TETRACYCLINE HYDROCHLORIDE capsule
Tetracycline Hydrochloride by
Drug Labeling and Warnings
Tetracycline Hydrochloride by is a Prescription medication manufactured, distributed, or labeled by STAT Rx USA LLC, PSS World Medical Inc.. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
SPL UNCLASSIFIED SECTION
For Oral Use
Rx only
To reduce the development of drug-resistant bacteria and maintain the effectiveness of tetracycline hydrochloride and other antibacterial drugs, tetracycline hydrochloride should be used only to treat or prevent infections that are proven or strongly suspected to be caused by bacteria.
-
DESCRIPTION
Tetracycline is a yellow, odorless, crystalline powder. Tetracycline is stable in air but exposure to strong sunlight causes it to darken. Its potency is affected in solutions of pH below 2 and is rapidly destroyed by alkali hydroxide solutions. Tetracycline is very slightly soluble in water, freely soluble in dilute acid and in alkali hydroxide solutions, sparingly soluble in alcohol, and practically insoluble in chloroform and in ether. The chemical name for tetracycline hydrochloride is 4-(Dimethylamino)-1,4,4a,5,5a,6,11,12a-octahydro-3,6,10,12,-12a-pentahydroxy-6-methyl-1,11-dioxo-2-naphthacenecar-boxamide monohydrochloride. Its structural formula is as follows:
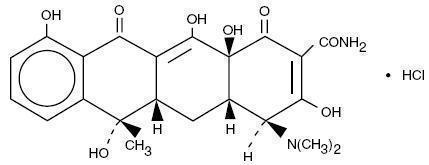
C22H24N208HCI M.W. 480.90
Each capsule, for oral administration, contains 250 mg or 500 mg tetracycline hydrochloride, and has the following inactive ingredients: colloidal silicon dioxide, D&C Yellow #10, gelatin, pregelatinized starch, propylene glycol, shellac glaze (modified), stearic acid, and titanium dioxide. The 250 mg capsules also contain black iron oxide, FD&C Blue #1 Aluminum Lake, FD&C Blue #2 Aluminum Lake, FD&C Red #40 Aluminum Lake, and FD&C Yellow #6. The 500 mg capsules also contain ammonium hydroxide, FD&C Blue #1, FD&C Red #40, and simethicone.
-
CLINICAL PHARMACOLOGY
Tetracyclines are readily absorbed and are bound to plasma proteins in varying degrees. They are concentrated by the liver in the bile and excreted in the urine and feces at high concentrations in a biologically active form.
Microbiology
Tetracyclines are primarily bacteriostatic and exert their antimicrobial effect by the inhibition of protein synthesis. Tetracycline is active against a wide range of gram-negative and gram-positive organisms. The drugs in the tetracycline class have closely similar antimicrobial spectra, and cross-resistance among them is common. While in vitro studies have demonstrated the susceptibility of most strains of the following microorganisms, clinical efficacy for infections other than those included in the INDICATIONS AND USAGE section has not been documented.
Gram-negative Bacteria
Neisseria gonorrhea
Haemophilus ducreyi
Haemophilus influenzae
Yersinia pestis (formerly Pasteurella pestis)
Francisella tularensis (formerly Pasteurella tularensis)
Vibrio cholera (formerly Vibrio comma)
Bartonella bacilliformis
Brucella species
Because many strains of the following groups of gram-negative microorganisms have been shown to be resistant to tetracyclines, culture and susceptibility testing are recommended:
Escherichia coli
Klebsiella species
Enterobacter aerogenes
Shigella species
Acinetobacter species (formerly Mima species and Herellea species)
Bacteroides species
Gram-positive Bacteria
Because many strains of the following groups of gram-positive microorganisms have been shown to be resistant to tetracycline, culture and susceptibility testing are recommended. Up to 44 percent of strains of Streptococcus pyogenes and 74 percent of Streptococcus faecalis have been found to be resistant to tetracycline drugs. Therefore, tetracyclines should not be used for streptococcal disease unless the organisms have been demonstrated to be susceptible.
Streptococcus pyogenes
Streptococcus pneumoniae
Enterococcus group (Streptococcus faecalis and Streptococcus faecium)
Alpha-hemolytic Streptococci (viridans group)
Susceptibility Testing
A tetracycline disk may be used to determine microbial susceptibility to drugs in the tetracycline class. If the Kirby-Bauer method of disk susceptibility testing is used, a 30 mcg tetracycline disk should give a zone of at least 19 mm when tested against a tetracycline susceptible bacterial strain. Microorganisms may be considered susceptible if the MIC (minimum inhibitory concentration) is not more than 4 mcg/mL and intermediate if the MIC is 4 to 12.5 mcg/mL.
-
INDICATIONS AND USAGE
To reduce the development of drug-resistant bacteria and maintain the effectiveness of tetracycline hydrochloride and other antibacterial drugs, tetracycline hydrochloride should be used only to treat or prevent infections that are proven or strongly suspected to be caused by susceptible bacteria. When culture and susceptibility information are available, they should be considered in selecting or modifying antibacterial therapy. In the absence of such data, local epidemiology and susceptibility patterns may contribute to the empiric selection of therapy.
Tetracycline is indicated in the treatment of infections caused by susceptible strains of the designated organisms in the conditions listed below:
- Upper respiratory tract infections caused by Streptococcus pyogenes, Streptococcus pneumoniae and Hemophilus influenzae. Note: Tetracycline should not be used for streptococcal disease unless the organism has been demonstrated to be susceptible.
- Lower respiratory tract infections caused by Streptococcus pyogenes, Streptococcus pneumoniae, Mycoplasma pneumoniae (Eaton agent, and Klebsiella sp.)
- Skin and soft tissue infections caused by Streptococcus pyogenes, Staphylococcus aureaus. (Tetracyclines are not the drugs of choice in the treatment of any type of staphylococcal infections.)
- Infections caused by rickettsia including Rocky Mountain spotted fever, typhus group infections, Q fever, rickettsialpox.
- Psittacosis or ornithosis caused by Chlamydia Psittaci.
- Infections caused by Chlamydia trachomatis such as uncomplicated urethral, endocervical or rectal infections, inclusion conjunctivitis, trachoma, and lymphogranuloma venereum.
- Granuloma inquinale caused by Calymmatobacterium granulomatis.
- Relapsing fever caused by Borrelia sp.
- Bartonellosis caused by Bartonella bacilliformis.
- Chancroid caused by Hemophilus ducreyi.
- Tularemia caused by Francisella tularensis.
- Plaque caused by Yersinia pestis.
- Cholera caused by Vibrio cholerae.
- Brucellosis caused by Brucella species (tetracycline may be used in conjunction with an aminoglycoside).
- Infections due to Campylobacter fetus.
- As adjunctive therapy in intestinal amebiasis caused by Entamoeba histolytica.
- Urinary tract infections caused by susceptible strains of Escherichia coli, Klebsiella, etc.
- Other infections caused by susceptible gram-negative organisms such as E. coli, Enterobacter aerogenes, Shigella sp., Acinetobacter sp., Klebsiella sp., and Bacteroides sp.
- In severe acne, adjunctive therapy with tetracycline may be useful.
When penicillin is contraindicated, tetracyclines are alternative drugs in the treatment of the following infections:
- Syphilis and yaws caused by Treponema pallidum and pertenue, respectively,
- Vincent’s infection caused by Fusobacterium fusiforme,
- Infections caused by Neisseria gonorrhoeae,
- Anthrax caused by Bacillus anthracis,
- Infections due to Listeria monocytogenes,
- Actinomycosis caused by Actinomyces species,
- Infections due to Clostridium species.
- CONTRAINDICATIONS
-
WARNINGS
THE USE OF DRUGS OF THE TETRACYCLINE CLASS DURING TOOTH DEVELOPMENT (LAST HALF OF PREGNANCY, INFANCY AND CHILDHOOD TO THE AGE OF 8 YEARS) MAY CAUSE PERMANENT DISCOLORATION OF THE TEETH (YELLOW - GRAY - BROWN). This adverse reaction is more common during long-term use of the drugs but has been observed following repeated short-term courses. Enamel hypoplasia has also been reported. TETRACYCLINE DRUGS, THEREFORE, SHOULD NOT BE USED IN THIS AGE GROUP UNLESS OTHER DRUGS ARE NOT LIKELY TO BE EFFECTIVE OR ARE CONTRAINDICATED.
All tetracyclines form a stable calcium complex in any bone forming tissue. A decrease in fibula growth rate has been observed in premature infants given oral tetracycline in doses of 25 mg/kg every six hours. This reaction was shown to be reversible when the drug was discontinued.
Results of animal studies indicate that tetracyclines cross the placenta, are found in fetal tissues and can have toxic effects on the developing fetus (often related to retardation of skeletal development). Evidence of embryotoxicity has also been noted in animals treated early in pregnancy. If this drug is used during pregnancy or if the patient becomes pregnant while taking this drug, the patient should be apprised of the potential hazard to the fetus. Tetracycline drugs should not be used during pregnancy unless absolutely necessary.
If renal impairment exists, even usual oral or parenteral doses may lead to excessive systemic accumulation of the drug and possible liver toxicity. Under such conditions, lower than usual total doses are indicated, and, if therapy is prolonged, serum level determinations of the drug may be advisable.
Photosensitivity manifested by an exaggerated sunburn reaction has been observed in some individuals taking tetracyclines. Patients apt to be exposed to direct sunlight or ultraviolet light should be advised that this reaction can occur with tetracycline drugs. Treatment should be discontinued at the first evidence of skin erythema.
The antianabolic action of the tetracyclines may cause an increase in BUN. While this is not a problem in those with normal renal function, in patients with significantly impaired renal function, higher serum levels of tetracycline may lead to azotemia, hyperphosphatemia and acidosis.
-
PRECAUTIONS
General
As with other antibiotics, use of this drug may result in overgrowth of nonsusceptible organisms, including fungi. If superinfection occurs, the antibiotic should be discontinued and appropriate therapy should be instituted.
All infections due to Group A beta-hemolytic streptococci should be treated for at least ten days.
Bulging fontanels in infants and benign intracranial hypertension in adults have been reported in individuals receiving tetracyclines. These conditions disappeared when the drug was discontinued.
Incision and drainage or other surgical procedures should be performed in conjunction with antibiotic therapy, when indicated.
Prescribing tetracycline in the absence of proven or strongly suspected bacterial infection or a prophylactic indication is unlikely to provide benefit to the patient and increases the risk of the development of drug-resistant bacteria.
Information for Patients
Patients should be counseled that antibacterial drugs including tetracycline should only be used to treat bacterial infections. They do not treat viral infections (e.g., the common cold). When tetracycline is prescribed to treat a bacterial infection, patients should be told that although it is common to feel better early in the course of therapy, the medication should be taken exactly as directed. Skipping doses or not completing the full course of therapy may (1) decrease the effectiveness of the immediate treatment and (2) increase the likelihood that bacteria will develop resistance and will not be treatable by tetracycline or other antibacterial drugs in the future.
Laboratory Tests
In venereal diseases, when coexistent syphilis is suspected, dark field examinations should be done before treatment is started and the blood serology repeated monthly for at least four months.
In long-term therapy, periodic laboratory evaluation of organ systems, including hematopoietic, renal and hepatic studies, should be performed.
Drug Interactions
Since bacteriostatic drugs may interfere with the bactericidal action of penicillin, it is advisable to avoid giving tetracycline in conjunction with penicillin or other bactericidal antibiotics.
Because the tetracyclines have been shown to depress plasma prothrombin activity, patients who are on anticoagulant therapy may require downward adjustment of their anticoagulant dosage.
The concurrent use of tetracycline and methoxyflurane has been reported to result in fatal renal toxicity.
Absorption of tetracyclines is impaired by antacids containing aluminum, calcium or magnesium and preparations containing iron, zinc, or sodium bicarbonate.
Concurrent use of tetracycline may render oral contraceptives less effective.
Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term animal studies are currently being conducted to determine whether tetracycline hydrochloride has carcinogenic potential. Some related antibiotics (oxytetracycline, minocycline) have shown evidence of oncogenic activity in rats.
In two in vitro mammalian cell assay systems (L 51784y mouse Iymphoma and Chinese hamster lung cells), there was evidence of mutagenicity at tetracycline hydrochloride concentrations of 60 and 10 mcg/mL, respectively.
Tetracycline hydrochloride had no effect on fertility when administered in the diet to male and female rats at a daily intake of 25 times the human dose.
-
ADVERSE REACTIONS
Gastrointestinal: anorexia, nausea, epigastric distress, vomiting, diarrhea, glossitis, black hairy tongue, dysphagia, enterocolitis, and inflammatory lesions (with monilial overgrowth) in the anogenital region.
Rare instances of esophagitis and esophageal ulceration have been reported in patients receiving particularly the capsule and also the tablet forms of tetracyclines.
Most of the patients were reported to have taken medication immediately before going to bed (see DOSAGE AND ADMINISTRATION).
Teeth: permanent discoloration of teeth may be caused during tooth development. Enamel hypoplasia has also been reported (see WARNINGS).
Skin: maculopapular and erythematous rashes. Exfoliative dermatitis has been reported but is uncommon. Onycholysis and discoloration of the nails have been reported rarely. Photosensitivity is discussed in WARNINGS.
Renal toxicity: rise in BUN has been reported and is apparently dose related.
Liver: hepatotoxicity and liver failure have been observed in patients receiving large doses of tetracycline and in tetracycline-treated patients with renal impairment.
Hypersensitivity reactions: urticaria, angioneurotic edema, anaphylaxis, anaphylactoid purpura, pericarditis, exacerbation of systemic lupus erythematosus, and serum sickness-like reactions, as fever, rash, and arthralgia.
Blood: hemolytic anemia, thrombocytopenia, thrombocytopenic purpura, neutropenia and eosinophilia have been reported.
Other: bulging fontanels in infants and intracranial pressure in adults (see PRECAUTIONS, General).
When given over prolonged periods, tetracyclines have been reported to produce brown-black microscopic discoloration of thyroid glands. No abnormalities of thyroid function studies are known to occur.
- OVERDOSAGE
-
DOSAGE AND ADMINISTRATION
Adults
Usual daily dose, 1 gram as 500 mg b.i.d. or 250 mg q.i.d. Higher doses such as 500 mg q.i.d. may be required for severe infections or for those infections which do not respond to the smaller doses.
Children above eight years of age
Usual daily dose, 10 to 20 mg/lb (25 to 50 mg/kg) body weight divided in four equal doses.
Therapy should be continued for at least 24 to 48 hours after symptoms and fever have subsided.
For treatment of brucellosis, 500 mg tetracycline q.i.d. for three weeks should be accompanied by streptomycin, 1 gram intramuscularly twice daily the first week and once daily the second week.
For the treatment of syphilis in patients allergic to penicillin, the following dosage of tetracycline is recommended: early syphilis (less than one year’s duration), 500 mg q.i.d. for 15 days. Syphilis of more than one year’s duration (except neurosyphilis), 500 mg q.i.d. for 30 days.
For treatment of gonorrhea, the recommended dose is 500 mg by mouth four times a day for seven days.
In cases of moderate to severe acne which, in the judgement of the clinician, require long-term treatment, the recommended initial dosage is 1 gram daily in divided doses. When improvement is noted, dosage should be gradually reduced to maintenance levels ranging from 125 mg to 500 mg daily. In some patients it may be possible to maintain adequate remission of lesions with alternate-day or intermittent therapy. Tetracycline therapy of acne should augment the other standard measures known to be of value. Duration of long-term treatment which can safely be recommended has not been established (see WARNINGS and Carcinogenesis, Mutagenesis, Impairment of Fertility).
Concomitant therapy
Absorption of tetracycline is impaired by antacids containing aluminum, calcium or magnesium and preparations containing iron, zinc, or sodium bicarbonate.
Food and some dairy products also interfere with absorption.
In the treatment of streptococcal infections, a therapeutic dose of tetracycline should be administered for at least ten days.
In patients with renal impairment (see WARNINGS): total dosage should be decreased by reduction of recommended individual doses and/or by extending time intervals between doses.
Uncomplicated urethral, endocervical or rectal infections in adults caused by Chlamydiatrachomatis: 500 mg, by mouth, four times a day for at least seven days.
Administration of adequate amounts of fluid with the capsule formulation of tetracycline is recommended to wash down the drug and reduce the risk of esophageal irritation and ulceration (see ADVERSE REACTIONS).
-
HOW SUPPLIED
Tetracycline Hydrochloride Capsules USP, 250 mg are available as orange opaque and yellow opaque capsules, imprinted with “Z” and “2416” in black ink, containing 250 mg of tetracycline hydrochloride, packaged in:
Bottles of 28 - NDC # 16590-216-28
Tetracycline Hydrochloride Capsules USP, 500 mg are available as black and yellow capsules, imprinted with "Z" and "2407" in white ink, containing 500 mg of tetracycline hydrochloride, packaged in:
Bottles of 28 - NDC # 16590-217-28
Bottles of 30 - NDC # 16590-217-30
Dispense in a tight, light resistant container as defined in the USP, with a child-resistant closure (as required).
Store at 20° to 25°C (68° to 77°F) [See USP Controlled Room Temperature].Relabeling and Repackaging by:
STAT Rx USA LLC
Gainesville, GA 30501
-
ANIMAL PHARMACOLOGY AND ANIMAL TOXICOLOGY
Hyperpigmentation of the thyroid has been produced by members of the tetracycline class in the following species: in rats by oxytetracycline, doxycycline, minocycline, tetracycline PO4 and methacycline; in minipigs by doxycycline, minocycline, tetracycline PO4 and methacycline; in dogs by doxycycline and minocycline; in monkeys by minocycline.
Minocycline, tetracycline PO4, methacycline, doxycycline, tetracycline base, oxytetracycline HCI and tetracycline HCI were goitrogenic in rats fed a low iodine diet. This goitrogenic effect was accomplished by high radioactive iodine uptake. Administration of minocycline also produced a large goiter with high radioiodine uptake in rats fed a relatively high iodine diet.
Treatment of various animal species with this class of drugs has also resulted in the induction of thyroid hyperplasia in the following: in rats and dogs (minocycline), in chickens (chlortetracycline) and in rats and mice (oxytetracycline). Adrenal gland hyperplasia has been observed in goats and rats treated with oxytetracycline.
TEVA PHARMACEUTICALS USA
Sellersville, PA 18960
Rev. B 3/2011
- SPL UNCLASSIFIED SECTION
- PACKAGE LABEL - TETRACYCLINE 250 MG CAPSULES
- PACKAGE LABEL - TETRACYCLINE 500 MG CAPSULES
-
INGREDIENTS AND APPEARANCE
TETRACYCLINE HYDROCHLORIDE
tetracycline hydrochloride capsuleProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 16590-216(NDC: 0172-2416) Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength TETRACYCLINE HYDROCHLORIDE (UNII: P6R62377KV) (TETRACYCLINE - UNII:F8VB5M810T) TETRACYCLINE HYDROCHLORIDE 250 mg Inactive Ingredients Ingredient Name Strength D&C YELLOW NO. 10 (UNII: 35SW5USQ3G) FD&C BLUE NO. 1 (UNII: H3R47K3TBD) FD&C BLUE NO. 2 (UNII: L06K8R7DQK) FD&C RED NO. 40 (UNII: WZB9127XOA) FD&C YELLOW NO. 6 (UNII: H77VEI93A8) FERROSOFERRIC OXIDE (UNII: XM0M87F357) GELATIN (UNII: 2G86QN327L) PROPYLENE GLYCOL (UNII: 6DC9Q167V3) SHELLAC (UNII: 46N107B71O) SILICON DIOXIDE (UNII: ETJ7Z6XBU4) STARCH, CORN (UNII: O8232NY3SJ) STEARIC ACID (UNII: 4ELV7Z65AP) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) Product Characteristics Color ORANGE (orange opaque) , YELLOW (yellow opaque) Score no score Shape CAPSULE Size 19mm Flavor Imprint Code Z;2416 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 16590-216-28 28 in 1 BOTTLE Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA060704 03/23/2010 TETRACYCLINE HYDROCHLORIDE
tetracycline hydrochloride capsuleProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 16590-217(NDC: 0172-2407) Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength TETRACYCLINE HYDROCHLORIDE (UNII: P6R62377KV) (TETRACYCLINE - UNII:F8VB5M810T) TETRACYCLINE HYDROCHLORIDE 500 mg Inactive Ingredients Ingredient Name Strength AMMONIA (UNII: 5138Q19F1X) D&C YELLOW NO. 10 (UNII: 35SW5USQ3G) FD&C BLUE NO. 1 (UNII: H3R47K3TBD) FD&C RED NO. 40 (UNII: WZB9127XOA) GELATIN (UNII: 2G86QN327L) PROPYLENE GLYCOL (UNII: 6DC9Q167V3) SHELLAC (UNII: 46N107B71O) SILICON DIOXIDE (UNII: ETJ7Z6XBU4) STARCH, CORN (UNII: O8232NY3SJ) STEARIC ACID (UNII: 4ELV7Z65AP) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) Product Characteristics Color black, yellow Score no score Shape CAPSULE Size 22mm Flavor Imprint Code Z;2407 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 16590-217-28 28 in 1 BOTTLE 2 NDC: 16590-217-30 30 in 1 BOTTLE Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA060704 03/23/2010 Labeler - STAT Rx USA LLC (786036330) Registrant - PSS World Medical Inc. (101822682) Establishment Name Address ID/FEI Business Operations STAT Rx USA LLC 786036330 relabel(16590-216, 16590-217) , repack(16590-216, 16590-217)
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.