IMIPRAMINE PAMOATE capsule
Imipramine Pamoate by
Drug Labeling and Warnings
Imipramine Pamoate by is a Prescription medication manufactured, distributed, or labeled by Hikma Pharmaceuticals USA Inc, West-Ward Columbus Inc.. Drug facts, warnings, and ingredients follow.
Drug Details [pdf]
-
BOXED WARNING
(What is this?)
Suicidality and Antidepressant Drugs
Antidepressants increased the risk compared to placebo of suicidal thinking and behavior (suicidality) in children, adolescents, and young adults in short-term studies of major depressive disorder (MDD) and other psychiatric disorders. Anyone considering the use of imipramine pamoate or any other antidepressant in a child, adolescent, or young adult must balance this risk with the clinical need. Short-term studies did not show an increase in the risk of suicidality with antidepressants compared to placebo in adults beyond age 24; there was a reduction in risk with antidepressants compared to placebo in adults aged 65 and older. Depression and certain other psychiatric disorders are themselves associated with increases in the risk of suicide. Patients of all ages who are started on antidepressant therapy should be monitored appropriately and observed closely for clinical worsening, suicidality, or unusual changes in behavior. Families and caregivers should be advised of the need for close observation and communication with the prescriber. Imipramine pamoate is not approved for use in pediatric patients (see WARNINGS: Clinical Worsening and Suicide Risk, PRECAUTIONS: Information for Patients, and PRECAUTIONS: Pediatric Use).
-
DESCRIPTION
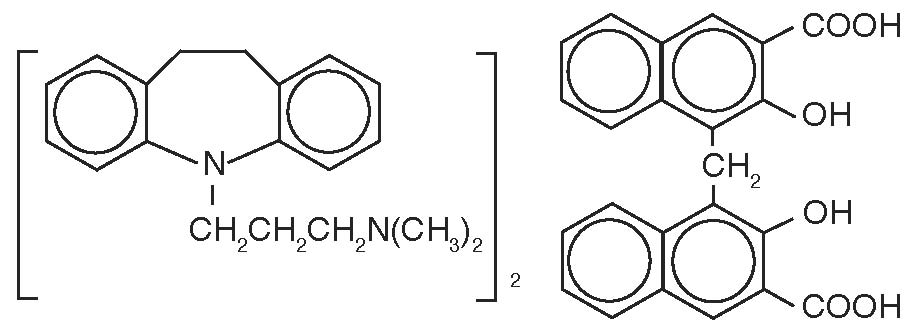
Imipramine Pamoate Capsules are a tricyclic antidepressant, available as capsules for oral administration. The 75 mg, 100 mg, 125 mg, and 150 mg capsules contain imipramine pamoate equivalent to 75 mg, 100 mg, 125 mg, and 150 mg of imipramine hydrochloride. Imipramine pamoate is 5-[3-(dimethylamino)propyl]-10,11-dihydro-5H-dibenz[b,f]azepine 4, 4'-methylenebis-(3-hydroxy-2-naphthoate) (2:1), and its structural formula is:
(C19H24N2)2●C23H16O6 M.W. = 949.18
Imipramine pamoate is a slightly yellow, crystalline powder. It is soluble in ethanol, in acetone, in ether, in chloroform, and in carbon tetrachloride, and is insoluble in water.
Inactive Ingredients: colloidal silicon dioxide, magnesium stearate, pregelatinized starch, sodium starch glycolate and talc.
Each capsule shell contains: black monogramming ink, FD&C Blue No. 1, FD&C Red No. 40, FD&C Yellow No. 6, gelatin, sodium lauryl sulfate and titanium dioxide. The 100 mg capsule shell also contains: D&C Yellow No. 10. The 125 mg capsule shell contains: FD&C Yellow No. 5. The black monogramming ink contains: ammonium hydroxide, iron oxide black, isopropyl alcohol, n-butyl alcohol, propylene glycol and shellac glaze.
- CLINICAL PHARMACOLOGY
- INDICATIONS AND USAGE
-
CONTRAINDICATIONS
Monoamine Oxidase Inhibitors (MAOIs)
The use of MAOIs intended to treat psychiatric disorders with imipramine pamoate or within 14 days of stopping treatment with imipramine pamoate is contraindicated because of an increased risk of serotonin syndrome. The use of imipramine pamoate within 14 days of stopping an MAOI intended to treat psychiatric disorders is also contraindicated (see WARNINGS and DOSAGE AND ADMINISTRATION).
Starting imipramine pamoate in a patient who is being treated with MAOIs such as linezolid or intravenous methylene blue is also contraindicated because of an increased risk of serotonin syndrome (see WARNINGS and DOSAGE AND ADMINISTRATION).
-
WARNINGS
Clinical Worsening and Suicide Risk
Patients with major depressive disorder (MDD), both adult and pediatric, may experience worsening of their depression and/or the emergence of suicidal ideation and behavior (suicidality) or unusual changes in behavior, whether or not they are taking antidepressant medications, and this risk may persist until significant remission occurs. Suicide is a known risk of depression and certain other psychiatric disorders, and these disorders themselves are the strongest predictors of suicide. There has been a long-standing concern, however, that antidepressants may have a role in inducing worsening of depression and the emergence of suicidality in certain patients during the early phases of treatment. Pooled analyses of short-term placebo-controlled trials of antidepressant drugs (SSRIs and others) showed that these drugs increase the risk of suicidal thinking and behavior (suicidality) in children, adolescents, and young adults (ages 18 to 24) with major depressive disorder (MDD) and other psychiatric disorders. Short-term studies did not show an increase in the risk of suicidality with antidepressants compared to placebo in adults beyond age 24; there was a reduction with antidepressants compared to placebo in adults aged 65 and older.
The pooled analyses of placebo-controlled trials in children and adolescents with MDD, obsessive compulsive disorder (OCD), or other psychiatric disorders included a total of 24 short-term trials of 9 antidepressant drugs in over 4400 patients. The pooled analyses of placebo-controlled trials in adults with MDD or other psychiatric disorders included a total of 295 short-term trials (median duration of 2 months) of 11 antidepressant drugs in over 77,000 patients. There was considerable variation in risk of suicidality among drugs, but a tendency toward an increase in the younger patients for almost all drugs studied. There were differences in absolute risk of suicidality across the different indications, with the highest incidence in MDD. The risk differences (drug vs placebo), however, were relatively stable within age strata and across indications. These risk differences (drug-placebo difference in the number of cases of suicidality per 1000 patients treated) are provided in Table 1.
Table 1 Age Range
Drug-Placebo Difference in Number of Cases of Suicidality per 1000 Patients Treated
Increases Compared to Placebo
<18
14 additional cases
18 to 24
5 additional cases
Decreases Compared to Placebo
25 to 64
1 fewer case
≥65
6 fewer cases
No suicides occurred in any of the pediatric trials. There were suicides in the adult trials, but the number was not sufficient to reach any conclusion about drug effect on suicide.
It is unknown whether the suicidality risk extends to longer-term use, i.e., beyond several months. However, there is substantial evidence from placebo-controlled maintenance trials in adults with depression that the use of antidepressants can delay the recurrence of depression.
All patients being treated with antidepressants for any indication should be monitored appropriately and observed closely for clinical worsening, suicidality, and unusual changes in behavior, especially during the initial few months of a course of drug therapy, or at times of dose changes, either increases or decreases.
The following symptoms, anxiety, agitation, panic attacks, insomnia, irritability, hostility, aggressiveness, impulsivity, akathisia (psychomotor restlessness), hypomania, and mania, have been reported in adult and pediatric patients being treated with antidepressants for major depressive disorder as well as for other indications, both psychiatric and nonpsychiatric. Although a causal link between the emergence of such symptoms and either the worsening of depression and/or the emergence of suicidal impulses has not been established, there is concern that such symptoms may represent precursors to emerging suicidality.
Consideration should be given to changing the therapeutic regimen, including possibly discontinuing the medication, in patients whose depression is persistently worse, or who are experiencing emergent suicidality or symptoms that might be precursors to worsening depression or suicidality, especially if these symptoms are severe, abrupt in onset, or were not part of the patient's presenting symptoms.
Families and caregivers of patients being treated with antidepressants for major depressive disorder or other indications, both psychiatric and nonpsychiatric, should be alerted about the need to monitor patients for the emergence of agitation, irritability, unusual changes in behavior, and the other symptoms described above, as well as the emergence of suicidality, and to report such symptoms immediately to healthcare providers. Such monitoring should include daily observation by families and caregivers. Prescriptions for imipramine pamoate should be written for the smallest quantity of capsules consistent with good patient management, in order to reduce the risk of overdose.
Screening Patients for Bipolar Disorder
A major depressive episode may be the initial presentation of bipolar disorder. It is generally believed (though not established in controlled trials) that treating such an episode with an antidepressant alone may increase the likelihood of precipitation of a mixed/manic episode in patients at risk for bipolar disorder. Whether any of the symptoms described above represent such a conversion is unknown. However, prior to initiating treatment with an antidepressant, patients with depressive symptoms should be adequately screened to determine if they are at risk for bipolar disorder; such screening should include a detailed psychiatric history, including a family history of suicide, bipolar disorder, and depression. It should be noted that imipramine pamoate is not approved for use in treating bipolar depression.
Extreme caution should be used when this drug is given to patients with cardiovascular disease because of the possibility of conduction defects, arrhythmias, congestive heart failure, myocardial infarction, strokes, and tachycardia. These patients require cardiac surveillance at all dosage levels of the drug; patients with increased intraocular pressure, history of urinary retention, or history of narrow-angle glaucoma because of the drug’s anticholinergic properties; hyperthyroid patients or those on thyroid medication because of the possibility of cardiovascular toxicity; patients with a history of seizure disorder because this drug has been shown to lower the seizure threshold; patients receiving guanethidine, clonidine, or similar agents, since imipramine pamoate may block the pharmacologic effects of these drugs; patients receiving methylphenidate hydrochloride. Since methylphenidate hydrochloride may inhibit the metabolism of imipramine pamoate, downward dosage adjustment of imipramine pamoate may be required when given concomitantly with methylphenidate hydrochloride.
Since imipramine pamoate may impair the mental and/or physical abilities required for the performance of potentially hazardous tasks, such as operating an automobile or machinery, the patient should be cautioned accordingly.
Imipramine pamoate capsules may enhance the CNS depressant effects of alcohol. Therefore, it should be borne in mind that the dangers inherent in a suicide attempt or accidental overdosage with the drug may be increased for the patient who uses excessive amounts of alcohol (see PRECAUTIONS).
Serotonin Syndrome
The development of a potentially life-threatening serotonin syndrome has been reported with SNRIs and SSRIs, including imipramine pamoate capsules, alone but particularly with concomitant use of other serotonergic drugs (including triptans, tricyclic antidepressants, fentanyl, lithium, tramadol, tryptophan, buspirone, and St. John’s Wort) and with drugs that impair metabolism of serotonin (in particular, MAOIs, both those intended to treat psychiatric disorders and also others, such as linezolid and intravenous methylene blue).
Serotonin syndrome symptoms may include mental status changes (e.g., agitation, hallucinations, delirium, and coma), autonomic instability (e.g., tachycardia, labile blood pressure, dizziness, diaphoresis, flushing, hyperthermia), neuromuscular changes (e.g., tremor, rigidity, myoclonus, hyperreflexia, incoordination), seizures, and/or gastrointestinal symptoms (e.g., nausea, vomiting, diarrhea). Patients should be monitored for the emergence of serotonin syndrome.
The concomitant use of imipramine pamoate capsules with MAOIs intended to treat psychiatric disorders is contraindicated. Imipramine pamoate should also not be started in a patient who is being treated with MAOIs such as linezolid or intravenous methylene blue. All reports with methylene blue that provided information on the route of administration involved intravenous administration in the dose range of 1 mg/kg to 8 mg/kg. No reports involved the administration of methylene blue by other routes (such as oral tablets or local tissue injection) or at lower doses. There may be circumstances when it is necessary to initiate treatment with an MAOI such as linezolid or intravenous methylene blue in a patient taking imipramine pamoate. Imipramine pamoate should be discontinued before initiating treatment with the MAOI (see CONTRAINDICATIONS and DOSAGE AND ADMINISTRATION).
If concomitant use of imipramine pamoate with other serotonergic drugs, including triptans, tricyclic antidepressants, fentanyl, lithium, tramadol, buspirone, tryptophan, and St. John’s Wort is clinically warranted, patients should be made aware of a potential increased risk for serotonin syndrome, particularly during treatment initiation and dose increases.
Treatment with imipramine pamoate and any concomitant serotonergic agents should be discontinued immediately if the above events occur and supportive symptomatic treatment should be initiated.
-
PRECAUTIONS
The 125 mg capsule contains FD&C Yellow No. 5 (tartrazine) which may cause allergic-type reactions (including bronchial asthma) in certain susceptible persons. Although the overall incidence of FD&C Yellow No. 5 (tartrazine) sensitivity in the general population is low, it is frequently seen in patients who also have aspirin hypersensitivity.
General
An ECG recording should be taken prior to the initiation of larger-than-usual doses of imipramine pamoate and at appropriate intervals thereafter until steady state is achieved. (Patients with any evidence of cardiovascular disease require cardiac surveillance at all dosage levels of the drug. See WARNINGS.) Elderly patients and patients with cardiac disease or a prior history of cardiac disease are at special risk of developing the cardiac abnormalities associated with the use of imipramine pamoate. It should be kept in mind that the possibility of suicide in seriously depressed patients is inherent in the illness and may persist until significant remission occurs. Such patients should be carefully supervised during the early phase of treatment with imipramine pamoate and may require hospitalization. Prescriptions should be written for the smallest amount feasible.
Hypomanic or manic episodes may occur, particularly in patients with cyclic disorders. Such reactions may necessitate discontinuation of the drug. If needed, imipramine pamoate may be resumed in lower dosage when these episodes are relieved. Administration of a tranquilizer may be useful in controlling such episodes.
An activation of the psychosis may occasionally be observed in schizophrenic patients and may require reduction of dosage and the addition of a phenothiazine.
Concurrent administration of imipramine pamoate with electroshock therapy may increase the hazards: such treatment should be limited to those patients for whom it is essential, since there is limited clinical experience.
Patients taking imipramine pamoate should avoid excessive exposure to sunlight since there have been reports of photosensitization.
Both elevation and lowering of blood sugar levels have been reported with imipramine pamoate use.
Imipramine pamoate should be used with caution in patients with significantly impaired renal or hepatic function.
Patients who develop a fever and a sore throat during therapy with imipramine pamoate should have leukocyte and differential blood counts performed.
Imipramine pamoate should be discontinued if there is evidence of pathological neutrophil depression.
Prior to elective surgery, imipramine pamoate should be discontinued for as long as the clinical situation will allow.
Information for Patients
Prescribers or other health professionals should inform patients, their families, and their caregivers about the benefits and risks associated with treatment with imipramine pamoate and should counsel them in its appropriate use. A patient Medication Guide about “Antidepressant Medicines, Depression and other Serious Mental Illness, and Suicidal Thoughts or Actions” is available for imipramine pamoate. The prescriber or health professional should instruct patients, their families, and their caregivers to read the Medication Guide and should assist them in understanding its contents. Patients should be given the opportunity to discuss the contents of the Medication Guide and to obtain answers to any questions they may have. The complete text of the Medication Guide is reprinted at the end of this document.
Patients should be advised of the following issues and asked to alert their prescriber if these occur while taking imipramine pamoate.
Clinical Worsening and Suicide Risk
Patients, their families, and their caregivers should be encouraged to be alert to the emergence of anxiety, agitation, panic attacks, insomnia, irritability, hostility, aggressiveness, impulsivity, akathisia (psychomotor restlessness), hypomania, mania, other unusual changes in behavior, worsening of depression, and suicidal ideation, especially early during antidepressant treatment and when the dose is adjusted up or down. Families and caregivers of patients should be advised to look for the emergence of such symptoms on a day-to-day basis, since changes may be abrupt. Such symptoms should be reported to the patient's prescriber or health professional, especially if they are severe, abrupt in onset, or were not part of the patient's presenting symptoms. Symptoms such as these may be associated with an increased risk for suicidal thinking and behavior and indicate a need for very close monitoring and possibly changes in the medication.
Patients should be advised that taking imipramine pamoate can cause mild pupillary dilation, which in susceptible individuals, can lead to an episode of angle-closure glaucoma. Pre-existing glaucoma is almost always open-angle glaucoma because angle-closure glaucoma, when diagnosed, can be treated definitively with iridectomy. Open-angle glaucoma is not a risk factor for angle-closure glaucoma. Patients may wish to be examined to determine whether they are susceptible to angle closure, and have a prophylactic procedure (e.g., iridectomy), if they are susceptible.
Drug Interactions
Drugs Metabolized by P450 2D6
The biochemical activity of the drug metabolizing isozyme cytochrome P450 2D6 (debrisoquin hydroxylase) is reduced in a subset of the Caucasian population (about 7% to 10% of Caucasians are so-called "poor metabolizers"); reliable estimates of the prevalence of reduced P450 2D6 isozyme activity among Asian, African, and other populations are not yet available. Poor metabolizers have higher than expected plasma concentrations of tricyclic antidepressants (TCAs) when given usual doses. Depending on the fraction of drug metabolized by P450 2D6, the increase in plasma concentration may be small, or quite large (8-fold increase in plasma AUC of the TCA).
In addition, certain drugs inhibit the activity of this isozyme and make normal metabolizers resemble poor metabolizers. An individual who is stable on a given dose of TCA may become abruptly toxic when given one of these inhibiting drugs as concomitant therapy. The drugs that inhibit cytochrome P450 2D6 include some that are not metabolized by the enzyme (quinidine; cimetidine) and many that are substrates for P450 2D6 (many other antidepressants, phenothiazines, and the Type 1C antiarrhythmics propafenone and flecainide). While all the selective serotonin reuptake inhibitors (SSRIs), e.g., fluoxetine, sertraline, and paroxetine, inhibit P450 2D6, they may vary in the extent of inhibition. The extent to which SSRI-TCA interactions may pose clinical problems will depend on the degree of inhibition and the pharmacokinetics of the SSRI involved. Nevertheless, caution is indicated in the co-administration of TCAs with any of the SSRIs and also in switching from one class to the other. Of particular importance, sufficient time must elapse before initiating TCA treatment in a patient being withdrawn from fluoxetine, given the long half-life of the parent and active metabolite (at least 5 weeks may be necessary).
Concomitant use of tricyclic antidepressants with drugs that can inhibit cytochrome P450 2D6 may require lower doses than usually prescribed for either the tricyclic antidepressant or the other drug. Furthermore, whenever one of these other drugs is withdrawn from co-therapy, an increased dose of tricyclic antidepressant may be required. It is desirable to monitor TCA plasma levels whenever a TCA is going to be co-administered with another drug known to be an inhibitor of P450 2D6.
The plasma concentration of imipramine may increase when the drug is given concomitantly with hepatic enzyme inhibitors (e.g., cimetidine, fluoxetine) and decrease by concomitant administration with hepatic enzyme inducers (e.g., barbiturates, phenytoin), and adjustment of the dosage of imipramine may therefore be necessary.
In occasional susceptible patients or in those receiving anticholinergic drugs (including antiparkinsonism agents) in addition, the atropine-like effects may become more pronounced (e.g., paralytic ileus). Close supervision and careful adjustment of dosage is required when imipramine pamoate is administered concomitantly with anticholinergic drugs.
Avoid the use of preparations, such as decongestants and local anesthetics, that contain any sympathomimetic amine (e.g., epinephrine, norepinephrine), since it has been reported that tricyclic antidepressants can potentiate the effects of catecholamines.
Caution should be exercised when imipramine pamoate is used with agents that lower blood pressure. Imipramine pamoate may potentiate the effects of CNS depressant drugs.
Patients should be warned that imipramine pamoate may enhance the CNS depressant effects of alcohol (see WARNINGS).
Monoamine Oxidase Inhibitors (MAOIs)
(See CONTRAINDICATIONS, WARNINGS, and DOSAGE AND ADMINISTRATION.)
Pregnancy
Animal reproduction studies have yielded inconclusive results (see also ANIMAL PHARMACOLOGY & TOXICOLOGY).
There have been no well-controlled studies conducted with pregnant women to determine the effect of imipramine on the fetus. However, there have been clinical reports of congenital malformations associated with the use of the drug. Although a causal relationship between these effects and the drug could not be established, the possibility of fetal risk from the maternal ingestion of imipramine cannot be excluded. Therefore, imipramine should be used in women who are or might become pregnant only if the clinical condition clearly justifies potential risk to the fetus.
Nursing Mothers
Limited data suggest that imipramine is likely to be excreted in human breast milk. As a general rule, a woman taking a drug should not nurse since the possibility exists that the drug may be excreted in breast milk and be harmful to the child.
Pediatric Use
Safety and effectiveness in the pediatric population have not been established (see BOX WARNING and WARNINGS: Clinical Worsening and Suicide Risk).
It is generally recommended that imipramine pamoate should not be used in children because of the increased potential for acute overdosage due to the high unit potency (75 mg, 100 mg, 125 mg, and 150 mg). Each capsule contains imipramine pamoate equivalent to 75 mg, 100 mg, 125 mg, or 150 mg imipramine hydrochloride. Anyone considering the use of imipramine pamoate in a child or adolescent must balance the potential risks with the clinical need.
Geriatric Use
In the literature, there were four well-controlled, randomized, double-blind, parallel group comparison clinical studies done with imipramine pamoate in the elderly population. There was a total number of 651 subjects included in these studies. These studies did not provide a comparison to younger subjects. There were no additional adverse experiences identified in the elderly.
Clinical studies of imipramine pamoate in the original application did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Post-marketing clinical experience has not identified differences in responses between the elderly and younger subjects. In general, dose selection for the elderly should be cautious, usually starting at the low end of the dosing range, reflecting greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
(See also DOSAGE AND ADMINISTRATION: Adolescent and Geriatric Patients)
(See also PRECAUTIONS: General)
-
ADVERSE REACTIONS
Note: Although the listing which follows includes a few adverse reactions which have not been reported with this specific drug, the pharmacological similarities among the tricyclic antidepressant drugs require that each of the reactions be considered when imipramine is administered.
Cardiovascular: Orthostatic hypotension, hypertension, tachycardia, palpitation, myocardial infarction, arrhythmias, heart block, ECG changes, precipitation of congestive heart failure, stroke.
Psychiatric: Confusional states (especially in the elderly) with hallucinations, disorientation, delusions; anxiety, restlessness, agitation; insomnia and nightmares; hypomania; exacerbation of psychosis.
Neurological: Numbness, tingling, paresthesias of extremities; incoordination, ataxia, tremors; peripheral neuropathy; extrapyramidal symptoms; seizures, alterations in EEG patterns; tinnitus.
Anticholinergic: Dry mouth, and, rarely, associated sublingual adenitis; blurred vision, disturbances of accommodation, mydriasis; constipation, paralytic ileus; urinary retention, delayed micturition, dilation of the urinary tract.
Allergic: Skin rash, petechiae, urticaria, itching, photosensitization; edema (general or of face and tongue); drug fever; cross-sensitivity with desipramine.
Hematologic: Bone marrow depression including agranulocytosis; eosinophilia; purpura; thrombocytopenia.
Gastrointestinal: Nausea and vomiting, anorexia, epigastric distress, diarrhea; peculiar taste, stomatitis, abdominal cramps, black tongue.
Endocrine: Gynecomastia in the male; breast enlargement and galactorrhea in the female; increased or decreased libido, impotence; testicular swelling; elevation or depression of blood sugar levels; inappropriate antidiuretic hormone (ADH) secretion syndrome.
Other: Jaundice (simulating obstructive); altered liver function; weight gain or loss; perspiration; flushing; urinary frequency; drowsiness, dizziness, weakness and fatigue; headache; parotid swelling; alopecia; proneness to falling.
Withdrawal Symptoms: Though not indicative of addiction, abrupt cessation of treatment after prolonged therapy may produce nausea, headache and malaise.
Postmarketing Experience
The following adverse drug reaction has been reported during post-approval use of imipramine pamoate. Because this reaction is reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate frequency.
Eye Disorders: Angle-closure glaucoma
-
OVERDOSAGE
Deaths may occur from overdosage with this class of drugs. Multiple drug ingestion (including alcohol) is common in deliberate tricyclic overdose. As the management is complex and changing, it is recommended that the physician contact a poison control center for current information on treatment. Signs and symptoms of toxicity develop rapidly after tricyclic overdose. Therefore, hospital monitoring is required as soon as possible.
Children have been reported to be more sensitive than adults to an acute overdosage of imipramine pamoate. An acute overdose of any amount in infants or young children, especially, must be considered serious and potentially fatal.
Manifestations
These may vary in severity depending upon factors such as the amount of drug absorbed, the age of the patient, and the interval between drug ingestion and the start of treatment. Critical manifestations of overdose include cardiac dysrhythmias, severe hypotension, convulsions, and CNS depression including coma. Changes in the electrocardiogram, particularly in QRS axis or width, are clinically significant indicators of tricyclic toxicity.
Other CNS manifestations may include drowsiness, stupor, ataxia, restlessness, agitation, hyperactive reflexes, muscle rigidity, athetoid and choreiform movements.
Cardiac abnormalities may include tachycardia, and signs of congestive failure. Respiratory depression, cyanosis, shock, vomiting, hyperpyrexia, mydriasis, and diaphoresis may also be present.
Management
Obtain an ECG and immediately initiate cardiac monitoring. Protect the patient’s airway, establish an intravenous line, and initiate gastric decontamination. A minimum of 6 hours of observation with cardiac monitoring and observation for signs of CNS or respiratory depression, hypotension, cardiac dysrhythmias and/or conduction blocks, and seizures is necessary. If signs of toxicity occur at any time during this period, extended monitoring is required. There are case reports of patients succumbing to fatal dysrhythmias late after overdose; these patients had clinical evidence of significant poisoning prior to death and most received inadequate gastrointestinal decontamination. Monitoring of plasma drug levels should not guide management of the patient.
Gastrointestinal Decontamination
All patients suspected of tricyclic overdose should receive gastrointestinal decontamination. This should include large volume gastric lavage followed by activated charcoal. If consciousness is impaired, the airway should be secured prior to lavage. Emesis is contraindicated.
Cardiovascular
A maximal limb-lead QRS duration of ≥0.1 seconds may be the best indication of the severity of the overdose. Intravenous sodium bicarbonate should be used to maintain the serum pH in the range of 7.45 to 7.55. If the pH response is inadequate, hyperventilation may also be used. Concomitant use of hyperventilation and sodium bicarbonate should be done with extreme caution, with frequent pH monitoring. A pH >7.6 or a pCO2 <20 mmHg is undesirable.
Dysrhythmias unresponsive to sodium bicarbonate therapy/hyperventilation may respond to lidocaine, bretylium, or phenytoin. Type 1A and 1C antiarrhythmics are generally contraindicated (e.g., quinidine, disopyramide, and procainamide).
In rare instances, hemoperfusion may be beneficial in acute refractory cardiovascular instability in patients with acute toxicity. However, hemodialysis, peritoneal dialysis, exchange transfusions, and forced diuresis generally have been reported as ineffective in tricyclic poisoning.
CNS
In patients with CNS depression, early intubation is advised because of the potential for abrupt deterioration. Seizures should be controlled with benzodiazepines, or if these are ineffective, other anticonvulsants (e.g., phenobarbital, phenytoin). Physostigmine is not recommended except to treat life-threatening symptoms that have been unresponsive to other therapies, and then only in consultation with a poison control center.
-
DOSAGE AND ADMINISTRATION
The following recommended dosages for imipramine pamoate should be modified as necessary by the clinical response and any evidence of intolerance.
Initial Adult Dosage
Outpatients
Therapy should be initiated at 75 mg/day. Dosage may be increased to 150 mg/day which is the dose level at which optimum response is usually obtained. If necessary, dosage may be increased to 200 mg/day.
Dosage higher than 75 mg/day may also be administered on a once-a-day basis after the optimum dosage and tolerance have been determined. The daily dosage may be given at bedtime. In some patients it may be necessary to employ a divided-dose schedule.
As with all tricyclics, the antidepressant effect of imipramine may not be evident for one to three weeks in some patients.
Hospitalized Patients
Therapy should be initiated at 100 to 150 mg/day and may be increased to 200 mg/day. If there is no response after two weeks, dosage should be increased to 250 to 300 mg/day.
Dosage higher than 150 mg/day may also be administered on a once-a-day basis after the optimum dosage and tolerance have been determined. The daily dosage may be given at bedtime. In some patients it may be necessary to employ a divided-dose schedule.
As with all tricyclics, the antidepressant effect of imipramine may not be evident for one to three weeks in some patients.
Adult Maintenance Dosage
Following remission, maintenance medication may be required for a longer period of time at the lowest dose that will maintain remission after which the dosage should gradually be decreased.
The usual maintenance dosage is 75 to 150 mg/day. The total daily dosage can be administered on a once-a-day basis, preferably at bedtime. In some patients it may be necessary to employ a divided-dose schedule.
In cases of relapse due to premature withdrawal of the drug, the effective dosage of imipramine should be reinstituted.
Adolescent and Geriatric Patients
Therapy in these age groups should be initiated with imipramine pamoate tablets at a total daily dosage of 25 to 50 mg, since imipramine pamoate capsules are not available in these strengths. Dosage may be increased according to response and tolerance, but it is generally unnecessary to exceed 100 mg/day in these patients. Imipramine pamoate capsules may be used when total daily dosage is established at 75 mg or higher.
The total daily dosage can be administered on a once-a-day basis, preferably at bedtime. In some patients it may be necessary to employ a divided-dose schedule.
As with all tricyclics, the antidepressant effect of imipramine may not be evident for one to three weeks in some patients.
Adolescent and geriatric patients can usually be maintained at lower dosage. Following remission, maintenance medication may be required for a longer period of time at the lowest dose that will maintain remission after which the dosage should gradually be decreased.
The total daily maintenance dosage can be administered on a once-a-day basis, preferably at bedtime. In some patients it may be necessary to employ a divided-dose schedule.
In cases of relapse due to premature withdrawal of the drug, the effective dosage of imipramine should be reinstituted.
Switching a Patient To or From a Monoamine Oxidase Inhibitor (MAOI) Intended to Treat Psychiatric Disorders
At least 14 days should elapse between discontinuation of an MAOI intended to treat psychiatric disorders and initiation of therapy with imipramine pamoate. Conversely, at least 14 days should be allowed after stopping imipramine pamoate before starting an MAOI intended to treat psychiatric disorders (see CONTRAINDICATIONS).
Use of Imipramine Pamoate with Other MAOIs, Such as Linezolid or Methylene Blue
Do not start imipramine pamoate in a patient who is being treated with linezolid or intravenous methylene blue because there is increased risk of serotonin syndrome. In a patient who requires more urgent treatment of a psychiatric condition, other interventions, including hospitalization, should be considered (see CONTRAINDICATIONS).
In some cases, a patient already receiving imipramine pamoate therapy may require urgent treatment with linezolid or intravenous methylene blue. If acceptable alternatives to linezolid or intravenous methylene blue treatment are not available and the potential benefits of linezolid or intravenous methylene blue treatment are judged to outweigh the risks of serotonin syndrome in a particular patient, imipramine pamoate should be stopped promptly, and linezolid or intravenous methylene blue can be administered. The patient should be monitored for symptoms of serotonin syndrome for two weeks or until 24 hours after the last dose of linezolid or intravenous methylene blue, whichever comes first. Therapy with imipramine pamoate may be resumed 24 hours after the last dose of linezolid or intravenous methylene blue (see WARNINGS).
The risk of administering methylene blue by non-intravenous routes (such as oral tablets or by local injection) or in intravenous doses much lower than 1 mg/kg with imipramine pamoate is unclear. The clinician should, nevertheless, be aware of the possibility of emergent symptoms of serotonin syndrome with such use (see WARNINGS).
-
HOW SUPPLIED
Imipramine Pamoate Capsules
75 mg capsules are supplied as light caramel opaque cap and light caramel opaque body with “54 591” printed on the cap and body, containing a light yellow to yellow powder.
NDC: 0054-0273-13: Bottle of 30 Capsules
NDC: 0054-0273-25: Bottle of 100 Capsules
100 mg capsules are supplied as light caramel opaque cap and rich yellow opaque body with “54 758” printed on the cap and body, containing a light yellow to yellow powder.
NDC: 0054-0274-13: Bottle of 30 Capsules
NDC: 0054-0274-25: Bottle of 100 Capsules
125 mg capsules are supplied as light caramel opaque cap and ivory opaque body with “54 466” printed on the cap and body, containing a light yellow to yellow powder.
NDC: 0054-0275-13: Bottle of 30 Capsules
150 mg capsules are supplied as light caramel opaque cap and light caramel opaque body with “54 161” printed on the cap and body, containing a light yellow to yellow powder.
NDC: 0054-0276-13: Bottle of 30 Capsules
NDC: 0054-0276-25: Bottle of 100 Capsules
Storage
Store at 20° to 25°C (68° to 77°F). [See USP Controlled Room Temperature.] Dispense in a tight, child-resistant container as defined in the USP/NF.
-
ANIMAL PHARMACOLOGY & TOXICOLOGY
A. Acute: Oral LD50:
-
Mouse 2185 mg/kg
-
Rat (F) 1142 mg/kg
- (M) 1807 mg/kg
- Rabbit 1016 mg/kg
-
Rat (F) 1142 mg/kg
- Dog 693 mg/kg (Emesis ED 50 )
B. Subacute
Two three-month studies in dogs gave evidence of an adverse drug effect on the testes, but only at the highest dose level employed, i.e., 90 mg/kg (10 times the maximum human dose). Depending on the histological section of the testes examined, the findings consisted of a range of degenerative changes up to and including complete atrophy of the seminiferous tubules, with spermatogenesis usually arrested.
Human studies show no definitive effect on sperm count, sperm motility, sperm morphology or volume of ejaculate.
Rat
One three-month study was done in rats at dosage levels comparable to those of the dog studies. No adverse drug effect on the testes was noted in this study, as confirmed by histological examination.
C. Reproduction/Teratogenic
Oral: Imipramine pamoate was fed to male and female albino rats for 28 weeks through two breeding cycles at dose levels of 15 mg/kg/day and 40 mg/kg/day (equivalent to 2 1/2 and 7 times the maximum human dose).
No abnormalities which could be related to drug administration were noted in gross inspection. Autopsies performed on pups from the second breeding likewise revealed no pathological changes in organs or tissues; however, a decrease in mean litter size from both matings was noted in the drug-treated groups and significant growth suppression occurred in the nursing pups of both sexes in the high group as well as in the females of the low-level group. Finally, the lactation index (pups weaned divided by number left to nurse) was significantly lower in the second litter of the high-level group.
Distr. by: West-Ward
Pharmaceuticals Corp.
Eatontown, NJ 07724
10005901/05
Revised August 2016
-
Mouse 2185 mg/kg
-
Medication Guide
Imipramine Pamoate Capsules
(im ip’ ra meen)
Rx Only
Antidepressant Medicines, Depression and other Serious Mental Illnesses, and Suicidal Thoughts or Actions
This product contains FD&C Yellow No. 5 (tartrazine) which may cause allergic-type reactions (including bronchial asthma) in certain susceptible persons. Although the overall incidence of FD&C Yellow No. 5 (tartrazine) sensitivity in the general population is low, it is frequently seen in patients who also have aspirin hypersensitivity.
Read the Medication Guide that comes with you or your family member’s antidepressant medicine. This Medication Guide is only about the risk of suicidal thoughts and actions with antidepressant medicines. Talk to your, or your family member’s, healthcare provider about:
- all risks and benefits of treatment with antidepressant medicines
- all treatment choices for depression or other serious mental illness
What is the most important information I should know about antidepressant medicines, depression and other serious mental illnesses, and suicidal thoughts or actions?
- 1. Antidepressant medicines may increase suicidal thoughts or actions in some children, teenagers, and young adults within the first few months of treatment.
- 2. Depression and other serious mental illnesses are the most important causes of suicidal thoughts and actions.Some people may have a particularly high risk of having suicidal thoughts or actions. These include people who have (or have a family history of) bipolar illness (also called manic-depressive illness) or suicidal thoughts or actions.
- 3. How can I watch for and try to prevent suicidal thoughts and actions in myself or a family member?
- Pay close attention to any changes, especially sudden changes, in mood, behaviors, thoughts, or feelings. This is very important when an antidepressant medicine is started or when the dose is changed.
- Call the healthcare provider right away to report new or sudden changes in mood, behavior, thoughts, or feelings.
- Keep all follow-up visits with the healthcare provider as scheduled. Call the healthcare provider between visits as needed, especially if you have concerns about symptoms.
Call a healthcare provider right away if you or your family member has any of the following symptoms, especially if they are new, worse, or worry you:
- thoughts about suicide or dying
- attempts to commit suicide
- new or worse depression
- new or worse anxiety
- feeling very agitated or restless
- panic attacks
- trouble sleeping (insomnia)
- new or worse irritability
- acting aggressive, being angry, or violent
- acting on dangerous impulses
- an extreme increase in activity and talking (mania)
- other unusual changes in behavior or mood
Visual problems
- eye pain
- changes in vision
- swelling or redness in or around the eye
Only some people are at risk for these problems. You may want to undergo an eye examination to see if you are at risk and receive preventative treatment if you are.
Who should not take imipramine pamoate capsules?
Do not take imipramine pamoate capsules if you:
-
take a monoamine oxidase inhibitor (MAOI). Ask your healthcare provider or pharmacist if you are not sure if you take an MAOI, including the antibiotic linezolid.
- o Do not take an MAOI within 2 weeks of stopping imipramine pamoate capsules unless directed to do so by your physician.
- o Do not start imipramine pamoate capsules if you stopped taking an MAOI in the last 2 weeks unless directed to do so by your physician.
What else do I need to know about antidepressant medicines?
- Never stop an antidepressant medicine without first talking to a healthcare provider. Stopping an antidepressant medicine suddenly can cause other symptoms.
- Antidepressants are medicines used to treat depression and other illnesses. It is important to discuss all the risks of treating depression and also the risks of not treating it. Patients and their families or other caregivers should discuss all treatment choices with the healthcare provider, not just the use of antidepressants.
- Antidepressant medicines have other side effects. Talk to the healthcare provider about the side effects of the medicine prescribed for you or your family member.
- Antidepressant medicines can interact with other medicines. Know all of the medicines that you or your family member takes. Keep a list of all medicines to show the healthcare provider. Do not start new medicines without first checking with your healthcare provider.
- Not all antidepressant medicines prescribed for children are FDA approved for use in children. Talk to your child’s healthcare provider for more information.
Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
This Medication Guide has been approved by the U.S. Food and Drug Administration.
Distr. by: West-Ward
Pharmaceuticals Corp.
Eatontown, NJ 07724
10005901/05
Revised August 2016
- PACKAGE/LABEL PRINCIPAL DISPLAY PANEL
- PACKAGE/LABEL PRINCIPAL DISPLAY PANEL
- PACKAGE/LABEL PRINCIPAL DISPLAY PANEL
- PACKAGE/LABEL PRINCIPAL DISPLAY PANEL
-
INGREDIENTS AND APPEARANCE
IMIPRAMINE PAMOATE
imipramine pamoate capsuleProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 0054-0273 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength IMIPRAMINE PAMOATE (UNII: MC34P30298) (IMIPRAMINE - UNII:OGG85SX4E4) IMIPRAMINE HYDROCHLORIDE 75 mg Inactive Ingredients Ingredient Name Strength SILICON DIOXIDE (UNII: ETJ7Z6XBU4) FD&C BLUE NO. 1 (UNII: H3R47K3TBD) FD&C RED NO. 40 (UNII: WZB9127XOA) FD&C YELLOW NO. 6 (UNII: H77VEI93A8) FERROSOFERRIC OXIDE (UNII: XM0M87F357) MAGNESIUM STEARATE (UNII: 70097M6I30) STARCH, CORN (UNII: O8232NY3SJ) SODIUM STARCH GLYCOLATE TYPE A POTATO (UNII: 5856J3G2A2) TALC (UNII: 7SEV7J4R1U) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) GELATIN, UNSPECIFIED (UNII: 2G86QN327L) Product Characteristics Color BROWN Score no score Shape CAPSULE Size 2mm Flavor Imprint Code 54;591 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 0054-0273-13 30 in 1 BOTTLE; Type 0: Not a Combination Product 04/19/2010 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA091099 04/19/2010 IMIPRAMINE PAMOATE
imipramine pamoate capsuleProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 0054-0274 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength IMIPRAMINE PAMOATE (UNII: MC34P30298) (IMIPRAMINE - UNII:OGG85SX4E4) IMIPRAMINE HYDROCHLORIDE 100 mg Inactive Ingredients Ingredient Name Strength SILICON DIOXIDE (UNII: ETJ7Z6XBU4) FD&C BLUE NO. 1 (UNII: H3R47K3TBD) FD&C RED NO. 40 (UNII: WZB9127XOA) FD&C YELLOW NO. 6 (UNII: H77VEI93A8) FERROUS OXIDE (UNII: G7036X8B5H) MAGNESIUM STEARATE (UNII: 70097M6I30) STARCH, CORN (UNII: O8232NY3SJ) SODIUM STARCH GLYCOLATE TYPE A POTATO (UNII: 5856J3G2A2) TALC (UNII: 7SEV7J4R1U) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) D&C YELLOW NO. 10 (UNII: 35SW5USQ3G) GELATIN, UNSPECIFIED (UNII: 2G86QN327L) Product Characteristics Color BROWN (Yellow) Score no score Shape CAPSULE Size 2mm Flavor Imprint Code 54;758 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 0054-0274-13 30 in 1 BOTTLE; Type 0: Not a Combination Product 04/19/2010 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA091099 04/19/2010 IMIPRAMINE PAMOATE
imipramine pamoate capsuleProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 0054-0275 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength IMIPRAMINE PAMOATE (UNII: MC34P30298) (IMIPRAMINE - UNII:OGG85SX4E4) IMIPRAMINE HYDROCHLORIDE 125 mg Inactive Ingredients Ingredient Name Strength SILICON DIOXIDE (UNII: ETJ7Z6XBU4) FD&C BLUE NO. 1 (UNII: H3R47K3TBD) FD&C RED NO. 40 (UNII: WZB9127XOA) FD&C YELLOW NO. 6 (UNII: H77VEI93A8) FERROUS OXIDE (UNII: G7036X8B5H) MAGNESIUM STEARATE (UNII: 70097M6I30) STARCH, CORN (UNII: O8232NY3SJ) SODIUM STARCH GLYCOLATE TYPE A POTATO (UNII: 5856J3G2A2) TALC (UNII: 7SEV7J4R1U) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) FD&C YELLOW NO. 5 (UNII: I753WB2F1M) GELATIN, UNSPECIFIED (UNII: 2G86QN327L) Product Characteristics Color BROWN (Ivory) Score no score Shape CAPSULE Size 2mm Flavor Imprint Code 54;466 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 0054-0275-13 30 in 1 BOTTLE; Type 0: Not a Combination Product 04/19/2010 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA091099 04/19/2010 IMIPRAMINE PAMOATE
imipramine pamoate capsuleProduct Information Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC: 0054-0276 Route of Administration ORAL Active Ingredient/Active Moiety Ingredient Name Basis of Strength Strength IMIPRAMINE PAMOATE (UNII: MC34P30298) (IMIPRAMINE - UNII:OGG85SX4E4) IMIPRAMINE HYDROCHLORIDE 150 mg Inactive Ingredients Ingredient Name Strength SILICON DIOXIDE (UNII: ETJ7Z6XBU4) FD&C BLUE NO. 1 (UNII: H3R47K3TBD) FD&C RED NO. 40 (UNII: WZB9127XOA) FD&C YELLOW NO. 6 (UNII: H77VEI93A8) FERROUS OXIDE (UNII: G7036X8B5H) MAGNESIUM STEARATE (UNII: 70097M6I30) STARCH, CORN (UNII: O8232NY3SJ) SODIUM STARCH GLYCOLATE TYPE A POTATO (UNII: 5856J3G2A2) TALC (UNII: 7SEV7J4R1U) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) GELATIN, UNSPECIFIED (UNII: 2G86QN327L) Product Characteristics Color BROWN Score no score Shape CAPSULE Size 2mm Flavor Imprint Code 54;161 Contains Packaging # Item Code Package Description Marketing Start Date Marketing End Date 1 NDC: 0054-0276-13 30 in 1 BOTTLE; Type 0: Not a Combination Product 04/19/2010 Marketing Information Marketing Category Application Number or Monograph Citation Marketing Start Date Marketing End Date ANDA ANDA091099 04/19/2010 Labeler - West-Ward Pharmaceuticals Corp. (080189610) Establishment Name Address ID/FEI Business Operations West-Ward Columbus Inc. 058839929 MANUFACTURE(0054-0273, 0054-0274, 0054-0275, 0054-0276)
© 2026 FDA.report
This site is not affiliated with or endorsed by the FDA.