SUCCINYLCHOLINE CHLORIDE injection
Succinylcholine Chloride by
Drug Labeling and Warnings
Succinylcholine Chloride by is a Prescription medication manufactured, distributed, or labeled by Medical Purchasing Solutions, LLC. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use succinylcholine chloride injection safely and effectively. See full prescribing information for succinylcholine chloride injection.
Succinylcholine chloride injection injection, for intravenous or intramuscular use.
Initial U.S. Approval: 1952WARNING: VENTRICULAR DYSRHYTHMIAS, CARDIAC ARREST, AND DEATH FROM HYPERKALEMIC RHABDOMYOLYSIS IN PEDIATRIC PATIENTS See full prescribing information for complete boxed warning.
- Acute rhabdomyolysis with hyperkalemia followed by ventricular dysrhythmias, cardiac arrest, and death has occurred after use in apparently healthy pediatric patients who were subsequently found to have undiagnosed skeletal muscle myopathy. (5.1)
- When a healthy-appearing pediatric patient develops cardiac arrest soon after administration of SUCCINYLCHOLINE CHLORIDE INJECTION, not felt to be due to other causes, immediate treatment for hyperkalemia should be instituted. In the presence of signs of malignant hyperthermia, appropriate treatment should be instituted concurrently. (5.1)
- Reserve use of SUCCINYLCHOLINE CHLORIDE INJECTION in pediatric patients for emergency intubation or instances where immediate securing of the airway is necessary, or for intramuscular use when a suitable vein is inaccessible. (5.1)
RECENT MAJOR CHANGES
Boxed Warning 08/2021 Dosage and Administration (2.1) 08/2021 Warnings and Precautions (5.1, 5.2, 5.4, 5.9, 5.10, 5.12, 5.13, 5.14) 08/2021 INDICATIONS AND USAGE
INDICATIONS AND USAGE (1)
Succinylcholine Chloride Injection, is a depolarizing neuromuscular blocker indicated in adults and pediatric patients: (1)
- as an adjunct to general anesthesia (1)
- to facilitate tracheal intubation (1)
- to provide skeletal muscle relaxation during surgery or mechanical ventilation. (1)
(1)
DOSAGE AND ADMINISTRATION
DOSAGE AND ADMINISTRATION (2)
- For intravenous or intramuscular use only. (2.1)
- Individualize dosage after careful assessment of the patient. (2.1)
- Accidental administration of neuromuscular blocking agents may be fatal. Store Succinylcholine Chloride Injection with the cap and ferrule intact and in a manner that minimizes the possibility of selecting the wrong product. (2.1)
- See full prescribing information for Succinylcholine Chloride Injection dosage recommendations, preparation instructions, and administration information. (2.2, 2.3, 2.4, 2.5, 2.6)
DOSAGE FORMS AND STRENGTHS
CONTRAINDICATIONS
- Skeletal muscle myopathies (4)
- Known hypersensitivity to succinylcholine (4)
- After the acute phase of injury following major burns, multiple trauma, extensive denervation of skeletal muscle, or upper motor neuron injury (4)
- Personal or familial history of malignant hyperthermia (4)
(4)
WARNINGS AND PRECAUTIONS
- Anaphylaxis: Severe anaphylactic reactions to neuromuscular blocking agents, including succinylcholine, have been reported. Some cases have been life-threatening and fatal. Take necessary precautions, such as the immediate availability of appropriate emergency treatment. (5.2)
- Risk of Death due to Medication Errors: Unintended administration of Succinylcholine Chloride Injection may result in paralysis, respiratory arrest and death. Confirm proper selection of intended product and avoid confusion with other injectable solutions that are present in critical care and other clinical settings. (5.3)
- Hyperkalemia: Succinylcholine Chloride Injection may induce serious cardiac arrhythmias or cardiac arrest due to hyperkalemia. (5.4)
- Malignant Hyperthermia: Succinylcholine administration has been associated with acute onset of malignant hyperthermia. Continuously monitor temperature and expired CO2. Intravenous dantrolene sodium is recommended as an adjunct to supportive measures in the management of malignant hyperthermia. (5.5)
- Bradycardia: Intravenous bolus administration may result in profound bradycardia or, rarely, asystole. The incidence is higher following a second dose of succinylcholine. Pretreatment with anticholinergic agents (e.g., atropine) may reduce the occurrence of bradyarrhythmias. (5.6)
ADVERSE REACTIONS
Adverse reactions reported with succinylcholine are cardiac arrest, malignant hyperthermia, arrhythmias, bradycardia, tachycardia, hypertension, hypotension, hyperkalemia, prolonged respiratory depression or apnea. (6) (6)
(6)
To report SUSPECTED ADVERSE REACTIONS, contact STI PHARMA LLC at +1-888-301-9680 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch. (6)
DRUG INTERACTIONS
- Drugs that May Enhance the Neuromuscular Blocking Action of Succinylcholine: promazine, oxytocin, aprotinin, certain non-penicillin antibiotics, quinidine, β-adrenergic blockers, procainamide, lidocaine, trimethaphan, lithium carbonate, magnesium salts, quinine, chloroquine, isoflurane, desflurane, metoclopramide, terbutaline, and drugs that reduce plasma cholinesterase activity. (7.1)
Revised: 1/2022
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
WARNING: VENTRICULAR DYSRHYTHMIAS, CARDIAC ARREST, AND DEATH FROM HYPERKALEMIC RHABDOMYOLYSIS IN PEDIATRIC PATIENTS1. INDICATIONS & USAGE
2. DOSAGE & ADMINISTRATION
2.1 Important Dosage and Administration Information
2.2 Dosage Recommendations for Intravenous Use in Adults
2.3 Dosage Recommendations for Intravenous Use in Pediatric Patients
2.4 Dosage Recommendations for Intramuscular Use in Adults and Pediatric Patients
2.5 Preparation of Succinylcholine Chloride Injection
2.6 Drug Incompatibility
3. DOSAGE FORMS AND STRENGTHS
4. CONTRAINDICATIONS
5. WARNINGS AND PRECAUTIONS
5.1 Ventricular Dysrhythmias, Cardiac Arrest, and Death From Hyperkalemic Rhabdomyolysis in Pediatric Patients
5.2 Anaphylaxis
5.3 Risk of Death due to Medication Errors
5.4 Hyperkalemia
5.5 Malignant Hyperthermia
5.6 Bradycardia
5.7 Increased Intraocular Pressure
5.8 Prolonged Neuromuscular Block due to Phase II Block and Tachyphylaxis
5.9 Risk of Prolonged Neuromuscular Block in Patients with Reduced Plasma Cholinesterase Activity
5.10 Risk of Additional Trauma in Patients With Fractures or Muscle Spasms
5.11 Increase in Intracranial Pressure
5.12 Risk of Aspiration due to Increase in Intragastric Pressure
5.13 Prolonged Neuromuscular Block in Patients with Hypokalemia or Hypocalcemia
5.14 Risks due to Inadequate Anesthesia
7. DRUG INTERACTIONS
7.1 Drugs that May Affect the Neuromuscular Blocking Action of Succinylcholine Chloride Injection
8. USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.4 Pediatric Use
8.5 Geriatric Use
10. OVERDOSAGE
11. DESCRIPTION
12. CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13. NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
16. HOW SUPPLIED
- * Sections or subsections omitted from the full prescribing information are not listed.
-
BOXED WARNING
(What is this?)
WARNING: VENTRICULAR DYSRHYTHMIAS, CARDIAC ARREST, AND DEATH FROM HYPERKALEMIC RHABDOMYOLYSIS IN PEDIATRIC PATIENTSWARNING: VENTRICULAR DYSRHYTHMIAS, CARDIAC ARREST, AND DEATH FROM
HYPERKALEMIC RHABDOMYOLYSIS IN PEDIATRIC PATIENTS
- Acute rhabdomyolysis with hyperkalemia followed by ventricular dysrhythmias, cardiac arrest, and death has occurred after the administration of succinylcholine to apparently healthy pediatric patients who were subsequently found to have undiagnosed skeletal muscle myopathy, most frequently Duchenne muscular dystrophy [see Warnings and Precautions (5.1)].
- When a healthy appearing pediatric patient develops cardiac arrest within minutes after administration of SUCCINYLCHOLINE CHLORIDE INJECTION, not felt to be due to inadequate ventilation, oxygenation or anesthetic overdose, immediate treatment for hyperkalemia should be instituted. In the presence of signs of malignant hyperthermia, appropriate treatment should be instituted concurrently [see Warnings and Precautions (5.1)].
- Reserve the use of SUCCINYLCHOLINE CHLORIDE INJECTION in pediatric patients for emergency intubation or instances where immediate securing of the airway is necessary, e.g., laryngospasm, difficult airway, full stomach, or for intramuscular use when a suitable vein is inaccessible [see Warnings and Precautions (5.1)].
- 1. INDICATIONS & USAGE
-
2. DOSAGE & ADMINISTRATION
2.1 Important Dosage and Administration Information
- Succinylcholine Chloride Injection is for intravenous or intramuscular use only.
- Succinylcholine Chloride Injection must be titrated to effect by or under supervision of experienced clinicians who are familiar with its actions and with appropriate neuromuscular monitoring techniques.
- Succinylcholine Chloride Injection should be administered only by those skilled in the management of artificial respiration and only when facilities are instantly available for tracheal intubation and for providing adequate ventilation of the patient, including the administration of oxygen under positive pressure and the elimination of CO2. The clinician must be prepared to assist or control respiration.
- The dosage of Succinylcholine Chloride Injection should be individualized and should always be determined by the clinician after careful assessment of the patient.
- To avoid distress to the patient, do not administer Succinylcholine Chloride Injection before unconsciousness has been induced [see Warnings and Precautions (5.14)].
- The occurrence of bradyarrhythmias with administration of Succinylcholine Chloride Injection may be reduced by pretreatment with anticholinergics (e.g., atropine) [see Warnings and Precautions (5.6)].
- Monitor neuromuscular function with a peripheral nerve stimulator when using Succinylcholine Chloride Injection by infusion [see Dosage and Administration (2.2), Warnings and Precautions (5.8)].
- Visually inspect Succinylcholine Chloride Injection for particulate matter and discoloration prior to administration, whenever solution and container permit. Do not administer solutions that are not clear and colorless.
- Succinylcholine Chloride Injection supplied in single-dose vials must be diluted before use. Succinylcholine Chloride Injection supplied in multiple-dose vials does not require dilution before use [see Dosage and Administration (2.5)].
Risk of Medication Errors Accidental administration of neuromuscular blocking agents may be fatal. Store Succinylcholine Chloride Injection with the cap and ferrule intact and in a manner that minimizes the possibility of selecting the wrong product [see Warnings and Precautions (5.3)].
2.2 Dosage Recommendations for Intravenous Use in Adults
For Short Surgical Procedures The average dose required to produce neuromuscular blockade and to facilitate tracheal intubation is 0.6 mg/kg Succinylcholine Chloride Injection given intravenously. The optimum intravenous dose of Succinylcholine Chloride Injection will vary among patients and may be from 0.3 mg/kg to 1.1 mg/kg for adults. Following intravenous administration of doses in this range, neuromuscular blockade develops in about 1 minute; maximum blockade may persist for about 2 minutes, after which recovery takes place within 4 to 6 minutes. A 5 to 10 mg intravenous test dose of Succinylcholine Chloride Injectionmay be used to determine the sensitivity of the patient and the individual recovery time [see Warnings and Precautions (5.9)].
For Long Surgical Procedures
Continuous Intravenous Infusion
The dosage of Succinylcholine Chloride Injection administered by continuous intravenous infusion depends upon the duration of the surgical procedure and the need for muscle relaxation.
Diluted Succinylcholine Chloride Injection solutions containing from 1 mg/mL to 2 mg/mL succinylcholine have commonly been used for continuous intravenous infusion [see Dosage and Administration (2.5)]. The more dilute solution (1 mg/mL) is probably preferable from the standpoint of ease of control of the rate of administration of Succinylcholine Chloride Injection and, hence, of relaxation. This diluted Succinylcholine Chloride Injection solution containing 1 mg/mL succinylcholine may be administered intravenously at a rate of 0.5 mg (0.5 mL) per minute to 10 mg (10 mL) per minute to obtain the required amount of relaxation. The amount required per minute will depend upon the individual response as well as the degree of relaxation required. The average rate of continuous intravenous infusion for an adult ranges between 2.5 mg per minute and 4.3 mg per minute.
Monitor neuromuscular function with a peripheral nerve stimulator when using Succinylcholine Chloride Injection by infusion in order to avoid overdose, detect development of Phase II block, follow its rate of recovery, and assess the effects of reversing agents [see Warnings and Precautions (5.8)].
Intermittent Intravenous Injection
Intermittent intravenous injections of Succinylcholine Chloride Injection may also be used to provide muscle relaxation for long procedures. An intravenous injection of 0.3 mg/kg to 1.1 mg/kg may be given initially, followed, at appropriate intervals, by further intravenous injections of 0.04 mg/kg to 0.07 mg/kg to maintain the degree of relaxation required.
2.3 Dosage Recommendations for Intravenous Use in Pediatric Patients
For emergency tracheal intubation or in instances where immediate securing of the airway is necessary, the intravenous dose of Succinylcholine Chloride Injection is 2 mg/kg for infants and other small pediatric patients; for older pediatric patients and adolescents the intravenous dose is 1 mg/kg [see Warnings and Precautions (5.1), Use in Specific Populations (8.4)]. The effective dose of Succinylcholine Chloride Injection in pediatric patients may be higher than that predicted by body weight dosing alone. For example, the usual adult intravenous dose of 0.6 mg/kg is comparable to a dose of 2 mg/kg to 3 mg/kg in neonates and infants up to 6 months of age and 1 mg/kg to 2 mg/kg in infants up to 2 years of age [see Clinical Pharmacology (12.3)].
2.4 Dosage Recommendations for Intramuscular Use in Adults and Pediatric Patients
If a suitable vein is inaccessible, Succinylcholine Chloride Injection may be administered intramuscularly at a dose of up to 3 mg/kg to 4 mg/kg to infants, older pediatric patients, or adults. The total dose administered by the intramuscular route should not exceed 150 mg. The onset of effect of succinylcholine given intramuscularly is usually observed in about 2 to 3 minutes.
2.5 Preparation of Succinylcholine Chloride Injection
Succinylcholine Chloride Injection supplied in single-dose vials must be diluted before use. Succinylcholine Chloride Injectionsupplied in multiple-dose vials does not require dilution before use.
Succinylcholine Chloride Injection may be diluted to 1 mg/mL or 2 mg/mL in a solution such as:
- 5% Dextrose Injection, USP, or
- 0.9% Sodium Chloride Injection, USP
Prepare the diluted Succinylcholine Chloride Injection solution for single patient use only. Store the diluted Succinylcholine Chloride Injection solution in a refrigerator [2 °C to 8 °C (36 °F to 46 °F)] and use within 24 hours after preparation. Visually inspect the diluted Succinylcholine Chloride Injection solution for particulate matter and discoloration prior to administration. Do not administer solutions that are not clear and colorless. Discard any unused portion of the diluted Succinylcholine Chloride Injection solution.
- 3. DOSAGE FORMS AND STRENGTHS
-
4. CONTRAINDICATIONS
Succinylcholine Chloride Injection is contraindicated:
- in patients with skeletal muscle myopathies [see Warnings and Precautions (5.1)]
- in patients with known hypersensitivity to succinylcholine. Severe anaphylactic reactions to succinylcholine have been reported [see Warnings and Precautions (5.2)]
- after the acute phase of injury following major burns, multiple trauma, extensive denervation of skeletal muscle, or upper motor neuron injury, which may result in severe hyperkalemia and cardiac arrest [see Warnings and Precautions (5.4)]
- in patients with personal or familial history of malignant hyperthermia [see Warnings and Precautions (5.5)]
-
5. WARNINGS AND PRECAUTIONS
5.1 Ventricular Dysrhythmias, Cardiac Arrest, and Death From Hyperkalemic Rhabdomyolysis in Pediatric Patients
There have been reports of ventricular dysrhythmias, cardiac arrest, and death secondary to acute rhabdomyolysis with hyperkalemia in apparently healthy pediatric patients who received succinylcholine. Many of these pediatric patients were subsequently found to have a skeletal muscle myopathy such as Duchenne muscular dystrophy whose clinical signs were not obvious.
The syndrome often presented as sudden cardiac arrest within minutes after the administration of succinylcholine. These pediatric patients were usually, but not exclusively, males, and most frequently 8 years of age or younger. There have also been reports in adolescents. There may be no signs or symptoms to alert the practitioner to which patients are at risk. A careful history and physical may identify developmental delays suggestive of a myopathy. A preoperative creatine kinase could identify some but not all patients at risk.
When a healthy-appearing pediatric patient develops cardiac arrest within minutes after administration of Succinylcholine Chloride Injection, not felt to be due to inadequate ventilation, oxygenation or anesthetic overdose, immediate treatment for hyperkalemia should be instituted. Due to the abrupt onset of this syndrome, routine resuscitative measures are likely to be unsuccessful. Careful monitoring of the electrocardiogram may alert the practitioner to peaked T-waves (an early sign). Administration of intravenous calcium, bicarbonate, and glucose with insulin, with hyperventilation have resulted in successful resuscitation in some of the reported cases. Extraordinary and prolonged resuscitative efforts have been effective in some cases. In addition, in the presence of signs of malignant hyperthermia, appropriate treatment should be initiated concurrently [see Warnings and Precautions (5.5)].
Because it is difficult to identify which patients are at risk, reserve the use of Succinylcholine Chloride Injection in pediatric patients for emergency intubation or instances where immediate securing of the airway is necessary, e.g., laryngospasm, difficult airway, full stomach, or for intramuscular use when a suitable vein is inaccessible.
5.2 Anaphylaxis
Severe anaphylactic reactions to neuromuscular blocking agents, including succinylcholine, have been reported. These reactions have, in some cases, been life-threatening and fatal. Due to the potential severity of these reactions, the necessary precautions, such as the immediate availability of appropriate emergency treatment, should be taken.
Allergic cross-reactivity between neuromuscular blocking agents, both depolarizing and non-depolarizing, has been reported in this class of drugs. Therefore, assess patients for previous anaphylactic reactions to other neuromuscular blocking agents before administering Succinylcholine Chloride Injection.
5.3 Risk of Death due to Medication Errors
Administration of Succinylcholine Chloride Injection results in paralysis, which may lead to respiratory arrest and death; this progression may be more likely to occur in a patient for whom it is not intended. Confirm proper selection of intended product and avoid confusion with other injectable solutions that are present in critical care and other clinical settings. If another healthcare provider is administering the product, ensure that the intended dose is clearly labeled and communicated.
5.4 Hyperkalemia
Succinylcholine Chloride Injection may induce serious cardiac arrhythmias or cardiac arrest due to hyperkalemia in patients with electrolyte abnormalities and those who may have digitalis toxicity.
Succinylcholine Chloride Injection is contraindicated after the acute phase of injury following major burns, multiple trauma, extensive denervation of skeletal muscle, or upper motor neuron injury [see Contraindications (4)]. The risk of hyperkalemia in these patients increases over time and usually peaks at 7 to 10 days after the injury. The risk is dependent on the extent and location of the injury. The precise time of onset and the duration of the risk period are undetermined.
Patients with chronic abdominal infection, subarachnoid hemorrhage, or conditions causing degeneration of central and peripheral nervous systems are at an increased risk of developing severe hyperkalemia after Succinylcholine Chloride Injection administration.
Consider avoiding use of Succinylcholine Chloride Injection in these patients or verify the patient’s baseline potassium levels are within the normal range prior to Succinylcholine Chloride Injection administration.
5.5 Malignant Hyperthermia
Succinylcholine administration has been associated with acute onset of malignant hyperthermia, a potentially fatal hypermetabolic state of skeletal muscle. The risk of developing malignant hyperthermia following succinylcholine administration increases with the concomitant administration of volatile anesthetics. Malignant hyperthermia frequently presents as intractable spasm of the jaw muscles (masseter spasm) which may progress to generalized rigidity, increased oxygen demand, tachycardia, tachypnea and profound hyperpyrexia. Successful outcome depends on recognition of early signs, such as jaw muscle spasm, acidosis, or generalized rigidity to initial administration of succinylcholine for tracheal intubation, or failure of tachycardia to respond to deepening anesthesia. Skin mottling, rising temperature and coagulopathies may occur later in the course of the hypermetabolic process. Recognition of the syndrome is a signal for discontinuance of anesthesia, attention to increased oxygen consumption, correction of acidosis, support of circulation, assurance of adequate urinary output and institution of measures to control rising temperature. Intravenous dantrolene sodium is recommended as an adjunct to supportive measures in the management of malignant hyperthermia. Consult the dantrolene prescribing information for additional information about the management of malignant hyperthermic crisis. Continuous monitoring of temperature and expired CO 2 is recommended as an aid to early recognition of malignant hyperthermia.
5.6 Bradycardia
Intravenous bolus administration of Succinylcholine Chloride Injection in pediatric patients (including infants) may result in profound bradycardia or, rarely, asystole. In both adult and pediatric patients the incidence of bradycardia, which may progress to asystole, is higher following a second dose of succinylcholine. The incidence and severity of bradycardia is higher in pediatric patients than adults. Whereas bradycardia is common in pediatric patients after an initial dose of 1.5 mg/kg, bradycardia is seen in adults only after repeated exposure. Pretreatment with anticholinergic agents (e.g., atropine) may reduce the occurrence of bradyarrhythmias.
5.7 Increased Intraocular Pressure
Succinylcholine causes an increase in intraocular pressure. Avoid Succinylcholine Chloride Injection in instances in which an increase in intraocular pressure is undesirable (e.g., narrow angle glaucoma, penetrating eye injury) unless the potential benefit of its use outweighs the potential risk.
5.8 Prolonged Neuromuscular Block due to Phase II Block and Tachyphylaxis
When Succinylcholine Chloride Injection is given over a prolonged period of time, the characteristic depolarization block of the myoneural junction (Phase I block) may change to a block with characteristics superficially resembling a non-depolarizing block (Phase II block). Prolonged respiratory muscle paralysis or weakness may be observed in patients manifesting this transition to Phase II block. Tachyphylaxis occurs with repeated administration [see Clinical Pharmacology (12.2)].
When Phase II block is suspected in cases of prolonged neuromuscular blockade, positive diagnosis should be made by peripheral nerve stimulation, prior to administration of any anticholinesterase drug. Reversal of Phase II block is a medical decision which must be made upon the basis of the patient, clinical pharmacology, and the experience and judgment of the clinician. The presence of Phase II block is indicated by fade of responses to successive stimuli (preferably "train of four"). The use of an anticholinesterase drug such as neostigmine to reverse Phase II block should be accompanied by appropriate doses of an anticholinergic drug to prevent disturbances of cardiac rhythm. After adequate reversal of Phase II block with an anticholinesterase agent, the patient should be continually observed for at least 1 hour for signs of return of muscle relaxation. Reversal should not be attempted unless: (1) a peripheral nerve stimulator is used to determine the presence of Phase II block (since anticholinesterase agents will potentiate succinylcholine-induced Phase I block), and (2) spontaneous recovery of muscle twitch has been observed for at least 20 minutes and has reached a plateau with further recovery proceeding slowly; this delay is to ensure complete hydrolysis of succinylcholine by plasma cholinesterase prior to administration of the anticholinesterase agent. Should the type of block be misdiagnosed, depolarization of the type initially induced by succinylcholine (i.e., Phase I block) will be prolonged by an anticholinesterase agent.
5.9 Risk of Prolonged Neuromuscular Block in Patients with Reduced Plasma Cholinesterase Activity
Succinylcholine Chloride Injection is not recommended in patients with known reduced plasma cholinesterase (pseudocholinesterase) activity due to the likelihood of prolonged neuromuscular block following administration of Succinylcholine Chloride Injection in such patients.
Plasma cholinesterase activity may be diminished in the presence of genetic abnormalities of plasma cholinesterase (e.g., patients heterozygous or homozygous for atypical plasma cholinesterase gene), pregnancy, severe liver or kidney disease, malignant tumors, infections, burns, anemia, decompensated heart disease, peptic ulcer, or myxedema. Plasma cholinesterase activity may also be diminished by chronic administration of oral contraceptives, glucocorticoids, or certain monoamine oxidase inhibitors and by irreversible inhibitors of plasma cholinesterase (e.g., organophosphate insecticides, echothiophate, and certain antineoplastic drugs) [see Drug Interactions (7.1)].
Patients homozygous for atypical plasma cholinesterase gene (1 in 2,500 patients) are extremely sensitive to the neuromuscular blocking effect of succinylcholine.
If Succinylcholine Chloride Injectionis administered to a patient homozygous for atypical plasma cholinesterase, resulting apnea or prolonged muscle paralysis should be treated with controlled respiration.
5.10 Risk of Additional Trauma in Patients With Fractures or Muscle Spasms
Succinylcholine Chloride Injection should be employed with caution in patients with fractures or muscle spasm because the initial muscle fasciculations may cause additional trauma.
Monitor neuromuscular transmission and the development of fasciculations throughout the use of neuromuscular blocking agents.
5.11 Increase in Intracranial Pressure
Succinylcholine Chloride Injection may cause a transient increase in intracranial pressure; however, adequate anesthetic induction prior to administration of Succinylcholine Chloride Injection will minimize this effect.
5.12 Risk of Aspiration due to Increase in Intragastric Pressure
Succinylcholine may increase intragastric pressure, which could result in regurgitation and possible aspiration
of stomach contents. Evaluate patients at risk for aspiration and regurgitation.Monitor patients during induction of anesthesia and neuromuscular blockade for clinical signs of vomiting and/or aspiration.
5.13 Prolonged Neuromuscular Block in Patients with Hypokalemia or Hypocalcemia
Neuromuscular blockade may be prolonged in patients with hypokalemia (e.g., after severe vomiting, diarrhea, digitalisation and diuretic therapy) or hypocalcemia (e.g., after massive transfusions). Correct severe electrolyte disturbances when possible.
In order to help preclude possible prolongation of neuromuscular block, monitor neuromuscular transmission throughout the use of Succinylcholine Chloride Injection.
5.14 Risks due to Inadequate Anesthesia
Neuromuscular blockade in the conscious patient can lead to distress. Use Succinylcholine Chloride Injection in the presence of appropriate sedation or general anesthesia. Monitor patients to ensure that the level of anesthesia is adequate. In emergency situations, however, it may be necessary to administer Succinylcholine Chloride Injection before unconsciousness is induced.
-
ADVERSE REACTIONS
The following clinically significant adverse reactions are discussed in greater detail in other sections of the labeling:
- Ventricular Dysrhythmias, Cardiac Arrest, and Death from Hyperkalemic Rhabdomyolysis in Pediatric Patients [see Warnings and Precautions (5.1)]
- Anaphylaxis [ see Warnings and Precautions (5.2)]
- Hyperkalemia [ see Warnings and Precautions (5.4)]
- Malignant Hyperthermia [ see Warnings and Precautions (5.5)]
- Bradycardia [ see Warnings and Precautions (5.6)]
- Increase in Intraocular Pressure [ see Warnings and Precautions (5.7)]
- Prolonged Neuromuscular Block due to Phase II Block and Tachyphylaxis [ see Warnings and Precautions (5.8)]
The following adverse reactions associated with the use of succinylcholine were identified in clinical studies or postmarketing reports. Because some of these reactions were reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure:
Cardiovascular disorders: Cardiac arrest, arrhythmias, bradycardia, tachycardia, hypertension, hypotension
Electrolyte disorders: Hyperkalemia
Eye disorders: Increased intraocular pressure
Gastrointestinal disorders: Excessive salivation
Immune system disorders: Hypersensitivity reactions including anaphylaxis (in some cases life-threatening and fatal)
Musculoskeletal disorders: Malignant hyperthermia, rhabdomyolysis with possible myoglobinuric acute renal failure, muscle
fasciculation, jaw rigidity, postoperative muscle pain
Respiratory disorders: Prolonged respiratory depression or apnea
Skin disorders: Rash
-
7. DRUG INTERACTIONS
7.1 Drugs that May Affect the Neuromuscular Blocking Action of Succinylcholine Chloride Injection
Drugs that may enhance the neuromuscular blocking action of succinylcholine include: promazine, oxytocin, aprotinin, certain non-penicillin antibiotics, quinidine, β-adrenergic blockers, procainamide, lidocaine, trimethaphan, lithium carbonate, magnesium salts, quinine, chloroquine, isoflurane, desflurane, metoclopramide, and terbutaline.
The neuromuscular blocking effect of succinylcholine may be enhanced by drugs that reduce plasma cholinesterase activity (e.g., chronically administered oral contraceptives, glucocorticoids, or certain monoamine oxidase inhibitors) or by drugs that irreversibly inhibit plasma cholinesterase [see Warnings and Precautions (5.9)].
If other neuromuscular blocking agents are to be used during the same procedure, consider the possibility of a synergistic or antagonistic effect
-
8. USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary Available data from published literature from case reports and case series over decades of use with succinylcholine during pregnancy have not identified a drug-associated risk of major birth defects, miscarriage, or adverse maternal or fetal outcomes. Succinylcholine is used commonly during delivery by caesarean section to provide muscle relaxation. If succinylcholine is used during labor and delivery, there is a risk for prolonged apnea in some pregnant women (see Clinical Considerations). Animal reproduction studies have not been conducted with succinylcholine chloride.
The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2-4% and 15-20%, respectively.
Clinical Considerations
Maternal Adverse Reactions
Plasma cholinesterase levels are decreased by approximately 24% during pregnancy and for several days postpartum which can prolong the effect of succinylcholine. Therefore, some pregnant patients may experience prolonged apnea.
Fetal/Neonatal Adverse Reactions
Apnea and flaccidity may occur in the newborn after repeated high doses to, or in the presence of atypical plasma cholinesterase in, the mother.
Labor or Delivery
Succinylcholine is commonly used to provide muscle relaxation during delivery by caesarean section. Succinylcholine is known to cross the placental barrier in an amount that is dependent on the concentration gradient between the maternal and fetal circulation.
8.2 Lactation
Risk Summary There are no data on the presence of succinylcholine or its metabolite in either human or animal milk, the effects on the breastfed infant, or the effects on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for Succinylcholine Chloride Injection and any potential adverse effects on the breastfed infant from Succinylcholine Chloride Injection or from the underlying maternal condition.
8.4 Pediatric Use
Safety and effectiveness of succinylcholine chloride have been established in pediatric patient age groups, neonate to adolescent. Because of a risk of ventricular dysrhythmias, cardiac arrest, and death from hyperkalemic rhabdomyolysis in pediatric patients, reserve the use of Succinylcholine Chloride Injection in pediatric patients for emergency intubation or instances where immediate securing of the airway is necessary, e.g., laryngospasm, difficult airway, full stomach, or for intramuscular use when a suitable vein is inaccessible [see Warnings and Precautions (5.1)].
Intravenous bolus administration of Succinylcholine Chloride Injection in pediatric patients (including infants) may result in profound bradycardia or, rarely, asystole. The incidence and severity of bradycardia is higher in pediatric patients than adults [see Warnings and Precautions (5.6)].
The effective dose of Succinylcholine Chloride Injection in pediatric patients may be higher than that predicted by body weight dosing alone [see Dosage and Administration (2.3)].
8.5 Geriatric Use
Clinical studies of Succinylcholine Chloride Injection did not include sufficient numbers of subjects aged 65 years and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients.
In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
-
10. OVERDOSAGE
Overdosage with Succinylcholine Chloride Injection may result in neuromuscular block beyond the time needed for surgery and anesthesia. This may be manifested by skeletal muscle weakness, decreased respiratory reserve, low tidal volume, or apnea. The primary treatment is maintenance of a patent airway and respiratory support until recovery of normal respiration is assured. Depending on the dose and duration of Succinylcholine Chloride Injection administration, the characteristic depolarizing neuromuscular block (Phase I) may change to a block with characteristics superficially resembling a non-depolarizing block (Phase II) [see Warnings and Precautions (5.8)].
-
11. DESCRIPTION
Succinylcholine Chloride Injection, USP is a sterile, nonpyrogenic solution to be used as a short-acting, depolarizing neuromuscular blocker for intravenous or intramuscular use. Succinylcholine Chloride Injection contains succinylcholine chloride as the active pharmaceutical ingredient.
Succinylcholine Chloride, USP is chemically designated C 14H 30Cl 2N 2O 4 and its molecular weight is 361.31. The chemical name of succinylcholine chloride is ethanaminium, 2,2'-[(1,4-dioxo-1,4 butanediyl)bis(oxy)]bis[N,N,N-trimethyl-], dichloride. Succinylcholine chloride is a diquaternary base consisting of the dichloride salt of the dicholine ester of succinic acid. It is a white, odorless, slightly bitter powder, very soluble in water. It has the following structural formula:
Succinylcholine Chloride Injection 200 mg/10 mL (20 mg/mL) is intended for multiple-dose administration and contains preservative. Each 1 mL of Succinylcholine Chloride Injection 200 mg/10 mL (20 mg/mL) multiple-dose fliptop vials contains: 20 mg of succinylcholine anhydrous (equivalent to 22.65 mg of Succinylcholine Chloride, USP), 1.8 mg of methylparaben and 0.2 mg of propylparaben as preservatives, 4.70 mg of sodium chloride as
iso-osmotic agent, and sodium hydroxide and hydrochloric acid as pH adjusters in water for injection. The pH of the solution is between 3.0 and 4.5, with an osmolarity of 0.338 mOsm/mL (calc.). -
12. CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Succinylcholine is a depolarizing neuromuscular blocker. As does acetylcholine, it combines with the cholinergic receptors of the motor end plate to produce depolarization. This depolarization may be observed as fasciculations. Subsequent neuromuscular transmission is inhibited so long as adequate concentration of succinylcholine remains at the receptor site. Onset of flaccid paralysis is rapid (less than one minute after intravenous administration), and with single administration lasts approximately 4 to 6 minutes.
The paralysis following administration of succinylcholine is progressive, with differing sensitivities of different muscles. This initially involves consecutively the levator muscles of the face, muscles of the glottis and finally the intercostals and the diaphragm and all other skeletal muscles.
12.2 Pharmacodynamics
Depending on the dose and duration of succinylcholine administration, the characteristic depolarizing neuromuscular block (Phase I block) may change to a block with characteristics superficially resembling a non-depolarizing block (Phase II block). This may be associated with prolonged respiratory muscle paralysis or weakness in patients who manifest the transition to Phase II block. Tachyphylaxis occurs with repeated administration [see Warnings and Precautions (5.8)]. The transition from Phase I to Phase II block has been reported in 7 of 7 patients studied under halothane anesthesia after an accumulated dose of 2 to 4 mg/kg succinylcholine (administered in repeated, divided doses). The onset of Phase II block coincided with the onset of tachyphylaxis and prolongation of spontaneous recovery. In another study, using balanced anesthesia (N2O/O2/narcotic-thiopental) and succinylcholine infusion, the transition was less abrupt, with great individual variability in the dose of succinylcholine required to produce Phase II block. Of 32 patients studied, 24 developed Phase II block. Tachyphylaxis was not associated with the transition to Phase II block, and 50% of the patients who developed Phase II block experienced prolonged recovery [see Warnings and Precautions (5.8)].
Succinylcholine has no direct effect on the myocardium. Succinylcholine stimulates both autonomic ganglia and muscarinic receptors which may cause changes in cardiac rhythm, including cardiac arrest. Changes in rhythm, including cardiac arrest, may also result from vagal stimulation, which may occur during surgical procedures, or from hyperkalemia, particularly in pediatric patients [see Warnings and Precautions (5.1, 5.4, 5.6), Use in Specific Populations (8.4)]. These effects are enhanced by halogenated anesthetics.
Succinylcholine causes an increase in intraocular pressure immediately after its injection and during the fasciculation phase, and increases which may persist after onset of complete paralysis [see Warnings and Precautions (5.7)].
Succinylcholine may cause increases in intracranial pressure immediately after its injection and during the fasciculation phase [see Warnings and Precautions (5.11)].
As with other neuromuscular blocking agents, the potential for releasing histamine is present following succinylcholine administration. Signs and symptoms of histamine-mediated release such as flushing, hypotension and bronchoconstriction are, however, uncommon with normal clinical usage.
Succinylcholine has no effect on consciousness, pain threshold or cerebration [see Warnings and Precautions (5.14)].
Succinylcholine has no direct action on the uterus or other smooth muscle structures.
12.3 Pharmacokinetics
Elimination Succinylcholine levels were reported to be below the detection limit of 2 μg/mL after 2.5 minutes of an intravenous bolus dose of 1 or 2 mg/kg in 14 anesthetized patients.
Metabolism
Succinylcholine is rapidly hydrolyzed by plasma cholinesterase to succinylmonocholine (which possesses clinically insignificant depolarizing muscle relaxant properties) and then more slowly to succinic acid and choline .
Excretion
About 10% of the drug is excreted unchanged in the urine.
Specific Populations
Pediatric Patients
Due to the relatively large volume of distribution in the pediatric patient versus the adult patient, the effective dose of Succinylcholine Chloride Injection in pediatric patients may be higher than that predicted by body weight dosing alone [see Dosage and Administration (2.3)].
-
13. NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis There have been no long-term studies performed in animals to evaluate carcinogenic potential of succinylcholine.
Mutagenesis Adequate studies have not been completed to evaluate the genotoxic potential of succinylcholine.
Impairment of Fertility There are no studies to evaluate the potential impact of succinylcholine on fertility.
-
16. HOW SUPPLIED
Succinylcholine Chloride Injection, USP is supplied as a clear, colorless solution in the following concentration and package:
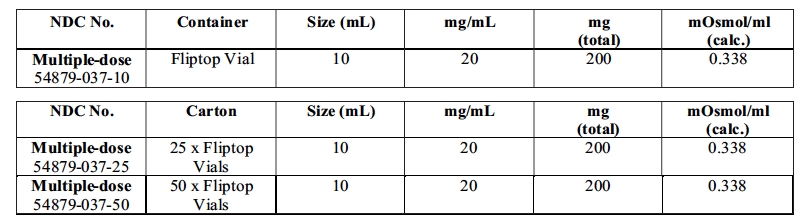
Refrigeration of the undiluted agent will assure full potency until expiration date. All units carry a date of expiration.
Store in refrigerator 2° to 8°C (36° to 46°F). The multi-dose vials are stable for up to 14 days at room temperature without significant loss of potency.
Manufactured in India for:
STI Pharma LLC
Newtown, PA 18940
1.888.301.9680
Revised: 09/2021 - SPL UNCLASSIFIED SECTION
- SPL UNCLASSIFIED SECTION
-
PACKAGE LABEL.PRINCIPAL DISPLAY PANEL
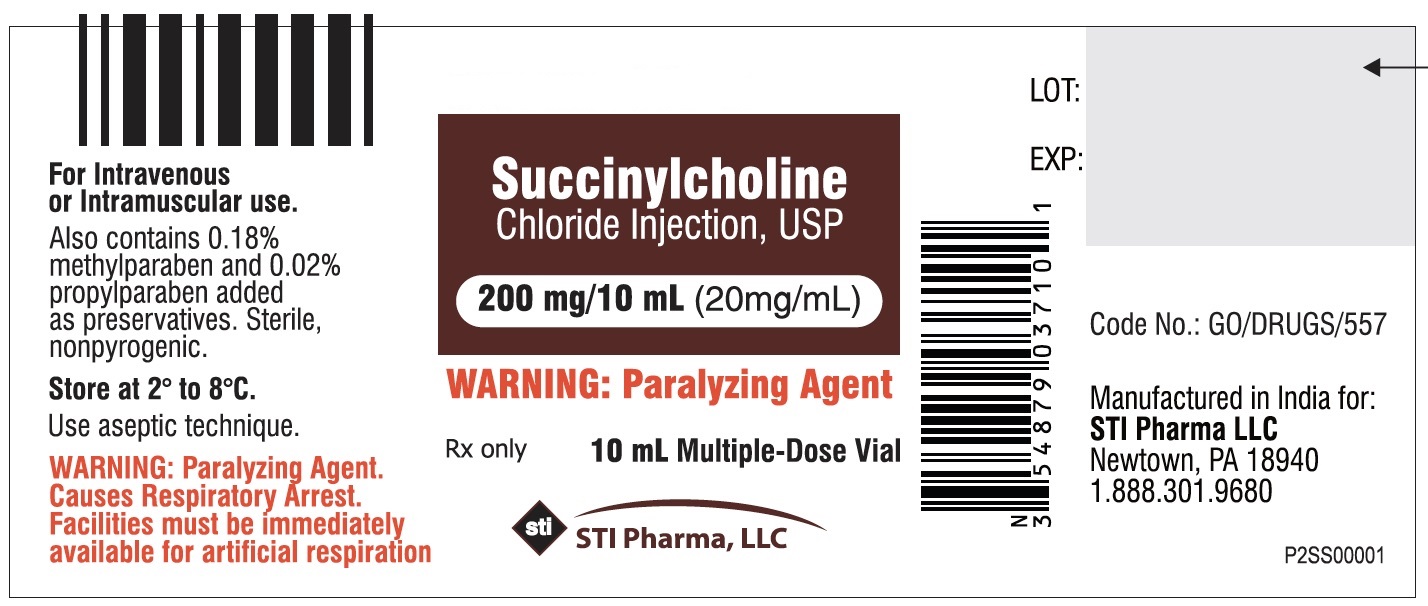
VIAL LABEL
Rx Only
For Intravenous or Intramuscular use.
Multiple-dose vial.
Succinylcholine Chloride Injection, USP.
200 mg / 10 mL
(20mg/mL)
Vial Label
10 mL multiple-dose vial.
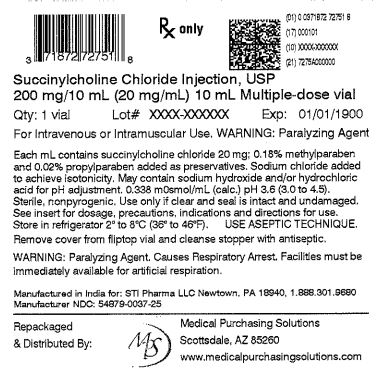
OUTER PACKAGE
NDC: 71872-7275-1
Rx Only
For Intravenous or Intramuscular use..
Succinylcholine Chloride Injection, USP.
200 mg / 10 mL
1 x 10 mL Multiple-dose vial
(20mg/mL)
-
INGREDIENTS AND APPEARANCE
SUCCINYLCHOLINE CHLORIDE
succinylcholine chloride injectionProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 71872-7275(NDC:54879-037) Route of Administration INTRAVENOUS, INTRAMUSCULAR Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength SUCCINYLCHOLINE CHLORIDE (UNII: I9L0DDD30I) (SUCCINYLCHOLINE - UNII:J2R869A8YF) SUCCINYLCHOLINE CHLORIDE 20 mg in 1 mL Inactive Ingredients Ingredient Name Strength SODIUM CHLORIDE (UNII: 451W47IQ8X) SODIUM HYDROXIDE (UNII: 55X04QC32I) HYDROCHLORIC ACID (UNII: QTT17582CB) METHYLPARABEN (UNII: A2I8C7HI9T) 1.8 mg in 1 mL PROPYLPARABEN (UNII: Z8IX2SC1OH) 0.2 mg in 1 mL Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 71872-7275-1 1 in 1 BAG 01/03/2022 1 10 mL in 1 VIAL, GLASS; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA214308 11/03/2020 Labeler - Medical Purchasing Solutions, LLC (601458529) Establishment Name Address ID/FEI Business Operations Medical Purchasing Solutions, LLC 601458529 repack(71872-7275)
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.