BETAMETHASONE VALERATE ointment
Betamethasone Valerate by
Drug Labeling and Warnings
Betamethasone Valerate by is a Prescription medication manufactured, distributed, or labeled by Preferred Pharmaceuticals Inc.. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
- SPL UNCLASSIFIED SECTION
-
DESCRIPTION:
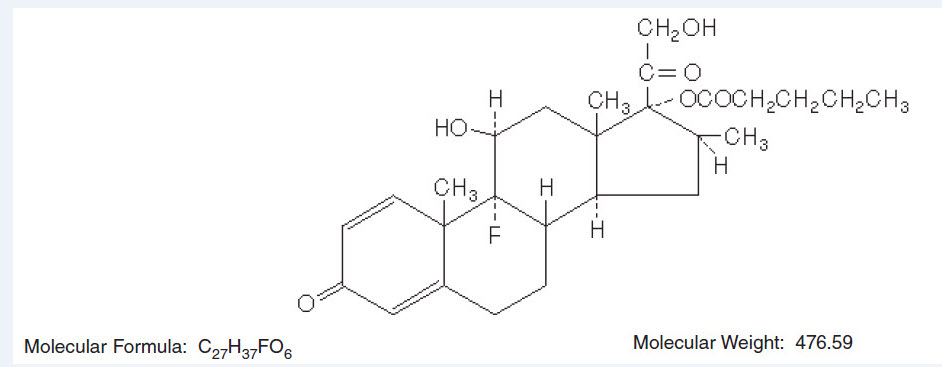
Betamethasone Valerate Cream, Ointment and Lotion contain betamethasone valerate USP, a synthetic adrenocorticosteroid for dermatologic use. Betamethasone, an analog of prednisolone, has a high degree of glucocorticoid activity and a slight degree of mineralocorticoid activity.
Betamethasone valerate is a white to practically white odorless crystalline powder practically insoluble in water, freely soluble in acetone and chloroform, soluble in alcohol, and slightly soluble in benzene and ether. Chemically, it is 9-fluoro-11β,17,21-trihydroxy-16β-methylpregna-1, 4-diene-3,20-dione 17-valerate. The structural formula is:
Each gram of the 0.1% Cream contains 1.2 mg betamethasone valerate (equivalent to 1 mg betamethasone) in a soft, white, hydrophilic cream of purified water, mineral oil, white petrolatum, polyethylene glycol 1000 monocetyl ether, cetostearyl alcohol, monobasic sodium phosphate and phosphoric acid or sodium hydroxide (to adjust pH, if required); chlorocresol is present as a preservative.
Each gram of the 0.1% Ointment contains 1.2 mg betamethasone valerate (equivalent to 1 mg betamethasone) in an ointment base of white petrolatum and mineral oil.
Each gram of the 0.1% Lotion contains 1.2 mg betamethasone valerate (equivalent to 1 mg betamethasone) in a vehicle of isopropyl alcohol and water slightly thickened with carbomer 934P. Sodium hydroxide is used to adjust pH.
-
CLINICAL PHARMACOLOGY:
Topical corticosteroids share anti-inflammatory, antipruritic and vasoconstrictive actions.
The mechanism of anti-inflammatory activity of the topical corticosteroids is unclear. Various laboratory methods, including vasoconstrictor assays, are used to compare and predict potencies and/or clinical efficacies of the topical corticosteroids. There is some evidence to suggest that a recognizable correlation exists between vasoconstrictor potency and therapeutic efficacy in man.
Pharmacokinetics: The extent of percutaneous absorption of topical corticosteroids is determined by many factors including the vehicle, the integrity of the epidermal barrier, and the use of occlusive dressings.
Topical corticosteroids can be absorbed from normal intact skin. Inflammation and/or other disease processes in the skin increase percutaneous absorption. Occlusive dressings substantially increase the percutaneous absorption of topical corticosteroids. Thus, occlusive dressings may be a valuable therapeutic adjunct for treatment of resistant dermatoses.
Once absorbed through the skin, topical corticosteroids are handled through pharmacokinetic pathways similar to systemically administered corticosteroids. Corticosteroids are bound to plasma proteins in varying degrees. Corticosteroids are metabolized primarily in the liver and are then excreted by the kidneys. Some of the topical corticosteroids and their metabolites are also excreted into the bile.
- INDICATIONS AND USAGE:
- CONTRAINDICATIONS:
-
PRECAUTIONS:
General: Systemic absorption of topical corticosteroids has produced reversible hypothalamic-pituitary-adrenal (HPA) axis suppression, manifestations of Cushing's syndrome, hyperglycemia, and glucosuria in some patients.
Conditions which augment systemic absorption include the application of the more potent steroids, use over large surface areas, prolonged use, and the addition of occlusive dressings.
Therefore, patients receiving a large dose of a potent topical steroid applied to a large surface area should be evaluated periodically for evidence of HPA axis suppression by using the urinary free cortisol and ACTH stimulation tests. If HPA axis suppression is noted, an attempt should be made to withdraw the drug, to reduce the frequency of application, or substitute to a less potent steroid.
Recovery of HPA axis function is generally prompt and complete upon discontinuation of the drug. Infrequently, signs and symptoms of steroid withdrawal may occur, requiring supplemental systemic corticosteroids.
Pediatric patients may absorb proportionally larger amounts of topical corticosteroids and thus be more susceptible to systemic toxicity (See PRECAUTIONS—Pediatric Use).
If irritation develops, topical corticosteroids should be discontinued and appropriate therapy instituted.
In the presence of dermatological infections, the use of an appropriate antifungal or antibacterial agent should be instituted. If a favorable response does not occur promptly, the corticosteroid should be discontinued until the infection has been adequately controlled.
Information for Patients: Patients using topical corticosteroids should receive the following information and instructions:
- 1. This medication is to be used as directed by the physician. It is for external use only. Avoid contact with the eyes.
- 2. Patients should be advised not to use this medication for any disorder other than that for which it was prescribed.
- 3. The treated skin area should not be bandaged or otherwise covered or wrapped as to be occlusive unless directed by the physician.
- 4. Patients should report any signs of local adverse reactions especially under occlusive dressing.
- 5. Parents of pediatric patients should be advised not to use tight-fitting diapers or plastic pants on a child being treated in the diaper area, as these garments may constitute occlusive dressings.
Laboratory tests: The following tests may be helpful in evaluating the HPA axis suppression:
- Urinary free cortisol test
- ACTH stimulation test
Carcinogenesis, Mutagenesis and Impairment of Fertility: Long-term animal studies have not been performed to evaluate the carcinogenic potential or the effect on fertility of topical corticosteroids.
Studies to determine mutagenicity with prednisolone and hydrocortisone have revealed negative results.
Pregnancy: Teratogenic Effects — Pregnancy Category C. Corticosteroids are generally teratogenic in laboratory animals when administered systemically at relatively low dosage levels. The more potent corticosteroids have been shown to be teratogenic after dermal application in laboratory animals. There are no adequate and well-controlled studies in pregnant women on teratogenic effects from topically applied corticosteroids. Therefore, topical corticosteroids should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. Drugs of this class should not be used extensively on pregnant patients, in large amounts, or for prolonged periods of time.
Nursing Mothers: It is not known whether topical administration of corticosteroids could result in sufficient systemic absorption to produce detectable quantities in breast milk. Systemically administered corticosteroids are secreted into breast milk in quantities not likely to have a deleterious effect on the infant. Nevertheless, caution should be exercised when topical corticosteroids are administered to a nursing woman.
Pediatric Use: Pediatric patients may demonstrate greater susceptibility to topical corticosteroid-induced HPA axis suppression and Cushing's syndrome than mature patients because of a larger skin surface area to body weight ratio.
Hypothalamic-pituitary-adrenal (HPA) axis suppression, Cushing's syndrome, and intracranial hypertension have been reported in children receiving topical corticosteroids. Manifestations of adrenal suppression in children include linear growth retardation, delayed weight gain, low plasma cortisol levels, and absence of response to ACTH stimulation. Manifestations of intracranial hypertension include bulging fontanelles, headaches, and bilateral papilledema.
Administration of topical corticosteroids to pediatric patients should be limited to the least amount compatible with an effective therapeutic regimen. Chronic corticosteroid therapy may interfere with the growth and development of children.
-
ADVERSE REACTIONS:
The following local adverse reactions are reported infrequently with topical corticosteroids, but may occur more frequently with the use of occlusive dressings. These reactions are listed in an approximate decreasing order of occurrence: burning, itching, irritation, dryness, folliculitis, hypertrichosis, acneiform eruptions, hypopigmentation, perioral dermatitis, allergic contact dermatitis, maceration of the skin, secondary infection, skin atrophy, striae and miliaria.
-
OVERDOSAGE:
Topically applied corticosteroids can be absorbed in sufficient amounts to produce systemic effects (See PRECAUTIONS).
-
DOSAGE AND ADMINISTRATION:
Apply a thin film of Betamethasone Valerate Cream or Ointment to the affected skin areas one to three times a day. Dosage once or twice a day is often effective.
Apply a few drops of Betamethasone Valerate Lotion to the affected area and massage lightly until it disappears. Apply twice daily, in the morning and at night. Dosage may be increased in stubborn cases. Following improvement, apply once daily. For the most effective and economical use, apply nozzle very close to affected area and gently squeeze bottle.
-
HOW SUPPLIED:
Betamethasone Valerate
Ointment USP, 0.1%
is supplied as follows:
15 g tubes NDC: 68788-7095-1
45 g tubes NDC: 68788-7095-4
Store at room temperature 15° - 30°C (59° - 86°F) [see USP Controlled Room Temperature].
E. FOUGERA & CO.
A division of
Fougera
PHARMACEUTICALS INC.
Melville, NY 11747I240F
R07/13
#57
Relabeled By: Preferred Pharmaceuticals Inc. - PACKAGE LABEL – PRINCIPAL DISPLAY PANEL – 15 GRAM CONTAINER
-
INGREDIENTS AND APPEARANCE
BETAMETHASONE VALERATE
betamethasone valerate ointmentProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 68788-7095(NDC:0168-0033) Route of Administration TOPICAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength BETAMETHASONE VALERATE (UNII: 9IFA5XM7R2) (BETAMETHASONE - UNII:9842X06Q6M) BETAMETHASONE 1 mg in 1 g Inactive Ingredients Ingredient Name Strength MINERAL OIL (UNII: T5L8T28FGP) PETROLATUM (UNII: 4T6H12BN9U) Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 68788-7095-1 15 g in 1 TUBE; Type 0: Not a Combination Product 02/12/2018 2 NDC: 68788-7095-4 45 g in 1 TUBE; Type 0: Not a Combination Product 02/12/2018 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA018865 02/12/2018 Labeler - Preferred Pharmaceuticals Inc. (791119022) Registrant - Preferred Pharmaceuticals Inc. (791119022) Establishment Name Address ID/FEI Business Operations Preferred Pharmaceuticals Inc. 791119022 RELABEL(68788-7095)
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.