MIRENA- levonorgestrel intrauterine device
Mirena by
Drug Labeling and Warnings
Mirena by is a Prescription medication manufactured, distributed, or labeled by Bayer HealthCare Pharmaceuticals Inc., Bayer Pharma Oy, Sterigenics Belgium Petit-Rechain S.A., Bayer AG. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use MIRENA safely and effectively. See full prescribing information for MIRENA.
MIRENA (levonorgestrel-releasing intrauterine system)
Initial U.S. Approval: 2000INDICATIONS AND USAGE
DOSAGE AND ADMINISTRATION
- Initial release rate of levonorgestrel (LNG) is 20 mcg/day; this rate is reduced by about 50% after 5 years; Mirena must be removed or replaced after 5 years. (2)
- To be inserted by a trained healthcare provider using strict aseptic technique. Follow insertion instructions exactly as described. (2.1)
- Patient should be re-examined and evaluated 4 to 6 weeks after insertion; then, yearly or more often if indicated. (2.2)
DOSAGE FORMS AND STRENGTHS
- One sterile intrauterine system consisting of a T-shaped polyethylene frame with a steroid reservoir containing 52 mg levonorgestrel packaged within a sterile inserter (3)
CONTRAINDICATIONS
- Pregnancy or suspicion of pregnancy. Cannot be used for post-coital contraception (4).
- Congenital or acquired uterine anomaly if it distorts the uterine cavity (4)
- Acute pelvic inflammatory disease (PID) or a history of PID unless there has been a subsequent intrauterine pregnancy (4)
- Postpartum endometritis or infected abortion in the past 3 months (4)
- Known or suspected uterine or cervical neoplasia (4)
- Known or suspected breast cancer or other progestin-sensitive cancer (4)
- Uterine bleeding of unknown etiology (4)
- Untreated acute cervicitis or vaginitis or other lower genital tract infections (4)
- Acute liver disease or liver tumor (benign or malignant) (4)
- Increased susceptibility to pelvic infection (4)
- A previous intrauterine device (IUD) that has not been removed (4)
- Hypersensitivity to any component of Mirena (4)
WARNINGS AND PRECAUTIONS
- Remove Mirena if pregnancy occurs with Mirena in place. If pregnancy occurs, there is increased risk of ectopic pregnancy including loss of fertility, pregnancy loss, septic abortion (including septicemia, shock and death), and premature labor and delivery. (5.1, 5.2)
- Group A streptococcal infection has been reported; strict aseptic technique is essential during insertion. (5.3)
- Before using Mirena, consider the risks of PID. (5.4)
- Bleeding patterns become altered, may remain irregular and amenorrhea may ensue. (5.5)
- Perforation may occur and may reduce contraceptive effectiveness. Risk is increased if inserted in lactating women and may be increased if inserted in women with fixed retroverted uteri and postpartum. (5.6)
- Partial or complete expulsion may occur. (5.7)
- Evaluate persistent enlarged ovarian follicles or ovarian cysts. (5.8)
ADVERSE REACTIONS
The most common adverse reactions (≥10% users) are alterations of menstrual bleeding patterns, abdominal/pelvic pain, amenorrhea, headache/migraine, genital discharge, and vulvovaginitis. (6.1).
To report SUSPECTED ADVERSE REACTIONS, contact Bayer HealthCare Pharmaceuticals Inc. at 1-888-842-2937 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
- Drugs or herbal products that induce certain enzymes, such as CYP3A4, may decrease the serum concentration of progestins. (7)
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.
Revised: 6/2017
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1. Insertion Instructions
2.2 Patient Follow-up
2.3 Removal of Mirena
2.4 Continuation of Contraception after Removal
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Ectopic Pregnancy
5.2 Intrauterine Pregnancy
5.3 Sepsis
5.4 Pelvic Infection
5.5 Irregular Bleeding and Amenorrhea
5.6 Perforation
5.7 Expulsion
5.8 Ovarian Cysts
5.9 Breast Cancer
5.10 Clinical Considerations for Use and Removal
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
6.2 Postmarketing Experience
7 DRUG INTERACTIONS
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.4 Pediatric Use
8.5 Geriatric Use
8.6 Hepatic Impairment
8.7 Renal Impairment
11 DESCRIPTION
11.1 Mirena
11.2 Inserter
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
14.1 Clinical Trials on Contraception
14.2 Clinical Trial on Heavy Menstrual Bleeding
15 REFERENCES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- * Sections or subsections omitted from the full prescribing information are not listed.
-
1 INDICATIONS AND USAGE
- Mirena is indicated for intrauterine contraception for up to 5 years.
- Mirena is also indicated for the treatment of heavy menstrual bleeding in women who choose to use intrauterine contraception as their method of contraception.
The system should be replaced after 5 years if continued use is desired.
-
2 DOSAGE AND ADMINISTRATION
Mirena contains 52 mg of levonorgestrel (LNG). Initially, LNG is released at a rate of approximately 20 mcg/day. This rate decreases progressively to half that value after 5 years.
Mirena must be removed by the end of the fifth year and can be replaced at the time of removal with a new Mirena if continued contraceptive protection is desired.
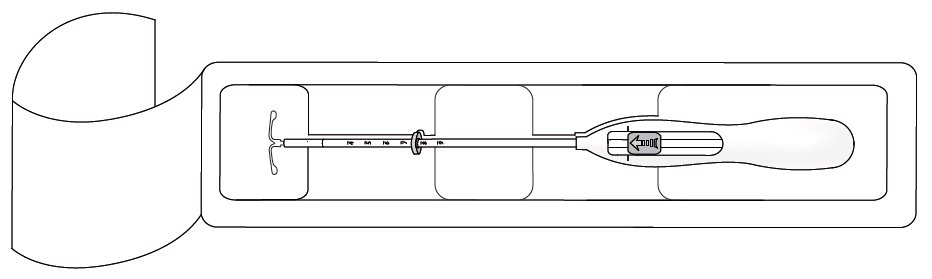
Mirena is supplied within an inserter in a sterile package (see Figure 1) that must not be opened until required for insertion [see Description (11.2)]. Do not use if the seal of the sterile package is broken or appears compromised. Use strict aseptic techniques throughout the insertion procedure [see Warnings and Precautions (5.3)].
2.1. Insertion Instructions
- A complete medical and social history should be obtained to determine conditions that might influence the selection of a levonorgestrel-releasing intrauterine system (LNG IUS) for contraception. If indicated, perform a physical examination, and appropriate tests for any forms of genital or other sexually transmitted infections. [See Contraindications (4) and Warnings and Precautions (5.10).]
- Follow the insertion instructions exactly as described in order to ensure proper placement and avoid premature release of Mirena from the inserter. Once released, Mirena cannot be re-loaded.
- Mirena should be inserted by a trained healthcare provider. Healthcare providers should become thoroughly familiar with the insertion instructions before attempting insertion of Mirena.
- Insertion may be associated with some pain and/or bleeding or vasovagal reactions (for example, syncope, bradycardia), or with seizure in an epileptic patient, especially in patients with a predisposition to these symptoms. Consider administering analgesics prior to insertion.
Timing of Insertion
Table 1: When to Insert Mirena Starting Mirena in women not currently using hormonal or intrauterine contraception
Mirena can be inserted any time the provider can be reasonably certain the woman is not pregnant. Consider the possibility of ovulation and conception prior to initiation of this product [see Contraindications (4)].
If Mirena is inserted during the first seven days of the menstrual cycle or immediately after a first trimester abortion, back up contraception is not needed.
If Mirena is not inserted during the first seven days of the menstrual cycle, a barrier method of contraception should be used or the patient should abstain from vaginal intercourse for seven days to prevent pregnancy.
Switching to Mirena from an oral, transdermal or vaginal hormonal contraceptive
Mirena may be inserted at any time, including during the hormone-free interval of the previous method.
If inserted during active use of the previous method, continue that method for 7 days after Mirena insertion or until the end of the current treatment cycle.
If the woman was using continuous hormonal contraception, discontinue that method seven days after Mirena insertion.
Switching to Mirena from an injectable progestin contraceptive
Mirena may be inserted at any time; a back-up method of contraception (such as condoms or spermicide) should also be used for 7 days if Mirena is inserted more than 3 months (13 weeks) after the last injection.
Switching to Mirena from a contraceptive implant or another IUS
Insert Mirena on the same day the implant or IUS is removed.
Mirena may be inserted at any time during the menstrual cycle.
Inserting Mirena after abortion or miscarriage
First-trimester
Mirena may be inserted immediately after a first-trimester abortion or miscarriage.
Second-trimester
Do not insert Mirena until a minimum of 6 weeks after second trimester abortion or miscarriage, or until the uterus is fully involuted. If involution is delayed, wait until involution is complete before insertion [see Warnings and Precautions (5.6, 5.7)].
If the woman has not yet had a period, consider the possibility of ovulation and conception occurring prior to insertion of Mirena. [See Contraindications (4), Warnings and Precautions (5.2), and FDA-Approved Patient Labeling.] Mirena can be inserted any time the provider can be reasonably certain the woman is not pregnant.
If Mirena is not inserted during the first 7 days of the menstrual cycle, a back-up method of contraception should be used or the patient should abstain from vaginal intercourse for 7 days to prevent pregnancy.
Inserting Mirena after Childbirth
Do not insert Mirena until a minimum of 6 weeks after delivery, or until the uterus is fully involuted. If involution is delayed, wait until involution is complete before insertion [see Warnings and Precautions (5.6, 5.7)].
If the woman has not yet had a period, consider the possibility of ovulations and conception occurring prior to insertion of Mirena. [See Contraindications (4), Warnings and Precautions (5.2), and FDA-Approved Patient Labeling.] Mirena can be inserted any time the provider can be reasonably certain the woman is not pregnant.
If Mirena is not inserted during the first 7 days of the menstrual cycle, a back-up method of contraception should be used or the patient should abstain from vaginal intercourse for 7 days to prevent pregnancy.
There is an increased risk of perforation in lactating women. [See Warnings and Precautions (5.7).]
Preparation for insertion
- Exclude pregnancy and confirm that there are no other contraindications to the use of Mirena.
- Ensure that the patient understands the contents of the Patient Information Booklet and obtain the signed patient informed consent located on the last page of the Patient Information Booklet. With the patient comfortably in lithotomy position, do a bimanual exam to establish the size, shape and position of the uterus.
- Gently insert a speculum to visualize the cervix.
- Thoroughly cleanse the cervix and vagina with a suitable antiseptic solution.
- Prepare to sound the uterine cavity. Grasp the upper lip of the cervix with a tenaculum forceps and gently apply traction to stabilize and align the cervical canal with the uterine cavity. Perform a paracervical block if needed. If the uterus is retroverted, it may be more appropriate to grasp the lower lip of the cervix. The tenaculum should remain in position and gentle traction on the cervix should be maintained throughout the insertion procedure.
- Gently insert a uterine sound to check the patency of the cervix, measure the depth of the uterine cavity in centimeters, confirm cavity direction, and detect the presence of any uterine anomaly. If you encounter difficulty or cervical stenosis, use dilatation, and not force, to overcome resistance. If cervical dilatation is required, consider using a paracervical block.
- The uterus should sound to a depth of 6 to 10 cm. Insertion of Mirena into a uterine cavity less than 6 cm by sounding may increase the incidence of expulsion, bleeding, pain, perforation, and possibly pregnancy.
Insertion Procedure
Proceed with insertion only after completing the above steps and ascertaining that the patient is appropriate for Mirena. Ensure use of aseptic technique throughout the entire procedure.
Step 1–Opening of the package
- Open the package (Figure 1). The contents of the package are sterile.
- Using sterile gloves lift the handle of the sterile inserter and remove from the sterile package.
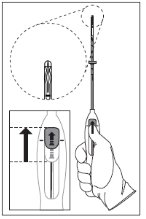
Step 2–Load Mirena into the insertion tube
- Push the slider forward as far as possible in the direction of the arrow thereby moving the insertion tube over the Mirena T-body to load Mirena into the insertion tube (Figure 2). The tips of the arms will meet to form a rounded end that extends slightly beyond the insertion tube.
- Maintain forward pressure with your thumb or forefinger on the slider. DO NOT move the slider downward at this time as this may prematurely release the threads of Mirena. Once the slider is moved below the mark, Mirena cannot be re-loaded.
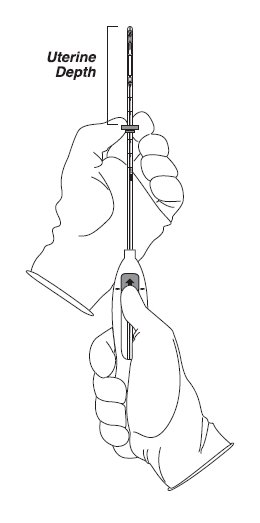
Step 3–Setting the flange
- Holding the slider in this forward position, set the upper edge of the flange to correspond to the uterine depth (in centimeters) measured during sounding (Figure 3).
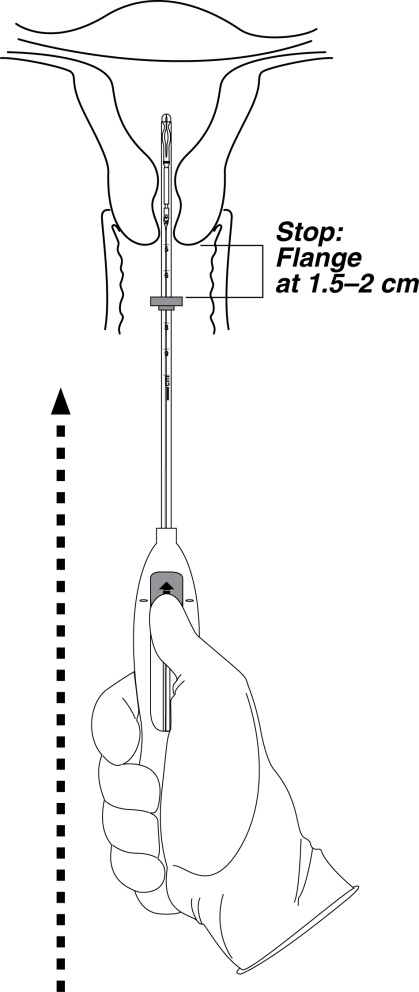
Step 4–Mirena is now ready to be inserted
- Continue holding the slider in this forward position. Advance the inserter through the cervix until the flange is approximately 1.5–2 cm from the cervix and then pause (Figure 4).
Do not force the inserter. If necessary, dilate the cervical canal.
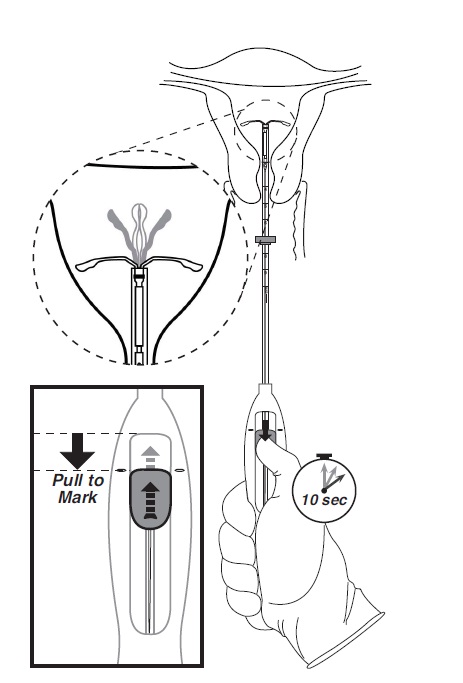
Step 5–Open the arms
While holding the inserter steady, move the slider down to the mark to release the arms of Mirena (Figure 5). Wait 10 seconds for the horizontal arms to open completely.
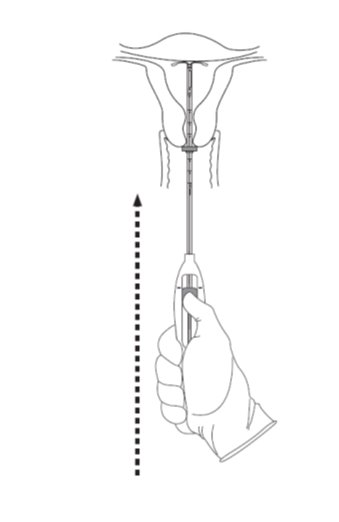
Step 6–Advance to fundal position
- Advance the inserter gently towards the fundus of the uterus until the flange touches the cervix. If you encounter fundal resistance do not continue to advance. Mirena is now in the fundal position (Figure 6). Fundal positioning of Mirena is important to prevent expulsion.
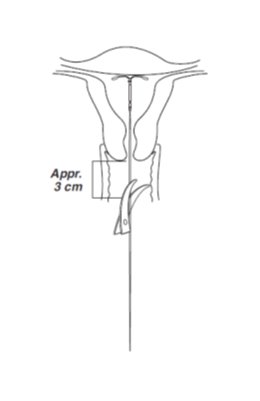
Step 7–Release Mirena and withdraw the inserter
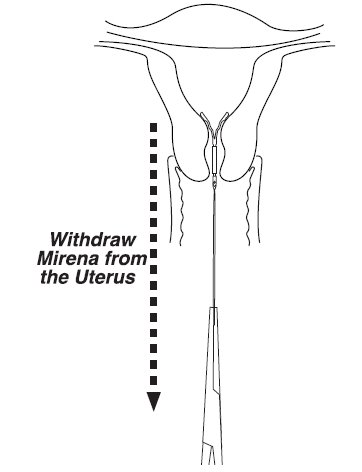
- Holding the entire inserter firmly in place, release Mirena by moving the slider all the way down (Figure 7).
- Continue to hold the slider all the way down while you slowly and gently withdraw the inserter from the uterus.
- Using a sharp, curved scissor, cut the threads perpendicular, leaving about 3 cm visible outside of the cervix [cutting threads at an angle may leave sharp ends (Figure 8)]. Do not apply tension or pull on the threads when cutting to prevent displacing Mirena.
Mirena insertion is now complete. Prescribe analgesics, if indicated. Keep a copy of the Consent Form with lot number for your records.
Important information to consider during or after insertion
- If you suspect that Mirena is not in the correct position, check placement (for example, using transvaginal ultrasound). Remove Mirena if it is not positioned completely within the uterus. A removed Mirena must not be re-inserted.
- If there is clinical concern, exceptional pain or bleeding during or after insertion, appropriate steps (such as physical examination and ultrasound) should be taken immediately to exclude perforation.
2.2 Patient Follow-up
- Reexamine and evaluate patients 4 to 6 weeks after insertion and once a year thereafter, or more frequently if clinically indicated.
2.3 Removal of Mirena
Timing of Removal
- Mirena should not remain in the uterus after 5 years.
- If pregnancy is not desired, the removal should be carried out during menstruation, provided the woman is still experiencing regular menses. If removal will occur at other times during the cycle, consider starting a new contraceptive method a week prior to removal. If removal occurs at other times during the cycle and the woman has had intercourse in the week prior to removal, she is at risk of pregnancy. [See Dosage and Administration (2.4).]
Removal Procedure
- Remove Mirena by applying gentle traction on the threads with forceps. (Figure 9).
- If the threads are not visible, determine location of Mirena by ultrasound [see Warnings and Precautions (5.10)].
- If Mirena is found to be in the uterine cavity on ultrasound exam, it may be removed using a narrow forceps, such as an alligator forceps. This may require dilation of the cervical canal. After removal of Mirena, examine the system to ensure that it is intact.
- Removal may be associated with some pain and/or bleeding or vasovagal reactions (for example, syncope, or a seizure in an epileptic patient).
2.4 Continuation of Contraception after Removal
- If pregnancy is not desired and if a woman wishes to continue using Mirena, a new system can be inserted immediately after removal any time during the cycle.
- If a patient with regular cycles wants to start a different birth control method, time removal and initiation of new method to ensure continuous contraception. Either remove Mirena during the first 7 days of the menstrual cycle and start the new method immediately thereafter or start the new method at least 7 days prior to removing Mirena if removal is to occur at other times during the cycle.
- If a patient with irregular cycles or amenorrhea wants to start a different birth control method, start the new method at least 7 days before removal.
- 3 DOSAGE FORMS AND STRENGTHS
-
4 CONTRAINDICATIONS
The use of Mirena is contraindicated when one or more of the following conditions exist:
- Pregnancy or suspicion of pregnancy; cannot be used for post-coital contraception [see Warnings and Precautions (5.2)]
- Congenital or acquired uterine anomaly including fibroids if they distort the uterine cavity
- Acute pelvic inflammatory disease or a history of pelvic inflammatory disease unless there has been a subsequent intrauterine pregnancy [see Warnings and Precautions (5.4)]
- Postpartum endometritis or infected abortion in the past 3 months
- Known or suspected uterine or cervical neoplasia
- Known or suspected breast cancer or other progestin-sensitive cancer, now or in the past
- Uterine bleeding of unknown etiology
- Untreated acute cervicitis or vaginitis, including bacterial vaginosis or other lower genital tract infections until infection is controlled
- Acute liver disease or liver tumor (benign or malignant)
- Conditions associated with increased susceptibility to pelvic infections [see Warnings and Precautions (5.4 )]
- A previously inserted intrauterine device (IUD) that has not been removed
- Hypersensitivity to any component of this product [see Adverse Reactions (6.2)]
-
5 WARNINGS AND PRECAUTIONS
5.1 Ectopic Pregnancy
Evaluate women for ectopic pregnancy if they become pregnant with Mirena in place because the likelihood of a pregnancy being ectopic is increased with Mirena. Up to half of pregnancies that occur with Mirena in place are likely to be ectopic. Also consider the possibility of ectopic pregnancy in the case of lower abdominal pain, especially in association with missed periods or if an amenorrheic woman starts bleeding.
The incidence of ectopic pregnancy in clinical trials with Mirena, which excluded women with a history of ectopic pregnancy, was approximately 0.1% per year. The risk of ectopic pregnancy, in women who have a history of ectopic pregnancy and use Mirena is unknown. Women with a previous history of ectopic pregnancy, tubal surgery or pelvic infection carry a higher risk of ectopic pregnancy. Ectopic pregnancy may result in loss of fertility.
5.2 Intrauterine Pregnancy
If pregnancy occurs while using Mirena, remove Mirena because leaving it in place may increase the risk of spontaneous abortion and preterm labor. Removal of Mirena or probing of the uterus may also result in spontaneous abortion. In the event of an intrauterine pregnancy with Mirena, consider the following:
Septic abortion
In patients becoming pregnant with an IUD in place, septic abortion - with septicemia, septic shock, and death - may occur.
Continuation of pregnancy
If a woman becomes pregnant with Mirena in place and if Mirena cannot be removed or the woman chooses not to have it removed, warn her that failure to remove Mirena increases the risk of miscarriage, sepsis, premature labor and premature delivery. Follow her pregnancy closely and advise her to report immediately any symptom that suggests complications of the pregnancy.
Long-term effects and congenital anomalies
When pregnancy continues with Mirena in place, long-term effects on the offspring are unknown. Congenital anomalies in live births have occurred infrequently. No clear trend towards specific anomalies has been observed. Because of the local exposure of the fetus to LNG, the possibility of teratogenicity following exposure to Mirena cannot be completely excluded. Some observational data support a small increased risk of masculinization of the external genitalia of the female fetus following exposure to progestins at doses greater than those currently used for oral contraception. Whether these data apply to Mirena is unknown.
5.3 Sepsis
Severe infection or sepsis, including Group A streptococcal sepsis (GAS), have been reported following insertion of Mirena. In some cases, severe pain occurred within hours of insertion followed by sepsis within days. Because death from GAS is more likely if treatment is delayed, it is important to be aware of these rare but serious infections. Aseptic technique during insertion of Mirena is essential in order to minimize serious infections such as GAS.
5.4 Pelvic Infection
Pelvic Inflammatory Disease (PID)
Mirena is contraindicated in the presence of known or suspected PID or in women with a history of PID unless there has been a subsequent intrauterine pregnancy [see Contraindications (4)]. IUDs have been associated with an increased risk of PID, most likely due to organisms being introduced into the uterus during insertion. In clinical trials, total combined upper genital infections were reported in 3.5% of Mirena users. More specifically, endometritis was reported in 2.1%, PID in 0.6%, and all other upper genital infections in ≤0.5% of women overall. These infections occurred more frequently within the first year. In a clinical trial with other IUDs1 and a clinical trial with an IUD similar to Mirena, the highest rate occurred within the first month after insertion.
Promptly examine users with complaints of lower abdominal or pelvic pain, odorous discharge, unexplained bleeding, fever, genital lesions or sores. Remove Mirena in cases of recurrent endometritis or PID, or if an acute pelvic infection is severe or does not respond to treatment.
Women at increased risk for PID
PID is often associated with a sexually transmitted infection, and Mirena does not protect against sexually transmitted infection. The risk of PID is greater for women who have multiple sexual partners, and also for women whose sexual partner(s) have multiple sexual partners. Women who have had PID are at increased risk for a recurrence or re-infection. In particular, ascertain whether the woman is at increased risk of infection (for example, leukemia, acquired immune deficiency syndrome [AIDS], IV drug abuse).
Treatment of PID
Following a diagnosis of PID, or suspected PID, bacteriologic specimens should be obtained and antibiotic therapy should be initiated promptly. Removal of Mirena after initiation of antibiotic therapy is usually appropriate. Guidelines for PID treatment are available from the Centers for Disease Control (CDC), Atlanta, Georgia.
Actinomycosis
Actinomycosis has been associated with IUDs. Symptomatic women should have Mirena removed and should receive antibiotics. The significance of actinomyces-like organisms on Pap smear in an asymptomatic IUD user is unknown, and so this finding alone does not always require Mirena removal and treatment. When possible, confirm a Pap smear diagnosis with cultures.
5.5 Irregular Bleeding and Amenorrhea
Mirena can alter the bleeding pattern and result in spotting, irregular bleeding, heavy bleeding, oligomenorrhea and amenorrhea. During the first three to six months of Mirena use, the number of bleeding and spotting days may be increased and bleeding patterns may be irregular. Thereafter the number of bleeding and spotting days usually decreases but bleeding may remain irregular. If bleeding irregularities develop during prolonged treatment, appropriate diagnostic measures should be taken to rule out endometrial pathology.
Amenorrhea develops in approximately 20% of Mirena users by one year. The possibility of pregnancy should be considered if menstruation does not occur within six weeks of the onset of previous menstruation. Once pregnancy has been excluded, repeated pregnancy tests are generally not necessary in amenorrheic women unless indicated, for example, by other signs of pregnancy or by pelvic pain [see Clinical Studies (14.1)].
In most women with heavy menstrual bleeding, the number of bleeding and spotting days may also increase during the initial months of therapy but usually decrease with continued use; the volume of blood loss per cycle progressively becomes reduced [see Clinical Studies (14.2)].
5.6 Perforation
Perforation (total or partial, including penetration/embedment of Mirena in the uterine wall or cervix) may occur most often during insertion, although the perforation may not be detected until sometime later. Perforation may reduce contraceptive efficacy and result in pregnancy. The incidence of perforation during clinical trials, which excluded breast-feeding women, was < 0.1%.
If perforation occurs, locate and remove Mirena. Surgery may be required. Delayed detection or removal of Mirena in case of perforation may result in migration outside the uterine cavity, adhesions, peritonitis, intestinal perforations, intestinal obstruction, abscesses and erosion of adjacent viscera.
The risk of perforation may be increased if Mirena is inserted when the uterus is fixed retroverted or not completely involuted. Delay Mirena insertion a minimum of six weeks or until involution is complete following a delivery or a second trimester abortion.
A large postmarketing safety study conducted in Europe over a 1-year observational period reported that lactation at the time of insertion of an IUD/IUS was associated with an increased risk of perforation. For Mirena users, the incidence of uterine perforation was reported as 6.3 per 1,000 insertions for lactating women, compared to 1.0 per 1,000 insertions for non-lactating women.
5.7 Expulsion
Partial or complete expulsion of Mirena may occur resulting in the loss of contraceptive protection. Expulsion may be associated with symptoms of bleeding or pain, or it may be asymptomatic and go unnoticed. Mirena typically decreases menstrual bleeding over time; therefore, an increase of menstrual bleeding may be indicative of an expulsion. The risk of expulsion may be increased when the uterus is not completely involuted. In clinical trials, a 4.5% expulsion rate was reported over the 5-year study duration.
Delay Mirena insertion a minimum of six weeks or until uterine involution is complete following a delivery or a second trimester abortion. Remove a partially expelled Mirena. If expulsion has occurred, a new Mirena can be inserted any time the provider can be reasonably certain the woman is not pregnant..
5.8 Ovarian Cysts
Because the contraceptive effect of Mirena is mainly due to its local effects within the uterus, ovulatory cycles with follicular rupture usually occur in women of fertile age using Mirena. Sometime atresia of the follicle is delayed and the follicle may continue to grow. Ovarian cysts have been reported in approximately 8% of women using Mirena. Most of these cysts are asymptomatic, although some may be accompanied by pelvic pain or dyspareunia.
In most cases the ovarian cysts disappear spontaneously during two to three months observation. Evaluate persistent ovarian cysts. Surgical intervention is not usually required.
5.9 Breast Cancer
Women who currently have or have had breast cancer, or have a suspicion of breast cancer, should not use hormonal contraception because some breast cancers are hormone-sensitive [see Contraindications (4)].
Spontaneous reports of breast cancer have been received during postmarketing experience with Mirena. Observational studies of the risk of breast cancer with use of a LNG-releasing IUS do not provide conclusive evidence of increased risk.
5.10 Clinical Considerations for Use and Removal
Use Mirena with caution after careful assessment if any of the following conditions exist, and consider removal of the system if any of them arise during use:
- Coagulopathy or use of anticoagulants
- Migraine, focal migraine with asymmetrical visual loss or other symptoms indicating transient cerebral ischemia
- Exceptionally severe headache
- Marked increase of blood pressure
- Severe arterial disease such as stroke or myocardial infarction
In addition, consider removing Mirena if any of the following conditions arise during use [see Contraindications (4)]:
- Uterine or cervical malignancy
- Jaundice
If the threads are not visible or are significantly shortened they may have broken or retracted into the cervical canal or uterus. Consider the possibility that the system may have been displaced (for example, expelled or perforated the uterus) [see Warnings and Precautions (5.6, 5.7)]. Exclude pregnancy and verify the location of Mirena, for example, by sonography, X-ray, or by gentle exploration of the cervical canal with a suitable instrument. If Mirena is displaced, remove it. A new Mirena may be inserted at that time or during the next menses if it is certain that conception has not occurred. If Mirena is in place with no evidence of perforation, no intervention is indicated.
-
6 ADVERSE REACTIONS
The following serious or otherwise important adverse reactions are discussed in elsewhere in the labeling:
- Ectopic Pregnancy [see Warnings and Precautions (5.1)]
- Intrauterine Pregnancy [see Warnings and Precautions (5.2)]
- Group A Streptococcal Sepsis (GAS) [see Warnings and Precautions (5.3)]
- Pelvic Inflammatory Disease [see Warnings and Precautions (5.4)]
- Alterations of Bleeding Patterns [see Warnings and Precautions (5.5)]
- Perforation [see Warnings and Precautions (5.6)]
- Expulsion [see Warnings and Precautions (5.7)]
- Ovarian Cysts [see Warnings and Precautions (5.8)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical studies of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The data provided reflect the experience with the use of Mirena in the adequate and well-controlled studies as well as in the supportive and uncontrolled studies for contraception and heavy menstrual bleeding (n=5,091). The data cover more than 12,101 women-years of exposure, mainly in the contraception studies (11,761 women-years). The frequencies of reported adverse drug reactions represent crude incidences.
The most common adverse reactions (≥10% users) are alterations of menstrual bleeding patterns [including unscheduled uterine bleeding (31.9%), decreased uterine bleeding (23.4%), increased scheduled uterine bleeding (11.9%), and female genital tract bleeding (3.5%)], abdominal/pelvic pain (22.6%), amenorrhea (18.4%), headache/migraine (16.3%), genital discharge (14.9%), and vulvovaginitis (10.5%). Adverse reactions reported in ≥ 5% of users are shown in Table 2.
Table 2: Adverse Reactions ≥ 5% Reported in Clinical Trials with Mirena System Organ Class
Adverse Reactions
% (N= 5,091)
Reproductive system and breast disorders
alteration of menstrual bleeding pattern, including:
unscheduled uterine bleeding
decreased uterine bleeding
increased scheduled uterine bleeding
female genital tract bleeding
31.9
23.4
11.9
3.5
amenorrhea
18.4
genital discharge
14.9
vulvovaginitis
10.5
breast pain
8.5
benign ovarian cyst and associated complications
7.5
dysmenorrhea
6.4
Gastrointestinal disorders
abdominal/pelvic pain
22.6
Nervous system disorders
headache/migraine
16.3
Musculoskeletal and connective tissue disorders
back pain
7.9
Skin and subcutaneous
tissue disordersacne
6.8
Psychiatric disorders
depression/depressive mood
6.4
Other adverse reactions occurring in <5% of subjects include alopecia, (partial and complete) device expulsion, hirsutism, nausea, and PID/endometritis.
6.2 Postmarketing Experience
The following adverse reactions have been identified during post approval use of Mirena. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
- Arterial thrombotic and venous thromboembolic events, including cases of pulmonary emboli, deep vein thrombosis and stroke
- Device breakage
- Hypersensitivity (including rash, urticaria and angioedema)
- Increased blood pressure
-
7 DRUG INTERACTIONS
No drug-drug interaction studies have been conducted with Mirena.
Drugs or herbal products that induce enzymes, including CYP3A4, that metabolize progestins may decrease the serum concentrations of progestins.
Some drugs or herbal products that may decrease the serum concentration of LNG include:
- Barbiturates
- Bosentan
- Carbamazepine
- Efavirenz
- Felbamate
- Griseofulvin
- Nevirapine
- Oxcarbazepine
- Phenytoin
- Rifabutin
- Rifampin
- St. John’s wort
- Topiramate
Significant changes (increase or decrease) in the serum concentrations of the progestin have been noted in some cases of co-administration with HIV protease inhibitors or with non-nucleoside reverse transcriptase inhibitors. CYP3A4 inhibitors such as itraconazole or ketoconazole may increase plasma hormone levels.
Consult the labeling of all concurrently used drugs to obtain further information about interactions with Mirena or the potential for enzyme alterations.
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
The use of Mirena is contraindicated in pregnancy or with a suspected pregnancy because there is no need for pregnancy prevention in a woman who is already pregnant and Mirena may cause adverse pregnancy outcomes [see Contraindications (4), Warnings and Precautions (5.1, 5.2)]. If a woman becomes pregnant with Mirena in place, the likelihood of ectopic pregnancy is increased and there is an increased risk of miscarriage, sepsis, premature labor, and premature delivery. Remove Mirena, if possible, if pregnancy occurs in a woman using Mirena. If Mirena cannot be removed, follow the pregnancy closely [see Warnings and Precautions (5.1, 5.2)].
Studies report no adverse effects on fetal and infant development associated with long-term use of contraceptive doses of oral progestins in a pregnant woman. However, there have been reported cases of masculinization of the external genitalia of the female fetus following exposure to progestins at doses greater than those currently used for oral contraception.
8.2 Lactation
Risk Summary
Published studies report the presence of LNG in human milk. Small amounts of progestins (approximately 0.1% of the total maternal doses) were detected in the breast milk of nursing mothers who used Mirena, resulting in exposure of LNG to the breastfed infants. There are no reports of adverse effects in breastfed infants with maternal use of progestin-only contraceptives. Isolated cases of decreased milk production have been reported with Mirena. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for Mirena and any potential adverse effects on the breastfed child from Mirena or from the underlying maternal condition.
8.4 Pediatric Use
Safety and efficacy of Mirena have been established in women of reproductive age. Efficacy is expected to be the same for postpubertal females under the age of 18 as for users 18 years and older. Use of this product before menarche is not indicated.
8.5 Geriatric Use
Mirena has not been studied in women over age 65 and is not approved for use in this population.
8.6 Hepatic Impairment
No studies were conducted to evaluate the effect of hepatic disease on the disposition of LNG released from Mirena [see Contraindications (4)].
-
11 DESCRIPTION
Mirena (levonorgestrel-releasing intrauterine system) contains 52 mg of LNG, a progestin, and is intended to provide an initial release rate of approximately 20 mcg/day of LNG.
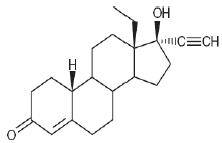
Levonorgestrel USP, (-)-13-Ethyl-17-hydroxy-18,19-dinor-17α-pregn-4-en-20-yn-3-one, the active ingredient in Mirena, has a molecular weight of 312.4, a molecular formula of C21H28O2, and the following structural formula:
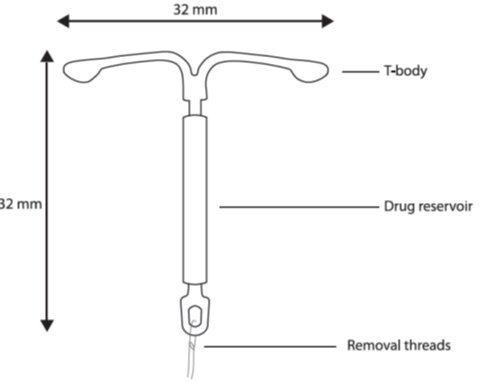
11.1 Mirena
Mirena consists of a T-shaped polyethylene frame (T-body) with a steroid reservoir (hormone elastomer core) around the vertical stem. The reservoir consists of a white or almost white cylinder, made of a mixture of levonorgestrel and silicone (polydimethylsiloxane), containing a total of 52 mg levonorgestrel. The reservoir is covered by a semi-opaque silicone (polydimethylsiloxane) membrane. The T-body is 32 mm in both the horizontal and vertical directions. The polyethylene of the T-body is compounded with barium sulfate, which makes it radiopaque. A monofilament brown polyethylene removal thread is attached to a loop at the end of the vertical stem of the T-body. The polyethylene of the removal thread contains iron oxide as a colorant (see Figure 10).
The components of Mirena, including its packaging, are not manufactured using natural rubber latex.
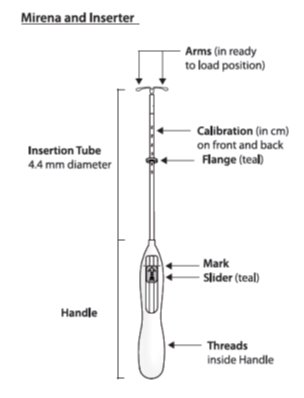
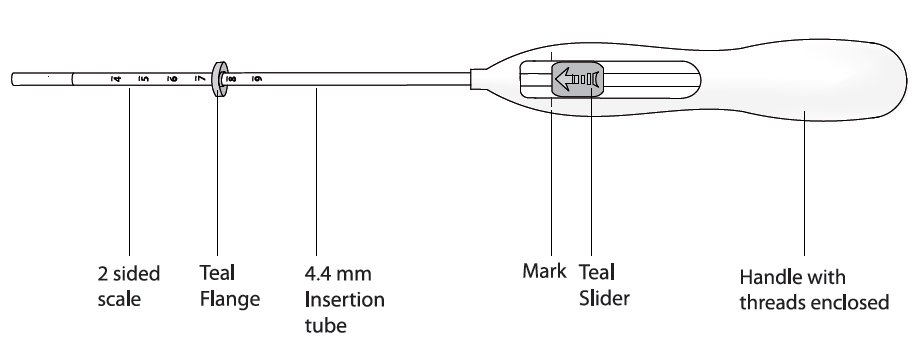
11.2 Inserter
Mirena is packaged sterile within an inserter. The inserter (Figure 11), which is used for insertion of Mirena into the uterine cavity, consists of a symmetric two-sided body and slider that are integrated with flange, lock, pre-bent insertion tube and plunger. The outer diameter of the insertion tube is 4.4 mm. The vertical stem of Mirena is loaded in the insertion tube at the tip of the inserter. The arms are pre-aligned in the horizontal position. The removal threads are contained within the insertion tube and handle. Once Mirena has been placed, the inserter is discarded.
Figure 11 Diagram of Inserter
Figure 11 Diagram of Inserter
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
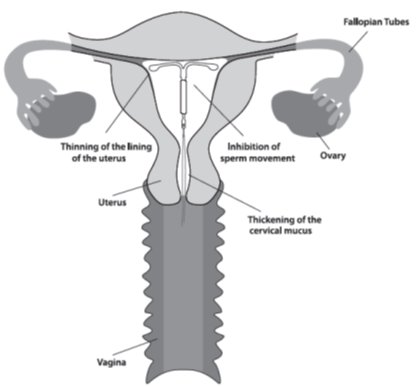
The local mechanism by which continuously released LNG enhances contraceptive effectiveness of Mirena has not been conclusively demonstrated. Studies of Mirena and similar LNG IUS prototypes have suggested several mechanisms that prevent pregnancy: thickening of cervical mucus preventing passage of sperm into the uterus, inhibition of sperm capacitation or survival, and alteration of the endometrium.
12.2 Pharmacodynamics
Mirena has mainly local progestogenic effects in the uterine cavity. The high local levels of LNG2 lead to morphological changes including stromal pseudodecidualization, glandular atrophy, a leukocytic infiltration and a decrease in glandular and stromal mitoses.
Ovulation is inhibited in some women using Mirena. In a 1-year study, approximately 45% of menstrual cycles were ovulatory, and in another study after 4 years, 75% of cycles were ovulatory.
12.3 Pharmacokinetics
Absorption
Low doses of LNG are administered into the uterine cavity with the Mirena intrauterine delivery system. The initial release rate is approximately 20 mcg/day over the first 3 months tested (day 0 to day 90). It is reduced to approximately 18 mcg/day after 1 year and then decreases progressively to approximately 10 mcg/day after 5 years.
A stable serum concentration, without peaks and troughs, of LNG of 150–200 pg/mL occurs after the first few weeks following insertion of Mirena. LNG concentrations after long-term use of 12, 24, and 60 months were 180±66 pg/mL, 192±140 pg/mL, and 159±59 pg/mL, respectively.
Distribution
The apparent volume of distribution of LNG is reported to be approximately 1.8 L/kg. It is about 97.5 to 99% protein-bound, principally to sex hormone binding globulin (SHBG) and, to a lesser extent, serum albumin.
Metabolism
Following absorption, LNG is conjugated at the 17β-OH position to form sulfate conjugates and, to a lesser extent, glucuronide conjugates in serum. Significant amounts of conjugated and unconjugated 3α, 5β- tetrahydrolevonorgestrel are also present in serum, along with much smaller amounts of 3α, 5α-tetrahydrolevonorgestrel and 16β-hydroxylevonorgestrel. LNG and its phase I metabolites are excreted primarily as glucuronide conjugates. Metabolic clearance rates may differ among individuals by several-fold, and this may account in part for wide individual variations in LNG concentrations seen in individuals using LNG–containing contraceptive products. In vitro studies have demonstrated that oxidative metabolism of LNG is catalyzed by CYP enzymes, especially CYP3A4.
Excretion
About 45% of LNG and its metabolites are excreted in the urine and about 32% are excreted in feces, mostly as glucuronide conjugates. The elimination half-life of LNG after daily oral doses is approximately 17 hours.
Specific Populations
Pediatric: Safety and efficacy of Mirena have been established in women of reproductive age. Use of this product before menarche is not indicated.
Geriatric: Mirena has not been studied in women over age 65 and is not currently approved for use in this population.
Race: No studies have evaluated the effect of race on pharmacokinetics of Mirena.
Hepatic Impairment: No studies were conducted to evaluate the effect of hepatic disease on the disposition of Mirena.
Renal Impairment: No formal studies were conducted to evaluate the effect of renal disease on the disposition of Mirena.
Drug-Drug Interactions
No drug-drug interaction studies were conducted with Mirena [see Drug Interactions (7)].
- 13 NONCLINICAL TOXICOLOGY
-
14 CLINICAL STUDIES
14.1 Clinical Trials on Contraception
Mirena has been studied for safety and efficacy in two large clinical trials in Finland and Sweden. In study sites having verifiable data and informed consent, 1,169 women 18 to 35 years of age at enrollment used Mirena for up to 5 years, for a total of 45,000 women-months of exposure. Of these, 5.6% (66) were nulliparous women. Subjects had previously been pregnant, had no history of ectopic pregnancy, had no history of pelvic inflammatory disease over the preceding 12 months, were predominantly Caucasian, and over 70% of the participants had previously used IUDs (intrauterine devices). The reported 12-month pregnancy rates were less than or equal to 0.2 per 100 women (0.2%) and the cumulative 5-year pregnancy rate was approximately 0.7 per 100 women (0.7%).
About 80% of women wishing to become pregnant conceived within 12 months after removal of Mirena.
14.2 Clinical Trial on Heavy Menstrual Bleeding
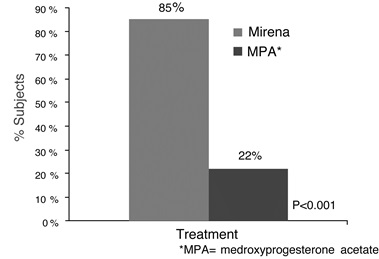
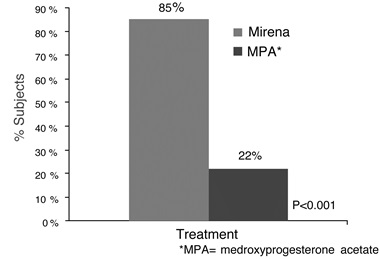
The efficacy of Mirena in the treatment of heavy menstrual bleeding was studied in a randomized, open-label, active-control, parallel-group trial comparing Mirena (n=79) to an approved therapy, medroxyprogesterone acetate (MPA) (n=81), over 6 cycles. The subjects included reproductive-aged women in good health, with no contraindications to the drug products and with confirmed heavy menstrual bleeding (≥ 80 mL menstrual blood loss [MBL]) determined using the alkaline hematin method. Excluded were women with organic or systemic conditions that may cause heavy uterine bleeding (except small fibroids, with total volume not > 5 mL). Treatment with Mirena showed a statistically significantly greater reduction in MBL (see Figure 12) and a statistically significantly greater number of subjects with successful treatment (see Figure 13). Successful treatment was defined as proportion of subjects with (1) end-of-study MBL < 80 mL and (2) a ≥ 50% decrease in MBL from baseline to end-of-study.
Figure 13 Proportion of Subjects with Successful Treatment
Figure 13 Proportion of Subjects with Successful Treatment
-
15 REFERENCES
1Farley T M M, Rosenberg M J, Rowe P J, Chen J, Meirik O. Intrauterine devices and pelvic inflammatory disease: an international perspective. Lancet 1992; 339:785-788.
2Nilsson CG, Haukkamaa M, Vierola H, Luukkainen T. Tissue concentrations of LNG in women using a LNG-releasing IUD. Clinical Endocrinol 1982;17:529-536.
-
16 HOW SUPPLIED/STORAGE AND HANDLING
Mirena (levonorgestrel-releasing intrauterine system), containing a total of 52 mg LNG, is available in a carton of one sterile unit NDC# 50419-423-01.
Mirena is supplied sterile. Mirena is sterilized with ethylene oxide. Do not resterilize. For single use only. Do not use if the inner package is damaged or open. Insert before the end of the month shown on the label.
Store at 25°C (77°F); with excursions permitted between 15–30°C (59–86°F) [see USP Controlled Room Temperature].
-
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient Information)
- Sexually Transmitted Infections: Counsel the patient that this product does not protect against HIV infection (AIDS) and other sexually transmitted infections (STIs).
- Risk of Ectopic Pregnancy: Inform the patient about the risks of ectopic pregnancy, including the loss of fertility. Teach her to recognize and report to her healthcare provider promptly any symptoms of ectopic pregnancy. [See Warnings and Precautions (5.1).]
- Pregnancy or Suspected Pregnancy: Counsel the patient to inform her healthcare provider if she determines or suspects she is pregnant with Mirena in place. Advise women of the potential risks if pregnancy occurs with Mirena in place. If Mirena cannot be removed in a pregnant patient, advise her to report immediately any symptom that suggests complications of the pregnancy.
- Pelvic Infection: Inform the patient about the possibility of pelvic inflammatory disease (PID) and that PID can cause tubal damage leading to ectopic pregnancy or infertility, or infrequently can necessitate hysterectomy, or cause death. Teach the patient to recognize and report to her healthcare provider promptly any symptoms of PID. These symptoms include development of menstrual disorders (prolonged or heavy bleeding), unusual vaginal discharge, abdominal or pelvic pain or tenderness, dyspareunia, chills, and fever. [See Warnings and Precautions (5.4).]
- Irregular Bleeding and Amenorrhea: Counsel the patient that irregular or prolonged bleeding and spotting, and/or cramps may occur during the first few weeks after insertion. If her symptoms continue or are severe she should report them to her healthcare provider. [See Warnings and Precautions (5.5).]
- Perforation and Expulsion: Counsel the patient that the IUS may be expelled from or perforate the uterus and instruct her on how she can check that the threads still protrude from the cervix. Caution her not to pull on the threads and displace Mirena. Inform her that there is no contraceptive protection if Mirena is displaced or expelled. [See Warnings and Precautions (5.6, 5.7).]
- Clinical Considerations for Use and Removal: Instruct the patient to contact her healthcare provider if she experiences any of the following:
- A stroke or heart attack
- Very severe or migraine headaches
- Unexplained fever
- Yellowing of the skin or whites of the eyes, as these may be signs of serious liver problems
- Pregnancy or suspected pregnancy
- Pelvic pain or pain during sex
- HIV positive seroconversion in herself or her partner
- Possible exposure to sexually transmitted infections (STIs)
- Unusual vaginal discharge or genital sores
- Severe vaginal bleeding or bleeding that lasts a long time, or if she misses a menstrual period
- Inability to feel Mirena's threads
Complete the Follow-up Reminder Card and give to the patient.
-
PATIENT PACKAGE INSERT
FDA-Approved Patient Labeling
Patient Information
Mirena® (mur-ā-nah)
(levonorgestrel-releasing intrauterine system)
Mirena does not protect against HIV infection (AIDS) and other sexually transmitted infections (STIs).
Read this Patient Information carefully before you decide if Mirena is right for you. This information does not take the place of talking with your gynecologist or other healthcare provider who specializes in women’s health. If you have any questions about Mirena, ask your healthcare provider. You should also learn about other birth control methods to choose the one that is best for you.
What is Mirena?
- Mirena is a hormone-releasing system placed in your uterus by your healthcare provider to prevent pregnancy for up to 5 years.
- Mirena can also lessen menstrual blood loss in women who have heavy menstrual flow and who also want to use a birth control method that is placed in the uterus to prevent pregnancy.
- Mirena can be removed by your healthcare provider at any time.
- Mirena Mirena can be used whether or not you have had a child.
Mirena is a small flexible plastic T-shaped system that slowly releases a progestin hormone called levonorgestrel that is often used in birth control pills. Because Mirena releases levonorgestrel into your uterus, only small amounts of the hormone enter your blood. Mirena does not contain estrogen.
Two thin threads are attached to the stem of Mirena. The threads are the only part of Mirena you can feel when Mirena is in your uterus; however, unlike a tampon string, the threads do not extend outside your body.
What if I need birth control for more than 5 years?
Mirena must be removed after 5 years. Your healthcare provider can place a new Mirena during the same office visit if you choose to continue using Mirena.
What if I want to stop using Mirena?
Mirena is intended for long-term use but you can stop using Mirena at any time by asking your healthcare provider to remove it. You could become pregnant as soon as Mirena is removed, so you should use another method of birth control if you do not want to become pregnant.
What if I change my mind about birth control and want to become pregnant in less than 5 years?
Your healthcare provider can remove Mirena at any time. You may become pregnant as soon as Mirena is removed. About 8 out of 10 women who want to become pregnant will become pregnant sometime in the first year after Mirena is removed.
How does Mirena work?
Mirena may work in several ways including thickening cervical mucus, inhibiting sperm movement, reducing sperm survival, and thinning the lining of your uterus. It is not known exactly how these actions work together to prevent pregnancy.
Mirena can cause your menstrual bleeding to be less by thinning the lining of the uterus.
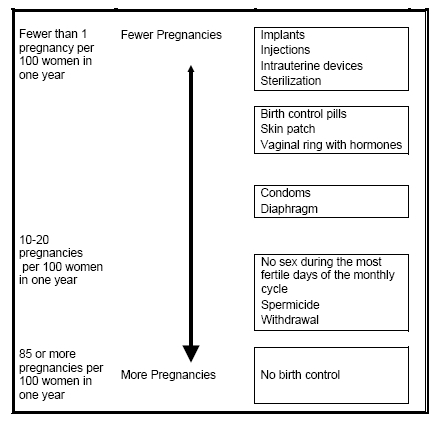
How well does Mirena work for contraception?
The following chart shows the chance of getting pregnant for women who use different methods of birth control. Each box on the chart contains a list of birth control methods that are similar in effectiveness. The most effective methods are at the top of the chart. The box on the bottom of the chart shows the chance of getting pregnant for women who do not use birth control and are trying to get pregnant.
Mirena, an intrauterine device (IUD), is in the box at the top of the chart.
How well does Mirena work for heavy menstrual bleeding?
In the clinical trial performed in women with heavy menstrual bleeding and treated with Mirena, almost 9 out of 10 were treated successfully and their blood loss was reduced by more than half.
Who might use Mirena?
You might choose Mirena if you:
- Want long-term birth control that provides a low chance of getting pregnant (less than 1 in 100)
- Want birth control that works continuously for up to 5 years
- Want birth control that is reversible
- Want a birth control method that you do not need to take daily
- Want treatment for heavy periods and are willing to use a birth control method that is placed in the uterus
- Want birth control that does not contain estrogen
Who should not use Mirena?
Do not use Mirena if you:
- Are or might be pregnant; Mirena cannot be used as an emergency contraceptive
- Have had a serious pelvic infection called pelvic inflammatory disease (PID) unless you have had a normal pregnancy after the infection went away
- Have an untreated pelvic infection now
- Have had a serious pelvic infection in the past 3 months after a pregnancy
- Can get infections easily. For example, if you have:
- Multiple sexual partners or your partner has multiple sexual partners
- Problems with your immune system
- Intravenous drug abuse.
- Have or suspect you might have cancer of the uterus or cervix
- Have bleeding from the vagina that has not been explained
- Have liver disease or liver tumor
- Have breast cancer or any other cancer that is sensitive to progestin (a female hormone), now or in the past
- Have an intrauterine device in your uterus already
- Have a condition of the uterus that changes the shape of the uterine cavity, such as large fibroid tumors
- Are allergic to levonorgestrel, silicone, polyethylene, silica, barium sulfate or iron oxide
Before having Mirena placed, tell your healthcare provider if you:
- Have had a heart attack
- Have had a stroke
- Were born with heart disease or have problems with your heart valves
- Have problems with blood clotting or take medicine to reduce clotting
- Have high blood pressure
- Recently had a baby or if you are breastfeeding
- Have severe migraine headaches.
How is Mirena placed?
Mirena is placed by your healthcare provider during an in-office visit.
First, your healthcare provider will examine your pelvis to find the exact position of your uterus. Your healthcare provider will then clean your vagina and cervix with an antiseptic solution, and slide a slim plastic tube containing Mirena into your uterus. Your healthcare provider will then remove the plastic tube, and leave Mirena in your uterus. Your healthcare provider will cut the threads to the right length. Placement takes only a few minutes.
You may experience pain, bleeding or dizziness during and after placement. If your symptoms do not pass within 30 minutes after placement, Mirena may not have been placed correctly. Your healthcare provider will examine you to see if Mirena needs to be removed or replaced.
Should I check that Mirena is in place?
Yes, you should check that Mirena is in proper position by feeling the removal threads. It is a good habit to do this once a month. Your healthcare provider should tell you how to check that Mirena is in place. First, wash your hands with soap and water. You can check by reaching up to the top of your vagina with clean fingers to feel the removal threads. Do not pull on the threads. If you feel more than just the threads or if you cannot feel the threads, Mirena may not be in the right position and may not prevent pregnancy. Use non-hormonal back-up birth control (such as condoms and spermicide) and ask your healthcare provider to check that Mirena is still in the right place.
How soon after placement of Mirena should I return to my healthcare provider?
Call your healthcare provider if you have any questions or concerns (see "When should I call my healthcare provider"). Otherwise, you should return to your healthcare provider for a follow-up visit 4 to 6 weeks after Mirena is placed to make sure that Mirena is in the right position.
Can I use tampons with Mirena?
Tampons may be used with Mirena.
What if I become pregnant while using Mirena?
Call your healthcare provider right away if you think you are pregnant. If you get pregnant while using Mirena, you may have an ectopic pregnancy. This means that the pregnancy is not in the uterus. Unusual vaginal bleeding or abdominal pain may be a sign of ectopic pregnancy.
Ectopic pregnancy is a medical emergency that often requires surgery. Ectopic pregnancy can cause internal bleeding, infertility, and even death.
There are also risks if you get pregnant while using Mirena and the pregnancy is in the uterus. Severe infection, miscarriage, premature delivery, and even death can occur with pregnancies that continue with an intrauterine device (IUD). Because of this, your healthcare provider may try to remove Mirena, even though removing it may cause a miscarriage. If Mirena cannot be removed, talk with your healthcare provider about the benefits and risks of continuing the pregnancy.
If you continue your pregnancy, see your healthcare provider regularly. Call your healthcare provider right away if you get flu-like symptoms, fever, chills, cramping, pain, bleeding, vaginal discharge, or fluid leaking from your vagina. These may be signs of infection.
It is not known if Mirena can cause long-term effects on the fetus if it stays in place during a pregnancy.
How will Mirena change my periods?
For the first 3 to 6 months, your period may become irregular and the number of bleeding days may increase. You may also have frequent spotting or light bleeding. Some women have heavy bleeding during this time. After you have used Mirena for a while, the number of bleeding and spotting days is likely to lessen. There is a small chance that your periods will stop altogether.
In some women with heavy bleeding, the total blood loss per cycle progressively decreases with continued use. The number of spotting and bleeding days may initially increase but then typically decreases in the months that follow.
Is it safe to breastfeed while using Mirena?
You may use Mirena when you are breastfeeding if more than six weeks have passed since you had your baby. If you are breastfeeding, Mirena is not likely to affect the quality or amount of your breast milk or the health of your nursing baby. However, isolated cases of decreased milk production have been reported among women using progestin-only birth control pills. The risk of Mirena becoming attached to (embedded) or going through the wall of the uterus is increased if Mirena is inserted while you are breastfeeding.
Will Mirena interfere with sexual intercourse?
You and your partner should not feel Mirena during intercourse. Mirena is placed in the uterus, not in the vagina. Sometimes your partner feels the threads. If this occurs, talk with your healthcare provider.
What are the possible side effects of using Mirena?
Mirena can cause serious side effects including:
- Pelvic inflammatory disease (PID). Some IUD users get a serious pelvic infection called pelvic inflammatory disease. PID is usually sexually transmitted. You have a higher chance of getting PID if you or your partner have sex with other partners. PID can cause serious problems such as infertility, ectopic pregnancy or pelvic pain that does not go away. PID is usually treated with antibiotics. More serious cases of PID may require surgery. A hysterectomy (removal of the uterus) is sometimes needed. In rare cases, infections that start as PID can even cause death.
- Tell your healthcare provider right away if you have any of these signs of PID: long-lasting or heavy bleeding, unusual vaginal discharge, low abdominal (stomach area) pain, painful sex, chills, or fever.
- Life-threatening infection. Life-threatening infection can occur within the first few days after Mirena is placed. Call your healthcare provider immediately if you develop severe pain or fever shortly after Mirena is placed.
- Perforation. Mirena may become attached to (embedded) or go through the wall of the uterus. This is called perforation. If this occurs, Mirena may no longer prevent pregnancy. If perforation occurs, Mirena may move outside the uterus and can cause internal scarring, infection, or damage to other organs, and you may need surgery to have Mirena removed. The risk of perforation is increased if Mirena is inserted while you are breastfeeding.
Common side effects of Mirena include:
- Pain, bleeding or dizziness during and after placement. If these symptoms do not stop 30 minutes after placement, Mirena may not have been placed correctly. Your healthcare provider will examine you to see if Mirena needs to be removed or replaced.
- Expulsion. Mirena may come out by itself. This is called expulsion. You may become pregnant if Mirena comes out. If you think that Mirena has come out, use a backup birth control method like condoms and spermicide and call your healthcare provider.
- Missed menstrual periods. About 2 out of 10 women stop having periods after 1 year of Mirena use. If you do not have a period for 6 weeks during Mirena use, call your healthcare provider. When Mirena is removed, your menstrual periods will come back.
- Changes in bleeding. You may have bleeding and spotting between menstrual periods, especially during the first 3 to 6 months. Sometimes the bleeding is heavier than usual at first. However, the bleeding usually becomes lighter than usual and may be irregular. Call your healthcare provider if the bleeding remains heavier than usual or increases after it has been light for a while.
- Cysts on the ovary. About 12 out of 100 women using Mirena develop a cyst on the ovary. These cysts usually disappear on their own in a month or two. However, cysts can cause pain and sometimes cysts will need surgery.
This is not a complete list of possible side effects with Mirena. For more information, ask your healthcare provider.
Call your doctor for medical advice about side effects. You may report side effects to the manufacturer at 1-888-842-2937, or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
After Mirena has been placed, when should I call my healthcare provider?
Call your healthcare provider if you have any concerns about Mirena. Be sure to call if you:
- Think you are pregnant
- Have pelvic pain or pain during sex
- Have unusual vaginal discharge or genital sores
- Have unexplained fever, flu-like symptoms or chills
- Might be exposed to sexually transmitted infections (STIs)
- Cannot feel Mirena's threads
- Develop very severe or migraine headaches
- Have yellowing of the skin or whites of the eyes. These may be signs of liver problems.
- Have had a stroke or heart attack
- Or your partner becomes HIV positive
- Have severe vaginal bleeding or bleeding that lasts a long time
General advice about prescription medicines
Medicines are sometimes prescribed for conditions that are not mentioned in patient information leaflets. This leaflet summarizes the most important information about Mirena. If you would like more information, talk with your healthcare provider. You can ask your healthcare provider for information about Mirena that is written for health providers.
For more information, go to www.mirena-us.com or call 1-888-842-2937
This Patient Information has been approved by the U.S. Food and Drug Administration.
This patient information booklet was updated June 2017.
Manufactured for:
Bayer HealthCare Pharmaceuticals Inc.
Whippany, NJ 07981Manufactured in Finland
© 2000, Bayer HealthCare Pharmaceuticals Inc.
All rights reserved. -
PRINCIPAL DISPLAY PANEL
Mirena (levonorgestrel-releasing intrauterine system) Carton
NDC: 50419-423-01
1 Sterile Unit
NEW contains updated single-handed inserter with no removable threads
IMPORTANT: To be inserted in the uterus by a trained healthcare provider. Mirena cannot be reloaded.. See physician insert for detailed instructions for use.
Mirena
(levonorgestrel-releasing intrauterine system)
Rx only
— 52 mg levonorgestrel
— 1 sterile unit
— intrauterine use
-
INGREDIENTS AND APPEARANCE
MIRENA
levonorgestrel intrauterine deviceProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 50419-423 Route of Administration INTRAUTERINE Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength LEVONORGESTREL (UNII: 5W7SIA7YZW) (LEVONORGESTREL - UNII:5W7SIA7YZW) LEVONORGESTREL 52 mg Inactive Ingredients Ingredient Name Strength DIMETHICONE (UNII: 92RU3N3Y1O) BARIUM SULFATE (UNII: 25BB7EKE2E) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 50419-423-01 1 in 1 CARTON; Type 4: Device Coated/Impregnated/Otherwise Combined with Drug 05/30/2014 2 NDC: 50419-423-08 1 in 1 CARTON; Type 4: Device Coated/Impregnated/Otherwise Combined with Drug 12/08/2016 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA021225 10/01/2009 Labeler - Bayer HealthCare Pharmaceuticals Inc. (005436809) Establishment Name Address ID/FEI Business Operations Bayer Schering Pharma Oy 369758383 MANUFACTURE(50419-423)

Trademark Results [Mirena]
Mark Image Registration | Serial | Company Trademark Application Date |
|---|---|
 MIRENA 97139728 not registered Live/Pending |
Mirena LLC 2021-11-23 |
 MIRENA 74718798 2039913 Live/Registered |
BAYER OY 1995-08-22 |
 MIRENA 74227376 not registered Dead/Abandoned |
Huhtamaki Oy 1991-12-05 |
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.