGY
Although clindamycin phosphate is inactive in vitro, rapid in vivo hydrolysis converts this compound to the antibacterially active clindamycin.
Cross resistance has been demonstrated between clindamycin and lincomycin.
Antagonism has been demonstrated between clindamycin and erythromycin.
Following multiple topical applications of clindamycin phosphate at a concentration equivalent to 10 mg clindamycin per mL in an isopropyl alcohol and water solution, very low levels of clindamycin are present in the serum (0–3 ng/mL) and less than 0.2% of the dose is recovered in urine as clindamycin.
Clindamycin activity has been demonstrated in comedones from acne patients. The mean concentration of antibiotic activity in extracted comedones after application of Clindamycin Phosphate Topical Solution USP, 1% for 4 weeks was 597 mcg/g of comedonal material (range 0–1490). Clindamycin in vitro inhibits all Propionibacterium acnes cultures tested (MICs 0.4 mcg/mL). Free fatty acids on the skin surface have been decreased from approximately 14% to 2% following application of clindamycin.
-
INDICATIONS AND USAGE
Clindamycin Phosphate Topical Solution USP, 1% is indicated in the treatment of acne vulgaris. In view of the potential for diarrhea, bloody diarrhea and pseudomembranous colitis, the physician should consider whether other agents are more appropriate. (See CONTRAINDICATIONS , WARNINGS and ADVERSE REACTIONS.)
- CONTRAINDICATIONS
-
WARNINGS
Orally and parenterally administered clindamycin has been associated with severe colitis which may result in patient death. Use of the topical formulation of clindamycin results in absorption of the antibiotic from the skin surface. Diarrhea, bloody diarrhea, and colitis (including pseudomembranous colitis) have been reported with the use of topical and systemic clindamycin.
Studies indicate a toxin(s) produced by clostridia is one primary cause of antibiotic-associated colitis. The colitis is usually characterized by severe persistent diarrhea and severe abdominal cramps and may be associated with the passage of blood and mucus. Endoscopic examination may reveal pseudomembranous colitis. Stool culture for Clostridium difficile and stool assay for C. difficile toxin may be helpful diagnostically.
When significant diarrhea occurs, the drug should be discontinued. Large bowel endoscopy should be considered to establish a definitive diagnosis in cases of severe diarrhea.
Antiperistaltic agents such as opiates and diphenoxylate with atropine may prolong and/or worsen the condition. Vancomycin has been found to be effective in the treatment of antibiotic-associated pseudomembranous colitis produced by Clostridium difficile.The usual adult dosage is 500 mg to 2 grams of vancomycin orally per day in three to four divided doses administered for 7 to 10 days. Cholestyramine or colestipol resins bind vancomycin in vitro.If both a resin and vancomycin are to be administered concurrently, it may be advisable to separate the time of administration of each drug.
Diarrhea, colitis, and pseudomembranous colitis have been observed to begin up to several weeks following cessation of oral and parenteral therapy with clindamycin.
-
PRECAUTIONS
General: Clindamycin Phosphate Topical Solution USP, 1% contains an alcohol base which will cause burning and irritation of the eye. In the event of accidental contact with sensitive surfaces (eye, abraded skin, mucous membranes), bathe with copious amounts of cool tap water. The solution has an unpleasant taste and caution should be exercised when applying medication around the mouth.
Clindamycin Phosphate should be prescribed with caution in atopic individuals.
Drug Interactions: Clindamycin has been shown to have neuromuscular blocking properties that may enhance the action of other neuromuscular blocking agents. Therefore it should be used with caution in patients receiving such agents.
Pregnancy: Teratogenic Effects—Pregnancy Category B. Reproduction studies have been performed in rats and mice using subcutaneous and oral doses of clindamycin ranging from 100 to 600 mg/kg/day and have revealed no evidence of impaired fertility or harm to the fetus due to clindamycin. There are, however, no adequate and well-controlled studies in pregnant women. Because animal reproduction studies are not always predictive of human response, this drug should be used during pregnancy only if clearly needed.
Nursing Mothers: It is not known whether clindamycin is excreted in human milk following use of clindamycin phosphate. However, orally and parenterally administered clindamycin has been reported to appear in breast milk. Because of the potential for serious adverse reactions in nursing infants, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
Pediatric Use: Safety and effectiveness in pediatric patients under the age of 12 has not been established.
Geriatric Use: Clinical studies for clindamycin did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients.
-
ADVERSE REACTIONS
In 18 clinical studies of various topical clindamycin formulations of clindamycin phosphate using placebo vehicle and/or active comparator drugs as controls, patients experienced a number of treatment emergent adverse dermatologic events [see table below].
Number of Patients Reporting Events Treatment Emergent Adverse Event Solution
n=553 (%)Gel
n=148 (%)Suspension
n=160 (%)# not recorded
* of 126 subjects
Burning 62 (11) 15 (10) 17 (11) Itching 36 ( 7) 15 (10) 17 (11) Burning/Itching 60 (11) # ( – ) # ( – ) Dryness 105(19) 34 (23) 29 (18) Erythema 86 (16) 10 ( 7) 22 (14) Oiliness/Oily Skin 8 ( 1) 26 (18) 12*(10) Peeling 61 (11) # ( – ) 11 ( 7) Orally and parenterally administered clindamycin has been associated with severe colitis which may end fatally.
Cases of diarrhea, bloody diarrhea and colitis (including pseudomembranous colitis) have been reported as adverse reactions in patients treated with oral and parenteral formulations of clindamycin and rarely with topical clindamycin (see WARNINGS).
Abdominal pain and gastrointestinal disturbances as well as gram-negative folliculitis have also been reported in association with the use of topical formulations of clindamycin.
-
OVERDOSAGE
Topically applied clindamycin phosphate can be absorbed in sufficient amounts to produce systemic effects (see WARNINGS).
-
DOSAGE AND ADMINISTRATION
Use a Clindamycin Phosphate Topical Solution pledget for the application of clindamycin phosphate twice daily to affected area.
More than one pledget may be used. Each pledget should be used only once and then be discarded. Remove pledget from foil just before use. Do not use if the seal is broken. Discard after single use.
-
HOW SUPPLIED
Clindamycin Phosphate Topical Solution USP, 1% containing clindamycin phosphate equivalent to 10 mg clindamycin per milliliter is available in the following sizes:
Carton of 60 single-use pledget applicators NDC 0168-0201-01
Store at 20° to 25°C (68°to 77°F)[see USP Controlled Room Temperature].
Protect from freezing.
E. FOUGERA & CO.
a division of Altana Inc.
MELVILLE, NEW YORK 11747IF5263
R10/05
#51 -
INGREDIENTS AND APPEARANCE
CLINDAMYCIN PHOSPHATE
clindamycin phosphate solutionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 0168-0201 Route of Administration TOPICAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength Clindamycin phosphate (UNII: EH6D7113I8) (Clindamycin - UNII:3U02EL437C) 10 mg in 1 mL Inactive Ingredients Ingredient Name Strength isopropyl alcohol (UNII: ND2M416302) propylene glycol (UNII: 6DC9Q167V3) water (UNII: 059QF0KO0R) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 0168-0201-01 60 in 1 CARTON 1 1 mL in 1 PACKET Labeler - E. FOUGERA & CO.
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.