LANTUS- insulin glargine injection, solution LANTUS SOLOSTAR- insulin glargine injection, solution
Lantus Solostar by
Drug Labeling and Warnings
Lantus Solostar by is a Prescription medication manufactured, distributed, or labeled by sanofi-aventis U.S. LLC, Sanofi-Aventis Deutschland GmbH, Sanofi S.p.A (Anagni). Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use LANTUS safely and effectively. See full prescribing information for LANTUS.
LANTUS® (insulin glargine injection) for subcutaneous injection
Initial U.S. Approval: 2000INDICATIONS AND USAGE
DOSAGE AND ADMINISTRATION
- Individualize dosage based on metabolic needs, blood glucose monitoring, glycemic control, type of diabetes prior insulin use. (2.1, 2.3, 2.4)
- Administer subcutaneously into the abdominal area, thigh, or deltoid once daily at any time of day, but at the same time every day. (2.1)
- Do not dilute or mix with any other insulin or solution. (2.1)
- Rotate injection sites to reduce risk of lipodystrophy and localized cutaneous amyloidosis. (2.2)
- Closely monitor glucose when changing to LANTUS and during initial weeks thereafter. (2.4)
DOSAGE FORMS AND STRENGTHS
CONTRAINDICATIONS
WARNINGS AND PRECAUTIONS
- Never share a LANTUS SoloStar prefilled pen between patients, even if the needle is changed. (5.1)
- Hyperglycemia or hypoglycemia with changes in insulin regimen: Make changes to a patient's insulin regimen (e.g., insulin strength, manufacturer, type, injection site or method of administration) under close medical supervision with increased frequency of blood glucose monitoring. (5.2)
- Hypoglycemia: May be life-threatening. Increase frequency of glucose monitoring with changes to: insulin dosage, coadministered glucose lowering medications, meal pattern, physical activity; and in patients with renal or hepatic impairment and hypoglycemia unawareness. (5.3, 6.1)
- Medication Errors: Accidental mix-ups between insulin products can occur. Instruct patients to check insulin labels before injection. (5.4, 6.3)
- Hypersensitivity reactions: Severe, life-threatening, generalized allergy, including anaphylaxis, can occur. Discontinue LANTUS. Monitor and treat if indicated. (5.5, 6.1)
- Hypokalemia: May be life-threatening. Monitor potassium levels in patients at risk of hypokalemia and treat if indicated. (5.6)
- Fluid retention and heart failure with concomitant use of thiazolidinediones (TZDs): Observe for signs and symptoms of heart failure; consider dosage reduction or discontinuation of TZD if heart failure occurs. (5.7)
ADVERSE REACTIONS
Adverse reactions commonly associated with LANTUS include hypoglycemia, allergic reactions, injection site reactions, lipodystrophy, pruritus, rash, edema and weight gain. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact sanofi-aventis at 1-800-633-1610 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.DRUG INTERACTIONS
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.
Revised: 11/2019
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Important Administration Instructions
2.2 General Dosing Instructions
2.3 Initiation of LANTUS Therapy
2.4 Changing to LANTUS from Other Insulin Therapies
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Never Share a LANTUS SoloStar Prefilled Pen, Syringe, or Needle Between Patients
5.2 Hyperglycemia or Hypoglycemia with Changes in Insulin Regimen
5.3 Hypoglycemia
5.4 Medication Errors
5.5 Hypersensitivity and Allergic Reactions
5.6 Hypokalemia
5.7 Fluid Retention and Heart Failure with Concomitant Use of PPAR-gamma Agonists
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
6.2 Immunogenicity
6.3 Postmarketing Experience
7 DRUG INTERACTIONS
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.4 Pediatric Use
8.5 Geriatric Use
8.6 Hepatic Impairment
8.7 Renal Impairment
8.8 Obesity
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
14.1 Overview of Clinical Studies
14.2 Clinical Studies in Adult and Pediatric Patients with Type 1 Diabetes
14.3 Clinical Studies in Adults with Type 2 Diabetes
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 How Supplied
16.2 Storage
17 PATIENT COUNSELING INFORMATION
- * Sections or subsections omitted from the full prescribing information are not listed.
- 1 INDICATIONS AND USAGE
-
2 DOSAGE AND ADMINISTRATION
2.1 Important Administration Instructions
- Administer LANTUS subcutaneously once daily at any time of day but at the same time every day.
- Prior to initiation of LANTUS, train patients on proper use and injection technique.
- Patient should follow the Instructions for Use to correctly administer LANTUS.
- Administer LANTUS subcutaneously into the abdominal area, thigh, or deltoid, and rotate injection sites within the same region from one injection to the next to reduce the risk of lipodystrophy and localized cutaneous amyloidosis. Do not inject into areas of lipodystrophy or localized cutaneous amyloidosis [see Warnings and Precautions (5.2), Adverse Reactions (6)].
- During changes to a patient's insulin regimen, increase the frequency of blood glucose monitoring [see Warnings and Precautions (5.2)].
- Visually inspect LANTUS vials and SoloStar prefilled pens for particulate matter and discoloration prior to administration. Only use if the solution is clear and colorless with no visible particles.
- The LANTUS SoloStar prefilled pen dials in 1-unit increments.
- Use LANTUS SoloStar prefilled pen with caution in patients with visual impairment who may rely on audible clicks to dial their dose.
- Refrigerate unused (unopened) LANTUS vials and SoloStar® prefilled pens.
- Do not administer intravenously or via an insulin pump.
- Do not dilute or mix LANTUS with any other insulin or solution.
- The SoloStar prefilled pen is for single patient use only [see Warnings and Precautions (5.1)].
2.2 General Dosing Instructions
- Individualize and adjust the dosage of LANTUS based on the individual's metabolic needs, blood glucose monitoring results and glycemic control goal.
- Dosage adjustments may be needed with changes in physical activity, changes in meal patterns (i.e., macronutrient content or timing of food intake), during acute illness, or changes in renal or hepatic function. Dosage adjustments should only be made under medical supervision with appropriate glucose monitoring [see Warnings and Precautions (5.2)].
2.3 Initiation of LANTUS Therapy
Type 1 Diabetes
- In patients with type 1 diabetes, LANTUS must be used concomitantly with short-acting insulin. The recommended starting dose of LANTUS in patients with type 1 diabetes should be approximately one-third of the total daily insulin requirements. Short-acting, premeal insulin should be used to satisfy the remainder of the daily insulin requirements.
Type 2 Diabetes
- The recommended starting dose of LANTUS in patients with type 2 diabetes who are not currently treated with insulin is 0.2 units/kg or up to 10 units once daily. One may need to adjust the amount and timing of short- or rapid-acting insulins and dosages of any oral antidiabetic drugs.
2.4 Changing to LANTUS from Other Insulin Therapies
- If changing patients from once-daily TOUJEO (insulin glargine) 300 units/mL to once-daily LANTUS, the recommended initial LANTUS dose is 80% of the TOUJEO dose that is being discontinued. This dose reduction will lower the likelihood of hypoglycemia [see Warnings and Precautions (5.3)].
- If changing from a treatment regimen with an intermediate or long-acting insulin to a regimen with LANTUS, a change in the dose of the basal insulin may be required and the amount and timing of the shorter-acting insulins and doses of any oral antidiabetic drugs may need to be adjusted.
- If changing patients from once-daily NPH insulin to once-daily LANTUS, the recommended initial LANTUS dose is the same as the dose of NPH that is being discontinued.
- If changing patients from twice-daily NPH insulin to once-daily LANTUS, the recommended initial LANTUS dosage is 80% of the total NPH dose that is being discontinued. This dosage reduction will lower the likelihood of hypoglycemia [see Warnings and Precautions (5.3)].
- 3 DOSAGE FORMS AND STRENGTHS
-
4 CONTRAINDICATIONS
LANTUS is contraindicated:
- during episodes of hypoglycemia [see Warnings and Precautions (5.3)]
- in patients with hypersensitivity to LANTUS or one of its excipients [see Warnings and Precautions (5.5)]
-
5 WARNINGS AND PRECAUTIONS
5.1 Never Share a LANTUS SoloStar Prefilled Pen, Syringe, or Needle Between Patients
LANTUS SoloStar prefilled pens must never be shared between patients, even if the needle is changed. Patients using LANTUS vials must never re-use or share needles or syringes with another person. Sharing poses a risk for transmission of blood-borne pathogens.
5.2 Hyperglycemia or Hypoglycemia with Changes in Insulin Regimen
Changes in an insulin regimen (e.g., insulin strength, manufacturer, type, injection site or method of administration) may affect glycemic control and predispose to hypoglycemia [see Warnings and Precautions (5.3)] or hyperglycemia. Repeated insulin injections into areas of lipodystrophy or localized cutaneous amyloidosis have been reported to result in hyperglycemia; and a sudden change in the injection site (to unaffected area) has been reported to result in hypoglycemia [see Adverse Reactions (6.)].
Make any changes to a patient's insulin regimen under close medical supervision with increased frequency of blood glucose monitoring. Advise patients who have repeatedly injected into areas of lipodystrophy or localized cutaneous amyloidosis to change the injection site to unaffected areas and closely monitor for hypoglycemia. For patients with type 2 diabetes, dosage adjustments of concomitant oral and antidiabetic products may be needed.
5.3 Hypoglycemia
Hypoglycemia is the most common adverse reaction associated with insulin, including LANTUS. Severe hypoglycemia can cause seizures, may be life-threatening or cause death. Hypoglycemia can impair concentration ability and reaction time; this may place an individual and others at risk in situations where these abilities are important (e.g., driving or operating other machinery).
Hypoglycemia can happen suddenly and symptoms may differ in each individual and change over time in the same individual. Symptomatic awareness of hypoglycemia may be less pronounced in patients with longstanding diabetes, in patients with diabetic nerve disease, in patients using medications that block the sympathetic nervous system (e.g., beta-blockers) [see Drug Interactions (7)], or in patients who experience recurrent hypoglycemia.
Risk Factors for Hypoglycemia
The risk of hypoglycemia after an injection is related to the duration of action of the insulin and, in general, is highest when the glucose lowering effect of the insulin is maximal. As with all insulin preparations, the glucose lowering effect time course of LANTUS may vary in different individuals or at different times in the same individual and depends on many conditions, including the area of injection as well as the injection site blood supply and temperature [see Clinical Pharmacology (12.2)]. Other factors which may increase the risk of hypoglycemia include changes in meal pattern (e.g., macronutrient content or timing of meals), changes in level of physical activity, or changes to coadministered medication [see Drug Interactions (7)]. Patients with renal or hepatic impairment may be at higher risk of hypoglycemia [see Use in Specific Populations (8.6, 8.7)].
Risk Mitigation Strategies for Hypoglycemia
Patients and caregivers must be educated to recognize and manage hypoglycemia. Self-monitoring of blood glucose plays an essential role in the prevention and management of hypoglycemia. In patients at higher risk for hypoglycemia and patients who have reduced symptomatic awareness of hypoglycemia, increased frequency of blood glucose monitoring is recommended.
The long-acting effect of LANTUS may delay recovery from hypoglycemia.
5.4 Medication Errors
Accidental mix-ups among insulin products, particularly between long-acting insulins and rapid-acting insulins, have been reported. To avoid medication errors between LANTUS and other insulins, instruct patients to always check the insulin label before each injection [see Adverse Reactions (6.3)].
5.5 Hypersensitivity and Allergic Reactions
Severe, life-threatening, generalized allergy, including anaphylaxis, can occur with insulin products, including LANTUS. If hypersensitivity reactions occur, discontinue LANTUS; treat per standard of care and monitor until symptoms and signs resolve [see Adverse Reactions (6.1)]. LANTUS is contraindicated in patients who have had hypersensitivity reactions to insulin glargine or one of the excipients [see Contraindications (4)].
5.6 Hypokalemia
All insulin products, including LANTUS, cause a shift in potassium from the extracellular to intracellular space, possibly leading to hypokalemia. Untreated hypokalemia may cause respiratory paralysis, ventricular arrhythmia, and death. Monitor potassium levels in patients at risk for hypokalemia, if indicated (e.g., patients using potassium-lowering medications, patients taking medications sensitive to serum potassium concentrations).
5.7 Fluid Retention and Heart Failure with Concomitant Use of PPAR-gamma Agonists
Thiazolidinediones (TZDs), which are peroxisome proliferator-activated receptor (PPAR)-gamma agonists, can cause dose-related fluid retention, particularly when used in combination with insulin. Fluid retention may lead to or exacerbate heart failure. Patients treated with insulin, including LANTUS, and a PPAR-gamma agonist should be observed for signs and symptoms of heart failure. If heart failure develops, it should be managed according to current standards of care, and discontinuation or dose reduction of the PPAR-gamma agonist must be considered.
-
6 ADVERSE REACTIONS
The following adverse reactions are discussed elsewhere:
- Hypoglycemia [see Warnings and Precautions (5.3)]
- Hypersensitivity and allergic reactions [see Warnings and Precautions (5.5)]
- Hypokalemia [see Warnings and Precautions (5.6)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in clinical trials of a drug cannot be directly compared to rates in the clinical trial of another drug and may not reflect the rates observed in practice.
The data in Table 1 reflect the exposure of 2327 patients with type 1 diabetes to LANTUS or NPH. The type 1 diabetes population had the following characteristics: Mean age was 38.5 years. Fifty four percent were male, 96.9% were Caucasian, 1.8% were Black or African American and 2.7% were Hispanic. The mean BMI was 25.1 kg/m2.
The data in Table 2 reflect the exposure of 1563 patients with type 2 diabetes to LANTUS or NPH. The type 2 diabetes population had the following characteristics: Mean age was 59.3 years. Fifty eight percent were male, 86.7% were Caucasian, 7.8% were Black or African American and 9% were Hispanic. The mean BMI was 29.2 kg/m2.
The frequencies of adverse events during LANTUS clinical trials in patients with type 1 diabetes mellitus and type 2 diabetes mellitus are listed in the tables below.
Table 1: Adverse Events in Pooled Clinical Trials up to 28 Weeks Duration in Adults with Type 1 Diabetes (adverse events with frequency ≥5%) LANTUS, %
(n=1257)NPH, %
(n=1070)- * Body system not specified
Upper respiratory tract infection 22.4 23.1 Infection* 9.4 10.3 Accidental injury 5.7 6.4 Headache 5.5 4.7 Table 2: Adverse Events in Pooled Clinical Trials up to 1 Year Duration in Adults with Type 2 Diabetes (adverse events with frequency ≥5%) LANTUS, %
(n=849)NPH, %
(n=714)- * Body system not specified
Upper respiratory tract infection 11.4 13.3 Infection* 10.4 11.6 Retinal vascular disorder 5.8 7.4 Table 3: Adverse Events in a 5-Year Trial of Adults with Type 2 Diabetes (adverse events with frequency ≥10%) LANTUS, %
(n=514)NPH, %
(n=503)Upper respiratory tract infection 29.0 33.6 Edema peripheral 20.0 22.7 Hypertension 19.6 18.9 Influenza 18.7 19.5 Sinusitis 18.5 17.9 Cataract 18.1 15.9 Bronchitis 15.2 14.1 Arthralgia 14.2 16.1 Pain in extremity 13.0 13.1 Back pain 12.8 12.3 Cough 12.1 7.4 Urinary tract infection 10.7 10.1 Diarrhea 10.7 10.3 Depression 10.5 9.7 Headache 10.3 9.3 Table 4: Adverse Events in a 28-Week Clinical Trial of Children and Adolescents with Type 1 Diabetes (adverse events with frequency ≥5%) LANTUS, %
(n=174)NPH, %
(n=175)- * Body system not specified
Infection* 13.8 17.7 Upper respiratory tract infection 13.8 16.0 Pharyngitis 7.5 8.6 Rhinitis 5.2 5.1 Severe Hypoglycemia
Hypoglycemia is the most commonly observed adverse reaction in patients using insulin, including LANTUS [see Warnings and Precautions (5.3)]. Tables 5, and 6, and 7 summarize the incidence of severe hypoglycemia in the LANTUS individual clinical trials. Severe symptomatic hypoglycemia was defined as an event with symptoms consistent with hypoglycemia requiring the assistance of another person and associated with either a blood glucose below 50 mg/dL (≤56 mg/dL in the 5-year trial and ≤36 mg/dL in the ORIGIN trial) or prompt recovery after oral carbohydrate, intravenous glucose or glucagon administration.
Percentages of LANTUS-treated adult patients experiencing severe symptomatic hypoglycemia in the LANTUS clinical trials [see Clinical Studies (14)] were comparable to percentages of NPH-treated patients for all treatment regimens (see Tables 5 and 6). In the pediatric phase 3 clinical trial, children and adolescents with type 1 diabetes had a higher incidence of severe symptomatic hypoglycemia in the two treatment groups compared to the adult trials with type 1 diabetes.
Table 5: Severe Symptomatic Hypoglycemia in Patients with Type 1 Diabetes Study A
Type 1 Diabetes
Adults
28 weeks
In combination with regular insulinStudy B
Type 1 Diabetes
Adults
28 weeks
In combination with regular insulinStudy C
Type 1 Diabetes
Adults
16 weeks
In combination with insulin lisproStudy D
Type 1 Diabetes
Pediatrics
26 weeks
In combination with regular insulinLANTUS
N=292NPH
N=293LANTUS
N=264NPH
N=270LANTUS
N=310NPH
N=309LANTUS
N=174NPH
N=175Percent of patients 10.6 15.0 8.7 10.4 6.5 5.2 23.0 28.6 Table 6: Severe Symptomatic Hypoglycemia in Patients with Type 2 Diabetes Study E
Type 2 Diabetes
Adults
52 weeks
In combination with oral agentsStudy F
Type 2 Diabetes
Adults
28 weeks
In combination with regular insulinStudy G
Type 2 Diabetes
Adults
5 years
In combination with regular insulinLANTUS
N=289NPH
N=281LANTUS
N=259NPH
N=259LANTUS
N=513NPH
N=504Percent of patients 1.7 1.1 0.4 2.3 7.8 11.9 Table 7 displays the proportion of patients experiencing severe symptomatic hypoglycemia in the LANTUS and Standard Care groups in the ORIGIN Trial [see Clinical Studies (14)].
Table 7: Severe Symptomatic Hypoglycemia in the ORIGIN Trial ORIGIN Trial
Median duration of follow-up: 6.2 yearsLANTUS
N=6231Standard Care
N=6273Percent of patients 5.6 1.8 Peripheral Edema
Some patients taking LANTUS have experienced sodium retention and edema, particularly if previously poor metabolic control is improved by intensified insulin therapy.
Lipodystrophy
Administration of insulin subcutaneously, including LANTUS, has resulted in lipoatrophy (depression in the skin) or lipohypertrophy (enlargement or thickening of tissue) in some patients [see Dosage and Administration (2.2)].
Insulin Initiation and Intensification of Glucose Control
Intensification or rapid improvement in glucose control has been associated with a transitory, reversible ophthalmologic refraction disorder, worsening of diabetic retinopathy, and acute painful peripheral neuropathy. However, long-term glycemic control decreases the risk of diabetic retinopathy and neuropathy.
Weight Gain
Weight gain has occurred with some insulin therapies including LANTUS and has been attributed to the anabolic effects of insulin and the decrease in glucosuria.
Allergic Reactions
Local allergy
As with any insulin therapy, patients taking LANTUS may experience injection site reactions, including redness, pain, itching, urticaria, edema, and inflammation. In clinical studies in adult patients, there was a higher incidence of treatment-emergent injection site pain in LANTUS-treated patients (2.7%) compared to NPH insulin-treated patients (0.7%). The reports of pain at the injection site did not result in discontinuation of therapy.
6.2 Immunogenicity
As with all therapeutic proteins, there is potential for immunogenicity. All insulin products can elicit the formation of insulin antibodies. The presence of such insulin antibodies may increase or decrease the efficacy of insulin and may require adjustment of the insulin dose. In phase 3 clinical trials of LANTUS, increases in titers of antibodies to insulin were observed in NPH insulin and LANTUS treatment groups with similar incidences.
6.3 Postmarketing Experience
The following adverse reactions have been identified during postapproval use of LANTUS. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Medication errors have been reported in which other insulins, particularly rapid-acting insulins, have been accidentally administered instead of LANTUS [see Patient Counseling Information (17)]. To avoid medication errors between LANTUS and other insulins, patients should be instructed to always verify the insulin label before each injection.
Localized cutaneous amyloidosis at the injection site has occurred. Hyperglycemia has been reported with repeated insulin injections into areas of localized cutaneous amyloidosis; hypoglycemia has been reported with a sudden change to an unaffected injection site.
-
7 DRUG INTERACTIONS
Table 8 includes clinically significant drug interactions with LANTUS.
Table 8: Clinically Significant Drug Interactions with LANTUS Drugs that May Increase the Risk of Hypoglycemia Drugs: Antidiabetic agents, ACE inhibitors, angiotensin II receptor blocking agents, disopyramide, fibrates, fluoxetine, monoamine oxidase inhibitors, pentoxifylline, pramlintide, salicylates, somatostatin analogs (e.g., octreotide), and sulfonamide antibiotics. Intervention: Dose reductions and increased frequency of glucose monitoring may be required when LANTUS is coadministered with these drugs. Drugs that May Decrease the Blood Glucose Lowering Effect of LANTUS Drugs: Atypical antipsychotics (e.g., olanzapine and clozapine), corticosteroids, danazol, diuretics, estrogens, glucagon, isoniazid, niacin, oral contraceptives, phenothiazines, progestogens (e.g., in oral contraceptives), protease inhibitors, somatropin, sympathomimetic agents (e.g., albuterol, epinephrine, terbutaline), and thyroid hormones. Intervention: Dose increases and increased frequency of glucose monitoring may be required when LANTUS is coadministered with these drugs. Drugs that May Increase or Decrease the Blood Glucose Lowering Effect of LANTUS Drugs: Alcohol, beta-blockers, clonidine, and lithium salts. Pentamidine may cause hypoglycemia, which may sometimes be followed by hyperglycemia. Intervention: Dose adjustment and increased frequency of glucose monitoring may be required when LANTUS is coadministered with these drugs. Drugs that May Blunt Signs and Symptoms of Hypoglycemia Drugs: beta-blockers, clonidine, guanethidine, and reserpine Intervention: Increased frequency of glucose monitoring may be required when LANTUS is coadministered with these drugs. -
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
Published studies with use of insulin glargine during pregnancy have not reported a clear association with insulin glargine and adverse developmental outcomes [see Data]. There are risks to the mother and fetus associated with poorly controlled diabetes in pregnancy [see Clinical Considerations].
Rats and rabbits were exposed to insulin glargine in animal reproduction studies during organogenesis, respectively 50 times and 10 times the human subcutaneous dose of 0.2 units/kg/day. Overall, the effects of insulin glargine did not generally differ from those observed with regular human insulin [see Data].
The estimated background risk of major birth defects is 6% to 10% in women with pregestational diabetes with an HbA1c >7 and has been reported to be as high as 20% to 25% in women with a HbA1c >10. The estimated background risk of miscarriage for the indicated population is unknown. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Clinical Considerations
Disease-associated maternal and/or embryo-fetal risk
Poorly controlled diabetes in pregnancy increases the maternal risk for diabetic ketoacidosis, preeclampsia, spontaneous abortions, preterm delivery, and delivery complications. Poorly controlled diabetes increases the fetal risk for major birth defects, stillbirth, and macrosomia-related morbidity.
Data
Human data
Published data do not report a clear association with insulin glargine and major birth defects, miscarriage, or adverse maternal or fetal outcomes when insulin glargine is used during pregnancy. However, these studies cannot definitely establish the absence of any risk because of methodological limitations including small sample size and some lacking comparator groups.
Animal data
Subcutaneous reproduction and teratology studies have been performed with insulin glargine and regular human insulin in rats and Himalayan rabbits. Insulin glargine was given to female rats before mating, during mating, and throughout pregnancy at doses up to 0.36 mg/kg/day, which is approximately 50 times the recommended human subcutaneous starting dose of 0.2 units/kg/day (0.007 mg/kg/day), on a mg/kg basis. In rabbits, doses of 0.072 mg/kg/day, which is approximately 10 times the recommended human subcutaneous starting dose of 0.2 units/kg/day on a mg/kg basis, were administered during organogenesis. The effects of insulin glargine did not generally differ from those observed with regular human insulin in rats or rabbits. However, in rabbits, five fetuses from two litters of the high-dose group exhibited dilation of the cerebral ventricles. Fertility and early embryonic development appeared normal.
8.2 Lactation
Risk Summary
There are either no or only limited data on the presence of insulin glargine in human milk, the effects on breastfed infant, or the effects on milk production. Endogenous insulin is present in human milk. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for LANTUS, and any potential adverse effects on the breastfed child from LANTUS or from the underlying maternal condition.
8.4 Pediatric Use
The safety and effectiveness of LANTUS have been established in pediatric patients (age 6 to 15 years) with type 1 diabetes [see Clinical Studies (14.2)]. The safety and effectiveness of LANTUS in pediatric patients younger than 6 years of age with type 1 diabetes and pediatric patients with type 2 diabetes have not been established.
The dosage recommendation when changing to LANTUS in pediatric patients (age 6 to 15 years) with type 1 diabetes is the same as that described for adults [see Dosage and Administration (2.2, 2.4), Clinical Studies (14)]. As in adults, the dosage of LANTUS must be individualized in pediatric patients (age 6 to 15 years) with type 1 diabetes based on metabolic needs and frequent monitoring of blood glucose.
In the pediatric clinical trial, pediatric patients (age 6 to 15 years) with type 1 diabetes had a higher incidence of severe symptomatic hypoglycemia compared to the adults in trials with type 1 diabetes [see Adverse Reactions (6.1)].
8.5 Geriatric Use
Of the total number of subjects in controlled clinical studies of patients with type 1 and type 2 diabetes who were treated with LANTUS, 15% were ≥65 years of age and 2% were ≥75 years of age. The only difference in safety or effectiveness in the subpopulation of patients ≥65 years of age compared to the entire study population was a higher incidence of cardiovascular events typically seen in an older population in the LANTUS and NPH treatment groups.
Nevertheless, caution should be exercised when LANTUS is administered to geriatric patients. In elderly patients with diabetes, the initial dosing, dose increments, and maintenance dosage should be conservative to avoid hypoglycemic reactions. Hypoglycemia may be difficult to recognize in the elderly.
8.6 Hepatic Impairment
The effect of hepatic impairment on the pharmacokinetics of LANTUS has not been studied. Frequent glucose monitoring and dose adjustment may be necessary for LANTUS in patients with hepatic impairment [see Warnings and Precautions (5.3)].
8.7 Renal Impairment
The effect of renal impairment on the pharmacokinetics of LANTUS has not been studied. Some studies with human insulin have shown increased circulating levels of insulin in patients with renal failure. Frequent glucose monitoring and dose adjustment may be necessary for LANTUS in patients with renal impairment [see Warnings and Precautions (5.3)].
-
10 OVERDOSAGE
Excess insulin administration may cause hypoglycemia and hypokalemia [see Warnings and Precautions (5.3, 5.6)]. Mild episodes of hypoglycemia can usually be treated with oral carbohydrates. Adjustments in drug dosage, meal patterns, or exercise may be needed.
More severe episodes of hypoglycemia with coma, seizure, or neurologic impairment may be treated with intramuscular/subcutaneous glucagon or concentrated intravenous glucose. After apparent clinical recovery from hypoglycemia, continued observation and additional carbohydrate intake may be necessary to avoid recurrence of hypoglycemia. Hypokalemia must be corrected appropriately.
-
11 DESCRIPTION
LANTUS (insulin glargine injection) is a sterile solution of insulin glargine for subcutaneous use. Insulin glargine is a recombinant human insulin analog that is a long-acting, parenteral blood-glucose-lowering agent [see Clinical Pharmacology (12)]. Insulin glargine has low aqueous solubility at neutral pH. At pH 4 insulin glargine is completely soluble. After injection into the subcutaneous tissue, the acidic solution is neutralized, leading to formation of microprecipitates from which small amounts of insulin glargine are slowly released, resulting in a relatively constant concentration/time profile over 24 hours with no pronounced peak. This profile allows once-daily dosing as a basal insulin. LANTUS is produced by recombinant DNA technology utilizing a non-pathogenic laboratory strain of Escherichia coli (K12) as the production organism. Insulin glargine differs from human insulin in that the amino acid asparagine at position A21 is replaced by glycine and two arginines are added to the C-terminus of the B-chain. Chemically, insulin glargine is 21A-Gly-30Ba-L-Arg-30Bb-L-Arg-human insulin and has the empirical formula C267H404N72O78S6 and a molecular weight of 6063. Insulin glargine has the following structural formula:
LANTUS consists of insulin glargine dissolved in a clear aqueous fluid. Each milliliter of LANTUS (insulin glargine injection) contains 100 units (3.6378 mg) insulin glargine.
The 10 mL vial presentation contains the following inactive ingredients per mL: 30 mcg zinc, 2.7 mg m-cresol, 20 mg glycerol 85%, 20 mcg polysorbate 20, and water for injection.
The 3 mL prefilled pen presentation contains the following inactive ingredients per mL: 30 mcg zinc, 2.7 mg m-cresol, 20 mg glycerol 85%, and water for injection.
The pH is adjusted by addition of aqueous solutions of hydrochloric acid and sodium hydroxide. LANTUS has a pH of approximately 4.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
The primary activity of insulin, including insulin glargine, is regulation of glucose metabolism. Insulin and its analogs lower blood glucose by stimulating peripheral glucose uptake, especially by skeletal muscle and fat, and by inhibiting hepatic glucose production. Insulin inhibits lipolysis and proteolysis, and enhances protein synthesis.
12.2 Pharmacodynamics
In clinical studies, the glucose-lowering effect on a molar basis (i.e., when given at the same doses) of intravenous insulin glargine is approximately the same as that for human insulin. Figure 1 shows results from a study in patients with type 1 diabetes conducted for a maximum of 24 hours after the injection. The median time between injection and the end of pharmacological effect was 14.5 hours (range: 9.5 to 19.3 hours) for NPH insulin, and 24 hours (range: 10.8 to >24.0 hours) (24 hours was the end of the observation period) for insulin glargine.
* Determined as amount of glucose infused to maintain constant plasma glucose levels Figure 1: Activity Profile in Patients with Type 1 Diabetes 
The duration of action after abdominal, deltoid, or thigh subcutaneous administration was similar. The time course of action of insulins, including LANTUS, may vary between individuals and within the same individual.
12.3 Pharmacokinetics
Absorption and Bioavailability
After subcutaneous injection of LANTUS in healthy subjects and in patients with diabetes, the insulin serum concentrations indicated a slower, more prolonged absorption and a relatively constant concentration/time profile over 24 hours with no pronounced peak in comparison to NPH insulin.
Metabolism and Elimination
A metabolism study in humans indicates that insulin glargine is partly metabolized at the carboxyl terminus of the B chain in the subcutaneous depot to form two active metabolites with in vitro activity similar to that of human insulin, M1 (21A-Gly-insulin) and M2 (21A-Gly-des-30B-Thr-insulin). Unchanged drug and these degradation products are also present in the circulation.
Special Populations
Age, race, and gender
Effect of age, race, and gender on the pharmacokinetics of LANTUS has not been evaluated. However, in controlled clinical trials in adults (n=3890) and a controlled clinical trial in pediatric patients (n=349), subgroup analyses based on age, race, and gender did not show differences in safety and efficacy between LANTUS and NPH insulin [see Clinical Studies (14)].
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
In mice and rats, standard two-year carcinogenicity studies with insulin glargine were performed at doses up to 0.455 mg/kg, which was for the rat approximately 65 times the recommended human subcutaneous starting dose of 0.2 units/kg/day (0.007 mg/kg/day) on a mg/kg basis. Histiocytomas were found at injection sites in male rats and mice in acid vehicle containing groups and are considered a response to chronic tissue irritation and inflammation in rodents. These tumors were not found in female animals, in saline control, or insulin comparator groups using a different vehicle.
Insulin glargine was not mutagenic in tests for detection of gene mutations in bacteria and mammalian cells (Ames and HGPRT-test) and in tests for detection of chromosomal aberrations (cytogenetics in vitro in V79 cells and in vivo in Chinese hamsters).
In a combined fertility and prenatal and postnatal study in male and female rats at subcutaneous doses up to 0.36 mg/kg/day, which was approximately 50 times the recommended human subcutaneous starting dose of 0.2 units/kg/day (0.007 mg/kg/day) maternal toxicity due to dose-dependent hypoglycemia, including some deaths, was observed. Consequently, a reduction of the rearing rate occurred in the high-dose group only. Similar effects were observed with NPH insulin.
-
14 CLINICAL STUDIES
14.1 Overview of Clinical Studies
The safety and effectiveness of LANTUS given once-daily at bedtime was compared to that of once-daily and twice-daily NPH insulin in open-label, randomized, active-controlled, parallel studies of 2,327 adult patients and 349 pediatric patients with type 1 diabetes mellitus and 1,563 adult patients with type 2 diabetes mellitus (see Tables 9–11). In general, the reduction in glycated hemoglobin (HbA1c) with LANTUS was similar to that with NPH insulin.
14.2 Clinical Studies in Adult and Pediatric Patients with Type 1 Diabetes
In two clinical studies (Studies A and B), patients with type 1 diabetes (Study A; n=585, Study B n=534) were randomized to 28 weeks of basal-bolus treatment with LANTUS or NPH insulin. Regular human insulin was administered before each meal. LANTUS was administered at bedtime. NPH insulin was administered either as once daily at bedtime or in the morning and at bedtime when used twice daily.
In Study A, the average age was 39.2 years. The majority of patients were White (99%) and 55.7% were male. The mean BMI was approximately 24.9 kg/m2. The mean duration of diabetes was 15.5 years.
In Study B, the average age was 38.5 years. The majority of patients were White (95.3%) and 50.6% were male. The mean BMI was approximately 25.8 kg/m2. The mean duration of diabetes was 17.4 years.
In another clinical study (Study C), patients with type 1 diabetes (n=619) were randomized to 16 weeks of basal-bolus treatment with LANTUS or NPH insulin. Insulin lispro was used before each meal. LANTUS was administered once daily at bedtime and NPH insulin was administered once or twice daily. The average age was 39.2 years. The majority of patients were White (96.9%) and 50.6% were male. The mean BMI was approximately 25.6 kg/m2. The mean duration of diabetes was 18.5 years.
In these 3 studies, LANTUS and NPH insulin had similar effects on HbA1c (Table 9) with a similar overall rate of severe symptomatic hypoglycemia [see Adverse Reactions (6.1)].
Table 9: Type 1 Diabetes Mellitus – Adult Study A Study B Study C Treatment duration 28 weeks 28 weeks 16 weeks Treatment in combination with Regular insulin Regular insulin Insulin lispro LANTUS NPH LANTUS NPH LANTUS NPH Number of subjects treated 292 293 264 270 310 309 HbA1c Baseline HbA1c 8.0 8.0 7.7 7.7 7.6 7.7 Adjusted mean change at trial end +0.2 +0.1 -0.2 -0.2 -0.1 -0.1 Treatment Difference (95% CI) +0.1 (0.0; +0.2) +0.1 (-0.1; +0.2) 0.0 (-0.1; +0.1) Basal insulin dose Baseline mean 21 23 29 29 28 28 Mean change from baseline -2 0 -4 +2 -5 +1 Total insulin dose Baseline mean 48 52 50 51 50 50 Mean change from baseline -1 0 0 +4 -3 0 Fasting blood glucose (mg/dL) Baseline mean 167 166 166 175 175 173 Adj. mean change from baseline -21 -16 -20 -17 -29 -12 Body weight (kg) Baseline mean 73.2 74.8 75.5 75.0 74.8 75.6 Mean change from baseline 0.1 -0.0 0.7 1.0 0.1 0.5 Type 1 Diabetes – Pediatric (see Table 10)
In a randomized, controlled clinical study (Study D), pediatric patients (age range 6 to 15 years) with type 1 diabetes (n=349) were treated for 28 weeks with a basal-bolus insulin regimen where regular human insulin was used before each meal. LANTUS was administered once daily at bedtime and NPH insulin was administered once or twice daily. The average age was 11.7 years. The majority of patients were White (96.8%) and 51.9% were male. The mean BMI was approximately 18.9 kg/m2. The mean duration of diabetes was 4.8 years. Similar effects on HbA1c (Table 10) were observed in both treatment groups [see Adverse Reactions (6.1)].
Table 10: Type 1 Diabetes Mellitus – Pediatric Study D Treatment duration 28 weeks Treatment in combination with Regular insulin LANTUS + Regular Insulin NPH + Regular Insulin Number of subjects treated 174 175 HbA1c Baseline mean 8.5 8.8 Change from baseline (adjusted mean) +0.3 +0.3 Difference from NPH (adjusted mean) 0.0 (95% CI ) (-0.2; +0.3) Basal insulin dose Baseline mean 19 19 Mean change from baseline -1 +2 Total insulin dose Baseline mean 43 43 Mean change from baseline +2 +3 Fasting blood glucose (mg/dL) Baseline mean 194 191 Mean change from baseline -23 -12 Body weight (kg) Baseline mean 45.5 44.6 Mean change from baseline 2.2 2.5 14.3 Clinical Studies in Adults with Type 2 Diabetes
In a randomized, controlled clinical study (Study E) (n=570), LANTUS was evaluated for 52 weeks in combination with oral antidiabetic medications (a sulfonylurea, metformin, acarbose, or combinations of these drugs). The average age was 59.5 years. The majority of patients were White (92.8%) and 53.7% were male. The mean BMI was approximately 29.1 kg/m2. The mean duration of diabetes was 10.3 years. LANTUS administered once daily at bedtime was as effective as NPH insulin administered once daily at bedtime in reducing HbA1c and fasting glucose (Table 11). The rate of severe symptomatic hypoglycemia was similar in LANTUS and NPH insulin treated patients [see Adverse Reactions (6.1)].
In a randomized, controlled clinical study (Study F), in patients with type 2 diabetes not using oral antidiabetic medications (n=518), a basal-bolus regimen of LANTUS once daily at bedtime or NPH insulin administered once or twice daily was evaluated for 28 weeks. Regular human insulin was used before meals, as needed. The average age was 59.3 years. The majority of patients were White (80.7%) and 60% were male. The mean BMI was approximately 30.5 kg/m2. The mean duration of diabetes was 13.7 years. LANTUS had similar effectiveness as either once- or twice-daily NPH insulin in reducing HbA1c and fasting glucose (Table 11) with a similar incidence of hypoglycemia [see Adverse Reactions (6.1)].
In a randomized, controlled clinical study (Study G), patients with type 2 diabetes were randomized to 5 years of treatment with once-daily LANTUS or twice-daily NPH insulin. For patients not previously treated with insulin, the starting dose of LANTUS or NPH insulin was 10 units daily. Patients who were already treated with NPH insulin either continued on the same total daily NPH insulin dose or started LANTUS at a dose that was 80% of the total previous NPH insulin dose. The primary endpoint for this study was a comparison of the progression of diabetic retinopathy by 3 or more steps on the Early Treatment Diabetic Retinopathy Study (ETDRS) scale. HbA1c change from baseline was a secondary endpoint. Similar glycemic control in the 2 treatment groups was desired in order to not confound the interpretation of the retinal data. Patients or study personnel used an algorithm to adjust the LANTUS and NPH insulin doses to a target fasting plasma glucose ≤100 mg/dL. After the LANTUS or NPH insulin dose was adjusted, other antidiabetic agents, including premeal insulin were to be adjusted or added. The average age was 55.1 years. The majority of patients were White (85.3%) and 53.9% were male. The mean BMI was approximately 34.3 kg/m2. The mean duration of diabetes was 10.8 years. The LANTUS group had a smaller mean reduction from baseline in HbA1c compared to the NPH insulin group, which may be explained by the lower daily basal insulin doses in the LANTUS group (Table 11). The incidences of severe symptomatic hypoglycemia were similar between groups [see Adverse Reactions (6.1)].
Table 11: Type 2 Diabetes Mellitus – Adult Study E Study F Study G Treatment duration 52 weeks 28 weeks 5 years Treatment in combination with Oral agents Regular insulin Regular insulin LANTUS NPH LANTUS NPH LANTUS NPH - * In Study G, the baseline dose of basal or total insulin was the first available on-treatment dose prescribed during the study (on visit month 1.5)
Number of subjects treated 289 281 259 259 513 504 HbA1c Baseline mean 9.0 8.9 8.6 8.5 8.4 8.3 Adjusted mean change from baseline -0.5 -0.4 -0.4 -0.6 -0.6 -0.8 LANTUS – NPH -0.1 +0.2 +0.2 95% CI for Treatment difference (-0.3; +0.1) (0.0; +0.4) (+0.1; +0.4) Basal insulin dose* Baseline mean 14 15 44.1 45.5 39 44 Mean change from baseline +12 +9 -1 +7 +23 +30 Total insulin dose* Baseline mean 14 15 64 67 48 53 Mean change from baseline +12 +9 +10 +13 +41 +40 Fasting blood glucose (mg/dL) Baseline mean 179 180 164 166 190 180 Adj. mean change from baseline -49 -46 -24 -22 -45 -44 Body weight (kg) Baseline mean 83.5 82.1 89.6 90.7 100 99 Adj. mean change from baseline 2.0 1.9 0.4 1.4 3.7 4.8 LANTUS Timing of Daily Dosing (see Table 12)
The safety and efficacy of LANTUS administered pre-breakfast, pre-dinner, or at bedtime were evaluated in a randomized, controlled clinical study in patients with type 1 diabetes (study H, n=378). Patients were also treated with insulin lispro at mealtime. The average age was 40.9 years. All patients were White (100%) and 53.7% were male. The mean BMI was approximately 25.3 kg/m2. The mean duration of diabetes was 17.3 years. LANTUS administered at different times of the day resulted in similar reductions in HbA1c compared to that with bedtime administration (see Table 12). In these patients, data are available from 8-point home glucose monitoring. The maximum mean blood glucose was observed just prior to injection of LANTUS regardless of time of administration.
In this study, 5% of patients in the LANTUS-breakfast arm discontinued treatment because of lack of efficacy. No patients in the other two arms discontinued for this reason. The safety and efficacy of LANTUS administered pre-breakfast or at bedtime were also evaluated in a randomized, active-controlled clinical study (Study I, n=697) in patients with type 2 diabetes not adequately controlled on oral antidiabetic therapy. All patients in this study also received glimepiride 3 mg daily. The average age was 60.8 years. The majority of patients were White (96.6%) and 53.7% were male. The mean BMI was approximately 28.7 kg/m2. The mean duration of diabetes was 10.1 years. LANTUS given before breakfast was at least as effective in lowering HbA1c as LANTUS given at bedtime or NPH insulin given at bedtime (see Table 12).
Table 12: LANTUS Timing of Daily Dosing in Type 1 (Study H) and Type 2 (Study I) Diabetes Mellitus Treatment duration
Treatment in combination withStudy H
24 weeks
Insulin lisproStudy I
24 weeks
GlimepirideLANTUS
BreakfastLANTUS
DinnerLANTUS
BedtimeLANTUS
BreakfastLANTUS
BedtimeNPH
Bedtime- * Intent-to-treat
- † Not applicable
Number of subjects treated* 112 124 128 234 226 227 HbA1c Baseline mean 7.6 7.5 7.6 9.1 9.1 9.1 Mean change from baseline -0.2 -0.1 0.0 -1.3 -1.0 -0.8 Basal insulin dose (U) Baseline mean 22 23 21 19 20 19 Mean change from baseline 5 2 2 11 18 18 Total insulin dose (U) NA† NA NA Baseline mean 52 52 49 Mean change from baseline 2 3 2 Body weight (kg) Baseline mean 77.1 77.8 74.5 80.7 82 81 Mean change from baseline 0.7 0.1 0.4 3.9 3.7 2.9 Five-Year Trial Evaluating the Progression of Retinopathy
Retinopathy was evaluated in the LANTUS clinical studies by analysis of reported retinal adverse events and fundus photography. The numbers of retinal adverse events reported for LANTUS and NPH insulin treatment groups were similar for patients with type 1 and type 2 diabetes.
LANTUS was compared to NPH insulin in a 5-year randomized clinical trial that evaluated the progression of retinopathy as assessed with fundus photography using a grading protocol derived from the Early Treatment Diabetic Retinopathy Scale (ETDRS). Patients had type 2 diabetes (mean age 55 years) with no (86%) or mild (14%) retinopathy at baseline. Mean baseline HbA1c was 8.4%. The primary outcome was progression by 3 or more steps on the ETDRS scale at study endpoint. Patients with prespecified postbaseline eye procedures (pan-retinal photocoagulation for proliferative or severe nonproliferative diabetic retinopathy, local photocoagulation for new vessels, and vitrectomy for diabetic retinopathy) were also considered as 3-step progressors regardless of actual change in ETDRS score from baseline. Retinopathy graders were blinded to treatment group assignment. The results for the primary endpoint are shown in Table 13 for both the per-protocol and intent-to-treat populations, and indicate similarity of LANTUS to NPH in the progression of diabetic retinopathy as assessed by this outcome.
Table 13: Number (%) of Patients with 3 or More Step Progression on ETDRS Scale at Endpoint LANTUS (%) NPH (%) Difference*,† (SE) 95% CI for difference - * Difference = LANTUS – NPH
- † Using a generalized linear model (SAS GENMOD) with treatment and baseline HbA1c strata (cutoff 9.0%) as the classified independent variables, and with binomial distribution and identity link function
Per-protocol 53/374 (14.2%) 57/363 (15.7%) -2.0% (2.6%) -7.0% to +3.1% Intent-to-Treat 63/502 (12.5%) 71/487 (14.6%) -2.1% (2.1%) -6.3% to +2.1% The Origin Study
The Outcome Reduction with Initial Glargine Intervention trial (i.e., ORIGIN) was an open-label, randomized, 2-by-2, factorial design study. One intervention in ORIGIN compared the effect of LANTUS to standard care on major adverse cardiovascular outcomes in 12,537 participants ≥50 years of age with abnormal glucose levels (i.e., impaired fasting glucose [IFG] and/or impaired glucose tolerance [IGT]) or early type 2 diabetes mellitus and established cardiovascular (i.e., CV) disease or CV risk factors at baseline.
The objective of the trial was to demonstrate that LANTUS use could significantly lower the risk of major cardiovascular outcomes compared to standard care. Two coprimary composite cardiovascular endpoints were used in ORIGIN. The first coprimary endpoint was the time to first occurrence of a major adverse cardiovascular event defined as the composite of CV death, nonfatal myocardial infarction and nonfatal stroke. The second coprimary endpoint was the time to the first occurrence of CV death or nonfatal myocardial infarction or nonfatal stroke or revascularization procedure or hospitalization for heart failure.
Participants were randomized to either LANTUS (N=6264) titrated to a goal fasting plasma glucose of ≤95 mg/dL or to standard care (N=6273). Anthropometric and disease characteristics were balanced at baseline. The mean age was 64 years and 8% of participants were 75 years of age or older. The majority of participants were male (65%). Fifty nine percent were Caucasian, 25% were Latin, 10% were Asian and 3% were Black. The median baseline BMI was 29 kg/m2. Approximately 12% of participants had abnormal glucose levels (IGT and/or IFG) at baseline and 88% had type 2 diabetes. For patients with type 2 diabetes, 59% were treated with a single oral antidiabetic drug, 23% had known diabetes but were on no antidiabetic drug and 6% were newly diagnosed during the screening procedure. The mean HbA1c (SD) at baseline was 6.5% (1.0). Fifty-nine percent of participants had had a prior cardiovascular event and 39% had documented coronary artery disease or other cardiovascular risk factors.
Vital status was available for 99.9% and 99.8% of participants randomized to LANTUS and standard care respectively at end of trial. The median duration of follow-up was 6.2 years (range: 8 days to 7.9 years). The mean HbA1c (SD) at the end of the trial was 6.5% (1.1) and 6.8% (1.2) in the LANTUS and standard care group respectively. The median dose of LANTUS at end of trial was 0.45 U/kg. Eighty-one percent of patients randomized to LANTUS were using LANTUS at end of the study. The mean change in body weight from baseline to the last treatment visit was 2.2 kg greater in the LANTUS group than in the standard care group.
Overall, the incidence of major adverse cardiovascular outcomes was similar between groups (see Table 14). All-cause mortality was also similar between groups.
Table 14: Cardiovascular Outcomes in ORIGIN – Time to First Event Analyses LANTUS
N=6264Standard Care
N=6273LANTUS vs Standard Care n
(Events per 100 PY)n
(Events per 100 PY)Hazard Ratio (95% CI) Coprimary endpoints CV death, nonfatal myocardial infarction, or nonfatal stroke 1041
(2.9)1013
(2.9)1.02 (0.94, 1.11) CV death, nonfatal myocardial infarction, nonfatal stroke, hospitalization for heart failure or revascularization procedure 1792
(5.5)1727
(5.3)1.04 (0.97, 1.11) Components of coprimary endpoints CV death 580 576 1.00 (0.89, 1.13) Myocardial Infarction (fatal or nonfatal) 336 326 1.03 (0.88, 1.19) Stroke (fatal or nonfatal) 331 319 1.03 (0.89, 1.21) Revascularizations 908 860 1.06 (0.96, 1.16) Hospitalization for heart failure 310 343 0.90 (0.77, 1.05) In the ORIGIN trial, the overall incidence of cancer (all types combined) or death from cancer (Table 15) was similar between treatment groups.
Table 15: Cancer Outcomes in ORIGIN – Time to First Event Analyses LANTUS
N=6264Standard Care
N=6273LANTUS vs Standard Care n
(Events per 100 PY)n
(Events per 100 PY)Hazard Ratio (95% CI) Cancer endpoints Any cancer event (new or recurrent) 559
(1.56)561
(1.56)0.99 (0.88, 1.11) New cancer events 524
(1.46)535
(1.49)0.96 (0.85, 1.09) Death due to Cancer 189
(0.51)201
(0.54)0.94 (0.77, 1.15) -
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 How Supplied
LANTUS (insulin glargine injection) is supplied as a clear solution containing 100 units per mL (U-100) available in:
- Carton of one 10 mL multiple-dose vial NDC: 0088-2220-33
- Carton of five 3 mL single-patient-use SoloStar prefilled pens NDC: 0088-2219-05
The LANTUS SoloStar prefilled pen dials in 1-unit increments.
Needles are not included in the packs.
BD Ultra-Fine® needles1 to be used in conjunction with SoloStar prefilled pens are sold separately and are manufactured by BD.
- 1 Other brands listed are the trademarks of their respective owners and are not trademarks of sanofi-aventis U.S. LLC
16.2 Storage
Dispense in the original sealed carton with the enclosed Instructions for Use.
LANTUS should not be stored in the freezer and should not be allowed to freeze. Discard LANTUS if it has been frozen. Protect LANTUS from direct heat and light.
Storage conditions are summarized in the following table.
Not in-use (unopened) Not in-use (unopened) In-use (opened) Refrigerated Room Temperature (36°F–46°F [2°C–8°C]) (below 86°F [30°C]) (see temperature below) 10 mL multiple-dose vial Until expiration date 28 days 28 days
Refrigerated or room temperature3 mL single-patient-use SoloStar prefilled pen Until expiration date 28 days 28 days
Room temperature only
(Do not refrigerate) -
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient Information and Instructions for Use).
Never Share a LANTUS SoloStar Prefilled Pen or Syringe Between Patients
Advise patients that they must never share a LANTUS SoloStar prefilled pen with another person, even if the needle is changed. Advise patients using LANTUS vials not to re-use or share needles or syringes with another person. Sharing carries a risk for transmission of blood-borne pathogens [see Warnings and Precautions (5.1)].
Hyperglycemia or Hypoglycemia
Inform patients that hypoglycemia is the most common adverse reaction with insulin. Inform patients of the symptoms of hypoglycemia. Inform patients that the ability to concentrate and react may be impaired as a result of hypoglycemia. This may present a risk in situations where these abilities are especially important, such as driving or operating other machinery. Advise patients who have frequent hypoglycemia or reduced or absent warning signs of hypoglycemia to use caution when driving or operating machinery [see Warnings and Precautions (5.3)].
Advise patients that changes in insulin regimen can predispose to hyperglycemia or hypoglycemia and that changes in insulin regimen should be made under close medical supervision [see Warnings and Precautions (5.2)].
Medications Errors
Instruct patients to always check the insulin label before each injection [see Warnings and Precautions (5.4)].
Administration
Advise patients that LANTUS must NOT be diluted or mixed with any other insulin or solution and that LANTUS must only be used if the solution is clear and colorless with no particles visible [see Dosage and Administration (2)].
- SPL UNCLASSIFIED SECTION
-
PATIENT PACKAGE INSERT
Patient Information
LANTUS® (LAN-tus)
(insulin glargine injection) for subcutaneous use, 100 Units/mL (U-100)Do not share your syringes with other people, even if the needle has been changed. You may give other people a serious infection, or get a serious infection from them.
What is LANTUS?
LANTUS is a long-acting man-made-insulin used to control high blood sugar in adults with diabetes mellitus.
- LANTUS is not for use to treat diabetic ketoacidosis.
- It is not known if LANTUS is safe and effective in children less than 6 years of age with type 1 diabetes.
- It is not known if LANTUS is safe and effective in children with type 2 diabetes.
Who should not use LANTUS?
Do not use LANTUS if you:
- are having an episode of low blood sugar (hypoglycemia).
- have an allergy to insulin glargine or any of the ingredients in LANTUS. See the end of this Patient Information leaflet for a complete list of ingredients in LANTUS.
What should I tell my healthcare provider before using LANTUS?
Before using LANTUS, tell your healthcare provider about all your medical conditions including if you:
- have liver or kidney problems.
- take other medicines, especially ones called TZDs (thiazolidinediones).
- have heart failure or other heart problems. If you have heart failure, it may get worse while you take TZDs with LANTUS.
- are pregnant, planning to become pregnant, or are breastfeeding. It is not known if LANTUS may harm your unborn baby or breastfeeding baby.
Tell your healthcare provider about all the medicines you take including prescription and over-the-counter medicines, vitamins, and herbal supplements.
Before you start using LANTUS, talk to your healthcare provider about low blood sugar and how to manage it.
How should I use LANTUS?
- Read the detailed Instructions for Use that come with your LANTUS insulin.
- Use LANTUS exactly as your healthcare provider tells you to. Your healthcare provider should tell you how much LANTUS to use and when to use it.
- Know the amount of LANTUS you use. Do not change the amount of LANTUS you use unless your healthcare provider tells you to.
- Check your insulin label each time you give your injection to make sure you are using the correct insulin.
- Do not re-use needles. Always use a new needle for each injection. Re-use of needles increases your risk of having blocked needles, which may cause you to get the wrong dose of LANTUS. Using a new needle for each injection lowers your risk of getting an infection.
- You may take LANTUS at any time during the day but you must take it at the same time every day.
- Only use LANTUS that is clear and colorless. If your LANTUS is cloudy or slightly colored, return it to your pharmacy for a replacement.
- LANTUS is injected under the skin (subcutaneously) of your upper legs (thighs), upper arms, or stomach area (abdomen).
- Do not use LANTUS in an insulin pump or inject LANTUS into your vein (intravenously).
-
Change (rotate) injection sites within the area you chose with each dose to reduce your risk of getting lipodystrophy (pits in skin or thickened skin) and localized cutaneous amyloidosis (skin with lumps) at the injection sites.
- Do not use the exact same spot for each injection.
- Do not inject where the skin has pits, is thickened, or has lumps.
- Do not inject where the skin is tender, bruised, scaly or hard, or into scars or damaged skin.
- Do not mix LANTUS with any other type of insulin or liquid medicine.
- Check your blood sugar levels. Ask your healthcare provider what your blood sugar should be and when you should check your blood sugar levels.
Keep LANTUS and all medicines out of the reach of children.
Your dose of LANTUS may need to change because of:
- a change in level of physical activity or exercise, weight gain or loss, increased stress, illness, change in diet, or because of the medicines you take.
What should I avoid while using LANTUS?
While using LANTUS do not:
- drive or operate heavy machinery, until you know how LANTUS affects you.
- drink alcohol or use over-the counter medicines that contain alcohol.
What are the possible side effects of LANTUS and other insulins?
LANTUS may cause serious side effects that can lead to death, including:
-
low blood sugar (hypoglycemia). Signs and symptoms that may indicate low blood sugar include:
- dizziness or light-headedness, sweating, confusion, headache, blurred vision, slurred speech, shakiness, fast heartbeat, anxiety, irritability or mood change, hunger.
-
severe allergic reaction (whole body reaction). Get medical help right away if you have any of these signs or symptoms of a severe allergic reaction:
- a rash over your whole body, trouble breathing, a fast heartbeat, or sweating.
- low potassium in your blood (hypokalemia).
-
Heart failure. Taking certain diabetes pills called TZDs (thiazolidinediones) with LANTUS may cause heart failure in some people. This can happen even if you have never had heart failure or heart problems before. If you already have heart failure it may get worse while you take TZDs with LANTUS. Your healthcare provider should monitor you closely while you are taking TZDs with LANTUS. Tell your healthcare provider if you have any new or worse symptoms of heart failure including:
- shortness of breath, swelling of your ankles or feet, sudden weight gain.
Get emergency medical help if you have:
- trouble breathing; shortness of breath; fast heartbeat; swelling of your face, tongue, or throat; sweating; extreme drowsiness; dizziness; confusion.
The most common side effects of LANTUS include:
- low blood sugar (hypoglycemia); weight gain; allergic reactions, including reactions at your injection site; skin thickening or pits at the injection site (lipodystrophy).
These are not all the possible side effects of LANTUS. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
General information about the safe and effective use of LANTUS.
Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. Do not use LANTUS for a condition for which it was not prescribed. Do not give LANTUS to other people, even if they have the same symptoms that you have. It may harm them.
This Patient Information leaflet summarizes the most important information about LANTUS. If you would like more information, talk with your healthcare provider. You can ask your pharmacist or healthcare provider for information about LANTUS that is written for healthcare professionals. For more information, go to www.lantus.com or call 1-800-633-1610.
What are the ingredients in LANTUS?
- Active ingredient: insulin glargine
- 10 mL vial inactive ingredients: zinc, m-cresol, glycerol, polysorbate, and water for injection
Manufactured by: sanofi-aventis U.S. LLC, Bridgewater, NJ 08807
This Patient Information has been approved by the U.S. Food and Drug Administration
Approved: November 2019
-
SPL UNCLASSIFIED SECTION
Instructions for Use
LANTUS® (LAN-tus)
(insulin glargine injection) for subcutaneous use
10 mL Vial (100 Units/mL, U-100)Read the Instructions for Use before you start taking LANTUS and each time you get a new LANTUS vial. There may be new information. This information does not take the place of talking to your healthcare provider about your medical condition or your treatment.
Do not share your LANTUS syringes with other people even if the needle has been changed. You may give other people a serious infection, or get a serious infection from them.
Supplies needed to give your injection:
- a LANTUS 10 mL vial
- a U-100 insulin syringe and needle
- 2 alcohol swabs
- 1 sharps container for throwing away used needles and syringes. See "Disposing of used needles and syringes" at the end of these instructions.
Preparing your LANTUS dose:
- Wash your hands with soap and water or with alcohol.
- Check the LANTUS label to make sure you are taking the right type of insulin. This is especially important if you use more than 1 type of insulin.
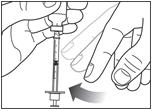
- Check the insulin to make sure it is clear and colorless. Do not use LANTUS if it is colored or cloudy, or if you see particles in the solution.
- Do not use LANTUS after the expiration date stamped on the label or 28 days after you first use it.
- Always use a syringe that is marked for U-100 insulin. If you use a syringe other than a U-100 insulin syringe, you may get the wrong dose of insulin.
- Always use a new syringe or needle for each injection. Do not re-use or share your syringes or needles with other people. You may give other people a serious infection or get a serious infection from them.
Step 1:
If you are using a new vial, remove the protective cap. Do not remove the stopper.

Step 2:
Wipe the top of the vial with an alcohol swab. You do not have to shake the vial of LANTUS before use.

Step 3:
Draw air into the syringe equal to your insulin dose. Put the needle through the rubber top of the vial and push the plunger to inject the air into the vial.


Step 4:
Leave the syringe in the vial and turn both upside down. Hold the syringe and vial firmly in one hand. Make sure the tip of the needle is in the insulin. With your free hand, pull the plunger to withdraw the correct dose into the syringe.

Step 5:
Before you take the needle out of the vial, check the syringe for air bubbles. If bubbles are in the syringe, hold the syringe straight up and tap the side of the syringe until the bubbles float to the top. Push the bubbles out with the plunger and draw insulin back in until you have the correct dose.
Step 6:
Remove the needle from the vial. Do not let the needle touch anything. You are now ready to inject.
Giving your LANTUS injection:
- Inject your insulin exactly as your healthcare provider has shown you.
- Inject your insulin under the skin (subcutaneously) of your upper legs (thighs), upper arms, or stomach area (abdomen).
- Change (rotate) your injection sites within the area you choose for each dose to reduce your risk of getting lipodystrophy (pits in the skin or thickened skin) and localized cutaneous amyloidosis (skin with lumps) at the injection sites.
- Do not inject where the skin has pits, is thickened, or has lumps.
- Do not inject where the skin is tender, bruised, scaly or hard, or into scars or damaged skin.
Step 7:
Choosing your injection site: LANTUS is injected under the skin (subcutaneously) of your upper arm, thigh, or stomach area (abdomen). Wipe the skin with an alcohol swab to clean the injection site. Let the injection site dry before you inject your dose.

Step 8:
- Pinch the skin.
- Insert the needle in the way your healthcare provider showed you.
- Release the skin.
- Slowly push in the plunger of the syringe all the way, making sure you have injected all the insulin.
- Leave the needle in the skin for about 10 seconds.

Step 9:
- Pull the needle straight out of your skin.
- Gently press the injection site for several seconds. Do not rub the area.
- Do not recap the used needle. Recapping the needle can lead to a needle stick injury.
Disposing of used needles and syringes:
- Put your used needles and syringes in a FDA-cleared sharps disposal container right away after use. Do not throw away (dispose of ) loose needles and syringes in your household trash.
- If you do not have a FDA-cleared sharps container, you may use a household container that is:
- made of a heavy-duty plastic,
- can be closed with a tight-fitting, puncture-resistant lid, without sharps being able to come out,
- upright and stable during use,
- leak resistant, and
- properly labeled to warn of hazardous waste inside the container.
- When your sharps disposal container is almost full, you will need to follow your community guidelines for the right way to dispose of your sharps disposal container. There may be state or local laws about how you should throw away used needles and syringes. For more information about safe sharps disposal, and for specific information about sharps disposal in the state that you live in, go to the FDA's website at: http://www.fda.gov/safesharpsdisposal.
- Do not dispose of your used sharps disposal container in your household trash unless your community guidelines permit this. Do not recycle your used sharps disposal container.
How should I store LANTUS?
- Store unused LANTUS vials in the refrigerator between 36°F to 46°F (2°C to 8°C).
- Store in-use (opened) LANTUS vials in a refrigerator or at room temperature below 86°F (30°C).
- Do not freeze LANTUS.
- Keep LANTUS out of direct heat and light.
- If a vial has been frozen or overheated, throw it away.
- The LANTUS vials you are using should be thrown away after 28 days, even if it still has insulin left in it.
This Instructions for Use has been approved by the U.S. Food and Drug Administration.
Revised: November 2019
sanofi-aventis U.S. LLC
Bridgewater, NJ 08807
A SANOFI COMPANY©2019 sanofi-aventis U.S. LLC
-
SPL UNCLASSIFIED SECTION
Patient Information
LANTUS® (LAN-tus)
(insulin glargine injection) for subcutaneous use, 100 Units/mL (U-100)Do not share your LANTUS SoloStar® pen with other people, even if the needle has been changed. You may give other people a serious infection, or get a serious infection from them.
What is LANTUS?
LANTUS is a long-acting man-made insulin used to control high blood sugar in adults with diabetes mellitus.
- LANTUS is not for use to treat diabetic ketoacidosis.
- It is not known if LANTUS is safe and effective in children less than 6 years of age with type 1 diabetes.
- It is not known if LANTUS is safe and effective in children with type 2 diabetes.
Who should not use LANTUS?
Do not use LANTUS if you:
- are having an episode of low blood sugar (hypoglycemia).
- have an allergy to insulin glargine or any of the ingredients in LANTUS. See the end of this Patient Information leaflet for a complete list of ingredients in LANTUS.
What should I tell my healthcare provider before using LANTUS?
Before using LANTUS, tell your healthcare provider about all your medical conditions including if you:
- have liver or kidney problems.
- take other medicines, especially ones called TZDs (thiazolidinediones).
- have heart failure or other heart problems. If you have heart failure, it may get worse while you take TZDs with LANTUS.
- are pregnant, planning to become pregnant, or are breastfeeding. It is not known if LANTUS may harm your unborn baby or breastfeeding baby.
Tell your healthcare provider about all the medicines you take including prescription and over-the-counter medicines, vitamins, and herbal supplements.
Before you start using LANTUS, talk to your healthcare provider about low blood sugar and how to manage it.
How should I use LANTUS?
- Read the detailed Instructions for Use that come with your LANTUS SoloStar single-patient-use prefilled pen.
- Use LANTUS exactly as your healthcare provider tells you to. Your healthcare provider should tell you how much LANTUS to use and when to use it.
- Know the amount of LANTUS you use. Do not change the amount of LANTUS you use unless your healthcare provider tells you to.
- Check your insulin label each time you give your injection to make sure you are using the correct insulin.
- LANTUS comes in a SoloStar single-patient-use prefilled pen that you must use to give your LANTUS. The dose counter on your pen shows your dose of LANTUS. Do not make any dose changes unless your healthcare provider tells you to.
- Do not use a syringe to remove LANTUS from your SoloStar disposable prefilled pen.
- Do not re-use needles. Always use a new needle for each injection. Re-use of needles increases your risk of having blocked needles, which may cause you to get the wrong dose of LANTUS. Using a new needle for each injection lowers your risk of getting an infection. If your needle is blocked, follow the instructions in Step 3 of the Instructions for Use.
- You may take LANTUS at any time during the day but you must take it at the same time every day.
- LANTUS is injected under the skin (subcutaneously) of your upper legs (thighs), upper arms, or stomach area (abdomen).
- Do not use LANTUS in an insulin pump or inject LANTUS into your vein (intravenously).
-
Change (rotate) your injection sites within area you chose with each dose to reduce your risk of getting lipodystrophy (pits in skin or thickened skin) and localized cutaneous amyloidosis (skin with lumps) at the injection sites.
- Do not use the exact same spot for each injection.
- Do not inject where the skin has pits, is thickened, or has lumps.
- Do not inject where skin is tender, bruised, scaly or hard, or into scars or damaged skin.
- Do not mix LANTUS with any other type of insulin or liquid medicine.
- Check your blood sugar levels. Ask your healthcare provider what your blood sugar should be and when you should check your blood sugar levels.
Keep LANTUS and all medicines out of the reach of children.
Your dose of LANTUS may need to change because of:
- a change in level of physical activity or exercise, weight gain or loss, increased stress, illness, change in diet, or because of the medicines you take.
What should I avoid while using LANTUS?
While using LANTUS do not:
- drive or operate heavy machinery, until you know how LANTUS affects you.
- drink alcohol or use over-the-counter medicines that contain alcohol.
What are the possible side effects of LANTUS and other insulins?
LANTUS may cause serious side effects that can lead to death, including:
-
low blood sugar (hypoglycemia). Signs and symptoms that may indicate low blood sugar include:
- dizziness or light-headedness, sweating, confusion, headache, blurred vision, slurred speech, shakiness, fast heartbeat, anxiety, irritability or mood change, hunger.
-
severe allergic reaction (whole body reaction). Get medical help right away if you have any of these signs or symptoms of a severe allergic reaction:
- a rash over your whole body, trouble breathing, a fast heartbeat, or sweating.
- low potassium in your blood (hypokalemia).
-
Heart failure. Taking certain diabetes pills called TZDs (thiazolidinediones) with LANTUS may cause heart failure in some people. This can happen even if you have never had heart failure or heart problems before. If you already have heart failure it may get worse while you take TZDs with LANTUS. Your healthcare provider should monitor you closely while you are taking TZDs with LANTUS. Tell your healthcare provider if you have any new or worse symptoms of heart failure including:
- shortness of breath, swelling of your ankles or feet, sudden weight gain.
Get emergency medical help if you have:
- trouble breathing; shortness of breath; fast heartbeat; swelling of your face, tongue, or throat; sweating; extreme drowsiness; dizziness; confusion.
The most common side effects of LANTUS include:
- low blood sugar (hypoglycemia); weight gain; allergic reactions, including reactions at your injection site; skin thickening or pits at the injection site (lipodystrophy).
These are not all the possible side effects of LANTUS. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
General information about the safe and effective use of LANTUS.
Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. Do not use LANTUS for a condition for which it was not prescribed. Do not give LANTUS to other people, even if they have the same symptoms that you have. It may harm them.
This Patient Information leaflet summarizes the most important information about LANTUS. If you would like more information, talk with your healthcare provider. You can ask your healthcare provider or pharmacist for information about LANTUS that is written for healthcare professionals. For more information about LANTUS call 1-800-633-1610 or go to the website www.lantus.com.
What are the ingredients in LANTUS?
- Active ingredient: insulin glargine
- 3 mL SoloStar prefilled pen inactive ingredients: zinc, m-cresol, glycerol, and water for injection
Hydrochloric acid and sodium hydroxide may be added to adjust the pH.
Manufactured by: sanofi-aventis U.S. LLC Bridgewater, NJ 08807
This Patient Information has been approved by the U.S. Food and Drug Administration
Revised: November 2019 -
SPL UNCLASSIFIED SECTION
Instructions for Use
LANTUS® SOLOSTAR® Single-Patient-Use Prefilled Pen
(insulin glargine injection)Your healthcare professional has decided that SoloStar is right for you. Talk with your healthcare professional about proper injection technique before using SoloStar.
Read these instructions carefully before using your SoloStar. If you are not able to follow all the instructions completely on your own, use SoloStar only if you have help from a person who is able to follow the instructions.
Do not share your LANTUS SoloStar pen with other people, even if the needle has been changed. You may give other people a serious infection, or get a serious infection from them.
People who are blind or have vision problems should not use LANTUS SoloStar single-patient-use prefilled pen without help from a person trained to use LANTUS SoloStar single-patient-use prefilled pen.
Follow these instructions completely each time you use SoloStar to ensure that you get an accurate dose. If you do not follow these instructions you may get too much or too little insulin, which may affect your blood glucose.
SoloStar is a disposable pen for the injection of insulin. Each SoloStar contains in total 300 units of insulin. You can set doses from 1 to 80 units in steps of 1 unit. The pen plunger moves with each dose. The plunger will only move to the end of the cartridge when 300 units of insulin have been given.
Keep this leaflet for future reference.
If you have any questions about SoloStar or about diabetes, ask your healthcare professional, go to www.lantus.com or call sanofi-aventis at 1-800-633-1610.

Important information for use of SoloStar:
- Do not share your LANTUS SoloStar pen with other people, even if the needle has been changed. You may give other people a serious infection, or get a serious infection from them.
- Do not re-use needles. Always attach a new needle before each use.
-
BD Ultra-Fine® needles2 are compatible with SoloStar. These are sold separately and are manufactured by BD. Contact your healthcare professional for further information.
- Always perform the safety test before each injection.
- Do not select a dose or press the injection button without a needle attached.
- If your injection is given by another person, special caution must be taken by this person to avoid accidental needle injury and transmission of infection.
- Never use SoloStar if it is damaged or if you are not sure that it is working properly.
- Always have a spare SoloStar in case your SoloStar is lost or damaged.
- Change (rotate) your injection sites within the area you choose for each dose (see "Places to inject").
- Inject your insulin exactly as your healthcare provider has shown you.
- Inject your insulin under the skin (subcutaneously) of your upper legs (thighs), upper arms, or stomach area (abdomen).
- Change (rotate) your injection sites within the area you choose for each dose to reduce your risk of getting lipodystrophy (pits in skin or thickened skin) and localized cutaneous amyloidosis (skin with lumps) at the injection sites.
- Do not inject where the skin has pits, is thickened, or has lumps.
- Do not inject where the skin is tender, bruised, scaly or hard, or into scars or damaged skin.
Step 1. Check the insulin
- A.
Check the label on your SoloStar to make sure you have the correct insulin. The LANTUS SoloStar is grey with a purple injection button.
- B. Take off the pen cap.
- C. Check the appearance of your insulin. LANTUS is a clear insulin. Do not use this SoloStar if the insulin is cloudy, colored or has particles.
- B. Take off the pen cap.
Step 2. Attach the needle
Do not re-use needles. Always use a new sterile needle for each injection. This helps prevent contamination and potential needle blocks.
- A. Wipe the Rubber Seal with alcohol.
- B.
Remove the protective seal from a new needle.
- C. Line up the needle with the pen, and keep it straight as you attach it (screw or push on, depending on the needle type).
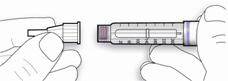
- C. Line up the needle with the pen, and keep it straight as you attach it (screw or push on, depending on the needle type).
- If the needle is not kept straight while you attach it, it can damage the rubber seal and cause leakage, or break the needle.
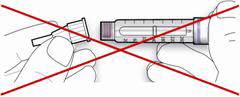
Step 3. Perform a Safety test
Always perform the safety test before each injection.
Performing the safety test ensures that you get an accurate dose by:- ensuring that pen and needle work properly
- removing air bubbles
- A.
Select a dose of 2 units by turning the dosage selector.
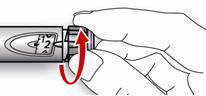
- B. Take off the outer needle cap and keep it to remove the used needle after injection. Take off the inner needle cap and discard it.
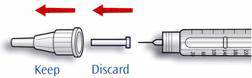
- C. Hold the pen with the needle pointing upwards.
- D. Tap the insulin reservoir so that any air bubbles rise up towards the needle.
- E. Press the injection button all the way in. Check if insulin comes out of the needle tip.

- B. Take off the outer needle cap and keep it to remove the used needle after injection. Take off the inner needle cap and discard it.
You may have to perform the safety test several times before insulin is seen.
- If no insulin comes out, check for air bubbles and repeat the safety test two more times to remove them.
- If still no insulin comes out, the needle may be blocked. Change the needle and try again.
- If no insulin comes out after changing the needle, your SoloStar may be damaged. Do not use this SoloStar.
Step 4. Select the dose
You can set the dose in steps of 1 unit, from a minimum of 1 unit to a maximum of 80 units. If you need a dose greater than 80 units, you should give it as two or more injections.
- A.
Check that the dose window shows "0" following the safety test.
- B. Select your required dose (in the example below, the selected dose is 30 units). If you turn past your dose, you can turn back down.

- B. Select your required dose (in the example below, the selected dose is 30 units). If you turn past your dose, you can turn back down.
- Do not push the injection button while turning, as insulin will come out.
- You cannot turn the dosage selector past the number of units left in the pen. Do not force the dosage selector to turn. In this case, either you can inject what is remaining in the pen and complete your dose with a new SoloStar or use a new SoloStar for your full dose.
Step 5. Inject the dose
- A.
Use the injection method as instructed by your healthcare professional.
- B. Insert the needle into the skin.

- C. Deliver the dose by pressing the injection button in all the way. The number in the dose window will return to "0" as you inject.

- D. Keep the injection button pressed all the way in.
Slowly count to 10 before you withdraw the needle from the skin. This ensures that the full dose will be delivered. - B. Insert the needle into the skin.
Step 6. Remove and discard the needle
Always remove the needle after each injection and store SoloStar without a needle attached. This helps prevent:
- Contamination and/or infection
- Entry of air into the insulin reservoir and leakage of insulin, which can cause inaccurate dosing.
- A.
Put the outer needle cap back on the needle, and use it to unscrew the needle from the pen. To reduce the risk of accidental needle injury, never replace the inner needle cap.
- If your injection is given by another person, special caution must be taken by this person when removing and disposing the needle. Follow recommended safety measures for removal and disposal of needles (e.g., a one-handed capping technique) in order to reduce the risk of accidental needle injury and transmission of infectious diseases.
- B. Dispose of the needle safely. Used needles should be placed in sharps containers (such as red biohazard containers), hard plastic containers (such as detergent bottles), or metal containers (such as an empty coffee can). Such containers should be sealed and disposed of properly.
If you are giving an injection to another person, you should remove the needle in an approved manner to avoid needle-stick injuries.- C. Always put the pen cap back on the pen, then store the pen until your next injection.
Storage Instructions
Please check the leaflet for the insulin for complete instructions on how to store SoloStar.
If your SoloStar is in cool storage, take it out 1 to 2 hours before you inject to allow it to warm up. Cold insulin is more painful to inject.
Keep SoloStar out of the reach and sight of children.
Keep your SoloStar in cool storage (36°F–46°F [2°C–8°C]) until first use. Do not allow it to freeze. Do not put it next to the freezer compartment of your refrigerator or next to a freezer pack.
Once you take your SoloStar out of cool storage, for use or as a spare, you can use it for up to 28 days. During this time it can be safely kept at room temperature up to 86°F (30°C). Do not use it after this time.
SoloStar in use must not be stored in a refrigerator.Do not use SoloStar after the expiration date printed on the label of the pen or on the carton.
Protect SoloStar from light.
Discard your used SoloStar as required by your local authorities.
Maintenance
Protect your SoloStar from dust and dirt.
You can clean the outside of your SoloStar by wiping it with a damp cloth.
Do not soak, wash, or lubricate the pen as this may damage it.
Your SoloStar is designed to work accurately and safely. It should be handled with care. Avoid situations where SoloStar might be damaged. If you are concerned that your SoloStar may be damaged, use a new one.
This Instructions for Use has been approved by the U.S. Food and Drug Administration.
Revised: November 2019
sanofi-aventis U.S. LLC
Bridgewater, NJ 08807
A SANOFI COMPANY©2019 sanofi-aventis U.S. LLC
- 2 The brands listed are the registered trademarks of their respective owners and are not trademarks of sanofi-aventis U.S. LLC
-
PRINCIPAL DISPLAY PANEL - 10 mL Vial Carton
NDC: 0088-2220-33
Rx onlyLantus®
insulin glargine
injection100 units/mL (U-100)
For subcutaneous
injection onlyDo not mix with
other insulinsUse only if solution
is clear and colorless
with no particles visibleUse with U-100
syringe onlyOne 10 mL multiple-dose vial
SANOFI
-
PRINCIPAL DISPLAY PANEL - 3 mL Pen Carton
NDC: 0088-2219-05
RX ONLY
Lantus® SoloStar®
insulin glargine injectionFor Single Patient Use Only
100 units/mL (U-100)
Five 3 mL Prefilled Pens – Dispense in this sealed cartonSolution for injection in a disposable insulin delivery device
Do not mix with other insulins
For subcutaneous injection only
Use only if solution is clear and colorless with no particles visible
Use within 28 days after initial use
*Needles not included (see back panel)SANOFI
-
INGREDIENTS AND APPEARANCE
LANTUS
insulin glargine injection, solutionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 0088-2220 Route of Administration SUBCUTANEOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength insulin glargine (UNII: 2ZM8CX04RZ) (insulin glargine - UNII:2ZM8CX04RZ) insulin glargine 100 [iU] in 1 mL Inactive Ingredients Ingredient Name Strength zinc (UNII: J41CSQ7QDS) 30 ug in 1 mL METACRESOL (UNII: GGO4Y809LO) 2.7 mg in 1 mL glycerin (UNII: PDC6A3C0OX) 20 mg in 1 mL polysorbate 20 (UNII: 7T1F30V5YH) 20 ug in 1 mL water (UNII: 059QF0KO0R) hydrochloric acid (UNII: QTT17582CB) sodium hydroxide (UNII: 55X04QC32I) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 0088-2220-33 1 in 1 CARTON 09/23/2009 1 10 mL in 1 VIAL, GLASS; Type 0: Not a Combination Product 2 NDC: 0088-2220-34 1 in 1 CARTON 09/23/2009 2 10 mL in 1 VIAL, GLASS; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA021081 09/23/2009 LANTUS SOLOSTAR
insulin glargine injection, solutionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 0088-2219 Route of Administration SUBCUTANEOUS Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength insulin glargine (UNII: 2ZM8CX04RZ) (insulin glargine - UNII:2ZM8CX04RZ) insulin glargine 100 [iU] in 1 mL Inactive Ingredients Ingredient Name Strength zinc (UNII: J41CSQ7QDS) 30 ug in 1 mL METACRESOL (UNII: GGO4Y809LO) 2.7 mg in 1 mL glycerin (UNII: PDC6A3C0OX) 20 mg in 1 mL water (UNII: 059QF0KO0R) hydrochloric acid (UNII: QTT17582CB) sodium hydroxide (UNII: 55X04QC32I) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 0088-2219-00 1 in 1 CARTON 09/23/2009 1 3 mL in 1 SYRINGE; Type 2: Prefilled Drug Delivery Device/System (syringe, patch, etc.) 2 NDC: 0088-2219-05 5 in 1 CARTON 09/23/2009 2 NDC: 0088-2219-01 3 mL in 1 SYRINGE; Type 2: Prefilled Drug Delivery Device/System (syringe, patch, etc.) Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date BLA BLA021081 09/23/2009 Labeler - sanofi-aventis U.S. LLC (783243835) Establishment Name Address ID/FEI Business Operations Sanofi-Aventis Deutschland GmbH 313218430 MANUFACTURE(0088-2220, 0088-2219) , ANALYSIS(0088-2219) , LABEL(0088-2219) , PACK(0088-2219) , API MANUFACTURE(0088-2219, 0088-2220) Establishment Name Address ID/FEI Business Operations Sanofi S.p.A (Anagni) 338454274 MANUFACTURE(0088-2220) , ANALYSIS(0088-2220) , LABEL(0088-2220) , PACK(0088-2220)
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.