XOFLUZA- baloxavir marboxil tablet, film coated
Xofluza by
Drug Labeling and Warnings
Xofluza by is a Prescription medication manufactured, distributed, or labeled by Genentech, Inc., F. Hoffmann-La Roche Ltd, F. Hoffmann-La Roche AG. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use XOFLUZA safely and effectively. See full prescribing information for XOFLUZA.
XOFLUZA® (baloxavir marboxil) tablets, for oral use
Initial U.S. Approval: 2018RECENT MAJOR CHANGES
INDICATIONS AND USAGE
XOFLUZA® is a polymerase acidic (PA) endonuclease inhibitor indicated for the treatment of acute uncomplicated influenza in patients 12 years of age and older who have been symptomatic for no more than 48 hours and who are:
- otherwise healthy, or
- at high risk of developing influenza-related complications1. (1)
Limitations of Use: Influenza viruses change over time, and factors such as the virus type or subtype, emergence of resistance, or changes in viral virulence could diminish the clinical benefit of antiviral drugs. Consider available information on drug susceptibility patterns for circulating influenza virus strains when deciding whether to use XOFLUZA. (1)
DOSAGE AND ADMINISTRATION
Take a single dose of XOFLUZA orally within 48 hours of symptom onset with or without food. Avoid co-administration of XOFLUZA with dairy products, calcium-fortified beverages, polyvalent cation-containing laxatives, antacids, or oral supplements (e.g., calcium, iron, magnesium, selenium, or zinc). The dose of XOFLUZA depends on weight. (2)
Patient Body Weight (kg) Recommended Single Oral Dose 40 to less than 80 Two 20 mg tablets taken at the same time for a total single dose of 40 mg
(blister card contains two 20 mg tablets)At least 80 Two 40 mg tablets taken at the same time for a total single dose of 80 mg
(blister card contains two 40 mg tablets)DOSAGE FORMS AND STRENGTHS
Tablets: 20 mg and 40 mg (3)
CONTRAINDICATIONS
XOFLUZA is contraindicated in patients with a history of hypersensitivity to baloxavir marboxil or any of its ingredients. (4)
WARNINGS AND PRECAUTIONS
Hypersensitivity such as anaphylaxis, angioedema, urticaria, and erythema multiforme: Initiate appropriate treatment if an allergic-like reaction occurs or is suspected. (5.1)
Risk of Bacterial Infection: Serious bacterial infections may begin with influenza-like symptoms, may coexist with, or occur as a complication of influenza. XOFLUZA has not been shown to prevent such complications. Prescribers should be alert to potential secondary bacterial infections and treat them as appropriate. (5.2)
ADVERSE REACTIONS
Adverse events reported in at least 1% of adult and adolescent subjects treated with XOFLUZA included diarrhea (3%), bronchitis (3%), nausea (2%), sinusitis (2%) and headache (1%). (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Genentech at 1-888-835-2555 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
USE IN SPECIFIC POPULATIONS
- Safety and efficacy in patients less than 12 years of age or weighing less than 40 kg have not been established. (8.4)
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.
Revised: 10/2019
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Hypersensitivity
5.2 Risk of Bacterial Infections
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
6.2 Postmarketing Experience
7 DRUG INTERACTIONS
7.1 Effect of Other Drugs on XOFLUZA
7.2 Vaccines
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.4 Pediatric Use
8.5 Geriatric Use
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
12.4 Microbiology
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
14.1 Treatment of Acute Uncomplicated Influenza – Otherwise Healthy Patients
14.2 Treatment of Acute Uncomplicated Influenza – High Risk Patients
15 REFERENCES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- * Sections or subsections omitted from the full prescribing information are not listed.
-
1 INDICATIONS AND USAGE
XOFLUZA® is indicated for the treatment of acute uncomplicated influenza in patients 12 years of age and older who have been symptomatic for no more than 48 hours and who are:
- otherwise healthy, or
- at high risk of developing influenza-related complications1 [see Clinical Studies (14.2)].
Limitations of Use:
Influenza viruses change over time, and factors such as the virus type or subtype, emergence of resistance, or changes in viral virulence could diminish the clinical benefit of antiviral drugs. Consider available information on drug susceptibility patterns for circulating influenza virus strains when deciding whether to use XOFLUZA [see Microbiology (12.4) and Clinical Studies (14)].
-
2 DOSAGE AND ADMINISTRATION
Initiate treatment with XOFLUZA within 48 hours of influenza symptom onset. XOFLUZA is taken orally as a single dose and may be taken with or without food. However, co-administration of XOFLUZA with dairy products, calcium-fortified beverages, polyvalent cation-containing laxatives, antacids or oral supplements (e.g., calcium, iron, magnesium, selenium, or zinc) should be avoided [see Drug Interactions (7.1), Clinical Pharmacology (12.3)].
Adults and Adolescents (12 years of age and older)
The recommended dose of XOFLUZA in patients 12 years of age or older is a single weight-based dose as follows:
Table 1 Recommended XOFLUZA Dosage in Adults and Adolescents 12 Years and Older Patient Body Weight (kg) Recommended Single Oral Dose 40 kg to less than 80 kg Two 20 mg tablets taken at the same time for a total single dose of 40 mg
(blister card contains two 20 mg tablets)At least 80 kg Two 40 mg tablets taken at the same time for a total single dose of 80 mg
(blister card contains two 40 mg tablets) - 3 DOSAGE FORMS AND STRENGTHS
-
4 CONTRAINDICATIONS
XOFLUZA is contraindicated in patients with a history of hypersensitivity to baloxavir marboxil or any of its ingredients. Serious allergic reactions have included anaphylaxis, angioedema, urticaria and erythema multiforme [see Warnings and Precautions (5.1)].
-
5 WARNINGS AND PRECAUTIONS
5.1 Hypersensitivity
Cases of anaphylaxis, urticaria, angioedema, and erythema multiforme have been reported in post-marketing experience with XOFLUZA. Appropriate treatment should be instituted if an allergic-like reaction occurs or is suspected. The use of XOFLUZA is contraindicated in patients with known hypersensitivity to XOFLUZA [see Contraindications (4) and Adverse Reactions (6.2)].
5.2 Risk of Bacterial Infections
There is no evidence of efficacy of XOFLUZA in any illness caused by pathogens other than influenza viruses. Serious bacterial infections may begin with influenza-like symptoms, may coexist with, or occur as a complication of influenza. XOFLUZA has not been shown to prevent such complications. Prescribers should be alert to potential secondary bacterial infections and treat them as appropriate.
-
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The safety profile of XOFLUZA is based on data from 3 placebo-controlled trials in which a total of 1,640 subjects received XOFLUZA: 1,334 subjects (81%) were 18 to 64 years of age, 209 subjects (13%) were adults 65 years of age or older and 97 subjects (6%) were adolescents 12 to 17 years of age. These trials included otherwise healthy adults and adolescents (N=910) and subjects at high risk of developing complications associated with influenza (N=730). Of these, 1,440 subjects received XOFLUZA at the recommended dose [see Clinical Studies (14)].
Table 2 displays the most common adverse events (regardless of causality assessment) reported in at least 1% of adult and adolescent subjects who received XOFLUZA at the recommended dose in Trials 1, 2 and 3.
Table 2 Incidence of Adverse Events Occurring in At Least 1% of Subjects Receiving XOFLUZA in the Acute Uncomplicated Influenza Trials 1, 2, and 3 Adverse Event XOFLUZA
(N = 1,440)Placebo
(N = 1,136)Diarrhea 3% 4% Bronchitis 3% 4% Nausea 2% 3% Sinusitis 2% 3% Headache 1% 1% 6.2 Postmarketing Experience
The following adverse reactions have been identified during postmarketing use of XOFLUZA. Because these reactions are reported voluntarily from a population of uncertain size, it is not possible to reliably estimate their frequency or establish a causal relationship to XOFLUZA exposure.
Body as a Whole: Swelling of the face, eyelids or tongue, dysphonia, angioedema, anaphylactic reactions, anaphylactic shock, anaphylactoid reactions
Skin and Subcutaneous Tissue Disorders: Rash, urticaria, erythema multiforme
Gastrointestinal disorders: Vomiting, bloody diarrhea, melena, colitis
Psychiatric: Delirium, abnormal behavior, and hallucinations
-
7 DRUG INTERACTIONS
7.1 Effect of Other Drugs on XOFLUZA
Co-administration with polyvalent cation-containing products may decrease plasma concentrations of baloxavir which may reduce XOFLUZA efficacy. Avoid co-administration of XOFLUZA with polyvalent cation-containing laxatives, antacids, or oral supplements (e.g., calcium, iron, magnesium, selenium, or zinc).
7.2 Vaccines
The concurrent use of XOFLUZA with intranasal live attenuated influenza vaccine (LAIV) has not been evaluated. Concurrent administration of antiviral drugs may inhibit viral replication of LAIV and thereby decrease the effectiveness of LAIV vaccination. Interactions between inactivated influenza vaccines and XOFLUZA have not been evaluated.
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
There are no available data on XOFLUZA use in pregnant women to inform a drug-associated risk of adverse developmental outcomes. There are risks to the mother and fetus associated with influenza virus infection in pregnancy (see Clinical Considerations). In animal reproduction studies, no adverse developmental effects were observed in rats or rabbits with oral administration of baloxavir marboxil at exposures approximately 5 (rats) and 7 (rabbits) times the systemic baloxavir exposure at the maximum recommended human dose (MRHD) (see Data).
The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defects, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2-4% and 15-20%, respectively.
Disease-associated maternal and/or embryo/fetal risk
Pregnant women are at higher risk of severe complications from influenza, which may lead to adverse pregnancy and/or fetal outcomes including maternal death, stillbirth, birth defects, preterm delivery, low birth weight and small for gestational age.
Data
Animal Data
Baloxavir marboxil was administered orally to pregnant rats (20, 200, or 1,000 mg/kg/day from gestation day 6 to 17) and rabbits (30, 100, or 1,000 mg/kg/day from gestation day 7 to 19). No adverse embryo-fetal effects were observed in rats up to the highest dose of baloxavir marboxil (1,000 mg/kg/day), resulting in systemic baloxavir exposure (AUC) of approximately 5 times the exposure at the MRHD. In rabbits, fetal skeletal variations occurred at a maternally toxic dose (1,000 mg/kg/day) resulting in 2 abortions out of 19 pregnancies. No adverse maternal or embryo-fetal effects were observed in rabbits at the middle dose (100 mg/kg/day) resulting in systemic baloxavir exposure (AUC) approximately 7 times the exposure at the MRHD.
In the prenatal and postnatal development study in rats, baloxavir marboxil was administered orally at 20, 200, or 1,000 mg/kg/day from gestation day 6 to postpartum/lactation day 20. No significant effects were observed in the offspring at maternal systemic baloxavir exposure (AUC) approximately 5 times the exposure at the MRHD.
8.2 Lactation
Risk Summary
There are no data on the presence of baloxavir marboxil in human milk, the effects on the breastfed infant, or the effects on milk production. Baloxavir and its related metabolites were present in the milk of lactating rats (see Data). The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for XOFLUZA and any potential adverse effects on the breastfed child from the drug or from the underlying maternal condition.
Data
In a lactation study, baloxavir and its related metabolites were excreted in the milk of lactating rats administered baloxavir marboxil (1 mg/kg) on postpartum/lactation day 11, with peak milk concentration approximately 5 times that of maternal plasma concentrations occurring 2 hours post-dose. No effects of baloxavir marboxil on growth and postnatal development were observed in nursing pups at the highest oral dose tested in rats. Maternal systemic exposure was approximately 5 times the baloxavir exposure in humans at the MRHD.
8.4 Pediatric Use
The safety and effectiveness of XOFLUZA for the treatment of acute uncomplicated influenza have been established in pediatric patients 12 years of age and older weighing at least 40 kg [see Adverse Reactions (6.1) and Clinical Studies (14)]. The safety and effectiveness of XOFLUZA have not been established in pediatric patients less than 12 years of age.
Treatment of Acute Uncomplicated Influenza in Otherwise Healthy Pediatric Patients
The safety and effectiveness of XOFLUZA in otherwise healthy pediatric patients 12 years of age and older weighing at least 40 kg is supported by one randomized, double-blind, controlled trial (Trial 2) [see Clinical Studies (14.1)]. In this phase 3 trial, 117 adolescents 12-17 years old were randomized and received either XOFLUZA (N=76) or placebo (N=41). The median time to alleviation of symptoms in influenza-infected adolescent subjects aged 12 to 17 years was 54 hours and 93 hours for subjects who received XOFLUZA (N=63) or placebo (N=27), respectively, and was comparable to that observed in the overall trial population [see Clinical Studies (14.1)]. Adverse events reported in adolescents were similar to those reported in adults [see Adverse Reactions (6.1)].
Treatment of Acute Uncomplicated Influenza in Pediatric Patients at High Risk for Influenza Complications
The safety and effectiveness of XOFLUZA in pediatric patients 12 years of age and older weighing at least 40 kg who are at high risk of developing influenza-related complications is supported by extrapolation from a clinical trial in otherwise healthy adults and adolescents with acute uncomplicated influenza (Trial 2), and from one randomized, double-blind, phase 3 controlled trial in patients at high risk for influenza complications (Trial 3) in which 38 adolescents aged 12 to 17 years were randomized and received either XOFLUZA (N=21) or placebo (N=17). The median time to improvement of influenza symptoms in the limited number of adolescent subjects aged 12 to 17 years who were infected with influenza was similar for subjects who received XOFLUZA (188 hours) or placebo (191 hours) (N=13 and N=12, respectively) [see Clinical Studies (14.2)]. Adverse events reported in adolescents were similar to those reported in adults [see Adverse Reactions (6.1)].
8.5 Geriatric Use
The safety and effectiveness of XOFLUZA in subjects 65 years of age and older has been established and is supported by one randomized, double-blind, controlled trial [see Clinical Studies (14.2)]. In Trial 3, of 730 XOFLUZA-treated subjects at high risk of influenza-related complications, 209 (29%) subjects were 65 years of age and older. The median time to improvement of influenza symptoms in subjects 65 years of age and older was 70 hours in subjects who received XOFLUZA (N=112) and 88 hours in those who received placebo (N=102). The safety profile observed for this population was similar to that reported in the overall trial population except for nausea, which was reported in 6% of elderly subjects compared to 1% of subjects from 18 to 64 years of age.
-
10 OVERDOSAGE
Treatment of an overdose of XOFLUZA should consist of general supportive measures including monitoring of vital signs and observation of the clinical status of the patient. There is no specific antidote for overdose with XOFLUZA.
Baloxavir is unlikely to be significantly removed by dialysis due to high serum protein binding [see Clinical Pharmacology (12.3)].
-
11 DESCRIPTION
XOFLUZA (baloxavir marboxil) is an antiviral PA endonuclease inhibitor. XOFLUZA is supplied as white to light yellow film-coated tablets for oral administration.
The active component of XOFLUZA is baloxavir marboxil. Baloxavir marboxil has a molecular weight of 571.55 and a partition coefficient (log P) of 2.26. It is freely soluble in dimethylsulfoxide, soluble in acetonitrile, slightly soluble in methanol and ethanol and practically insoluble in water.
The chemical name of baloxavir marboxil is ({(12aR)-12-[(11S)-7,8-Difluoro-6,11-dihydrodibenzo[b,e]thiepin-11-yl]-6,8-dioxo-3,4,6,8,12,12a-hexahydro-1H-[1,4]oxazino[3,4-c]pyrido[2,1-f][1,2,4]triazin-7-yl}oxy)methyl methyl carbonate. The empirical formula of baloxavir marboxil is C27H23F2N3O7S and the chemical structure is shown below.
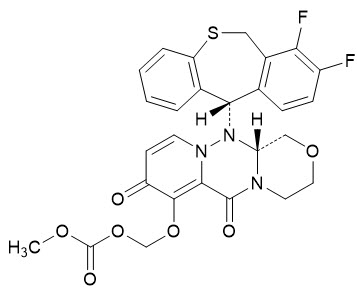
The inactive ingredients of XOFLUZA are: croscarmellose sodium, hypromellose, lactose monohydrate, microcrystalline cellulose, povidone, sodium stearyl fumarate, talc, and titanium dioxide.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Baloxavir marboxil is an antiviral drug with activity against influenza virus [see Microbiology (12.4)].
12.2 Pharmacodynamics
Cardiac Electrophysiology
At twice the expected exposure from recommended dosing, XOFLUZA did not prolong the QTc interval.
Exposure-Response Relationships
When XOFLUZA is dosed by weight, as recommended (40 mg in patients weighing 40-80 kg; and 80 mg in patients weighing at least 80 kg), no difference in baloxavir exposure-response (time to alleviation of influenza symptoms in the Otherwise Healthy population or time to improvement of influenza symptoms in the High Risk population) relationship has been observed.
12.3 Pharmacokinetics
Baloxavir marboxil is a prodrug that is almost completely converted to its active metabolite, baloxavir, following oral administration.
In Trial 2, at the recommended dose of 40 mg for subjects weighing less than 80 kg, the mean (CV%) values of baloxavir Cmax and AUC0-inf were 96.4 ng/mL (45.9%) and 6160 ng∙hr/mL (39.2%), respectively. At the recommended dose of 80 mg for subjects weighing 80 kg and more, the mean (CV%) values of baloxavir Cmax and AUC0-inf were 107 ng/mL (47.2%) and 8009 ng∙hr/mL (42.4%), respectively. Refer to Table 3 for pharmacokinetic parameters of baloxavir in healthy subjects. The pharmacokinetic profile of XOFLUZA was similar for adults and adolescents who were otherwise healthy and those at high risk of developing influenza-related complications.
Table 3 Pharmacokinetic Parameters of Plasma Baloxavir - * Median
- † Meal: approximately 400 to 500 kcal including 150 kcal from fat
- ‡ in vitro
- § Geometric mean (geometric CV%)
- ¶ Apparent terminal elimination half-life
- # Baloxavir is primarily metabolized by UGT1A3 with minor contribution from CYP3A4
- Þ Ratio of radioactivity to radio-labeled [14C]-baloxavir marboxil dose in mass balance study
Absorption Tmax (hr)* 4 Effect of food (relative to fasting)† Cmax: ↓48%, AUC0-inf: ↓36% Distribution % Bound to human serum proteins‡ 92.9 - 93.9 Ratio of blood cell to blood 48.5% - 54.4% Volume of distribution (V/F, L)§ 1180 (20.8%) Elimination Major route of elimination Metabolism Clearance (CL/F, L/hr)§ 10.3 (22.5%) t1/2 (hr) §, ¶ 79.1 (22.4%) Metabolism Metabolic pathways# UGT1A3, CYP3A4 Excretion % of dose excreted in urineÞ 14.7 (Total radioactivity), 3.3 (Baloxavir) % of dose excreted in fecesÞ 80.1 (Total radioactivity) Specific Populations
There were no clinically significant differences in the pharmacokinetics of baloxavir based on age (adolescents as compared to adults), or sex.
Patients with Renal Impairment
A population pharmacokinetic analysis did not identify a clinically meaningful effect of renal function on the pharmacokinetics of baloxavir in patients with creatinine clearance (CrCl) 50 mL/min and above. The effects of severe renal impairment on the pharmacokinetics of baloxavir marboxil or its active metabolite, baloxavir, have not been evaluated.
Patients with Hepatic Impairment
In a clinical study comparing pharmacokinetics of baloxavir in subjects with moderate hepatic impairment (Child-Pugh class B) to subjects with normal hepatic function, no clinically meaningful differences in the pharmacokinetics of baloxavir were observed.
The pharmacokinetics in patients with severe hepatic impairment have not been evaluated.
Drug Interaction Studies
Clinical Studies
No clinically significant changes in the pharmacokinetics of baloxavir marboxil and its active metabolite, baloxavir, were observed when co-administered with itraconazole (combined strong CYP3A and P-gp inhibitor), probenecid (UGT inhibitor), or oseltamivir.
No clinically significant changes in the pharmacokinetics of the following drugs were observed when co-administered with baloxavir marboxil: midazolam (CYP3A4 substrate), digoxin (P-gp substrate), rosuvastatin (BCRP substrate), or oseltamivir.
In Vitro Studies Where Drug Interaction Potential Was Not Further Evaluated Clinically
Cytochrome P450 (CYP) Enzymes: Baloxavir marboxil and its active metabolite, baloxavir, did not inhibit CYP1A2, CYP2B6, CYP2C8, CYP2C9, CYP2C19, or CYP2D6. Baloxavir marboxil and its active metabolite, baloxavir, did not induce CYP1A2, CYP2B6, or CYP3A4.
Uridine diphosphate (UDP)-glucuronosyl transferase (UGT) Enzymes: Baloxavir marboxil and its active metabolite, baloxavir, did not inhibit UGT1A1, UGT1A3, UGT1A4, UGT1A6, UGT1A9, UGT2B7, or UGT2B15.
Transporter Systems: Both baloxavir marboxil and baloxavir are substrates of P-glycoprotein (P-gp). Baloxavir did not inhibit organic anion transporting polypeptides (OATP) 1B1, OATP1B3, organic cation transporter (OCT) 1, OCT2, organic anion transporter (OAT) 1, OAT3, multidrug and toxin extrusion (MATE) 1, or MATE2K.
Potential for Interactions with Polyvalent Cations: Baloxavir may form a chelate with polyvalent cations such as calcium, aluminum, or magnesium in food or medications. A significant decrease in baloxavir exposure was observed when XOFLUZA was co-administered with calcium, aluminum, magnesium, or iron in monkeys. No study has been conducted in humans.
12.4 Microbiology
Mechanism of Action
Baloxavir marboxil is a prodrug that is converted by hydrolysis to baloxavir, the active form that exerts anti-influenza virus activity. Baloxavir inhibits the endonuclease activity of the polymerase acidic (PA) protein, an influenza virus-specific enzyme in the viral RNA polymerase complex required for viral gene transcription, resulting in inhibition of influenza virus replication. The 50% inhibitory concentration (IC50) values of baloxavir ranged from 1.4 to 3.1 nM (n=4) for influenza A viruses and 4.5 to 8.9 nM (n=3) for influenza B viruses in a PA endonuclease assay. Viruses with reduced susceptibility to baloxavir have amino acid substitutions in the PA protein.
Antiviral Activity
The antiviral activity of baloxavir against laboratory strains and clinical isolates of influenza A and B viruses was determined in an MDCK cell-based plaque reduction assay. The median 50% effective concentration (EC50) values of baloxavir were 0.73 nM (n=31; range: 0.20-1.85 nM) for subtype A/H1N1 strains, 0.83 nM (n=33; range: 0.35-2.63 nM) for subtype A/H3N2 strains, and 5.97 nM (n=30; range: 2.67-14.23 nM) for type B strains. In an MDCK cell-based virus titer reduction assay, the 90% effective concentration (EC90) values of baloxavir against avian subtypes A/H5N1 and A/H7N9 were in the range of 0.80 to 3.16 nM. The relationship between antiviral activity in cell culture and clinical response to treatment in humans has not been established.
Resistance
Cell culture: Influenza A virus isolates with reduced susceptibility to baloxavir were selected by serial passage of virus in cell culture in the presence of increasing concentrations of baloxavir. Reduced susceptibility of influenza A virus to baloxavir was conferred by amino acid substitutions I38T (A/H1N1 and A/H3N2) and E199G (A/H3N2) in the PA protein of the viral RNA polymerase complex.
Clinical studies: Influenza A and B viruses with treatment-emergent amino acid substitutions at positions associated with reduced susceptibility to baloxavir in cell culture were observed in clinical studies (Table 4). The overall frequencies of treatment-emergent amino acid substitutions associated with reduced susceptibility to baloxavir in Trials 1, 2, and 3 [see Clinical Studies (14)] were 2.7% (5/182), 11% (39/370), and 5.5% (16/290), respectively.
Table 4 Treatment-Emergent Amino Acid Substitutions in PA Associated with Reduced Susceptibility to Baloxavir Influenza Type/Subtype A/H1N1 A/H3N2 B Amino Acid Substitution E23K/R, I38F/N/T E23G/K, A37T, I38M/T, E199G I38T None of the treatment-emergent substitutions associated with reduced susceptibility to baloxavir were identified in virus from pre-treatment respiratory specimens in the clinical studies. Strains containing substitutions known to be associated with reduced susceptibility to baloxavir were identified in approximately 0.05% of PA sequences in the National Center for Biotechnology Information/GenBank database (queried August 2018).
Prescribers should consider currently available surveillance information on influenza virus drug susceptibility patterns and treatment effects when deciding whether to use XOFLUZA.
Cross-Resistance
Cross-resistance between baloxavir and neuraminidase (NA) inhibitors, or between baloxavir and M2 proton pump inhibitors (adamantanes), is not expected, because these drugs target different viral proteins. Baloxavir is active against NA inhibitor-resistant strains, including A/H1N1 and A/H5N1 viruses with the NA substitution H275Y (A/H1N1 numbering), A/H3N2 virus with the NA substitutions E119V and R292K, A/H7N9 virus with the NA substitution R292K (A/H3N2 numbering), and type B virus with the NA substitutions R152K and D198E (A/H3N2 numbering). The NA inhibitor oseltamivir is active against viruses with reduced susceptibility to baloxavir, including A/H1N1 virus with PA substitutions E23K or I38F/T, A/H3N2 virus with PA substitutions E23G/K, A37T, I38M/T, or E199G, and type B virus with the PA substitution I38T. Influenza virus may carry amino acid substitutions in PA that reduce susceptibility to baloxavir and at the same time carry resistance-associated substitutions for NA inhibitors and M2 proton pump inhibitors. The clinical relevance of phenotypic cross-resistance evaluations has not been established.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Mutagenesis
Baloxavir marboxil and the active metabolite, baloxavir, were not mutagenic in in vitro and in in vivo genotoxicity assays which included bacterial mutation assays in S. typhimurium and E. coli, micronucleus tests with cultured mammalian cells, and in the rodent micronucleus assay.
Impairment of Fertility
In a fertility and early embryonic development study in rats, doses of baloxavir marboxil at 20, 200, or 1,000 mg/kg/day were administered to females for 2 weeks before mating, during mating and until day 7 of pregnancy. Males were dosed for 4 weeks before mating and throughout mating. There were no effects on fertility, mating performance, or early embryonic development at any dose level, resulting in systemic drug exposure (AUC) approximately 5 times the MRHD.
-
14 CLINICAL STUDIES
14.1 Treatment of Acute Uncomplicated Influenza – Otherwise Healthy Patients
Two randomized controlled double-blinded clinical trials conducted in two different influenza seasons evaluated efficacy and safety of XOFLUZA in otherwise healthy subjects with acute uncomplicated influenza.
In Trial 1, a placebo-controlled phase 2 dose-finding trial, a single oral dose of XOFLUZA was compared with placebo in 400 adult subjects 20 to 64 years of age in Japan. All subjects in Trial 1 were Asian, the majority of subjects were male (62%), and the mean age was 38 years. In this trial, among subjects who received XOFLUZA and had influenza virus typed, influenza A/H1N1 was the predominant strain (63%), followed by influenza B (25%), and influenza A/H3N2 (12%).
In Trial 2 (NCT02954354), a phase 3 active- and placebo-controlled trial, XOFLUZA was studied in 1,436 adults and adolescents with signs and symptoms of influenza in the U.S. and Japan. Subjects were 12 to 64 years of age and weighed at least 40 kg. Adults ages 20 to 64 years received weight-based XOFLUZA (subjects who weighed 40 to less than 80 kg received 40 mg and subjects who weighed 80 kg and above received 80 mg) or placebo as a single oral dose on Day 1 or oseltamivir twice a day for 5 days. Subjects in the XOFLUZA and placebo arms received a placebo for the duration of oseltamivir dosing after XOFLUZA or placebo dosing in that arm. Adolescent subjects 12 to less than 20 years of age received weight-based XOFLUZA or placebo as a single oral dose.
Seventy-eight percent of subjects in Trial 2 were Asian, 17% were White, and 4% were Black or African American. The mean age was 34 years, and 11% of subjects were less than 20 years of age; 54% of subjects were male and 46% female. In Trial 2, 1,062 of 1,436 enrolled subjects had influenza confirmed by RT-PCR and were included in the efficacy analysis (XOFLUZA N=455, placebo N=230, or oseltamivir N=377). Among subjects who received XOFLUZA and had influenza virus typed, influenza A/H3N2 was the predominant strain (90%), followed by influenza B (9%), and influenza A/H1N1 (2%).
In both Trials 1 and 2, eligible subjects had an axillary temperature of at least 38°C, at least one moderate or severe respiratory symptom (cough, nasal congestion, or sore throat), and at least one moderate or severe systemic symptom (headache, feverishness or chills, muscle or joint pain, or fatigue) and all were treated within 48 hours of symptom onset. Subjects participating in the trial were required to self-assess their influenza symptoms as "none", "mild", "moderate" or "severe" twice daily. The primary efficacy population was defined as those with a positive rapid influenza diagnostic test (Trial 1) or positive influenza RT-PCR (Trial 2) at trial entry.
The primary endpoint of both trials, time to alleviation of symptoms, was defined as the time when all seven symptoms (cough, sore throat, nasal congestion, headache, feverishness, myalgia, and fatigue) had been assessed by the subject as none or mild for a duration of at least 21.5 hours.
In both trials, XOFLUZA treatment at the recommended dose resulted in a statistically significant shorter time to alleviation of symptoms compared with placebo in the primary efficacy population (Tables 5 and 6).
Table 5 Time to Alleviation of Symptoms after Single Dose in Otherwise Healthy Adults with Acute Uncomplicated Influenza in Trial 1 (Median Hours) XOFLUZA 40 mg
(95% CI*)
N = 100Placebo
(95% CI*)
N = 100- * CI: Confidence interval
- † XOFLUZA treatment resulted in a statistically significant shorter time to alleviation of symptoms compared to placebo using the Gehan-Breslow's generalized Wilcoxon test (p-value: 0.014, adjusted for multiplicity using the Bonferroni method). The primary analysis using the Cox Proportional Hazards Model did not reach statistical significance (p-value: 0.165).
Adults (20 to 64 Years of Age) 50 hours†
(45, 64)78 hours
(68, 89)Table 6 Time to Alleviation of Symptoms after Single Dose in Otherwise Healthy Subjects 12 Years of Age and Older with Acute Uncomplicated Influenza in Trial 2 (Median Hours) XOFLUZA 40 mg or 80 mg
(95% CI*)
N = 455Placebo
(95% CI*)
N = 230- * CI: Confidence interval
- † XOFLUZA treatment resulted in a statistically significant shorter time to alleviation of symptoms compared to placebo using the Peto-Prentice's generalized Wilcoxon test (p-value: <0.001).
Subjects (≥ 12 Years of Age) 54 hours†
(50, 59)80 hours
(73, 87)In Trial 2, there was no difference in the time to alleviation of symptoms between subjects (age ≥ 20) who received XOFLUZA (54 hours) and those who received oseltamivir (54 hours). For adolescent subjects (12 to 17 years of age) in Trial 2, the median time to alleviation of symptoms for subjects infected with influenza and who received XOFLUZA (N=63) was 54 hours (95% CI of 43, 81) compared to 93 hours (95% CI of 64, 118) in the placebo arm (N=27).
The number of subjects who received XOFLUZA at the recommended dose and who were infected with influenza type B virus was limited, including 24 subjects in Trial 1 and 38 subjects in Trial 2. In the influenza B subset in Trial 1, the median time to alleviation of symptoms in subjects who received 40 mg XOFLUZA was 63 hours (95% CI of 43, 70) compared to 83 hours (95% CI of 58, 93) in subjects who received placebo. In the influenza B subset in Trial 2, the median time to alleviation of symptoms in subjects who received 40 mg or 80 mg XOFLUZA was 93 hours (95% CI of 53, 135) compared to 77 hours (95% CI of 47, 189) in subjects who received placebo.
14.2 Treatment of Acute Uncomplicated Influenza – High Risk Patients
Trial 3 (NCT02949011) was a randomized, double-blind, placebo- and active-controlled trial to evaluate the efficacy and safety of a single oral dose of XOFLUZA compared with placebo or oseltamivir, in adult and adolescent subjects 12 years of age or older with influenza who were at high risk of developing influenza-related complications.
A total of 2,182 subjects with signs and symptoms of influenza were randomized to receive a single oral dose of 40 mg or 80 mg of XOFLUZA according to body weight (subjects who weighed 40 to less than 80 kg received 40 mg and subjects who weighed 80 kg and above received 80 mg) (N=729), oseltamivir 75 mg twice daily for 5 days (N=725), or placebo (N=728). Twenty-eight percent of subjects were Asian, 59% were White, and 10% were Black or African American. The mean age was 52 years, and 3% of subjects were less than 18 years of age; 43% of subjects were male and 57% female.
High risk factors were based on the Centers for Disease Control definition1 of health factors known to increase the risk of developing serious complications from influenza. The majority of subjects had underlying asthma or chronic lung disease, diabetes, heart disease, morbid obesity, or were 65 years of age or older.
In Trial 3, 1,158 of the 2,182 enrolled subjects had influenza confirmed by RT-PCR and were included in the efficacy analysis (XOFLUZA N=385, placebo N=385, or oseltamivir N=388). Among subjects in whom only one type/subtype of influenza virus was identified, 50% were infected with subtype A/H3N2, 43% were infected with type B, and 7% were infected with subtype A/H1N1.
Eligible subjects had an axillary temperature of at least 38°C, at least one moderate or severe respiratory symptom (cough, nasal congestion, or sore throat), and at least one moderate or severe systemic symptom (headache, feverishness or chills, muscle or joint pain, or fatigue) and all were treated within 48 hours of symptom onset. Subjects participating in the trial were required to self-assess their influenza symptoms as "none", "mild", "moderate" or "severe" twice daily. A total of 215 subjects (19%) had pre-existing symptoms (cough, muscle or joint pain, or fatigue) associated with their underlying high-risk condition that were worsened due to influenza infection. The primary efficacy endpoint was time to improvement of influenza symptoms (cough, sore throat, headache, nasal congestion, feverishness or chills, muscle or joint pain, and fatigue). This endpoint included alleviation of new symptoms and improvement of any pre-existing symptoms that had worsened due to influenza. A statistically significant improvement in the primary endpoint was observed for XOFLUZA when compared with placebo, see Table 7.
Table 7 Time to Improvement of Symptoms After Single Dose in High Risk Subjects 12 Years of Age and Older with Acute Uncomplicated Influenza in Trial 3 (Median Hours) XOFLUZA 40/80 mg
(95% CI*)
N=385Placebo
(95% CI*)
N=385- * CI: Confidence Interval
- † XOFLUZA treatment resulted in a significant reduction in Time to Improvement of Influenza Symptoms compared to placebo using Peto-Prentice's generalized Wilcoxon test (p-value: <0.001).
73†
(67, 85)102†
(93, 113)There was no statistically significant difference in the median time to improvement of influenza symptoms in the subjects who received XOFLUZA (73 hours) and those who received oseltamivir (81 hours). The median time to improvement of influenza symptoms in the limited number of adolescent subjects aged 12 to 17 years infected with influenza virus was similar for subjects who received XOFLUZA (188 hours) or placebo (191 hours) (N=13 and N=12, respectively).
For subjects infected with type B virus, the median time to improvement of influenza symptoms was 75 hours in the XOFLUZA group (95% CI of 67, 90) compared to 101 hours in the placebo group (95% CI of 83, 116).
- 15 REFERENCES
-
16 HOW SUPPLIED/STORAGE AND HANDLING
XOFLUZA Tablets:
-
20 mg white to light yellow, oblong shaped film-coated tablets debossed with "
 772" on one side and "20" on the other side available as:
772" on one side and "20" on the other side available as:- 2 × 20 mg tablets per blister card in secondary packaging: NDC: 50242-828-02
- 40 mg white to light yellow, oblong shaped film-coated tablets debossed with "BXM40" on one side available as:
- 2 × 40 mg tablets per blister card in secondary packaging: NDC: 50242-860-02
-
-
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient Information).
Important Dosing Information
Instruct patients to begin treatment with XOFLUZA as soon as possible at the first appearance of influenza symptoms, within 48 hours of onset of symptoms. XOFLUZA can be taken with or without food, but advise patients not to take with dairy products, calcium-fortified beverages, polyvalent cation-containing laxatives, antacids or oral supplements (e.g., calcium, iron, magnesium, selenium, or zinc) [see Dosage and Administration (2) and Drug Interactions (7.1)].
Advise patients to follow the healthcare provider's dosing recommendation for a single, one-time dose of XOFLUZA. XOFLUZA is dosed based on weight and is available in blister cards containing two tablets of 20 mg to be taken together as a single 40 mg dose and blister cards containing two tablets of 40 mg to be taken together as a single 80 mg dose [see How Supplied/Storage and Handling (16)].
Hypersensitivity
Advise patients and/or caregivers of the risk of severe allergic reactions such as anaphylaxis, angioedema, urticaria and erythema multiforme. Instruct patients and/or caregivers to seek immediate medical attention if an allergic-like reaction occurs or is suspected [see Contraindications (4), and Warnings and Precautions (5.1)].
Influenza Vaccines
Because of the potential for antivirals to decrease the effectiveness of live attenuated influenza vaccine, advise patients to consult their healthcare provider prior to receiving a live attenuated influenza vaccine after taking XOFLUZA [see Drug Interactions (7.2)].
- SPL UNCLASSIFIED SECTION
-
PATIENT PACKAGE INSERT
This Patient Information has been approved by the U.S. Food and Drug Administration. Revised: 10/2019 PATIENT INFORMATION
XOFLUZA® (zoh-FLEW-zuh)
(baloxavir marboxil)
tabletsWhat is XOFLUZA?
XOFLUZA is a prescription medicine used to treat the flu (influenza) in people 12 years of age and older who have had flu symptoms for no more than 48 hours.
It is not known if XOFLUZA is safe and effective in children less than 12 years of age or weighing less than 88 pounds (40 kg).Do not take XOFLUZA if you are allergic to baloxavir marboxil or any of the ingredients in XOFLUZA.
See the end of this leaflet for a complete list of ingredients in XOFLUZA.Before you take XOFLUZA, tell your healthcare provider about all of your medical conditions, including if you: - are pregnant or plan to become pregnant. It is not known if XOFLUZA can harm your unborn baby.
- are breastfeeding or plan to breastfeed. It is not known if XOFLUZA passes into your breast milk.
Talk to your healthcare provider before you receive a live flu vaccine after taking XOFLUZA.How should I take XOFLUZA? - Take XOFLUZA exactly as your healthcare provider tells you to.
- Your healthcare provider will prescribe 2 tablets of XOFLUZA you will take at the same time as a single dose.
- Take XOFLUZA with or without food.
- Do not take XOFLUZA with dairy products, calcium-fortified beverages, laxatives, antacids or oral supplements containing iron, zinc, selenium, calcium or magnesium.
- If you take too much XOFLUZA, go to the nearest emergency room right away.
What are the possible side effects of XOFLUZA?
XOFLUZA may cause serious side effects, including:- Allergic reactions. Get emergency medical help right away if you develop any of these signs and symptoms of an allergic reaction:
- trouble breathing
- skin rash, hives or blisters
- swelling of your face, throat or mouth
- dizziness or lightheadedness
The most common side effects of XOFLUZA in adults and adolescents include: - diarrhea
- bronchitis
- sinusitis
- headache
- nausea
XOFLUZA is not effective in treating infections other than influenza. Other kinds of infections can appear like flu or occur along with flu and may need different kinds of treatment. Tell your healthcare provider if you feel worse or develop new symptoms during or after treatment with XOFLUZA or if your flu symptoms do not start to get better.
These are not all the possible side effects of XOFLUZA.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.How should I store XOFLUZA? - Store XOFLUZA at room temperature between 68°F to 77°F (20°C to 25°C).
- Store XOFLUZA in the blister package that it comes in.
General information about the safe and effective use of XOFLUZA.
Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. Do not use XOFLUZA for a condition for which it was not prescribed. Do not give XOFLUZA to other people, even if they have the same symptoms that you have. It may harm them. You can ask for information about XOFLUZA that is written for health professionals.What are the ingredients in XOFLUZA?
Active ingredient: baloxavir marboxil
Inactive ingredients: croscarmellose sodium, hypromellose, lactose monohydrate, microcrystalline cellulose, povidone, sodium stearyl fumarate, talc, and titanium dioxide.
Distributed by: Genentech USA, Inc., A Member of the Roche Group 1 DNA Way, South San Francisco, CA 94080-4990
Manufactured by: Shionogi Pharma Co., Ltd. 2-5-1 Mishima, Settsu, Osaka 566-0022, Japan
XOFLUZA® is a registered trademark of Genentech, Inc. © 2019 Genentech USA, Inc.
For more information, go to www.XOFLUZA.com or call 1-855-XOFLUZA (1-855-963-5892).Representative sample of labeling (see the HOW SUPPLIED section for complete listing):
-
PRINCIPAL DISPLAY PANEL - 20 mg Tablet Blister Pack Carton
Xofluza®
(baloxavir marboxil) tablets
20 mg per tabletNDC: 50242-828-02
Contains 40 mg total dose (2 x 20 mg tablets)
Usual dosage:
Take both tablets in this package
as a single, one-time doseLIFT HERE
TO OPENRx only
Genentech
10218807
-
PRINCIPAL DISPLAY PANEL - 40 mg Tablet Blister Pack Carton
Xofluza®
(baloxavir marboxil) tablets
40 mg per tabletNDC: 50242-860-02
Contains 80 mg total dose (2 x 40 mg tablets)
Usual dosage:
Take both tablets in this package
as a single, one-time doseLIFT HERE
TO OPENRx only
Genentech
10218834
-
INGREDIENTS AND APPEARANCE
XOFLUZA
baloxavir marboxil tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 50242-828 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength BALOXAVIR MARBOXIL (UNII: 505CXM6OHG) (BALOXAVIR - UNII:4G86Y4JT3F) BALOXAVIR MARBOXIL 20 mg Inactive Ingredients Ingredient Name Strength LACTOSE MONOHYDRATE (UNII: EWQ57Q8I5X) CROSCARMELLOSE SODIUM (UNII: M28OL1HH48) POVIDONE K25 (UNII: K0KQV10C35) MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) SODIUM STEARYL FUMARATE (UNII: 7CV7WJK4UI) HYPROMELLOSE, UNSPECIFIED (UNII: 3NXW29V3WO) TALC (UNII: 7SEV7J4R1U) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) Product Characteristics Color YELLOW (white to light yellow) Score no score Shape OVAL Size 9mm Flavor Imprint Code 772;20 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 50242-828-02 1 in 1 CARTON 10/24/2018 1 2 in 1 BLISTER PACK; Type 0: Not a Combination Product 2 NDC: 50242-828-86 1 in 1 CARTON 10/24/2018 2 2 in 1 BLISTER PACK; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA210854 10/24/2018 XOFLUZA
baloxavir marboxil tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 50242-860 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength BALOXAVIR MARBOXIL (UNII: 505CXM6OHG) (BALOXAVIR - UNII:4G86Y4JT3F) BALOXAVIR MARBOXIL 40 mg Inactive Ingredients Ingredient Name Strength LACTOSE MONOHYDRATE (UNII: EWQ57Q8I5X) CROSCARMELLOSE SODIUM (UNII: M28OL1HH48) POVIDONE K25 (UNII: K0KQV10C35) MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) SODIUM STEARYL FUMARATE (UNII: 7CV7WJK4UI) HYPROMELLOSE, UNSPECIFIED (UNII: 3NXW29V3WO) TALC (UNII: 7SEV7J4R1U) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) Product Characteristics Color YELLOW (white to light yellow) Score no score Shape OVAL Size 11mm Flavor Imprint Code BXM40 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 50242-860-02 1 in 1 CARTON 10/24/2018 1 2 in 1 BLISTER PACK; Type 0: Not a Combination Product 2 NDC: 50242-860-87 1 in 1 CARTON 10/24/2018 2 2 in 1 BLISTER PACK; Type 0: Not a Combination Product Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA210854 10/24/2018 Labeler - Genentech, Inc (080129000)
 772" on one side and "20" on the other side.
772" on one side and "20" on the other side.Trademark Results [Xofluza]
Mark Image Registration | Serial | Company Trademark Application Date |
|---|---|
 XOFLUZA 90777855 not registered Live/Pending |
Genentech, Inc. 2021-06-16 |
 XOFLUZA 87920532 not registered Live/Pending |
Genentech, Inc. 2018-05-14 |
 XOFLUZA 87762294 not registered Live/Pending |
Shionogi & Co., Ltd. 2018-01-19 |
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.