AZITHROMYCIN DIHYDRATE- azithromycin tablet, film coated
Azithromycin Dihydrate by
Drug Labeling and Warnings
Azithromycin Dihydrate by is a Prescription medication manufactured, distributed, or labeled by Cambridge Therapeutics Technologies, LLC. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use AZITHROMYCIN TABLETS safely and effectively. See full prescribing information for AZITHROMYCIN TABLETS.
AZITHROMYCIN tablets, for oral use
Initial U.S. Approval: 1991RECENT MAJOR CHANGES
None
INDICATIONS AND USAGE
Azithromycin is a macrolide antibacterial drug indicated for mild to moderate infections caused by designated, susceptible bacteria:
-
Acute bacterial exacerbations of chronic bronchitis in adults (1.1)
-
Acute bacterial sinusitis in adults (1.1)
-
Uncomplicated skin and skin structure infections in adults (1.1)
-
Urethritis and cervicitis in adults (1.1)
-
Genital ulcer disease in men (1.1)
-
Acute otitis media in pediatric patients (1.2)
-
Community-acquired pneumonia in adults and pediatric patients (1.1, 1.2)
-
Pharyngitis/tonsillitis in adults and pediatric patients (1.1, 1.2)
Limitation of Use:
Azithromycin should not be used in patients with pneumonia who are judged to be inappropriate for oral therapy because of moderate to severe illness or risk factors. (1.3)
To reduce the development of drug-resistant bacteria and maintain the effectiveness of azithromycin and other antibacterial drugs, azithromycin should be used only to treat infections that are proven or strongly suspected to be caused by susceptible bacteria.
DOSAGE AND ADMINISTRATION
- Adult Patients
Infection Recommended Dose/Duration of Therapy Community-acquired pneumonia (mild severity)
Pharyngitis/tonsillitis (second-line therapy)
Skin/skin structure (uncomplicated)500 mg as a single dose on Day 1, followed by 250 mg once daily on Days 2 through 5. Acute bacterial exacerbations of chronic bronchitis (mild to moderate) 500 mg as a single dose on Day 1, followed by 250 mg once daily on Days 2 through 5 or 500 mg once daily for 3 days. Acute bacterial sinusitis 500 mg once daily for 3 days. Genital ulcer disease (chancroid) Non-gonococcal urethritis and cervicitis One single 1 gram dose. Gonococcal urethritis and cervicitis One single 2 gram dose. - Pediatric Patients
Infection Recommended Dose/Duration of Therapy Acute otitis media 30 mg/kg as a single dose or 10 mg/kg once daily for 3 days or 10 mg/kg as a single dose on Day 1 followed by 5 mg/kg/day on Days 2 through 5. Acute bacterial sinusitis 10 mg/kg once daily for 3 days. Community-acquired pneumonia 10 mg/kg as a single dose on Day 1 followed by 5 mg/kg once daily on Days 2 through 5. Pharyngitis/tonsillitis 12 mg/kg once daily for 5 days. DOSAGE FORMS AND STRENGTHS
-
Azithromycin tablets, USP 250 mg and 500 mg (3)
CONTRAINDICATIONS
WARNINGS AND PRECAUTIONS
- Serious (including fatal) allergic and skin reactions: Discontinue azithromycin if reaction occurs. (5.1)
- Hepatotoxicity: Severe, and sometimes fatal, hepatotoxicity has been reported, Discontinue azithromycin immediately if signs and symptoms of hepatitis occur. (5.2)
- Prolongation of QT interval and cases of torsades de pointes have been reported. This risk which can be fatal should be considered in patients with certain cardiovascular disorders including known QT prolongation or history torsades de pointes, those with proarrhythmic conditions, and with other drugs that prolong the QT interval. (5.3)
-
Clostridium difficile-associated diarrhea: Evaluate patients if diarrhea occurs. (5.4)
-
Azithromycin may exacerbate muscle weakness in persons with myasthenia gravis. (5.5)
ADVERSE REACTIONS
Most common adverse reactions are diarrhea (5 to 14%), nausea (3 to 18%), abdominal pain (3 to 7%), or vomiting (2 to 7%). (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Cambridge Therapeutic Technologies, LLC at 1-844-810-0004 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
USE IN SPECIFIC POPULATIONS
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.
Revised: 1/2017
-
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
1.1 Adult Patients
1.2 Pediatric Patients
1.3 Limitations of Use
2 DOSAGE AND ADMINISTRATION
2.1 Adult Patients
2.2 Pediatric Patients1
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
4.1 Hypersensitivity
4.2 Hepatic Dysfunction
5 WARNINGS AND PRECAUTIONS
5.1 Hypersensitivity
5.2 Hepatotoxicity
5.3 QT Prolongation
5.4 Clostridium difficile-Associated Diarrhea (CDAD)
5.5 Exacerbation of Myasthenia Gravis
5.6 Use in Sexually Transmitted Infections
5.7 Development of Drug-Resistant Bacteria
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
6.2 Postmarketing Experience
6.3 Laboratory Abnormalities
7 DRUG INTERACTIONS
7.1 Nelfinavir
7.2 Warfarin
7.3 Potential Drug-Drug Interactions with Macrolides
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.3 Nursing Mothers
8.4 Pediatric Use
8.5 Geriatric Use
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
12.4 Microbiology
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
13.2 Animal Toxicology and/or Pharmacology
14 CLINICAL STUDIES
14.1 Adult Patients
14.2 Pediatric Patients
15 REFERENCES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
17.1 General Patient Counseling
17.2 See FDA-approved Patient Labeling
- * Sections or subsections omitted from the full prescribing information are not listed.
-
1 INDICATIONS AND USAGE
To reduce the development of drug-resistant bacteria and maintain the effectiveness of azithromycin and other antibacterial drugs, azithromycin should be used only to treat infections that are proven or strongly suspected to be caused by susceptible bacteria. When culture and susceptibility information are available, they should be considered in selecting or modifying antibacterial therapy. In the absence of such data, local epidemiology and susceptibility patterns may contribute to the empiric selection of therapy.
Azithromycin tablets, are a macrolide antibacterial drug indicated for the treatment of patients with mild to moderate infections caused by susceptible strains of the designated microorganisms in the specific conditions listed below. Recommended dosages and durations of therapy in adult and pediatric patient populations vary in these indications [see Dosage and Administration (2)].
1.1 Adult Patients
- Acute bacterial exacerbations of chronic bronchitis due to Haemophilus influenzae, Moraxella catarrhalis, or Streptococcus pneumoniae.
- Acute bacterial sinusitis due to Haemophilus influenzae, Moraxella catarrhalis or Streptococcus pneumoniae.
- Community-acquired pneumonia due to Chlamydophila pneumoniae, Haemophilus influenzae, Mycoplasma pneumoniae, or Streptococcus pneumoniae in patients appropriate for oral therapy.
- Pharyngitis/tonsillitis caused by Streptococcus pyogenes as an alternative to first-line therapy in individuals who cannot use first-line therapy.
- Uncomplicated skin and skin structure infections due to Staphylococcus aureus, Streptococcus pyogenes, or Streptococcus agalactiae.
- Urethritis and cervicitis due to Chlamydia trachomatis or Neisseria gonorrhoeae.
- Genital ulcer disease in men due to Haemophilus ducreyi (chancroid). Due to the small number of women included in clinical trials, the efficacy of azithromycin in the treatment of chancroid in women has not been established.
1.2 Pediatric Patients
[see Use in Specific Populations (8.4) and Clinical Studies (14.2)]
-
Acute otitis media (>6 months of age) caused by Haemophilus influenzae, Moraxella catarrhalis, or Streptococcus pneumoniae
-
Community-acquired pneumonia (>6 months of age) due to Chlamydophila pneumoniae, Haemophilus influenzae, Mycoplasma pneumonia, or Streptococcus pneumoniae in patients appropriate for oral therapy.
-
Pharyngitis/tonsillitis (>2 years of age) caused by Streptococcus pyogenes as an alternative to first-line therapy in individuals who cannot use first-line therapy.
1.3 Limitations of Use
Azithromycin should not be used in patients with pneumonia who are judged to be inappropriate for oral therapy because of moderate to severe illness or risk factors such as any of the following:
-
patients with cystic fibrosis,
-
patients with nosocomial infections,
-
patients with known or suspected bacteremia,
-
patients requiring hospitalization,
-
elderly or debilitated patients, or
-
patients with significant underlying health problems that may compromise their ability to respond to their illness (including immunodeficiency or functional asplenia).
-
2 DOSAGE AND ADMINISTRATION
2.1 Adult Patients
[see Indications and Usage (1.1) and Clinical Pharmacology (12.3)]
Infection* Recommended Dose/Duration of Therapy Community-acquired pneumonia
Pharyngitis/tonsillitis (second-line therapy)
Skin/skin structure (uncomplicated)500 mg as a single-dose on Day 1, followed by
250 mg once daily on Days 2 through 5Acute bacterial exacerbations of chronic obstructive pulmonary disease 500 mg once daily for 3 days
OR
500 mg as a single dose on Day 1, followed by 250 mg once daily on Days 2 through 5Acute bacterial sinusitis 500 mg once daily for 3 days Genital ulcer disease (chancroid) One single 1 gram dose Non-gonococcal urethritis and cervicitis One single 1 gram dose Gonococcal urethritis and cervicitis One single 2 gram dose *DUE TO THE INDICATED ORGANISMS [see Indications and Usage (1.1)] Azithromycin tablets can be taken with or without food.
2.2 Pediatric Patients1
Infection* Recommended Dose/Duration of Therapy Acute otitis media 30m mg/kg as a single dose or 10 mg/kg once daily
for 3 days or 10 mg/kg as a single dose on Day 1
followed by 5 mg/kg/day on Days 2 through 5.Acute bacterial sinusitis 10 mg/kg once daily for 3 days. Community-acquired pneumonia 10 mg/kg as a single dose on Day 1 followed by
5 mg/kg once daily on Days 2 through 5.Pharyngitis/tonsillitis 12 mg/kg once daily for 5 days. *DUE TO THE INDICATED ORGANISMS[see Indications and Usage (1.2)]
1see dosing tables below for maximum doses evaluated by indicationAzithromycin for oral suspension can be taken with or without food.
PEDIATRIC DOSAGE GUIDELINES FOR OTITIS MEDIA, ACUTE BACTERIAL SINUSITIS, AND COMMUNITY- ACQUIRED PNEUMONIA
(Age 6 months and above, [see Use in Specific Populations (8.4)])
Based on Body WeightOTITIS MEDIA AND COMMUNITY-ACQUIRED PNEUMONIA: (5-Day Regimen)* Dosing Calculated on 10 mg/kg/day Day 1 and 5 mg/kg/day Days 2 to 5. Weight 100 mg/5 mL 200 mg/5 mL Total mL per
Treatment
CourseTotal mg per
Treatment
CourseKg Lbs. Day 1 Days 2 to 5 Day 1 Days 2 to 5 5 11 2.5 mL;
(½ tsp)1.25 mL;
(¼ tsp)7.5 mL 150 mg 10 22 5 mL;
(1tsp)2.5 mL;
(½ tsp)15 mL 300 mg 20 44 5 mL;
(1 tsp)2.5 mL;
(½ tsp)15 mL 600 mg 30 66 7.5 mL;
(1½ tsp)3.75 mL;
(¾ tsp)22.5 mL 900 mg 40 88 10 mL;
(2 tsp)5 mL;
(1 tsp)30 mL 1200 mg 50 and
above110 and
above12.5 mL;
(2½ tsp)6.25 mL;
(1¼ tsp)37.5 mL 1500 mg *Effectiveness of the 3-day or 1-day regimen in pediatric patients with community-acquired pneumonia has not been established.
OTITIS MEDIA AND ACUTE BACTERIAL SINUSITIS: (3-Day Regimen)* Dosing Calculated on 10 mg/kg/day Weight 100 mg/5 mL 200 mg/5 mL Total mL per
Treatment CourseTotal mg per
Treatment CourseKg Lbs. Days 1 to 3 Days 1 to 3 5 11 2.5 mL; (1/2 tsp) 7.5 mL 150 mg 10 22 5 mL; (1 tsp) 15 mL 300 mg 20 44 5 mL (1 tsp) 15 mL 600 mg 30 66 7.5 mL (1½ tsp) 22.5 mL 900 mg 40 88 10 mL (2 tsp) 30 mL 1200 mg 50 and
above110 and
above12.5 mL (2 ½ tsp)
37.5 mL 1500 mg *Effectiveness of the 5-day or 1-day regimen in pediatric patients with acute bacterial sinusitis has not been established.
OTITIS MEDIA: (1-Day Regimen) Dosing Calculated on 30 mg/kg as a single dose Weight 200 mg/5 mL Total mL per
Treatment CourseTotal mg per
Treatment CourseKg Lbs. 1-Day Regimen 5 11 3.75 mL;(3/4 tsp) 3.75 mL 150 mg 10 22 7.5 mL;(1½ tsp) 7.5 mL 300mg 20 44 15 mL;(3 tsp)
15 mL 600 mg 30 66 22.5 mL;(4½ tsp)
22.5 mL 900 mg 40 88 30 mL;(6 tsp)
30 mL 1200 mg 50 and above 110 and above 37.5 mL;(7½ tsp)
37.5 mL 1500 mg The safety of re-dosing azithromycin in pediatric patients who vomit after receiving 30 mg/kg as a single dose has not been established. In clinical studies involving 487 patients with acute otitis media given a single 30 mg/kg dose of azithromycin, eight patients who vomited within 30 minutes of dosing were re-dosed at the same total dose.
Pharyngitis/Tonsillitis
The recommended dose of azithromycin for children with pharyngitis/tonsillitis is 12 mg/kg once daily for 5 days. (See chart below).PEDIATRIC DOSAGE GUIDELINES FOR PHARYNGITIS/TONSILLITIS
(Age 2 years and above, [see Use in Specific Populations (8.4)])
Based on Body WeightPHARYNGITIS/TONSILLITIS: (5-Day Regimen) Dosing Calculated on 12 mg/kg/day for 5 days Weight 200 mg/5 mL Total mL per
Treatment CourseTotal mg per
Treatment CourseKg Lbs. Day 1 to 5 8 18 2.5 mL; (½ tsp) 12.5 mL 500 mg 17 37 5 mL; (1 tsp)
25 mL 1000 mg 25 55 7.5 mL; (1½ tsp)
37.5 mL 1500 mg 33 73 10 mL; (2 tsp)
50 mL 2000 mg 40 88 12.5 mL; (2½ tsp) 62.5 mL 2500 mg - 3 DOSAGE FORMS AND STRENGTHS
- 4 CONTRAINDICATIONS
-
5 WARNINGS AND PRECAUTIONS
5.1 Hypersensitivity
Serious allergic reactions, including angioedema, anaphylaxis, and dermatologic reactions including Stevens-Johnson syndrome, and toxic epidermal necrolysis have been reported in patients on azithromycin therapy [see Contraindications (4.1)].
Fatalities have been reported. Cases of Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) have also been reported. Despite initially successful symptomatic treatment of the allergic symptoms, when symptomatic therapy was discontinued, the allergic symptoms recurred soon thereafter in some patients without further azithromycin exposure. These patients required prolonged periods of observation and symptomatic treatment. The relationship of these episodes to the long tissue half-life of azithromycin and subsequent prolonged exposure to antigen is presently unknown.
If an allergic reaction occurs, the drug should be discontinued and appropriate therapy should be instituted. Physicians should be aware that allergic symptoms may reappear when symptomatic therapy has been discontinued.
5.2 Hepatotoxicity
Abnormal liver function, hepatitis, cholestatic jaundice, hepatic necrosis, and hepatic failure have been reported, some of which have resulted in death. Discontinue azithromycin immediately if signs and symptoms of hepatitis occur.
5.3 QT Prolongation
Prolonged cardiac repolarization and QT interval, imparting a risk of developing cardiac arrhythmia and torsades de pointes, have been seen with treatment with macrolides, including azithromycin. Cases of torsades de pointes have been spontaneously reported during postmarketing surveillance in patients receiving azithromycin. Providers should consider the risk of QT prolongation which can be fatal when weighing the risks and benefits of azithromycin for at-risk groups including:
-
patients with known prolongation of the QT interval, a history of torsades de pointes, congenital long QT syndrome, bradyarrhythmias or uncompensated heart failure
-
patients on drugs known to prolong the QT interval
-
patients with ongoing proarrhythmic conditions such as uncorrected hypokalemia or hypomagnesemia, clinically significant bradycardia, and in patients receiving Class IA (quinidine, procainamide) or Class III (dofetilide, amiodarone, sotalol) antiarrhythmic agents.
Elderly patients may be more susceptible to drug-associated effects on the QT interval.
5.4 Clostridium difficile-Associated Diarrhea (CDAD)
Clostridium difficile-associated diarrhea has been reported with use of nearly all antibacterial agents, including azithromycin, and may range in severity from mild diarrhea to fatal colitis. Treatment with antibacterial agents alters the normal flora of the colon, leading to overgrowth of C. difficile.
C. difficile produces toxins A and B which contribute to the development of CDAD. Hypertoxin producing strains of C. difficile cause increased morbidity and mortality, as these infections can be refractory to antibacterial therapy and may require colectomy. CDAD must be considered in all patients who present with diarrhea following antibiotic use. Careful medical history is necessary since CDAD has been reported to occur over two months after the administration of antibacterial agents.
If CDAD is suspected or confirmed, ongoing antibiotic use not directed against C. difficile may need to be discontinued. Appropriate fluid and electrolyte management, protein supplementation, antibiotic treatment of C. difficile, and surgical evaluation should be instituted as clinically indicated.
5.5 Exacerbation of Myasthenia Gravis
Exacerbation of symptoms of myasthenia gravis and new onset of myasthenic syndrome have been reported in patients receiving azithromycin therapy.
5.6 Use in Sexually Transmitted Infections
Azithromycin tablets, at the recommended dose, should not be relied upon to treat syphilis. Antibacterial agents used to treat non-gonococcal urethritis may mask or delay the symptoms of incubating syphilis. All patients with sexually transmitted urethritis or cervicitis should have a serologic test for syphilis and appropriate testing for gonorrhea performed at the time of diagnosis. Appropriate antibacterial therapy and follow-up tests for these diseases should be initiated if infection is confirmed.
-
-
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
In clinical trials, most of the reported side effects were mild to moderate in severity and were reversible upon discontinuation of the drug. Potentially serious adverse reactions of angioedema and cholestatic jaundice were reported. Approximately 0.7% of the patients (adults and pediatric patients) from the 5-day multiple-dose clinical trials discontinued azithromycin therapy because of treatment-related adverse reactions. In adults given 500 mg/day for 3 days, the discontinuation rate due to treatment-related adverse reactions was 0.6%. In clinical trials in pediatric patients given 30 mg/kg, either as a single dose or over 3 days, discontinuation from the trials due to treatment-related adverse reactions was approximately 1%. Most of the adverse reactions leading to discontinuation were related to the gastrointestinal tract, e.g., nausea, vomiting, diarrhea, or abdominal pain [see Clinical Studies (14.2)].
Adults
Multiple-dose regimens
Overall, the most common treatment-related adverse reactions in adult patients receiving multiple-dose regimens of azithromycin were related to the gastrointestinal system with diarrhea/loose stools (4 to 5%), nausea (3%), and abdominal pain (2 to 3%) being the most frequently reported.No other adverse reactions occurred in patients on the multiple-dose regimens of azithromycin with a frequency greater than 1%. Adverse reactions that occurred with a frequency of 1% or less included the following:
Cardiovascular
Palpitations, chest pain.Gastrointestinal
Dyspepsia, flatulence, vomiting, melena, and cholestatic jaundice.Genitourinary
Monilia, vaginitis, and nephritis.Nervous System
Dizziness, headache, vertigo, and somnolence.General
Fatigue.Allergic
Rash, pruritus, photosensitivity, and angioedema.Single 1-gram dose regimen
Overall, the most common adverse reactions in patients receiving a single-dose regimen of 1 gram of azithromycin were related to the gastrointestinal system and were more frequently reported than in patients receiving the multiple-dose regimen.Adverse reactions that occurred in patients on the single 1-gram dosing regimen of azithromycin with a frequency of 1% or greater included diarrhea/loose stools (7%), nausea (5%), abdominal pain (5%), vomiting (2%), dyspepsia (1%), and vaginitis (1%).
Single 2-gram dose regimen
Overall, the most common adverse reactions in patients receiving a single 2-gram dose of azithromycin were related to the gastrointestinal system. Adverse reactions that occurred in patients in this study with a frequency of 1% or greater included nausea (18%), diarrhea/loose stools (14%), vomiting (7%), abdominal pain (7%), vaginitis (2%), dyspepsia (1%), and dizziness (1%). The majority of these complaints were mild in nature.Pediatric Patients
Single and Multiple-dose regimens: The types of adverse reactions in pediatric patients were comparable to those seen in adults, with different incidence rates for the dosage regimens recommended in pediatric patients.Acute Otitis Media
For the recommended total dosage regimen of 30 mg/kg, the most frequent adverse reactions (≥1%) attributed to treatment were diarrhea, abdominal pain, vomiting, nausea, and rash [see Dosage and Administration (2) and Clinical Studies (14.2)].The incidence, based on dosing regimen, is described in the table below:
Dosage Regimen Diarrhea % Abdominal Pain % Vomiting % Nausea % Rash % 1-day 4.3 % 1.4 % 4.9 % 1.0 % 1.0 % 3-day 2.6 % 1.7 % 2.3 % 0.4 % 0.6 % 5-day 1.8 % 1.2 % 1.1 % 0.5 % 0.4 % Community-Acquired Pneumonia
For the recommended dosage regimen of 10 mg/kg on Day 1 followed by 5 mg/kg on Days 2 to 5, the most frequent adverse reactions attributed to treatment were diarrhea/loose stools, abdominal pain, vomiting, nausea, and rash.The incidence is described in the table below:
Dosage Regimen Diarrhea/Loose stools % Abdominal Pain % Vomiting % Nausea % Rash % 5-day 5.8 % 1.9 % 1.9 % 1.9 % 1.6 % Pharyngitis/Tonsillitis
For the recommended dosage regimen of 12 mg/kg on Days 1 to 5, the most frequent adverse reactions attributed to treatment were diarrhea, vomiting, abdominal pain, nausea, and headache.The incidence is described in the table below:
Dosage Regimen Diarrhea % Abdominal Pain % Vomiting % Nausea % Rash % Headache % 5-day 5.4 % 3.4 % 5.6 % 1.8 % 0.7 % 1.1 % With any of the treatment regimens, no other adverse reactions occurred in pediatric patients treated with azithromycin with a frequency greater than 1%. Adverse reactions that occurred with a frequency of 1% or less included the following:
Cardiovascular
Chest pain.Gastrointestinal
Dyspepsia, constipation, anorexia, enteritis, flatulence, gastritis, jaundice, loose stools, and oral moniliasis.Hematologic and Lymphatic
Anemia and leukopenia.Nervous System
Headache (otitis media dosage), hyperkinesia, dizziness, agitation, nervousness, and insomnia.General
Fever, face edema, fatigue, fungal infection, malaise, and pain.Allergic
Rash and allergic reaction.Respiratory
Cough, pharyngitis, pleural effusion, and rhinitis.Skin and Appendages
Eczema, fungal dermatitis, pruritus, sweating, urticaria, and vesiculobullous rash.Special Senses
Conjunctivitis.6.2 Postmarketing Experience
The following adverse reactions have been identified during post-approval use of azithromycin. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Adverse reactions reported with azithromycin during the postmarketing period in adult and/or pediatric patients for which a causal relationship may not be established include:
Allergic
Arthralgia, edema, urticaria, and angioedema.Cardiovascular
Arrhythmias including ventricular tachycardia and hypotension. There have been reports of QT prolongation and torsades de pointes.Gastrointestinal
Anorexia, constipation, dyspepsia, flatulence, vomiting/diarrhea, pseudomembranous colitis, pancreatitis, oral candidiasis, pyloric stenosis, and reports of tongue discoloration.General
Asthenia, paresthesia, fatigue, malaise, and anaphylaxis.Genitourinary
Interstitial nephritis and acute renal failure and vaginitis.Hematopoietic
Thrombocytopenia.Liver/Biliary
Abnormal liver function, hepatitis, cholestatic jaundice, hepatic necrosis, and hepatic failure [see Warnings and Precautions (5.2)].Nervous System
Convulsions, dizziness/vertigo, headache, somnolence, hyperactivity, nervousness, agitation, and syncope.Psychiatric
Aggressive reaction and anxiety.Skin/Appendages
Pruritus, serious skin reactions including erythema multiforme, Stevens-Johnson Syndrome, toxic epidermal necrolysis, and DRESS.Special Senses
Hearing disturbances including hearing loss, deafness and/or tinnitus, and reports of taste/smell perversion and/or loss.6.3 Laboratory Abnormalities
Adults
Clinically significant abnormalities (irrespective of drug relationship) occurring during the clinical trials were reported as follows: with an incidence of greater than 1%: decreased hemoglobin, hematocrit, lymphocytes, neutrophils, and blood glucose; elevated serum creatine phosphokinase, potassium, ALT, GGT, AST, BUN, creatinine, blood glucose, platelet count, lymphocytes, neutrophils, and eosinophils; with an incidence of less than 1%: leukopenia, neutropenia, decreased sodium, potassium, platelet count, elevated monocytes, basophils, bicarbonate, serum alkaline phosphatase, bilirubin, LDH, and phosphate. The majority of subjects with elevated serum creatinine also had abnormal values at baseline. When follow-up was provided, changes in laboratory tests appeared to be reversible.In multiple-dose clinical trials involving more than 5,000 patients, four patients discontinued therapy because of treatment-related liver enzyme abnormalities and one because of a renal function abnormality.
Pediatric Patients
One, Three, and Five Day Regimens
Laboratory data collected from comparative clinical trials employing two 3-day regimens (30 mg/kg or 60 mg/kg in divided doses over 3 days), or two 5-day regimens (30 mg/kg or 60 mg/kg in divided doses over 5 days) were similar for regimens of azithromycin and all comparators combined, with most clinically significant laboratory abnormalities occurring at incidences of 1 to 5%. Laboratory data for patients receiving 30 mg/kg as a single dose were collected in one single center trial. In that trial, an absolute neutrophil count between 500 to 1,500 cells/mm3 was observed in 10/64 patients receiving 30 mg/kg as a single dose, 9/62 patients receiving 30 mg/kg given over 3 days, and 8/63 comparator patients. No patient had an absolute neutrophil count <500 cells/mm3.In multiple-dose clinical trials involving approximately 4,700 pediatric patients, no patients discontinued therapy because of treatment-related laboratory abnormalities.
-
7 DRUG INTERACTIONS
7.1 Nelfinavir
Co-administration of nelfinavir at steady-state with a single oral dose of azithromycin resulted in increased azithromycin serum concentrations. Although a dose adjustment of azithromycin is not recommended when administered in combination with nelfinavir, close monitoring for known adverse reactions of azithromycin, such as liver enzyme abnormalities and hearing impairment, is warranted [see Adverse Reactions (6)].
7.2 Warfarin
Spontaneous postmarketing reports suggest that concomitant administration of azithromycin may potentiate the effects of oral anticoagulants such as warfarin, although the prothrombin time was not affected in the dedicated drug interaction study with azithromycin and warfarin. Prothrombin times should be carefully monitored while patients are receiving azithromycin and oral anticoagulants concomitantly.
7.3 Potential Drug-Drug Interactions with Macrolides
Interactions with digoxin or phenytoin have not been reported in clinical trials with azithromycin; however, no specific drug interaction studies have been performed to evaluate potential drug-drug interactions. However, drug interactions have been observed with other macrolide products. Until further data are developed regarding drug interactions when digoxin or phenytoin are used concomitantly with azithromycin careful monitoring of patients is advised.
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Teratogenic Effects
Pregnancy Category B
Reproduction studies have been performed in rats and mice at doses up to moderately maternally toxic dose concentrations (i.e., 200 mg/kg/day). These daily doses in rats and mice, based on body surface area, are estimated to be 4 and 2 times, respectively, an adult daily dose of 500 mg. In the animal studies, no evidence of harm to the fetus due to azithromycin was found. There are, however, no adequate and well-controlled studies in pregnant women. Because animal reproduction studies are not always predictive of human response, azithromycin should be used during pregnancy only if clearly needed.8.3 Nursing Mothers
Azithromycin has been reported to be excreted in human breast milk in small amounts. Caution should be exercised when azithromycin is administered to a nursing woman.
8.4 Pediatric Use
[see Clinical Pharmacology (12.3), Indications and Usage (1.2), and Dosage and Administration (2.2)]
Safety and effectiveness in the treatment of pediatric patients with acute otitis media, acute bacterial sinusitis and community-acquired pneumonia under 6 months of age have not been established. Use of azithromycin for the treatment of acute bacterial sinusitis and community-acquired pneumonia in pediatric patients (6 months of age or greater) is supported by adequate and well-controlled trials in adults.
Pharyngitis/Tonsillitis
Safety and effectiveness in the treatment of pediatric patients with pharyngitis/tonsillitis under 2 years of age have not been established.8.5 Geriatric Use
In multiple-dose clinical trials of oral azithromycin, 9% of patients were at least 65 years of age (458/4949) and 3% of patients (144/4949) were at least 75 years of age. No overall differences in safety or effectiveness were observed between these subjects and younger subjects, and other reported clinical experience has not identified differences in response between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
Elderly patients may be more susceptible to development of torsades de pointes arrhythmias than younger patients [see Warnings and Precautions (5.3)].
- 10 OVERDOSAGE
-
11 DESCRIPTION
Azithromycin tablets, USP contain the active ingredient azithromycin, a macrolide antibacterial drug, for oral administration. Azithromycin has the chemical name (2R,3S,4R,5R,8R,10R,11R,12S,13S,14R)-13-[(2,6-dideoxy-3-C-methyl-3-O-methyl-α-L-ribo-hexopyranosyl) oxy]-2-ethyl-3,4,10-trihydroxy-3,5,6,8,10,12,14-heptamethyl-11-[[3,4,6-trideoxy-3- (dimethylamino)-β-D-xylo-hexopyranosyl]oxy]-1-oxa-6-azacyclopentadecan-15-one. Azithromycin is derived from erythromycin; however, it differs chemically from erythromycin in that a methyl-substituted nitrogen atom is incorporated into the lactone ring. Its molecular formula is C38H72N2O12, and its molecular weight is 749. Azithromycin has the following structural formula:
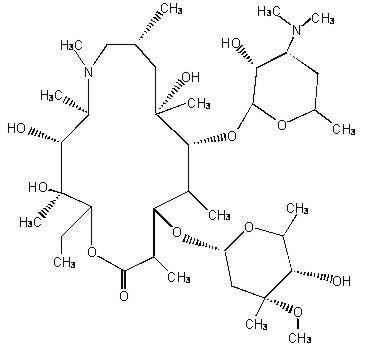
Azithromycin, as the dihydrate, is a white to almost white crystalline powder, with a molecular formula of C38H72N2O122H2O and a molecular weight of 785.02.
Azithromycin tablets, USP are supplied for oral administration as film-coated, white, oval, biconvex tablets containing azithromycin dihydrate equivalent to either 250 mg or 500 mg azithromycin and the following inactive ingredients: dibasic calcium phosphate dihydrate, hydroxypropyl cellulose, croscarmellose sodium, magnesium stearate and Opadry II white (Opadry II white contains the following components: hypromellose, lactose monohydrate, titanium dioxide and triacetin).
-
12 CLINICAL PHARMACOLOGY
12.2 Pharmacodynamics
Based on animal models of infection, the antibacterial activity of azithromycin appears to correlate with the ratio of area under the concentration-time curve to minimum inhibitory concentration (AUC/MIC) for certain pathogens (S. pneumoniae and S. aureus). The principal pharmacokinetic/pharmacodynamic parameter best associated with clinical and microbiological cure has not been elucidated in clinical trials with azithromycin.
Cardiac Electrophysiology
QTc interval prolongation was studied in a randomized, placebo-controlled parallel trial in 116 healthy subjects who received either chloroquine (1,000 mg) alone or in combination with oral azithromycin (500 mg, 1,000 mg, and 1,500 mg once daily). Co-administration of azithromycin increased the QTc interval in a dose- and concentration-dependent manner. In comparison to chloroquine alone, the maximum mean (95% upper confidence bound) increases in QTcF were 5 (10) ms, 7 (12) ms and 9 (14) ms with the co-administration of 500 mg, 1,000 mg and 1,500 mg azithromycin, respectively.12.3 Pharmacokinetics
Following oral administration of a single 500 mg dose (two 250 mg tablets) to 36 fasted healthy male volunteers, the mean (SD) pharmacokinetic parameters were AUC0-72 = 4.3 (1.2) mcg·hr/mL; Cmax=0.5 (0.2) mcg/mL; Tmax= 2.2 (0.9) hours. Two azithromycin 250 mg tablets are bioequivalent to a single 500 mg tablet.
In a two-way crossover study, 12 adult healthy volunteers (6 males, 6 females) received 1,500 mg of azithromycin administered in single daily doses over either 5 days (two 250 mg tablets on day 1, followed by one 250 mg tablet on days 2 to 5) or 3 days (500 mg per day for days 1 to 3). Due to limited serum samples on day 2 (3-day regimen) and days 2 to 4 (5-day regimen), the serum concentration-time profile of each subject was fit to a 3-compartment model and the AUC0-∞ for the fitted concentration profile was comparable between the 5-day and 3-day regimens.
3-Day Regimen 5-Day Regimen Pharmacokinetic Parameter [mean (SD)] Day 1 Day 3 Day 1 Day 5 Cmax (serum, mcg/mL) 0.44 (0.22) 0.54 (0.25) 0.43 (0.20) 0.24 (0.06) Serum AUC0-∞ (mcg·hr/mL) 17.4 (6.2)* 14.9 (3.1)* Serum T1/2 71.8 hr 68.9 hr *Total AUC for the entire 3-day and 5-day regimens.
Absorption
The absolute bioavailability of azithromycin 250 mg capsules is 38%.In a two-way crossover study in which 12 healthy subjects received a single 500 mg dose of azithromycin (two 250 mg tablets) with or without a high fat meal, food was shown to increase Cmax by 23% but had no effect on AUC.
When azithromycin oral suspension was administered with food to 28 adult healthy male subjects, Cmax increased by 56% and AUC was unchanged.
Distribution
The serum protein binding of azithromycin is variable in the concentration range approximating human exposure, decreasing from 51% at 0.02 mcg/mL to 7% at 2 mcg/mL.The antibacterial activity of azithromycin is pH related and appears to be reduced with decreasing pH, However, the extensive distribution of drug to tissues may be relevant to clinical activity.
Azithromycin has been shown to penetrate into human tissues, including skin, lung, tonsil, and cervix. Extensive tissue distribution was confirmed by examination of additional tissues and fluids (bone, ejaculum, prostate, ovary, uterus, salpinx, stomach, liver, and gallbladder). As there are no data from adequate and well-controlled studies of azithromycin treatment of infections in these additional body sites, the clinical significance of these tissue concentration data is unknown.
Following a regimen of 500 mg on the first day and 250 mg daily for 4 days, very low concentrations were noted in cerebrospinal fluid (less than 0.01 mcg/mL) in the presence of noninflamed meninges.
Metabolism
In vitro and in vivo studies to assess the metabolism of azithromycin have not been performed.Elimination
Plasma concentrations of azithromycin following single 500 mg oral and IV doses declined in a polyphasic pattern resulting in a mean apparent plasma clearance of 630 mL/min and terminal elimination half-life of 68 hours. The prolonged terminal half-life is thought to be due to extensive uptake and subsequent release of drug from tissues. Biliary excretion of azithromycin, predominantly as unchanged drug, is a major route of elimination. Over the course of a week, approximately 6% of the administered dose appears as unchanged drug in urine.Specific Populations
Renal Insufficiency
Azithromycin pharmacokinetics was investigated in 42 adults (21 to 85 years of age) with varying degrees of renal impairment. Following the oral administration of a single 1.0 g dose of azithromycin (4 x 250 mg capsules), mean Cmax and AUC0-120 increased by 5.1% and 4.2%, respectively, in subjects with mild to moderate renal impairment (GFR 10 to 80 mL/min) compared to subjects with normal renal function (GFR >80 mL/min). The mean Cmax and AUC0-120 increased 61% and 35%, respectively, in subjects with severe renal impairment (GFR <10 mL/min) compared to subjects with normal renal function (GFR >80 mL/min).Hepatic Insufficiency
The pharmacokinetics of azithromycin in subjects with hepatic impairment has not been established.Gender
There are no significant differences in the disposition of azithromycin between male and female subjects. No dosage adjustment is recommended based on gender.Geriatric Patients
Pharmacokinetic parameters in older volunteers (65 to 85 years old) were similar to those in young adults (18 to 40 years old) for the 5-day therapeutic regimen. Dosage adjustment does not appear to be necessary for older patients with normal renal and hepatic function receiving treatment with this dosage regimen [see Geriatric Use (8.5)].Pediatric Patients
In two clinical studies, azithromycin for oral suspension was dosed at 10 mg/kg on day 1, followed by 5 mg/kg on days 2 through 5 in two groups of pediatric patients (aged 1 to 5 years and 5 to 15 years, respectively). The mean pharmacokinetic parameters on day 5 were Cmax =0.216 mcg/mL, Tmax =1.9 hours, and AUC0-24 =1.822 mcg·hr/mL for the 1- to 5-year-old group and were Cmax =0.383 mcg/mL, Tmax =2.4 hours, and AUC0-24 =3.109 mcg·hr/mL for the 5- to 15-year-old group.In another study, 33 pediatric patients received doses of 12 mg/kg/day (maximum daily dose 500 mg) for 5 days, of whom 31 patients were evaluated for azithromycin pharmacokinetics following a low fat breakfast. In this study, azithromycin concentrations were determined over a 24 hour period following the last daily dose. Patients weighing above 41.7 kg received the maximum adult daily dose of 500 mg. Seventeen patients (weighing 41.7 kg or less) received a total dose of 60 mg/kg. The following table shows pharmacokinetic data in the subset of pediatric patients who received a total dose of 60 mg/kg.
Pharmacokinetic Parameter
[mean (SD)]5-Day Regimen
(12 mg/kg for 5 days)N 17 Cmax (mcg/mL) 0.5 (0.4) Tmax (hr) 2.2 (0.8) AUC0-24 (mcg hr/mL) 3.9 (1.9) Single dose pharmacokinetics of azithromycin in pediatric patients given doses of 30 mg/kg have not been studied [see Dosage and Administration (2)].
Drug interaction studies were performed with azithromycin and other drugs likely to be co-administered. The effects of co-administration of azithromycin on the pharmacokinetics of other drugs are shown in Table 1 and the effects of other drugs on the pharmacokinetics of azithromycin are shown in Table 2.
Co-administration of azithromycin at therapeutic doses had a modest effect on the pharmacokinetics of the drugs listed in Table 1. No dosage adjustment of drugs listed in Table 1 is recommended when co-administered with azithromycin.
Co-administration of azithromycin with efavirenz or fluconazole had a modest effect on the pharmacokinetics of azithromycin. Nelfinavir significantly increased the Cmax and AUC of azithromycin. No dosage adjustment of azithromycin is recommended when administered with drugs listed in Table 2 [see Drug Interactions (7.3)].
Table 1. Drug Interactions: Pharmacokinetic Parameters for Co-administered Drugs in the Presence of Azithromycin Co-administered Drug Dose of Co-administered Drug Dose of Azithromycin n Ratio (with/without azithromycin) of
Co-administered Drug
Pharmacokinetic Parameters (90% CI);
No Effect = 1.00Mean Cmax Mean AUC Atorvastatin 10 mg/day for 8 days 500 mg/day orally on days 6 to 8 12 0.83
(0.63 to 1.08)1.01
(0.81 to 1.25)Carbamazepine 200 mg/day for 2 days, then 200 mg twice a day for 18 days 500 mg/day orally for days 16 to 18 7 0.97
(0.88 to 1.06)0.96
(0.88 to 1.06)Cetirizine 20 mg/day for 11 days 500 mg orally on day 7, then 250 mg/day on days 8 to 11 14 1.03
(0.93 to 1.14)1.02
(0.92 to 1.13)Didanosine 200 mg orally twice a day for 21 days 1200 mg/day orally on days 8 to 21 6 1.44
(0.85 to 2.43)1.14
(0.83 to 1.57)Efavirenz 400 mg/day for 7 days 600 mg orally on day 7 14 1.04* 0.95* Fluconazole 200 mg orally single dose 1200 mg orally single dose 18 1.04
(0.98 to 1.11)1.01
(0.97 to 1.05)Indinavir 800 mg three times a day for 5 days 1200 mg orally on day 5 18 0.96
(0.86 to 1.08)0.90
(0.81 to 1.00)Midazolam 15 mg orally on day 3 500 mg/day orally for 3 days 12 1.27
(0.89 to 1.81)1.26
(1.01 to 1.56)Nelfinavir 750 mg three times a day for 11 days 1,200 mg orally on day 9 14 0.90
(0.81 to 1.01)0.85
(0.78 to 0.93)Sildenafil 100 mg on days 1 and 4 500 mg/day orally for 3 days 12 1.16
(0.86 to 1.57)0.92
(0.75 to 1.12)Theophylline 4 mg/kg IV on days 1, 11, 25 500 mg orally on day 7, 250 mg/day on days 8 to 11 10 1.19
(1.02 to 1.40)1.02
(0.86 to 1.22)Theophylline 300 mg orally twice a day for 15 days 500 mg orally on day 6, then 250 mg/day on days 7 to 10 8 1.09
(0.92 to 1.29)1.08
(0.89 to 1.31)Triazolam 0.125 mg on day 2 500 mg orally on day 1, then 250 mg/day on day 2 12 1.06* 1.02* Trimethoprim/Sulfamethoxazole 160 mg/800 mg/day orally for 7 days 1200 mg orally on day 7 12 0.85
(0.75 to 0.97)/ 0.90 (0.78 to 1.03)0.87
(0.80 to 0.95/0.96(0.88 to 1.03)Zidovudine 500 mg/day orally for 21 days 600 mg/day orally for 14 days 5 1.12
(0.42 to 3.02)0.94
(0.52 to 1.70)Zidovudine 500 mg/day orally for 21 days 1200 mg/day orally for 14 days 4 1.31
(0.43 to 3.97)1.30
(0.69 to 2.43)* - 90% Confidence interval not reported
Table 2. Drug Interactions: Pharmacokinetic Parameters for Azithromycin in the Presence of Co-administered Drugs [see Drug Interactions (7)]. Co-administered Drug Dose of
Co-administered DrugDose of Azithromycin n Ratio (with/without co-administered drug)
of Azithromycin Pharmacokinetic Parameters (90% CI);
No Effect = 1.00Mean Cmax Mean AUC Efavirenz 400 mg/day for 7 days 600 mg orally on day 7 14 1.22
(1.04 to 1.42)0.92* Fluconazole 200 mg orally single dose 1,200 mg orally single dose 18 0.82
(0.66 to 1.02)1.07
(0.94 to 1.22)Nelfinavir 750 mg three times a day for 11 days 1,200 mg orally on day 9 14 2.36
(1.77 to 3.15)2.12
(1.80 to 2.50)* - 90% Confidence interval not reported
12.4 Microbiology
Mechanism of Action
Azithromycin acts by binding to the 50S ribosomal subunit of susceptible microorganisms and interferes with bacterial protein synthesis. Nucleic acid synthesis is not affected.Cross Resistance
Azithromycin demonstrates cross resistance with erythromycin resistant Gram positive isolates.Azithromycin has been shown to be active against most isolates of the following bacteria, both in vitro and in clinical [see Indications and Usage (1)].
Gram-Positive Bacteria
Staphylococcus aureus
Streptococcus agalactiae
Streptococcus pneumoniae
Streptococcus pyogenesGram-Negative Bacteria
Haemophilus ducreyi
Haemophilus influenzae
Moraxella catarrhalis
Neisseria gonorrhoeaeOther Bacteria
Chlamydophila pneumoniae
Chlamydia trachomatis
Mycoplasma pneumoniaeThe following in vitro data are available, but their clinical significance is unknown. Azithromycin exhibits in vitro minimal inhibitory concentrations (MICs) of 4.0 mcg/ml or less against most (≥90%) isolates of the following bacteria; however, the safety and effectiveness of azithromycin in treating clinical infections due to these bacteria have not been established in adequate and well-controlled trials.
Gram-Positive Bacteria
Beta-hemolytic streptococci (Groups C, F, G)Viridans group streptococci
Gram-Negative Bacteria
Bordetella pertussis
Legionella pneumophilaAnaerobic Bacteria
Prevotella bivia
Peptostreptococcus speciesOther Bacteria
Ureaplasma urealyticumSusceptibility Testing Methods
When available, the clinical microbiology laboratory should provide the results of in vitro susceptibility test results for antibacterial drugs used in resident hospitals to the physician as periodic reports that describe the susceptibility profile of nosocomial and community-acquired pathogens. These reports should aid the physician in selecting an antibacterial drug product for treatment.Dilution Techniques
Quantitative methods are used to determine minimal inhibitory concentrations (MICs). These MICs provide estimates of the susceptibility of bacteria to antibacterial compounds. The MICs should be determined using a standardized test method1,2,3 (broth or agar). The MIC values should be interpreted according to criteria provided in Table 1.Diffusion Techniques
Quantitative methods that require measurement of zone diameters can also provide reproducible estimates of the susceptibility of bacteria to antibacterial compounds. The zone size provides an estimate of the susceptibility of bacteria to antibacterial compounds. The zone size should be determined using a standardized method2,3. This procedure uses paper disk impregnated with 15 mcg azithromycin to test the susceptibility of bacteria to azithromycin. The disk diffusion interpretive criteria are provided in Table 1.Table 1: Susceptibility Test Interpretive Criteria for Azithromycina Pathogen Minimum Inhibitory
Concentrations (mcg/mL)Disk Diffusion
(zone diameter in mm)S I R S I R Haemophilus influenzaeb ≤4 - - ≥12 Staphylococcus aureus ≤2 4 ≥8 ≥18 14 to 17 ≤13 Streptococci including S. pneumoniae ≤0.5 1 ≥2 ≥18 14 to 17 ≤13 aClarithromycin is used for susceptibility testing due to its better solubility
bInsufficient information is available to determine Intermediate or Resistant interpretive criteria
The ability to correlate MIC values and plasma drug levels is difficult as azithromycin concentrates in macrophages and tissues [see Clinical Pharmacology (12)].
A report of “Susceptible” indicates that the pathogen is likely to inhibit growth of the pathogen if the antibacterial compound reaches the concentration at the infection site necessary to inhibit growth of the pathogen. A report of “Intermediate” indicates that the result should be considered equivocal, and if the microorganism is not fully susceptible to alternative clinically feasible drugs, the test should be repeated. This category implies possible clinical applicability in body sites where the drug is physiologically concentrated. This category also provides a buffer zone that prevents small uncontrolled technical factors from causing major discrepancies in interpretation. A report of “Resistant” indicates that the antibacterial is not likely to inhibit growth of the pathogen if the antibacterial compound reaches the concentrations usually achievable at the infection site; other therapy should be selected.
Quality Control
Standardized susceptibility test procedures require the use of laboratory controls to monitor and ensure the accuracy and precision of supplies and reagents used in the assay, and the techniques of the individuals performing the test1,2,3. Standard azithromycin powder should provide the following range of MIC values provided in Table 4. For the diffusion technique using the 15 mcg azithromycin disk the criteria provided in Table 4 should be achieved.Table 4: Acceptable Quality Control Ranges for Susceptibility Testing Quality Control Organism Minimum Inhibitory Concentrations (mcg/mL) Disk Diffusion (zone diameters in mm) Staphylococcus aureus
ATCC* 25923Not Applicable 21 to 26 Staphylococcus aureus
ATCC 292130.5 to 2 Not Applicable Haemophilus Influenzae
ATCC 492471.0 to 4.0 13 to 21 Streptococcus pneumoniae
ATCC 496190.06 to 0.25 19 to 25 *ATCC = American Type Culture Collection
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term studies in animals have not been performed to evaluate carcinogenic potential. Azithromycin has shown no mutagenic potential in standard laboratory tests: mouse lymphoma assay, human lymphocyte clastogenic assay, and mouse bone marrow clastogenic assay. No evidence of impaired fertility due to azithromycin was found in rats given daily doses up to 10 mg/kg (approximately 0.2 times an adult daily dose of 500 mg based on body surface area).
13.2 Animal Toxicology and/or Pharmacology
Phospholipidosis (intracellular phospholipid accumulation) has been observed in some tissues of mice, rats, and dogs given multiple doses of azithromycin. It has been demonstrated in numerous organ systems (e.g., eye, dorsal root ganglia, liver, gallbladder, kidney, spleen, and/or pancreas) in dogs and rats treated with azithromycin at doses which, expressed on the basis of body surface area, are similar to or less than the highest recommended adult human dose. This effect has been shown to be reversible after cessation of azithromycin treatment. Based on the pharmacokinetic data, phospholipidosis has been seen in the rat (50 mg/kg/day dose) at the observed maximal plasma concentration of 1.3 mcg/mL (1.6 times the observed Cmax of 0.821 mcg/mL at the adult dose of 2 g). Similarly, it has been shown in the dog (10 mg/kg/day dose) at the observed maximal serum concentration of 1 mcg/mL (1.2 times the observed Cmax of 0.821 mcg/mL at the adult dose of 2 g). Phospholipidosis was also observed in neonatal rats dosed for 18 days at 30 mg/kg/day, which is less than the pediatric dose of 60 mg/kg based on the surface area. It was not observed in neonatal rats treated for 10 days at 40 mg/kg/day with mean maximal serum concentrations of 1.86 mcg/mL, approximately 1.5 times the Cmax of 1.27 mcg/mL at the pediatric dose. Phospholipidosis has been observed in neonatal dogs (10 mg/kg/day) at maximum mean whole blood concentrations of 3.54 mcg/mL, approximately 3 times the pediatric dose Cmax. The significance of these findings for animals and for humans is unknown.
-
14 CLINICAL STUDIES
14.1 Adult Patients
Acute Bacterial Exacerbations of Chronic Bronchitis
In a randomized, double-blind controlled clinical trial of acute exacerbation of chronic bronchitis (AECB), azithromycin (500 mg once daily for 3 days) was compared with clarithromycin (500 mg twice daily for 10 days). The primary endpoint of this trial was the clinical cure rate at Days 21 to 24. For the 304 patients analyzed in the modified intent-to-treat analysis at the Days 21 to 24 visit, the clinical cure rate for 3 days of azithromycin was 85% (125/147) compared to 82% (129/157) for 10 days of clarithromycin.The following outcomes were the clinical cure rates at the Days 21 to 24 visit for the bacteriologically evaluable patients by pathogen:
Pathogen Azithromycin (3 Days) Clarithromycin (10 Days) S. pneumoniae 29/32 (91%) 21/27 (78%) H. influenzae 12/14 (86%) 14/16 (88%) M. catarrhalis 11/12 (92%) 12/15 (80%) Acute Bacterial Sinusitis
In a randomized, double-blind, double-dummy controlled clinical trial of acute bacterial sinusitis, azithromycin (500 mg once daily for 3 days) was compared with amoxicillin/clavulanate (500/125 mg three times a day for 10 days). Clinical response assessments were made at Day 10 and Day 28. The primary endpoint of this trial was prospectively defined as the clinical cure rate at Day 28. For the 594 patients analyzed in the modified intent to treat analysis at the Day 10 visit, the clinical cure rate for 3 days of azithromycin was 88% (268/303) compared to 85% (248/291) for 10 days of amoxicillin/clavulanate. For the 586 patients analyzed in the modified intent to treat analysis at the Day 28 visit, the clinical cure rate for 3 days of azithromycin was 71.5% (213/298) compared to 71.5% (206/288), with a 97.5% confidence interval of –8.4 to 8.3, for 10 days of amoxicillin/clavulanate.In an open label, non-comparative study requiring baseline transantral sinus punctures, the following outcomes were the clinical success rates at the Day 7 and Day 28 visits for the modified intent to treat patients administered 500 mg of azithromycin once daily for 3 days with the following pathogens:
Clinical Success Rates of Azithromycin (500 mg per day for 3 Days)
Pathogen Day 7 Day28 S. pneumoniae 23/26 (88%) 21/25 (84%) H. influenzae 28/32 (87%) 24/32 (75%) M. catarrhalis 14/15 (93%) 13/15 (87%) 14.2 Pediatric Patients
From the perspective of evaluating pediatric clinical trials, Days 11 to 14 were considered on-therapy evaluations because of the extended half-life of azithromycin. Days 11 to 14 data are provided for clinical guidance. Days 24 to 32 evaluations were considered the primary test of cure endpoint.
Pharyngitis/Tonsillitis
In three double-blind controlled studies, conducted in the United States, azithromycin (12 mg/kg once a day for 5 days) was compared to penicillin V (250 mg three times a day for 10 days) in the treatment of pharyngitis due to documented Group A β-hemolytic streptococci (GABHS or S. pyogenes). Azithromycin was clinically and microbiologically statistically superior to penicillin at Day 14 and Day 30 with the following clinical success (i.e., cure and improvement) and bacteriologic efficacy rates (for the combined evaluable patient with documented GABHS):Three U.S. Streptococcal Pharyngitis Studies
Azithromycin vs. Penicillin V
EFFICACY RESULTSDay 14 Day 30 Bacteriologic Eradication: Azithromycin 323/340 (95%) 255/330 (77%) Penicillin V 242/332 (73%) 206/325 (63%) Clinical Success (cure plus improvement): Azithromycin 336/343 (98%) 310/330 (94%) Penicillin V 284/338 (84%) 241/325 (74%) Approximately 1% of azithromycin-susceptible S. pyogenes isolates were resistant to azithromycin following therapy.
Acute Otitis Media
Efficacy using azithromycin given over 5 days (10 mg/kg on Day 1 followed by 5 mg/kg on Days 2 to 5).Trial 1
In a double-blind, controlled clinical study of acute otitis media performed in the United States, azithromycin (10 mg/kg on Day 1 followed by 5 mg/kg on Days 2 to 5) was compared to amoxicillin/clavulanate potassium (4:1). For the 553 patients who were evaluated for clinical efficacy, the clinical success rate (i.e., cure plus improvement) at the Day 11 visit was 88% for azithromycin and 88% for the control agent. For the 521 patients who were evaluated at the Day 30 visit, the clinical success rate was 73% for azithromycin and 71% for the control agent.Trial 2
In a non-comparative clinical and microbiologic trial performed in the United States, where significant rates of beta-lactamase producing organisms (35%) were found, 131 patients were evaluable for clinical efficacy. The combined clinical success rate (i.e., cure and improvement) at the Day 11 visit was 84% for azithromycin. For the 122 patients who were evaluated at the Day 30 visit, the clinical success rate was 70% for azithromycin.Microbiologic determinations were made at the pre-treatment visit. Microbiology was not reassessed at later visits. The following clinical success rates were obtained from the evaluable group:
Pathogen Day 11 Day 30 Azithromycin Azithromycin S. pneumoniae 61/74 (82%) 40/56 (71%) H. influenzae 43/54 (80%) 30/47 (64%) M. catarrhalis 28/35 (80%) 19/26 (73%) S. pyogenes 11/11 (100%) 7/7 (100%) Overall 177/217 (82%) 97/137 (73%) Trial 3
In another controlled comparative clinical and microbiologic study of otitis media performed in the United States, azithromycin (10 mg/kg on Day 1 followed by 5 mg/kg on Days 2 to 5) was compared to amoxicillin/clavulanate potassium (4:1). This study utilized two of the same investigators as Protocol 2 (above), and these two investigators enrolled 90% of the patients in Protocol 3. For this reason, Protocol 3 was not considered to be an independent study. Significant rates of beta-lactamase producing organisms (20%) were found. Ninety-two (92) patients were evaluable for clinical and microbiologic efficacy. The combined clinical success rate (i.e., cure and improvement) of those patients with a baseline pathogen at the Day 11 visit was 88% for azithromycin vs. 100% for control; at the Day 30 visit, the clinical success rate was 82% for azithromycin vs. 80% for control.Microbiologic determinations were made at the pre-treatment visit. Microbiology was not reassessed at later visits. At the Day 11 and Day 30 visits, the following clinical success rates were obtained from the evaluable group:
Pathogen Day 11 Day 30 Azithromycin Control Azithromycin Control S. pneumoniae 25/29 (86%) 26/26 (100%) 22/28 (79%) 18/22 (82%) H. influenzae 9/11 (82%) 9/9 (100%) 8/10 (80%) 6/8 (75%) M. catarrhalis 7/7 (100%) 5/5 (100%) 5/5 (100%) 2/3 (66%) S. pyogenes 2/2 (100%) 5/5 (100%) 2/2 (100%) 4/4 (100%) Overall 43/49 (88%) 45/45 (100%) 37/45 (82%) 30/37 (81%) Efficacy using azithromycin given over 3 days (10 mg/kg/day).
Trial 4
In a double-blind, controlled, randomized clinical study of acute otitis media in pediatric patients from 6 months to 12 years of age, azithromycin (10 mg/kg per day for 3 days) was compared to amoxicillin/clavulanate potassium (7:1) in divided doses q12h for 10 days. Each patient received active drug and placebo matched for the comparator.For the 366 patients who were evaluated for clinical efficacy at the Day 12 visit, the clinical success rate (i.e., cure plus improvement) was 83% for azithromycin and 88% for the control agent. For the 362 patients who were evaluated at the Days 24 to 28 visit, the clinical success rate was 74% for azithromycin and 69% for the control agent.
Efficacy using azithromycin 30 mg/kg given as a single dose
Trial 5
A double-blind, controlled, randomized trial was performed at nine clinical centers. Pediatric patients from 6 months to 12 years of age were randomized 1:1 to treatment with either azithromycin (given at 30 mg/kg as a single dose on Day 1) or amoxicillin/clavulanate potassium (7:1), divided q12h for 10 days. Each child received active drug, and placebo matched for the comparator.Clinical response (Cure, Improvement, Failure) was evaluated at End of Therapy (Days 12 to 16) and Test of Cure (Days 28 to 32). Safety was evaluated throughout the trial for all treated subjects. For the 321 subjects who were evaluated at End of Treatment, the clinical success rate (cure plus improvement) was 87% for azithromycin, and 88% for the comparator. For the 305 subjects who were evaluated at Test of Cure, the clinical success rate was 75% for both azithromycin and the comparator.
Trial 6
In a non-comparative clinical and microbiological trial, 248 patients from 6 months to 12 years of age with documented acute otitis media were dosed with a single oral dose of azithromycin (30 mg/kg on Day 1).For the 240 patients who were evaluable for clinical modified Intent-to-Treat (MITT) analysis, the clinical success rate (i.e., cure plus improvement) at Day 10 was 89% and for the 242 patients evaluable at Days 24 to 28, the clinical success rate (cure) was 85%.
Presumed Bacteriologic Eradication Day 10 Days 24 to 28 S. pneumoniae 70/76 (92%) 67/76 (88%) H. influenzae 30/42 (71%) 28/44 (64%) M. catarrhalis 10/10 (100%) 10/10 (100%) Overall 110/128 (86%) 105/130 (81%) -
15 REFERENCES
-
Clinical and Laboratory Standards Institute (CLSI). Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria that Grow Aerobically; Approved Standard - Ninth Edition. CLSI document M07-A9, Clinical and Laboratory Standards Institute, 950 West Valley Road, Suite 2500, Wayne, Pennsylvania 19087, USA, 2012.
-
Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing; Twenty-third Informational Supplement, CLSI document M100-S23. CLSI document M100-S23, Clinical and Laboratory Standards Institute, 950 West Valley Road, Suite 2500, Wayne, Pennsylvania 19087, USA, 2013.
-
Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Disk Diffusion Susceptibility Tests; Approved Standard – Eleventh Edition CLSI document M02-A11, Clinical and Laboratory Standards Institute, 950 West Valley Road, Suite 2500, Wayne, Pennsylvania 19087, USA, 2012.
-
-
16 HOW SUPPLIED/STORAGE AND HANDLING
Azithromycin Tablets, USP 250 mg are supplied as white, oval, biconvex film coated tablets containing azithromycin dihydrate equivalent to 250 mg of azithromycin.
Azithromycin Tablets, USP 250 mg are engraved “APO” on one side and “AZ250” on the other side. These are packaged in bottles and blister cards of 6 tablets as follows:
NDC: 70882-107-06 Package of 6 Tablets (1 x 6 unit-of-dose blisters)
Azithromycin Tablets, USP 500 mg are supplied as white, oval, biconvex film coated tablets containing azithromycin dihydrate equivalent to 500 mg of azithromycin.
Azithromycin Tablets, USP 500 mg are engraved “APO” on one side and “AZ500” on the other. These are packaged in bottles and blister cards of 3 tablets as follows:
NDC: 70882-118-03 Package of 3 Tablets (1 x 3 unit-of-dose blisters)
Storage: Store at 20° to 25°C (68° to 77°F); excursions permitted from 15° to 30°C (59° to 86°F) [See USP Controlled Room Temperature].
-
17 PATIENT COUNSELING INFORMATION
17.1 General Patient Counseling
General Patient Counseling
Azithromycin tablets and oral suspension can be taken with or without food.Patients should also be cautioned not to take aluminum- and magnesium-containing antacids and azithromycin simultaneously.
The patient should be directed to discontinue azithromycin immediately and contact a physician if any signs of an allergic reaction occur.
Patients should be counseled that antibacterial drugs including azithromycin should only be used to treat bacterial infections. They do not treat viral infections (e.g., the common cold). When azithromycin is prescribed to treat a bacterial infection, patients should be told that although it is common to feel better early in the course of the therapy, the medication should be taken exactly as directed. Skipping doses or not completing the full course of therapy may (1) decrease the effectiveness of the immediate treatment and (2) increase the likelihood that bacteria will develop resistance and will not be treatable by azithromycin or other antibacterial drugs in the future.
Diarrhea is a common problem caused by antibacterials which usually ends when the antibacterial is discontinued. Sometimes after starting treatment with antibacterials patients can develop watery and bloody stools (with or without stomach cramps and fever) even as late as two or more months after having taken the last dose of the antibacterial drug. If this occurs, patients should contact their physician as soon as possible.
17.2 See FDA-approved Patient Labeling
See FDA-approved Patient Labeling
AZITHROMYCIN TABLETS, USP
250 mg and 500 mgManufactured by Apotex Inc.
Toronto, Ontario
Canada, M9L 1T9Distributed by Cambridge Therapeutic Technologies, LLC
Teaneck, NJ 07666Packaged by Legacy Pharmaceutical Packaging, LLC
Earth City, MO 63045Revised: December 2016
20529 -
Patient Information
Azithromycin Tablets
(ay zith" roe mye' sin)Read this Patient Information leaflet before you start taking azithromycin tablets and each time you get a refill. There may be new information. This information does not take the place of talking to your healthcare provider about your medical condition or your treatment.
What are azithromycin tablets?
Azithromycin tablets are a macrolide antibiotic prescription medicine used in adults 18 years or older to treat certain infections caused by certain germs called bacteria. These bacterial infections include:
-
acute worsening of chronic bronchitis
-
acute sinus infection
-
community-acquired pneumonia
-
infected throat or tonsils
-
skin infections
-
infections of the urethra or cervix
-
genital ulcers in men
Azithromycin tablets are also used in children to treat:
-
ear infections
-
community-acquired pneumonia
-
infected throat or tonsils
Azithromycin should not be taken by people who cannot tolerate oral medications because they are very ill or have certain other risk factors including:
- have cystic fibrosis
- have hospital acquired infections
- have known or suspected bacteria in the blood
- need to be in the hospital
- are elderly
- have any medical problems that can lower the ability of the immune system to fight infections
Azithromycin tablets are not for viral infections such as the common cold.
It is not known if azithromycin tablets are safe and effective for genital ulcers in women.
It is not known if azithromycin tablets are safe and effective for children with ear infections, sinus infections, and community-acquired pneumonia under 6 months of age.
It is not known if azithromycin tablets are safe and effective for infected throat or tonsils in children under 2 years of age.
Who should not take azithromycin tablets?
Do not take azithromycin tablets if you:
- have had a severe allergic reaction to certain antibiotics known as macrolides or ketolides including azithromycin and erythromycin.
- have a history of cholestatic jaundice or hepatic dysfunction that happened with the use of azithromycin.
What should I tell my healthcare provider before taking azithromycin tablets?
Before you take azithromycin tablets, tell your healthcare provider if you:
-
have pneumonia
-
have cystic fibrosis
-
have known or suspected bacteremia (bacterial infection in the blood)
-
have liver or kidney problems
-
have an irregular heartbeat, especially a problem called “QT prolongation”
-
have a problem that causes muscle weakness (myasthenia gravis)
-
have any other medical problems
-
are pregnant or plan to become pregnant. It is not known if azithromycin will harm your unborn baby.
-
are breastfeeding or plan to breastfeed. Azithromycin has been reported to pass into breast milk. Talk to your healthcare provider about the best way to feed your baby while you take azithromycin tablets.
Tell your healthcare provider about all the medicines you take, including prescription and non-prescription medicines, vitamins, and herbal supplements.
Azithromycin tablets and other medicines may affect each other causing side effects. Azithromycin tablets may affect the way other medicines work, and other medicines may affect how azithromycin tablets work.
Especially tell your healthcare provider if you take:
-
nelfinavir
-
a blood thinner (warfarin)
-
digoxin
-
phenytoin
-
an antacid that contains aluminum or magnesium
Know the medicines you take. Keep a list of your medicines and show it to your healthcare provider and pharmacist when you get a new medicine.
How should I take azithromycin tablets?
-
Take azithromycin tablets exactly as your healthcare provider tells you to take it.
-
Azithromycin tablets can be taken with or without food.
- Do not skip any doses of azithromycin tablets or stop taking it, even if you begin to feel better, until you finish your prescribed treatment unless you have a serious allergic reaction or your healthcare provider tells you to stop taking azithromycin tablets. “See What are the possible side effects of azithromycin tablets?” If you skip doses, or do not complete the total course of azithromycin tablets your treatment may not work as well and your infection may be harder to treat. Taking all of your azithromycin tablet doses will help lower the chance that the bacteria will become resistant to azithromycin tablets.
-
If the bacteria becomes resistant to azithromycin, azithromycin tablets and other antibiotic medicines may not work for you in the future.
-
If you take too many azithromycin tablets, call your healthcare provider or get medical help right away.
What are the possible side effects of azithromycin tablets?
Azithromycin tablets can cause serious side effects, including:
-
Serious allergic reactions. Allergic reactions can happen in people taking azithromycin the active ingredient in azithromycin tablets, even after only 1 dose. Stop taking azithromycin tablets and get emergency medical help right away if you have any of the following symptoms of a severe allergic reaction:
-
trouble breathing or swallowing
-
swelling of the lips, tongue, face
-
throat tightness, hoarseness
-
rapid heartbeat
-
faintness
-
skin rash (hives)
-
new onset of fever and swollen lymph nodes
-
Stop taking azithromycin tablets at the first sign of a skin rash and call your healthcare provider. Skin rash may be a sign of a more serious reaction to azithromycin tablets.
-
Liver damage (hepatotoxicity). Hepatotoxicity can happen in people who take azithromycin tablets. Call your healthcare provider right away if you have unexplained symptoms such as:
- nausea or vomiting
- stomach pain
- fever
- weakness
- abdominal pain or tenderness
- itching
- unusual tiredness
- loss of appetite
- change in the color of your bowel movements
- dark colored urine
- yellowing of your skin or of the whites of your eyes
Stop taking azithromycin tablets and tell your healthcare provider right away if you have yellowing of your skin or white part of your eyes, or if you have dark urine. These can be signs of a serious reaction to azithromycin tablets (a liver problem).
-
Serious heart rhythm changes (QT prolongation and torsades de pointes).
Tell your healthcare provider right away if you have a change in your heartbeat (a fast or irregular heartbeat), or if you feel faint and dizzy. Azithromycin tablets may cause a rare heart problem known as prolongation of the QT interval. This condition can cause an abnormal heartbeat and can be very dangerous. The chances of this happening are higher in people:
- who are elderly
- with a family history of prolonged QT interval
- with low blood potassium
- who take certain medicines to control heart rhythm (antiarrhythmics)
-
Worsening of myasthenia gravis (a problem that causes muscle weakness). Certain antibiotics like azithromycin tablets may cause worsening of myasthenia gravis symptoms, including muscle weakness and breathing problems. Call your healthcare provider right away if you have any worsening muscle weakness or breathing problems.
-
Diarrhea. Tell your healthcare provider right away if you have watery diarrhea, diarrhea that does not go away, or bloody stools. You may experience cramping and a fever. This could happen after you have finished your azithromycin tablets.
The most common side effects of azithromycin tablets include:
- nausea
- stomach pain
- vomiting
These are not all the possible side effects of azithromycin tablets. Tell your healthcare provider about any side effect that bothers you or that does not go away.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
How should I store azithromycin tablets?
-
Store azithromycin tablets at 20° to 25°C (68° to 77°F), excursions permitted to 15ºto 30º C (59ºto 86º F) [see Controlled Room Temperature].
-
Safely throw away any medicine that is out of date or no longer needed.
Keep azithromycin tablets and all medicines out of the reach of children.
General information about the safe and effective use of azithromycin tablets.
Medicines are sometimes prescribed for purposes other than those listed in the Patient Information leaflet. Do not use azithromycin tablets for a condition for which it was not prescribed. Do not give azithromycin tablets to other people, even if they have the same symptoms you have. It may harm them.
This Patient Information leaflet summarizes the most important information about azithromycin tablets. If you would like more information, talk with your healthcare provider. You can ask your pharmacist or healthcare provider for information about azithromycin tablets that is written for health professionals.
For more information, contact Cambridge Therapeutic Technologies, LLC at 1-844-810-0004.
What are the ingredients in azithromycin tablets?
Active ingredient: azithromycin dihydrate
Inactive ingredients: dibasic calcium phosphate dihydrate, hydroxypropyl cellulose, croscarmellose sodium, magnesium stearate and Opadry II white (Opadry II white contains the following components: hypromellose, lactose monohydrate, titanium dioxide and triacetin).
This Patient Information has been approved by the U.S. Food and Drug Administration.
AZITHROMYCIN TABLETS, USP
250 mg and 500 mgManufactured by Apotex Inc.
Toronto, Ontario
Canada, M9L 1T9Distributed by
Cambridge Therapeutic Technologies, LLC
Teaneck, NJ 07666Packaged by
Legacy Pharmaceutical Packaging, LLC
Earth City, MO 63045Revised: December 2016
20529 -
- Azithromycin Tablets, USP 250 mg
- Azithromycin Tablets, USP 500 mg
-
INGREDIENTS AND APPEARANCE
AZITHROMYCIN DIHYDRATE
azithromycin tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 70882-107(NDC: 60505-2581) Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength AZITHROMYCIN DIHYDRATE (UNII: 5FD1131I7S) (AZITHROMYCIN ANHYDROUS - UNII:J2KLZ20U1M) AZITHROMYCIN ANHYDROUS 250 mg Inactive Ingredients Ingredient Name Strength DIBASIC CALCIUM PHOSPHATE DIHYDRATE (UNII: O7TSZ97GEP) HYDROXYPROPYL CELLULOSE (TYPE H) (UNII: RFW2ET671P) CROSCARMELLOSE SODIUM (UNII: M28OL1HH48) MAGNESIUM STEARATE (UNII: 70097M6I30) HYPROMELLOSES (UNII: 3NXW29V3WO) LACTOSE MONOHYDRATE (UNII: EWQ57Q8I5X) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) TRIACETIN (UNII: XHX3C3X673) Product Characteristics Color WHITE Score no score Shape OVAL Size 13mm Flavor Imprint Code APO;AZ250 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 70882-107-06 6 in 1 BLISTER PACK; Type 0: Not a Combination Product 07/18/2011 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA065507 07/18/2011 AZITHROMYCIN DIHYDRATE
azithromycin tablet, film coatedProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 70882-118(NDC: 60505-2582) Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength AZITHROMYCIN DIHYDRATE (UNII: 5FD1131I7S) (AZITHROMYCIN ANHYDROUS - UNII:J2KLZ20U1M) AZITHROMYCIN ANHYDROUS 500 mg Inactive Ingredients Ingredient Name Strength DIBASIC CALCIUM PHOSPHATE DIHYDRATE (UNII: O7TSZ97GEP) HYDROXYPROPYL CELLULOSE (TYPE H) (UNII: RFW2ET671P) CROSCARMELLOSE SODIUM (UNII: M28OL1HH48) MAGNESIUM STEARATE (UNII: 70097M6I30) HYPROMELLOSES (UNII: 3NXW29V3WO) LACTOSE MONOHYDRATE (UNII: EWQ57Q8I5X) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) TRIACETIN (UNII: XHX3C3X673) Product Characteristics Color WHITE Score no score Shape OVAL Size 16mm Flavor Imprint Code APO;AZ500 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 70882-118-03 3 in 1 BLISTER PACK; Type 0: Not a Combination Product 07/18/2011 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA065509 07/18/2011 Labeler - Cambridge Therapeutics Technologies, LLC (080072003)
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.