SUTENT- sunitinib malate capsule
SUTENT by
Drug Labeling and Warnings
SUTENT by is a Prescription medication manufactured, distributed, or labeled by Pfizer Laboratories Div Pfizer Inc, Pfizer Italia S.r.l., Pfizer Asia Manufacturing Pte Ltd, Pfizer Ireland Pharmaceuticals Unlimited Company. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use SUTENT safely and effectively. See full prescribing information for SUTENT.
SUTENT® (sunitinib malate) capsules, for oral use
Initial U.S. Approval: 2006WARNING: HEPATOTOXICITY
See full prescribing information for complete boxed warning.
Hepatotoxicity has been observed in clinical trials and postmarketing experience. Hepatotoxicity may be severe, and in some cases fatal. Monitor hepatic function and interrupt, reduce, or discontinue dosing as recommended [see Warnings and Precautions (5.1)].
RECENT MAJOR CHANGES
Dosage and Administration, Dose Modification for End-Stage Renal Disease (ESRD) Patients on Hemodialysis (2.6) 05/2019 INDICATIONS AND USAGE
SUTENT is a kinase inhibitor indicated for:
- the treatment of gastrointestinal stromal tumor (GIST) after disease progression on or intolerance to imatinib mesylate. (1.1)
- the treatment of advanced renal cell carcinoma (RCC). (1.2)
- the adjuvant treatment of adult patients at high risk of recurrent RCC following nephrectomy. (1.3)
- the treatment of progressive, well-differentiated pancreatic neuroendocrine tumors (pNET) in patients with unresectable locally advanced or metastatic disease. (1.4)
DOSAGE AND ADMINISTRATION
GIST and Advanced RCC:
- 50 mg orally once daily, with or without food, 4 weeks on treatment followed by 2 weeks off. (2.1)
Adjuvant RCC:
- 50 mg orally once daily, with or without food, 4 weeks on treatment followed by 2 weeks off for nine 6-week cycles. (2.2)
pNET:
- 37.5 mg orally once daily, with or without food, continuously without a scheduled off-treatment period. (2.3)
Dose Modification:
- Dose interruptions and/or dose adjustments of 12.5 mg recommended based on individual safety and tolerability. (2.4)
DOSAGE FORMS AND STRENGTHS
- Capsules: 12.5 mg, 25 mg, 37.5 mg, 50 mg (3)
CONTRAINDICATIONS
- None (4)
WARNINGS AND PRECAUTIONS
- Hepatotoxicity, including fatal liver failure, has been observed. Monitor liver function tests before initiation of treatment, during each cycle of treatment, and as clinically indicated. Interrupt SUTENT for Grade 3 or 4 drug-related hepatic adverse reactions and discontinue if there is no resolution. Do not restart SUTENT if patients experience severe changes in liver function tests or have signs and symptoms of liver failure. (5.1)
- Cardiovascular events including myocardial ischemia, myocardial infarction, left ventricular ejection fraction declines to below the lower limit of normal and cardiac failure including death have occurred. Monitor patients for signs and symptoms of congestive heart failure. Discontinue SUTENT for clinical manifestations of congestive heart failure. (5.2)
- Prolonged QT intervals and Torsade de Pointes have been observed. Monitor patients at higher risk for developing QT interval prolongation. Consider monitoring of electrocardiograms and electrolytes. (5.3)
- Hypertension may occur. Monitor blood pressure and treat as needed. (5.4)
- Hemorrhagic events, including tumor-related hemorrhage, and viscus perforation (both with fatal events) have occurred. Perform serial complete blood counts and physical examinations. (5.5)
- Cases of Tumor Lysis Syndrome (TLS) (some fatal) have been reported primarily in patients with RCC and GIST with high tumor burden. Monitor these patients closely and treat as clinically indicated. (5.6)
- Thrombotic microangiopathy (TMA), including thrombotic thrombocytopenic purpura and hemolytic uremic syndrome, sometimes leading to renal failure or a fatal outcome, has been reported. Discontinue SUTENT in patients developing TMA. (5.7)
- Proteinuria, including renal failure or a fatal outcome, has occurred. Monitor urine protein. Interrupt treatment for 24-hour urine protein ≥3 grams. Discontinue for repeat episodes of protein ≥3 grams despite dose reductions or nephrotic syndrome. (5.8)
- Necrotizing fasciitis, erythema multiforme, Stevens-Johnson syndrome (SJS), and toxic epidermal necrolysis (TEN) (some fatal) have occurred. Discontinue SUTENT if these events occur. (5.9)
- Thyroid dysfunction may occur. Patients with signs and/or symptoms suggestive of hypothyroidism or hyperthyroidism should have laboratory monitoring of thyroid function performed and be treated as per standard medical practice. (5.10)
- Hypoglycemia may occur. Check blood glucose levels regularly and assess if antidiabetic drug dose modifications are required. (5.11)
- Osteonecrosis of the jaw has been reported. Consider preventive dentistry prior to treatment with SUTENT. If possible, avoid invasive dental procedures, particularly in patients receiving intravenous bisphosphonate therapy. (5.12)
- Wound Healing: Impaired wound healing has occurred with SUTENT. Temporary interruption of therapy with SUTENT is recommended in patients undergoing major surgical procedures. (5.13)
- Embryo-Fetal Toxicity: Can cause fetal harm. Advise patients of potential risk to a fetus and to use effective contraception. (5.14, 8.1, 8.3)
ADVERSE REACTIONS
- The most common adverse reactions (≥25%) are fatigue/asthenia, diarrhea, mucositis/stomatitis, nausea, decreased appetite/anorexia, vomiting, abdominal pain, hand-foot syndrome, hypertension, bleeding events, dysgeusia/altered taste, dyspepsia, and thrombocytopenia. (6)
To report SUSPECTED ADVERSE REACTIONS, contact Pfizer Inc at 1-800-438-1985 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide.
Revised: 5/2019
-
Table of Contents
FULL PRESCRIBING INFORMATION: CONTENTS*
WARNING: HEPATOTOXICITY
1 INDICATIONS AND USAGE
1.1 Gastrointestinal Stromal Tumor (GIST)
1.2 Advanced Renal Cell Carcinoma (RCC)
1.3 Adjuvant Treatment of Renal Cell Carcinoma (RCC)
1.4 Advanced Pancreatic Neuroendocrine Tumors (pNET)
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dose for GIST and Advanced RCC
2.2 Recommended Dose for Adjuvant Treatment of RCC
2.3 Recommended Dose for pNET
2.4 Dose Modification for Adverse Reactions
2.5 Dose Modification for Co-administration of Strong CYP3A4 Inhibitors or Inducers
2.6 Dose Modification for End-Stage Renal Disease (ESRD) Patients on Hemodialysis
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Hepatotoxicity
5.2 Cardiovascular Events
5.3 QT Interval Prolongation and Torsade de Pointes
5.4 Hypertension
5.5 Hemorrhagic Events and Viscus Perforation
5.6 Tumor Lysis Syndrome (TLS)
5.7 Thrombotic Microangiopathy
5.8 Proteinuria
5.9 Dermatologic Toxicities
5.10 Thyroid Dysfunction
5.11 Hypoglycemia
5.12 Osteonecrosis of the Jaw (ONJ)
5.13 Wound Healing
5.14 Embryo-Fetal Toxicity
6 ADVERSE REACTIONS
6.1 Clinical Trials Experience
6.2 Postmarketing Experience
7 DRUG INTERACTIONS
7.1 Effect of Other Drugs on SUTENT
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.3 Females and Males of Reproductive Potential
8.4 Pediatric Use
8.5 Geriatric Use
8.6 Hepatic Impairment
8.7 Renal Impairment
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
14.1 Gastrointestinal Stromal Tumor
14.2 Renal Cell Carcinoma
14.3 Pancreatic Neuroendocrine Tumors
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
- * Sections or subsections omitted from the full prescribing information are not listed.
-
BOXED WARNING
(What is this?)
WARNING: HEPATOTOXICITY
Hepatotoxicity has been observed in clinical trials and postmarketing experience. Hepatotoxicity may be severe, and in some cases, fatal. Monitor hepatic function and interrupt, reduce, or discontinue dosing as recommended [see Warnings and Precautions (5.1)].
-
1 INDICATIONS AND USAGE
1.1 Gastrointestinal Stromal Tumor (GIST)
SUTENT is indicated for the treatment of gastrointestinal stromal tumor after disease progression on or intolerance to imatinib mesylate.
1.2 Advanced Renal Cell Carcinoma (RCC)
SUTENT is indicated for the treatment of advanced renal cell carcinoma.
-
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dose for GIST and Advanced RCC
The recommended dose of SUTENT for gastrointestinal stromal tumor (GIST) and advanced renal cell carcinoma (RCC) is one 50 mg oral dose taken once daily, on a schedule of 4 weeks on treatment followed by 2 weeks off (Schedule 4/2). SUTENT may be taken with or without food.
2.2 Recommended Dose for Adjuvant Treatment of RCC
The recommended dose of SUTENT for the adjuvant treatment of RCC is 50 mg taken orally once daily, on a schedule of 4 weeks on treatment followed by 2 weeks off (Schedule 4/2), for nine 6-week cycles. SUTENT may be taken with or without food.
2.3 Recommended Dose for pNET
The recommended dose of SUTENT for pancreatic neuroendocrine tumors (pNET) is 37.5 mg taken orally once daily continuously without a scheduled off-treatment period. SUTENT may be taken with or without food.
2.4 Dose Modification for Adverse Reactions
Dose interruption and/or dose modification in 12.5 mg increments or decrements is recommended based on individual safety and tolerability. The maximum dose administered in the pNET study was 50 mg daily. In the adjuvant RCC study, the minimum dose administered was 37.5 mg.
2.5 Dose Modification for Co-administration of Strong CYP3A4 Inhibitors or Inducers
Strong CYP3A4 inhibitors such as ketoconazole may increase sunitinib plasma concentrations. Selection of an alternate concomitant medication with no or minimal enzyme inhibition potential is recommended. A dose reduction for SUTENT to a minimum of 37.5 mg (GIST and RCC) or 25 mg (pNET) daily should be considered if SUTENT must be co-administered with a strong CYP3A4 inhibitor [see Drug Interactions (7.1) and Clinical Pharmacology (12.3)].
CYP3A4 inducers such as rifampin may decrease sunitinib plasma concentrations. Selection of an alternate concomitant medication with no or minimal enzyme induction potential is recommended. A dose increase for SUTENT to a maximum of 87.5 mg (GIST and RCC) or 62.5 mg (pNET) daily should be considered if SUTENT must be co-administered with a CYP3A4 inducer. If dose is increased, the patient should be monitored carefully for toxicity [see Drug Interactions (7.1) and Clinical Pharmacology (12.3)].
2.6 Dose Modification for End-Stage Renal Disease (ESRD) Patients on Hemodialysis
No starting dose adjustment is required in patients with end-stage renal disease (ESRD) on hemodialysis. However, given the decreased exposure compared to patients with normal renal function, subsequent doses may be increased gradually up to 2-fold based on safety and tolerability [see Clinical Pharmacology (12.3)].
-
3 DOSAGE FORMS AND STRENGTHS
12.5 mg capsules
Hard gelatin capsule with orange cap and orange body, printed with white ink "Pfizer" on the cap and "STN 12.5 mg" on the body.
25 mg capsules
Hard gelatin capsule with caramel cap and orange body, printed with white ink "Pfizer" on the cap and "STN 25 mg" on the body.
- 4 CONTRAINDICATIONS
-
5 WARNINGS AND PRECAUTIONS
5.1 Hepatotoxicity
SUTENT can cause severe hepatotoxicity, resulting in liver failure or death. Liver failure occurred at an incidence of <1% in clinical trials. Liver failure signs include jaundice, elevated transaminases and/or hyperbilirubinemia in conjunction with encephalopathy, coagulopathy, and/or renal failure. Monitor liver function tests (alanine aminotransferase [ALT], aspartate aminotransferase [AST], and bilirubin) before initiation of treatment, during each cycle of treatment, and as clinically indicated. Interrupt SUTENT for Grade 3 or 4 drug-related hepatic adverse reactions and discontinue if there is no resolution. Do not restart SUTENT if patients subsequently experience severe changes in liver function tests or have other signs and symptoms of liver failure.
Safety in patients with ALT or AST >2.5 × upper limit of normal (ULN) or, if due to liver metastases, >5.0 × ULN has not been established.
5.2 Cardiovascular Events
Discontinue SUTENT in the presence of clinical manifestations of congestive heart failure (CHF). Interrupt SUTENT and/or reduce the dose in patients without clinical evidence of CHF who have an ejection fraction of >20% but <50% below baseline or below the lower limit of normal if baseline ejection fraction is not obtained.
In patients without cardiac risk factors a baseline evaluation of ejection fraction should be considered. Carefully monitor patients for clinical signs and symptoms of CHF while receiving SUTENT. Baseline and periodic evaluations of left ventricular ejection fraction (LVEF) should also be considered while these patients are receiving SUTENT.
Cardiovascular events, including heart failure, cardiomyopathy, myocardial ischemia, and myocardial infarction, some of which were fatal, have been reported.
In patients treated with SUTENT (N=7527) for GIST, advanced RCC, adjuvant treatment of RCC and pNET, 3% of patients experienced heart failure; 71% of the patients with heart failure were reported as recovered. Fatal cardiac failure was reported in <1% of patients.
In the adjuvant treatment of RCC study, 11 patients in each arm experienced a decreased ejection fraction meeting Grade 2 CTCAE criteria (LVEF 40–50% and a 10–19% decrease from baseline). No patients had a Grade 3–4 decrease in ejection fraction. The ejection fractions of three patients in the SUTENT arm and 2 patients in the placebo arm did not return to ≥50% or baseline by the time of last measurement. No patients who received SUTENT were diagnosed with CHF.
Patients who presented with cardiac events within 12 months prior to SUTENT administration, such as myocardial infarction (including severe/unstable angina), coronary/peripheral artery bypass graft, symptomatic CHF, cerebrovascular accident or transient ischemic attack, or pulmonary embolism were excluded from SUTENT clinical studies. Patients with prior anthracycline use or cardiac radiation were also excluded from some studies. It is unknown whether patients with these concomitant conditions may be at a higher risk of developing drug-related left ventricular dysfunction.
5.3 QT Interval Prolongation and Torsade de Pointes
SUTENT can cause QT interval prolongation in a dose-dependent manner, which may lead to an increased risk for ventricular arrhythmias including Torsade de Pointes. Torsade de Pointes has been observed in <0.1% of SUTENT-exposed patients.
Monitor patients with a history of QT interval prolongation, patients who are taking antiarrhythmics, or patients with relevant pre-existing cardiac disease, bradycardia, or electrolyte disturbances. When using SUTENT, periodic monitoring with on-treatment electrocardiograms and electrolytes (magnesium, potassium) should be considered. Concomitant treatment with strong CYP3A4 inhibitors may increase sunitinib plasma concentrations and dose reduction of SUTENT should be considered [see Dosage and Administration (2.5)].
5.4 Hypertension
Monitor patients for hypertension and treat as needed with standard antihypertensive therapy. In cases of severe hypertension, temporary suspension of SUTENT is recommended until hypertension is controlled.
In patients treated with SUTENT (N=7527) in GIST, advanced RCC, adjuvant treatment of RCC and pNET, 29% of patients experienced hypertension. Grade 3 hypertension was reported in 7% of patients, and Grade 4 hypertension was reported in 0.2% of patients.
5.5 Hemorrhagic Events and Viscus Perforation
Hemorrhagic events reported through postmarketing experience, some of which were fatal, have included GI, respiratory, tumor, urinary tract, and brain hemorrhages. In patients treated with SUTENT (N=7527) for GIST, advanced RCC, adjuvant treatment of RCC and pNET, 30% of patients experienced hemorrhagic events, and 4.2% of patients experienced a Grade 3 or 4 event. Epistaxis was the most common hemorrhagic adverse reaction and gastrointestinal hemorrhage was the most common Grade ≥3 event.
Tumor-related hemorrhage has been observed in patients treated with SUTENT. These events may occur suddenly, and in the case of pulmonary tumors, may present as severe and life-threatening hemoptysis or pulmonary hemorrhage. Cases of pulmonary hemorrhage, some with a fatal outcome, have been observed in clinical trials and have been reported in postmarketing experience in patients treated with SUTENT for metastatic RCC, GIST, and metastatic lung cancer. SUTENT is not approved for use in patients with lung cancer. Clinical assessment of hemorrhagic events should include serial complete blood counts (CBCs) and physical examinations.
Serious, sometimes fatal, gastrointestinal complications including gastrointestinal perforation, have been reported in patients with intra-abdominal malignancies treated with SUTENT.
5.6 Tumor Lysis Syndrome (TLS)
Cases of TLS, some fatal, occurred in clinical trials and have been reported in postmarketing experience, primarily in patients with RCC or GIST treated with SUTENT. Patients generally at risk of TLS are those with high tumor burden prior to treatment. Monitor these patients closely and treat as clinically indicated.
5.7 Thrombotic Microangiopathy
Thrombotic microangiopathy (TMA), including thrombotic thrombocytopenic purpura and hemolytic uremic syndrome, sometimes leading to renal failure or a fatal outcome, occurred in clinical trials and in postmarketing experience of SUTENT as monotherapy and administered in combination with bevacizumab. Discontinue SUTENT in patients developing TMA. Reversal of the effects of TMA has been observed after treatment was discontinued.
5.8 Proteinuria
Proteinuria and nephrotic syndrome have been reported. Some of these cases have resulted in renal failure and fatal outcomes. Monitor patients for the development or worsening of proteinuria. Perform baseline and periodic urinalyses during treatment, with follow up measurement of 24-hour urine protein as clinically indicated. Interrupt SUTENT and dose reduce for 24-hour urine protein ≥3 grams. Discontinue SUTENT for patients with nephrotic syndrome or repeat episodes of urine protein ≥3 grams despite dose reductions. The safety of continued SUTENT treatment in patients with moderate to severe proteinuria has not been systematically evaluated.
5.9 Dermatologic Toxicities
Severe cutaneous reactions have been reported, including cases of erythema multiforme (EM), Stevens-Johnson syndrome (SJS), and toxic epidermal necrolysis (TEN), some of which were fatal. If signs or symptoms of EM, SJS, or TEN (e.g., progressive skin rash often with blisters or mucosal lesions) are present, discontinue SUTENT treatment. If a diagnosis of SJS or TEN is suspected, SUTENT treatment must not be re-started.
Necrotizing fasciitis, including fatal cases, has been reported in patients treated with SUTENT, including of the perineum and secondary to fistula formation. Discontinue SUTENT in patients who develop necrotizing fasciitis.
5.10 Thyroid Dysfunction
Baseline laboratory measurement of thyroid function is recommended and patients with hypothyroidism or hyperthyroidism should be treated as per standard medical practice prior to the start of SUTENT treatment. All patients should be observed closely for signs and symptoms of thyroid dysfunction, including hypothyroidism, hyperthyroidism, and thyroiditis, while on SUTENT treatment. Patients with signs and/or symptoms suggestive of thyroid dysfunction should have laboratory monitoring of thyroid function performed and be treated as per standard medical practice.
Cases of hyperthyroidism, some followed by hypothyroidism, have been reported in clinical trials and through postmarketing experience.
5.11 Hypoglycemia
SUTENT can result in symptomatic hypoglycemia, which may lead to loss of consciousness, or require hospitalization. Hypoglycemia has occurred in clinical trials in 2% of the patients treated with SUTENT for advanced RCC and GIST and in approximately 10% of the patients treated with SUTENT for pNET. In the adjuvant treatment of RCC study, no patients on SUTENT experienced hypoglycemia. For patients being treated with SUTENT for pNET, pre-existing abnormalities in glucose homeostasis were not present in all patients who experienced hypoglycemia. Reductions in blood glucose levels may be worse in diabetic patients. Check blood glucose levels regularly during and after discontinuation of treatment with SUTENT. Assess if antidiabetic drug dosage needs to be adjusted to minimize the risk of hypoglycemia.
5.12 Osteonecrosis of the Jaw (ONJ)
ONJ has been observed in clinical trials and has been reported in postmarketing experience in patients treated with SUTENT. Concomitant exposure to other risk factors, such as bisphosphonates or dental disease, may increase the risk of osteonecrosis of the jaw. Consider preventive dentistry prior to treatment with SUTENT. If possible, avoid invasive dental procedures while on SUTENT treatment, particularly in patients receiving intravenous bisphosphonate therapy.
5.13 Wound Healing
Cases of impaired wound healing have been reported during SUTENT therapy. Temporary interruption of SUTENT therapy is recommended for precautionary reasons in patients undergoing major surgical procedures. There is limited clinical experience regarding the timing of reinitiation of therapy following major surgical intervention. Therefore, the decision to resume SUTENT therapy following a major surgical intervention should be based upon clinical judgment of recovery from surgery.
5.14 Embryo-Fetal Toxicity
Based on findings from animal studies and its mechanism of action, SUTENT can cause fetal harm when administered to pregnant woman. Administration of sunitinib to pregnant rats and rabbits during the period of organogenesis resulted in teratogenicity at approximately 5.5 and 0.3 times the clinical systemic exposure (AUC) at the recommended daily doses (RDD) of 50 mg/day, respectively.
Advise pregnant women of the potential risk to a fetus. Advise females of reproductive potential to use effective contraception during treatment with SUTENT and for 4 weeks following the final dose [see Clinical Pharmacology (12.1) and Use in Specific Populations (8.1, 8.3)].
-
6 ADVERSE REACTIONS
The following serious adverse reactions are discussed in greater detail in other sections of the labeling.
- Hepatotoxicity [see Warnings and Precautions (5.1)]
- Cardiovascular Events [see Warnings and Precautions (5.2)]
- QT Interval Prolongation and Torsade de Pointes [see Warnings and Precautions (5.3)]
- Hypertension [see Warnings and Precautions (5.4)]
- Hemorrhagic Events [see Warnings and Precautions (5.5)]
- Tumor Lysis Syndrome (TLS) [see Warnings and Precautions (5.6)]
- Thrombotic Microangiopathy [see Warnings and Precautions (5.7)]
- Proteinuria [see Warnings and Precautions (5.8)]
- Dermatologic Toxicities [see Warnings and Precautions (5.9)]
- Thyroid Dysfunction [see Warnings and Precautions (5.10)]
- Hypoglycemia [see Warnings and Precautions (5.11)]
- Osteonecrosis of the Jaw (ONJ) [see Warnings and Precautions (5.12)]
- Wound Healing [see Warnings and Precautions (5.13)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The data described in the Warnings and Precautions reflect exposure to SUTENT (N = 7527) in GIST, advanced RCC, adjuvant treatment of RCC, and pNET [see Warnings and Precautions (5.1, 5.13)]. In this database, the most common adverse reactions (≥25%) are fatigue/asthenia, diarrhea, mucositis/stomatitis, nausea, decreased appetite/anorexia, vomiting, abdominal pain, hand-foot syndrome, hypertension, bleeding events, dysgeusia/altered taste, dyspepsia, and thrombocytopenia.
The data below reflect exposure to SUTENT in 966 patients who participated in the treatment phase of randomized trials of GIST (n=202), advanced RCC (n=375), adjuvant treatment of RCC (n=306), and pNET (n=83) [see Clinical Studies (14.1, 14.2, 14.3)].
Gastrointestinal Stromal Tumor (GIST)
The safety of SUTENT was evaluated in Study 1, a randomized, double-blind, placebo-controlled trial in which previously treated patients with GIST received SUTENT 50 mg daily on Schedule 4/2 (n=202) or placebo (n=102).
Median duration of blinded study treatment was 2 cycles for patients on SUTENT (mean: 3.0; range: 1–9) and 1 cycle (mean; 1.8; range: 1–6) for patients on placebo at the time of the interim analysis. Dose reductions occurred in 23 patients (11%) on SUTENT and none on placebo. Dose interruptions occurred in 59 patients (29%) on SUTENT and 31 patients (30%) on placebo. The rates of treatment-emergent, nonfatal adverse reactions resulting in permanent discontinuation were 7% and 6% in the SUTENT and placebo groups, respectively.
Most treatment-emergent adverse reactions in both study arms were Grade 1 or 2 in severity. Grade 3 or 4 treatment-emergent adverse reactions were reported in 56% versus 51% of patients on SUTENT versus placebo, respectively, in the double-blind treatment phase of the trial. Table 1 compares the incidence of common (≥10%) treatment-emergent adverse reactions for patients receiving SUTENT and reported more commonly in patients receiving SUTENT than in patients receiving placebo.
Table 1. Adverse Reactions Reported in Study 1 in ≥10% of GIST Patients Who Received SUTENT in the Double-Blind Treatment Phase and More Commonly Than in Patients Given Placebo* Adverse Reaction GIST SUTENT (N=202) Placebo (N=102) All Grades % Grade 3–4 % All Grades % Grade 3–4 % Abbreviations: GIST=gastrointestinal stromal tumor; N=number of patients. - * Common Terminology Criteria for Adverse Events (CTCAE), version 3.0.
- † Includes decreased appetite.
Any Adverse Reaction 94 56 97 51 Gastrointestinal Diarrhea 40 4 27 0 Mucositis/stomatitis 29 1 18 2 Constipation 20 0 14 2 Cardiac Hypertension 15 4 11 0 Dermatology Skin discoloration 30 0 23 0 Rash 14 1 9 0 Hand-foot syndrome 14 4 10 3 Neurology Altered taste 21 0 12 0 Musculoskeletal Myalgia/limb pain 14 1 9 1 Metabolism/Nutrition Anorexia† 33 1 29 5 Asthenia 22 5 11 3 In the double-blind treatment phase of GIST Study 1, oral pain other than mucositis/stomatitis occurred in 12 patients (6%) on SUTENT versus 3 (3%) on placebo. Hair color changes occurred in 15 patients (7%) on SUTENT versus 4 (4%) on placebo. Alopecia was observed in 10 patients (5%) on SUTENT versus 2 (2%) on placebo.
Table 2 provides common (≥10%) treatment-emergent laboratory abnormalities.
Table 2. Laboratory Abnormalities Reported in Study 1 in ≥10% of GIST Patients Who Received SUTENT or Placebo in the Double-Blind Treatment Phase* Laboratory Parameter GIST SUTENT (N=202) Placebo (N=102) All Grades* % Grade 3–4*,† % All Grades* % Grade 3–4*,‡ % Abbreviations: ALT=alanine aminotransferase; AST=aspartate aminotransferase; GIST=gastrointestinal stromal tumor; LVEF=left ventricular ejection fraction; N=number of patients. - * Common Terminology Criteria for Adverse Events (CTCAE), version 3.0.
- † Grade 4 laboratory abnormalities in patients on SUTENT included alkaline phosphatase (1%), lipase (2%), creatinine (1%), potassium decreased (1%), neutrophils (2%), hemoglobin (2%), and platelets (1%).
- ‡ Grade 4 laboratory abnormalities in patients on placebo included amylase (1%), lipase (1%), and hemoglobin (2%).
Any 68 (34) 22 (22) Gastrointestinal AST/ALT 39 2 23 1 Lipase 25 10 17 7 Alkaline phosphatase 24 4 21 4 Amylase 17 5 12 3 Total bilirubin 16 1 8 0 Indirect bilirubin 10 0 4 0 Cardiac Decreased LVEF 11 1 3 0 Renal/Metabolic Creatinine 12 1 7 0 Potassium decreased 12 1 4 0 Sodium increased 10 0 4 1 Hematology Neutrophils 53 10 4 0 Lymphocytes 38 0 16 0 Platelets 38 5 4 0 Hemoglobin 26 3 22 2 After an interim analysis, the study was unblinded and patients on the placebo arm were given the opportunity to receive open-label SUTENT treatment [see Clinical Studies (14.1)]. For 241 patients randomized to the SUTENT arm, including 139 who received SUTENT in both the double-blind and open-label treatment phases, the median duration of SUTENT treatment was 6 cycles (mean: 8.5; range: 1–44). For the 255 patients who ultimately received open-label SUTENT treatment, median duration of study treatment was 6 cycles (mean: 7.8; range: 1–37) from the time of the unblinding. A total of 118 patients (46%) required dosing interruptions, and a total of 72 patients (28%) required dose reductions. The incidence of treatment-emergent adverse reactions resulting in permanent discontinuation was 20%. The most common Grade 3 or 4 treatment-related adverse reactions experienced by patients receiving SUTENT in the open-label treatment phase were fatigue (10%), hypertension (8%), asthenia (5%), diarrhea (5%), hand-foot syndrome (5%), nausea (4%), abdominal pain (3%), anorexia (3%), mucositis (2%), vomiting (2%), and hypothyroidism (2%).
Advanced Renal Cell Carcinoma (RCC)
The safety of SUTENT was evaluated in Study 3, a double-blind, active-controlled trial in which previously untreated patients with locally advanced or metastatic RCC received SUTENT 50 mg daily on Schedule 4/2 (n=375) or IFN-α 9 million International Units (MIU) (n=360). The median duration of treatment was 11.1 months (range: 0.4–46.1) for SUTENT treatment and 4.1 months (range: 0.1–45.6) for IFN-α treatment. Dose interruptions occurred in 202 patients (54%) on SUTENT and 141 patients (39%) on IFN-α. Dose reductions occurred in 194 patients (52%) on SUTENT and 98 patients (27%) on IFN-α. Discontinuation rates due to adverse reactions were 20% for SUTENT and 24% for IFN-α. Most treatment-emergent adverse reactions in both study arms were Grade 1 or 2 in severity. Grade 3 or 4 treatment-emergent adverse reactions were reported in 77% versus 55% of patients on SUTENT versus IFN-α, respectively.
Table 3 compares the incidence of common (≥10%) treatment-emergent adverse reactions for patients receiving SUTENT versus IFN-α.
Table 3. Adverse Reactions Reported in Study 3 in ≥10% of Patients With RCC Who Received SUTENT or IFN-α* Adverse Reaction Treatment-Naïve RCC SUTENT (N=375) IFN-α (N=360) All Grades % Grade 3–4† % All Grades % Grade 3–4‡ % Abbreviations: ARs=adverse reactions; IFN=interferon-α; N=number of patients; RCC=renal cell carcinoma. - * Common Terminology Criteria for Adverse Events (CTCAE), version 3.0.
- † Grade 4 ARs in patients on SUTENT included back pain (1%), arthralgia (<1%), dyspnea (<1%), asthenia (<1%), fatigue (<1%), limb pain (<1%) and rash (<1%).
- ‡ Grade 4 ARs in patients on IFN-α included dyspnea (1%), fatigue (1%), abdominal pain (<1%), and depression (<1%).
- § Includes flank pain.
- ¶ Includes ageusia, hypogeusia, and dysgeusia.
- # Includes decreased appetite.
- Þ Includes 1 patient with Grade 5 gastric hemorrhage.
- ß Includes depressed mood.
Any Adverse Reaction 99 77 99 55 Constitutional Fatigue 62 15 56 15 Asthenia 26 11 22 6 Fever 22 1 37 <1 Weight decreased 16 <1 17 1 Chills 14 1 31 0 Chest Pain 13 2 7 1 Influenza like illness 5 0 15 <1 Gastrointestinal Diarrhea 66 10 21 <1 Nausea 58 6 41 2 Mucositis/stomatitis 47 3 5 <1 Vomiting 39 5 17 1 Dyspepsia 34 2 4 0 Abdominal pain§ 30 5 12 1 Constipation 23 1 14 <1 Dry mouth 13 0 7 <1 GERD/reflux esophagitis 12 <1 1 0 Flatulence 14 0 2 0 Oral pain 14 <1 1 0 Glossodynia 11 0 1 0 Hemorrhoids 10 0 2 0 Cardiac Hypertension 34 13 4 <1 Edema peripheral 24 2 5 1 Ejection fraction decreased 16 3 5 2 Dermatology Rash 29 2 11 <1 Hand-foot syndrome 29 8 1 0 Skin discoloration/yellow skin 25 <1 0 0 Dry skin 23 <1 7 0 Hair color changes 20 0 <1 0 Alopecia 14 0 9 0 Erythema 12 <1 1 0 Pruritus 12 <1 7 <1 Neurology Altered taste¶ 47 <1 15 0 Headache 23 1 19 0 Dizziness 11 <1 14 1 Musculoskeletal Back pain 28 5 14 2 Arthralgia 30 3 19 1 Pain in extremity/limb discomfort 40 5 30 2 Endocrine Hypothyroidism 16 2 1 0 Respiratory Cough 27 1 14 <1 Dyspnea 26 6 20 4 Nasopharyngitis 14 0 2 0 Oropharyngeal pain 14 <1 2 0 Upper respiratory tract infection 11 <1 2 0 Metabolism/Nutrition Anorexia# 48 3 42 2 Hemorrhage/Bleeding Bleeding, all sites 37 4Þ 10 1 Psychiatric Insomnia 15 <1 10 0 Depressionß 11 0 14 1 Treatment-emergent Grade 3–4 laboratory abnormalities are presented in Table 4.
Table 4. Laboratory Abnormalities Reported in Study 3 in ≥10% of Treatment-Naïve RCC Patients Who Received SUTENT or IFN-α Laboratory Parameter Treatment-Naïve RCC SUTENT (N=375) IFN-α (N=360) All Grades* % Grade 3–4*,† % All Grades* % Grade 3–4*,‡ % Abbreviations: ALT=alanine aminotransferase; AST=aspartate aminotransferase; IFN=interferon-α; N=number of patients; RCC=renal cell carcinoma. - * Common Terminology Criteria for Adverse Events (CTCAE), version 3.0.
- † Grade 4 laboratory abnormalities in patients on SUTENT included uric acid (14%), lipase (3%), neutrophils (2%), lymphocytes (2%), hemoglobin (2%), platelets (1%), amylase (1%), ALT (<1%), creatine kinase (<1%), creatinine (<1%), glucose increased (<1%), calcium decreased (<1%), phosphorous (<1%), potassium increased (<1%), and sodium decreased (<1%).
- ‡ Grade 4 laboratory abnormalities in patients on IFN-α included uric acid (8%), lymphocytes (2%), lipase (1%), neutrophils (1%), amylase (<1%), calcium increased (<1%), glucose decreased (<1%), potassium increased (<1%), and hemoglobin (<1%).
Gastrointestinal AST 56 2 38 2 ALT 51 3 40 2 Lipase 56 18 46 8 Alkaline phosphatase 46 2 37 2 Amylase 35 6 32 3 Total bilirubin 20 1 2 0 Indirect bilirubin 13 1 1 0 Renal/Metabolic Creatinine 70 <1 51 <1 Creatine kinase 49 2 11 1 Uric acid 46 14 33 8 Calcium decreased 42 1 40 1 Phosphorus 31 6 24 6 Albumin 28 1 20 0 Glucose increased 23 6 15 6 Sodium decreased 20 8 15 4 Glucose decreased 17 0 12 <1 Potassium increased 16 3 17 4 Calcium increased 13 <1 10 1 Potassium decreased 13 1 2 <1 Sodium increased 13 0 10 0 Hematology Neutrophils 77 17 49 9 Hemoglobin 79 8 69 5 Platelets 68 9 24 1 Lymphocytes 68 18 68 26 Leukocytes 78 8 56 2 Long-Term Safety in RCC
The long-term safety of SUTENT in patients with metastatic RCC was analyzed across 9 completed clinical studies conducted in the first-line, bevacizumab-refractory, and cytokine-refractory treatment settings. The analysis included 5739 patients, of whom 807 (14%) were treated for at least 2 years and 365 (6%) for at least 3 years. Prolonged treatment with SUTENT did not appear to be associated with new types of adverse reactions. There appeared to be no increase in the yearly incidence of adverse reactions at later time points. Hypothyroidism increased during the second year of treatment with new cases reported up to year 4.
Adjuvant Treatment of RCC
The safety of SUTENT was evaluated in S-TRAC, a randomized, double-blind, placebo-controlled trial in which patients who had undergone nephrectomy for RCC received SUTENT 50 mg daily (n=306) on Schedule 4/2 or placebo (n=304). The median duration of treatment was 12.4 months (range: 0.13–14.9) for SUTENT and 12.4 months (range: 0.03–13.7) for placebo. Permanent discontinuation due to an adverse reaction occurred in 28% of patients on SUTENT and 6% on placebo. Adverse reactions leading to permanent discontinuation in >2% of patients include hand-foot syndrome and fatigue/asthenia. Dosing interruptions or delays occurred in 166 (54%) and 84 (28%) patients on SUTENT and placebo, respectively. One hundred forty patients (45.8%) out of 306 patients in the SUTENT arm and 15 patients (5%) out of 304 patients in the placebo arm had dose reductions.
Table 5 compares the incidence of common (≥10%) treatment-emergent adverse reactions for patients receiving SUTENT versus placebo.
Table 5. Adverse Reactions Reported in S-TRAC in ≥10% of Patients With RCC Who Received SUTENT and More Commonly Than in Patients Given Placebo* Adverse Reaction Adjuvant Treatment of RCC SUTENT (N=306) Placebo (N=304) All Grades % Grade 3–4 % All Grades % Grade 3–4 % Abbreviations: ARs=adverse reactions; N=number of patients; RCC=renal cell carcinoma. - * Common Terminology Criteria for Adverse Events (CTCAE), version 3.0.
- † Includes edema localized, face edema, eyelid edema, periorbital edema, swelling face, and eye edema.
- ‡ Includes mucosal inflammation, stomatitis apthous ulcer, mouth ulceration, tongue ulceration, oropharyngeal pain and oral pain.
- § Includes abdominal pain, abdominal pain lower, and abdominal pain upper.
- ¶ Includes hypertension, blood pressure increased, blood pressure systolic increased, blood pressure diastolic increased, and hypertensive crisis.
- # Includes dermatitis, dermatitis psoriasiform, exfoliative rash, genital rash, rash, rash erythematous, rash follicular, rash generalized, rash macular, rash maculopapular, rash papular, and rash pruritic.
- Þ Includes ageusia, hypogeusia, and dysgeusia.
- ß Includes epistaxis, gingival bleeding, rectal hemorrhage, hemoptysis, anal hemorrhage, upper gastrointestinal hemorrhage, hematuria.
Any Adverse Reaction 99 60 88 15 Constitutional Fatigue/Asthenia 57 8 34 2 Localized edema† 18 <1 <1 0 Pyrexia 12 <1 6 0 Gastrointestinal Mucositis/Stomatitis‡ 61 6 15 0 Diarrhea 57 4 22 <1 Nausea 34 2 15 0 Dyspepsia 27 1 7 0 Abdominal pain§ 25 2 9 <1 Vomiting 19 2 7 0 Constipation 12 0 11 0 Cardiac Hypertension¶ 39 8 14 1 Edema/Peripheral edema 10 <1 7 0 Dermatology Hand-foot syndrome 50 16 10 <1 Hair color changes 22 0 2 0 Rash# 24 2 12 0 Skin discoloration/Yellow skin 18 0 1 0 Dry skin 14 0 6 0 Neurology Altered tasteÞ 38 <1 6 0 Headache 19 <1 12 0 Musculoskeletal Pain in extremity 15 <1 7 0 Arthralgia 11 <1 10 0 Endocrine Hypothyroidism/TSH increased 24 <1 4 0 Metabolism/Nutrition Anorexia/Decreased appetite 19 <1 5 0 Hemorrhage/Bleeding Bleeding events, all sitesß 24 <1 5 <1 Grade 4 adverse reactions in patients on SUTENT included hand-foot syndrome (1%), fatigue (<1%), abdominal pain (< 1%), stomatitis (<1%), and pyrexia (< 1%). Grade 4 adverse reactions in patients on placebo included asthenia (<1%) and hypertension (<1%).
Grade 3–4 laboratory abnormalities that occurred in ≥2% of patients receiving SUTENT include neutropenia (13%), thrombocytopenia (5%), leukopenia (3%), lymphopenia (3%), elevated alanine aminotransferase (2%), elevated aspartate aminotransferase (2%), hyperglycemia (2%), and hyperkalemia (2%).
Advanced Pancreatic Neuroendocrine Tumors (pNET)
The safety of SUTENT was evaluated in Study 6, a randomized, double-blind, placebo-controlled trial in which patients with progressive pNET received SUTENT 37.5 mg daily continuous dosing (n=83) or placebo (n=82). The median number of days on treatment was 139 days (range: 13–532 days) for patients on SUTENT and 113 days (range: 1–614 days) for patients on placebo. Nineteen patients (23%) on SUTENT and 4 patients (5%) on placebo were on study for >1 year. Dose interruptions occurred in 25 patients (30%) on SUTENT and 10 patients (12%) on placebo. Dose reductions occurred in 26 patients (31%) on SUTENT and 9 patients (11%) on placebo. Discontinuation rates due to adverse reactions were 22% for SUTENT and 17% for placebo.
Most treatment-emergent adverse reactions in both study arms were Grade 1 or 2 in severity. Grade 3 or 4 treatment-emergent adverse reactions were reported in 54% versus 50% of patients on SUTENT versus placebo, respectively. Table 6 compares the incidence of common (≥10%) treatment-emergent adverse reactions for patients receiving SUTENT and reported more commonly in patients receiving SUTENT than in patients receiving placebo.
Table 6. Adverse Reactions Reported in the pNET Study 6 in ≥10% of Patients Who Received SUTENT and More Commonly Than in Patients Given Placebo* Adverse Reaction pNET SUTENT (N=83) Placebo (N=82) All Grades % Grade 3–4† % All Grades % Grade 3–4 % Abbreviations: N=number of patients; pNET=pancreatic neuroendocrine tumors. - * Common Terminology Criteria for Adverse Events (CTCAE), version 3.0.
- † Grade 4 adverse reactions in patients on SUTENT included fatigue (1%).
- ‡ Includes aphthous stomatitis, gingival pain, gingivitis, glossitis, glossodynia, mouth ulceration, oral discomfort, oral pain, tongue ulceration, mucosal dryness, mucosal inflammation, and dry mouth.
- § Includes abdominal discomfort, abdominal pain, and abdominal pain upper.
- ¶ Includes hematemesis, hematochezia, hematoma, hemoptysis, hemorrhage, melena, and metrorrhagia.
Any Adverse Reaction 99 54 95 50 Constitutional Asthenia 34 5 27 4 Fatigue 33 5 27 9 Weight decreased 16 1 11 0 Gastrointestinal Diarrhea 59 5 39 2 Stomatitis/oral syndromes‡ 48 6 18 0 Nausea 45 1 29 1 Abdominal pain§ 39 5 34 10 Vomiting 34 0 31 2 Dyspepsia 15 0 6 0 Cardiac Hypertension 27 10 5 1 Dermatology Hair color changes 29 1 1 0 Hand-foot syndrome 23 6 2 0 Rash 18 0 5 0 Dry skin 15 0 11 0 Neurology Dysgeusia 21 0 5 0 Headache 18 0 13 1 Musculoskeletal Arthralgia 15 0 6 0 Psychiatric Insomnia 18 0 12 0 Hemorrhage/Bleeding Bleeding events¶ 22 0 10 4 Epistaxis 21 1 5 0 Table 7 provides common (≥10%) treatment-emergent laboratory abnormalities.
Table 7. Laboratory Abnormalities Reported in the pNET Study 6 in ≥10% of Patients Who Received SUTENT Laboratory Parameter pNET SUTENT Placebo N All Grades* % Grade 3–4*,† % N All Grades* % Grade 3–4*,‡ % Abbreviations: ALT=alanine aminotransferase; AST=aspartate aminotransferase; N=number of patients; pNET=pancreatic neuroendocrine tumors. - * Common Terminology Criteria for Adverse Events (CTCAE), version 3.0.
- † Grade 4 laboratory abnormalities in patients on SUTENT included creatinine (4%), lipase (4%), glucose decreased (2%), glucose increased (2%), neutrophils (2%), ALT (1%), AST (1%), platelets (1%), potassium increased (1%), and total bilirubin (1%).
- ‡ Grade 4 laboratory abnormalities in patients on placebo included creatinine (3%), alkaline phosphatase (1%), glucose increased (1%), and lipase (1%).
Gastrointestinal AST increased 82 72 5 80 70 3 ALT increased 82 61 4 80 55 3 Alkaline phosphatase increased 82 63 10 80 70 11 Total bilirubin increased 82 37 1 80 28 4 Amylase increased 74 20 4 74 10 1 Lipase increased 75 17 5 72 11 4 Renal/Metabolic Glucose increased 82 71 12 80 78 18 Albumin decreased 81 41 1 79 37 1 Phosphorus decreased 81 36 7 77 22 5 Calcium decreased 82 34 0 80 19 0 Sodium decreased 82 29 2 80 34 3 Creatinine increased 82 27 5 80 28 5 Glucose decreased 82 22 2 80 15 4 Potassium decreased 82 21 4 80 14 0 Magnesium decreased 52 19 0 39 10 0 Potassium increased 82 18 1 80 11 1 Hematology Neutrophils decreased 82 71 16 80 16 0 Hemoglobin decreased 82 65 0 80 55 1 Platelets decreased 82 60 5 80 15 0 Lymphocytes decreased 82 56 7 80 35 4 Venous Thromboembolic Events
In patients treated with SUTENT (N=7527) for GIST, advanced RCC, adjuvant treatment of RCC and pNET, 3.5% of patients experienced a venous thromboembolic event; 2.2% Grade 3–4.
Reversible Posterior Leukoencephalopathy Syndrome
There have been reports (<1%), some fatal, of patients presenting with seizures and radiological evidence of reversible posterior leukoencephalopathy syndrome (RPLS). Patients with seizures and signs/symptoms consistent with RPLS, such as hypertension, headache, decreased alertness, altered mental functioning, and visual loss, including cortical blindness, should be controlled with medical management including control of hypertension. Temporary suspension of SUTENT is recommended; following resolution, treatment may be resumed at the discretion of the treating healthcare provider.
Pancreatic Function
Pancreatitis was observed in 5 patients (1%) receiving SUTENT for treatment-naïve RCC compared to 1 patient (<1%) receiving IFN-α. In a trial of patients receiving adjuvant treatment for RCC, 1 patient (<1%) on SUTENT and none on placebo experienced pancreatitis. Pancreatitis was observed in 1 patient (1%) receiving SUTENT for pNET and 1 patient (1%) receiving placebo.
6.2 Postmarketing Experience
The following adverse reactions have been identified during post-approval use of SUTENT. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
- Blood and lymphatic system disorders: hemorrhage associated with thrombocytopenia1. Suspension of SUTENT is recommended; following resolution, treatment may be resumed at the discretion of the treating healthcare provider.
- Gastrointestinal disorders: esophagitis.
- Hepatobiliary disorders: cholecystitis, particularly acalculous cholecystitis.
- Immune system disorders: hypersensitivity reactions, including angioedema.
- Infections and infestations: serious infection (with or without neutropenia)1. The infections most commonly observed with SUTENT treatment include respiratory, urinary tract, skin infections, and sepsis/septic shock.
- Musculoskeletal and connective tissue disorders: fistula formation, sometimes associated with tumor necrosis and/or regression1; myopathy and/or rhabdomyolysis with or without acute renal failure1. Patients with signs or symptoms of muscle toxicity should be managed as per standard medical practice.
- Renal and urinary disorders: renal impairment and/or failure1.
- Respiratory disorders: pulmonary embolism1, pleural effusion1.
- Skin and subcutaneous tissue disorders: pyoderma gangrenosum, including positive dechallenges.
- Vascular disorders: arterial thromboembolic events1. The most frequent events included cerebrovascular accident, transient ischemic attack, and cerebral infarction.
- 1 including some fatalities.
-
7 DRUG INTERACTIONS
7.1 Effect of Other Drugs on SUTENT
Strong CYP3A4 Inhibitors
Co-administration with strong CYP3A4 inhibitors may increase sunitinib plasma concentrations [see Clinical Pharmacology (12.3)]. Select an alternate concomitant medication with no or minimal enzyme inhibition potential. Consider a dose reduction for SUTENT when it is co-administered with strong CYP3A4 inhibitors [see Dosage and Administration (2.5)].
Strong CYP3A4 Inducers
Co-administration with strong CYP3A4 inducers may decrease sunitinib plasma concentrations [see Clinical Pharmacology (12.3)]. Select an alternate concomitant medication with no or minimal enzyme induction potential. Consider a dose increase for SUTENT when it must be co-administered with CYP3A4 inducers [see Dosage and Administration (2.5)].
-
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
Based on animal reproduction studies and its mechanism of action, SUTENT can cause fetal harm when administered to a pregnant woman [see Clinical Pharmacology (12.1)]. There are no available data in pregnant women to inform a drug-associated risk. In animal developmental and reproductive toxicology studies, oral administration of sunitinib to pregnant rats and rabbits throughout organogenesis resulted in teratogenicity (embryolethality, craniofacial and skeletal malformations) at 5.5 and 0.3 times the AUC in patients administered the recommended daily doses (RDD), respectively (see Data). Advise pregnant women or females of reproductive potential of the potential hazard to a fetus.
The background risk of major birth defects and miscarriage for the indicated populations are unknown. However, the estimated background risk in the United States (U.S.) general population of major birth defects is 2%–4% and of miscarriage is 15%–20% of clinically recognized pregnancies.
Data
Animal Data
In a female fertility and early embryonic development study, female rats were administered oral sunitinib (0.5, 1.5, 5 mg/kg/day) for 21 days prior to mating and for 7 days after mating. Embryolethality was observed at 5 mg/kg/day (approximately 5 times the AUC in patients administered the RDD of 50 mg/day).
In embryo-fetal developmental toxicity studies, oral sunitinib was administered to pregnant rats (0.3, 1.5, 3, 5 mg/kg/day) and rabbits (0.5, 1, 5, 20 mg/kg/day) during the period of organogenesis. In rats, embryolethality and skeletal malformations of the ribs and vertebrae were observed at the dose of 5 mg/kg/day (approximately 5.5 times the systemic exposure [combined AUC of sunitinib + primary active metabolite] in patients administered the RDD). No adverse fetal effects were observed in rats at doses ≤3 mg/kg/day (approximately 2 times the AUC in patients administered the RDD). In rabbits, embryolethality was observed at 5 mg/kg/day (approximately 3 times the AUC in patients administered the RDD), and craniofacial malformations (cleft lip and cleft palate) were observed at ≥1 mg/kg/day (approximately 0.3 times the AUC in patients administered the RDD of 50 mg/day).
Sunitinib (0.3, 1, 3 mg/kg/day) was evaluated in a pre- and postnatal development study in pregnant rats. Maternal body weight gains were reduced during gestation and lactation at doses ≥1 mg/kg/day (approximately 0.5 times the AUC in patients administered the RDD). At 3 mg/kg/day (approximately 2 times the AUC in patients administered the RDD), reduced neonate body weights were observed at birth and persisted in the offspring of both sexes during the preweaning period and in males during postweaning period. No adverse developmental effects were observed at doses ≤1 mg/kg/day.
8.2 Lactation
There is no information regarding the presence of sunitinib and its metabolites in human milk. Sunitinib and its metabolites were excreted in rat milk at concentrations up to 12-fold higher than in plasma (see Data). Because of the potential for serious adverse reactions in breastfed infants from SUTENT, advise a lactating woman not to breastfeed during treatment with SUTENT and for at least 4 weeks after the last dose.
8.3 Females and Males of Reproductive Potential
Based on animal reproduction studies and its mechanism of action, SUTENT can cause fetal harm when administered to a pregnant woman [see Pregnancy (8.1) and Clinical Pharmacology (12.1)].
Pregnancy Testing
Females of reproductive potential should have a pregnancy test before treatment with SUTENT is started.
Contraception
Infertility
Based on findings in animals, male and female fertility may be compromised by treatment with SUTENT [see Nonclinical Toxicology (13.1)].
8.4 Pediatric Use
The safety and effectiveness of SUTENT in pediatric patients have not been established. Safety and pharmacokinetics of sunitinib were assessed in an open-label study (NCT00387920) in pediatric patients 2 years to <17 years of age (n=29) with refractory solid tumors. In addition, efficacy, safety and pharmacokinetics of sunitinib was assessed in another open-label study (NCT01462695) in pediatric patients 2 years to <17 years of age (n=27) with high-grade glioma or ependymoma. The maximum tolerated dose (MTD) normalized for body surface area (BSA) was lower in pediatric patients compared to adults. Sunitinib was poorly tolerated in pediatric patients. The occurrence of dose-limiting cardiotoxicity prompted an amendment of the NCT00387920 study to exclude patients with previous exposure to anthracyclines or cardiac radiation. No responses were reported in patients in either of the trials.
Apparent clearance and volume of distribution normalized for BSA for sunitinib and its active major metabolite were lower in pediatrics as compared to adults.
The effect on open tibial growth plates in pediatric patients who received SUTENT has not been adequately studied. See Juvenile Animal Toxicity Data below.
Juvenile Animal Toxicity Data
Physeal dysplasia was observed in cynomolgus monkeys with open growth plates treated for ≥3 months (3 month dosing 2, 6, 12 mg/kg/day; 8 cycles of dosing 0.3, 1.5, 6.0 mg/kg/day) with sunitinib at doses that were >0.4 times the RDD based on systemic exposure (AUC). In developing rats treated continuously for 3 months (1.5, 5.0, and 15.0 mg/kg) or 5 cycles (0.3, 1.5, and 6.0 mg/kg/day), bone abnormalities consisted of thickening of the epiphyseal cartilage of the femur and an increase of fracture of the tibia at doses ≥5 mg/kg (approximately 10 times the RDD based on AUC). Additionally, caries of the teeth were observed in rats at >5 mg/kg. The incidence and severity of physeal dysplasia were dose related and were reversible upon cessation of treatment; however, findings in the teeth were not. A no-effect level was not observed in monkeys treated continuously for 3 months, but was 1.5 mg/kg/day when treated intermittently for 8 cycles. In rats the no-effect level in bones was ≤2 mg/kg/day.
8.5 Geriatric Use
Of 825 patients with GIST or metastatic RCC who received SUTENT on clinical studies, 277 (34%) were 65 and over. In the pNET study, 22 patients (27%) who received SUTENT were 65 and over. No overall differences in safety or effectiveness were observed between younger and older patients. Among the 158 patients at least age 65 receiving adjuvant SUTENT/placebo for RCC, the hazard ratio for disease-free survival was 0.59 (95% CI: 0.36, 0.95). Among patients 65 years and older receiving adjuvant SUTENT/placebo for RCC, 50 patients (16%) in the SUTENT arm experienced a Grade 3–4 adverse reaction, compared to 15 patients (5%) in the placebo arm.
8.6 Hepatic Impairment
No starting dose adjustment is required in patients with mild or moderate (Child-Pugh Class A or B) hepatic impairment [see Clinical Pharmacology (12.3)]. SUTENT was not studied in patients with severe (Child-Pugh Class C) hepatic impairment.
8.7 Renal Impairment
No starting dose adjustment is recommended in patients with mild (CLcr 50 to 80 mL/min), moderate (CLcr 30 to <50 mL/min), or severe (CLcr <30 mL/min) renal impairment who are not on dialysis [see Clinical Pharmacology (12.3)].
In patients with end-stage renal disease (ESRD) on hemodialysis, no starting dose adjustment is recommended. However, subsequent doses may be increased gradually up to 2-fold based on safety and tolerability [see Clinical Pharmacology (12.3)].
-
10 OVERDOSAGE
Treatment of overdose with SUTENT should consist of general supportive measures. There is no specific antidote for overdosage with SUTENT. If indicated, elimination of unabsorbed drug should be achieved by emesis or gastric lavage. Cases of accidental overdose have been reported; these cases were associated with adverse reactions consistent with the known safety profile of SUTENT, or without adverse reactions. A case of intentional overdose involving the ingestion of 1500 mg of SUTENT in an attempted suicide was reported without adverse reaction. In nonclinical studies, mortality was observed following as few as 5 daily doses of 500 mg/kg (3000 mg/m2) in rats. At this dose, signs of toxicity included impaired muscle coordination, head shakes, hypoactivity, ocular discharge, piloerection, and gastrointestinal distress. Mortality and similar signs of toxicity were observed at lower doses when administered for longer durations.
-
11 DESCRIPTION
SUTENT, an oral multi-kinase inhibitor, is the malate salt of sunitinib. Sunitinib malate is described chemically as Butanedioic acid, hydroxy-, (2S)-, compound with N-[2-(diethylamino)ethyl]-5-[(Z)-(5-fluoro-1,2-dihydro-2-oxo-3H-indol-3-ylidine)methyl]-2,4-dimethyl-1H-pyrrole-3-carboxamide (1:1). The molecular formula is C22H27FN4O2 ∙ C4H6O5 and the molecular weight is 532.6 Daltons.
The chemical structure of sunitinib malate is:
Sunitinib malate is a yellow to orange powder with a pKa of 8.95. The solubility of sunitinib malate in aqueous media over the range pH 1.2 to pH 6.8 is in excess of 25 mg/mL. The log of the distribution coefficient (octanol/water) at pH 7 is 5.2.
SUTENT (sunitinib malate) capsules are supplied as printed hard shell capsules containing sunitinib malate equivalent to 12.5 mg, 25 mg, 37.5 mg or 50 mg of sunitinib together with mannitol, croscarmellose sodium, povidone (K-25) and magnesium stearate as inactive ingredients.
The orange gelatin capsule shells contain titanium dioxide and red iron oxide. The caramel gelatin capsule shells contain titanium dioxide, red iron oxide, yellow iron oxide, and black iron oxide. The yellow gelatin capsule shells contain titanium dioxide and yellow iron oxide. The white printing ink contains shellac, propylene glycol, sodium hydroxide, povidone, and titanium dioxide. The black printing ink contains shellac, propylene glycol, potassium hydroxide, and black iron oxide.
-
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Sunitinib is a small molecule that inhibits multiple receptor tyrosine kinases (RTKs), some of which are implicated in tumor growth, pathologic angiogenesis, and metastatic progression of cancer. Sunitinib was evaluated for its inhibitory activity against a variety of kinases (>80 kinases) and was identified as an inhibitor of platelet-derived growth factor receptors (PDGFRα and PDGFRβ), vascular endothelial growth factor receptors (VEGFR1, VEGFR2, and VEGFR3), stem cell factor receptor (KIT), Fms-like tyrosine kinase-3 (FLT3), colony stimulating factor receptor Type 1 (CSF-1R), and the glial cell-line derived neurotrophic factor receptor (RET). Sunitinib inhibition of the activity of these RTKs has been demonstrated in biochemical and cellular assays, and inhibition of function has been demonstrated in cell proliferation assays. The primary metabolite exhibits similar potency compared to sunitinib in biochemical and cellular assays.
Sunitinib inhibited the phosphorylation of multiple RTKs (PDGFRβ, VEGFR2, KIT) in tumor xenografts expressing RTK targets in vivo and demonstrated inhibition of tumor growth or tumor regression and/or inhibited metastases in some experimental models of cancer. Sunitinib demonstrated the ability to inhibit growth of tumor cells expressing dysregulated target RTKs (PDGFR, RET, or KIT) in vitro and to inhibit PDGFRβ- and VEGFR2-dependent tumor angiogenesis in vivo.
12.2 Pharmacodynamics
Cardiac Electrophysiology
SUTENT can cause QT interval prolongation in a dose-dependent manner, which may lead to an increased risk for ventricular arrhythmias including Torsade de Pointes [see Warnings and Precautions (5.3)].
12.3 Pharmacokinetics
The pharmacokinetics of sunitinib and sunitinib malate have been evaluated in healthy volunteers and in patients with solid tumors.
Sunitinib AUC and Cmax increase proportionately over a dose range of 25–100 mg (0.5 to 2 times the approved recommended 50 mg once daily dosage). The pharmacokinetics were similar in healthy subjects and in the solid tumor patients, including patients with GIST and RCC. No significant changes in the pharmacokinetics of sunitinib or the primary active metabolite were observed with repeated daily administration or with repeated cycles. With repeated daily administration, sunitinib accumulates 3- to 4-fold while the primary metabolite accumulates 7- to 10-fold. Steady-state concentrations of sunitinib and its primary active metabolite are achieved within 10 to 14 days. By Day 14, combined plasma concentrations of sunitinib and its active metabolite ranged from 63 to 101 ng/mL.
Absorption
Following oral administration of sunitinib, the time to maximum plasma concentration (Tmax) ranged from 6 to 12 hours.
Distribution
The apparent volume of distribution (Vd/F) for sunitinib is 2230 L. Binding of sunitinib and its primary active metabolite to human plasma protein in vitro is 95% and 90%, respectively, with no concentration dependence in the range of 100 to 4000 ng/mL.
Elimination
Following administration of a single oral dose in healthy volunteers, the terminal half-lives of sunitinib and its primary active metabolite are approximately 40 to 60 hours and 80 to 110 hours, respectively. Sunitinib total oral clearance (CL/F) ranged from 34 to 62 L/h with an interpatient variability of 40%.
Metabolism
Sunitinib is metabolized primarily by the cytochrome P450 enzyme, CYP3A4, to produce its primary active metabolite, which is further metabolized by CYP3A4. The primary active metabolite comprises 23% to 37% of the total exposure. After a radiolabeled dose, sunitinib and its active metabolite were the major drug-related compounds identified in plasma, accounting for 91.5% of radioactivity.
Specific Populations
No clinically significant differences in the pharmacokinetics of SUTENT or the primary active metabolite were observed based on age (18 to 84 years), body weight (34 to 168 kg), creatinine clearance, race (White, Black, or Asian), sex, or Eastern Cooperative Oncology Group (ECOG) score, mild (Child-Pugh Class A) or moderate (Child-Pugh Class B) hepatic impairment.
Renal Impairment
No clinically significant differences in the pharmacokinetics of sunitinib or its active metabolite were predicted or observed in patients with mild (CLcr 50 to 80 mL/min), moderate (CLcr 30 to <50 mL/min), or severe (CLcr <30 mL/min) renal impairment who are not on dialysis, compared to patients with normal renal function (CLcr >80 mL/min). Although sunitinib was not eliminated through hemodialysis, the sunitinib systemic exposure was 47% lower in patients with end stage renal disease (ESRD) on hemodialysis compared to patients with normal renal function.
Hepatic Impairment
No clinically significant differences in the pharmacokinetics of sunitinib or its active metabolite were predicted or observed in patients with mild exocrine (Child-Pugh Class A) or moderate (Child-Pugh Class B) hepatic impairment compared to patients with normal hepatic function.
Drug Interaction Studies
Clinical Studies
In Vitro Studies
In vitro studies in human hepatocytes and microsomes indicated that sunitinib and the primary active metabolite do not induce CYP1A2, CYP2E1, and CYP3A4/5, or inhibit CYP1A2, CYP2A6, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6, CYP2E1, CYP3A4/5, and CYP4A9/11 at clinically relevant concentrations.
-
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
The carcinogenic potential of sunitinib has been evaluated in 2 species: rasH2 transgenic mice and Sprague-Dawley rats. There were similar positive findings in both species. In rasH2 transgenic mice, gastroduodenal carcinomas and/or gastric mucosal hyperplasia, as well as an increased incidence of background hemangiosarcomas were observed at doses ≥25 mg/kg/day following daily dose administration of sunitinib in studies of 1 or 6 months duration. No proliferative changes were observed in rasH2 transgenic mice at 8 mg/kg/day. Similarly, in a 2-year rat carcinogenicity study, administration of sunitinib in 28-day cycles followed by 7-day dose-free periods resulted in findings of duodenal carcinoma at doses as low as 1 mg/kg/day (approximately 0.9 times the AUC in patients given the RDD of 50 mg/day). At the high dose of 3 mg/kg/day (approximately 8 times the AUC in patients at the RDD of 50 mg/day), the incidence of duodenal tumors was increased and was accompanied by findings of gastric mucous cell hyperplasia and by an increased incidence of pheochromocytoma and hyperplasia of the adrenal gland.
Sunitinib did not cause genetic damage when tested in in vitro assays (bacterial mutation [Ames test], human lymphocyte chromosome aberration) and an in vivo rat bone marrow micronucleus test.
In a female fertility and early embryonic development study, female rats were administered oral sunitinib (0.5, 1.5, 5 mg/kg/day) for 21 days prior to mating and for 7 days after mating. Preimplantation loss was observed in females administered 5 mg/kg/day (approximately 5 times the AUC in patients administered the RDD of 50 mg/day). No adverse effects on fertility were observed at doses ≤1.5 mg/kg/day (approximately 1 time the clinical AUC at the RDD of 50 mg/day). In addition, effects on the female reproductive system were identified in a 3-month oral repeat-dose monkey study (2, 6, 12 mg/kg/day). Ovarian changes (decreased follicular development) were noted at 12 mg/kg/day (approximately 5 times the AUC in patients administered the RDD), while uterine changes (endometrial atrophy) were noted at ≥2 mg/kg/day (approximately 0.4 times the AUC in patients administered the RDD). With the addition of vaginal atrophy, the uterine and ovarian effects were reproduced at 6 mg/kg/day (approximately 0.8 times the AUC in patients administered the RDD) in a 9-month monkey study (0.3, 1.5, and 6 mg/kg/day administered daily for 28 days followed by a 14 day respite).
In a male fertility study, no reproductive effects were observed in male rats dosed with 1, 3, or 10 mg/kg/day oral sunitinib for 58 days prior to mating with untreated females. Fertility, copulation, conception indices, and sperm evaluation (morphology, concentration, and motility) were unaffected by sunitinib at doses ≤10 mg/kg/day approximately ≥26 times the AUC in patients administered the RDD).
-
14 CLINICAL STUDIES
14.1 Gastrointestinal Stromal Tumor
Study 1
Study 1 (NCT#00075218) was a 2-arm, international, randomized, double-blind, placebo-controlled trial of SUTENT in patients with GIST who had disease progression during prior imatinib mesylate (imatinib) treatment or who were intolerant of imatinib. The objective was to compare time-to-tumor progression (TTP) in patients receiving SUTENT plus best supportive care versus patients receiving placebo plus best supportive care. Other objectives included progression-free survival (PFS), objective response rate (ORR), and overall survival (OS). Patients were randomized (2:1) to receive either 50 mg SUTENT or placebo orally, once daily, on Schedule 4/2 until disease progression or withdrawal from the study for another reason. Treatment was unblinded at the time of disease progression. Patients randomized to placebo were then offered crossover to open-label SUTENT and patients randomized to SUTENT were permitted to continue treatment per investigator judgment.
At the time of a prespecified interim analysis, the intent-to-treat (ITT) population included 312 patients. Two hundred seven (207) patients were randomized to the SUTENT arm and 105 patients were randomized to the placebo arm. Demographics were comparable between the SUTENT and placebo groups with regard to age (69% versus 72% <65 years for SUTENT versus placebo, respectively), gender (male: 64% versus 61%), race (White: 88% both arms, Asian: 5% both arms, Black: 4% both arms, remainder not reported), and performance status (ECOG 0: 44% versus 46%, ECOG 1: 55% versus 52%, and ECOG 2: 1% versus 2%). Prior treatment included surgery (94% versus 93%) and radiotherapy (8% versus 15%). Outcome of prior imatinib treatment was also comparable between arms with intolerance (4% versus 4%), progression within 6 months of starting treatment (17% versus 16%), or progression beyond 6 months (78% versus 80%) balanced.
The planned interim efficacy and safety analysis was performed after 149 TTP events had occurred. There was a statistically significant advantage for SUTENT over placebo in TTP, meeting the primary endpoint. Efficacy results are summarized in Table 8 and the Kaplan-Meier curve for TTP is shown in Figure 1.
Table 8. GIST Efficacy Results From Study 1 (Double-Blind Treatment Phase) Efficacy Parameter SUTENT
(N=207)Placebo
(N=105)p-value
(log-rank test)HR
(95% CI)Abbreviations: CI=confidence interval; GIST=gastrointestinal stromal tumor; HR=hazard ratio; N=number of patients; PR=partial response. - * Time from randomization to progression; deaths prior to documented progression were censored at time of last radiographic evaluation.
- † A comparison is considered statistically significant if the p-value is <0.00417 (O'Brien Fleming stopping boundary).
- ‡ Time from randomization to progression or death due to any cause.
- § Pearson chi-square test.
Time-to-tumor progression*
[median, weeks (95% CI)]27.3
(16.0, 32.1)6.4
(4.4, 10.0)<0.0001† 0.33
(0.23, 0.47)Progression-free survival‡
[median, weeks (95% CI)]24.1
(11.1, 28.3)6.0
(4.4, 9.9)<0.0001 0.33
(0.24, 0.47)Objective response rate (PR)
[%, (95% CI)]6.8
(3.7, 11.1)0 0.006§ Figure 1. Kaplan-Meier Curve of TTP in GIST Study 1 (Intent-to-Treat Population)
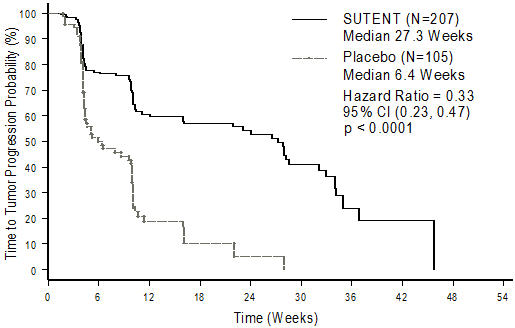
Abbreviations: CI=confidence interval; GIST=gastrointestinal stromal tumor; N=number of patients; TTP=time-to-tumor progression.
The final ITT population enrolled in the double-blind treatment phase of the study included 243 patients randomized to the SUTENT arm and 118 patients randomized to the placebo arm. After the primary endpoint was met at the interim analysis, the study was unblinded, and patients on the placebo arm were offered open-label SUTENT treatment. Ninety-nine (99) of the patients initially randomized to placebo crossed over to receive SUTENT in the open-label treatment phase. At the protocol specified final analysis of OS, the median OS was 72.7 weeks for the SUTENT arm and 64.9 weeks for the placebo arm [hazard ratio (HR)=0.876, 95% confidence interval (CI) (0.679, 1.129)].
Study 2
Study 2 was an open-label, multi-center, single-arm, dose-escalation study conducted in patients with GIST following progression on, or intolerance to imatinib. Following identification of the recommended regimen (50 mg once daily on Schedule 4/2), 55 patients in this study received the 50 mg dose of SUTENT on treatment Schedule 4/2. Partial responses (PR) were observed in 5 of 55 patients (9.1% PR rate; 95% CI: 3.0%, 20.0%).
14.2 Renal Cell Carcinoma
Treatment-Naïve RCC
Study 3 (NCT#00083889) was a multi-center, international, randomized study comparing single-agent SUTENT with IFN-α was conducted in patients with treatment-naïve RCC. The objective was to compare PFS in patients receiving SUTENT versus patients receiving IFN-α. Other endpoints included ORR, OS, and safety. Seven hundred fifty (750) patients were randomized (1:1) to receive either 50 mg SUTENT once daily on Schedule 4/2 or to receive IFN-α administered subcutaneously at 9 million international units (MIU) 3 times a week. Patients were treated until disease progression or withdrawal from the study.
The ITT population included 750 patients, 375 randomized to SUTENT and 375 randomized to IFN-α. Demographics were comparable between the SUTENT and IFN-α groups with regard to age (59% versus 67% <65 years for SUTENT versus IFN-α, respectively), gender (male: 71% versus 72%), race (White: 94% versus 91%, Asian: 2% versus 3%, Black: 1% versus 2%, remainder not reported), and performance status (ECOG 0: 62% versus 61%, ECOG 1: 38% each arm, ECOG 2: 0 versus 1%). Prior treatment included nephrectomy (91% versus 89%) and radiotherapy (14% each arm). The most common site of metastases present at screening was the lung (78% versus 80%, respectively), followed by the lymph nodes (58% versus 53%, respectively) and bone (30% each arm); the majority of the patients had multiple (2 or more) metastatic sites at baseline (80% versus 77%, respectively).
There was a statistically significant advantage for SUTENT over IFN-α in the endpoint of PFS (see Table 9 and Figure 2). In the prespecified stratification factors of lactate dehydrogenase (LDH) (>1.5 ULN versus ≤1.5 ULN), ECOG performance status (0 versus 1), and prior nephrectomy (yes versus no), the hazard ratio favored SUTENT over IFN-α. The ORR was higher in the SUTENT arm (see Table 9).
Table 9. Treatment-Naïve RCC Efficacy Results (Interim Analysis) Efficacy Parameter SUTENT
(N=375)IFN-α
(N=375)p-value
(log-rank test)HR
(95% CI)Abbreviations: CI=confidence interval; HR=hazard ratio; N=number of patients; INF-α=interferon-alfa; NA=not applicable; RCC=renal cell carcinoma. - * Assessed by blinded core radiology laboratory; 90 patients' scans had not been read at time of analysis.
- † A comparison is considered statistically significant if the p-value is <0.0042 (O'Brien Fleming stopping boundary).
- ‡ Pearson chi-square test.
Progression-free survival*
[median, weeks (95% CI)]47.3
(42.6, 50.7)22.0
(16.4, 24.0)<0.000001† 0.415
(0.320, 0.539)Objective response rate*
[%, (95% CI)]27.5
(23.0, 32.3)5.3
(3.3, 8.1)<0.001‡ NA Figure 2. Kaplan-Meier Curve of PFS in Treatment-Naïve RCC Study 3 (Intent-to-Treat Population)
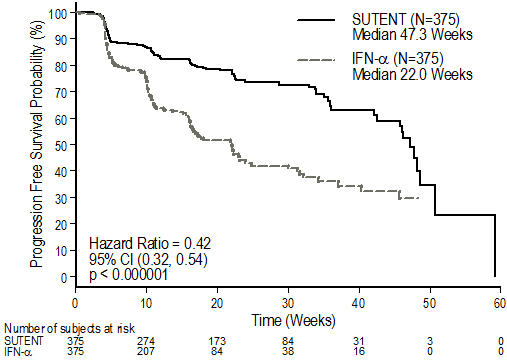
Abbreviations: CI=confidence interval; INF-α=interferon-alfa; N=number of patients; PFS=progression-free survival; RCC=renal cell carcinoma.
At the protocol-specified final analysis of OS, the median OS was 114.6 weeks for the SUTENT arm and 94.9 weeks for the IFN-α arm (HR=0.821; 95% CI: 0.673, 1.001). The median OS for the IFN-α arm includes 25 patients who discontinued IFN-α treatment because of disease progression and crossed over to treatment with SUTENT as well as 121 patients (32%) on the IFN-α arm who received post-study cancer treatment with SUTENT.
Cytokine-Refractory RCC
The use of single-agent SUTENT in the treatment of cytokine-refractory RCC was investigated in 2 single-arm, multi-center studies. All patients enrolled into these studies experienced failure of prior cytokine-based therapy. In Study 4 (NCT#00077974), failure of prior cytokine therapy was based on radiographic evidence of disease progression defined by response evaluation criteria in solid tumors (RECIST) or World Health Organization (WHO) criteria during or within 9 months of completion of 1 cytokine therapy treatment (IFN-α, interleukin-2, or IFN-α plus interleukin-2; patients who were treated with IFN-α alone must have received treatment for at least 28 days). In Study 5 (NCT#00054886), failure of prior cytokine therapy was defined as disease progression or unacceptable treatment-related toxicity. The endpoint for both studies was ORR. Duration of response (DR) was also evaluated.
One hundred and six patients (106) were enrolled into Study 4 and 63 patients were enrolled into Study 5. Patients received 50 mg SUTENT on Schedule 4/2. Therapy was continued until the patients met withdrawal criteria or had progressive disease. The baseline age, gender, race, and ECOG performance statuses of the patients were comparable between Studies 4 and 5. Approximately 86%–94% of patients in the 2 studies were White. Men comprised 65% of the pooled population. The median age was 57 years and ranged from 24 to 87 years in the studies. All patients had an ECOG performance status <2 at the screening visit.
The baseline malignancy and prior treatment history of the patients were comparable between Studies 4 and 5. Across the 2 studies, 95% of the pooled population of patients had at least some component of clear-cell histology. All patients in Study 4 were required to have a histological clear-cell component. Most patients enrolled in the studies (97% of the pooled population) had undergone nephrectomy; prior nephrectomy was required for patients enrolled in Study 4. All patients had received 1 previous cytokine regimen. Metastatic disease present at the time of study entry included lung metastases in 81% of patients. Liver metastases were more common in Study 4 (27% versus 16% in Study 5) and bone metastases were more common in Study 5 (51% versus 25% in Study 4); 52% of patients in the pooled population had at least 3 metastatic sites. Patients with known brain metastases or leptomeningeal disease were excluded from both studies.
The ORR and DR data from Studies 4 and 5 are provided in Table 10. There were 36 PRs in Study 4 as assessed by a core radiology laboratory for an ORR of 34.0% (95% CI: 25.0%, 43.8%). There were 23 PRs in Study 5 as assessed by the investigators for an ORR of 36.5% (95% CI: 24.7%, 49.6%). The majority (>90%) of objective disease responses were observed during the first 4 cycles; the latest reported response was observed in Cycle 10. DR data from Study 4 is premature as only 9 of 36 patients (25%) responding to treatment had experienced disease progression or died at the time of the data cutoff.
Table 10. Cytokine-Refractory RCC Efficacy Results Efficacy Parameter Study 4
(N=106)Study 5
(N=63)Abbreviations: CI=confidence interval; N=number of patients; NR=not reached; RCC=renal cell carcinoma. - * Assessed by blinded core radiology laboratory.
- † Assessed by investigators.
- ‡ Data not mature enough to determine upper confidence limit.
Objective response rate
[%, (95% CI)]34.0*
(25.0, 43.8)36.5†
(24.7, 49.6)Duration of response
[median, weeks (95% CI)]NR‡
(42.0, ‡)54†
(34.3, 70.1)Adjuvant Treatment of RCC
In the adjuvant treatment setting, SUTENT was investigated in S-TRAC (NCT#00375674), a multi-center, international, randomized, double-blind, placebo-controlled, trial in patients with high risk of recurrent RCC following nephrectomy. Patients were required to have clear cell histology and high risk of recurrence defined as ≥T3 and/or N+ tumors. Six hundred fifteen (615) patients were randomized 1:1 to receive either 50 mg SUTENT once daily on Schedule 4/2 or placebo. Patients were treated for 9 cycles (approximately 1 year), or until disease recurrence, unacceptable toxicity, or withdrawal of consent.
Demographics were generally comparable between the SUTENT and placebo arms with regard to age (median age 58 years), gender (73% male), and race (84% White, 12% Asian and 4% Other). At randomization, most patients had an ECOG performance status of 0 (74% SUTENT and 72% placebo). The remainder of the patients had an ECOG performance status of 1; 1 patient on SUTENT had a performance status of 2.
The major efficacy outcome measure was disease-free survival (DFS) in patients receiving SUTENT versus placebo as assessed by blinded independent central review (BICR). Overall survival was an additional endpoint. There was a statistically significant improvement in DFS in patients who were treated with SUTENT compared to placebo (Table 11 and Figure 3). Prespecified subgroup analyses are presented in Table 12. At the time of the DFS analysis, overall survival data were not mature, with 141/615 (23%) patient deaths.
Table 11. Disease-free Survival Results as Assessed by BICR in Adjuvant RCC (Intent to Treat Population) SUTENT
N = 309Placebo
N = 306p-value* HR* (95% CI) Abbreviations: BICR=blinded independent central review; CI=confidence interval; DFS=disease-free survival; HR=hazard ratio; N=number of patients; RCC=renal cell carcinoma. - * P-value based on log-rank test stratified by University of California Los Angeles Integrated Staging System (UISS) prognostic group; HR based on a Cox proportional hazard model stratified by UISS prognostic group
Median DFS [years (95% CI)] 6.8 (5.8, NR) 5.6 (3.8, 6.6) 0.03 0.76 (0.59, 0.98) DFS Events 113 (36.6%) 144 (47.1%) 5 Year DFS Rate 59.3% 51.3% Table 12. Disease-free Survival by Baseline Disease Characteristics Number of Events/ Total
n/NMedian DFS
[years (95% CI)]HR*
(95% CI)SUTENT Placebo SUTENT Placebo Abbreviations: CI=confidence interval; DFS=disease-free survival; HR=hazard ratio; N=number of patients; n=number of events; NR=not reached - * HR based on a Cox proportional hazards model
- † T3 Intermediate: T3, N0 or NX, M0, any Fuhrman's grade, ECOG PS 0 OR T3, N0 or NX, M0, Fuhrman's grade 1, ECOG PS ≥ 1
- ‡ T3 High: T3, N0 or NX, M0, Fuhrman's grade ≥ 2, ECOG PS ≥ 1
- § T4/Node Positive: T4, N0 or NX, M0, any Fuhrman's grade, any ECOG PS OR Any T, N1–2, M0, any Fuhrman's grade, any ECOG PS
T3 Intermediate† 35/115 46/112 NR
(5.2, NR)6.4
(4.7, NR)0.82
(0.53, 1.28)T3 High‡ 63/165 79/166 6.8
(5.0, NR)5.3
(2.9, NR)0.77
(0.55, 1.07)T4/Node Positive§ 15/29 19/28 3.5
(1.2, NR)1.7
(0.4, 3.0)0.62
(0.31, 1.23)Figure 3. Kaplan-Meier Curve of Disease-free Survival as Assessed by BICR (Intent-to-Treat Population)
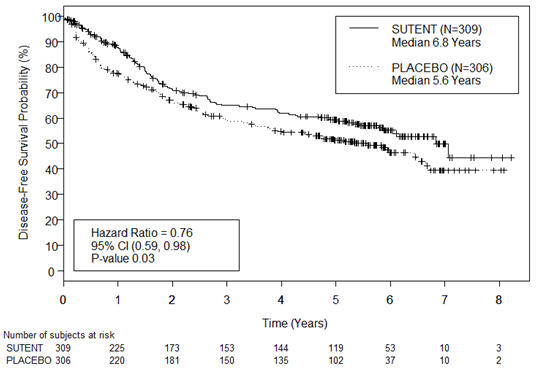
Abbreviations: BICR=blinded independent central review; CI=confidence interval; N=number of patients.
14.3 Pancreatic Neuroendocrine Tumors
Study 6 (NCT#00428597) was a multi-center, international, randomized, double-blind, placebo-controlled study of single-agent SUTENT conducted in patients with unresectable pNET. Patients were required to have documented RECIST-defined disease progression within the prior 12 months and were randomized (1:1) to receive either 37.5 mg SUTENT (N=86) or placebo (N=85) once daily without a scheduled off-treatment period. The primary objective was to compare PFS in patients receiving SUTENT versus patients receiving placebo. Other endpoints included OS, ORR, and safety. Use of somatostatin analogs was allowed in the study.
Demographics were comparable between the SUTENT and placebo groups. Additionally, 49% of SUTENT patients had nonfunctioning tumors vs 52% of placebo patients, and 92% patients in both arms had liver metastases. A total of 66% of SUTENT patients received prior systemic therapy compared with 72% of placebo patients and 35% of SUTENT patients had received somatostatin analogs compared with 38% of placebo patients. Patients were treated until disease progression or withdrawal from the study. Upon disease progression or study closure, patients were offered access to SUTENT in a separate extension study.
As recommended by the Independent Data Monitoring Committee, the study was terminated prematurely prior to the prespecified interim analysis. This may have led to an overestimate of the magnitude of PFS effect. A clinically significant improvement for SUTENT over placebo in PFS was seen by both investigator and independent assessment. A hazard ratio favoring SUTENT was observed in all subgroups of baseline characteristics evaluated. OS data were not mature at the time of the analysis. There were 9 deaths in the SUTENT arm and 21 deaths in the placebo arm. A statistically significant difference in ORR favoring SUTENT over placebo was observed. Efficacy results are summarized in Table 13 and the Kaplan-Meier curve for PFS is in Figure 4.
Table 13. pNET Study 6 Efficacy Results Efficacy Parameter SUTENT
(N=86)Placebo
(N=85)p-value HR
(95% CI)Abbreviations: CI=confidence interval; HR=hazard ratio; N=number of patients; NA=not applicable; pNET=pancreatic neuroendocrine tumors. - * 2-sided unstratified log-rank test.
- † Fisher's Exact test.
Progression-free survival
[median, months (95% CI)]10.2
(7.4, 16.9)5.4
(3.4, 6.0)0.000146* 0.427
(0.271, 0.673)Objective response rate
[%, (95% CI)]9.3
(3.2, 15.4)0 0.0066† NA Figure 4. Kaplan-Meier Curve of PFS in the pNET Study 6
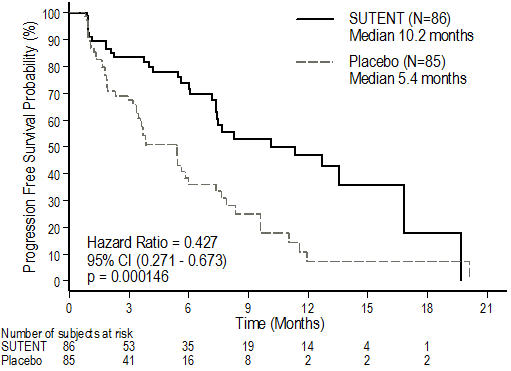
Abbreviations: CI=confidence interval; N=number of patients; PFS=progression-free survival; pNET=pancreatic neuroendocrine tumors.
-
16 HOW SUPPLIED/STORAGE AND HANDLING
12.5 mg capsules
Hard gelatin capsule with orange cap and orange body, printed with white ink "Pfizer" on the cap, "STN 12.5 mg" on the body; available in:
Bottles of 28 capsules: NDC: 0069-0550-3825 mg capsules
Hard gelatin capsule with caramel cap and orange body, printed with white ink "Pfizer" on the cap, "STN 25 mg" on the body; available in:
Bottles of 28 capsules: NDC: 0069-0770-3837.5 mg capsules
Hard gelatin capsule with yellow cap and yellow body, printed with black ink "Pfizer" on the cap, "STN 37.5 mg" on the body; available in:
Bottles of 28 capsules: NDC: 0069-0830-3850 mg capsules
Hard gelatin capsule with caramel cap and caramel body, printed with white ink "Pfizer" on the cap, "STN 50 mg" on the body; available in:
Bottles of 28 capsules: NDC: 0069-0980-38 -
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Medication Guide).
Hepatotoxicity
Inform patients of the signs and symptoms of hepatotoxicity. Advise patients to contact their healthcare provider immediately for signs or symptoms of hepatotoxicity [see Warnings and Precautions (5.1)].
Cardiovascular Events
Advise patients to contact their healthcare provider if they develop symptoms of heart failure [see Warnings and Precautions (5.2)].
QT Prolongation and Torsade de Pointes
Inform patients of the signs and symptoms of QT prolongation. Advise patients to contact their healthcare provider immediately in the event of syncope, pre-syncopal symptoms, and cardiac palpitations [see Warnings and Precautions (5.3)].
Hypertension
Inform patients of the signs and symptoms of hypertension. Advise patients to undergo routine blood pressure monitoring and to contact their health care provider if blood pressure is elevated or if they experience signs or symptoms of hypertension [see Warnings and Precautions (5.4)].
Hemorrhagic Events
Advise patients that SUTENT can cause severe bleeding. Advise patients to immediately contact their healthcare provider for bleeding or symptoms of bleeding [see Warnings and Precautions (5.5)].
Gastrointestinal Disorders
Advise patients that gastrointestinal disorders such as diarrhea, nausea, vomiting, and constipation may develop during SUTENT treatment and to seek immediate medical attention if they experience persistent or severe abdominal pain because cases of gastrointestinal perforation and fistula have been reported in patients taking SUTENT [see Warnings and Precautions (5.5) and Adverse Reactions (6.1)].
Dermatologic Effects and Toxicities
Advise patients that depigmentation of the hair or skin may occur during treatment with SUTENT due to the drug color (yellow). Other possible dermatologic effects may include dryness, thickness or cracking of skin, blister or rash on the palms of the hands and soles of the feet. Severe dermatologic toxicities including Stevens-Johnson syndrome, Toxic Epidermal Necrolysis, erythema multiforme, and necrotizing fasciitis have been reported. Advise patients to immediately inform their healthcare provider if severe dermatologic reactions occur [see Warnings and Precautions (5.9) and Adverse Reactions (6.1)].
Thyroid Dysfunction
Advise patients that SUTENT can cause thyroid dysfunction. Advise patient to contact their healthcare provider if symptoms of abnormal thyroid function occur [see Warnings and Precautions (5.10)].
Hypoglycemia
Advise patients that SUTENT can cause severe hypoglycemia and may be more severe in patients with diabetes taking antidiabetic medications. Inform patients of the signs, symptoms, and risks associated with hypoglycemia. Advise patients to immediately inform their healthcare provider if severe signs or symptoms of hypoglycemia occur [see Warnings and Precautions (5.11)].
Osteonecrosis of the Jaw
Advise patients to consider preventive dentistry prior to treatment with SUTENT. Inform patients being treated with SUTENT, particularly who are receiving bisphosphonates, to avoid invasive dental procedures if possible [see Warnings and Precautions (5.12)].
If possible, avoid invasive dental procedures while on SUTENT treatment, particularly in patients receiving intravenous bisphosphonate therapy.
Concomitant Medications
Advise patients to inform their healthcare providers of all concomitant medications, including over-the-counter medications and dietary supplements [see Drug Interactions (7)].
Embryo-Fetal Toxicity
Advise females to inform their healthcare provider if they are pregnant or become pregnant. Inform female patients of the risk to a fetus and potential loss of the pregnancy [see Use in Specific Populations (8.1)].
Advise females of reproductive potential to use effective contraception during treatment and for 4 weeks after receiving the last dose of SUTENT [see Warnings and Precautions (5.14) and Use in Specific Populations (8.1, 8.3)].
Advise males with female partners of reproductive potential to use effective contraception during treatment and for 7 weeks after receiving the last dose of SUTENT [see Warnings and Precautions (5.14) and Use in Specific Populations (8.1, 8.3)].
Lactation
Advise lactating women not to breastfeed during treatment with SUTENT and for at least 4 weeks after the last dose [see Use in Specific Populations (8.2)].
Infertility
Advise patients that male and female fertility may be compromised by treatment with SUTENT [see Use in Specific Populations (8.3) and Nonclinical Toxicology (13.1)].
- SPL UNCLASSIFIED SECTION
-
MEDICATION GUIDE
This Medication Guide has been approved by the U.S. Food and Drug Administration. Revised: November 2017 MEDICATION GUIDE
SUTENT® (su TENT)
(sunitinib malate)
CapsulesWhat is the most important information I should know about SUTENT?
SUTENT can cause serious side effects including:-
Severe liver problems, that can lead to death. Tell your healthcare provider right away if you develop any of the following signs and symptoms of liver problems during treatment with SUTENT:
- itching
- yellow eyes or skin
- dark urine
- pain or discomfort in the right upper stomach area
See "What are the possible side effects of SUTENT?" for more information about side effects.What is SUTENT?
SUTENT is a prescription medicine used to treat:- a rare cancer of the stomach, bowel, or esophagus called gastrointestinal stromal tumor (GIST) and when:
- you have taken the medicine imatinib mesylate (Gleevec®) and it did not stop the cancer from growing, or
- you cannot take imatinib mesylate (Gleevec®).
- advanced kidney cancer (advanced renal cell carcinoma or RCC).
- adults with kidney cancer that has not spread (localized), and who are at high risk of RCC coming back again after having kidney surgery.
- a type of pancreatic cancer called pancreatic neuroendocrine tumors (pNET), that has progressed and cannot be treated with surgery.
Before taking SUTENT tell your healthcare provider about all of your medical conditions, including if you: - have any heart problems
- have high blood pressure
- have thyroid problems
- have a history of low blood sugar or diabetes
- have kidney function problems (other than cancer)
- have liver problems
- have any bleeding problem
- plan to have any surgery or dental procedures
- have seizures
- have or have had pain in the mouth, teeth or jaw, swelling or sores inside the mouth, numbness or a feeling of heaviness in the jaw, or loosening of a tooth
- are pregnant or plan to become pregnant. SUTENT can harm your unborn baby.
Females who are able to become pregnant:- Your healthcare provider should do a pregnancy test before you start treatment with SUTENT.
- You should use effective birth control (contraception) during treatment and for at least 4 weeks after your last dose of SUTENT.
- Tell your healthcare provider right away if you become pregnant or think you are pregnant during treatment with SUTENT.
SUTENT may cause fertility problems in males and females. Tell your healthcare provider if this is a concern for you. - are breastfeeding or plan to breastfeed. Do not breastfeed during treatment with SUTENT and for at least 4 weeks (1 month) after the last dose.
Tell your healthcare provider about all the medicines you take, including prescription medicines and over-the-counter medicines, vitamins, and herbal supplements. Using SUTENT with certain other medicines can cause serious side effects.
You may have an increased risk of severe jaw bone problems (osteonecrosis) if you take SUTENT and a bisphosphonate medicine. Especially tell your healthcare provider if you are taking or have taken an osteoporosis medicine.
Know the medicines you take. Keep a list of them to show your healthcare provider and pharmacist when you get a new medicine.How should I take SUTENT? - Take SUTENT exactly the way your healthcare provider tells you.
- Take SUTENT 1 time each day with or without food.
- If you take SUTENT for GIST or RCC, you will usually take your medicine for 4 weeks (28 days) and then stop for 2 weeks (14 days). This is 1 cycle of treatment. You will repeat this cycle for as long as your healthcare provider tells you to.
- If you take SUTENT for pNET, take it 1 time each day until your healthcare provider tells you to stop.
- Do not drink grapefruit juice or eat grapefruit during your treatment with SUTENT. They may cause you to have too much SUTENT in your body.
- Your healthcare provider may do blood tests before each cycle of treatment to check you for side effects.
- If you miss a dose of Sutent by less than 12 hours, take the missed dose right away. If you miss a dose of SUTENT by more than 12 hours, just take your next dose at your regular time. Do not make up the missed dose. Tell your healthcare provider about any missed dose.
- Call your healthcare provider right away, if you take too much SUTENT.
What are possible side effects of SUTENT?
SUTENT may cause serious side effects, including:- See "What is the most important information I should know about SUTENT?"
- Heart problems. Heart problems may include heart failure, heart attack and heart muscle problems (cardiomyopathy) that can lead to death. Tell your healthcare provider if you feel very tired, are short of breath, or have swollen feet and ankles. Your healthcare provider may stop your treatment with SUTENT if you have signs and symptoms of heart failure.
- Abnormal heart rhythm changes. Changes in the electrical activity of your heart called QT prolongation can cause irregular heart beats that can be life threatening. Your healthcare provider may do electrocardiograms and blood tests (electrolytes) to watch for these problems during your treatment with SUTENT. Tell your healthcare provider immediately if you feel dizzy, faint, or have abnormal heartbeats during your treatment with SUTENT
- you feel faint or lightheaded, or you pass out
- dizziness
- feel your heart beat is irregular or fast
- High blood pressure. High blood pressure is common with SUTENT, and may sometimes be severe. Follow your healthcare provider's instructions about having your blood pressure checked regularly. Call your healthcare provider if your blood pressure is high, or if you have any of the following signs or symptoms of high blood pressure:
- severe headache
- lightheadedness
- dizziness
- change in vision
Your healthcare provider may prescribe medicine for you to treat high blood pressure, if needed. Your healthcare provider may temporarily stop your treatment with SUTENT until your high blood pressure is controlled. - Bleeding problems. Bleeding is common with SUTENT, but SUTENT can also cause severe bleeding problems that can lead to death. Call your healthcare provider right away if you have any of these symptoms or a serious bleeding problem during treatment with SUTENT, including:
- painful, swollen stomach (abdomen)
- vomiting blood
- black, sticky stools
- bloody urine
- headache or change in your mental status
- coughing up blood
Your healthcare provider: - can tell you about other symptoms to watch for
- may do blood tests if needed and monitor you for bleeding
- Serious stomach and intestinal problems, that can sometimes lead to death. Some people have had tears in their stomach or intestine (perforation), or have developed an abnormal opening between the stomach and intestine (fistula). Get medical help right away if you get stomach-area (abdominal) pain that does not go away or is severe during treatment with SUTENT.
- Tumor lysis syndrome (TLS). TLS is caused by the fast breakdown of cancer cells and may lead to death. TLS can cause kidney failure and the need for dialysis treatment, abnormal heart rhythm, seizure, and sometimes death. Your healthcare provider may do blood tests to check you for TLS.
- Thrombotic microangiopathy (TMA) including thrombotic thrombocytopenia purpura (TTP) and hemolytic uremic syndrome (HUS). TMA is a condition that involves injury to the smallest blood vessels, and blood clots that can happen while taking SUTENT. TMA is accompanied by a decrease in red cells and cells that are involved with clotting. TMA may harm your body's organs such as the brain and kidneys, and can sometimes lead to death. Your healthcare provider may tell you to stop taking SUTENT if you develop TMA.
- Protein in your urine. Some people who have taken SUTENT have developed protein in their urine, and in some cases, kidney problems that can lead to death. Your healthcare provider will check you for this problem. If there is too much protein in your urine, your healthcare provider may tell you to stop taking SUTENT.
-
Serious skin and mouth reactions. Treatment with SUTENT has caused severe skin reactions that can lead to death, including:
- severe rash with blisters or peeling of the skin.
- painful sores or ulcers on the skin, lips or inside the mouth.
- tissue damage (necrotizing fasciitis).
- Thyroid problems. Your healthcare provider may do tests to check your thyroid function during SUTENT treatment. Tell your healthcare provider if you have any of the following signs and symptoms during your treatment with SUTENT:
- tiredness that gets worse and does not go away
- loss of appetite
- problems with heat
- feeling nervous or agitated, tremors
- sweating
- nausea or vomiting
- diarrhea
- fast heat rate
- weight gain or weight loss
- feeling depressed
- irregular menstrual periods or no menstrual periods
- headache
- hair loss
- Low blood sugar (hypoglycemia). Low blood sugar can happen with SUTENT, and may cause you to become unconscious, or you may need to be hospitalized. Low blood sugar with SUTENT may be worse in people who have diabetes and take antidiabetic medicines. Your healthcare provider should check your blood sugar levels regularly during treatment with SUTENT and may need to adjust the dose of your antidiabetic medicines. Signs and symptoms of low blood sugar may include:
- headache
- drowsiness
- weakness
- dizziness
- confusion
- irritability
- hunger
- fast heart beat
- sweating
- feeling jittery
Call your healthcare provider right away if you have any signs or symptoms of severe low blood sugar during your treatment with SUTENT. - Jaw-bone problems (osteonecrosis). Severe jaw bone problems have happened in some people who take SUTENT. Certain risk factors such as taking a bisphosphonate medicine or having dental disease may increase your risk of getting osteonecrosis. Your healthcare provider may tell you to see your dentist before you start taking SUTENT. Your healthcare provider may tell you to avoid dental procedures, if possible, during your treatment with SUTENT, especially if you are receiving a bisphosphonate medicine into a vein (intravenous).
-
Wound healing problems. Wounds may not heal properly during SUTENT treatment. Tell your healthcare provider if you have or plan to have any surgery before starting or during treatment with SUTENT.
- Your healthcare provider may tell you to temporarily stop taking SUTENT if you are planning to have certain types of surgery.
- Your healthcare provider should tell you when you may start taking SUTENT again after surgery.
- tiredness
- weakness
- diarrhea
- pain, swelling or sores inside of your mouth
- nausea
- loss of appetite
- indigestion
- vomiting
- stomach-area (abdominal) pain
- blisters or rash on the palms of your hands and soles of your feet
- high blood pressure
- taste changes
- low platelet counts
The medicine in SUTENT is yellow, and it may make your skin look yellow. Your skin and hair may get lighter in color. SUTENT may also cause other skin problems including: dryness, thickness or cracking of the skin.
These are not all of the possible side effects of SUTENT. For more information, ask your healthcare provider or pharmacist.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.How do I store SUTENT? - Store SUTENT at room temperature, between 68°F to 77°F (20°C to 25°C).
General information about the safe and effective use of SUTENT.
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use SUTENT for a condition for which it was not prescribed. Do not give SUTENT to other people, even if they have the same symptoms that you have. It may harm them.
You can ask your healthcare provider or pharmacist for information about SUTENT that is written for health professionals.What are the ingredients in SUTENT?
Active ingredient: sunitinib malate
Inactive ingredients: mannitol, croscarmellose sodium, povidone (K-25), and magnesium stearate.
Orange gelatin capsule shells: titanium dioxide, and red iron oxide.
Caramel gelatin capsule shells: titanium dioxide, red iron oxide, yellow iron oxide, and black iron oxide.
Yellow gelatin capsule shells: titanium dioxide and yellow iron oxide.
White printing ink: shellac, propylene glycol, sodium hydroxide, povidone, and titanium dioxide.
Black printing ink: shellac, propylene glycol, potassium hydroxide and black iron oxide.
Gleevec® is a registered trademark of Novartis Pharmaceuticals Corporation.
LAB-0361-10.0
For more information go to www.SUTENT.com or call 1-877-5-SUTENT. -
Severe liver problems, that can lead to death. Tell your healthcare provider right away if you develop any of the following signs and symptoms of liver problems during treatment with SUTENT:
-
PRINCIPAL DISPLAY PANEL - 12.5 mg Capsule Bottle Label
ALWAYS DISPENSE WITH MEDICATION GUIDE
NDC: 0069-0550-38
Pfizer
Sutent®
(sunitinib malate)12.5 mg*
Capsules
28 Capsules
Rx only
-
PRINCIPAL DISPLAY PANEL - 25 mg Capsule Bottle Label
ALWAYS DISPENSE WITH MEDICATION GUIDE
NDC: 0069-0770-38
Pfizer
Sutent®
(sunitinib malate)25 mg*
Capsules
28 Capsules
Rx only
-
PRINCIPAL DISPLAY PANEL - 50 mg Capsule Bottle Label
ALWAYS DISPENSE WITH MEDICATION GUIDE
NDC: 0069-0980-38
Pfizer
Sutent®
(sunitinib malate)50 mg*
Capsules
28 Capsules
Rx only
-
PRINCIPAL DISPLAY PANEL - 37.5 mg Capsule Bottle Label
ALWAYS DISPENSE WITH MEDICATION GUIDE
NDC: 0069-0830-38
Pfizer
Sutent®
(sunitinib malate)37.5 mg*
Capsules
28 Capsules
Rx only
-
INGREDIENTS AND APPEARANCE
SUTENT
sunitinib malate capsuleProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 0069-0550 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength SUNITINIB MALATE (UNII: LVX8N1UT73) (SUNITINIB - UNII:V99T50803M) SUNITINIB 12.5 mg Inactive Ingredients Ingredient Name Strength MANNITOL (UNII: 3OWL53L36A) CROSCARMELLOSE SODIUM (UNII: M28OL1HH48) POVIDONE K25 (UNII: K0KQV10C35) MAGNESIUM STEARATE (UNII: 70097M6I30) GELATIN, UNSPECIFIED (UNII: 2G86QN327L) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) FERRIC OXIDE RED (UNII: 1K09F3G675) SHELLAC (UNII: 46N107B71O) PROPYLENE GLYCOL (UNII: 6DC9Q167V3) SODIUM HYDROXIDE (UNII: 55X04QC32I) POVIDONE, UNSPECIFIED (UNII: FZ989GH94E) POTASSIUM HYDROXIDE (UNII: WZH3C48M4T) Product Characteristics Color ORANGE Score no score Shape CAPSULE Size 14mm Flavor Imprint Code Pfizer;STN;12;5;mg Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 0069-0550-38 28 in 1 BOTTLE; Type 0: Not a Combination Product 01/26/2006 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA021938 01/26/2006 SUTENT
sunitinib malate capsuleProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 0069-0770 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength SUNITINIB MALATE (UNII: LVX8N1UT73) (SUNITINIB - UNII:V99T50803M) SUNITINIB 25 mg Inactive Ingredients Ingredient Name Strength MANNITOL (UNII: 3OWL53L36A) CROSCARMELLOSE SODIUM (UNII: M28OL1HH48) POVIDONE K25 (UNII: K0KQV10C35) MAGNESIUM STEARATE (UNII: 70097M6I30) GELATIN, UNSPECIFIED (UNII: 2G86QN327L) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) FERRIC OXIDE RED (UNII: 1K09F3G675) FERRIC OXIDE YELLOW (UNII: EX438O2MRT) FERROSOFERRIC OXIDE (UNII: XM0M87F357) SHELLAC (UNII: 46N107B71O) PROPYLENE GLYCOL (UNII: 6DC9Q167V3) SODIUM HYDROXIDE (UNII: 55X04QC32I) POVIDONE, UNSPECIFIED (UNII: FZ989GH94E) POTASSIUM HYDROXIDE (UNII: WZH3C48M4T) Product Characteristics Color ORANGE, BROWN (caramel) Score no score Shape CAPSULE Size 16mm Flavor Imprint Code Pfizer;STN;25;mg Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 0069-0770-38 28 in 1 BOTTLE; Type 0: Not a Combination Product 01/26/2006 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA021938 01/26/2006 SUTENT
sunitinib malate capsuleProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 0069-0980 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength SUNITINIB MALATE (UNII: LVX8N1UT73) (SUNITINIB - UNII:V99T50803M) SUNITINIB 50 mg Inactive Ingredients Ingredient Name Strength MANNITOL (UNII: 3OWL53L36A) CROSCARMELLOSE SODIUM (UNII: M28OL1HH48) POVIDONE K25 (UNII: K0KQV10C35) MAGNESIUM STEARATE (UNII: 70097M6I30) GELATIN, UNSPECIFIED (UNII: 2G86QN327L) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) FERRIC OXIDE RED (UNII: 1K09F3G675) FERRIC OXIDE YELLOW (UNII: EX438O2MRT) FERROSOFERRIC OXIDE (UNII: XM0M87F357) SHELLAC (UNII: 46N107B71O) PROPYLENE GLYCOL (UNII: 6DC9Q167V3) SODIUM HYDROXIDE (UNII: 55X04QC32I) POVIDONE, UNSPECIFIED (UNII: FZ989GH94E) POTASSIUM HYDROXIDE (UNII: WZH3C48M4T) Product Characteristics Color BROWN (caramel) Score no score Shape CAPSULE Size 18mm Flavor Imprint Code Pfizer;STN;50;mg Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 0069-0980-38 28 in 1 BOTTLE; Type 0: Not a Combination Product 01/26/2006 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA021938 01/26/2006 SUTENT
sunitinib malate capsuleProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 0069-0830 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength SUNITINIB MALATE (UNII: LVX8N1UT73) (SUNITINIB - UNII:V99T50803M) SUNITINIB 37.5 mg Inactive Ingredients Ingredient Name Strength MANNITOL (UNII: 3OWL53L36A) CROSCARMELLOSE SODIUM (UNII: M28OL1HH48) POVIDONE K25 (UNII: K0KQV10C35) MAGNESIUM STEARATE (UNII: 70097M6I30) GELATIN, UNSPECIFIED (UNII: 2G86QN327L) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) FERRIC OXIDE RED (UNII: 1K09F3G675) FERRIC OXIDE YELLOW (UNII: EX438O2MRT) FERROSOFERRIC OXIDE (UNII: XM0M87F357) SHELLAC (UNII: 46N107B71O) PROPYLENE GLYCOL (UNII: 6DC9Q167V3) SODIUM HYDROXIDE (UNII: 55X04QC32I) POVIDONE, UNSPECIFIED (UNII: FZ989GH94E) POTASSIUM HYDROXIDE (UNII: WZH3C48M4T) Product Characteristics Color YELLOW Score no score Shape CAPSULE Size 16mm Flavor Imprint Code Pfizer;STN;37;5;mg Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 0069-0830-38 28 in 1 BOTTLE; Type 0: Not a Combination Product 07/12/2014 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date NDA NDA021938 07/12/2014 Labeler - Pfizer Laboratories Div Pfizer Inc (134489525) Establishment Name Address ID/FEI Business Operations Pfizer Ireland Pharmaceuticals 896090987 API MANUFACTURE(0069-0830, 0069-0980, 0069-0770, 0069-0550) Establishment Name Address ID/FEI Business Operations Pfizer Italia S.r.l. 458521908 ANALYSIS(0069-0550, 0069-0770, 0069-0830, 0069-0980) , MANUFACTURE(0069-0550, 0069-0770, 0069-0830, 0069-0980) , PACK(0069-0550, 0069-0770, 0069-0830, 0069-0980)

Trademark Results [SUTENT]
Mark Image Registration | Serial | Company Trademark Application Date |
|---|---|
 SUTENT 78750554 3170173 Live/Registered |
C.P. PHARMACEUTICALS INTERNATIONAL C.V. 2005-11-09 |
 SUTENT 78639799 not registered Dead/Abandoned |
Pharmacia & Upjohn Company LLC 2005-05-31 |
 SUTENT 76388649 2948764 Live/Registered |
C.P. PHARMACEUTICALS INTERNATIONAL C.V. 2002-03-26 |
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.