These highlights do not include all the information needed to use LAMIVUDINE TABLETS safely and effectively. See full prescribing information for LAMIVUDINE TABLETS. LAMIVUDINE Tablets Initial U.S. Approval: 1995
Lamivudine by
Drug Labeling and Warnings
Lamivudine by is a Prescription medication manufactured, distributed, or labeled by REMEDYREPACK INC.. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
LAMIVUDINE- lamivudine tablet, film coated
REMEDYREPACK INC.
----------
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use LAMIVUDINE TABLETS safely and effectively. See full prescribing information for LAMIVUDINE TABLETS.
LAMIVUDINE Tablets Initial U.S. Approval: 1995
WARNING: LACTIC ACIDOSIS AND SEVERE HEPATOMEGALY, EXACERBATIONS OF HEPATITS B, and DIFFERENT FORMULATIONS OF LAMIVUDINE
|
FULL PRESCRIBING INFORMATION
WARNING: RISK OF LACTIC ACIDOSIS, EXACERBATIONS OF HEPATITIS B IN CO- INFECTED PATIENTS UPON DISCONTINUATION OF LAMIVUDINE, DIFFERENT FORMULATIONS OF LAMIVUDINE.
WARNING: LACTIC ACIDOSIS AND SEVERE HEPATOMEGALY, EXACERBATIONS OF HEPATITIS B, and DIFFERENT FORMULATIONS OF LAMIVUDINE.Lactic Acidosis and Severe Hepatomegaly with Steatosis
Lactic acidosis and severe hepatomegaly with steatosis, including fatal cases, have been reported with the use of nucleoside analogues and other antiretrovirals. Discontinue lamivudine tablets if clinical or laboratory findings suggestive of lactic acidosis or pronounced hepatotoxicity occur
[see
Warnings and Precautions (5.1)].
Exacerbations of Hepatitis B
Severe acute exacerbations of hepatitis B have been reported in patients who are co-infected with hepatitis B virus (HBV) and human immunodeficiency virus (HIV-l) and have discontinued lamivudine. Hepatic function should be monitored closely with both clinical and laboratory follow-up for at least several months in patients who discontinue lamivudine and are co-infected with HIV-l and HBV. If appropriate, initiation of anti-hepatitis B therapy may be warranted
[see
Warnings and Precautions (5.2)]
.
Important Differences among Lamivudine-Containing Products
Lamivudine tablets (used to treat HIV-l infection) contain a higher dose of the active ingredient (lamivudine) than EPIVIR-HBV
® Tablets (used to treat chronic HBV infection). Patients with HIV-l infection should receive only dosage forms appropriate for treatment of HIV-1
[see
Warnings and Precautions (5.2)]
.
1 INDICATIONS & USAGE
Lamivudine Tablet is a nucleoside analogue indicated in combination with other antiretroviral agents for the treatment of human immunodeficiency virus type 1 (HIV-l) infection.
Limitation of use:
The dosage of this product is for HIV-1and not for HBV.
2 DOSAGE & ADMINISTRATION
2.1 Recommended Dosage for Adult Patients
The recommended dosage of lamivudine tablets in HIV-1-infected adults is 300 mg daily, administered as either 150 mg taken orally twice daily or 300 mg taken orally once daily with or without food. If lamivudine is administered to a patient infected with HIV-1 and HBV, the dosage indicated for HIV-l therapy should be used as part of an appropriate combination regimen [see Warnings and Precautions ( 5.2)].
2.2 Recommended Dosage for Pediatric Patients
The recommended dosage of lamivudine oral solution in HIV-1-infected pediatric patients aged 3 months and older is 4 mg per kg taken orally twice daily (up to a maximum of 300 mg daily), administered in combination with other antiretroviral agents.
Lamivudine scored tablet is the preferred formulation for HIV-l-infected pediatric patients who weigh at least 14 kg and for whom a solid dosage form is appropriate. Before prescribing lamivudine scored tablets, pediatric patients should be assessed for the ability to swallow tablets. For patients unable to safely and reliably swallow lamivudine tablets, the oral solution formulation should be prescribed
[see Warnings and Precautions (5.6)].The recommended oral dosage of lamivudine tablets for HIV-1-infected pediatric patients is presented in Table 1.
Table 1. Dosing Recommendations for Lamivudine Scored (150-mg) Tablets in Pediatric Patients
| Weight (kg)
| Twice-Daily Dosing Regimen Using Scored 150-mg Tablet
|
||
| AM Dose
| PM Dose
| Total Daily Dose
|
|
| 14 to <20
| ½ tablet (75 mg)
| ½ tablet (75 mg)
| 150 mg
|
| ≥20 to <25
| ½ tablet (75 mg)
| 1 tablet (150 mg)
| 225 mg
|
| ≥25
| 1 tablet (150 mg)
| 1 tablet (150 mg)
| 300 mg
|
Additional pediatric use information for patients aged 3 months and above is approved for ViiV Healthcare Company's EPIVIR
® (lamivudine) tablets and oral solution. However, due to ViiV Healthcare Company's marketing exclusivity rights, this drug product is not labeled with that pediatric information.
2.3 Patients With Renal Impairment
Dosing of lamivudine is adjusted in accordance with renal function. Dosage adjustments are listed in Table 2
[see
Clinical Pharmacology (12.3)].
Table 2. Adjustment of Dosage of Lamivudine in Adults and Adolescents (Greater than or Equal to 25 kg) in Accordance With Creatinine Clearance
| Creatinine Clearance (mL/min)
| Recommended Dosage of Lamivudine
|
| ≥50
| 150 mg twice daily or 300 mg once daily
|
| 30-49
| 150 mg once daily
|
| 15-29
| 150 mg first dose, then 100 mg once daily
|
| 5-14
| 150 mg first dose, then 50 mg once daily
|
| <5
| 50 mg first dose, then 25 mg once daily
|
No additional dosing of lamivudine is required after routine (4-hour) hemodialysis or peritoneal dialysis.
Although there are insufficient data to recommend a specific dose adjustment of lamivudine in pediatric patients with renal impairment, a reduction in the dose and/or an increase in the dosing interval should be considered.
3 DOSAGE FORMS & STRENGTHS
Lamivudine Scored Tablets
150 mg, are white capsule shaped, biconvex, scored film coated tablets debossed with 'J' on one side and '16'on the other side, 1 and 6 seperated by a score line.
Lamivudine Tablets
300 mg, are white capsule shaped, biconvex, film coated tablets debossed with '17' on one side and 'J' on the other side.
4 CONTRAINDICATIONS
Lamivudine tablets are contraindicated in patients with a previous hypersensitivity reaction to lamivudine.
5 WARNINGS AND PRECAUTIONS
5.1 Lactic Acidosis and Severe Hepatomegaly with Steatosis
Lactic acidosis and severe hepatomegaly with steatosis, including fatal cases, have been reported with the use of nucleoside analogues alone or in combination, including lamivudine and other antiretrovirals. A majority of these cases have been in women. Obesity and prolonged nucleoside exposure may be risk factors. Particular caution should be exercised when administering lamivudine to any patient with known risk factors for liver disease; however, cases also have been reported in patients with no known risk factors. Treatment with lamivudine should be suspended in any patient who develops clinical or laboratory findings suggestive of lactic acidosis or pronounced hepatotoxicity (which may include hepatomegaly and steatosis even in the absence of marked transaminase elevations).
5.2 Patients with Hepatitis B Virus Co-infection
Clinical and laboratory evidence of exacerbations of hepatitis have occurred after discontinuation of lamivudine.These exacerbations have been detected primarily by serum ALT elevations in addition to re-emergence of HBV DNA. Although most events appear to have been self-limited, fatalities have been reported in some cases. Similar events have been reported from postmarketing experience after changes from lamivudine-containing HIV-1 treatment regimens to non-lamivudine-containing regimens in patients infected with both HIV-1 and HBV. The causal relationship to discontinuation of lamivudine treatment is unknown. Patients should be closely monitored with both clinical and laboratory follow-up for at least several months after stopping treatment.
Lamivudine tablets contain a higher dose of the same active ingredient (lamivudine) than EPIVIR- HBV tablets. EPIVIR-HBV was developed for patients with chronic hepatitis B. The formulation and dosage of lamivudine in EPIVIR-HBV are not appropriate for patients co-infected with HIV-1 and HBV. Safety and efficacy of lamivudine have not been established for treatment of chronic hepatitis B in patients co-infected with HIV-1 and HBV. If treatment with EPIVIR-HBV is prescribed for chronic hepatitis B for a patient with unrecognized or untreated HIV-1 infection, rapid emergence of HIV-1 resistance is likely to result because of the subtherapeutic dose and the inappropriateness of monotherapy HIV-1 treatment. If a decision is made to administer lamivudine to patients co-infected with HIV-1 and HBV, lamivudine tablets, lamivudine oral solution, or another product containing the higher dose of lamivudine should be used as part of an appropriate combination regimen.
of lamivudine have not been established for treatment of chronic hepatitis B in subjects dually infected with HIV-1 and HBV (see full prescribing information for
of hepatitis B virus variants associated with resistance to lamivudine has also been reported in HIV-1-infected patients who have received lamivudine-
regimens in the presence of concurrent infection with hepatitis B virus.
Posttreatment Exacerbations of Hepatitis
Clinical and laboratory evidence of exacerbations of hepatitis have occurred after discontinuation of lamivudine.These exacerbations have been detected primarily by serum ALT elevations in addition to re-emergence of HBV DNA. Although most events appear to have been self-limited, fatalities have been reported in some cases. Similar events have been reported from postmarketing experience after changes from lamivudine-containing HIV-1 treatment regimens to non-lamivudine-containing regimens in patients infected with both HIV-1 and HBV. The causal relationship to discontinuation of lamivudine treatment is unknown. Patients should be closely monitored with both clinical and laboratory follow-up for at least several months after stopping treatment.
Important Differences among Lamivudine-Containing Products
Lamivudine tablets contain a higher dose of the same active ingredient (lamivudine) than EPIVIR- HBV tablets. EPIVIR-HBV was developed for patients with chronic hepatitis B. The formulation and dosage of lamivudine in EPIVIR-HBV are not appropriate for patients co-infected with HIV-1 and HBV. Safety and efficacy of lamivudine have not been established for treatment of chronic hepatitis B in patients co-infected with HIV-1 and HBV. If treatment with EPIVIR-HBV is prescribed for chronic hepatitis B for a patient with unrecognized or untreated HIV-1 infection, rapid emergence of HIV-1 resistance is likely to result because of the subtherapeutic dose and the inappropriateness of monotherapy HIV-1 treatment. If a decision is made to administer lamivudine to patients co-infected with HIV-1 and HBV, lamivudine tablets, lamivudine oral solution, or another product containing the higher dose of lamivudine should be used as part of an appropriate combination regimen.
Emergence of Lamivudine-Resistant HBV
Safety and efficacy of lamivudine have not been established for treatment of chronic hepatitis B in subjects dually infected with HIV-1 and HBV (see full prescribing information for
EPIVIR-HBV). Emergence of hepatitis B virus variants associated with resistance to lamivudine has also been reported in HIV-1-infected patients who have received lamivudine-
containing antiretroviral regimens in the presence of concurrent infection with hepatitis B virus.
5.3 Use with Interferon- and Ribavirin-Based Regimens
In vitro studies have shown ribavirin can reduce the phosphorylation of pyrimidine nucleoside analogues such as lamivudine. Although no evidence of a pharmacokinetic or pharmacodynamic interaction (e.g., loss of HIV-l/HCV virologic suppression) was seen when ribavirin was coadministered with lamivudine in HIV-l/HCV co-infected patients [see Clinical Pharmacology (12.3)],hepatic decompensation (some fatal) has occurred in HIV-l/HCV co-infected patients receiving combination antiretroviral therapy for HIV-1 and interferon alfa with or without ribavirin. Patients receiving interferon alfa with or without ribavirin and lamivudine should be closely monitored for treatment-associated toxicities, especially hepatic decompensation. Discontinuation of lamivudine should be considered as medically appropriate. Dose reduction or discontinuation of interferon alfa, ribavirin, or both should also be considered if worsening clinical toxicities are observed, including hepatic decompensation (e.g., Child-Pugh greater than 6). See the full prescribing information for interferon and ribavirin.
5.4 Pancreatitis
In pediatric patients with a history of prior antiretroviral nucleoside exposure, a history of pancreatitis, or other significant risk factors for the development of pancreatitis, lamivudine should be used with caution. Treatment with lamivudine should be stopped immediately if clinical signs, symptoms, or laboratory abnormalities suggestive of pancreatitis occur [see Adverse Reactions (6.1)] .
5.5 Immune Reconstitution Syndrome
Immune reconstitution syndrome has been reported in patients treated with combination antiretrovira1 therapy, including lamivudine. During the initial phase of combination antiretroviral treatment, patients whose immune system responds may develop an inflammatory respond to indolent or residual opportunistic infections (such as
Mycobacterium avium infection, cytomegalovirus,
Pneumocystis jirovecii pneumonia [PCP], or tuberculosis), which may necessitate further evaluation and treatment.
Autoimmune disorders (such as Graves’ disease, polymyositis, and Guillain-Barré syndrome) have also been reported to occur in the setting of immune reconstitution, however, the time to onset is more variable, and can occur many months after initiation of treatment.
5.6 Lower Virologic Suppression Rates and Increased Risk of Viral Resistance with Oral Solution
who received lamivudine oral solution concomitantly with other antiretroviral oral solutions at any time in the ARROW trial had lower rates of virologic suppression, lower plasma lamivudine
, and developed viral resistance more frequently than those receiving lamivudine tablets
scored tablet is the preferred formulation for HIV-1-infected pediatric patients who weigh at least 14 kg and for whom a solid dosage form is appropriate. Consider more frequent monitoring of HIV-1
load when treating with lamivudine oral solution.
Pediatric subjects who received lamivudine oral solution concomitantly with other antiretroviral oral solutions at any time in the ARROW trial had lower rates of virologic suppression, lower plasma lamivudine
exposure, and developed viral resistance more frequently than those receiving lamivudine tablets
[see Clinical Pharmacology (
12.3),Microbiology
(12.4),Clinical Studies (
14.2)].
Lamivudine scored tablet is the preferred formulation for HIV-1-infected pediatric patients who weigh at least 14 kg and for whom a solid dosage form is appropriate. Consider more frequent monitoring of HIV-1
viral load when treating with lamivudine oral solution.
5.7 Fat Redistribution
Redistribution/accumulation of body fat including central obesity, dorsocervical fat enlargement (buffalo hump), peripheral wasting, facial wasting, breast enlargement, and "cushingoid appearance" have been observed in patients receiving antiretroviral therapy. The mechanism and long-term consequences of these events are currently unknown. A causal relationship has not been established.
6 ADVERSE REACTIONS
The following adverse reactions are discussed in greater detail in other sections of the labeling:
Lactic acidosis and severe hepatomegaly with steatosis
[see
Boxed Warning, Warnings and Precautions (5.1)].
Exacerbations of hepatitis B
[see
Boxed Warning, Warnings and Precautions (5.2)].
Hepatic decompensation in patients co-infected with HIV-l and Hepatitis C
[see
Warnings and Precautions (5.3)].
Pancreatitis
[see Warnings and Precautions (5.4) ].
Immune reconstitution syndrome
[see
Warnings and Precautions (5.5)].
Fat redistribution
[see
Warnings and Precautions (5.7)].
6.1 Clinical Trials Experience in Adult Subjects
Clinical Trials Experience in Adult Subjects
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The safety profile of lamivudine in adults is primarily based on 3,568 HIV-l-infected subjects in 7 clinical trials.
The most common adverse reactions are headache, nausea, malaise, fatigue, nasal signs and symptoms, diarrhea and cough.
Selected clinical adverse reactions of in greater than or equal to 5% of subjects during therapy with lamivudine 150 mg twice daily plus RETROVIR ® 200 mg 3 times daily for up to 24 weeks are listed in Table 3.
Table 3. Selected Clinical Adverse Reactions (Greater than or Equal to 5% Frequency) in Four Controlled Clinical Trials (NUCA3001, NUCA3002, NUCB3001, NUCB3002)
| Adverse Reaction |
Lamivudine 150 mg Twice Daily plus Zidovudine (n = 251) |
Zidovudine a (n = 230) |
| Body as a Whole | ||
| Headache | 35% | 27% |
| Malaise & fatigue | 27% | 23% |
| Fever or chills | 10% | 12% |
| Digestive | ||
| Nausea | 33% | 29% |
| Diarrhea | 18% | 22% |
| Nausea & vomiting | 13% | 12% |
| Anorexia and/or decreased appetite | 10% | 7% |
| Abdominal pain | 9% | 11% |
| Abdominal cramps | 6% | 3% |
| Dyspepsia | 5% | 5% |
| Nervous System | ||
| Neuropathy | 12% | 10% |
| Insomnia & other sleep disorders | 11% | 7% |
| Dizziness | 10% | 4% |
| Depressive Disorders | 9% | 4% |
| Respiratory | ||
| Nasal signs & symptoms | 20% | 11% |
| Cough | 18% | 13% |
| Skin | ||
| Skin rashes | 9% | 6% |
| Musculoskeletal | ||
| Musculoskeletal pain | 12% | 10% |
| Myalgia | 8% | 6% |
| Arthralgia | 5% | 5% |
aEither zidovudine monotherapy or zidovudine in combination with zalcitabine.
Pancreatitis: Pancreatitis was observed in 9 out of 2,613 adult subjects (0.3%) who received lamivudine in the controlled clinical trials EPV20001, NUCA3001, NUCB3001, NUCA3002, NUCB3002, and NUCB3007
[see Warnings and Precautions (5.5) ].
Lamivudine 300 mg Once Daily
: The types and frequencies of clinical adverse reactions reported in subjects receiving lamivudine 300 mg once daily or lamivudine 150 mg twice daily (in 3-drug combination regimens in EPV20001 and EPV40001) for48 weeks were similar.
Selected laboratory abnormalities observed during therapy are summarized in Table 4.
Table 4.Frequencies of Selected Grade 3 to 4 Laboratory Abnormalities in Adults in Four 24-Week Surrogate Endpoint Trials (NUCA3001, NUCA3002, NUCB3001, NUCB3002) and a Clinical End point Trial (NUCB3007)
|
Test (Threshold Level) | 24-Week Surogate Endpoint Trials a | Clinical Endpoint Trial a | ||
| Lamivudine plus Zidovudine | Zidovudine b | Lamivudine plus Current Therapy c | Placebo plus Current Therapy c | |
| Absolute neutrophil count
(<750/mm 3) | 7.2% | 5.4% | 15% | 13% |
| Hemoglobin (<8.0 g/dL) | 2.9% | 1.8% | 2.2% | 3.4% |
| Platelets (<50,000/mm 3) | 0.4% | 1.3% | 2.8% | 3.8% |
| ALT (>5.0 x ULN) | 3.7% | 3.6% | 3.8% | 1.9% |
| AST (>5.0 x ULN) | 1.7% | 1.8% | 4.0% | 2.1% |
| Bilirubin (>2.5 x ULN) | 0.8% | 0.4% | ND | ND |
| Amylase (>2.0 x ULN) | 4.2% | 1.5% | 2.2% | 1.1% |
a The median duration on study was 12 months.
b Either zidovudine monotherapy or zidovudine in combination with zalcitabine.
c Current therapy was either zidovudine, zidovudine plus didonasine, or zidovudine plus zalcitabine
ULN = Upper limit of normal
ND = Not done.
The frequencies of selected laboratory abnormalities reported in subjects receiving lamivudine 300 mg once daily or lamivudine 150 mg twice daily (in 3-drug combination regimens in EPV20001 and EPV40001) were similar.
The frequencies of selected laboratory abnormalities reported in subjects receiving lamivudine 300 mg once daily or lamivudine 150 mg twice daily (in 3-drug combination regimens in EPV20001 and EPV40001) were similar.
Clinical Trials Experience in Pediatric Subjects
Selected clinical adverse reactions and physical findings with a greater than or equal to5% frequency during therapy with lamivudine 4 mg per kg twice daily plus zidovudine 160 mg per m 2 3 times daily in therapy-naive (less than or equal to 56 days of antiretroviral therapy) pediatric subjects are listed in Table 5.
Table 5. Selected Clinical Adverse Reactions and Physical Findings (Greater than or Equal to 5% frequency) in Pediatric Subjects in Trial ACTG300
| Adverse Reaction
| La m ivudine plus
Zidovudine (n = 236) | Didanosine
(n = 235) |
| Body as a Whole
|
|
|
| Fever
| 25%
| 32%
|
| Digestive
|
|
|
| Hepatomegaly
| 11%
| 11%
|
| Nausea & vo miting
| 8%
| 7%
|
| Diarrhea
| 8%
| 6%
|
| Sto matitis
| 6%
| 12%
|
| Splenomegaly
| 5%
| 8%
|
| Respiratory
|
|
|
| Cough
| 15%
| 18%
|
| Abno r mal breath so unds/wheezi ng
| 7%
| 9%
|
| Ear, Nose, and Throat
|
|
|
| Signs or sy mpto ms of ear s
a
| 7%
| 6%
|
| Nasal discharge or congestion
| 8%
| 11%
|
| Other
|
|
|
| Skin rashes
| 12%
| 14%
|
| Ly mphadenopathy
| 9%
| 11%
|
a Includes pain, discharge, erythema, or swelling of an ear.
Pancreatitis
Pancreatitis, which has been fatal in some cases, has been observed in antiretroviral nucleoside-experienced pediatric subjects receiving lamivudine alone or in combination with other antiretroviral agents. In an open-label dose-escalation trial (NUCA2002), 14 subjects (14%) developed pancreatitis while receiving monotherapy with lamivudine. Three of these subjects died of complications of pancreatitis. In a second open-label trial (NUCA2005), 12 subjects (18%) developed pancreatitis. In Trial ACTG300, pancreatitis was not observed in 236 subjects randomized to lamivudine plus zidovudine. Pancreatitis was observed in 1 subject in this trial who received open-label lamivudine in combination with zidovudine and ritonavir following discontinuation of didanosine monotherapy
[see
Warnings and Precautions (5.4)].
Paresthesias and Peripheral Neuropathies
Paresthesias and peripheral neuropathies were reported in 15 subjects (15%) in Trial NUCA2002, 6 subjects (9%) in Trial NUCA2005, and 2 subjects (less than 1%) in Trial ACTG300.
Selected laboratory abnormalities experienced by therapy-naive (less than or equal to 56 days of antiretroviral therapy) pediatric subjects are listed in Table 6.
Table 6. Frequencies of Selected Grade 3 to 4 Laboratory Abnormalities in Pediatric Subjects in Trial ACTG300
|
Test (Threshold Level) |
La m ivudine plus Zidovudine |
Didanosine |
| Absolute
neutrophilcount (<400/mm
3) Hemoglobin (<7 g/dL)
Platelets(<50,000/mm 3) ALT (>10 x ULN) AST (>10 x ULN) Lipase (>2.5 x ULN) Total Amylase (>2.5 x ULN) | 8%
4% 1% 1% 2% 3% 3% | 3%
2% 3% 3% 4% 3% 3% |
ULN = Upper limit of normal.
Additional pediatric use information for patients aged 3 months and above is approved for ViiV Healthcare Company's EPIVIR ® (lamivudine) tablets and oral solution. However, due to ViiV Healthcare Company's marketing exclusivity rights, this drug product is not labeled with that pediatric information.
Neonates
Limited short-term safety information is available from 2 small, uncontrolled trials in South Africa in neonates receiving lamivudine with or without zidovudine for the first week of life following maternal treatment starting at Week 38 or 36 of gestation [see Clinical Pharmacology (12.3)].Selected adverse reactions reported in these neonates included increased liver function tests, anemia, diarrhea, electrolyte disturbances, hypoglycemia, jaundice and hepatomegaly, rash, respiratory infections, and sepsis; 3 neonates died (1 from gastroenteritis with acidosis and convulsions, 1 from traumatic injury, and 1 from unknown causes). Two other nonfatal gastroenteritis or diarrhea cases were reported, including 1 with convulsions; 1 infant had transient renal insufficiency associated with dehydration. The absence of control groups limits assessments of causality, but it should be assumed that perinatally exposed infants may be at risk for adverse reactions comparable to those reported in pediatric and adult HIV-1-infected patients treated with lamivudine-containing combination regimens. Long-term effects of in utero and infant lamivudine exposure are not known.
6.2 Postmarketing Experience
The following adverse reactions have been identified during post-approval use of lamivudine. Because these reactions are reported voluntarily from a population of unknown size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure. These reactions have been chosen for inclusion due to a combination of their seriousness, frequency of reporting, or potential causal connection to lamivudine.
Body as a Whole
Redistribution/accumulation of body fat
[see Warnings and Precautions (5.7)].
Endocrine and Metabolic
Hyperglycemia.
General
Weakness
Hemic and Lymphatic
Anemia (including pure red cell aplasia and severe anemias progressing on therapy).
Hepatic and Pancreatic
Lactic acidosis and hepatic steatosis, posttreatment exacerbation of hepatitis B
[see Boxed Warning, Warnings and Precautions (5.1,5.2)].
Hypersensitivity
Anaphylaxis, urticaria.
Musculoskeletal
Muscle weakness, CPK elevation, rhabdomyolysis.
Skin
Alopecia, pruritus.
7 DRUG INTERACTIONS
Lamivudine is predominantly eliminated in the urine by active organic cationic secretion. The possibility of interactions with other drugs administered concurrently should be considered, particularly when their main route of elimination is active renal secretion via the organic cationic transport system (e.g., trimethoprim). [see Clinical Pharmacology ( 12.3)]. No data are available regarding interactions with other drugs that have renal clearance mechanisms similar to that of lamivudine.
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Teratogenic Effects
Pregnancy Exposure Registry
There is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to lamivudine during pregnancy. Physicians are encouraged to register patients by calling the Antiretroviral Pregnancy Registry at 1-800-258-4263.
Risk Summary
Available data from the Antiretroviral Pregnancy Registry show no difference in the risk of overall major birth defects for lamivudine compared with the background rate for major birth defects of 2.7% in the US reference population of the Metropolitan Atlanta Congenital Defects program (MACDP). Lamivudine produced embryonic toxicity in rabbits at a dose that produced similar human exposures as the recommended clinical dose. The relevance of animal findings to human pregnancy registry data is not known.
Data
Human Data: Based on prospective reports from the Antiretroviral Pregnancy Registry of over 11,000 exposures to lamivudine during pregnancy resulting in live births (including over 4,300 exposed in first trimester), there was no difference between lamivudine and overall birth defects compared with the background birth defect rate of 2.7% in the US reference population of MACDP. The prevalence of defects in the first trimester was 3.1% (95% CI: 2.6% to 3.7%).
Lamivudine pharmacokinetics were studied in pregnant women during 2 clinical trials conducted in south Africa. The trials assessed pharmacokinetics in 16 women at 36 weeks gestation using 150 mg lamivudine twice daily with zidovudine, 10 women at 38 weeks gestation using 150 mg lamivudine twice daily with zidovudine, and 10 women at 38 weeks gestation using lamivudine 300 mg twice daily without other antiretrovirals. These trials were not designed or powered to provide efficacy information. Lamivudine pharmacokinetics in pregnant women were similar to those seen in non-pregnant adults and in postpartum women. Lamivudine concentrations were generally similar in maternal, neonatal, and umbilical cord serum samples. In a subset of subjects, amniotic fluid specimens were collected following natural rupture of membranes and confirmed that lamivudine crosses the placenta in humans. Amniotic fluid concentrations of lamivudine were typically 2 times greater than maternal serum levels and ranged from 1.2 to 2.5 mcg per ml (150 mg twice daily) and 2.1 to 5.2 mcg per ml (300 mg twice daily).
Animal data: Studies in pregnant rats showed that lamivudine is transferred to the fetus through the placenta. Reproduction studies with orally administrated lamivudine have been performed in rats and rabbits at doses producing plasma levels up to approximately 35 times that for the recommended adult HIV dose. No evidence of teratogenicity due to lamivudine was observed. Evidence of embryo-lethality was seen in the rabbit at exposure levels similar to those observed in humans but there was no indication of this effect in the rat at exposure levels up to 35 times those in humans.
8.2 Lactation
Risk Summary
The Centers for Disease control and Prevention recommended that HIV-1-infected mothers in the United States not breastfeed their infants to avoid risking postnatal transmission of HIV-1 infection. Because of the potential for HIV-1 transmission mothers should be instructed not to breastfeed.
8.4 Pediatric Use
The safety and effectiveness of lamivudine in combination with other antiretroviral agents have been established in pediatric patients aged 3 months and older. Lamivudine scored tablet is the preferred formulation for HIV-1-infected pediatric patients who weigh at least 14 kg and for whom a solid dosage form is appropriate because pediatric subjects who received lamivudine oral solution had lower rates of virologic suppression, lower plasma lamivudine exposure, and developed viral resistance more frequently than those receiving lamivudine tablets in the ARROW trial [see Dosage and Administration (2.2), Warnings and Precautions (5.6),Adverse Reactions (6.1),Clinical Pharmacology (12.3),Clinical Studies (14.2)].
8.5 Geriatric Use
Clinical trials of lamivudine did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. In general, caution should be exercised in the administration of lamivudine tablets in elderly patients reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy [see Dosage and Administration (2.3), Clinical Pharmacology (12.3)] .
8.6 Patients With Impaired Renal Function
Reduction of the dosage of lamivudine is recommended for patients with impaired renal function [see Dosage and Administration (2.3), Clinical Pharmacology (12.3)]
10 OVERDOSAGE
There is no known specific treatment for overdose with lamivudine. If overdose occurs, the patient should be monitored and standard supportive treatment applied as required. Because a negligible amount of lamivudine was removed via (4-hour) hemodialysis, continuous ambulatory peritoneal dialysis, and automated peritoneal dialysis, it is not known if continuous hemodialysis would provide clinical benefit in a lamivudine overdose event.
11 DESCRIPTION
Lamivudine USP (also known as 3TC), a synthetic nucleoside analogue with activity against HIV-1 and HBV. The chemical name of lamivudine USP is 2(1H) - Pyrimidinone, 4-amino-1- [2- (hydroxymethyl)-1,3-oxathio-lan-5-yl], (2R-cis)-. It has a molecular formula of C 8H 11N 3O 3S and a molecular weight of 229.26. It has the following structural formula:
Lamivudine USP is a white to an off white solid and soluble in water.
Lamivudine tablets are for oral administration. Each film-coated tablet contains 150 mg or 300 mg of lamivudine USP and the following inactive ingredients: crospovidone, isomalt, isopropyl alcohol, magnesium stearate and methylene chloride. The tablets are coated with opadry white containing hypromellose, polyethylene glycol, polysorbate 80 and titanium dioxide.
12 CLINICAL PHARMACOLOGY
12.3 Pharmacokinetics
Pharmacokinetics in Adults
The pharmacokinetic properties of lamivudine have been studied in asymptomatic, HIV-l-infected adult subjects after administration of single intravenous (IV) doses ranging from 0.25 to 8 mg per kg, as well as single and multiple (twice-daily regimen) oral doses ranging from 0.25 to 10 mg per kg.
The pharmacokinetic properties of lamivudine have also been studied as single and multiple oral doses ranging from 5 mg to 600 mg per day administered to HBV-infected subjects.
The steady-state pharmacokinetic properties of the lamivudine 300-mg tablet once daily for 7 days compared with the lamivudine 150-mg tablet twice daily for 7 days were assessed in a crossover trial in 60 healthy subjects. Lamivudine 300 mg once daily resulted in lamivudine exposures that were similar to lamivudine 150 mg twice daily with respect to plasma AUC 24,ss; however, C max,ss was 66% higher and the trough value was 53% lower compared with the 150-mg twice-daily regimen. Intracellular lamivudine triphosphate exposures in peripheral blood mononuclear cells were also similar with respect to AUC 24,ss and C max24,ss; however, trough values were lower compared with the 150-mg twice-daily regimen. Inter-subject variability was greater for intracellular lamivudine triphosphate concentrations versus lamivudine plasma trough concentrations.
The pharmacokinetics of lamivudine was evaluated in 12 adult HIV-1-infected subjects dosed with lamivudine 150 mg twice daily in combination with other antiretroviral agents. The geometric mean (95% CI) for AUC (0 to 12) was 5.53 (4.58, 6.67) mcg.h per mL and for Cmax was 1.40 (1.17, 1.69) mcg per mL.
Absorption and Bioavailability: Following oral administration, lamivudine is rapidly absorbed and extensively distributed. Absolute bioavailability in 12 adult subjects was 86%± 16% (mean±SD) for the 150-mg tablet and 87% ±13% for the oral solution. After oral administration of 2 mg per kg twice a day to 9 adults with HIV-1, the peak serum lamivudine concentration (C max) was 1.5 0.5 mcg per mL (mean ±SD). The area under the plasma concentration versus time curve (AUC) and Cmax increased in proportion to oral dose over the range from 0.25 to 10 mg per kg.
The accumulation ratio of lamivudine in HIV-1-positive asymptomatic adults with normal renal function was 1.50 following 15 days of oral administration of 2 mg per kg twice daily.
Effects of Food on Oral Absorption: Lamivudine tablets and oral solution may be administered with or without food. An investigational 25-mg dosage form of lamivudine was administered orally to 12 asymptomatic, HIV-1-infected subjects on 2 occasions, once in the fasted state and once with food (1,099 kcal; 75 grams fat, 34 grams protein, 72 grams carbohydrate). Absorption of lamivudine was slower in the fed state (T max: 3.2 ± 1.3 hours) compared with the fasted state (T max: 0.9 ± 0.3 hours); C max in the fed state was 40% ± 23% (mean ± SD) lower than in the fasted state. There was no significant difference in systemic exposure (AUC∞) in the fed and fasted states.
Distribution: The apparent volume of distribution after IV administration of lamivudine to 20 subjects was 1.3 ± 0.4 L per kg, suggesting that lamivudine distributes into extravascular spaces. Volume of distribution was independent of dose and did not correlate with body weight.
Binding of lamivudine to human plasma proteins is low (less than 36%). In vitro studies showed that over the concentration range of 0.1 to 100 mcg per mL, the amount of lamivudine associated with erythrocytes ranged from 53% to 57% and was independent of concentration.
Metabolism: Metabolism of lamivudine is a minor route of elimination. In humans, the only known metabolite of lamivudine is the trans-sulfoxide metabolite (approximately 5% of an oral dose after 12 hours). Serum concentrations of this metabolite have not been determined. Lamivudine is not significantly metabolized by cytochrome P450 enzymes.
Elimination: The majority of lamivudine is eliminated unchanged in urine by active organic cationic secretion. In 9 healthy subjects given a single 300-mg oral dose of lamivudine, renal clearance was 199.7± 56.9 mL per min (mean±SD). In 20 HIV-l-infected subjects given a single IV dose, renal clearance was 280.4 ± 75.2 mL per min (mean ±SD), representing 71% ± 16% (mean ±SD) of total clearance of lamivudine.
In most single-dose trials in HIV-1-infected subjects, HBV-infected subjects, or healthy subjects with serum sampling for 24 hours after dosing, the observed mean elimination half-life (t1/2) ranged from 5 to 7 hours. In HIV-1-infected subjects, total clearance was 398.5 ±69.1 mL per min (mean ± SD). Oral clearance and elimination half- life were independent of dose and body weight over an oral dosing range of 0.25 to 10 mg per kg.
Special Populations
Renal Impairment: The pharmacokinetic properties of lamivudine have been determined in a small group of HIV-1-infected adults with impaired renal function (Table 7).
Table 7. Pharmacokinetic Parameters (Mean ± SD) after a Single 300-mg Oral Dose of Lamivudine in 3 Groups of Adults with Varying Degrees of Renal Function
|
Parameter |
Creatinine Clearance Criterion (Number of Subjects) |
||
|
>60 mL/min (n = 6) |
10-30 mL/min (n = 4) |
<10 mL/min (n = 6) |
|
|
Creatinine clearance (mL/min) |
111 ± 14 |
28 ± 8 |
6 ± 2 |
|
C max (mcg/mL) |
2.6 ± 0.5 |
3.6 ± 0.8 |
5.8 ± 1.2 |
|
AUC ¥(mcg·h/mL) |
11 ± 1.7 |
48 ± 19 |
157 ± 74 |
|
Cl/F (mL/min) |
464 ± 76 |
114 ± 34 |
36 ± 11 |
T max was not significantly affected by renal function. Based on these observations, it is recommended that the dosage of lamivudine be modified in patients with renal impairment [see Dosage and Administration (2.3)].
Based on a trial in otherwise healthy subjects with impaired renal function, hemodialysis increased lamivudine clearance from a mean of 64 to 88 mL per min; however, the length of time of hemodialysis (4 hours) was insufficient to significantly alter mean lamivudine exposure after a single-dose administration. Continuous ambulatory peritoneal dialysis and automated peritoneal dialysis have negligible effects on lamivudine clearance. Therefore, it is recommended, following correction of dose for creatinine clearance, that no additional dose modification be made after routine hemodialysis or peritoneal dialysis.
The effects of renal impairment on lamivudine pharmacokinetics in pediatric patients are not known.
Hepatic Impairment: The pharmacokinetic properties of lamivudine have been determined in adults with impaired hepatic function. Pharmacokinetic parameters were not altered by diminishing hepatic function. Safety and efficacy of lamivudine have not been established in the presence of decompensated liver disease.
Pregnancy: Lamivudine pharmacokinetics were studied in 36 pregnant women during
2 clinical trials conducted in South Africa. Lamivudine pharmacokinetics in pregnant women were similar to those seen in non-pregnant adults and in postpartum women. Lamivudine concentrations were generally similar in maternal, neonatal, and umbilical cord serum samples.
Pediatric Patients: The pharmacokinetics of lamivudine have been studied after either single or repeat doses of lamivudine in 210 pediatric subjects. Pediatric subjects receiving lamivudine oral solution according to the recommended dosage regimen achieved approximately 25% lower plasma concentrations of lamivudine compared with HIV-1-infected adults. Pediatric subjects receiving lamivudine oral tablets achieved plasma concentrations comparable to or slightly higher than those observed in adults. The absolute bioavailability of both lamivudine tablets and oral solution are lower in children than adults. The relative bioavailability of lamivudine oral solution is approximately 40% lower than tablets containing lamivudine in pediatric subjects despite no difference in adults. The mechanisms for the diminished absolute bioavailability of lamivudine and relative bioavailability of lamivudine solution are unknown.
Distribution of lamivudine into cerebrospinal fluid (CSF) was assessed in 38 pediatric subjects after multiple oral dosing with lamivudine. CSF samples were collected between 2 and 4 hours postdose. At the dose of 8 mg per kg per day, CSF lamivudine concentrations in 8 subjects ranged from 5.6% to 30.9% (mean ±SD of 14.2%±7.9%) of the concentration in a simultaneous serum sample, with CSF lamivudine concentrations ranging from 0.04 to 0.3 mcg per mL.
Limited, uncontrolled pharmacokinetic and safety data are available from administration of lamivudine (and zidovudine) to 36 infants aged up to 1 week in 2 trials in South Africa. In these trials, lamivudine clearance was substantially reduced in 1-week-old neonates relative to pediatric subjects (aged over 3 months) studied previously. There is insufficient information to establish the time course of changes in clearance between the immediate neonatal period and the age-ranges over 3 months old [see Adverse Reactions (6.1)].
Additional pediatric use information for patients aged 3 months and above is approved for ViiV Healthcare Company's EPIVIR ® (lamivudine) tablets and oral solution. However, due to ViiV Healthcare Company's marketing exclusivity rights, this drug product is not labeled with that pediatric information.
Geriatric Patients: The pharmacokinetics of lamivudine after administration of lamivudine to subjects over 65 years have not been studied [see Use in Specific Populations (8.5)].
Gender: There are no significant or clinically relevant gender differences in lamivudine pharmacokinetics.
Race: There are no significant or clinically relevant racial differences in lamivudine pharmacokinetics.
Drug Interactions
Interferon Alfa: There was no significant pharmacokinetic interaction between lamivudine and interferon alfa in a trial of 19 healthy male subjects [see Warnings and Precautions (5.3)].
Ribavirin: In vitro data indicate ribavirin reduces phosphorylation of lamivudine, stavudine, and zidovudine. However, no pharmacokinetic (e.g., plasma concentrations or intracellular triphosphorylated active metabolite concentrations) or pharmacodynamic (e.g., loss of HIV-l/HCV virologic suppression) interaction was observed when ribavirin and lamivudine (n = 18), stavudine (n = 10), or zidovudine (n = 6) were coadministered as part of a multi-drug regimen to HIV-l/HCV co-infected subjects [see Warnings and Precautions (5.3)].
Trimethoprim/Sulfamethoxazole: Lamivudine and TMP/SMX were coadministered to 14 HIV-1-positive subjects in a single-center, open-label, randomized, crossover trial. Each subject received treatment with a single 300-mg dose of lamivudine and TMP 160 mg/SMX 800 mg once a day for 5 days with concomitant administration of lamivudine 300 mg with the fifth dose in a crossover design. Coadministration of TMP/SMX with lamivudine resulted in an increase of 43% ±23% (mean±SD) in lamivudine AUC, a decrease of 29%±13% in lamivudine oral clearance, and a decrease of 30%±36% in lamivudine renal clearance. The pharmacokinetic properties of TMP and SMX were not altered by coadministration with lamivudine. There is no information regarding the effect on lamivudine pharmacokinetics of higher doses of TMP/SMX such as those used in treat PCP.
Zidovudine: No clinically significant alterations in lamivudine or zidovudine pharmacokinetics were observed in 12 asymptomatic HIV-l-infected adult subjects given a single dose of zidovudine (200 mg) in combination with multiple doses of lamivudine (300 mg every 12 hours).
12.4 Microbiology
Mechanism of Action
Lamivudine is a synthetic nucleoside analogue. Intracellularly, lamivudine is phosphorylated to its active 5'-triphosphate metabolite, lamivudine triphosphate (3TC-TP). The principal mode of action of 3TC-TP is inhibition of HIV-1 reverse transcriptase (RT) via DNA chain termination after incorporation of the nucleotide analogue.
Antiviral Activity
The antiviral activity of lamivudine against HIV-1 was assessed in a number of cell lines including monocytes and fresh human peripheral blood lymphocytes (PBMCs) using standard susceptibility assays. EC
50 values were in the range of 0.003 to 15 microM (1 microM = 0.23 mcg per mL). The median EC
50 values of lamivudine were 60 nM (range: 20 to 70 nM), 35 nM (range: 30 to 40 nM), 30 nM (range: 20 to 90 nM), 20 nM (range: 3 to 40 nM), 30 nM (range: 1 to 60 nM), 30 nM (range: 20 to 70 nM), 30 nM (range: 3 to 70 nM), and 30 nM (range: 20 to 90 nM) against HIV-1 clades A-G and group O viruses (n = 3 except n = 2 for clade B) respectively. The EC
50 values against HIV-2 isolates (n = 4) ranged from 0.003 to 0.120 microM in PBMCs. Lamivudine was not antagonistic to all tested anti-HIV agents. Ribavirin (50 microM) used in the treatment of chronic HCV infection decreased the anti-HIV-1 activity of lamivudine by 3.5-fold in MT-4 cells.
Resistance
Lamivudine-resistant variants of HIV-1 have been selected in cell culture. Genotypic analysis showed that the resistance was due to a specific amino acid substitution in the HIV-1 reverse transcriptase at codon 184 changing the methionine to either valine or isoleucine (M184V/I).
HIV-1 strains resistant to both lamivudine and zidovudine have been isolated from subjects. Susceptibility of clinical isolates to lamivudine and zidovudine was monitored in controlled clinical trials. In subjects receiving lamivudine monotherapy or combination therapy with lamivudine plus zidovudine, HIV-1 isolates from most subjects became phenotypically and genotypically resistant to lamivudine within 12 weeks.
Genotypic and Phenotypic Analysis of On-Therapy HIV-1 Isolates from Subjects with Virologic Failure
Trial EPV20001: Fifty-three of 554 (10%) subjects enrolled in EPV20001 were identified as virological failures (plasma HIV-l RNA level greater than or equal to 400 copies per mL) by Week 48. Twenty-eight subjects were randomized to the lamivudine once-daily treatment group and 25 to the lamivudine twice-daily treatment group. The median baseline plasma HIV-l RNA levels of subjects in the lamivudine once-daily group and lamivudine twice-daily group were 4.9 log
10 copies per mL and 4.6 log
10 copies per mL, respectively.
Genotypic analysis of on-therapy isolates from 22 subjects identified as virologic failures in the lamivudine once-daily group showed that isolates from 8 of 22 subjects contained treatment-emergent lamivudine resistance-associated substitution (M184V or M184I), isolates from 0 of 22 subjects contained treatment-emergent amino acid substitutions associated with zidovudine resistance (M41L, D67N, K70R, L210W, T215Y/F, or K219Q/E), and isolates from 10 of 22 subjects contained treatment-emergent amino acid substitutions associated with efavirenz resistance (L100I, K101E, K103N, V108I, or Y181C).
Genotypic analysis of on-therapy isolates from subjects (n = 22) in the lamivudine twice-daily treatment group showed that isolates from 5 of 22 subjects contained treatment-emergent lamivudine resistance substitutions, isolates from 1 of 22 subjects contained treatment-emergent zidovudine resistance substitutions, and isolates from 7 of 22 subjects contained treatment-emergent efavirenz resistance substitutions.
Phenotypic analysis of baseline-matched on-therapy HIV-l isolates from subjects (n =13) receiving lamivudine once daily showed that isolates from 7 of 13 subjects showed an 85-to 299-fold decrease in susceptibility to lamivudine, isolates from 12 of 13 subjects were susceptible to zidovudine, and isolates from 8 of 13 subjects exhibited a 25-to 295-fold decrease in susceptibility to efavirenz.
Phenotypic analysis of baseline-matched on-therapy HIV-1 isolates from subjects (n=13) receiving lamivudine twice daily showed that isolates from 4 of 13 subjects exhibited a 29-to 159-fold decrease in susceptibility to lamivudine, isolates from all 13 subjects were susceptible to zidovudine, and isolates from 3 of 13 subjects exhibited a 21-to 342-fold decrease in susceptibility to efavirenz.
Trial EPV40001: Fifty subjects received lamivudine 300 mg once daily plus zidovudine 300 mg twice daily plus abacavir 300 mg twice daily and 50 subjects received lamivudine 150 mg plus zidovudine 300 mg plus abacavir 300 mg all twice-daily. The median baseline plasma HIV-1 RNA levels for subjects in the 2 groups were 4.79 log
10 copies per mL and 4.83 log
10 copies per mL, respectively. Fourteen of 50 subjects in the lamivudine once-daily treatment group and 9 of 50 subjects in the lamivudine twice-daily group were identified as virologic failures.
Genotypic analysis of on-therapy HIV-1 isolates from subjects (n = 9) in the lamivudine once-daily treatment group showed that isolates from 6 subjects had an abacavir and/or lamivudine resistance-associated substitution M184V alone. On-therapy isolates from subjects (n = 6) receiving lamivudine twice daily showed that isolates from 2 subjects had M184V alone and isolates from 2 subjects harbored the M184V substitution in combination with zidovudine resistance-associated amino acid substitutions.
Phenotypic analysis of on-therapy isolates from subjects (n = 6) receiving lamivudine once daily showed that HIV-l isolates from 4 subjects exhibited a 32- to 53-fold decrease in susceptibility to lamivudine. HIV-1 isolates from these 6 subjects were susceptible to zidovudine.
Phenotypic analysis of on-therapy isolates from subjects (n = 4) receiving lamivudine twice daily showed that HIV-l isolates from 1 subject exhibited a 45-fold decrease in susceptibility to lamivudine and a 4.5-fold decrease in susceptibility to zidovudine.
Pediatrics: Pediatric subjects receiving lamivudine oral solution concomitantly with other antiretroviral oral solutions (abacavir, nevirapine/efavirenz, or zidovudine) in ARROW developed viral resistance more frequently than those receiving tablets. At randomization to once-daily or twice-daily dosing of lamivudine plus abacavir, 13% of subjects who started on tablets and 32% of subjects who started on solution had resistance substitutions. The resistance profile observed in pediatrics is similar to that observed in adults in terms of the genotypic substitutions detected and relative frequency, with the most commonly detected substitutions at M184 (V or I)
[see Clinical
Studies (14.2)].
Cross-Resistance
Cross-resistance has been observed among nucleoside reverse transcriptase inhibitors (NRTIs). Lamivudine-resistant HIV-1 mutants were cross-resistant in cell culture to didanosine (ddI). Cross-resistance is also expected with abacavir and emtricitabine as these select M184V substitutions.
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis & Mutagenesis & Impairment Of Fertility
Carcinogenesis
Long-term carcinogenicity studies with lamivudine in mice and rats showed no evidence of carcinogenic potential at exposures up to 10 times (mice) and 58 times (rats) the human exposures at the recommended dose of 300 mg.
Mutagenesis
Lamivudine was mutagenic in an L5178Y mouse lymphoma assay and clastogenic in a cytogenetic assay using cultured human lymphocytes. Lamivudine was not mutagenic in a microbial mutagenicity assay, in an
in vitro cell transformation assay, in a rat micronucleus test, in a rat bone marrow cytogenetic assay, and in an assay for unscheduled DNA synthesis in rat liver. Lamivudine showed no evidence of
in vivo genotoxic activity in the rat at oral doses of up to 2,000 mg per kg, producing plasma levels of 35 to 45 times those in humans at the recommended dose for HIV-1 infection.
Impairment of Fertility
In a study of reproductive performance, lamivudine administered to rats at doses up to 4,000 mg per kg per day, producing plasma levels 47 to 70 times those in humans, revealed no evidence of impaired fertility and no effect on the survival, growth, and development to weaning of the offspring.
14 CLINICAL STUDIES
The use of lamivudine is based on the results of clinical studies in HIV-1-infected subjects in combination regimens with other antiretroviral agents. Information from trials with clinical endpoints or a combination of CD4+ cell counts and HIV-l RNA measurements is included below as documentation of the contribution of lamivudine to a combination regimen in controlled trials.
14.1 Adult Subjects
Clinical Endpoint Trial
NUCB3007 (CAESAR) was a multicenter, double-blind, placebo-controlled trial comparing continued current therapy (zidovudine alone [62% of subjects] or zidovudine with didanosine or zalcitabine [38% of subjects]) to the addition of lamivudine or lamivudine plus an investigational non-nucleoside reverse transcriptase inhibitor (NNRTI), randomized 1:2:1. A total of 1,816 HIV-l-infected adults with 25 to 250 CD4+ cells/mm
3 (median = 122 cells/mm
3) at baseline were enrolled: median age was 36 years, 87% were male, 84% were nucleoside-experienced, and 16% were therapy-naive. The median duration on study was 12 months. Results are summarized in Table 8.
Table 8. Number of Subjects (%) With at Least One HIV-1 Disease Progression Event or Death
|
Endpoint | Current Therapy
(n= 460) | Lamivudine plus Current Therapy
(n=896) | Lamivudine plus an NNRTI
a plus Current Therapy (n=460)
|
| HIV-1 progression or death
| 90 (19.6%)
| 86 (9.6%)
| 41 (8.9%)
|
| Death
| 27 (5.9%)
| 23 (2.6%)
|
14 (3%) |
a An investigational non-nucleoside reverse transcriptase inhibitor not approved in the United States
Surrogate Endpoint Trials
Dual Nucleoside Analogue Trials: Principal clinical trials in the initial development of lamivudine compared lamivudine/zidovudine combinations with zidovudine monotherapy or with zidovudine plus zalcitabine. These trials demonstrated the antiviral effect of lamivudine in a 2-drug combination. More recent uses of lamivudine in treatment of HIV-1 infection incorporate it into multiple- drug regimens containing at least 3 antiretroviral drugs for enhanced viral suppression.
Dose Regimen Comparison Surrogate Endpoint Trials in Therapy-Naive Adults:
EPV20001 was a multicenter, double-blind, controlled trial in which subjects were randomized 1:1 to receive lamivudine 300 mg once daily or lamivudine 150 mg twice daily, in combination with zidovudine 300 mg twice daily and efavirenz 600 mg once daily. A total of 554 antiretroviral treatment-naive HIV-1-infected adults enrolled: male (79%), Caucasian (50%), median age of 35 years, baseline CD4+ cell counts of 69 to 1,089 cells/mm
3 (median = 362 cells/mm
3), and median baseline plasma HIV-1 RNA of 4.66 log
10 copies/mL. Outcomes of treatment through 48 weeks are summarized in Figure 1 and Table 9.
Figure 1. Virologic Response through Week 48, EPV20001
ab (Intent-to-Treat)
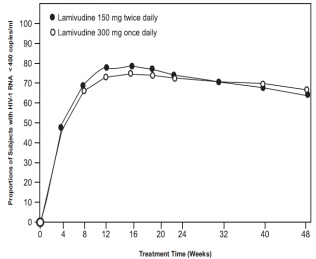
a Roche AMPLICOR HIV-1 MONITOR.
b Responders at each visit are subjects who had achieved and maintained
HIV-1 RNA less than 400 copies per mL without discontinuation by that visit.
Table 9. Outcomes of Randomized Treatment through 48 Weeks (Intent-to- Treat)
| Outcome
| Lamivudine300mg
Once Daily plus Zidovudine plus Efavirenz (n = 278) | Lamivudine150mg
Twice Daily plus Zidovudine plus Efavirenz (n = 276) |
| Responder
a
| 67%
| 65%
|
| Virologic failure
b
| 8%
| 8%
|
| Discontinued due to clinical progression
| <1%
| 0%
|
| Discontinued due to adverse events
| 6%
| 12%
|
| Discontinued due to other reasons
c
| 18%
| 14%
|
a Achieved confirmed plasma HIV-1 RNA <400 copies/mL and maintained through 48 weeks.
b Achieved suppression but rebounded by Week 48, discontinued due to virologic failure, insufficient viral response according to the investigator, or never suppressed through
Week 48.
c Includes consent withdrawn, lost to followup, protocol violation, data outside the study-defined schedule, and randomized but never initiated treatment.
The proportions of subjects with HIV-l RNA less than 50 copies per mL (via Roche Ultrasensitive assay) through Week 48 were 61% for subjects receiving lamivudine 300 mg once daily and 63% for subjects receiving lamivudine 150 mg twice daily. Median increases in CD4+ cell counts were 144 cells per mm
3 at Week 48 in subjects receiving lamivudine 300 mg once daily and 146 cells per mm
3 for subjects receiving lamivudine 150 mg twice daily.
A small, randomized, open-label pilot trial, EPV40001, was conducted in Thailand. A total of 159 treatment-naive adult subjects (male 32%, Asian 100%, median age 30 years, baseline median CD4+ cell count 380 cells per mm
3, median plasma HIV-1 RNA 4.8 log
10 copies per mL) were enrolled. Two of the treatment arms in this trial provided a comparison between lamivudine 300 mg once daily (n=54) and lamivudine 150 mg twice daily (n=52), each in combination with zidovudine 300 mg twice daily and abacavir 300 mg twice daily. In intent-to-treat analyses of 48-week data, the proportions of subjects with HIV-1 RNA below 400 copies per mL were 61% (33 of 54) in the group randomized to once-daily lamivudine and 75% (39 of 52) in the group randomized to receive all 3 drugs twice daily; the proportions with HIV-l RNA below 50 copies per mL were 54% (29 of 54) in the once-daily lamivudine group and 67% (35 of 52) in the all-twice-daily group; and the median increases in CD4+ cell counts were 166 cells per mm
3 in the once-daily lamivudine group and 216 cells per mm
3 in the all-twice-daily group.
14.2 Pediatric Subjects
Clinical Endpoint Trial
ACTG300 was a multicenter, randomized, double-blind trial that provided for comparison of lamivudine plus RETROVIR (zidovudine) with didanosine monotherapy. A total of 471 symptomatic, HIV-1-infected therapy-naive (less than or equal to 56 days of antiretroviral therapy) pediatric subjects were enrolled in these 2 treatment arms. The median age was 2.7 years (range: 6 weeks to 14 years), 58% were female, and 86% were non-white. The mean baseline CD4+cell count was 868 cells per mm3 (mean: 1,060 cells per mm
3 and range: 0 to 4,650 cells per mm3 for subjects aged less than or equal to 5 years; mean: 419 cells per mm
3 and range: 0 to 1,555 cells per mm
3 for subjects aged over 5 years) and the mean baseline plasma HIV-1 RNA was 5 log
10 copies per mL. The median duration on trial was 10.1 months for the subjects receiving lamivudine plus zidovudine and 9.2 months for subjects receiving didanosine monotherapy. Results are summarized in Table 10.
Table 10. Number of Subjects (%) Reaching a Primary Clinical Endpoint (Disease Progression or Death)
| Endpoint
| La m ivudine plus
Zidovudine (n = 236) | Didanosine
(n = 235) |
| HIV-1 disease progression or death (total)
Physical growth failure Central nervous system deterioration CDC Clinical Category C Death | 15 (6.4%)
7 (3%) 4 (1.7%) 2 (0.8%) 2 (0.8%) | 37 (15.7%)
6 (2.6%) 12 (5.1%) 8 (3.4%) 11 (4.7%) |
Additional pediatric use information for patients aged 3 months and above is approved for ViiV Healthcare Company's EPIVIR ® (lamivudine) tablets and oral solution. However, due to ViiV Healthcare Company's marketing exclusivity rights, this drug product is not labeled with that pediatric information.
16 HOW SUPPLIED/STORAGE AND HANDLING
Lamivudine Scored Tablets, 150 mg
White capsule shaped, biconvex, scored film coated tablets debossed with "J" on one side and "16" on the other side, 1 and 6 seperated by a score line.
Bottle of 60 tablets
NDC 31722-753-60
Bottle of 600 tablets
NDC 31722-753-06
Blister Card of 10 Unit-dose tablets
NDC 31722-753-31
Blister pack of 100 (10 x 10) Unit-dose tablets
NDC 31722-753-32
Lamivudine Tablets, 300 mg
White capsule shaped, biconvex, film coated tablets debossed with "17" on one side and "J" on the other side.
Bottle of 30 tablets
NDC 31722-754-30
Bottle of 600 tablets
NDC 31722-754-06
Blister Card of 10 Unit-dose tablets
NDC 31722-754-31
Blister pack of 100 (10 x 10) Unit-dose tablets
NDC 31722-754-32
Recommended Storage:
Store at 20° to 25°C (68° to 77°F) [see USP Controlled Room Temperature]. Preserve in well-closed, light-resistant containers.
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labelling (Patient Information).
Lactic Acidosis/Hepatomegaly
Advise patients that lactic acidosis and severe hepatomegaly with steatosis have been reported with use of nucleoside analogues and other antiretrovirals. Advise patients to stop taking lamivudine tablets if they develop clinical symptoms suggestive of lactic acidosis or pronounced hepatotoxicity
[see Warnings and Precautions (5.1)].
Patients with Hepatitis B or C Co-infection
Inform patients co-infected with HIV-1 and HBV that deterioration of liver disease has occurred in some cases when treatment with lamivudine was discontinued. Advice patients to discuss any changes in regimen with their healthcare provider
[see Warnings and
Precautions (5.2)].
Inform patients with HIV-1/HCV co-infection that hepatic decompensation (some fatal) has occurred in HIV-1/HCV co-infected patients receiving combination antiretroviral therapy for HIV-1 and interferon alfa with or without ribavirin
[see Warnings and Precautions (5.3)].
Differences in Formulations of Lamivudine
Advise patients that lamivudine tablets contain a higher dose of the same active ingredient (lamivudine) as EPIVIR-HBV tablets. If a decision is made to include lamivudine in the HIV-1 treatment regimen of a patient co-infected with HIV-1 and HBV, the formulation and dosage of lamivudine in lamivudine tablets (not EPIVIR-HBV) should be used [see Warnings and Precautions (5.2)].
Related Products that are Not Recommended
Inform patients that they should not take lamivudine with ATRIPLA ®, COMBIVIR ®, COMPLERA ®, DUTREBIS TM, EMTRIVA ®, EPIVIR-HBV, EPZICOM ®, STRIBILD ®, TRIUMEQ ®, TRIZIVIR ®, or TRUVADA ® .
Risk of Pancreatitis
Advice parents or guardians to monitor pediatric patients for signs and symptoms of pancreatitis [see Warnings and Precautions (5.5)].
Immune Reconstitution Syndrome
Advise patients to inform their healthcare provider immediately of any signs and symptoms of infection as inflammation from previous infection may occur soon after combination antiretroviral therapy, including when lamivudine is started [see Warnings and Precautions (5.5)].
Redistribution/Accumulation of Body Fat
Inform patients that redistribution or accumulation of body fat may occur in patients receiving antiretroviral therapy and that the cause and long-term health effects of these conditions are not known at this time [see Warnings and
Pregnancy Registry
Advise patients that there is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to lamivudine during pregnancy [see Use in Specific
Lactation
Instruct women with HIV-1 infection not to breastfeed because HIV-1 can be passed to the baby in the breast milk [see Use in Specific Populations (8.2)].
Missed Dosage
Instruct patients that if they miss a dose of lamivudine tablets, to take it as soon as they remember. Advise patients not to double their next dose or take more than the prescribed dose [see Dosage and Administration (2)].
RETROVIR is registered trademark of the ViiV Healthcare group of companies.
EPIVIR-HBV is a trademark licensed to the GSK group of companies.

Manufactured for:
Camber Pharmaceuticals, Inc.,
Piscataway, NJ 08854
By: HETERO TM
Hetero Labs Limited,Unit V, Polepally, 2037443
Jadcherla, Mahaboob Nagar-509 301, India.
Revised: 08/2016
PATIENT INFORMATION
PATIENT INFORMATION
LAMIVUDINE
(lah-MEH-vyoo-deen)
TabletsWhat is the most important information I should know about lamivudine tablets?
Lamivudine tablets can cause serious side effects, including:
Build-up of an acid in your blood (lactic acidosis). Lactic acidosis can happen in some people who take lamivudine tablets. Lactic acidosis is a serious medical emergency that can cause death.
Call your healthcare provider right away if you get any of the following symptoms that could be signs of lactic acidosis:
feel very weak or tired feel cold, especially in your arms and legs
unusual (not normal) muscle pain feel dizzy or light-headed
trouble breathing have a fast or irregular heartbeat
stomach pain with nausea and vomiting
Severe liver problems can happen in people who take lamivudine tablets. In some cases these serious liver problems can lead to death. Your liver may become large (hepatomegaly) and you may develop fat in your liver (steatosis).
Call your healthcare provider right away if you get any of the following signs or symptoms of liver problems:
your skin or the white part of your eyes loss of appetite for several days or longer
turns yellow (jaundice) nausea
dark or "tea-colored” urine pain, aching, or tenderness on the right
light-colored stools (bowel side of your stomach area
movements)
You may be more likely to get lactic acidosis or serious liver problems if you are female, very overweight (obese), or have been taking nucleoside analog medicines for a long time.
Worsening of hepatitis B virus in people who have HIV-1 infection. If you have HIV-1 (Human Immunodeficiency Virus type 1) and hepatitis B virus (HBV) infection, your HBV may get worse (flare-up) if you stop taking lamivudine tablets. A "flare-up”is when your HBV infection suddenly returns in a worse way than before. Worsening liver disease from HBV can be serious and may lead to death.
Do not run out of lamivudine tablets. Refill your prescription or talk to your healthcare provider before your lamivudine tablets is all gone.
Do not stop lamivudine tablets without first talking to your healthcare provider.
If you stop taking lamivudine tablets, your healthcare provider will need to check your health often and do blood tests regularly for several months to check your liver.
Resistant Hepatitis B Virus (HBV). If you have HIV-1 and hepatitis B, the hepatitis B virus can change (mutate) during your treatment with lamivudine and become
harder to treat (resistant).
Use with interferon and ribavirin-based regimens. Worsening of liver disease that has caused death has happened in people infected with both HIV-1 and hepatitis C virus who are taking antiretroviral medicines and are also being treated for hepatitis C with interferon with or without ribavirin. If you are taking lamivudine and interferon with or without ribavirin, tell your healthcare provider if you have any new symptoms.
What are lamivudine tablets?
Lamivudine tablets are a prescription HIV-1 medicine used with other antiretroviral medicines to treat HIV-1 infections in adults and children aged 3 months and older. HIV-1 is the virus that causes Acquired Immune Deficiency Syndrome (AIDS).
Lamivudine tablets (used to treat HIV-1 infection) contain a higher dose of the same active ingredient (lamivudine) than is in the medicine EPIVIR-HBV tablets (used to treat HBV). If you have both HIV-1 and HBV, you should not use EPIVIR-HBV to treat your infections.
The safety and effectiveness of lamivudine tablets have not been established in children under 3 months of age.
Who should not take lamivudine tablets?
Do not take lamivudine tablets if you are allergic to lamivudine or any of the ingredients in lamivudine tablets. See the end of this Patient Information Leaflet for a complete list of ingredients in lamivudine tablets.
What should I tell my healthcare provider before taking lamivudine tablets?
Before you take lamivudine tablets, tell your healthcare provider if you:
have or have had liver problems, including hepatitis B or C virus infection.
have kidney problems.
have diabetes.
are pregnant or plan to become pregnant. Taking lamivudine tablets during pregnancy has not been associated with an increased risk of birth defects. Talk to your healthcare provider if you are pregnant or plan to become pregnant.
Pregnancy Registry. There is a pregnancy registry for women who take antiretroviral medicines during pregnancy. The purpose of this registry is to collect information about the health of you and your baby. Talk to your healthcare provider about how you can take part in this registry.
are breastfeeding or plan to breastfeed.
Do not breastfeed if you take lamivudine tablets.
You should not breastfeed if you have HIV-1 because of the risk of passing HIV-1 to your baby.
Tell your healthcare provider about all the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements.
Some medications interact with lamivudine tablets. Keep a list of your medicines to show your healthcare provider and pharmacist. You can ask your healthcare provider or pharmacist for a list of medicines that interact with lamivudine.
Do not start taking a new medicine without telling your healthcare provider. Your healthcare provider can tell you if it is safe to take lamivudine with other medicines.
How should I take lamivudine tablets?
Take lamivudine tablets exactly as your healthcare provider tells you to take it.
If you miss a dose of lamivudine tablets, take it as soon as you remember. Do not take 2 doses at the same time or take more than what your healthcare provider tells you to take.
Stay under the care of a healthcare provider during treatment with lamivudine tablets.
Lamivudine tablets may be taken with or without foo.
For children 3 months and older, your healthcare provider will prescribe a dose of lamivudine tablets based on your child’s body weight.
Tell your healthcare provider if you or your child has trouble swallowing tablets. Lamivudine also comes as a liquid (oral solution).
Do not run out of lamivudine. The virus in your blood may increase and the virus may become harder to treat. When your supply starts to run low, get more from
your healthcare provider or pharmacy.
If you take too much lamivudine tablets, call your healthcare provider or go to the nearest hospital emergency room right away.
What are the possible side effects of lamivudine tablets?
Lamivudine tablets can cause serious side effects including:
See "What is the most important information I should know about lamivudine tablets?”
Risk of inflammation of the pancreas (pancreatitis). Children may be at risk for developing pancreatitis during treatment with lamivudine tablets if they:
have taken nucleoside analogue have a history of pancreatitis
medicines in the past have other risk factors for pancreatitis
Call your healthcare provider right away if your child develops signs and symptoms of pancreatitis including severe upper stomach-area pain, with or without nausea and vomiting. Your healthcare provider may tell you to stop giving lamivudine tablets to your child if their symptoms and blood test results show that your child may have pancreatitis.
Changes in your immune system (Immune Reconstitution Syndrome) can happen when you start taking HIV-1 medicines. Your immune system may get stronger and begin to fight infections that have been hidden in your body for a long time. Tell your healthcare provider right away if you start having new symptoms after you start taking lamivudine tablets.
Changes in body fat can happen in people who take HIV-1 medicines. These changes may include increased amount of fat in the upper back and neck (“buffalo hump"), breast, and around the middle of your body (trunk). Loss of fat from the legs, arms, and face may also happen. The exact cause and long-term health effects of these conditions are not known.
The most common side effects of lamivudine tablets in adults include:
headache nasal signs and symptoms
nausea diarrhea
generally not feeling well cough
tiredness
The most common side effects of lamivudine tablets in children include fever and cough.
Tell your healthcare provider if you have any side effect that bothers you or that does not go away. These are not all the possible side effects of lamivudine tablets. Call your healthcare provider for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
How should I store lamivudine tablets?
Store lamivudine tablets at room temperature between 68° F to 77°F (20° to 25°C) [see USP Controlled Room Temperature].
Keep lamivudine tablets and all medicines out of the reach of children.
General information about the safe and effective use of lamivudine tablets.
Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. Do not use lamivudine tablets for a condition for which it was not prescribed. Do not give lamivudine tablets to other people, even if they have the same symptoms that you have. It may harm them.
You can ask your healthcare provider or pharmacist for information about lamivudine tablets that is written for health professionals.
What are the ingredients in lamivudine tablets?
Active ingredient: lamivudine USP
Inactive ingredients: crospovidone, isomalt, isopropyl alcohol, magnesium stearate and methylene chloride. The tablets are coated with opadry white containing hypromellose, polyethylene glycol, polysorbate 80 and titanium dioxide.
EPIVIR-HBV is a trademark licensed to the GSK group of companies.
This Patient Information has been approved by the U.S. Food and Drug Administration.

Manufactured for:
Camber Pharmaceuticals, Inc., 2037444
Piscataway, NJ 08854
By: HETERO TM
Hetero Labs Limited,Unit V, Polepally,
Jadcherla, Mahaboob Nagar-509 301, India.
Revised: 08/2016
DRUG: Lamivudine
GENERIC: Lamivudine
DOSAGE: TABLET, FILM COATED
ADMINSTRATION: ORAL
NDC: 70518-0440-0
NDC: 70518-0440-1
COLOR: white
SHAPE: CAPSULE
SCORE: Two even pieces
SIZE: 15 mm
IMPRINT: J;16
PACKAGING: 30 in 1 BLISTER PACK
PACKAGING: 14 in 1 BLISTER PACK
ACTIVE INGREDIENT(S):
- LAMIVUDINE 150mg in 1
INACTIVE INGREDIENT(S):
- CROSPOVIDONE
- POLYETHYLENE GLYCOLS
- HYPROMELLOSES
- POLYSORBATE 80
- METHYLENE CHLORIDE
- ISOMALT
- ISOPROPYL ALCOHOL
- MAGNESIUM STEARATE
- TITANIUM DIOXIDE
| LAMIVUDINE
lamivudine tablet, film coated |
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
|
||||||||||||||||||||||
| Labeler - REMEDYREPACK INC. (829572556) |