MEFLOQUINE HYDROCHLORIDE tablet
Mefloquine Hydrochloride by
Drug Labeling and Warnings
Mefloquine Hydrochloride by is a Prescription medication manufactured, distributed, or labeled by H.J. Harkins Company, Inc., West-ward Pharmaceutical Corp. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
DESCRIPTION
Mefloquine Hydrochloride Tablets are an antimalarial agent available as 250-mg tablets of mefloquine hydrochloride (equivalent to 228.0 mg of the free base) for oral administration.
Mefloquine hydrochloride is a 4-quinolinemethanol derivative with the specific chemical name of (R*,S*)-(±)-α-2-piperidinyl-2,8-bis (trifluoromethyl)-4-quinolinemethanol hydrochloride. It is a 2-aryl substituted chemical structural analog of quinine. The drug is a white to almost white crystalline compound, slightly soluble in water.
Mefloquine hydrochloride has a calculated molecular weight of 414.78 and the following structural formula:
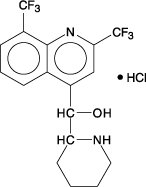
Each tablet, for oral administration, contains 250 mg mefloquine hydrochloride and the following inactive ingredients: colloidal silicon dioxide, corn starch, crospovidone, lactose monohydrate, lactose spray dried, magnesium stearate, microcrystalline cellulose, polysorbate 80, polyvinylpyrrolidone and talc.
-
CLINICAL PHARMACOLOGY
Pharmacokinetics
Absorption
The absolute oral bioavailability of mefloquine has not been determined since an intravenous formulation is not available. The bioavailability of the tablet formation compared with an oral solution was over 85%. The presence of food significantly enhances the rate and extent of absorption, leading to about a 40% increase in bioavailability. In healthy volunteers, plasma concentrations peak 6 to 24 hours (median, about 17 hours) after a single dose of Mefloquine Hydrochloride Tablets. In a similar group of volunteers, maximum plasma concentrations in μg/L are roughly equivalent to the dose in milligrams (for example, a single 1000 mg dose produces a maximum concentration of about 1000 μg/L). In healthy volunteers, a dose of 250 mg once weekly produces maximum steady-state plasma concentrations of 1000 to 2000 μg/L, which are reached after 7 to 10 weeks.
Distribution
In healthy adults, the apparent volume of distribution is approximately 20 L/kg, indicating extensive tissue distribution. Mefloquine may accumulate in parasitized erythrocytes. Experiments conducted in vitro with human blood using concentrations between 50 and 1000 mg/mL showed a relatively constant erythrocyte-to-plasma concentration ratio of about 2 to 1. The equilibrium reached in less than 30 minutes was found to be reversible. Protein binding is about 98%.
Mefloquine crosses the placenta. Excretion into breast milk appears to be minimal (see PRECAUTIONS: Nursing Mothers).
Metabolism
Mefloquine is extensively metabolized in the liver by the cytochrome P450 system. In vitro and in vivo studies strongly suggested that CYP3A4 is the major isoform involved.
Two metabolites of mefloquine have been identified in humans. The main metabolite, 2,8-bis-trifluoromethyl-4-quinoline carboxylic acid, is inactive in Plasmodium falciparum. In a study in healthy volunteers, the carboxylic acid metabolite appeared in plasma 2 to 4 hours after a single oral dose. Maximum plasma concentrations of the metabolite, which were about 50% higher than those of mefloquine, were reached after 2 weeks. Thereafter, plasma levels of the main metabolite and mefloquine declined at a similar rate. The area under the plasma concentration-time curve (AUC) of the main metabolite was 3 to 5 times larger than that of the parent drug. The other metabolite, an alcohol, was present in minute quantities only.
Elimination
In several studies in healthy adults, the mean elimination half-life of mefloquine varied between 2 and 4 weeks, with an average of about 3 weeks. Total clearance, which is essentially hepatic, is in the order of 30 mL/min. There is evidence that mefloquine is excreted mainly in the bile and feces. In volunteers, urinary excretion of unchanged mefloquine and its main metabolite under steady-state condition accounted for about 9% and 4% of the dose, respectively. Concentrations of other metabolites could not be measured in the urine.
Pharmacokinetics in Special Clinical Situations
Children and the Elderly
No relevant age-related changes have been observed in the pharmacokinetics of mefloquine. Therefore, the dosage for children has been extrapolated from the recommended adult dose.
No pharmacokinetic studies have been performed in patients with renal insufficiency since only a small proportion of the drug is eliminated renally. Mefloquine and its main metabolite are not appreciably removed by hemodialysis. No special chemoprophylactic dosage adjustments are indicated for dialysis patients to achieve concentrations in plasma similar to those in healthy persons.
Although clearance of mefloquine may increase in late pregnancy, in general, pregnancy has no clinically relevant effect on the pharmacokinetics of mefloquine.
The pharmacokinetics of mefloquine may be altered in acute malaria.
Pharmacokinetic differences have been observed between various ethnic populations. In practice, however, these are of minor importance compared with host immune status and sensitivity of the parasite.
During long-term prophylaxis (>2 years), the trough concentrations and the elimination half-life of mefloquine were similar to those obtained in the same population after 6 months of drug use, which is when they reached steady state.
In vitro and in vivo studies showed no hemolysis associated with glucose-6-phosphate dehydrogenase deficiency (see ANIMAL TOXICOLOGY).
Microbiology
Mechanism of Action
Mefloquine is an antimalarial agent which acts as a blood schizonticide. Its exact mechanism of action is not known.
Activity In Vitro and In Vivo
Mefloquine is active against the erythrocytic stages of Plasmodium species (See INDICATIONS AND USAGE). However, the drug has no effect against the exoerythrocytic (hepatic) stages of the parasite. Mefloquine is effective against malaria parasites resistant to chloroquine (see INDICATIONS AND USAGE).
Drug Resistance
Strains of P. falciparum with decreased susceptibility to mefloquine can be selected in vitro or in vivo. Resistance of P. falciparum to mefloquine has been reported in areas of multi-drug resistance in South East Asia. Increased incidences of resistance have also been reported in other parts of the world.
-
INDICATIONS AND USAGE
Treatment of Acute Malaria Infections
Mefloquine Hydrochloride Tablets are indicated for the treatment of mild to moderate acute malaria caused by mefloquine-susceptible strains of P. falciparum (both chloroquine-susceptible and resistant strains) or by Plasmodium vivax. There are insufficient clinical data to document the effect of mefloquine in malaria caused by P. ovale or P. malariae.
- Note: Patients with acute P. vivax malaria, treated with Mefloquine Hydrochloride Tablets, are at high risk of relapse because Mefloquine Hydrochloride Tablets do not eliminate exoerythrocytic (hepatic phase) parasites. To avoid relapse, after initial treatment of the acute infection with mefloquine, patients should subsequently be treated with an 8-aminoquinoline derivative (e.g., primaquine).
-
CONTRAINDICATIONS
Use of Mefloquine Hydrochloride Tablets is contraindicated in patients with a known hypersensitivity to mefloquine or related compounds (e.g., quinine and quinidine) or to any of the excipients contained in the formulation. Mefloquine Hydrochloride Tablets should not be prescribed for prophylaxis in patients with active depression, a recent history of depression, generalized anxiety disorder, psychosis, or schizophrenia or other major psychiatric disorders, or with a history of convulsions.
-
WARNINGS
In case of life-threatening, serious or overwhelming malaria infections due to P. falciparum, patients should be treated with an intravenous antimalarial drug. Following completion of intravenous treatment, Mefloquine Hydrochloride Tablets may be given to complete the course of therapy.
Halofantrine should not be administered with Mefloquine Hydrochloride Tablets or within 15 weeks of the last dose of Mefloquine Hydrochloride Tablets due to the risk of a potentially fatal prolongation of the QTc interval (see CLINICAL PHARMACOLOGY: Pharmacokinetics: Elimination).
Ketoconazole should not be administered with Mefloquine Hydrochloride Tablets or within 15 weeks of the last dose of Mefloquine Hydrochloride Tablets due to the risk of a potentially fatal prolongation of the QTc interval. Ketoconazole increases plasma concentrations and elimination half-life of mefloquine following co-administration (see CLINICAL PHARMACOLOGY: Pharmacokinetics: Elimination and PRECAUTIONS: Drug Interactions).
Mefloquine may cause psychiatric symptoms in a number of patients, ranging from anxiety, paranoia, and depression to hallucinations and psychotic behavior. On occasions, these symptoms have been reported to continue long after mefloquine has been stopped. Rare cases of suicidal ideation and suicide have been reported though no relationship to drug administration has been confirmed. To minimize the chances of these adverse events, mefloquine should not be taken for prophylaxis in patients with active depression or with a recent history of depression, generalized anxiety disorder, psychosis, or schizophrenia or other major psychiatric disorders. Mefloquine Hydrochloride Tablets should be used with caution in patients with a previous history of depression.
During prophylactic use, if psychiatric symptoms such as acute anxiety, depression, restlessness or confusion occur, these may be considered prodromal to a more serious event. In these cases, the drug must be discontinued and an alternative medication should be substituted.
Concomitant administration of Mefloquine Hydrochloride Tablets and quinine or quinidine may produce electrocardiographic abnormalities.
Concomitant administration of Mefloquine Hydrochloride Tablets and quinine or chloroquine may increase the risk of convulsions.
-
PRECAUTIONS
Hypersensitivity Reactions
Hypersensitivity reactions ranging from mild cutaneous events to anaphylaxis cannot be predicted. In patients with epilepsy, Mefloquine Hydrochloride Tablets may increase the risk of convulsions. The drug should therefore be prescribed only for curative treatment in such patients and only if there are compelling medical reasons for its use (see PRECAUTIONS: Drug Interactions).
Central and Peripheral Nervous System Effects
Caution should be exercised with regard to activities requiring alertness and fine motor coordination such as driving, piloting aircraft, operating machinery, and deep-sea diving, as dizziness or vertigo, a loss of balance, or other disorders of the central or peripheral nervous system have been reported during and following the use of Mefloquine Hydrochloride Tablets. Because of the long half-life of mefloquine, adverse reactions to mefloquine may occur or persist up to several weeks after discontinuation of the drug. In a small number of patients, dizziness or vertigo and loss of balance have been reported to continue for months after discontinuation of the drug (see ADVERSE REACTIONS: Postmarketing).
Mefloquine Hydrochloride Tabletsshould be used with caution in patients with psychiatric disturbances because mefloquine use has been associated with emotional disturbances (see ADVERSE REACTIONS).
Use in Patients with Hepatic Impairment
In patients with impaired liver function the elimination of mefloquine may be prolonged, leading to higher plasma levels and a higher risk of adverse reactions.
Long-Term Use
This drug has been administered for longer than one year. If the drug is to be administered for a prolonged period, periodic evaluations including liver function tests should be performed.
Although retinal abnormalities seen in humans with long-term chloroquine use have not been observed with mefloquine use, long-term feeding of mefloquine to rats resulted in dose-related ocular lesions (retinal degeneration, retinal edema and lenticular opacity at 12.5 mg/kg/day and higher) (see ANIMAL TOXICOLOGY). Therefore, periodic ophthalmic examinations are recommended.
Cardiac Effects
Parenteral studies in animals show that mefloquine, a myocardial depressant, possesses 20% of the anti-fibrillatory action of quinidine and produces 50% of the increase in the PR interval reported with quinine. The effect of mefloquine on the compromised cardiovascular system has not been evaluated. However, transitory and clinically silent ECG alterations have been reported during the use of mefloquine. Alterations included sinus bradycardia, sinus arrhythmia, first degree AV-block, prolongation of the QTc interval and abnormal T waves (see also cardiovascular effects under PRECAUTIONS: Drug Interactions and ADVERSE REACTIONS). The benefits of Mefloquine Hydrochloride Tablets therapy should be weighed against the possibility of adverse effects in patients with cardiac disease.
Drug Resistance and Cross-Resistance
Geographical drug resistance patterns of P. falciparum occur and the preferred choice of malaria prophylaxis might be different from one area to another. For example, resistance of P. falciparum to mefloquine has been reported, predominately in areas of multi-drug resistance in South-East Asia. Cross-resistance between mefloquine and halofantrine and cross-resistance between mefloquine and quinine have been observed in some regions. For current advice on geographical resistance patterns competent national expert centers should be consulted.
Agranulocytosis and Aplastic Anemia
Cases of agranulocytosis and aplastic anemia have been reported during Mefloquine Hydrochloride Tablets therapy (see ADVERSE REACTIONS).
Laboratory Tests
Periodic evaluation of hepatic function should be performed during prolonged prophylaxis.
Information for Patients
Medication Guide: As required by law, a Mefloquine Hydrochloride Tablets Medication Guide is supplied to patients when Mefloquine Hydrochloride Tablets are dispensed. An information wallet card is also supplied to patients when Mefloquine Hydrochloride Tablets are dispensed. Patients should be instructed to read the Medication Guide when mefloquine is received and to carry the information wallet card with them when they are taking Mefloquine Hydrochloride Tablets. The complete texts of the Medication Guide and information wallet card are reprinted at the end of this document.
Patients should be advised:
- that malaria can be a life-threatening infection in the traveler;
- that Mefloquine Hydrochloride Tablets are being prescribed to help prevent or treat this serious infection;
- that in a small percentage of cases, patients are unable to take this medication because of side effects, including dizziness or vertigo and loss of balance, and it may be necessary to change medications. Although side effects of dizziness or vertigo and loss of balance are usually mild and do not cause people to stop taking the medication, in a small number of patients it has been reported that these symptoms may continue for months after discontinuation of the drug;
- that when used as prophylaxis, the first dose of Mefloquine Hydrochloride Tablets should be taken one week prior to arrival in an endemic area;
- that if the patients experience psychiatric symptoms such as acute anxiety, depression, restlessness or confusion, these may be considered prodromal to a more serious event. In these cases, the drug must be discontinued and an alternative medication should be substituted;
- that no chemoprophylactic regimen is 100% effective, and protective clothing, insect repellents, and bednets are important components of malaria prophylaxis;
- to seek medical attention for any febrile illness that occurs after return from a malarious area and to inform their physician that they may have been exposed to malaria.
Drug Interactions
Drug-drug interactions with Mefloquine Hydrochloride Tablets have not been explored in detail. There is one report of cardiopulmonary arrest, with full recovery, in a patient who was taking a beta blocker (propranolol) (see PRECAUTIONS: Cardiac Effects). The effects of mefloquine on the compromised cardiovascular system have not been evaluated. The benefits of mefloquine therapy should be weighed against the possibility of adverse effects in patients with cardiac disease.
Halofantrine and Other Antimalarials
Halofantrine should not be administered with Mefloquine Hydrochloride Tablets or within 15 weeks of the last dose of Mefloquine Hydrochloride Tablets due to the risk of a potentially fatal prolongation of the QTc interval (see WARNINGS).
Concomitant administration of Mefloquine Hydrochloride Tablets and other related antimalarial compounds (e.g., quinine, quinidine and chloroquine) may produce electrocardiographic abnormalities and increase the risk of convulsions (see WARNINGS). If these drugs are to be used in the initial treatment of severe malaria, Mefloquine Hydrochloride Tablets administration should be delayed at least 12 hours after the last dose. Clinically significant QTc prolongation has not been found with mefloquine alone.
Ketoconazole (Potent Inhibitor of CYP3A4)
Co-administration of a single 500 mg oral dose of Mefloquine Hydrochloride Tablets with 400 mg of ketoconazole once daily for 10 days in 8 healthy volunteers resulted in an increase in the mean Cmax and AUC of mefloquine by 64% and 79%, respectively, and an increase in the mean elimination half-life of mefloquine from 322 hours to 448 hours. Ketoconazole should not be administered with Mefloquine Hydrochloride Tablets or within 15 weeks of the last dose of Mefloquine Hydrochloride Tablets due to the risk of a potentially fatal prolongation of the QTc interval (see WARNINGS).
Other Drugs that Prolong the QTc Interval
Co-administration of other drugs known to alter cardiac conduction (e.g., anti-arrhythmic or beta-adrenergic blocking agents, calcium channel blockers, antihistamines or H1-blocking agents, tricyclic antidepressants and phenothiazines) might also contribute to a prolongation of the QTc interval. There are no data that conclusively establish whether the concomitant administration of mefloquine and the above listed agents has an effect on cardiac function.
Anticonvulsants
In patients taking an anticonvulsant (e.g., valproic acid, carbamazepine, phenobarbital or phenytoin), the concomitant use of Mefloquine Hydrochloride Tablets may reduce seizure control by lowering the plasma levels of the anticonvulsant. Therefore, patients concurrently taking antiseizure medication and Mefloquine Hydrochloride Tablets should have the blood level of their antiseizure medication monitored and the dosage adjusted appropriately (see PRECAUTIONS).
Vaccines
When Mefloquine Hydrochloride Tablets are taken concurrently with oral live typhoid vaccines, attenuation of immunization cannot be excluded. Vaccinations with attenuated live bacteria should therefore be completed at least 3 days before the first dose of Mefloquine Hydrochloride Tablets.
Rifampin (Potent Inducer of CYP3A4)
Co-administration of a single 500 mg oral dose of Mefloquine Hydrochloride Tablets and 600 mg of rifampin once daily for 7 days in 7 healthy Thai volunteers resulted in a decrease in the mean Cmax and AUC of mefloquine by 19% and 68%, respectively, and a decrease in the mean elimination half-life of mefloquine from 305 hours to 113 hours. Rifampin should be used cautiously in patients taking Mefloquine Hydrochloride Tablets .
Inhibitors and Inducers of CYP3A4
Mefloquine does not inhibit or induce the CYP 450 enzyme system. Thus, concomitant administration of Mefloquine Hydrochloride Tablets and substrates of the CYP 450 enzyme system is not expected to result in a drug interaction. However, mefloquine is metabolized by CYP3A4 and inhibitors of CYP3A4 may modify the pharmacokinetics/metabolism of mefloquine, leading to an increase in mefloquine plasma concentrations and potential risk of adverse reactions. Therefore, Mefloquine Hydrochloride Tablets should be used with caution when administered concomitantly with CYP3A4 inhibitors. Similarly, inducers of CYP3A4 may modify the pharmacokinetics/metabolism of mefloquine, leading to a decrease in mefloquine plasma concentrations and potential reduction in efficacy of Mefloquine Hydrochloride Tablets. Therefore, Mefloquine Hydrochloride Tablets should also be used with caution when administered concomitantly with CYP3A4 inducers.
Substrates and Inhibitors of P-glycoprotein
It has been shown in vitro that mefloquine is a substrate and an inhibitor of P-glycoprotein. Therefore, drug-drug interactions could also occur with drugs that are substrates or are known to modify the expression of this transporter. The clinical relevance of these interactions is not known to date.
Other Potential Interactions
No other drug interactions are known. Nevertheless, the effects of Mefloquine Hydrochloride Tablets on travelers receiving comedication, particularly diabetics or patients using anticoagulants, should be checked before departure.
In clinical trials, the concomitant administration of sulfadoxine and pyrimethamine did not alter the adverse reaction profile of mefloquine.
Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
The carcinogenic potential of mefloquine was studied in rats and mice in 2-year feeding studies at doses of up to 30 mg/kg/day. No treatment-related increases in tumors of any type were noted.
Mutagenesis
The mutagenic potential of mefloquine was studied in a variety of assay systems including: Ames test, a host-mediated assay in mice, fluctuation tests and a mouse micronucleus assay. Several of these assays were performed with and without prior metabolic activation. In no instance was evidence obtained for the mutagenicity of mefloquine.
Impairment of Fertility
Fertility studies in rats at doses of 5, 20, and 50 mg/kg/day of mefloquine have demonstrated adverse effects on fertility in the male at the high dose of 50 mg/kg/day, and in the female at doses of 20 and 50 mg/kg/day. Histopathological lesions were noted in the epididymides from male rats at doses of 20 and 50 mg/kg/day. Administration of 250 mg/week of mefloquine (base) in adult males for 22 weeks failed to reveal any deleterious effects on human spermatozoa.
Pregnancy
Pregnancy Category B
Data from published studies in pregnant women have shown no increase in the risk of teratogenic effects or adverse pregnancy outcomes following mefloquine treatment or prophylaxis during pregnancy. Reproduction studies in mice, rats and rabbits have shown teratogenic effects at doses similar to the clinical acute treatment dose in humans. Despite the animal findings, it would appear that the possibility of fetal harm is remote, if the drug is used during pregnancy. Nevertheless, because the studies in humans cannot rule out the possibility of harm, mefloquine should be used during pregnancy only if clearly needed.
Published data on mefloquine use during pregnancy include randomized controlled trials, intervention trials, prospective and retrospective cohort studies, and case series. These data showed that pregnant women who took mefloquine at various doses for both prevention and treatment of malaria did not have an increased risk of teratogenic effects or adverse pregnancy outcomes compared to the background rate in the general population. These data include more than 700 exposures to mefloquine in the first trimester of pregnancy and over 2,000 exposures in the second and third trimester.
Mefloquine administered to pregnant mice, rats, and rabbits was teratogenic at doses similar to the clinical acute treatment dose of 21 to 25 mg/kg, based on body surface area comparisons. In all three animal species, CNS effects (e.g., exencephaly, hydrocephaly or partially missing medulla oblongata) and craniofacial malformations were observed. At the same doses, mefloquine was also embryotoxic in mice and rabbits. All of these findings were observed at doses that were maternally toxic.
Nursing Mothers
Mefloquine is excreted in human milk in small amounts, the activity of which is unknown. Based on a study in a few subjects, low concentrations (3% to 4%) of mefloquine were excreted in human milk following a dose equivalent to 250 mg of the free base. Caution should be exercised when administered to a nursing woman.
Pediatric Use
Use of Mefloquine Hydrochloride Tablets to treat acute, uncomplicated P. falciparum malaria in pediatric patients is supported by evidence from adequate and well-controlled studies of Mefloquine Hydrochloride Tablets in adults with additional data from published open-label and comparative trials using Mefloquine Hydrochloride Tablets to treat malaria caused by P. falciparum in patients younger than 16 years of age. The safety and effectiveness of Mefloquine Hydrochloride Tablets for the treatment of malaria in pediatric patients below the age of 6 months have not been established.
In several studies, the administration of Mefloquine Hydrochloride Tablets for the treatment of malaria was associated with early vomiting in pediatric patients. Early vomiting was cited in some reports as a possible cause of treatment failure. If a second dose is not tolerated, the patient should be monitored closely and alternative malaria treatment considered if improvement is not observed within a reasonable period of time (see DOSAGE AND ADMINISTRATION).
Geriatric Use
Clinical studies of Mefloquine Hydrochloride Tablets did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. Since electrocardiographic abnormalities have been observed in individuals treated with Mefloquine Hydrochloride Tablets (see PRECAUTIONS) and underlying cardiac disease is more prevalent in elderly than in younger patients, the benefits of Mefloquine Hydrochloride Tablets therapy should be weighed against the possibility of adverse cardiac effects in elderly patients.
-
ADVERSE REACTIONS
Clinical
At the doses used for treatment of acute malaria infections, the symptoms possibly attributable to drug administration cannot be distinguished from those symptoms usually attributable to the disease itself.
Among subjects who received mefloquine for prophylaxis of malaria, the most frequently observed adverse experience was vomiting (3%). Dizziness, syncope, extrasystoles and other complaints affecting less than 1% were also reported.
Among subjects who received mefloquine for treatment, the most frequently observed adverse experiences included: dizziness, myalgia, nausea, fever, headache, vomiting, chills, diarrhea, skin rash, abdominal pain, fatigue, loss of appetite, and tinnitus. Those side effects occurring in less than 1% included bradycardia, hair loss, emotional problems, pruritus, asthenia, transient emotional disturbances and telogen effluvium (loss of resting hair). Seizures have also been reported.
Two serious adverse reactions were cardiopulmonary arrest in one patient shortly after ingesting a single prophylactic dose of mefloquine while concomitantly using propranolol (see PRECAUTIONS: Drug Interactions), and encephalopathy of unknown etiology during prophylactic mefloquine administration. The relationship of encephalopathy to drug administration could not be clearly established.
Laboratory
The most frequently observed laboratory alterations which could be possibly attributable to drug administration were decreased hematocrit, transient elevation of transaminases, leukopenia and thrombocytopenia. These alterations were observed in patients with acute malaria who received treatment doses of the drug and were attributed to the disease itself.
During prophylactic administration of mefloquine to indigenous populations in malaria-endemic areas, the following occasional alterations in laboratory values were observed: transient elevation of transaminases, leukocytosis or thrombocytopenia.
Because of the long half-life of mefloquine, adverse reactions to Mefloquine Hydrochloride Tablets may occur or persist up to several weeks after discontinuation of the drug.
Postmarketing
Postmarketing surveillance indicates that the same kind of adverse experiences are reported during prophylaxis, as well as acute treatment. Because these experiences are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to Mefloquine Hydrochloride Tablets exposure.
The most frequently reported adverse events are nausea, vomiting, loose stools or diarrhea, abdominal pain, dizziness or vertigo, loss of balance, and neuropsychiatric events such as headache, somnolence, and sleep disorders (insomnia, abnormal dreams). These are usually mild and may decrease despite continued use. In a small number of patients it has been reported that dizziness or vertigo and loss of balance may continue for months after discontinuation of the drug.
Occasionally, more severe neuropsychiatric disorders have been reported such as: sensory and motor neuropathies (including paresthesia, tremor and ataxia), convulsions, agitation or restlessness, anxiety, depression, mood swings, panic attacks, memory impairment, confusion, hallucinations, aggression, psychotic or paranoid reactions and encephalopathy. Rare cases of suicidal ideation and suicide have been reported though no relationship to drug administration has been confirmed.
Other less frequently reported adverse events include:
Cardiovascular Disorders: circulatory disturbances (hypotension, hypertension, flushing, syncope), chest pain, tachycardia or palpitation, bradycardia, irregular heart rate, extrasystoles, A-V block, and other transient cardiac conduction alterations
Skin Disorders: rash, exanthema, erythema, urticaria, pruritus, edema, hair loss, erythema multiforme, and Stevens-Johnson syndrome
Musculoskeletal Disorders: muscle weakness, muscle cramps, myalgia, and arthralgia
Respiratory Disorders: dyspnea, pneumonitis of possible allergic etiology
Hepatobiliary Disorders: drug-related hepatic disorders from asymptomatic transient transaminase elevations to hepatic failure drug-related hepatic disorders from asymptomatic transient transaminase elevations to hepatic failure
Blood and Lymphatic System Disorders: agranulocytosis, aplastic anemia agranulocytosis, aplastic anemia
Other Symptoms: visual disturbances, vestibular disorders including tinnitus and hearing impairment, asthenia, malaise, fatigue, fever, hyperhidrosis, chills, dyspepsia and loss of appetite
To report SUSPECTED ADVERSE REACTIONS, contact West-ward Pharmaceutical Corp. at 1-877-233- 2001, and the FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
-
OVERDOSAGE
Symptoms and Signs
In cases of overdosage with Mefloquine Hydrochloride Tablets, the symptoms mentioned under ADVERSE REACTIONS may be more pronounced.
Treatment
Patients should be managed by symptomatic and supportive care following Mefloquine Hydrochloride Tablets overdose. There are no specific antidotes. Monitor cardiac function (if possible by ECG) and neuropsychiatric status for at least 24 hours. Provide symptomatic and intensive supportive treatment as required, particularly for cardiovascular disturbances.
-
DOSAGE AND ADMINISTRATION
(see INDICATIONS AND USAGE)
Adult Patients
Treatment of mild to moderate malaria in adults caused by P. vivax or mefloquine-susceptible strains of P. falciparum
Five tablets (1250 mg) mefloquine hydrochloride to be given as a single oral dose. The drug should not be taken on an empty stomach and should be administered with at least 8 oz (240 mL) of water.
If a full-treatment course with Mefloquine Hydrochloride Tablets does not lead to improvement within 48 to 72 hours, Mefloquine Hydrochloride Tablets should not be used for retreatment. An alternative therapy should be used. Similarly, if previous prophylaxis with mefloquine has failed, Mefloquine Hydrochloride Tablets should not be used for curative treatment.
- Note: Patients with acute P. vivax malaria, treated with Mefloquine Hydrochloride Tablets, are at high risk of relapse because Mefloquine Hydrochloride Tablets do not eliminate exoerythrocytic (hepatic phase) parasites. To avoid relapse after initial treatment of the acute infection with Mefloquine Hydrochloride Tablets, patients should subsequently be treated with an 8-aminoquinoline derivative (e.g., primaquine).
Malaria Prophylaxis
One 250 mg Mefloquine Hydrochloride Tablet once weekly.
Prophylactic drug administration should begin 1 week before arrival in an endemic area. Subsequent weekly doses should be taken regularly, always on the same day of each week, preferably after the main meal. To reduce the risk of malaria after leaving an endemic area, prophylaxis must be continued for 4 additional weeks to ensure suppressive blood levels of the drug when merozoites emerge from the liver. Tablets should not be taken on an empty stomach and should be administered with at least 8 oz (240 mL) of water.
In certain cases, e.g., when a traveler is taking other medication, it may be desirable to start prophylaxis 2 to 3 weeks prior to departure, in order to ensure that the combination of drugs is well tolerated (see PRECAUTIONS: Drug Interactions).
When prophylaxis with Mefloquine Hydrochloride Tablets fails, physicians should carefully evaluate which antimalarial to use for therapy.
Pediatric Patients
Treatment of mild to moderate malaria in pediatric patients caused by mefloquine-susceptible strains of P. falciparum
Twenty (20) to 25 mg/kg body weight. Splitting the total therapeutic dose into 2 doses taken 6 to 8 hours apart may reduce the occurrence or severity of adverse effects. Experience with Mefloquine Hydrochloride Tablets in pediatric patients weighing less than 20 kg is limited. The drug should not be taken on an empty stomach and should be administered with ample water. The tablets may be crushed and suspended in a small amount of water, milk or other beverage for administration to small children and other persons unable to swallow them whole.
If a full-treatment course with Mefloquine Hydrochloride Tablets does not lead to improvement within 48 to 72 hours, Mefloquine Hydrochloride Tablets should not be used for retreatment. An alternative therapy should be used. Similarly, if previous prophylaxis with mefloquine has failed, Mefloquine Hydrochloride Tablets should not be used for curative treatment.
In pediatric patients, the administration of Mefloquine Hydrochloride Tablets for the treatment of malaria has been associated with early vomiting. In some cases, early vomiting has been cited as a possible cause of treatment failure (see PRECAUTIONS). If a significant loss of drug product is observed or suspected because of vomiting, a second full dose of Mefloquine Hydrochloride Tablets should be administered to patients who vomit less than 30 minutes after receiving the drug. If vomiting occurs 30 to 60 minutes after a dose, an additional half-dose should be given. If vomiting recurs, the patient should be monitored closely and alternative malaria treatment considered if improvement is not observed within a reasonable period of time.
The safety and effectiveness of Mefloquine Hydrochloride Tablets to treat malaria in pediatric patients below the age of 6 months have not been established.
Malaria Prophylaxis
The recommended prophylactic dose of Mefloquine Hydrochloride Tablets is approximately 5 mg/kg body weight once weekly. One 250 mg Mefloquine Hydrochloride Tablet should be taken once weekly in pediatric patients weighing over 45 kg. In pediatric patients weighing less than 45 kg, the weekly dose decreases in proportion to body weight:
30 to 45 kg: 3/4 tablet
20 to 30 kg: 1/2 tabletExperience with Mefloquine Hydrochloride Tablets in pediatric patients weighing less than 20 kg is limited.
- HOW SUPPLIED
-
ANIMAL TOXICOLOGY
Ocular lesions were observed in rats fed mefloquine daily for 2 years. All surviving rats given 30 mg/kg/day had ocular lesions in both eyes characterized by retinal degeneration, opacity of the lens, and retinal edema. Similar but less severe lesions were observed in 80% of female and 22% of male rats fed 12.5 mg/kg/day for 2 years. At doses of 5 mg/kg/day, only corneal lesions were observed. They occurred in 9% of rats studied.
Revised 07/11
-
MEDICATION GUIDE
Read this entire Medication Guide before you start taking Mefloquine Hydrochloride Tablets and each time you get a refill. There may be new information. This information does not take the place of talking to your doctor about your medical condition or your treatment.
What is the most important information I should know about Mefloquine Hydrochloride Tablets?
Your doctor or pharmacist will give you an Information Wallet Card along with this Medication Guide. It has important information about Mefloquine Hydrochloride Tablets and should be carried with you at all times while you take Mefloquine Hydrochloride Tablets.
Mefloquine Hydrochloride Tablets can cause serious mental problems.
- Some people who take mefloquine have sudden serious mental problems, including:
- severe anxiety
- paranoia (feelings of mistrust towards others)
- hallucinations (seeing or hearing things that are not there)
- depression
- feeling restless
- unusual behavior
- feeling confused
In some patients these serious side effects can go on after Mefloquine is stopped.
- Some people who take Mefloquine Hydrochloride Tablets think about suicide (putting an end to their life). Some people who were taking Mefloquine Hydrochloride Tablets committed suicide. It is not known whether Mefloquine Hydrochloride Tablets were responsible for those suicides.
If you have any of these serious mental problems, or you develop other serious side effects or mental problems, you should call your doctor right away as it may be necessary to stop taking Mefloquine Hydrochloride Tablets and use another medicine to prevent malaria.
You need to take malaria prevention medicine before you travel to a malaria area, while you are in a malaria area, and after you return from a malaria area.
If you are told by a doctor to stop taking Mefloquine Hydrochloride Tablets because of the side effects or for other reasons, you will need to take another malaria medicine.
If you do not have access to a doctor or to another medicine and have to stop taking Mefloquine Hydrochloride Tablets, leave the malaria area and contact a doctor as soon as possible because leaving the malaria area may not protect you from getting malaria. You will still need to take a malaria prevention medicine for another 4 weeks.
- Do not take halofantrine (used to treat malaria) or ketoconazole (used for fungal infections) with Mefloquine Hydrochloride Tablets or within 15 weeks of your last dose of Mefloquine Hydrochloride Tablets. You may have serious heart problems that can lead to death. Do not take quinine (Qualaquin) or quinidine (used to treat malaria or irregular heart beat) with Mefloquine Hydrochloride Tablets. You may have serious heart problems.
- Do not take quinine (Qualaquin) or chloroquine (Aralen) (used to treat malaria) with Mefloquine Hydrochloride Tablets. You may have a greater risk for convulsions (seizures).
What are Mefloquine Hydrochloride Tablets?
Mefloquine Hydrochloride Tablets are a prescription medicine used to prevent and treat malaria. Malaria can be a life-threatening infection. Mefloquine does not work for all types of malaria.
It is not known if Mefloquine Hydrochloride Tablets are safe and effective in children under 6 months old for the treatment of malaria.
It is not known how well Mefloquine Hydrochloride Tablets work to prevent malaria in infants weighing less than 44 lbs (20 kg).
Who should not take Mefloquine Hydrochloride Tablets?
Do not take Mefloquine Hydrochloride Tablets if you have:
- depression or had depression recently
- had recent mental problems, including anxiety disorder, schizophrenia, or psychosis (losing touch with reality)
- seizures or had seizures (epilepsy or convulsions)
- an allergy to quinine, quinidine, mefloquine or any ingredients in mefloquine. See the end of this Medication Guide for a complete list of ingredients in mefloquine.
Talk to your doctor before you take Mefloquine Hydrochloride Tablets if you have any of the conditions listed above.
What should I tell my doctor before taking Mefloquine Hydrochloride Tablets?
Before taking Mefloquine Hydrochloride Tablets, tell your doctor about all your medical conditions, including if you have:
- heart disease
- liver problems
- seizures or epilepsy
- diabetes
- blood clotting problems or take blood thinner medicines (anticoagulants)
- mental problems
- are pregnant or plan to become pregnant. It is not known if mefloquine will harm your unborn baby. Talk to you doctor if you are pregnant or plan to become pregnant.
- use birth control while you take mefloquine and for 3 months after you stop mefloquine. If you have an unplanned pregnancy, talk to your doctor right away.
- are breast-feeding or plan to breast-feed. Mefloquine can pass through your milk and may harm your baby. Ask your doctor whether you will need to stop breast-feeding or use another medicine.
After leaving a malaria area, if you have a fever contact your doctor right away.
Tell your doctor about all the medicines you take, including prescription and nonprescription medicines, vitamins, and herbal supplements. Mefloquine Hydrochloride Tablets and other medicines may affect each other causing side effects.
Know the medicines you take. Keep a list of them and show it to your doctor and pharmacist when you get a new medicine.
Especially tell your doctor if you take:
- ketoconazole used to treat fungal infections
- halofantrine, quinine (Qualaquin), quinidine, chloroquine (Aralen) or other medicines used to treat malaria
- anti-arrhythmic medicines, beta-adrenergic blocking medicines and calcium channel blockers used to treat heart problems or high blood pressure
- antihistamines or H1-blocking agents used to treat allergies
- tricyclic antidepressants used to treat depression
- phenothiazines used to treat mental problems
- anticonvulsants used to treat seizures
- vaccines containing live bacteria. Your doctor may want you to finish receiving your vaccines at least 3 days before you start mefloquine.
- rifampin and rifampin-containing products (Rifadin, Rifamate, Rifater, Rimactane) used to treat infections
Ask your doctor or pharmacist for a list of these medicines if you are not sure.
How should I take Mefloquine Hydrochloride Tablets?
- Take Mefloquine Hydrochloride Tablets exactly as your doctor tells you to take it. Your doctor will tell you how many Mefloquine Hydrochloride Tablets to take and when to take them.
- You will start taking Mefloquine Hydrochloride Tablets to prevent malaria between 1 to 3 weeks before you travel to a malaria area.
- Take Mefloquine Hydrochloride Tablets just after eating your main meal and with at least one cup (8 ounces) of water.
- Do not take Mefloquine Hydrochloride Tablets on an empty stomach.
- If you vomit after taking Mefloquine Hydrochloride Tablets, call your healthcare provider to see if you should take another dose.
- Continue taking Mefloquine Hydrochloride Tablets for 4 weeks after returning from a malaria area.
- Mefloquine Hydrochloride Tablets may be crushed and mixed with a small amount of water, milk or other beverage for children or other people unable to swallow Mefloquine Hydrochloride Tablets whole. Your doctor will tell you the correct dose for your child based on your child’s weight.
- If you take Mefloquine Hydrochloride Tablets for a year or longer, your doctor should check your
- eyes, especially if you have trouble seeing while you take Mefloquine Hydrochloride Tablets
- liver function to see if there has been damage to your liver
- Use protective clothing, insect repellents, and bednets to protect you from being bitten by mosquitoes. Medicine alone does not always stop you from catching malaria from mosquito bites.
What should I avoid while taking Mefloquine Hydrochloride Tablets?
Avoid activities such as driving a car or using heavy machinery or other activities needing alertness and careful movements (fine motor coordination) until you know how mefloquine affects you. You may feel dizzy or lose your balance. This could happen for months after you stop taking mefloquine. See “What are the possible side effects of mefloquine?”
What are the possible side effects of Mefloquine Hydrochloride Tablets?
Also see “What is the most important information I should know about Mefloquine Hydrochloride Tablets?”
Mefloquine Hydrochloride Tablets may cause serious side effects, including:
- convulsions (seizures)
- liver problems
- heart problems
The most common side effects of Mefloquine Hydrochloride Tablets include:
- nausea
- vomiting
- diarrhea
- abdominal pain
- dizziness or loss of balance (vertigo), which may continue for months after mefloquine is stopped
- headache
- sleeping problems (sleepiness, unable to sleep, bad dreams)
The most common side effects in people who take Mefloquine Hydrochloride Tablets for treatment include:
- muscle pain
- fever
- chills
- skin rash
- fatigue
- loss of appetite
- ringing in the ears
- irregular heart beat
Tell your doctor if you have any side effect that bothers you or that does not go away. These are not all the possible side effects of Mefloquine Hydrochloride Tablets. For more information, ask your doctor or pharmacist.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
How should I store Mefloquine Hydrochloride Tablets?
- Store Mefloquine Hydrochloride Tablets between 59ºF to 86ºF (15ºC to 30ºC)
- Safely throw away medicine that is out of date or no longer needed.
Keep Mefloquine Hydrochloride Tablets and all medicines out of the reach of children.
General information about the safe and effective use of Mefloquine Hydrochloride Tablets.
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use Mefloquine Hydrochloride Tablets for a condition for which it was not prescribed. Do not give mefloquine to other people, even if they have the same symptoms that you have. It may harm them.
This Medication Guide summarizes the most important information about mefloquine. If you would like more information, talk with your doctor. You can ask your pharmacist or doctor for information about mefloquine that is written for health professionals.
If you have any questions or would like more information about Mefloquine Hydrochloride Tablets, you can call West-ward Pharmaceutical Corp., the manufacturer of Mefloquine Hydrochloride Tablets, at 1-877-233-2001.
What are the ingredients in Mefloquine Hydrochloride Tablets?
Active ingredients: mefloquine hydrochloride
Inactive ingredients: colloidal silicon dioxide, corn starch, crospovidone, lactose monohydrate, lactose spray dried, magnesium stearate, microcrystalline cellulose, polysorbate 80, polyvinylpyrrolidone and talc.
This Medication Guide has been approved by the U.S. Food and Drug Administration.
Information Wallet Card
Mefloquine Hydrochloride Tablets
It is important that you read the entire Medication Guide for additional
information on Mefloquine Hydrochloride Tablets.
Carry this wallet card with you when you are taking Mefloquine Hydrochloride Tablets.You need to take malaria prevention medicine before you travel to a malaria area, while you are in a malaria area, and after you return from a malaria area.
Mefloquine Hydrochloride Tablets can cause serious mental problems in some people. If you takeMefloquine Hydrochloride Tablets and you have sudden signs of serious mental problems (such as: severe anxiety, feelings of mistrust towards others, seeing or hearing things that are not there, depression, feeling restless, unusual behavior or feeling confused), you should contact a doctor right away as it may be necessary to stop taking Mefloquine Hydrochloride Tablets and take different medicine to prevent malaria.
Other side effects from Mefloquine Hydrochloride Tablets may include: convulsions, liver problems, and heart problems. The most common side effects of Mefloquine Hydrochloride Tablets include nausea, vomiting, diarrhea, abdominal pain, dizziness or loss of balance (vertigo) which may continue for months after Mefloquine Hydrochloride Tablets are stopped, headache, and sleeping problems (sleepiness, unable to sleep, bad dreams).
While you take Mefloquine Hydrochloride Tablets, do not take:
- Halofantrine (used to treat malaria)
- Ketoconazole (used for fungal infections)
- Quinine (Qualaquin) or quinidine (used to treat malaria or irregular heart beat)
- Chloroquine (Aralen) (used to treat malaria)
Avoid activities such as driving a car or using heavy machinery or other activities needing alertness and careful movements (fine motor coordination) until you know how Mefloquine Hydrochloride Tablets affect you.
Other medicines are approved in the United States for malaria prevention. However, not all malaria medicines work equally well in different malaria areas. Before you travel, talk to your doctor about your travel plans.
If you have any serious side effects, and cannot get another medicine, leave the malaria area and contact a doctor as soon as possible because leaving the malaria area may not protect you from getting malaria. You will still need to take a malaria prevention medicine.
Call your doctor for medical advice about side effects.
You may report side effects to FDA at 1-800-FDA-1088.
Card Revised: 03/10
Manufactured by:
West-ward Pharmaceutical Corp.
Eatontown, NJ 07724
Revised March 2010 - Some people who take mefloquine have sudden serious mental problems, including:
-
PRINCIPAL DISPLAY PANEL
Repacked by:H.J. Harkins Company, Inc.
Nipomo, CA 93444
NDC: 0143-1282-22
Mefloquine Hydrochloride Tablet 250 mg
-
INGREDIENTS AND APPEARANCE
MEFLOQUINE HYDROCHLORIDE
mefloquine hydrochloride tabletProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 52959-803(NDC: 0143-1282) Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength MEFLOQUINE HYDROCHLORIDE (UNII: 5Y9L3636O3) (MEFLOQUINE - UNII:TML814419R) MEFLOQUINE HYDROCHLORIDE 250 mg Inactive Ingredients Ingredient Name Strength COLLOIDAL SILICON DIOXIDE (UNII: ETJ7Z6XBU4) STARCH, CORN (UNII: O8232NY3SJ) CROSPOVIDONE (UNII: 68401960MK) LACTOSE MONOHYDRATE (UNII: EWQ57Q8I5X) MAGNESIUM STEARATE (UNII: 70097M6I30) CELLULOSE, MICROCRYSTALLINE (UNII: OP1R32D61U) POLYSORBATE 80 (UNII: 6OZP39ZG8H) POVIDONE K30 (UNII: U725QWY32X) TALC (UNII: 7SEV7J4R1U) Product Characteristics Color WHITE (white) Score 2 pieces Shape ROUND (round) Size 12mm Flavor Imprint Code WW282 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 52959-803-25 25 in 1 BOTTLE Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA077699 04/21/2010 Labeler - H.J. Harkins Company, Inc. (147681894) Establishment Name Address ID/FEI Business Operations West-ward Pharmaceutical Corp 001230762 MANUFACTURE
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.